You might also like
- Cranial Strains and MalocclusionDocument5 pagesCranial Strains and MalocclusionRyan Dobbeck100% (1)
- Sample OSCE Stations DentalDocument7 pagesSample OSCE Stations DentalEbn Seena90% (10)
- Anorexia and Bulimia InterviewDocument11 pagesAnorexia and Bulimia InterviewramondiazdtNo ratings yet
- Psychological Testing ExplainedDocument12 pagesPsychological Testing ExplainedUniversity of Madras International Conference100% (2)
- 7 HR Data Sets for People Analytics Under 40 CharactersDocument14 pages7 HR Data Sets for People Analytics Under 40 CharactersTaha Ahmed100% (1)
- Current Trends On Assessment and EvaluationDocument25 pagesCurrent Trends On Assessment and EvaluationDian Palupi100% (1)
- Physiotherapy Based On The Bobath Concept For Adults With HemiplegiaDocument7 pagesPhysiotherapy Based On The Bobath Concept For Adults With HemiplegiaDr. Sunil Sahu (PT)No ratings yet
- Comparing Various Short-Form Geriatric Depression Scales Leads To The GDS-5/15Document5 pagesComparing Various Short-Form Geriatric Depression Scales Leads To The GDS-5/15lucial86No ratings yet
- ID Hubungan Status Spiritual Dengan KualitaDocument3 pagesID Hubungan Status Spiritual Dengan KualitaRetno Anggraini100% (1)
- Stimsonm Researchcritiquen531Document11 pagesStimsonm Researchcritiquen531api-270067627No ratings yet
- Interventions For The Prevention of Postpartum Depression in Adolescent Mothers: A Systematic ReviewDocument11 pagesInterventions For The Prevention of Postpartum Depression in Adolescent Mothers: A Systematic Reviewnur fadhilahNo ratings yet
- The Minnesota Living With Heart Failure QuestionnaDocument11 pagesThe Minnesota Living With Heart Failure Questionnamgarcía_62490No ratings yet
- Original PapersDocument8 pagesOriginal Papersرقية ياسينNo ratings yet
- Mellits and Cheek FormulaDocument5 pagesMellits and Cheek FormulafadhlialbaniNo ratings yet
- Health and Quality of Life OutcomesDocument7 pagesHealth and Quality of Life OutcomesMuhammad Adnan MalikNo ratings yet
- Review of Studies Evaluating Psychotherapy in Bulimia Nervosa: The Influence of Research MethodsDocument6 pagesReview of Studies Evaluating Psychotherapy in Bulimia Nervosa: The Influence of Research MethodsBitter MoonNo ratings yet
- Physiotherapy Based On The Bobath ConceptpdfDocument6 pagesPhysiotherapy Based On The Bobath ConceptpdfmatsNo ratings yet
- Characteristics of Depression in Hemodialysis Patients: Symptoms, Quality of Life and Mortality RiskDocument7 pagesCharacteristics of Depression in Hemodialysis Patients: Symptoms, Quality of Life and Mortality RiskMirza RisqaNo ratings yet
- Validation of The Short Form of The Hypertension Quality of Life Questionnaire (MINICHAL)Document35 pagesValidation of The Short Form of The Hypertension Quality of Life Questionnaire (MINICHAL)Adi SaputraNo ratings yet
- The Menopause Rating Scale (MRS)Document8 pagesThe Menopause Rating Scale (MRS)Nurfadila RasyidNo ratings yet
- Health and Quality of Life Outcomes: Development of The Well-Being Questionnaire Short-Form in Japanese: The W-BQ12Document10 pagesHealth and Quality of Life Outcomes: Development of The Well-Being Questionnaire Short-Form in Japanese: The W-BQ12Steven irvingNo ratings yet
- Appraisal of An Article On Prognosis: 1998, 22:442-445. Marc Lester, James Warner and Bob BlizardDocument5 pagesAppraisal of An Article On Prognosis: 1998, 22:442-445. Marc Lester, James Warner and Bob BlizardViela MarcNo ratings yet
