You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- HeartsInHarmony PDFDocument103 pagesHeartsInHarmony PDFVanessa100% (9)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Botanical Drugs in Ayurveda and Traditional Chinese MedicineDocument50 pagesBotanical Drugs in Ayurveda and Traditional Chinese Medicinecharanmann9165No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- White Crane Medicine's Qi GongDocument5 pagesWhite Crane Medicine's Qi GongtansoeiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Helping Children and Youth With Self-Harm BehavioursDocument7 pagesHelping Children and Youth With Self-Harm BehavioursjanachidambaramNo ratings yet
- Vestibular Reha PDFDocument657 pagesVestibular Reha PDFRetnoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
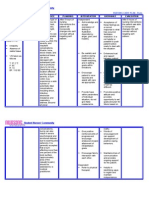
- Disseminated Intravascular CoagulationDocument2 pagesDisseminated Intravascular CoagulationGerardLum100% (1)
- Endodontic Clinic Manual 2015 - 1Document134 pagesEndodontic Clinic Manual 2015 - 1Adina Popa100% (2)
- Hypertension in PregnancyDocument5 pagesHypertension in PregnancyVammy Beverly ValentineNo ratings yet
- EC2021-Medical Electronics Notes For All Five UnitsDocument147 pagesEC2021-Medical Electronics Notes For All Five UnitsJason Jackson100% (1)
- 1 Burn NCPDocument2 pages1 Burn NCPkingjoy100% (1)
- Enoxaparin (Lovenox)Document1 pageEnoxaparin (Lovenox)ENo ratings yet
- Qualitative ResearchDocument14 pagesQualitative Researchhayleymeredith67% (3)
- European PRM Board ExamDocument23 pagesEuropean PRM Board ExamAmer WasimNo ratings yet
- Alzheimer's DiseaseDocument469 pagesAlzheimer's DiseaseGastón G. Fernández100% (3)
- Ebp Final ReflectionDocument2 pagesEbp Final Reflectionapi-239573049No ratings yet
- Meredith Lundquist Evidence Table FinaleditDocument24 pagesMeredith Lundquist Evidence Table Finaleditapi-239573049No ratings yet
- Opb Final ReflectionDocument2 pagesOpb Final Reflectionapi-239573049No ratings yet
- Article 3Document8 pagesArticle 3api-239573049No ratings yet
- Summerlin EvalDocument7 pagesSummerlin Evalapi-239573049No ratings yet
- Meredith Hayley-651 Occupational Profile & Intervention PlanDocument20 pagesMeredith Hayley-651 Occupational Profile & Intervention Planapi-239573049No ratings yet
- Reflection LeadershipDocument2 pagesReflection Leadershipapi-239573049No ratings yet
- Article 1Document7 pagesArticle 1api-239573049No ratings yet
- Reflection - Social JusticeDocument2 pagesReflection - Social Justiceapi-239573049No ratings yet
- Meredith, Hayley - Weekly Review FormsDocument9 pagesMeredith, Hayley - Weekly Review Formsapi-239573049No ratings yet
- Meredith Hayley - Personal Leadership Development PlanDocument5 pagesMeredith Hayley - Personal Leadership Development Planapi-239573049No ratings yet
- Meredith Hayley at Device Roll Wrap Yoga MatDocument14 pagesMeredith Hayley at Device Roll Wrap Yoga Matapi-239573049No ratings yet
- Immigrant PresentationDocument27 pagesImmigrant Presentationapi-239573049No ratings yet
- Meredith Lundquist CatDocument12 pagesMeredith Lundquist Catapi-239573049No ratings yet
- Group Activity AnalysisDocument10 pagesGroup Activity Analysisapi-239573049No ratings yet
- Professional Dev PlanDocument2 pagesProfessional Dev Planapi-239573049No ratings yet
- Hensley Meredith FieldworkevidencesynthesisDocument11 pagesHensley Meredith Fieldworkevidencesynthesisapi-239573049No ratings yet
- Semester 3 EvalDocument5 pagesSemester 3 Evalapi-239573049No ratings yet
- Meredith Hayley - Occupational Profile Intervention PlanDocument21 pagesMeredith Hayley - Occupational Profile Intervention Planapi-239573049No ratings yet
- Semester 4 EvalDocument4 pagesSemester 4 Evalapi-239573049No ratings yet
- Semester 2 EvalDocument4 pagesSemester 2 Evalapi-239573049No ratings yet
- Bishoff Hensley Hua Jerse Meredith Perea Group Case StudyDocument24 pagesBishoff Hensley Hua Jerse Meredith Perea Group Case Studyapi-254946087No ratings yet
- Quantitative PaperDocument17 pagesQuantitative PaperhayleymeredithNo ratings yet
- June 2007-NPT 1 - RationaleDocument15 pagesJune 2007-NPT 1 - Rationaleяoxel яayмoи eитяeиaNo ratings yet
- The Squiggle-Drawing Game in Child PsychotherapyDocument12 pagesThe Squiggle-Drawing Game in Child PsychotherapyCaramel GazelleNo ratings yet
- Barna Standards of Practice 2012Document42 pagesBarna Standards of Practice 2012evangelinaNo ratings yet
- Ce Booklet Fall 14Document28 pagesCe Booklet Fall 14api-279863771No ratings yet
- Sepsis Flow Chart FinalDocument2 pagesSepsis Flow Chart FinalDevindraPrptNo ratings yet
- Changing Face of Homoeopathic Pharmacy: Lecture by Dr. P. N. VarmaDocument44 pagesChanging Face of Homoeopathic Pharmacy: Lecture by Dr. P. N. VarmawasiuddinNo ratings yet
- What Is Mindfulness?Document2 pagesWhat Is Mindfulness?Vaseem SyedNo ratings yet
- Gap Co2 Cocc 2018Document9 pagesGap Co2 Cocc 2018Cesar Rivas CamposNo ratings yet
- Agency Treatment Service (S) Residential # Mat Slots # Detox Beds # Residential BedsDocument3 pagesAgency Treatment Service (S) Residential # Mat Slots # Detox Beds # Residential BedsNEWS CENTER Maine100% (1)
- Evaluation of A Trial of Syringe Vending Machines in Canberra, ACT, AustraliaDocument78 pagesEvaluation of A Trial of Syringe Vending Machines in Canberra, ACT, AustraliaDavid McDonaldNo ratings yet
- Case Study 2Document7 pagesCase Study 2desdav100% (1)
- Retinoblastoma Clinical and Pathological ClassificationDocument9 pagesRetinoblastoma Clinical and Pathological ClassificationSonia SaulésNo ratings yet
- Significance of History Taking Oral SurgeryDocument32 pagesSignificance of History Taking Oral SurgeryFourthMolar.com0% (1)
- 9694 s11 QP 21Document8 pages9694 s11 QP 21mstudy123456No ratings yet
- PsychiaDocument9 pagesPsychiaNoel RafaelNo ratings yet
- TMP - Neonatal Sundries CHeRP 2007522642027Document2 pagesTMP - Neonatal Sundries CHeRP 2007522642027sofyanbachriNo ratings yet
- Dosing and Administration Guide: IndicationDocument12 pagesDosing and Administration Guide: IndicationenggajbNo ratings yet