Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate
Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical College, B Y L Nair Hospital, Mumbai, India
Abstract: Background: Dizziness is a nonspecific term used by patients to describe a variety of symptoms. The terms dizziness, vertigo, faintness and blackouts are not synonymous but are often used interchangeably by patients. Postural blackout is a subtype of dizziness and is a result of postural hypotension, a feature of autonomic dysfunction. Case reports: We present detailed case histories of two patients treated elsewhere as postural dizziness and vertigo without a specific diagnosis. Postural blackouts were misinterpreted as postural dizziness and positional vertigo. On detailed evaluation these were postural hypotension (PH) and postural blackouts. There were additional features of autonomic dysfunction, parkinsonism and ataxia. A diagnosis of multiple system atrophy was made as per the second consensus statement on diagnosis of multiple system atrophy. Discussion: A clinical algorithm to evaluate dizziness subtypes is discussed. Clarification of the term dizziness is necessary for a correct etiological diagnosis. A detailed history, neurological examination, bedside autonomic function testing and follow up is necessary in all patients presenting with dizziness. Conclusion: Postural hypotension is an important cause of postural blackouts. Multiple system atrophy should be considered in patients with postural dizziness/blackouts. Key words: Dizziness, postural blackout, autonomic dysfunction, multiple system atrophy.
Introduction: Dizziness is a term used by patients to describe a variety of abnormal head sensations (usually disequilibrium). It may be described as a) sense of motion, spinning sensation, vertigo, b) imbalance or disequilibrium, c) impending loss of consciousness, presyncope, near faint, blackout d) syncope, e) seizure or f) lightheadedness due to psychiatric disorders like panic, hyperventilation. (1-3) Hence it is important to elucidate the meaning of dizziness and ask the patient to describe the abnormal sensation without using the word dizziness. Postural blackout Case Reports: Case 1: A 46 year old right handed man presented with dizziness, black-outs on standing, urinary frequency and thrashing movements of limbs during sleep since one and half years. Five months later he had gait ataxia. On examination he had significant orthostatic hypotension. Blood pressure was 140/90 mm of Hg when supine and 106/72 mm of Hg three minutes after standing. Hence detailed autonomic function testing was done. 30 seconds bradycardia: 15 seconds tachycardia ratio on standing was 0.95 (N >1.04). Valsalva ratio of the longest RR interval in phase 4 to the shortest RR interval in phase 2 of Valsalva maneuver was 1.20 (normal>1.45). Diastolic BP remained 90 mm of Hg on handgrip maneuvers and ice cold immersion testing. On
is a subtype of dizziness due to postural hypotension (PH). Medications, cardiovascular disorders and autonomic dysfunction are some of the causes of PH. We report two patients with recurrent postural blackouts due to PH being treated elsewhere as dizziness and positional vertigo. A methodical approach, detailed neurological evaluation and bedside autonomic function testing lead to the correct diagnosis of multiple system atrophy (MSA). We discuss the approach to patients presenting with symptoms of dizziness and postural blackouts. neurological examination his higher mental functions, speech, cranial nerves, motor examination, reflexes and sensory examination were unremarkable. He had significant gait ataxia and swayed on either side while walking. Magnetic resonance imaging (MRI) brain revealed ponto-cerebellar atrophy and hot cross bun sign. A diagnosis of probable Multiple system atrophy cerebellar variant (MSA-C) was made as per the second consensus statement for diagnosis of MSA.(4) He was advised to avoid rapid postural changes. He was symptomatically better with frequent liquid meals with extra salt, lower limb elastic compression stockings and antiTrendelenburg position during sleep. Dream enactment with thrashing limb movements during sleep (Rapid eye movement (REM) sleep behavior disorder) responded to clonazepam.