- Manual Therapy: Systematic ReviewDocument8 pagesManual Therapy: Systematic Reviewubiktrash1492No ratings yet
- Calidad de Vida en TBDocument17 pagesCalidad de Vida en TBcarlaccvNo ratings yet
- Short Report: Education and Psychological Aspects Modification and Validation of The Revised Diabetes Knowledge ScaleDocument5 pagesShort Report: Education and Psychological Aspects Modification and Validation of The Revised Diabetes Knowledge ScaleadninaninNo ratings yet
- LBP PDFDocument20 pagesLBP PDFHanifanDanuNo ratings yet
- Motivation Implementation of Hba1C Decrease in Patients Diabetes Mellitus (Riview Literature) Christianto NugrohoDocument6 pagesMotivation Implementation of Hba1C Decrease in Patients Diabetes Mellitus (Riview Literature) Christianto Nugrohomarisa isahNo ratings yet
- Interpreting Validity Indexes For Diagnostic TestsDocument10 pagesInterpreting Validity Indexes For Diagnostic TestsJudson BorgesNo ratings yet
- Ebm&Rm Obs Student SGT 23Document14 pagesEbm&Rm Obs Student SGT 23Sara Abdi OsmanNo ratings yet
- Jurnal JkmsDocument8 pagesJurnal JkmsArif Kurniawan ListiantoNo ratings yet
- Migraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesDocument14 pagesMigraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesRetno ManggalihNo ratings yet
- The Metabolic Syndrome: Comparison of Newly Proposed IDF, Modified ATP III and WHO Criteria and Their AgreementsDocument6 pagesThe Metabolic Syndrome: Comparison of Newly Proposed IDF, Modified ATP III and WHO Criteria and Their AgreementsjoelNo ratings yet
- Body CheckingDocument10 pagesBody CheckingSol Pennisi100% (1)
- BMC Public Health: Relationship Between Body Image Disturbance and Incidence of Depression: The SUN Prospective CohortDocument9 pagesBMC Public Health: Relationship Between Body Image Disturbance and Incidence of Depression: The SUN Prospective CohortAnca RaduNo ratings yet
- Sleep-Disordered Breathing and Gestational Diabetes Mellitus - Luque Fernandez - Diabetes Care - 2013Document8 pagesSleep-Disordered Breathing and Gestational Diabetes Mellitus - Luque Fernandez - Diabetes Care - 2013Marco EspinoNo ratings yet
- A Critical Review of The Literature On An Aspect of Nursing Practice and Analysis of TWO Primary Research Studies Related To This TopicDocument10 pagesA Critical Review of The Literature On An Aspect of Nursing Practice and Analysis of TWO Primary Research Studies Related To This TopicJohnny Kehoe0% (1)
- Article Critique JUNE 26, 2022Document7 pagesArticle Critique JUNE 26, 2022jessicaNo ratings yet
- Tfeq21 PDFDocument10 pagesTfeq21 PDFDarin MonerNo ratings yet
- DiabetesDocument15 pagesDiabetesJunior GonzalesNo ratings yet
- DQoL Jacobson 1988 PDFDocument8 pagesDQoL Jacobson 1988 PDFeunikieNo ratings yet
- KruskalDocument4 pagesKruskalGERLY TRAYANo ratings yet
- Norms For The Beck Depression Inventory (BDI-II) in A Large Dutch Community SampleDocument6 pagesNorms For The Beck Depression Inventory (BDI-II) in A Large Dutch Community SamplefanzefirlNo ratings yet
- Predicting Basal Metabolic Rate in The Obese Is DiDocument7 pagesPredicting Basal Metabolic Rate in The Obese Is DiShannon LopezNo ratings yet
- Current Databases On Biological Variation: Pros, Cons and ProgressDocument10 pagesCurrent Databases On Biological Variation: Pros, Cons and ProgressCarlos PardoNo ratings yet
- UntitledDocument7 pagesUntitledapi-247066569No ratings yet
