You might also like
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- Geriatrics: Roger E. ThomasDocument44 pagesGeriatrics: Roger E. ThomasSubhash SharmaNo ratings yet
- Soap2 PDFDocument13 pagesSoap2 PDFframc3sca2911No ratings yet
- Prescribing Patterns of Drugs in Outpatient Department of Paediatrics in Tertiary Care HospitalDocument12 pagesPrescribing Patterns of Drugs in Outpatient Department of Paediatrics in Tertiary Care HospitalAleena Maria KurisinkalNo ratings yet
- Polypharmacy Guidance 2018Document85 pagesPolypharmacy Guidance 2018stuckinbedNo ratings yet
- Helping Patients Make The Most of Their MedicinesDocument13 pagesHelping Patients Make The Most of Their MedicinesArif ShikalgarNo ratings yet
- Pharmacoepidemiology and Pharmacovigilance: Synergistic Tools to Better Investigate Drug SafetyFrom EverandPharmacoepidemiology and Pharmacovigilance: Synergistic Tools to Better Investigate Drug SafetyRating: 4.5 out of 5 stars4.5/5 (3)
- 11 Octubre 7 EUMDocument9 pages11 Octubre 7 EUMJuliana SanchezNo ratings yet
- Physician Factors Associated With Polypharmacy and Potentially Inappropriate Medication UseDocument9 pagesPhysician Factors Associated With Polypharmacy and Potentially Inappropriate Medication UseratnatriaaNo ratings yet
- Chapter 1 - Pharma DostDocument3 pagesChapter 1 - Pharma DostabinchandrakumarNo ratings yet
- Essential Pharmacology For Inpatient CareFrom EverandEssential Pharmacology For Inpatient CareRating: 4.5 out of 5 stars4.5/5 (7)
- 15 UsePrescription PDFDocument14 pages15 UsePrescription PDFIJAERS JOURNALNo ratings yet
- Pharmacoepidemiology: Past, Present and FutureDocument57 pagesPharmacoepidemiology: Past, Present and FutureMuhammad TaufikNo ratings yet
- Pharmacoepidemiology: Origin & EvolutionDocument5 pagesPharmacoepidemiology: Origin & EvolutiongowthamNo ratings yet
- Non-Adherence To Diabetes Treatment at Mulago Hospital in Uganda: Prevalence and Associated FactorsDocument10 pagesNon-Adherence To Diabetes Treatment at Mulago Hospital in Uganda: Prevalence and Associated FactorsPaulineNo ratings yet
- Bahan 2-DikonversiDocument11 pagesBahan 2-DikonversiMaya ismayaNo ratings yet
- Mr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaDocument6 pagesMr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaHariom RajputNo ratings yet
- Monitoring of Patients On Long-Term Glucocorticoid TherapyDocument10 pagesMonitoring of Patients On Long-Term Glucocorticoid TherapyFitriyana WinarnoNo ratings yet
- 2018 Value-in-HeDocument7 pages2018 Value-in-HeArchie CabacheteNo ratings yet
- Prevalence and Predictors of Potentially Inappropriate Medications Among Home Care Elderly Patients in QatarDocument7 pagesPrevalence and Predictors of Potentially Inappropriate Medications Among Home Care Elderly Patients in QatarSundas EjazNo ratings yet
- Article Wjpps 1469869064Document10 pagesArticle Wjpps 1469869064Lucia SibiiNo ratings yet
- Renal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysFrom EverandRenal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysNo ratings yet
- Drug Prescribing Patterns in Elderly Patients in A Tertiary Level HospitalDocument6 pagesDrug Prescribing Patterns in Elderly Patients in A Tertiary Level Hospitalsangita sukumaranNo ratings yet
- (JURNAL, Eng) Potentially Inappropriate Prescribing To Older Patients in Primary Care in The Netherlands, A Retrospective Longitudinal StudyDocument6 pages(JURNAL, Eng) Potentially Inappropriate Prescribing To Older Patients in Primary Care in The Netherlands, A Retrospective Longitudinal StudyAurellia Annisa WulandariNo ratings yet
