You might also like
- Formaldehyde - All-Rounder or Toxicant: Reserve This SpaceDocument19 pagesFormaldehyde - All-Rounder or Toxicant: Reserve This SpaceMinh Tuyen MaiNo ratings yet
- Profiles of Drug Substances Excipients and Related Methodology Volume 30 2003 PDFDocument322 pagesProfiles of Drug Substances Excipients and Related Methodology Volume 30 2003 PDFchemtabNo ratings yet
- Understanding Carbamates in 40 CharactersDocument6 pagesUnderstanding Carbamates in 40 CharactersIrma Juan AndreasNo ratings yet
- 8 Environmental Toxicology ATSDR Tox ProfilesDocument20 pages8 Environmental Toxicology ATSDR Tox ProfilesAurora Çizmja100% (1)
- Chemical Phosphorous Removal and Online AnalysisDocument31 pagesChemical Phosphorous Removal and Online AnalysisKrishna PedapatiNo ratings yet
- Collection Preservation of Water and Waste-Water SamplesDocument26 pagesCollection Preservation of Water and Waste-Water SamplesWaleed El-azabNo ratings yet
- Prof. David Kirkland Kirkland ConsultingDocument25 pagesProf. David Kirkland Kirkland Consultingsrikanthannabathuni4575100% (1)
- 3 Chemical Dual Use AwarenessDocument7 pages3 Chemical Dual Use AwarenessismailinesNo ratings yet
- EnviroChem Additional PDFDocument503 pagesEnviroChem Additional PDFJane PollyNo ratings yet
- Iron Toxic Heavy Metals Fact SheetDocument1 pageIron Toxic Heavy Metals Fact SheetosumexNo ratings yet
- Quaternary Ammonium Compounds - Document TranscriptDocument9 pagesQuaternary Ammonium Compounds - Document TranscriptChe_libreNo ratings yet
- Lab Report 1 (Handwritten)Document3 pagesLab Report 1 (Handwritten)Nurul NadiaNo ratings yet
- Tsunoda, Humio - Tsunoda, Masashi - Yu, Ming-Ho-Environmental Toxicology - Biological and Health Effects of Pollutants, Third Edition-CRC PresDocument373 pagesTsunoda, Humio - Tsunoda, Masashi - Yu, Ming-Ho-Environmental Toxicology - Biological and Health Effects of Pollutants, Third Edition-CRC PresEğitim ParaylaNo ratings yet
- Arsenic ToxicityDocument26 pagesArsenic ToxicityDyar MzafarNo ratings yet
- Water & Wastewater Sampling MethodsDocument23 pagesWater & Wastewater Sampling MethodsLipQin YeoNo ratings yet
- Anthranilic acid: precursor to tryptophanDocument20 pagesAnthranilic acid: precursor to tryptophanGlibNo ratings yet
- Alkalinity, Salinity, Dissolved Oxygen, Electrical Conductivity Etc. in An Aquatic System, TheseDocument8 pagesAlkalinity, Salinity, Dissolved Oxygen, Electrical Conductivity Etc. in An Aquatic System, TheseElaiza M. PontriasNo ratings yet
- A Guide To Kjeldahl Nitrogen Determination Methods and ApparatusDocument13 pagesA Guide To Kjeldahl Nitrogen Determination Methods and ApparatusNoranisza MahmudNo ratings yet
- OECD SIDS Profile: AcetanilideDocument96 pagesOECD SIDS Profile: AcetanilideIrfan LutfiantoNo ratings yet
- Determination of Heavy Metal in Marine Fish 2Document6 pagesDetermination of Heavy Metal in Marine Fish 2Muhammad Zainul MuttaqinNo ratings yet
- Diesel Particulate Matter and Occupational Health IssuesDocument13 pagesDiesel Particulate Matter and Occupational Health IssuesKaren Pacheco DeLacruzNo ratings yet
- Particulate Matter PDFDocument11 pagesParticulate Matter PDFFazry FachruronyNo ratings yet
- Advanced Oxidation Processes for Wastewater TreatmentDocument22 pagesAdvanced Oxidation Processes for Wastewater Treatmentจิรพัฒน์ทิพย์รัตน์0% (1)
- Calcium HypochloriteDocument260 pagesCalcium HypochloriteWidya Pradipta100% (1)
- Environmental Chemistry PDFDocument3 pagesEnvironmental Chemistry PDFdrupad malikNo ratings yet
- Environmental Toxicology-BookDocument125 pagesEnvironmental Toxicology-BookAneelaNo ratings yet
- What Are HydrogelsDocument4 pagesWhat Are HydrogelsHossein NajafzadehNo ratings yet
- Critical Reviews in Analytical Chemistry 431782232013Document47 pagesCritical Reviews in Analytical Chemistry 431782232013Jairo William Vergara DelbastosNo ratings yet
- Importance Water Quality ControlDocument10 pagesImportance Water Quality ControlYS YSNo ratings yet
