You might also like
- P8 Carrivick - Anti-Mullerian Hormone Stability - Effects of Temperature and TimeDocument1 pageP8 Carrivick - Anti-Mullerian Hormone Stability - Effects of Temperature and TimeYondri Mandaku TasidjawaNo ratings yet
- Pato Fisiologi Kuliah 4 TemperatureDocument16 pagesPato Fisiologi Kuliah 4 TemperatureYondri Mandaku TasidjawaNo ratings yet
- Protein Metabolism: Department of Biochemistry Medical Faculti of Hasanuddin UniversityDocument80 pagesProtein Metabolism: Department of Biochemistry Medical Faculti of Hasanuddin UniversityYondri Mandaku TasidjawaNo ratings yet
- Urin 1Document10 pagesUrin 1Mardatillah WiranataNo ratings yet
- Blood Bank Lab WorksheetDocument1 pageBlood Bank Lab WorksheetYondri Mandaku TasidjawaNo ratings yet
- Cell Base Model of HaemostasisDocument25 pagesCell Base Model of HaemostasisYondri Mandaku TasidjawaNo ratings yet
- Detection IHCDocument129 pagesDetection IHCYondri Mandaku TasidjawaNo ratings yet
- Haider Study (2 PerhidrosisDocument7 pagesHaider Study (2 PerhidrosisYondri Mandaku TasidjawaNo ratings yet
- Critical Evaluation of Diagnosis and Outcomes of Gestational DiabetesDocument23 pagesCritical Evaluation of Diagnosis and Outcomes of Gestational DiabetesYondri Mandaku TasidjawaNo ratings yet
- All About AnorexiaDocument19 pagesAll About Anorexiajdthx4uNo ratings yet
- Bio Identical VitaminsDocument24 pagesBio Identical VitaminshamzaloNo ratings yet
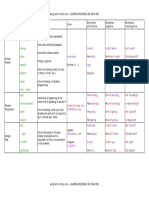
- Tenses Table PDFDocument5 pagesTenses Table PDFAlejandra Neira GonzálezNo ratings yet
- Laparoscopic Sleeve Gastrectomy: Perioperative Outcomes, Weight Loss and Impact On Type 2 Diabetes Mellitus Over 2 YearsDocument5 pagesLaparoscopic Sleeve Gastrectomy: Perioperative Outcomes, Weight Loss and Impact On Type 2 Diabetes Mellitus Over 2 YearsYondri Mandaku TasidjawaNo ratings yet
- Circulating Fragments of N-Terminal Pro-B-Type Natriuretic Peptides in Plasma of Heart Failure PatientsDocument9 pagesCirculating Fragments of N-Terminal Pro-B-Type Natriuretic Peptides in Plasma of Heart Failure PatientsYondri Mandaku TasidjawaNo ratings yet
- Red Wine and Diabetes Health: Getting Skin in The Game: R. Paul RobertsonDocument8 pagesRed Wine and Diabetes Health: Getting Skin in The Game: R. Paul RobertsonYondri Mandaku TasidjawaNo ratings yet
- 260 FullDocument7 pages260 FullYondri Mandaku TasidjawaNo ratings yet
- Artigo 13 - DM GestacionalDocument8 pagesArtigo 13 - DM GestacionalfahlevyNo ratings yet
- ADA Standards of Medical Care 2013 FINAL 21 Dec 2012Document146 pagesADA Standards of Medical Care 2013 FINAL 21 Dec 2012Mike MythiasNo ratings yet
- Curva ROC Metabolk-PasienDocument1 pageCurva ROC Metabolk-PasienYondri Mandaku TasidjawaNo ratings yet
- Print 1Document11 pagesPrint 1Yondri Mandaku TasidjawaNo ratings yet
- Nutrients 04 00208 v2Document23 pagesNutrients 04 00208 v2Yondri Mandaku TasidjawaNo ratings yet
- Aus Anorexia Nervosa PDFDocument31 pagesAus Anorexia Nervosa PDFYondri Mandaku Tasidjawa100% (1)
- 2147 FullDocument8 pages2147 FullYondri Mandaku TasidjawaNo ratings yet
- Nutrients: The Potential Role of Vitamin D Enhanced Foods in Improving Vitamin D StatusDocument19 pagesNutrients: The Potential Role of Vitamin D Enhanced Foods in Improving Vitamin D StatusYondri Mandaku TasidjawaNo ratings yet
- D-Vitamin PLOS OneDocument7 pagesD-Vitamin PLOS OneYondri Mandaku TasidjawaNo ratings yet
- Ijo 201233 ADocument8 pagesIjo 201233 AYondri Mandaku TasidjawaNo ratings yet
- Healing Power of Sunlight and Witamin DDocument26 pagesHealing Power of Sunlight and Witamin Djecan100% (1)