- 1471 2474 13 180 PDFDocument8 pages1471 2474 13 180 PDFDini BayuariNo ratings yet
- Ka 1Document6 pagesKa 1DHIVYANo ratings yet
- PolypharmacyDocument4 pagesPolypharmacyJeffrey Tan100% (1)
- 18 Gouri Et AlDocument6 pages18 Gouri Et AleditorijmrhsNo ratings yet
- 1268 PDFDocument5 pages1268 PDFCMargs ConceptsNo ratings yet
- The Study of Drug Usage Patterns in Pediatric Patients at MGM Hospital, Navi MumbaiDocument10 pagesThe Study of Drug Usage Patterns in Pediatric Patients at MGM Hospital, Navi Mumbairajesh sumanNo ratings yet
- Medicacion InapropiadaDocument22 pagesMedicacion Inapropiadaagu oliveroNo ratings yet
- Faculty of Medicine, Novi Sad, SerbiaDocument5 pagesFaculty of Medicine, Novi Sad, SerbiaAnkete FNo ratings yet
- Interventions in Nursing HomesDocument18 pagesInterventions in Nursing Homesvictory818No ratings yet
- Pa Issue Brief FinalDocument21 pagesPa Issue Brief FinalAsja AvdićNo ratings yet
- Inappropriate Use of Proton Pump Inhibitors in Elderly Patients Discharged From Acute Care HospitalsDocument6 pagesInappropriate Use of Proton Pump Inhibitors in Elderly Patients Discharged From Acute Care HospitalsFitriNo ratings yet
- Bpac Polypharmacy Poem 2006 PFDocument20 pagesBpac Polypharmacy Poem 2006 PFJacob Alexander MarpaungNo ratings yet
- Assessing Adherence Before Changing Hypertension MedicationDocument4 pagesAssessing Adherence Before Changing Hypertension MedicationSyifa MunawarahNo ratings yet
- TrialsDocument25 pagesTrialsJason_Cordova_5798No ratings yet
- Assessment On Prevalence of Polypharmacy in Geriatric Patients With Cardiovascular DiseasesDocument12 pagesAssessment On Prevalence of Polypharmacy in Geriatric Patients With Cardiovascular DiseasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pharmacy: Ingestible Sensors and Medication Adherence: Focus On Use in Serious Mental IllnessDocument11 pagesPharmacy: Ingestible Sensors and Medication Adherence: Focus On Use in Serious Mental IllnessArif IrpanNo ratings yet
- Prescription Completeness and Drug Use PatternDocument7 pagesPrescription Completeness and Drug Use Patternadane yehualawNo ratings yet
- The Effect of A Structured Medication Review On Quality of Life in Parkinson's Disease The Study ProtocolDocument7 pagesThe Effect of A Structured Medication Review On Quality of Life in Parkinson's Disease The Study ProtocolGurgehNo ratings yet
- 1642-Article Text-7699-1-10-20200623Document5 pages1642-Article Text-7699-1-10-20200623mtgnzgaNo ratings yet
- HPCP Assignment 2Document8 pagesHPCP Assignment 2mokshmshah492001No ratings yet
- Drug Utilization ReviewDocument36 pagesDrug Utilization ReviewEdilma VargasNo ratings yet
- 21 Iajps21102017 PDFDocument9 pages21 Iajps21102017 PDFBaru Chandrasekhar RaoNo ratings yet
- Literature Review PolypharmacyDocument12 pagesLiterature Review Polypharmacyea8p6td0100% (1)
- Goh2009 PDFDocument10 pagesGoh2009 PDFekaNo ratings yet
- Medicine Price Surveys, Analyses and Comparisons: Evidence and Methodology GuidanceFrom EverandMedicine Price Surveys, Analyses and Comparisons: Evidence and Methodology GuidanceSabine VoglerNo ratings yet
- Lorne Basskin - Practical PE ArticleDocument5 pagesLorne Basskin - Practical PE ArticleCatalina Dumitru0% (1)
- 11 UptodateDocument34 pages11 UptodaterosairoNo ratings yet
- Ka 2Document8 pagesKa 2DHIVYANo ratings yet
- Ad Hoc Data Sources for Pharmacoepidemiological StudiesDocument11 pagesAd Hoc Data Sources for Pharmacoepidemiological StudiesVINAY KUMARNo ratings yet
