You might also like
- Clinical Sports Psychiatry: An International PerspectiveFrom EverandClinical Sports Psychiatry: An International PerspectiveDavid A. BaronRating: 5 out of 5 stars5/5 (1)
- Hypnosis For Sports 1Document48 pagesHypnosis For Sports 1Mahamoudou Smac Sawadogo100% (3)
- Trance and Treatment - Clinical Uses of Hypnosis. by Herbert SpiegelDocument574 pagesTrance and Treatment - Clinical Uses of Hypnosis. by Herbert Spiegelytytyt100% (16)
- ElkinsGaryEd2017HandbookofmedicalandpsychologicalhypnosisFoundationsapplicationsandprofessionalissuesNewYorkNYSpringerPublishing PDFDocument6 pagesElkinsGaryEd2017HandbookofmedicalandpsychologicalhypnosisFoundationsapplicationsandprofessionalissuesNewYorkNYSpringerPublishing PDFScarlett LinLattNo ratings yet
- Basic Ericksonian Hypnosis Ebook PDFDocument155 pagesBasic Ericksonian Hypnosis Ebook PDFFelipe Osorio100% (4)
- The Art and Practice of Hypnotic Induction: Favorite Methods of Master Clinicians: Voices of Experience, #1From EverandThe Art and Practice of Hypnotic Induction: Favorite Methods of Master Clinicians: Voices of Experience, #1Rating: 5 out of 5 stars5/5 (1)
- Hypnotherapy ExplainedDocument171 pagesHypnotherapy ExplainedDonald Cabrera Astudillo100% (8)
- The Jacquin Rope Workout 2013 Updated PDFDocument42 pagesThe Jacquin Rope Workout 2013 Updated PDFbeliefsastrange100% (2)
- Hypno CBTDocument12 pagesHypno CBTJiwan PrasadNo ratings yet
- Integrative Hypnosis Comprehensive Course in ChangeDocument774 pagesIntegrative Hypnosis Comprehensive Course in ChangeCostica Dron100% (9)
- Handbook of Hypnotic Techniques Vol. 1: Favorite Methods of Master Clinicians: Voices of Experience, #4From EverandHandbook of Hypnotic Techniques Vol. 1: Favorite Methods of Master Clinicians: Voices of Experience, #4Rating: 5 out of 5 stars5/5 (2)
- Volume Iii Clinical and Medical Hypnotherapy: Hypnoanesthesia, Pain Control, and Improved HealthFrom EverandVolume Iii Clinical and Medical Hypnotherapy: Hypnoanesthesia, Pain Control, and Improved HealthRating: 4 out of 5 stars4/5 (2)
- Yapko Hypnosis DepressionDocument3 pagesYapko Hypnosis Depression11111No ratings yet
- Handbook of Hypnotic Techniques, Vol. 2: Favorite Methods of Master Clinicians: Voices of Experience, #5From EverandHandbook of Hypnotic Techniques, Vol. 2: Favorite Methods of Master Clinicians: Voices of Experience, #5No ratings yet
- Ericksonian HypnotherapyDocument4 pagesEricksonian HypnotherapyArttacla100% (1)
- The Wisdom of Milton EricsonDocument19 pagesThe Wisdom of Milton Ericsonbbhglobal70% (10)
- Hypnotherapy and Intuitive Hypnosis: The most effective therapeutic and explorative method of the 21st centuryFrom EverandHypnotherapy and Intuitive Hypnosis: The most effective therapeutic and explorative method of the 21st centuryNo ratings yet
- Medical and Dental Hypnosis - HartlandDocument540 pagesMedical and Dental Hypnosis - HartlandAnonymous qUziTl100% (10)
- Indirect Hypnotic TherapyDocument10 pagesIndirect Hypnotic Therapyfllorinv7No ratings yet
- Big Book of HypnotherapyDocument846 pagesBig Book of HypnotherapyKolee Nnah100% (4)
- Investigative Forensic HypnosisDocument23 pagesInvestigative Forensic HypnosisPaul MazziottaNo ratings yet