- Ammonia PDFDocument5 pagesAmmonia PDFiulia100% (1)
- Isolation Purification and Identification of CurcuminoidsDocument5 pagesIsolation Purification and Identification of CurcuminoidsNguyenVan HanNo ratings yet
- Determination of VOC's in Aqueous Samples by Using Purge & Trap - GCMSDDocument5 pagesDetermination of VOC's in Aqueous Samples by Using Purge & Trap - GCMSDAbu WildanNo ratings yet
- Assignment 1 Atomic Absorption SpectroscDocument22 pagesAssignment 1 Atomic Absorption Spectroscpakpolitics206No ratings yet
- Environmental ToxicologyDocument10 pagesEnvironmental ToxicologyOmer SyedNo ratings yet
- Green Chemistry Metrics: Calculating Atom Economy, E-Factor and Mass YieldDocument28 pagesGreen Chemistry Metrics: Calculating Atom Economy, E-Factor and Mass Yieldpower-xNo ratings yet
- FTIR Analysis of Membrane SamplesDocument2 pagesFTIR Analysis of Membrane SamplesNuraienee JaminganNo ratings yet
- Iodometry Analysis of Oxidizing AgentsDocument3 pagesIodometry Analysis of Oxidizing AgentsTrecia Dela CruzNo ratings yet
- Analytical Quality Control 2007Document93 pagesAnalytical Quality Control 2007jeneveuxpasNo ratings yet
- Ilnas-En Iso 15587-1:2002Document7 pagesIlnas-En Iso 15587-1:2002Alejandro MoralesNo ratings yet
- Determination of ChromiumDocument15 pagesDetermination of ChromiumSunghava upadhayaNo ratings yet
- Water Quality Monitoring and GuidelinesDocument16 pagesWater Quality Monitoring and GuidelinesyingNo ratings yet
- Biochemistry of MethyltrophsDocument447 pagesBiochemistry of MethyltrophsMisya ChristinaNo ratings yet
- LSD-NEERI - Water Quality AnalysisDocument68 pagesLSD-NEERI - Water Quality AnalysisSubrahmanyan EdamanaNo ratings yet
- Digestion Methods for Solid SamplesDocument59 pagesDigestion Methods for Solid SamplesAnonymous NQzoR9mQNo ratings yet
- What Is PhotocatalystDocument6 pagesWhat Is Photocatalystr96221029No ratings yet
- Pesticide Residue Analysis in LaboratoryDocument21 pagesPesticide Residue Analysis in LaboratoryErwin Nur CahyantoNo ratings yet
- Principles of Ecotoxicology (PDFDrive)Document332 pagesPrinciples of Ecotoxicology (PDFDrive)Essekhyr HassanNo ratings yet
- Hazardous Drugs List 2016 161Document42 pagesHazardous Drugs List 2016 161ethylenepluschlorineNo ratings yet
- D 3731 - 87 r98 - Rdm3mzetoddsotgDocument4 pagesD 3731 - 87 r98 - Rdm3mzetoddsotgDavid AriasNo ratings yet
- Practical Titration PDFDocument164 pagesPractical Titration PDFCojocaru George0% (1)
- Reuse Sewage Water with NanotechnologyDocument18 pagesReuse Sewage Water with NanotechnologyRahul patilNo ratings yet
- Determination of Azithromycin by Ion-Pair HPLC With UV DetectionDocument5 pagesDetermination of Azithromycin by Ion-Pair HPLC With UV DetectionandresdelrojoNo ratings yet
- EE Lab Manual (1) BackupDocument207 pagesEE Lab Manual (1) BackupVamshi ChaitanyaNo ratings yet
- Removal of Pharmaceuticals From Wastewater by Fungal TreatmentDocument7 pagesRemoval of Pharmaceuticals From Wastewater by Fungal TreatmentAmirahShaleha0% (1)
- Biointerface Characterization by Advanced IR SpectroscopyFrom EverandBiointerface Characterization by Advanced IR SpectroscopyC.-M. PradierRating: 5 out of 5 stars5/5 (1)
- Insecticides: Analytical Methods for Pesticides, Plant Growth Regulators, and Food Additives, Vol. 2From EverandInsecticides: Analytical Methods for Pesticides, Plant Growth Regulators, and Food Additives, Vol. 2No ratings yet
- Biosynthesis of AntibioticsFrom EverandBiosynthesis of AntibioticsJ SnellNo ratings yet
- Hazardous Substances and Human Health: Exposure, Impact and External Cost Assessment at the European ScaleFrom EverandHazardous Substances and Human Health: Exposure, Impact and External Cost Assessment at the European ScaleNo ratings yet
- MyxedemaDocument16 pagesMyxedemaalaamedNo ratings yet
- Fatal Flu PresentationDocument26 pagesFatal Flu PresentationalaamedNo ratings yet
- Fatal Flu (H1N1-H5N1)Document15 pagesFatal Flu (H1N1-H5N1)alaamedNo ratings yet
