You might also like
- TMP 75 AADocument9 pagesTMP 75 AAFrontiersNo ratings yet
- Novel Strategy For Measuring Creatine Kinase Reaction Rate in The in Vivo HeartDocument10 pagesNovel Strategy For Measuring Creatine Kinase Reaction Rate in The in Vivo HeartYoung-Hoon SungNo ratings yet
- Original ArticleDocument7 pagesOriginal ArticleIntan AnanthaNo ratings yet
- Impact of Extracranial Contamination On Regional Cerebral Oxygen Saturation - A Comparison of Three Cerebral Oximetry TechnologiesDocument5 pagesImpact of Extracranial Contamination On Regional Cerebral Oxygen Saturation - A Comparison of Three Cerebral Oximetry TechnologiesRaluca LNo ratings yet
- Jvms 83 997Document7 pagesJvms 83 997Blanca A SerranoNo ratings yet
- tmp6585 TMPDocument8 pagestmp6585 TMPFrontiersNo ratings yet
- JCB FM 2013222 ADocument11 pagesJCB FM 2013222 Adelphinas8No ratings yet
- Biochemical Factors Concerned in the Functional Activity of the Nervous System: First International Meeting of the International Society for Neurochemistry, Strasbourg, 1967From EverandBiochemical Factors Concerned in the Functional Activity of the Nervous System: First International Meeting of the International Society for Neurochemistry, Strasbourg, 1967D. RichterNo ratings yet
- Central Role For Aldose Reductase Pathway in Myocardial Ischemic InjuryDocument8 pagesCentral Role For Aldose Reductase Pathway in Myocardial Ischemic Injurysinta mahastutiNo ratings yet
- European Journal of PharmacologyDocument6 pagesEuropean Journal of Pharmacologyliska ramdanawatiNo ratings yet
- MRM 28494Document13 pagesMRM 28494Mz AndroidNo ratings yet
- Cellular and Ionic Mechanisms Underlying Erythromycin-Induced Long QT Intervals and Torsade de PointesDocument13 pagesCellular and Ionic Mechanisms Underlying Erythromycin-Induced Long QT Intervals and Torsade de PointesAaron KaplanNo ratings yet
- Cordycepin - CA1 Membrane HyperpolarizationDocument5 pagesCordycepin - CA1 Membrane Hyperpolarizationttqnhu.rhmNo ratings yet
- Chest 1975 Capone 577 82Document8 pagesChest 1975 Capone 577 82ativonNo ratings yet
- Citicoline Improved Cardiac Function in Dysautonomia ModelDocument12 pagesCiticoline Improved Cardiac Function in Dysautonomia ModelShaimaa NasrNo ratings yet
- T. Lapainis Et Al - A Multichannel Native Fluorescence Detection System For Capillary Electrophoretic Analysis of Neurotransmitters in Single NeuronsDocument9 pagesT. Lapainis Et Al - A Multichannel Native Fluorescence Detection System For Capillary Electrophoretic Analysis of Neurotransmitters in Single NeuronsSour60No ratings yet
- Michael R. Gold and David H. Cohen - The Discharge Characteristics of Vagal Cardiac Neurons During Classically Conditioned Heart Rate ChangeDocument9 pagesMichael R. Gold and David H. Cohen - The Discharge Characteristics of Vagal Cardiac Neurons During Classically Conditioned Heart Rate ChangeLuammmNo ratings yet
- Lung Lobe Torsion in Seven Juvenile DogsDocument7 pagesLung Lobe Torsion in Seven Juvenile DogsKelvinSueyzyNo ratings yet
- Echo 2Document16 pagesEcho 2Indera VyasNo ratings yet
- Lamotrigina y VejezDocument6 pagesLamotrigina y VejezJosé Luis SHNo ratings yet