Case 2: A 50 year old man presented with urinary frequency and incontinence since four years. Three years later he had postural dizziness, black-outs, impotence eand thrashing movements of limbs in sleep. He had slowness of activity and rest tremors in both hands since last six months. On examination he had significant PH. Blood pressure was 102/60 mm of Hg when supine and 72/44 mm of Hg three minutes after standing. The 30 seconds bradycardia: 15 seconds tachycardia ratio was 0.94 (N >1.04). Valsalva ratio was 1.28 (normal>1.45). There was no diastolic rise in BP on handgrip maneuvers and ice cold immersion testing. On neurological examination higher mental functions, speech and cranial nerve examination was normal. There was
symmetrical bradykinesia and cogwheel rigidity. Power was normal, deep tendon reflexes were exaggerated with bilateral extensor plantar response. Sensory system was normal, there were no cerebellar signs and gait was normal. MRI Brain was normal. Diagnosis of probable MSA-Parkinsonian variant (MSA-P) was made as per the second consensus statement for diagnosis of MSA.(4) He was advised to avoid rapid postural changes. Postural symptoms improved with frequent liquid meals with extra salt, lower limb elastic compression stockings and antiTrendelenburg position. During sleep. Levodopa was started for parkinsonian symptoms. REM sleep behavior disorder responded to clonazepam.
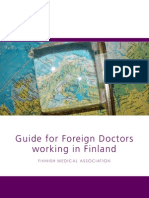
Dizziness
Loss of Consciousness Syncope * Head up Tilt test * Holter *Cardiac electrophysiology Seizure * EEG * CT/MRI
Vertigo Central Peripheral
* Hallpike Maneuver * Head impulse Test * Audiometry test * MRI/ MRA
Postural Blackouts * Medications * Diabetes
Ataxia Cerebellar Sensory
Vague/light headedness heaviness in the head * Anxiety
* MSA
* other neuropathies
* Depression
* Hyperventillation
Discussion: Both patients had symptoms of postural dizziness and blackouts due to orthostatic hypotension (OH). Case one had OH leading to postural blackouts from the onset. This was being treated as positional vertigo. Case two had urinary symptoms at the onset and developed postural blackouts three years later. On close enquiry both patients denied having rotatory vertigo. OH was being treated as positional vertigo and dizziness. The terms dizziness and vertigo are not interchangeable and are frequently misused by patients. Dizziness is a broad nonspecific term.(5) While vertigo, postural blackouts are specific subtypes of dizziness. Hence these symptoms have to be elucidated carefully.(6) An
algorithm to approach a patient with these symptoms is suggested (fig 1). The symptoms of blackouts were reproduced during examination for PH. There was no evidence for any other cause of PH (fig 1, table 1). PH is a common feature of autonomic dysfunction. Symptoms of PH include postural blackouts, postural dizziness, reeling sensation, coat hanger pain and tiredness. In patients over 50 years these symptoms should be carefully evaluated for the presence of PH/OH and other autonomic disturbances by doing bedside autonomic function tests. It is essential to evaluate for other causes of PH in all patients with postural blackouts, postural dizziness, reeling sensation, coat hanger pain and tiredness.
Differential diagnosis of episodic loss of consciousness, vertigo, blackouts Seizure Vertigo Tongue bite Rotation of self/environment Tonic (posturing), Clonic activity Duration- seconds in positional vertigo, Amnesia for the event minutes, hours in vestibulopathy Confusion, headache after the event Brainstem symptoms (diplopia, dysarthria) in Syncope vertebrobasilar ischemia Prolonged standing Postural blackouts Sweating Orthostatic hypotension Pallor Medication history antihypertensive, Ataxia diuretics, antipsychotics, parkinsonian drugs Cerebellar Cardiovascular illness arrhythmia, cardiac Sensory failure, valvular disease Vague description of symptoms Anxiety, depression, hyperventilation Normal examination
Both patients had history of urinary frequency and thrashing movements of limbs in sleep. Urinary frequency was wrongly attributed to prostatism a common condition in people over 50 years. In both patients the prostate was enlarged but there was no outflow obstruction. Urinary frequency is an early feature of autonomic dysfunction. Thrashing movements of limbs in sleep was misinterpreted as seizures. Dream enactment manifesting as thrashing
movements of limbs in sleep is a REM sleep behavior disorder specific for synucleinopathies like MSA.(7) Both patients had pure autonomic symptoms for a variable period of time. Parkinsonian and cerebellar signs were seen after a follow up of few years. Hence a close follow-up for development of parkinsonism or cerebellar features is essential in patients presenting with postural blackouts.