- Pregnancy dating by fetal CRLDocument10 pagesPregnancy dating by fetal CRLHeru Eko SutrisnoNo ratings yet
- Diagnosis and Testing in Bronchiolitis: A Systematic ReviewDocument8 pagesDiagnosis and Testing in Bronchiolitis: A Systematic ReviewDaniel IrrazabalNo ratings yet
- Assessing Illness Perceptions with the Brief IPQDocument14 pagesAssessing Illness Perceptions with the Brief IPQsunNo ratings yet
- Chronic Illnesses Are Becoming An Increasingly Serious Public Health Issue Across The WorldDocument7 pagesChronic Illnesses Are Becoming An Increasingly Serious Public Health Issue Across The WorldHaneenNo ratings yet
- IWQOL Reference For Data TransformationDocument10 pagesIWQOL Reference For Data TransformationkenetmartinNo ratings yet
- 3. Psychosocial Adjustment to Illness ScaleDocument12 pages3. Psychosocial Adjustment to Illness ScaleABD.NASIRNo ratings yet
- Measuring fatigue in sarcoidosis_ The FatigueDocument13 pagesMeasuring fatigue in sarcoidosis_ The FatigueVăn HưngNo ratings yet
- Body Image ScaleDocument9 pagesBody Image ScaleJorgeNo ratings yet
- Meta-Analysis of The Relationship Between Breaks in Sedentary Behavior and Cardiometabolic HealthDocument11 pagesMeta-Analysis of The Relationship Between Breaks in Sedentary Behavior and Cardiometabolic HealthIvan HeriawanNo ratings yet
- Jurnal Bedah (Heri) 2Document22 pagesJurnal Bedah (Heri) 2Elvis WAhyuni SiregarNo ratings yet
- 06 Original 02Document7 pages06 Original 02normanahmad92No ratings yet
- Involuntary Weight Loss. Does A Negative Baseline Evaluation Provide Adequate Reassurance?Document5 pagesInvoluntary Weight Loss. Does A Negative Baseline Evaluation Provide Adequate Reassurance?nacxit6No ratings yet
- Blood Type DietDocument6 pagesBlood Type DietMarialoretoAGNo ratings yet
- Tmp94e1 TMPDocument11 pagesTmp94e1 TMPFrontiersNo ratings yet
- Mult2 - Novas Ref Avaliação Curvas InfantilDocument16 pagesMult2 - Novas Ref Avaliação Curvas InfantilDanielle Raquel GonçalvesNo ratings yet
- Dsur5104 Exercises3Document4 pagesDsur5104 Exercises3Abhiraj ChakrabartiNo ratings yet
- BJC 2015310 ADocument12 pagesBJC 2015310 AJuliana SoaresNo ratings yet
- The World Health Organization Adult ADHD Self-Report Scale (ASRS) : A Short Screening Scale For Use in The General PopulationDocument12 pagesThe World Health Organization Adult ADHD Self-Report Scale (ASRS) : A Short Screening Scale For Use in The General PopulationMihaela VișanNo ratings yet
- Interpreting Change Scores For Pain and Functional Status in Low Back Pain - Towards International Consensus Regarding Minimal Important ChangeDocument6 pagesInterpreting Change Scores For Pain and Functional Status in Low Back Pain - Towards International Consensus Regarding Minimal Important ChangeAmbar MonzoncilloNo ratings yet
- How To Help Someone With A Mental IllnessDocument2 pagesHow To Help Someone With A Mental IllnessAreej Craxi SultanNo ratings yet
- Causes of War of IndependenceDocument5 pagesCauses of War of IndependenceAreej Craxi SultanNo ratings yet
- ThailandDocument16 pagesThailandAreej Craxi SultanNo ratings yet
- Mid To Late 20th CenturyDocument8 pagesMid To Late 20th CenturyAreej Craxi SultanNo ratings yet
- The Industrial RevolutionDocument5 pagesThe Industrial RevolutionAreej Craxi SultanNo ratings yet
- MSQ1967 Long FormDocument7 pagesMSQ1967 Long FormAreej Craxi SultanNo ratings yet