- Research Paper NS11021, A Novel Opener of Large-Conductance Ca - Activated K Channels, Enhances Erectile Responses in RatsDocument12 pagesResearch Paper NS11021, A Novel Opener of Large-Conductance Ca - Activated K Channels, Enhances Erectile Responses in RatsCarlos LabradaNo ratings yet
- Effect of Melatonin On Blood Pressure and Nitric Oxide Generation in Rats With Metabolic SyndromeDocument8 pagesEffect of Melatonin On Blood Pressure and Nitric Oxide Generation in Rats With Metabolic SyndromeExcelsis Deo SombolinggiNo ratings yet
- A Po Table: Non-Invasive Blood Glucose Monitor: S Be Strips (-+lo%), To &50Document4 pagesA Po Table: Non-Invasive Blood Glucose Monitor: S Be Strips (-+lo%), To &50anon_235673045No ratings yet
- Pluripotent Anti-Inflammatory Immunomodulatory Effects of Papaverine Against Cerebral Ischemic-Reperfusion InjuryDocument23 pagesPluripotent Anti-Inflammatory Immunomodulatory Effects of Papaverine Against Cerebral Ischemic-Reperfusion InjuryDragomir MirunaNo ratings yet
- Soluble A Peptide Increases Excitatory Neurotransmission and Induces Epileptiform Activity in Hippocampal NeuronsDocument15 pagesSoluble A Peptide Increases Excitatory Neurotransmission and Induces Epileptiform Activity in Hippocampal NeuronsClaudia Alejandra Lopez ToroNo ratings yet
- LLLT - Hypercholesterolemia (Animal Study)Document8 pagesLLLT - Hypercholesterolemia (Animal Study)prettysia suvarlyNo ratings yet
- Evaluation of Morphological Changes in Experimental Models of Myocardial Infarction: Electron and Light Microscopical EvidenceDocument11 pagesEvaluation of Morphological Changes in Experimental Models of Myocardial Infarction: Electron and Light Microscopical EvidenceRania QhalisyaNo ratings yet
- Bathia 2000 Toxicity 1.42Document11 pagesBathia 2000 Toxicity 1.42fradannusNo ratings yet
- 2020 Sanjeev Physiology International 2020Document15 pages2020 Sanjeev Physiology International 2020maloymandalNo ratings yet
- Effect of Curcumin On Inhibiting Atherogenesis by Down-Regulating Lipocalin-2 Expression in Apolipoprotein E Knockout MiceDocument11 pagesEffect of Curcumin On Inhibiting Atherogenesis by Down-Regulating Lipocalin-2 Expression in Apolipoprotein E Knockout MicemaulanaardhiNo ratings yet
- Eeg Time Series Data Analysis in Focal Cerebral Ischemic Rat ModelDocument10 pagesEeg Time Series Data Analysis in Focal Cerebral Ischemic Rat ModelAnonymous UXBSV13cNo ratings yet
- Effect of Hypoxia On Vasodilator Responses To SNAP and Levcromakalim in Guinea Pig Basilar ArteryDocument6 pagesEffect of Hypoxia On Vasodilator Responses To SNAP and Levcromakalim in Guinea Pig Basilar ArteryAnon0123No ratings yet
- Decreased Accumulation of Ultrasound Contrast in The Liver of Nonalcoholic Steatohepatitis Rat ModelDocument8 pagesDecreased Accumulation of Ultrasound Contrast in The Liver of Nonalcoholic Steatohepatitis Rat ModeldavdavdavdavdavdavdaNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptRoar SyltebøNo ratings yet
- Marco Fuenzalida Et Al - Changes of The EPSP Waveform Regulate The Temporal Window For Spike-Timing-Dependent PlasticityDocument9 pagesMarco Fuenzalida Et Al - Changes of The EPSP Waveform Regulate The Temporal Window For Spike-Timing-Dependent PlasticityFedrmNo ratings yet