- ### Sve U Jednom Od Steve G JonesDocument1,975 pages### Sve U Jednom Od Steve G JonesDarko Zhì Huì100% (1)
- Analytical Hypnotherapy Principles and Practice - E. A. BarnettDocument512 pagesAnalytical Hypnotherapy Principles and Practice - E. A. BarnettAntonio Martins100% (22)
- Hypnosis SuggestionDocument80 pagesHypnosis SuggestionMike5555555100% (13)
- Hypnosis Induction TechnicsDocument100 pagesHypnosis Induction TechnicsVít ChládNo ratings yet
- HypnotherapyDocument16 pagesHypnotherapyAnonymous lsnDTjvNo ratings yet
- Richard Nongard's Big Book of Hypnosis Scripts How To Create Lasting Change Using Contextual Hypnotherapy, Mindfulness Meditation and Hypnotic Phenomena by Richard NongardDocument203 pagesRichard Nongard's Big Book of Hypnosis Scripts How To Create Lasting Change Using Contextual Hypnotherapy, Mindfulness Meditation and Hypnotic Phenomena by Richard NongardDan Zen92% (24)
- 9781845904654Document18 pages9781845904654ObrienFinancial0% (1)
- Ideo Motor Response DemonstrationDocument0 pagesIdeo Motor Response DemonstrationAnonymous Y2qwEuANo ratings yet
- HypnosisDocument328 pagesHypnosisPabloAPacheco93% (14)
- On Theoretical Concepts and Techniques Presented in Class.: Julie Docherty 1Document5 pagesOn Theoretical Concepts and Techniques Presented in Class.: Julie Docherty 1bettyboop1312100% (2)
- BHS IN34 Dave Elman Induction PDFDocument4 pagesBHS IN34 Dave Elman Induction PDFJaktron100% (1)
- Hypnosis For Chronic PainDocument8 pagesHypnosis For Chronic Painmatthew.dyson2663No ratings yet
- Sports HypnosisDocument2 pagesSports HypnosisManoj GaurNo ratings yet
- Clinical Hypnosis Training Manual From A-ZDocument446 pagesClinical Hypnosis Training Manual From A-Zgalegator100% (6)
- Stanford Hypnotic Susceptibility ScaleDocument56 pagesStanford Hypnotic Susceptibility Scalebigthangs100% (4)
- How The Mind Works PTDDocument7 pagesHow The Mind Works PTDblackvenumNo ratings yet
- Hypnosis Scripts 2Document174 pagesHypnosis Scripts 2byron100% (26)
- Medical Meditation: How to Reduce Pain, Decrease Complications and Recover Faster from Surgery, Disease and IllnessFrom EverandMedical Meditation: How to Reduce Pain, Decrease Complications and Recover Faster from Surgery, Disease and IllnessRating: 5 out of 5 stars5/5 (2)
- Mike Mandel LessonsDocument12 pagesMike Mandel LessonsCaio AndradeNo ratings yet
- Street Hypnosis Worlds Leading Street Hypnotist Shows Techniques For The Office Stage and StreetDocument259 pagesStreet Hypnosis Worlds Leading Street Hypnotist Shows Techniques For The Office Stage and StreetLes Gorm100% (1)
- Potential Not PathologyDocument153 pagesPotential Not PathologyGilsonCostaNo ratings yet
- ChildrensHypnosisScripts IndexDocument1 pageChildrensHypnosisScripts IndexRaphaela Alencar0% (1)
- Richard Nongard - Speak EricksonianDocument137 pagesRichard Nongard - Speak Ericksonianasf zsxasd94% (18)
- The Dave Elman InductionDocument5 pagesThe Dave Elman InductionAr Hitesh Parmar100% (5)
- Memory and HypnosisDocument7 pagesMemory and HypnosisshadowraithsNo ratings yet
- Handbook of Ericksonian HypnosisDocument82 pagesHandbook of Ericksonian HypnosisMaurício Alejándro Kehrwald100% (2)