Conclusion: An algorithm to evaluate dizziness subtypes is suggested. Postural blackout, a subtype of dizziness, is due to PH/OH. The two cases we present suggest that postural blackout, a subtype of dizziness, may be due to PH/OH. MSA should be considered in patients with postural dizziness/blackouts. References 1. Delaney KA. Bedside Diagnosis of Vertigo: Value of the History and Neurological Examination. Academic Emergency Medicine. 2003 Dec 1;10 (12):138895. 2. Karatas M. Central vertigo and dizziness: epidemiology, differential diagnosis, and common causes. Neurologist. 2008 Nov;14(6):35564. 3. Rogers G, OFlynn N. NICE guideline: transient loss of consciousness (blackouts) in adults and young people. Br J Gen Pract. 2011 Jan;61(582):402. 4. Stefanova N, Bcke P, Duerr S, Wenning GK. Multiple system atrophy: an update. Lancet Neurol. 2009 Dec;8(12):11728. 5. Post RE, Dickerson LM. Dizziness: a diagnostic approach. Am Fam Physician. 2010 Aug 15;82(4):3618, 369. 6. Kutz JW Jr. The dizzy patient. Med. Clin. North Am. 2010 Sep;94(5):9891002. 7. Arnulf I. REM sleep behavior disorder: Motor manifestations and pathophysiology. Movement Disorders. 2012;27(6):67789.
You might also like
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- Approach To QuadriplegiaDocument4 pagesApproach To QuadriplegiaPraveen BabuNo ratings yet
- Latreille 2018Document41 pagesLatreille 2018Rezky 'kiki' Oktarianti SyahputriNo ratings yet
- Vestibular DisordersDocument8 pagesVestibular DisordersHilwy Al-haninNo ratings yet
- Algoritmo diferencial de debilidad proximal en paciente con miopatia adquirida por nemalina.Document7 pagesAlgoritmo diferencial de debilidad proximal en paciente con miopatia adquirida por nemalina.Farid Santiago Abedrabbo LombeydaNo ratings yet
- Brain: Cerebral Causes and Consequences of Parkinsonian Resting Tremor: A Tale of Two Circuits?Document21 pagesBrain: Cerebral Causes and Consequences of Parkinsonian Resting Tremor: A Tale of Two Circuits?Putu Gede SudiraNo ratings yet
- Sertraline and Rapid Eye Movement Sleep Without Atonia: An 8-Week, Open-Label Study in Depressed PatientsDocument38 pagesSertraline and Rapid Eye Movement Sleep Without Atonia: An 8-Week, Open-Label Study in Depressed PatientsKaren Ruste Villaluna-AbulenciaNo ratings yet
- Rajput 2021Document4 pagesRajput 202120.009 Diki Permadi Pratama PutraNo ratings yet
- CCJM Essential Tremor Choosing The Right Management Plan For Your PatientDocument8 pagesCCJM Essential Tremor Choosing The Right Management Plan For Your PatientBrian HarrisNo ratings yet
- Jurnal Psikiatri 4Document13 pagesJurnal Psikiatri 4Dati DelianaNo ratings yet
- Essential Tremor - Practice Essentials, Background, EtiologyDocument6 pagesEssential Tremor - Practice Essentials, Background, EtiologydilaNo ratings yet
- TremorDocument14 pagesTremorEcaterina LungociuNo ratings yet
- A Child With Repeated Movements During Sleep: Patient28Document3 pagesA Child With Repeated Movements During Sleep: Patient28Mitul PatelNo ratings yet
- Autonomic Disfunction in Primary Sleep DisorderDocument64 pagesAutonomic Disfunction in Primary Sleep DisorderRikizu HobbiesNo ratings yet
- HipotensiónDocument1 pageHipotensiónMartin RodriguezNo ratings yet
- A Case of Patient With Cerebellar Variant of Stiff Person SyndromeDocument4 pagesA Case of Patient With Cerebellar Variant of Stiff Person SyndromelaraviNo ratings yet
- Hemiparkinsonism-Hemiatrophy Syndrome: Case ReportDocument3 pagesHemiparkinsonism-Hemiatrophy Syndrome: Case ReportMuhammad JamalNo ratings yet
- Sleep Consult TemplateDocument5 pagesSleep Consult Templatesbonvallet3912100% (1)
