You might also like
- Exam Facts NCLEX PN Nursing Study GuideFrom EverandExam Facts NCLEX PN Nursing Study GuideRating: 3.5 out of 5 stars3.5/5 (6)
- Hesi Exit RN 2021 v1 160 QuestionsDocument4 pagesHesi Exit RN 2021 v1 160 Questionsqwivy.com33% (6)
- Medical Abbreviations GlossaryDocument15 pagesMedical Abbreviations Glossarydbryant0101100% (9)
- Dimensional Analysis For Nursing StudentsFrom EverandDimensional Analysis For Nursing StudentsNo ratings yet
- Chicago Review Press NCLEX-PN Practice Test and ReviewFrom EverandChicago Review Press NCLEX-PN Practice Test and ReviewRating: 4 out of 5 stars4/5 (4)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Hesi Hints MaternityDocument4 pagesHesi Hints MaternityThomas Stewart91% (11)
- 2009 HESI Practice - Comprehensive ExamDocument26 pages2009 HESI Practice - Comprehensive ExamQueennitaNo ratings yet
- Comprehensive Exam ReviewDocument35 pagesComprehensive Exam ReviewIndia91% (92)
- Sickle Cell AnemiaDocument37 pagesSickle Cell Anemiahazelposis75% (4)
- Hesi Exit Exam Over 700 QuestionsDocument12 pagesHesi Exit Exam Over 700 QuestionsRM Morales0% (1)
- The Chicago Review Press NCLEX-RN Practice Test and ReviewFrom EverandThe Chicago Review Press NCLEX-RN Practice Test and ReviewRating: 4 out of 5 stars4/5 (20)
- HESI Test - Free Most Up To Date SampleDocument13 pagesHESI Test - Free Most Up To Date Sample22oct201481% (32)
- OB HesiDocument3 pagesOB HesiLeena Lapena100% (4)
- Hesi Review For MaternityDocument29 pagesHesi Review For MaternitySteam Lc86% (21)
- DDocument56 pagesDDarren Balbas100% (1)
- Comprehensive Hesi Review 1Document68 pagesComprehensive Hesi Review 1Tamara Smith-Williams100% (26)
- New Text DocumentDocument3 pagesNew Text DocumentTro Wact100% (1)
- Peds ATI TakeawaysDocument4 pagesPeds ATI TakeawaysNiki95% (19)
- NCLEXstudyguidevmDocument31 pagesNCLEXstudyguidevmAnonymous vqG0paWG100% (1)
- First-Trimester Screening for Chromosomal DefectsDocument50 pagesFirst-Trimester Screening for Chromosomal DefectsManikandan PerumalNo ratings yet
- Maternal-Newborn Care ATIDocument29 pagesMaternal-Newborn Care ATIAn Nguyen90% (20)
- 2019 Rationales HESI TEST BANK MED SURG Version 2Document1 page2019 Rationales HESI TEST BANK MED SURG Version 2Prettygirl71650% (4)
- Hesi Community Health ExamDocument12 pagesHesi Community Health ExamAna BienneNo ratings yet
- Hesi ReviewDocument59 pagesHesi ReviewKrista Howe100% (3)
- Hypertension in Pregnancy ACOG 2013Document10 pagesHypertension in Pregnancy ACOG 2013lcmurillo100% (1)
- HESI NCLEX Study Guide: Essential Tips, Normal Values, MedicationsDocument21 pagesHESI NCLEX Study Guide: Essential Tips, Normal Values, MedicationsCaitlin Elliott100% (2)
- Ob HesiDocument1 pageOb HesiJoyzoey93% (27)
- Hesi Helpful HintsDocument6 pagesHesi Helpful Hintsbirenbirenpat100% (1)
- HESI Hints + More Chapter 1-Intro To TestingDocument29 pagesHESI Hints + More Chapter 1-Intro To TestingAngel Nwankwo100% (2)
- Practice Test Fundamental HesiDocument27 pagesPractice Test Fundamental HesiToTo Borgella88% (8)
- Nursing Test Taking SkillsDocument6 pagesNursing Test Taking SkillsNurseStuffNo ratings yet
- Med-Surg HESI TOPICSDocument6 pagesMed-Surg HESI TOPICSjustjesko0l100% (3)
- NATIONAL COUNCIL LICENSURE EXAMINATION FOR REGISTERED NURSES (NCLEX-RN): Passbooks Study GuideFrom EverandNATIONAL COUNCIL LICENSURE EXAMINATION FOR REGISTERED NURSES (NCLEX-RN): Passbooks Study GuideNo ratings yet
- ATI Predictor 2010 Topics To ReviewDocument8 pagesATI Predictor 2010 Topics To ReviewJonathon95% (19)
- Exam 1 ER Chest PainDocument10 pagesExam 1 ER Chest Paindinkinspdd50% (2)
- Hesi HintsDocument42 pagesHesi HintsJohn Thomas100% (2)
- Community Health HesiDocument5 pagesCommunity Health Hesisakurablossom0890% (31)
