You might also like
- Bihs PDFDocument4 pagesBihs PDFFredrikus Lay Berkh MansNo ratings yet
- Lecture 1 antihypertensionSDSDocument7 pagesLecture 1 antihypertensionSDSSara AbbasNo ratings yet
- Anti-Anginal Drugs PharmacologyDocument24 pagesAnti-Anginal Drugs PharmacologyDharun RanganathanNo ratings yet
- Drugs Used in Heart FailureDocument27 pagesDrugs Used in Heart Failurealeah morenoNo ratings yet
- beta-blockers-and-calcium-channel-blockersDocument34 pagesbeta-blockers-and-calcium-channel-blockersnevena.stankovic986No ratings yet
- PharmaAntianginal DrugsDocument175 pagesPharmaAntianginal DrugsNidal AbboudNo ratings yet
- Drugs For Systemic Hypertension and Angina: What's New?Document6 pagesDrugs For Systemic Hypertension and Angina: What's New?Diana GarcíaNo ratings yet
- Heat Failure DrugsDocument8 pagesHeat Failure DrugsDaniel MwiluNo ratings yet
- Pharmacology Chapter 42 p-3Document19 pagesPharmacology Chapter 42 p-3sho bartNo ratings yet
- Cardio Lab MedsDocument11 pagesCardio Lab MedsDianne Erika MeguinesNo ratings yet
- Case Study Number 1Document5 pagesCase Study Number 1Kevin Kyle RizarriNo ratings yet
- Anti Hypertensive 20191211Document35 pagesAnti Hypertensive 20191211helloitsmenadNo ratings yet
- Pharmacotherapy of Hypertention TerbaruDocument45 pagesPharmacotherapy of Hypertention TerbarulisaNo ratings yet
- Angina PectorisDocument4 pagesAngina PectorisKrishnendu RayNo ratings yet
- HTN Treatment Options: Choosing the Right DrugDocument46 pagesHTN Treatment Options: Choosing the Right DrugvishvasNo ratings yet
- Ischemic Heart Diease PDFDocument33 pagesIschemic Heart Diease PDFMahamed Wefkey OmranNo ratings yet
- Calcium Channel Blockers: Mechanisms, Types, Uses & Side EffectsDocument6 pagesCalcium Channel Blockers: Mechanisms, Types, Uses & Side EffectsManyal Kutin KoakNo ratings yet
- Cardiac ArrhythmiaDocument101 pagesCardiac ArrhythmiaYuvraj ChauhanNo ratings yet
- Anesthetic Management of The Hypertensive Patient: Part II: Continuing Education in Honor of Norman Trieger, DMD, MDDocument8 pagesAnesthetic Management of The Hypertensive Patient: Part II: Continuing Education in Honor of Norman Trieger, DMD, MDFitri Aesthetic centerNo ratings yet
- UKMLA QbankDocument1 pageUKMLA Qbankdrjames730No ratings yet
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- ACE Inhibitors and ARBsDocument20 pagesACE Inhibitors and ARBsMylene MendozaNo ratings yet
- Chapter 17 Cardiovascular DrugsDocument35 pagesChapter 17 Cardiovascular Drugsaisyahasrii_No ratings yet
- 6.a.antianginal DrugsDocument19 pages6.a.antianginal DrugswinnirNo ratings yet
- 10 and 11 Treatment of Hypertension and AnginaDocument10 pages10 and 11 Treatment of Hypertension and AnginaBrandon AviciiNo ratings yet
- Drugs Without Positive Inotropic Effect Used in HFDocument12 pagesDrugs Without Positive Inotropic Effect Used in HFDana HamarshehNo ratings yet
- ACE Inhibitors or ARBsDocument3 pagesACE Inhibitors or ARBsJill QuilangNo ratings yet
