Katie Kloss LMT 900 NW 8th Avenue Gainesville, FL 32601 352.328.
9971
Massage Therapy Intake Form
Name __________________________________________________ Date ___________________________
Address __________________________________________________________________________________ Street City State Zip Date of Birth __________________ Occupation __________________ Phone # ____________________
Emergency Contact _________________________________________________________________________ Name Relationship Phone Number
What are your goals and/or expectations for this therapy session?
Have you ever received massage or other bodywork before? If yes, please describe your experience:
Yes
No
Are you currently taking any medications or supplements? If yes, please explain:
Yes
No
Have you ever had surgery and/or been hospitalized for any reason? If yes, please explain:
Yes
No
Have you suffered any major injuries in the past five years? If yes, please explain:
Yes
No
Are you currently seeing a physician, physical therapist, or chiropractor for any ongoing issue? If yes, please explain:
Yes
No
Do you have any allergies and/or skin sensitivities? If yes, please explain:
Yes
No
Do you have any restrictions or limitations that would affect your ability to receive massage? If yes, please explain:
Yes
No
Are there any specific areas of your body that you would like me to focus on? If yes, please specify:
Yes
No
Are there any specific areas of your body that you would like me to avoid? If yes, please specify:
Yes
No
Are you currently experiencing any pain?
Yes
No
If yes, please rate your current pain level on the following scale: 0 1 2 3 4 5 6 7 8 9 10 Yes No
Are you currently experiencing any stress?
If yes, please rate your current stress level on the following scale: 0 1 2 3 4 5 6 7 8 9 10
Are you wearing contact lenses? Are you wearing a hearing aid? Are you wearing dentures? Do you have a pacemaker? Are you taking any blood thinners? Do you bruise easily? Are you currently pregnant?
Yes Yes Yes Yes Yes Yes Yes
No No No No No No No _________ weeks
Please indicate all of the following conditions that apply to you (past or present). Y N anemia anxiety asthma autoimmune condition back pain blood clots broken bones bruxism bursitis cancer cardiovascular disease carpal tunnel syndrome chemical dependency (drugs/alcohol) chronic fatigue chronic pain constipation Crohns disease depression diabetes dizziness edema epilepsy fibromyalgia headaches heart attack hemophilia hepatitis herpes simplex high blood pressure HIV/AIDS IBS Y N insomnia low blood pressure lupus migraines multiple sclerosis muscle strain/sprain neuropathy numbness/tingling osteoarthritis osteoporosis panic disorder paralysis Parkinsons disease plantar fasciitis psoriasis PTSD respiratory issues rheumatoid arthritis sciatica scoliosis seizures shingles sinus problems stroke tendonitis thrombosis TMJ disorder/dysfunction tuberculosis varicose veins whiplash other __________________
Please use the space below to explain all YES answers:
I, _____________________________________, voluntarily consent to receive therapeutic massage services, including any related modalities within the scope of practice of my licensed massage therapist. I affirm that all of the information I have provided in this agreement is true and accurate to the best of my knowledge. I assume full responsibility for notifying the therapist of any changes to my physical and/or mental health that may occur at any point during the course of treatment. I hereby waive and release my therapist and any affiliated massage establishments and/or entities from all liability (past, present, and/or future) relating to massage therapy and/or bodywork. I understand that my personal health information and any other client records maintained by my therapist are private and confidential. I understand that my information will not be disclosed or released to any third party without my prior written consent or a subpoena or other court order. I understand that massage therapists are not physicians and that massage therapy should not be construed as a substitute for medical examination and/or treatment provided by a licensed physician. I understand that massage therapists do not diagnose any physical or mental illnesses, that they do not prescribe any medical treatments or drugs/medications, and that they do not perform any spinal or skeletal manipulations. I understand that any and all information provided to me by my therapist is strictly intended for general educational purposes only and is not diagnostically prescriptive in nature. I understand that payment is due in full at the time of service unless otherwise specified by the therapist. I agree to pay for each session with either cash or a credit/debit card (Visa, AmEx, Mastercard, Discover). I understand that my massage therapist does not accept checks as a form of payment. I agree to adhere to the following rates for each session unless otherwise specified by the therapist: $35 / 30 minutes $65 / 60 minutes $95 / 90 minutes I understand that if I am late for an appointment, the length of that session will not be extended. I agree that I will still be liable for the full payment of that appointment. If I need to cancel or reschedule an appointment for any reason, I agree that I must contact my massage therapist at least 24 hours before my scheduled appointment time in order to avoid being charged a fee. I understand that I will be responsible of the full value of the missed appointment. Emergency circumstances will be considered on an individual basis. I understand that massage therapy is strictly professional in nature. I agree that any form of misconduct on my behalf, including but not limited to any sexually suggestive or otherwise inappropriate remarks and/or gestures, will absolutely not be tolerated. I understand that any such misconduct will result in the immediate termination of the session. I understand that I will be held accountable for the full payment for the terminated appointment and that I will not be allowed to book any future appointments at this establishment. I affirm that I have carefully read this agreement in its entirety and that I fully understand and agree to all of the terms and conditions enumerated therein. I acknowledge that I am signing this legally binding document on my own free will. ____________________________________________ Client Signature ____________________________________________ Therapist Signature _________________________________________ Date _________________________________________ Date
You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- EnglishDocument56 pagesEnglishPankaj SharmaNo ratings yet
- Pharmacology Objective QuestionsDocument415 pagesPharmacology Objective QuestionsharisNo ratings yet
- Cobalt 60 VS Iridium 192Document6 pagesCobalt 60 VS Iridium 192Rares PNo ratings yet
- Accidental Intravenous Infusion of Air: A Concise ReviewDocument5 pagesAccidental Intravenous Infusion of Air: A Concise ReviewSiswand BIn Mohd AliNo ratings yet
- Pulpotomy and Pulpectomy in Children: Pulpotomy For Primary TeethDocument10 pagesPulpotomy and Pulpectomy in Children: Pulpotomy For Primary TeethVinayak SinghNo ratings yet
- Psychoanalytic EssayDocument7 pagesPsychoanalytic Essayapi-462360394No ratings yet
- About A Metered-Dose Inhaler (MDI)Document6 pagesAbout A Metered-Dose Inhaler (MDI)Sasgia ArumNo ratings yet
- ProgramaDocument2 pagesProgramaJean AntoineNo ratings yet
- Spiramycin Drug Information for Toxoplasmosis TreatmentDocument14 pagesSpiramycin Drug Information for Toxoplasmosis TreatmentRevina AmaliaNo ratings yet
- Hook Nail Deformity Surgical Treatment With A Homodigital Advancement Flap 1995 The Journal of Hand Surgery British European VolumeDocument6 pagesHook Nail Deformity Surgical Treatment With A Homodigital Advancement Flap 1995 The Journal of Hand Surgery British European VolumeProfesseur Christian DumontierNo ratings yet
- Avoiding Toxic Relationships in RecoveryDocument4 pagesAvoiding Toxic Relationships in RecoverymelodyfathiNo ratings yet
- Jcad 13 2 33Document11 pagesJcad 13 2 33ntnquynhproNo ratings yet
- Complementary and Alternative Medicines Among ResiDocument10 pagesComplementary and Alternative Medicines Among ResiKaye Reyes-HapinNo ratings yet
- AnemiaDocument40 pagesAnemiaRajaNo ratings yet
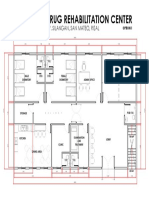
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNo ratings yet
- Endotracheal Tube ETT Insertion IntubationDocument3 pagesEndotracheal Tube ETT Insertion IntubationmochkurniawanNo ratings yet
- National Institute of Disaster ManagementDocument32 pagesNational Institute of Disaster ManagementJainNo ratings yet
- CKD CHCRTDocument28 pagesCKD CHCRTNurhidayati KeriyunNo ratings yet
- Divine Intervention Episode 22 Obgyn Shelf Review PDFDocument167 pagesDivine Intervention Episode 22 Obgyn Shelf Review PDFSwisskelly1100% (1)
- Trigger Finger PostopDocument2 pagesTrigger Finger PostopNandaSuryaWijayaNo ratings yet
- Tgwellness Massage g10pdfDocument71 pagesTgwellness Massage g10pdfStephenNo ratings yet
- Hydralazine Drug StudyDocument1 pageHydralazine Drug Studymilkv71% (7)
- Cervical Cancer (ECC)Document14 pagesCervical Cancer (ECC)Legi VamelaNo ratings yet
- Ankylosing SpodylitisDocument13 pagesAnkylosing SpodylitisMuzlifah Abdul RahmanNo ratings yet
- Acupuncture in Practice by Anthony CampbellDocument179 pagesAcupuncture in Practice by Anthony CampbellRuth Manel100% (13)
- Camptodactyly: Christian Dumontier MD, PHD Centre de La Main Guadeloupe - FwiDocument49 pagesCamptodactyly: Christian Dumontier MD, PHD Centre de La Main Guadeloupe - FwiProfesseur Christian Dumontier100% (1)
- Preventive DentistryDocument3 pagesPreventive DentistryMoataz Mohamed BarakatNo ratings yet
- ESMRDocument23 pagesESMRbiogene_bdNo ratings yet
- Magic of TouchDocument28 pagesMagic of TouchkurniawatiNo ratings yet
- Conflict Resolution Lesson Plan PDFDocument2 pagesConflict Resolution Lesson Plan PDFapi-448873912No ratings yet