- The International Handbook of Clinical HypnosisDocument12 pagesThe International Handbook of Clinical Hypnosisbobbysingersyahoo25% (4)
- Rossi-Neuroscience Observing Consciousness Mirror Neurons HypnosisDocument16 pagesRossi-Neuroscience Observing Consciousness Mirror Neurons Hypnosisdiablero999No ratings yet
- How To Study Stephen Brooks Style of HypnotherapyDocument38 pagesHow To Study Stephen Brooks Style of HypnotherapyMahendra Bairathi100% (2)
- Script Book HypnosisDocument557 pagesScript Book Hypnosiseeliz98% (41)
- Hypnotic Techniques for Chronic Pain Management: Favorite Methods for Master Clinicians: Voices of Experience, #2From EverandHypnotic Techniques for Chronic Pain Management: Favorite Methods for Master Clinicians: Voices of Experience, #2Rating: 5 out of 5 stars5/5 (3)
- Taking Hypnosis to the Next Level: Valuable Tips for Enhancing Your Clinical PracticeFrom EverandTaking Hypnosis to the Next Level: Valuable Tips for Enhancing Your Clinical PracticeRating: 5 out of 5 stars5/5 (2)
- Sports Hypnosis in Practice: Scripts, Strategies and Case ExamplesFrom EverandSports Hypnosis in Practice: Scripts, Strategies and Case ExamplesNo ratings yet
- Migraine Relief with Hypnosis: How a Few Minutes Every Day Can Give You Energy, Clarity, and Enthusiasm to Take Care of Yourself and Your FamilyFrom EverandMigraine Relief with Hypnosis: How a Few Minutes Every Day Can Give You Energy, Clarity, and Enthusiasm to Take Care of Yourself and Your FamilyNo ratings yet
- Medical Hypnosis - Volume I - The Principles of HypnotherapyFrom EverandMedical Hypnosis - Volume I - The Principles of HypnotherapyNo ratings yet
- Tracking The Implicit Acquisition of Nonadjacent Transitional Probabilities by ErpsDocument21 pagesTracking The Implicit Acquisition of Nonadjacent Transitional Probabilities by ErpsKrisztina PálfiNo ratings yet
- A Therapist's Guide To Brief Cognitive Behavioral TherapyDocument111 pagesA Therapist's Guide To Brief Cognitive Behavioral TherapyMustafa Šuvalija95% (22)
- Drivers and Effects of Internationalising Innovation by SMEsDocument45 pagesDrivers and Effects of Internationalising Innovation by SMEsAnonymous 2Tjl8NMNNo ratings yet
- Tdcs Implicit Motor Sequence LearningDocument6 pagesTdcs Implicit Motor Sequence LearningKrisztina PálfiNo ratings yet
- Tdcs Implicit Motor Sequence LearningDocument6 pagesTdcs Implicit Motor Sequence LearningKrisztina PálfiNo ratings yet
- Tdcs Implicit Motor Sequence LearningDocument6 pagesTdcs Implicit Motor Sequence LearningKrisztina PálfiNo ratings yet
- Resilience of AthletesDocument7 pagesResilience of AthletesKrisztina PálfiNo ratings yet
- 2014 Umarex USA AIRGUN CatalogDocument75 pages2014 Umarex USA AIRGUN CatalogGene GattiNo ratings yet
- Stronglifts 5x5Document42 pagesStronglifts 5x5Dylan JamesNo ratings yet
- RespirationDocument35 pagesRespirationnabeeha malhiNo ratings yet
- IeSF Event ManualDocument26 pagesIeSF Event ManualMartinNo ratings yet
- Teen Habits Online and OfflineDocument1 pageTeen Habits Online and OfflinebohucNo ratings yet
- Mitas Terra Force EF EH Leaflet ENDocument2 pagesMitas Terra Force EF EH Leaflet ENlucscurtuNo ratings yet