- Trait Viewpoint of Personality 8Document20 pagesTrait Viewpoint of Personality 8Areej Craxi SultanNo ratings yet
- Basketball Prison Ball Lesson PlansDocument4 pagesBasketball Prison Ball Lesson Plansapi-273012822No ratings yet
- Unit 1 Vocab. ReadingDocument4 pagesUnit 1 Vocab. ReadingNhật KiênNo ratings yet
- Attitudes of student teachers towards teaching professionDocument6 pagesAttitudes of student teachers towards teaching professionHuma Malik100% (1)
- Cube Roots of Unity (Definition, Properties and Examples)Document1 pageCube Roots of Unity (Definition, Properties and Examples)Nipun RajvanshiNo ratings yet
- Interview With Mitch Drazin Before and After EditingDocument3 pagesInterview With Mitch Drazin Before and After Editingapi-285005584No ratings yet
- Positive DisciplineDocument16 pagesPositive DisciplineClarice Joy TuazonNo ratings yet
- FEDERAL PUBLIC SERVICE COMMISSION SCREENING/PROFESSIONAL TESTSDocument36 pagesFEDERAL PUBLIC SERVICE COMMISSION SCREENING/PROFESSIONAL TESTSCh Hassan TajNo ratings yet
- Faculty Screening J.ODocument2 pagesFaculty Screening J.OIvy CalladaNo ratings yet
- Practical Research 2 Quarter 4 Module 5 Lesson 1Document2 pagesPractical Research 2 Quarter 4 Module 5 Lesson 1juvy abelleraNo ratings yet
- Agenda Setting Syllabus 2010Document2 pagesAgenda Setting Syllabus 2010Arta Novita HarlanNo ratings yet
- Person Resididng Outside ManipurDocument21 pagesPerson Resididng Outside ManipurNguwruw Chungpha MoyonNo ratings yet
- EN5VC IIIf 3.8 - 2023 2024 - Day2Document3 pagesEN5VC IIIf 3.8 - 2023 2024 - Day2Ma. Feliza Saligan100% (1)
- 1443835153Document268 pages1443835153Nori LofindieNo ratings yet
- Managing The Primary Classroom: - How Physical Class Environment Contribute To Effective LessonDocument16 pagesManaging The Primary Classroom: - How Physical Class Environment Contribute To Effective LessonJannah AziziNo ratings yet
- AreWomenOutperformingMenInShort-TermMemory Nikola Rashkov 700951Document8 pagesAreWomenOutperformingMenInShort-TermMemory Nikola Rashkov 700951charmela pabillonNo ratings yet
- 7C.3 Particles and ForcesDocument19 pages7C.3 Particles and Forcesharold hargridNo ratings yet
- Shaurya Brochure PDFDocument12 pagesShaurya Brochure PDFAbhinav ShresthNo ratings yet
- Personal Position PaperDocument18 pagesPersonal Position Paperapi-258330934No ratings yet
- (ACV-S06) Week 06 - Pre-Task - Quiz - Weekly Quiz (PA) - INGLES IV (36824)Document5 pages(ACV-S06) Week 06 - Pre-Task - Quiz - Weekly Quiz (PA) - INGLES IV (36824)Gianfranco Riega galarzaNo ratings yet
- Weekly Home Learning Plan: Learning Area: TLE 7 - COOKERYDocument1 pageWeekly Home Learning Plan: Learning Area: TLE 7 - COOKERYCriselAlamag100% (1)
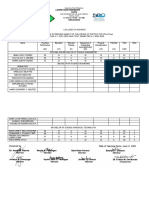
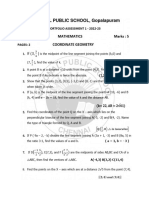
- G10 - Portfolio Assessment 1 - 2022-2023Document2 pagesG10 - Portfolio Assessment 1 - 2022-2023ayush rajeshNo ratings yet
- Software Engg. Question Paper - 40 CharacterDocument14 pagesSoftware Engg. Question Paper - 40 Characteranon_572289632No ratings yet
- Results of 2011 SMOPS (For Webpage)Document14 pagesResults of 2011 SMOPS (For Webpage)Thích Toán HọcNo ratings yet
- Simulations A Tool For Testing Virtual Reality in The Language ClassroomDocument10 pagesSimulations A Tool For Testing Virtual Reality in The Language ClassroomSyed Qaiser HussainNo ratings yet
- Core OM - Term 1 - 2019Document5 pagesCore OM - Term 1 - 2019chandel08No ratings yet