- Exit Hesi v3Document2 pagesExit Hesi v3Amy90% (10)
- 2016 HESI Exam Version 4Document30 pages2016 HESI Exam Version 4Anonymous LiMoTl100% (10)
- Sickle Cell AnemiaDocument10 pagesSickle Cell AnemiaNader Smadi100% (1)
- Pediatrics HESI Guide 2Document26 pagesPediatrics HESI Guide 2hellmanns1100% (15)
- Hesi Pre TestDocument5 pagesHesi Pre Testjosie teeh100% (1)
- Revised OB Handout Part 1 MAY 2023 PNLE RefresherDocument15 pagesRevised OB Handout Part 1 MAY 2023 PNLE RefresherMatelyn OargaNo ratings yet
- ATI PN Maternal Newborn NotesDocument13 pagesATI PN Maternal Newborn NotesDiamond Blackwell100% (6)
- Medsurg ATIDocument7 pagesMedsurg ATIloveoverpride12% (17)
- NGT InsertionDocument10 pagesNGT Insertionapi-3722454100% (3)
- 440 - Med Surg HESI 2Document8 pages440 - Med Surg HESI 2Chalcey Polson87% (15)
- Psych NSG Sample QuestionsDocument7 pagesPsych NSG Sample Questionspaul100% (8)
- HESI V2 2015 Exit ExamDocument10 pagesHESI V2 2015 Exit ExamHailey Olert100% (10)
- Medsurg and Pharm HESI ReviewDocument8 pagesMedsurg and Pharm HESI ReviewSarah Vance100% (4)
- High RiskDocument38 pagesHigh RiskDiana Rose R. Ulep100% (1)
- NCLEX Success PrayerDocument377 pagesNCLEX Success Prayerjkrix100% (2)
- 2009 HESI Practice - FundamentalsDocument14 pages2009 HESI Practice - FundamentalsQueennita100% (1)
- HESIDocument29 pagesHESIJustin Bunn100% (18)
- Q A Random - 16Document8 pagesQ A Random - 16ja100% (1)
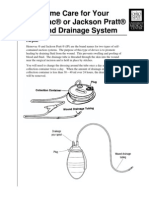
- Jackson PrattDocument7 pagesJackson PrattjulialeoNo ratings yet
- Hesi v4 Sample 2015Document2 pagesHesi v4 Sample 2015james67% (3)
- Exit Hesi Study Plan #1 10 5 11Document1 pageExit Hesi Study Plan #1 10 5 11mmgoodall22100% (1)
- Maternal Hesi Q RDocument1 pageMaternal Hesi Q RSho Ngo25% (4)
- Pediatric HESI Review 2016Document9 pagesPediatric HESI Review 2016Brittany78% (9)
- Evolve Reach - Powered by HESIDocument7 pagesEvolve Reach - Powered by HESIangelsarerare14% (7)
- NCLEX Study GuideDocument2 pagesNCLEX Study GuideLogin Nurse100% (1)
- Exam1 100731100921 Phpapp02Document34 pagesExam1 100731100921 Phpapp02Yaj CruzadaNo ratings yet
- Review of Med Surg Exam QuestionsDocument30 pagesReview of Med Surg Exam QuestionsAntonella Vitale100% (3)
- Quiz 2-Med Surg-Final Review QuestionsDocument4 pagesQuiz 2-Med Surg-Final Review QuestionsSarah Blockno100% (2)
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Parsing Nursing NotesDocument28 pagesParsing Nursing NotesjulialeoNo ratings yet
- Vancomycin Dosing and Monitoring in AdultsDocument1 pageVancomycin Dosing and Monitoring in AdultsjulialeoNo ratings yet
- Parsing Nursing NotesDocument28 pagesParsing Nursing NotesjulialeoNo ratings yet
- Article Wound DrainsDocument8 pagesArticle Wound DrainsZeynab AbokarNo ratings yet
- US Army Medical Course MD0918-100 - Nursing Care Related To The Gastrointestinal and Urinary SystemsDocument137 pagesUS Army Medical Course MD0918-100 - Nursing Care Related To The Gastrointestinal and Urinary SystemsGeorges100% (1)
- Article Wound DrainsDocument8 pagesArticle Wound DrainsZeynab AbokarNo ratings yet
- British Heart Journal, 1977, 39, 1019-1025Document7 pagesBritish Heart Journal, 1977, 39, 1019-1025julialeoNo ratings yet
- Review Notes For NCLEX CGFNS - Aortic AneurysmsDocument2 pagesReview Notes For NCLEX CGFNS - Aortic Aneurysmswyndz100% (3)
- Psychiatric Nursing QaDocument20 pagesPsychiatric Nursing QajulialeoNo ratings yet
- FellowshipbrochureDocument4 pagesFellowshipbrochurejulialeo100% (2)
- Breast SurgDocument9 pagesBreast SurgjulialeoNo ratings yet
- Nurse Patient ShipDocument97 pagesNurse Patient Shipcharby12108272100% (2)
- Sickle Cell AnemiaDocument23 pagesSickle Cell AnemiaJesmin_36No ratings yet