- BMC Medicine: Patient-Centred Tuberculosis Treatment Delivery Under Programmatic Conditions in Tanzania: A Cohort StudyDocument10 pagesBMC Medicine: Patient-Centred Tuberculosis Treatment Delivery Under Programmatic Conditions in Tanzania: A Cohort StudyNay Lin HtikeNo ratings yet
- Drug Utilisation Study of UTIDocument4 pagesDrug Utilisation Study of UTIviva.anu24No ratings yet
- Pharmacocinetics GeriatricDocument11 pagesPharmacocinetics GeriatricDiana Chavarro RodriguezNo ratings yet
- IkhsanDocument14 pagesIkhsanSilvia Icha RiskiNo ratings yet
- Makalah KesehatanDocument9 pagesMakalah KesehatanNini RahmiNo ratings yet
- Brad FordDocument12 pagesBrad FordQi ChaoNo ratings yet
- BT 2019Document13 pagesBT 2019biotech_vidhyaNo ratings yet
- Facs ProtocolDocument7 pagesFacs ProtocolmisterxNo ratings yet
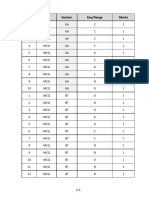
- Q.No. Type Section Key/Range MarksDocument3 pagesQ.No. Type Section Key/Range Marksbiotech_vidhyaNo ratings yet
- Stripping For ReprobingDocument2 pagesStripping For ReprobingStella SalvatoreNo ratings yet
- Components Reaction MixtureDocument3 pagesComponents Reaction Mixturebiotech_vidhyaNo ratings yet
- SDS PageDocument2 pagesSDS Pagebiotech_vidhyaNo ratings yet
- Troubleshooting SDS-PAGE 1Document3 pagesTroubleshooting SDS-PAGE 1biotech_vidhyaNo ratings yet
- Stripping For ReprobingDocument2 pagesStripping For ReprobingStella SalvatoreNo ratings yet
- TNPSC Group 1 Prelim Book List PDFDocument2 pagesTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaNo ratings yet
- Polymerasen GuideDocument16 pagesPolymerasen Guidebiotech_vidhyaNo ratings yet
- Polymerase Chain Reaction (PCR)Document3 pagesPolymerase Chain Reaction (PCR)biotech_vidhyaNo ratings yet
- Buffer Preparation Guide for DNA/Protein Work (Shi LabDocument6 pagesBuffer Preparation Guide for DNA/Protein Work (Shi Labbiotech_vidhyaNo ratings yet
- Buffer Preparation Guide for DNA/Protein Work (Shi LabDocument6 pagesBuffer Preparation Guide for DNA/Protein Work (Shi Labbiotech_vidhyaNo ratings yet
- Whole Cell ExtractDocument1 pageWhole Cell Extractbiotech_vidhyaNo ratings yet
- Nuclear ExtractsDocument2 pagesNuclear Extractsbiotech_vidhyaNo ratings yet
- TNPSC Group 1 Prelim Book List PDFDocument2 pagesTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaNo ratings yet
- Befcv List PDFDocument22 pagesBefcv List PDFbiotech_vidhyaNo ratings yet
- TNPSC Group 1 Prelim Book List PDFDocument2 pagesTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaNo ratings yet
- Qpaper PondyDocument21 pagesQpaper Pondybiotech_vidhyaNo ratings yet
- ESE 2017 Mechanical Engineering Prelims Exam Detailed SolutionDocument52 pagesESE 2017 Mechanical Engineering Prelims Exam Detailed SolutionpataNo ratings yet
- Ies 17 Set A Me Q ADocument67 pagesIes 17 Set A Me Q Abiotech_vidhyaNo ratings yet
- Mechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010Document20 pagesMechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010biotech_vidhyaNo ratings yet
- Img Word-To PDFDocument3 pagesImg Word-To PDFbiotech_vidhyaNo ratings yet
- A.E. (Mechanical Engineering I) 2007Document24 pagesA.E. (Mechanical Engineering I) 2007Mukesh KumarNo ratings yet
- Qpaper PondyDocument21 pagesQpaper Pondybiotech_vidhyaNo ratings yet
- TDC 41597 A (Mechanical Engg.) - 2012Document20 pagesTDC 41597 A (Mechanical Engg.) - 2012biotech_vidhyaNo ratings yet
- Recruitment RulesDocument5 pagesRecruitment Rulesbiotech_vidhyaNo ratings yet
- Part and Mold Design GuideDocument170 pagesPart and Mold Design GuideminhtintinNo ratings yet
- 1 TolerancesDocument1 page1 Tolerancesbiotech_vidhyaNo ratings yet