You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Belly Fat Diet John ChathamDocument92 pagesThe Belly Fat Diet John ChathamGurpreet Kaur100% (3)
- EMT Refresher FlyerDocument2 pagesEMT Refresher FlyerBillR.YoungNo ratings yet
- Know Your Council PDFDocument28 pagesKnow Your Council PDFAnonymous LH6vOd9IqNo ratings yet
- XG10000E (Manual Del Propietario)Document20 pagesXG10000E (Manual Del Propietario)Mauro GalloNo ratings yet
- CHN-RLE Module 3 (Bag Technique)Document5 pagesCHN-RLE Module 3 (Bag Technique)Ems Rio BalNo ratings yet
- 01 A History of The Pharmaceutical IndustryDocument8 pages01 A History of The Pharmaceutical IndustryHayat NaqviNo ratings yet
- End of Service Incubator 5400Document1 pageEnd of Service Incubator 5400Faizal FlNo ratings yet
- Paxica - Employee Handbook 08.01.2018Document30 pagesPaxica - Employee Handbook 08.01.2018Jelyn DeseoNo ratings yet
- Assessing and Managing Ineffective Tissue PerfusionDocument1 pageAssessing and Managing Ineffective Tissue PerfusionKryza CastilloNo ratings yet
- A Dangerous Divide: The State of Inequality in MalawiDocument24 pagesA Dangerous Divide: The State of Inequality in MalawiOxfamNo ratings yet
- PCWHS SSG PPAs Progress Report 2021 2022Document62 pagesPCWHS SSG PPAs Progress Report 2021 2022Tanglaw Laya May PagasaNo ratings yet
- Air PollutionDocument16 pagesAir Pollutionvgs127350% (2)
- Chison User Manual of Q9-V2.0-20140814Document232 pagesChison User Manual of Q9-V2.0-20140814WaleedNo ratings yet
- Physical Examination of The SkinDocument4 pagesPhysical Examination of The SkinJessica Febrina WuisanNo ratings yet
- BATTLE IN THE BRAIN: PROMOTING MENTAL HEALTH AWARENESSDocument12 pagesBATTLE IN THE BRAIN: PROMOTING MENTAL HEALTH AWARENESSJomerNo ratings yet
- Normalization ExercisesDocument6 pagesNormalization ExercisesWava Jahn Vargas100% (1)
- Ganesh Genesis Fire: Case StudyDocument22 pagesGanesh Genesis Fire: Case StudyAshishNo ratings yet
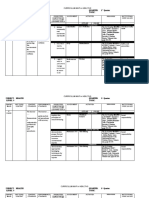
- The Learner The Learner : 1 QuarterDocument4 pagesThe Learner The Learner : 1 QuarterRode Jane SumambanNo ratings yet
- Uv Light Form Old ControlDocument7 pagesUv Light Form Old ControlAnonymous m0vmAykNo ratings yet
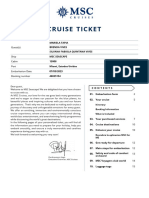
- Tickets CruceroDocument24 pagesTickets CruceroEugenio Alberto Neira VeraNo ratings yet
- Dental Ethics PrinciplesDocument25 pagesDental Ethics PrinciplesIbrahim AbdelHadiNo ratings yet
- 30 Day Porn-Free ChallengeDocument104 pages30 Day Porn-Free ChallengeGabriel Reis100% (2)
- General Questions About Sex: Frequently Asked Questions (Faqs)Document4 pagesGeneral Questions About Sex: Frequently Asked Questions (Faqs)Nitin DewanganNo ratings yet
- Guidelines For Farm TourismDocument14 pagesGuidelines For Farm TourismRAMJANNE12No ratings yet
- Global Pharmaceutical Industry-OverviewDocument6 pagesGlobal Pharmaceutical Industry-OverviewNaveen Reddy50% (4)
- Law of Persons Chapter 2 NotesDocument17 pagesLaw of Persons Chapter 2 Noteskeegan van ballegooyenNo ratings yet
- Republic V Cagandahan DigestDocument2 pagesRepublic V Cagandahan DigestJustin Paras100% (1)
- Albion Metal ChelationDocument6 pagesAlbion Metal ChelationI. Murali KrishnaNo ratings yet
- AUTISM CENTER Case Study by RedietDocument75 pagesAUTISM CENTER Case Study by RedietŘeðiét Ăłemñeh100% (1)
- Form 3 Meitheal Planning ReviewDocument3 pagesForm 3 Meitheal Planning ReviewtqsnrNo ratings yet