- BloodDocument5 pagesBloodIstván PortörőNo ratings yet
- Ejm 19483 Original - Article Erdogmus - OzgenDocument6 pagesEjm 19483 Original - Article Erdogmus - OzgenArya GuganNo ratings yet
- Electron spin resonance spectroscopy study of ascorbic acid's effect on exercise-induced oxidative stressDocument6 pagesElectron spin resonance spectroscopy study of ascorbic acid's effect on exercise-induced oxidative stresssakuraleeshaoranNo ratings yet
- Chepalgia JournalDocument10 pagesChepalgia JournalRanintha SurbaktiNo ratings yet
- Kondo 2000, Putative Ryanodine Receptors in The Sarcolemma of Ventricular Myocytes.Document7 pagesKondo 2000, Putative Ryanodine Receptors in The Sarcolemma of Ventricular Myocytes.Alessio LissoniNo ratings yet
- Taniguchi 1983Document10 pagesTaniguchi 1983Giulia AndreeaNo ratings yet
- TMP F204Document2 pagesTMP F204FrontiersNo ratings yet
- Journal of Electroanalytical Chemistry: SciencedirectDocument8 pagesJournal of Electroanalytical Chemistry: SciencedirectLeau Sorina-AlexandraNo ratings yet
- Pilot Study of The Effectiveness of Butterfly Technique of SCENAR Therapy On Heart Rate VariabilityDocument7 pagesPilot Study of The Effectiveness of Butterfly Technique of SCENAR Therapy On Heart Rate VariabilityParallaxsterNo ratings yet
- Z. Yan Et Al - Coordinated Expression of Muscarininc Receptor Messenger RNAs in Straital Medium Spiny NeuronsDocument8 pagesZ. Yan Et Al - Coordinated Expression of Muscarininc Receptor Messenger RNAs in Straital Medium Spiny NeuronsJunmajNo ratings yet
- Rhythm Dynamics of the Aging Heart: an Experimental StudyDocument41 pagesRhythm Dynamics of the Aging Heart: an Experimental StudyHongyu LiNo ratings yet
- Biosensors: Single-Drop Analysis of Epinephrine and Uric Acid On A Screen-Printed Carbon ElectrodeDocument17 pagesBiosensors: Single-Drop Analysis of Epinephrine and Uric Acid On A Screen-Printed Carbon Electrodewidia waatiNo ratings yet
- Korean Journal of AcupunctureDocument3 pagesKorean Journal of AcupuncturenaemNo ratings yet
- T.G.J. Allen and G. Burnstock - Intracellular Studies of The Electrophysiological Properties of Cultured Intracardiac Neurones of The Guinea-PigDocument18 pagesT.G.J. Allen and G. Burnstock - Intracellular Studies of The Electrophysiological Properties of Cultured Intracardiac Neurones of The Guinea-PigLuammmNo ratings yet
- Proton-Nuclear-Magnetic-Resonance Studies of Serum, Plasma and Urine From Fasting Normal Diabetic SubjectsDocument11 pagesProton-Nuclear-Magnetic-Resonance Studies of Serum, Plasma and Urine From Fasting Normal Diabetic SubjectsKeyla MaydeeNo ratings yet
- BF02462837Document4 pagesBF02462837ttqnhu.rhmNo ratings yet
- Mecanismos 2Document8 pagesMecanismos 2Arellano M VictorNo ratings yet
- Receptor For Activated C Kinase 1 in Rats With IscDocument7 pagesReceptor For Activated C Kinase 1 in Rats With IscEko SiswantoNo ratings yet
- Bear&KirkwoodDocument11 pagesBear&KirkwoodswagatarcNo ratings yet
- Effects of Low Concentrations of 4-Aminopyridine On CA1 Pyramidal Cells of The HippocampusDocument18 pagesEffects of Low Concentrations of 4-Aminopyridine On CA1 Pyramidal Cells of The HippocampusJortegloriaNo ratings yet