- Aus Anorexia Nervosa PDFDocument31 pagesAus Anorexia Nervosa PDFYondri Mandaku Tasidjawa100% (1)
- GDM PresetationDocument26 pagesGDM PresetationYondri Mandaku TasidjawaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Interview of A Tourism ExpertDocument2 pagesInterview of A Tourism ExpertDianna Kyla Cabacis UyNo ratings yet
- TUGAS MANDIRI Self InsightDocument9 pagesTUGAS MANDIRI Self InsightIrna Yunita AnnabelleNo ratings yet
- Scientific Method PPTDocument17 pagesScientific Method PPTJoshua Ramon MontanoNo ratings yet
- INGLESDocument20 pagesINGLESNikollay PeñaNo ratings yet
- End FeelDocument16 pagesEnd FeelLoganathan ChandrasekarNo ratings yet
- Installation Manual Frilo2010 EngDocument20 pagesInstallation Manual Frilo2010 Engrioma3mprNo ratings yet
- Math51H Translated For The Mathematical UnderdogDocument738 pagesMath51H Translated For The Mathematical UnderdogHow Si Yu100% (1)
- Community, Engagement, Solidarity and CitizenshipDocument10 pagesCommunity, Engagement, Solidarity and CitizenshipCyrrha Fe QuesabaNo ratings yet
- Phy582 Syllabus Mac2014Document2 pagesPhy582 Syllabus Mac2014Puteri HaslindaNo ratings yet
- FSD CB CT HandbookDocument17 pagesFSD CB CT Handbookgiriprasad gunalanNo ratings yet
- SOS in Software EngineeringDocument4 pagesSOS in Software EngineeringUltimate DiamondHeadNo ratings yet
- Adult Learners InfographicDocument3 pagesAdult Learners Infographicapi-658327748No ratings yet
- PE11-Q3-M4-Engages in MVPA - A Healthy LifestyleDocument16 pagesPE11-Q3-M4-Engages in MVPA - A Healthy LifestyleDarren Gonzales81% (16)
- Super Safari Activity Book Level 1 Sample Unit PDFDocument8 pagesSuper Safari Activity Book Level 1 Sample Unit PDFtuandt0983% (6)
- Test Bank For Interpersonal Communication Everyday Encounters 9th Edition Julia T WoodDocument8 pagesTest Bank For Interpersonal Communication Everyday Encounters 9th Edition Julia T Woodamberperezrqemidcbyx100% (26)
- Ready For PET Teacher's BookDocument66 pagesReady For PET Teacher's Bookalicia100% (1)
- Enhancing English Spelling SkillsDocument48 pagesEnhancing English Spelling Skills본술파No ratings yet
- Importance of Quantitative Research Across FieldsDocument6 pagesImportance of Quantitative Research Across FieldsJap Caranza LagunillaNo ratings yet
- Mikaila Domingo ResumeDocument2 pagesMikaila Domingo Resumeapi-440192020No ratings yet
- Spma 1p92 ResumeDocument2 pagesSpma 1p92 Resumeapi-548074204No ratings yet
- Mandatory CLE requirements for Philippine lawyersDocument2 pagesMandatory CLE requirements for Philippine lawyersJana GreenNo ratings yet
- 100 Riddles For Third Grade SampleDocument5 pages100 Riddles For Third Grade Samplemahnoor abroNo ratings yet
- Experiment 9 Diffraction Gratings: 1. How A Diffraction Grating Works?Document5 pagesExperiment 9 Diffraction Gratings: 1. How A Diffraction Grating Works?MNA tounsa sharifNo ratings yet
- DLL Tle He 6 Q1 W5Document5 pagesDLL Tle He 6 Q1 W5Louie EscuderoNo ratings yet
- Mathematics: The Normal CurveDocument20 pagesMathematics: The Normal CurveAlliyah Manzano CalvoNo ratings yet
- Methods and Approaches in Language TeachingDocument21 pagesMethods and Approaches in Language TeachingAnnie Freckles100% (3)
- Syllabus ptsv2Document7 pagesSyllabus ptsv2adam593No ratings yet
- FCI Expected Cut Off Marks 2015 AG3 JEDocument3 pagesFCI Expected Cut Off Marks 2015 AG3 JESushant SawantNo ratings yet
- The Image of God - A PsychoanalyticDocument16 pagesThe Image of God - A PsychoanalyticKNo ratings yet
- Assessment For Lesson 1.3 RPHDocument2 pagesAssessment For Lesson 1.3 RPHMikaela ImperioNo ratings yet