- Parasomnias in ChildhoodDocument20 pagesParasomnias in ChildhoodCherie HanNo ratings yet
- 52 Tripathy EtalDocument5 pages52 Tripathy EtaleditorijmrhsNo ratings yet
- Clinical Case Conference on Conversion Disorder Diagnosis and TreatmentDocument8 pagesClinical Case Conference on Conversion Disorder Diagnosis and TreatmentLiza MelendrezNo ratings yet
- Vertigo and Its Management PDFDocument21 pagesVertigo and Its Management PDFNitya KrishnaNo ratings yet
- Sleep DisordersDocument19 pagesSleep DisordersKaren MogiNo ratings yet
- A Case of A Patient With Both Chorea and Restless Legs SyndromeDocument4 pagesA Case of A Patient With Both Chorea and Restless Legs SyndromeNicolas SaputraNo ratings yet
- Algoritmo diferencial de la ataxia sensitiva en mielopatia por cobre secundaria a celiaquiaDocument7 pagesAlgoritmo diferencial de la ataxia sensitiva en mielopatia por cobre secundaria a celiaquiaFarid Santiago Abedrabbo LombeydaNo ratings yet
- Sleep: Important Considerations in Management of PainDocument8 pagesSleep: Important Considerations in Management of PainMáximo Wladimir Viedma OlivaNo ratings yet
- Evaluation and Management of Autonomic Nervous System DisordersDocument10 pagesEvaluation and Management of Autonomic Nervous System DisordersbpppbbNo ratings yet
- 1era Crisis Epileptic ADocument6 pages1era Crisis Epileptic Aalvarorm1No ratings yet
- Feline Neurological ExamDocument161 pagesFeline Neurological Examaurora heryantiNo ratings yet
- Types of Seizure & Status Epilepticus: Prepared By: Ivy Joy A. Benitez, BSN 4-ADocument28 pagesTypes of Seizure & Status Epilepticus: Prepared By: Ivy Joy A. Benitez, BSN 4-AyviyojNo ratings yet
- The Neurohospitalist-2011-Cha-32-40 PDFDocument10 pagesThe Neurohospitalist-2011-Cha-32-40 PDFeviherdiantiNo ratings yet
- Phi RythmDocument6 pagesPhi RythmStanley IgweNo ratings yet
- SchnekDocument8 pagesSchnekKarma SetiyawanNo ratings yet
- Sleep DisorderDocument2 pagesSleep DisorderMaira IrshadNo ratings yet
- A Middle Aged Woman With Nausea Weight Loss and Orthostatic HypotensionDocument7 pagesA Middle Aged Woman With Nausea Weight Loss and Orthostatic Hypotensioniri_balNo ratings yet
- 171120se-Bvsspa Sod 14008603Document5 pages171120se-Bvsspa Sod 1400860306trahosNo ratings yet
- Cns ExaminationDocument17 pagesCns ExaminationJuana Maria Garcia Espinoza100% (1)
- Cerebral Palsy Practice Essentials: Signs and SymptomsDocument11 pagesCerebral Palsy Practice Essentials: Signs and SymptomsTahsinur RahmanNo ratings yet
- Extrapyramidal DiseaseDocument54 pagesExtrapyramidal Diseasemirabel IvanaliNo ratings yet
- Prof. DR. Aboe Amar Joesoef, DR, Sp.S. (K)Document44 pagesProf. DR. Aboe Amar Joesoef, DR, Sp.S. (K)Ryan FeizalNo ratings yet
- Autonomic Testing, Methods and TechniquesDocument15 pagesAutonomic Testing, Methods and TechniquesYanina Pérez de VillarrealNo ratings yet
- Tidur IdDocument9 pagesTidur Idviga ristikaNo ratings yet
- Postictal Visual Impairment Sign of Reversible EncephalopathyDocument2 pagesPostictal Visual Impairment Sign of Reversible EncephalopathyalysandrNo ratings yet
- Eeg, PSG, Sleep DisordersDocument48 pagesEeg, PSG, Sleep DisordersIoana MunteanuNo ratings yet
- Nagaratnam - 2004 Vestibular Dysfunction and Anxiety Disorder Interface - ElderlyDocument13 pagesNagaratnam - 2004 Vestibular Dysfunction and Anxiety Disorder Interface - ElderlyJuan Hernández GarcíaNo ratings yet
- Parkinsons Disease Copy 3Document41 pagesParkinsons Disease Copy 3Raghad AbbadyNo ratings yet
- Neurological History and Physical ExaminationDocument21 pagesNeurological History and Physical Examinationg3murtulu100% (1)