- Programming and Periodization NotesDocument2 pagesProgramming and Periodization NotesBhavesh HotwaniNo ratings yet
- Template CV Sat Diver Ver 2Document5 pagesTemplate CV Sat Diver Ver 2subsea7divingcvNo ratings yet
- Makiwara Training Carl CestariDocument7 pagesMakiwara Training Carl Cestaritharaka1226No ratings yet
- LRE077ENG - Curriculum Training Suspension Systems - Air Suspension SystemsDocument207 pagesLRE077ENG - Curriculum Training Suspension Systems - Air Suspension SystemsHugo DelagarzaNo ratings yet
- Desert Exposure July 2013Document56 pagesDesert Exposure July 2013desertexposureNo ratings yet
- Ferrari 458 ItaliaDocument13 pagesFerrari 458 ItaliaBikram PrajapatiNo ratings yet
- Descriptive Text FeaturesDocument11 pagesDescriptive Text Featuresaisha rpbNo ratings yet
- PC Blues Deel 1Document454 pagesPC Blues Deel 1Christiaan PiensNo ratings yet
- 58thnssc CircularDocument10 pages58thnssc CircularDarshanSundareshNo ratings yet
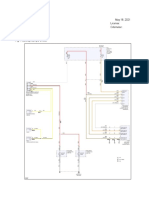
- Exterior Lights: Ymms: May 18, 2021 Engine: 3.3L Eng License: Vin: Odometer: 2017 Kia Sorento SXDocument4 pagesExterior Lights: Ymms: May 18, 2021 Engine: 3.3L Eng License: Vin: Odometer: 2017 Kia Sorento SXAndre VPNo ratings yet
- Missing Enhancement Options For Action ProfilesDocument20 pagesMissing Enhancement Options For Action ProfilesmsankarNo ratings yet
- JIU JITSU The Effective Japanese Mode of Self Defense Illustrated by Snapshots of K Koyama Amp A Minami 1916Document102 pagesJIU JITSU The Effective Japanese Mode of Self Defense Illustrated by Snapshots of K Koyama Amp A Minami 1916Mark Zlomislic100% (1)
- Permutation & CombinationDocument12 pagesPermutation & CombinationsuchipatelNo ratings yet
- Fanatic Magazine 006Document3 pagesFanatic Magazine 006Psygnosis ReddevilsNo ratings yet
- Barbearias em Jaboatão Dos GuararapesDocument12 pagesBarbearias em Jaboatão Dos GuararapesLucasNo ratings yet
- (Everyman Chess Series.) Motwani, Paul Anthony - The Most Instructive Games of The Young Grandmasters (1999, Everyman)Document180 pages(Everyman Chess Series.) Motwani, Paul Anthony - The Most Instructive Games of The Young Grandmasters (1999, Everyman)BrunoNo ratings yet
- Choose Your: by Linda SteinerDocument2 pagesChoose Your: by Linda SteinerHeryanto ChandrawarmanNo ratings yet
- Andreatta Article James LeBeauDocument8 pagesAndreatta Article James LeBeauxjaxNo ratings yet
- Registro de Asistencia y Evaluación Modulo 3 - Trabajos en Alturas (1-170)Document40 pagesRegistro de Asistencia y Evaluación Modulo 3 - Trabajos en Alturas (1-170)catalina belloNo ratings yet
- HandbookDocument96 pagesHandbookFummy OmnipotentNo ratings yet
- The Business of Sports: India - A Sporting Nation in The MakingDocument49 pagesThe Business of Sports: India - A Sporting Nation in The MakingIshan Shukla100% (1)
- Improve Your Health with Proper Fitness Goals and PrinciplesDocument15 pagesImprove Your Health with Proper Fitness Goals and PrinciplesJanelle Dava100% (1)
- Newtrasdata Ecu ListDocument7 pagesNewtrasdata Ecu ListdoktorskiNo ratings yet
- Underground Legal SteroidsDocument86 pagesUnderground Legal Steroidsbigpapaprause100% (11)