- Sympathetic Modulation by Antihypertensive DrugsDocument3 pagesSympathetic Modulation by Antihypertensive Drugsthomas albertNo ratings yet
- Lei 1998Document12 pagesLei 19980hitk0No ratings yet
- Marcel Hörning Et Al - Wave Emission On Interacting Heterogeneities in Cardiac TissueDocument8 pagesMarcel Hörning Et Al - Wave Emission On Interacting Heterogeneities in Cardiac TissueGretymjNo ratings yet
- Adenosine A1 Receptors Mediate Mobilization of Calcium in Human Bronchial Smooth MuscDocument7 pagesAdenosine A1 Receptors Mediate Mobilization of Calcium in Human Bronchial Smooth MuscLeonel LedezmaNo ratings yet
- Parent-Ver-Sch-0-6yrs Color PDFDocument2 pagesParent-Ver-Sch-0-6yrs Color PDFDM XyzNo ratings yet
- Zeman - Consciousness - ReviewDocument27 pagesZeman - Consciousness - ReviewBogdan BNo ratings yet
- Product Guide FALL 2017 Product Guide: Europe EnglishDocument60 pagesProduct Guide FALL 2017 Product Guide: Europe EnglishBogdan BNo ratings yet
- Servey Question ExamDocument14 pagesServey Question ExamalokkritsimNo ratings yet
- Zeman - Consciousness - ReviewDocument27 pagesZeman - Consciousness - ReviewBogdan BNo ratings yet
- MindfulnessWell BeingDocument27 pagesMindfulnessWell BeingchandusgNo ratings yet
- Baars Theatre of ConsciousnessDocument210 pagesBaars Theatre of ConsciousnessBogdan BNo ratings yet
- CFQ and Its CorrelatesDocument16 pagesCFQ and Its CorrelatesBogdan BNo ratings yet
- Identify MindDocument54 pagesIdentify MindBogdan BNo ratings yet
- Pos Psy and EduDocument15 pagesPos Psy and EduBogdan BNo ratings yet
- Conscious PerceptionDocument2 pagesConscious PerceptionBogdan BNo ratings yet
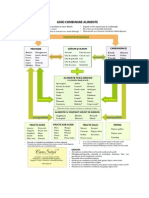
- Food CategoryDocument1 pageFood CategoryBogdan BNo ratings yet
- Educatie InterculturalaDocument161 pagesEducatie InterculturalaBogdan B100% (1)
- Anchor ItemsDocument20 pagesAnchor ItemsBogdan BNo ratings yet
- RadiestezieDocument41 pagesRadiestezielacrimioara_cenusa100% (3)
- Food Combining 2Document1 pageFood Combining 2Bogdan BNo ratings yet
- Popol Vuh - Sacred Book of The Quichè Maya PeopleDocument287 pagesPopol Vuh - Sacred Book of The Quichè Maya PeopleAvalonRa100% (8)
- EHTPA CurriculumDocument109 pagesEHTPA Curriculumjle_dl0% (1)
- The Earliest Relationship Parents, Infants, and The Drama of EaDocument280 pagesThe Earliest Relationship Parents, Infants, and The Drama of EaBogdan BNo ratings yet
- How Facebook, TikTok and YouTube Impact Teen Mental Health and WellbeingDocument2 pagesHow Facebook, TikTok and YouTube Impact Teen Mental Health and WellbeingBogdan BNo ratings yet
- Food Combining ChartDocument1 pageFood Combining ChartBogdan BNo ratings yet
- Popol Vuh - Sacred Book of The Quichè Maya PeopleDocument287 pagesPopol Vuh - Sacred Book of The Quichè Maya PeopleAvalonRa100% (8)
- Lab Report 2000 Words Heavily EditedDocument6 pagesLab Report 2000 Words Heavily EditedKevin WilliamNo ratings yet
- Nurseslabs Lab ValuesDocument2 pagesNurseslabs Lab ValuesJiro ManawariNo ratings yet
- Secondary Immunodeficiency in ChildrenDocument16 pagesSecondary Immunodeficiency in Childrenryan20eNo ratings yet
- Complete Blood Count and Biochemistry Panel ResultsDocument8 pagesComplete Blood Count and Biochemistry Panel Resultsgunjan pratapNo ratings yet