- NEUROBEHAVIURrDocument21 pagesNEUROBEHAVIURrSandra DewiNo ratings yet
- 1 s2.0 S0749073922000219 MainDocument15 pages1 s2.0 S0749073922000219 Mainbdjxk95cyhNo ratings yet
- Epilepsia CursivaDocument3 pagesEpilepsia Cursiva---No ratings yet
- Newman Toker 2015Document23 pagesNewman Toker 2015Icha IchaNo ratings yet
- Encefalitis LimbicaDocument11 pagesEncefalitis LimbicaRandy UlloaNo ratings yet
- Benefits and Limitations of Vojta ApproachDocument50 pagesBenefits and Limitations of Vojta ApproachAlice Teodorescu100% (3)
- Medically Intractable SeizuresDocument26 pagesMedically Intractable SeizuresNarianne Mae Solis Bedoy100% (1)
- DR A.A.Ayu Meidiary, SPS: Department of Neurology, Sanglah General Hospital, Udayana University DenpasarDocument47 pagesDR A.A.Ayu Meidiary, SPS: Department of Neurology, Sanglah General Hospital, Udayana University DenpasarKertiasihwayanNo ratings yet
- General Neuro ExaminationDocument27 pagesGeneral Neuro ExaminationnourmdstudentNo ratings yet
- Detecting metabolic encephalopathiesDocument16 pagesDetecting metabolic encephalopathiesAnggi SetyariniNo ratings yet
- Episodic Astasia-Abasia Associated With Hyper-Perfusion in The Subthalamic Region and Dorsal BrainstemDocument3 pagesEpisodic Astasia-Abasia Associated With Hyper-Perfusion in The Subthalamic Region and Dorsal BrainstemAnonymous vnv6QFNo ratings yet
- Sleep and Neurologic DiseaseFrom EverandSleep and Neurologic DiseaseMitchell G. MiglisNo ratings yet
- Case Report: Rasmussen's Encephalitis Treated Successfully With RituximabDocument16 pagesCase Report: Rasmussen's Encephalitis Treated Successfully With RituximabCureusNo ratings yet
- Musculosleketal Risk Assesment Among Nurses in Pateint Manual Handling in Hospital Wards - A Cross Sectional StudyDocument10 pagesMusculosleketal Risk Assesment Among Nurses in Pateint Manual Handling in Hospital Wards - A Cross Sectional StudyCureusNo ratings yet
- Premodern Transcendental Perspectives On The Missing Heritability Problem and Some Intelligence ConundrumsDocument33 pagesPremodern Transcendental Perspectives On The Missing Heritability Problem and Some Intelligence ConundrumsCureusNo ratings yet
- Epidemiology of Angioid Streaks-Associated Choroidal Neovascular Membranes in The United KingdomDocument20 pagesEpidemiology of Angioid Streaks-Associated Choroidal Neovascular Membranes in The United KingdomCureusNo ratings yet
- Transanal Endoscopic Microsurgery by Using Single Incision PortDocument10 pagesTransanal Endoscopic Microsurgery by Using Single Incision PortCureusNo ratings yet
- From The From The Patient's Point of View: Patient Centered Outcomes in Spine SurgeryDocument17 pagesFrom The From The Patient's Point of View: Patient Centered Outcomes in Spine SurgeryCureusNo ratings yet
- Oncothermia: A New Paradigm in Cancer TherapiesDocument31 pagesOncothermia: A New Paradigm in Cancer TherapiesCureus100% (1)
- Pipeline Embolization For The Treatment of A Progressively Enlarging Symptomatic Carotid Artery Petrous Segment Pseudoaneurysm. Case Report.Document13 pagesPipeline Embolization For The Treatment of A Progressively Enlarging Symptomatic Carotid Artery Petrous Segment Pseudoaneurysm. Case Report.CureusNo ratings yet
- Applications of Silk in Drug Delivery: Advancement in Pharmaceutical Dosage FormsDocument17 pagesApplications of Silk in Drug Delivery: Advancement in Pharmaceutical Dosage FormsCureus100% (1)
- Cost-Minimization Analysis: Should Partial Breast Irradiation Be Utilized Over Whole Breast Irradiation Assuming Equivalent Clinical Outcomes?Document16 pagesCost-Minimization Analysis: Should Partial Breast Irradiation Be Utilized Over Whole Breast Irradiation Assuming Equivalent Clinical Outcomes?CureusNo ratings yet