- Sickle Cell AnemiaDocument5 pagesSickle Cell Anemiajulialeo100% (2)
- Review Notes For NCLEX CGFNS - Aortic AneurysmsDocument2 pagesReview Notes For NCLEX CGFNS - Aortic Aneurysmswyndz100% (3)
- Triage and Response: Quick LookDocument16 pagesTriage and Response: Quick LookjulialeoNo ratings yet
- National Institutes of Health SicklecellbookletDocument16 pagesNational Institutes of Health Sicklecellbookletjulialeo100% (2)
- Triage and Response: Quick LookDocument16 pagesTriage and Response: Quick LookjulialeoNo ratings yet
- PN Dhapter59Document4 pagesPN Dhapter59julialeoNo ratings yet
- PN Dhapter57Document5 pagesPN Dhapter57julialeoNo ratings yet
- PN Dhapter58Document7 pagesPN Dhapter58julialeoNo ratings yet
- Management Placenta PreviaDocument24 pagesManagement Placenta PreviaMuhammad RifaldiNo ratings yet
- Obstetrics Study Guide 2: in The Name of GodDocument122 pagesObstetrics Study Guide 2: in The Name of GodMariam MohamedNo ratings yet
- Ectopic Molar Pregnancy A Case ReportDocument4 pagesEctopic Molar Pregnancy A Case ReportInternational Journal of Innovative Science and Research Technology100% (1)
- Vaginal Bleeding in Pregnancy - Teaching Care PlanDocument3 pagesVaginal Bleeding in Pregnancy - Teaching Care PlannajmulNo ratings yet
- Ob 11Document4 pagesOb 11Alleya SheeneNo ratings yet
- Fetal MacrosomiaDocument4 pagesFetal MacrosomiaCristhian CruzNo ratings yet
- 3rd Trimester Bleeding and Postpartum HemorrhageDocument100 pages3rd Trimester Bleeding and Postpartum Hemorrhagepeanutbutter ohNo ratings yet
- International Fetal Size Standards in Early Pregnancy: Centiles Gestational Age (Weeks + Days)Document4 pagesInternational Fetal Size Standards in Early Pregnancy: Centiles Gestational Age (Weeks + Days)Shoaib AlamNo ratings yet
- Prompt 2022Document12 pagesPrompt 2022cecilferrosNo ratings yet
- MCN Test 2 AnswerDocument3 pagesMCN Test 2 AnswerJhessel CelosoNo ratings yet
- Afhs0801 0044 2Document6 pagesAfhs0801 0044 2Noval FarlanNo ratings yet
- 1 Chapter 21 Pregnancy Complication BLEEDING DURING PREGNANCYDocument76 pages1 Chapter 21 Pregnancy Complication BLEEDING DURING PREGNANCYCAÑADA, JOHANNELYN M.No ratings yet
- Multiple PregnancyDocument16 pagesMultiple Pregnancyjane7arian7berzabalNo ratings yet
- Relationship Between Husband Support and Antenatal Care VisitsDocument9 pagesRelationship Between Husband Support and Antenatal Care VisitsWIDANINGSIH -No ratings yet
- Hiperemesis GravidarumDocument12 pagesHiperemesis GravidarumDayita ApritutiNo ratings yet
- 7726 25518 1 PBDocument12 pages7726 25518 1 PBElsa SapnawatiNo ratings yet
- Pregnancy calculations and OB scoresDocument4 pagesPregnancy calculations and OB scoresBenj GilbuenaNo ratings yet
- Reproductive Healthcare ServicesDocument6 pagesReproductive Healthcare ServicesKhairun NaharNo ratings yet
- Amniotic Fluid Disoder: Muhammad IzzatDocument26 pagesAmniotic Fluid Disoder: Muhammad IzzatcopperNo ratings yet
- PARTOGRAPHYDocument6 pagesPARTOGRAPHYapi-3705046100% (1)
- Far Eastern UniversityDocument5 pagesFar Eastern UniversitySophia Nicole BernasNo ratings yet
- Maternal, Child Health Prog-Part 2Document23 pagesMaternal, Child Health Prog-Part 2Ann Justine OrbetaNo ratings yet
- Perinatal Care Manual 4 EditionDocument457 pagesPerinatal Care Manual 4 EditionWei XinNo ratings yet
- Pengaruh Pemberian Kurma Terhadap Kemajuan Persalinan Kala Ii Ibu Bersalin Di Rumah Sakit Aura Syifa Kabupaten KediriDocument9 pagesPengaruh Pemberian Kurma Terhadap Kemajuan Persalinan Kala Ii Ibu Bersalin Di Rumah Sakit Aura Syifa Kabupaten KediriNadyaFirdausiNo ratings yet
- Assisted Breech Delivery1Document28 pagesAssisted Breech Delivery1swatisinghnigeria100% (4)
- Daftar PustakaDocument2 pagesDaftar PustakamumutdwsNo ratings yet