- Rolling NAJSPTDocument13 pagesRolling NAJSPTDiego LacerdaNo ratings yet
- Unit 4 Human Value & EthicsDocument20 pagesUnit 4 Human Value & EthicsElaiyarjaNo ratings yet
- Navy Weed Control & Plant Growth RegDocument179 pagesNavy Weed Control & Plant Growth RegSpace_Hulker100% (1)
- Anosmia in Covid-19 Infection - A Case SeriesDocument4 pagesAnosmia in Covid-19 Infection - A Case SeriesIJAR JOURNALNo ratings yet
- Genetic Algorithm Based PID Control Tuning For A Model BioreactorDocument13 pagesGenetic Algorithm Based PID Control Tuning For A Model BioreactorertyucbNo ratings yet
- Effects of Hypotonic, Isotonic & Hypertonic SolutionsDocument19 pagesEffects of Hypotonic, Isotonic & Hypertonic SolutionsTanesh SelvarajuNo ratings yet
- The Study of Life: Teacher Notes and AnswersDocument4 pagesThe Study of Life: Teacher Notes and AnswersHector AguilarNo ratings yet
- Microb Monitor 2 Instructions UseDocument5 pagesMicrob Monitor 2 Instructions UseArluky NovandyNo ratings yet
- Chapter 3 - Antibody Topic NotesDocument10 pagesChapter 3 - Antibody Topic NotesAngelica Joy GonzalesNo ratings yet
- GNM German New Medicine OverviewDocument6 pagesGNM German New Medicine OverviewHoria Teodor Costan100% (2)
- SEKOLAH KEBANGSAAN TEBONG BAHASA INGGERIS TESTDocument8 pagesSEKOLAH KEBANGSAAN TEBONG BAHASA INGGERIS TESTkomathyNo ratings yet
- Timetable LECTURESDocument4 pagesTimetable LECTURESRebeccaNo ratings yet
- QC ABO RH BloodDocument62 pagesQC ABO RH BloodrhoderickNo ratings yet
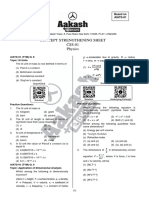
- Concept Strengthening Sheet (CSS-01) Based On AIATS-01 RMDocument19 pagesConcept Strengthening Sheet (CSS-01) Based On AIATS-01 RMB54 Saanvi SinghNo ratings yet
- Chemistry in Everyday LifeDocument14 pagesChemistry in Everyday LifeAkhil NandanNo ratings yet
- Fourtee: Echinoderms and HemichordatesDocument20 pagesFourtee: Echinoderms and HemichordatesMaharani Putri Chania100% (1)
- Frances Boa Methodology QuestionDocument39 pagesFrances Boa Methodology Questionmonday125No ratings yet
- Evalution ReportDocument44 pagesEvalution ReportkamilNo ratings yet
- Year 12 Biology - CH 10 Genes and DNADocument4 pagesYear 12 Biology - CH 10 Genes and DNAJessica100% (1)
- Shellfish Morphology GuideDocument9 pagesShellfish Morphology GuideParimita SharmaNo ratings yet
- Pathogenic FungiDocument65 pagesPathogenic FungiTamara ElyasNo ratings yet
- Immunomodulatory and Growth Performance Effects of Ginsemg ExtractsDocument13 pagesImmunomodulatory and Growth Performance Effects of Ginsemg ExtractsOliver TalipNo ratings yet
- Learning Activity Sheet: SUBJECT: Earth and Life Science Mastery Test For Quarter 2 - Week 1&2Document1 pageLearning Activity Sheet: SUBJECT: Earth and Life Science Mastery Test For Quarter 2 - Week 1&2Kiara Ash BeethovenNo ratings yet
- Bioteknologi: Epi Supri Wardi, M.Si Universitas Perintis Indonesia (UPERTIS) Padang, 2021Document28 pagesBioteknologi: Epi Supri Wardi, M.Si Universitas Perintis Indonesia (UPERTIS) Padang, 2021Mezi ZhahriNo ratings yet
- Bor Kavcic: Electrodynamics of Human HeartDocument14 pagesBor Kavcic: Electrodynamics of Human HearttohunabohunNo ratings yet
- Combined Stresses in PlantsDocument281 pagesCombined Stresses in Plantsmdg21No ratings yet