- 2008 Bulletin of UsmleDocument40 pages2008 Bulletin of UsmleSai Pardhu100% (1)
- Management of Senile and Complicated CataractDocument11 pagesManagement of Senile and Complicated CataractalaamedNo ratings yet
- Medical SpecialityDocument1 pageMedical Specialityalaamed100% (1)
- Simulation Study of Cryogenic Air Separation PDFDocument58 pagesSimulation Study of Cryogenic Air Separation PDFAHMEDNo ratings yet
- Fisher 1975 VTM DepositsDocument18 pagesFisher 1975 VTM DepositsEdm SanNo ratings yet
- 2004 Chemistry - James Ruse With SolutionsDocument36 pages2004 Chemistry - James Ruse With SolutionsWilliam HouNo ratings yet
- CIBATOOLDocument4 pagesCIBATOOLEuclides RezendeNo ratings yet
- Racor Oil Filtration Hydraulic Filter Cart 7768Document2 pagesRacor Oil Filtration Hydraulic Filter Cart 7768sinter-musicNo ratings yet
- Characterization of NanoparticlesDocument16 pagesCharacterization of NanoparticlesPrasun SarkarNo ratings yet
- Haber Process - Case StudyDocument3 pagesHaber Process - Case StudycmkkaranNo ratings yet
- Low-pH Cement Design for Nuclear Waste StorageDocument15 pagesLow-pH Cement Design for Nuclear Waste StorageMss BranchesNo ratings yet
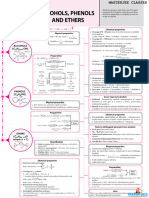
- Alcohols Phenols and EthersDocument1 pageAlcohols Phenols and EthersNitisha GuptaNo ratings yet
- Optimization, Characterization and Antibacterial Activity of Green Synthesized Silver Nanoparticles Using Moringa Oleifera Leaf ExtractDocument10 pagesOptimization, Characterization and Antibacterial Activity of Green Synthesized Silver Nanoparticles Using Moringa Oleifera Leaf ExtractshilpashreeNo ratings yet
- Sermaloy J Diffused Slurry Aluminide Coating: AdvantagesDocument1 pageSermaloy J Diffused Slurry Aluminide Coating: Advantagesbigsteve9088No ratings yet
- Identify Welding Defects & DiscontinuitiesDocument21 pagesIdentify Welding Defects & DiscontinuitiesJoanna AprilNo ratings yet
- Evaluation of antacid and carminative properties of Cucumis sativusDocument6 pagesEvaluation of antacid and carminative properties of Cucumis sativusAFRIZANo ratings yet
- Refining Processes 2004 PDFDocument293 pagesRefining Processes 2004 PDFramachandran_chem100% (1)
- Foxboro CFT50 Digital Coriolis Mass Flow TransmitterDocument4 pagesFoxboro CFT50 Digital Coriolis Mass Flow TransmitterPhaniNo ratings yet
- Materials Science II Chapter 10Document41 pagesMaterials Science II Chapter 10Rebeca CremonezNo ratings yet
- ASTM D 5454 11 Humedad Con AnalizadorDocument3 pagesASTM D 5454 11 Humedad Con AnalizadorCarlos Lopez BlumenkronNo ratings yet
- Drug-Food InteractionsDocument32 pagesDrug-Food Interactionstaskinsaiyed082No ratings yet
- Advancement in Internal Field Joint Coating SystemsDocument5 pagesAdvancement in Internal Field Joint Coating SystemsKnight rider100% (1)
- CH - 12 - Slides - Journal B.Document53 pagesCH - 12 - Slides - Journal B.Eyad AlqurashiNo ratings yet
- Litsearch UreaDocument126 pagesLitsearch Ureaemmet11100% (1)
- Maximising Molecular Sieve Performance in Gas ProcessingDocument18 pagesMaximising Molecular Sieve Performance in Gas ProcessingAhmed ElShora100% (1)
- Textile TechnologyDocument5 pagesTextile TechnologyKaye NicolasNo ratings yet
- ESI's Casting Simulation Suite Optimizes Casting ProcessesDocument16 pagesESI's Casting Simulation Suite Optimizes Casting Processesprasanna100% (1)
- Practice Naming Ionic Covalent CompoundsDocument2 pagesPractice Naming Ionic Covalent CompoundsAjay NaikNo ratings yet
- Welding Safety: By: Eng'r. Domz CanedaDocument30 pagesWelding Safety: By: Eng'r. Domz CanedaJohn BelmesNo ratings yet
- Electroplating Lab CHEM 401Document10 pagesElectroplating Lab CHEM 401anak gamerNo ratings yet
- FDS Verification GuideDocument338 pagesFDS Verification GuideDarkoNo ratings yet
- The Leaf MCQDocument5 pagesThe Leaf MCQSanjay Ku AgrawalNo ratings yet
- Wellboost 13967Document2 pagesWellboost 13967Bassem BalghouthiNo ratings yet