- Classification of Brain Metastases Prognostic Groups Utilizing Artificial Neural Network ApproachesDocument32 pagesClassification of Brain Metastases Prognostic Groups Utilizing Artificial Neural Network ApproachesCureusNo ratings yet
- Ruptured Intracranial Dermoid Cyst: Unusually Rapid Disease Course Leading To A Fatal OutcomeDocument10 pagesRuptured Intracranial Dermoid Cyst: Unusually Rapid Disease Course Leading To A Fatal OutcomeCureusNo ratings yet
- Outcome of Wearing High Heel Shoes in Young GenerationDocument16 pagesOutcome of Wearing High Heel Shoes in Young GenerationCureusNo ratings yet
- The Use of Facebook Among Seventy-Seven Departments of Anesthesia in United States Medical SchoolsDocument14 pagesThe Use of Facebook Among Seventy-Seven Departments of Anesthesia in United States Medical SchoolsCureusNo ratings yet
- Daily Singing Practice As A Means of Improving Pulmonary Function and Quality of Life in Emphysema Patients.Document16 pagesDaily Singing Practice As A Means of Improving Pulmonary Function and Quality of Life in Emphysema Patients.CureusNo ratings yet
- Robotic Radiosurgery For Liver MetastasesDocument23 pagesRobotic Radiosurgery For Liver MetastasesCureusNo ratings yet
- Cardiac Radiosurgery (CyberHeart™) For Treatment of Arrhythmia: Physiologic and Histopathologic Correlation in The Porcine ModelDocument28 pagesCardiac Radiosurgery (CyberHeart™) For Treatment of Arrhythmia: Physiologic and Histopathologic Correlation in The Porcine ModelCureusNo ratings yet
- Test Paper 001Document7 pagesTest Paper 001CureusNo ratings yet
- Effects of Corneal Crosslinking For Keratoconus Assessed With Anterior Segment Optical Coherence TomographyDocument3 pagesEffects of Corneal Crosslinking For Keratoconus Assessed With Anterior Segment Optical Coherence TomographyCureusNo ratings yet
- Two Part Pterional Craniotomy: Technical NoteDocument17 pagesTwo Part Pterional Craniotomy: Technical NoteCureusNo ratings yet
- Smart Device Use Among Resident Physicians at Stanford HospitalDocument26 pagesSmart Device Use Among Resident Physicians at Stanford HospitalCureusNo ratings yet
- Stereotactic Radiosurgery For The Treatment of Brain Metastases From Non Small Cell Lung Carcinoma: A Multi-Institutional ExperienceDocument19 pagesStereotactic Radiosurgery For The Treatment of Brain Metastases From Non Small Cell Lung Carcinoma: A Multi-Institutional ExperienceCureusNo ratings yet
- Emerging Neurosurgical Applications of Synchrotron-Generated MicrobeamsDocument17 pagesEmerging Neurosurgical Applications of Synchrotron-Generated MicrobeamsCureusNo ratings yet
- Endometriosis: Diagnosis and Treatment: From Fingernails To The RobotDocument17 pagesEndometriosis: Diagnosis and Treatment: From Fingernails To The RobotCureusNo ratings yet
- Calibration of Force/torque and Acceleration For An Independent Safety Layer in Medical Robotic SystemsDocument14 pagesCalibration of Force/torque and Acceleration For An Independent Safety Layer in Medical Robotic SystemsCureusNo ratings yet
- Gamma Knife Radiosurgery For Breast Cancer Metastases To The Brain: Outcomes and Prognostic Factors From A Large Prospectively Collected DatabaseDocument18 pagesGamma Knife Radiosurgery For Breast Cancer Metastases To The Brain: Outcomes and Prognostic Factors From A Large Prospectively Collected DatabaseCureusNo ratings yet
- GammaKnife Radiosurgery For Melanoma Brain MetastasesDocument9 pagesGammaKnife Radiosurgery For Melanoma Brain MetastasesCureusNo ratings yet
- Feasibility of Fiducial-Free Prone-Position Treatments With CyberKnife For Lower Lumbar/sacral Spine LesionsDocument5 pagesFeasibility of Fiducial-Free Prone-Position Treatments With CyberKnife For Lower Lumbar/sacral Spine LesionsCureusNo ratings yet
- High Speed Direct SAD Radiosurgery Beam ScannerDocument15 pagesHigh Speed Direct SAD Radiosurgery Beam ScannerCureusNo ratings yet
- Parkinson-Plus SyndromeDocument2 pagesParkinson-Plus SyndromeRuth May de VillaNo ratings yet
- Hearing Recovery From Deafness Caused by Bromate IntoxicationDocument3 pagesHearing Recovery From Deafness Caused by Bromate IntoxicationFefita lamNo ratings yet
- Elective BookDocument226 pagesElective BookThiago Vargas da CostaNo ratings yet
- Assessment of Gait Disorders in ChildrenDocument3 pagesAssessment of Gait Disorders in ChildrenMadalina RarincaNo ratings yet
- How NeuroAid helps diagnose neurodegenerative diseasesDocument8 pagesHow NeuroAid helps diagnose neurodegenerative diseasesInnovate. NPSNo ratings yet
- Treatment Dysarthria EfficacyDocument12 pagesTreatment Dysarthria EfficacySwathi GeethaNo ratings yet
- Chorda Tympani..Document3 pagesChorda Tympani..Sheeba NoorNo ratings yet
- Meniere DiseaseDocument36 pagesMeniere DiseaseThamizharasan SivamaniNo ratings yet
- Chapter 14 Neurologic Disorders Study Guide Outline #2Document12 pagesChapter 14 Neurologic Disorders Study Guide Outline #2Del Delgado100% (1)
- THTDocument6 pagesTHTchumNo ratings yet
- Audiology NotesDocument3 pagesAudiology NotesSaera Hafiz NikitaNo ratings yet
- Proceedings: 2019 Canine ConferenceDocument48 pagesProceedings: 2019 Canine ConferenceJUAN DAVID PEÑUELA CORREANo ratings yet
- Dandy-Walker SyndromeDocument12 pagesDandy-Walker SyndromeHarshita bansalNo ratings yet
- Iap Guidelines For Epilepsy 2014Document45 pagesIap Guidelines For Epilepsy 2014Karpur ShirsatNo ratings yet
- Manual Neuro HDPE 2017Document20 pagesManual Neuro HDPE 2017Irfan GondalNo ratings yet
- Review DBSDocument8 pagesReview DBSEtonia PangNo ratings yet
- Developmental Apraxia of SpeechDocument4 pagesDevelopmental Apraxia of SpeechStella PapadopoulouNo ratings yet
- Baycrest Annual Report 2009 2010Document58 pagesBaycrest Annual Report 2009 2010BaycrestNo ratings yet
- Causes of PseudoseizuresDocument8 pagesCauses of PseudoseizuresDewangga Primananda Susanto100% (1)
- Differential DiagnosisDocument5 pagesDifferential Diagnosisjoanna gurtizaNo ratings yet
- Final Document For Ia PDFDocument19 pagesFinal Document For Ia PDFVamsi HashmiNo ratings yet
- Tekle-Haimanot 1990Document15 pagesTekle-Haimanot 1990Sayak ChowdhuryNo ratings yet
- Guide For Foreign Doctors Working in FinlandDocument10 pagesGuide For Foreign Doctors Working in FinlandNick BourNo ratings yet
- Music For Children With Hearing Loss A Resource For Parents and TeachersDocument337 pagesMusic For Children With Hearing Loss A Resource For Parents and TeachersCamila Bastos100% (1)
- Ataxia Physical Therapy and Rehabilitation Applications For Ataxic PatientsDocument19 pagesAtaxia Physical Therapy and Rehabilitation Applications For Ataxic PatientsAnastasios ChortisNo ratings yet
- Bio7 ch48Document20 pagesBio7 ch48freezo1994No ratings yet
- Cerebral Palsy - Critical Elements of CareDocument25 pagesCerebral Palsy - Critical Elements of CaremarkoNo ratings yet
- 15.IJBCP Anticonvulsant Effect of CCB Roopa Jan2018Document4 pages15.IJBCP Anticonvulsant Effect of CCB Roopa Jan2018Karuna Sree PNo ratings yet
- Biography: Ktus-Docol-4 - 08-Sep-2010Document4 pagesBiography: Ktus-Docol-4 - 08-Sep-2010Ana Lu LoboNo ratings yet
- Artículo de GeriatríaDocument14 pagesArtículo de GeriatríaMaria Guadalupe Hernandez JimenezNo ratings yet