- Pharmacotherapy of Congestive Heart Failure (CHF)Document163 pagesPharmacotherapy of Congestive Heart Failure (CHF)Aditya rathoreNo ratings yet
- Vasodil - Ischemic Heart DiseaseDocument52 pagesVasodil - Ischemic Heart DiseaseNorms YoramNo ratings yet
- AntiHypertensives (Autosaved)Document64 pagesAntiHypertensives (Autosaved)UsamaNo ratings yet
- Obat Yang Bekerja Pada Sistem KardiovaskulerDocument18 pagesObat Yang Bekerja Pada Sistem KardiovaskulerMuhammad IkbalNo ratings yet
- Anti Hypertensive Drugs - ACE InhibitorDocument16 pagesAnti Hypertensive Drugs - ACE InhibitorApurba Sarker Apu100% (1)
- Cardiovascular System Pharmacology: Pharmacology Ii DR E KeziaDocument15 pagesCardiovascular System Pharmacology: Pharmacology Ii DR E KeziaJohnNo ratings yet
- ACE Inhibitors & Angiotensin II Antagonists: October 1997Document4 pagesACE Inhibitors & Angiotensin II Antagonists: October 1997indee533No ratings yet
- Antihypertension: Prajogo WibowoDocument45 pagesAntihypertension: Prajogo WibowoDesti Ratna PutriNo ratings yet
- Antihypertensive Pharmacologic Agents: Nr33 K Burger, Msed, MSN, RN, CneDocument28 pagesAntihypertensive Pharmacologic Agents: Nr33 K Burger, Msed, MSN, RN, CneLopez JoeNo ratings yet
- FARMAKOGNOSI - Obat AntihipertensiDocument7 pagesFARMAKOGNOSI - Obat AntihipertensiTrianisa FebyNo ratings yet
- Cardiovascular Pharmacology ConceptsDocument11 pagesCardiovascular Pharmacology ConceptsHuney Kumar100% (1)
- Congestive Heart Failure Drug TreatmentDocument12 pagesCongestive Heart Failure Drug TreatmentDian NugraNo ratings yet
- Cardiovascular PharmacologyDocument61 pagesCardiovascular PharmacologyTeeOne920% (1)
- Cilnidipine 1Document62 pagesCilnidipine 1dkhandke0% (1)
- Uses and AdministrationDocument5 pagesUses and AdministrationVera CarolinaNo ratings yet
- Ischemic Heart Disease Revised LMKDocument50 pagesIschemic Heart Disease Revised LMKLateef KhanNo ratings yet
- CVS (HF, HTN) PharmacologyDocument99 pagesCVS (HF, HTN) PharmacologyCherenet TomaNo ratings yet
- HP 200704 Pharmacological PDFDocument5 pagesHP 200704 Pharmacological PDFIndira Damar PangestuNo ratings yet
- 1 Antihypertensive DrugsDocument14 pages1 Antihypertensive DrugsReda SoNo ratings yet
- Antihypertensive Drugs: HypertensionDocument8 pagesAntihypertensive Drugs: Hypertensionalmastar officeNo ratings yet
- Antihypertensive Drugs: S. Parasuraman, M.Pharm., PH.D.Document44 pagesAntihypertensive Drugs: S. Parasuraman, M.Pharm., PH.D.Shreya SinhaNo ratings yet
- Angiotensin Receptor Blockers (ARBs) PDFDocument3 pagesAngiotensin Receptor Blockers (ARBs) PDFpriya singhNo ratings yet
- Heart FailureDocument37 pagesHeart FailureNashita NowshinNo ratings yet
- Antihypertensive Drugs: Dr/Azza Baraka Prof of Clinical Pharmacology Faculty of Medicine Alexandria UniversityDocument71 pagesAntihypertensive Drugs: Dr/Azza Baraka Prof of Clinical Pharmacology Faculty of Medicine Alexandria UniversityMoonAIRNo ratings yet
- Vasodilators by Hiren PatelDocument28 pagesVasodilators by Hiren PatelHiren_Patel_2427No ratings yet
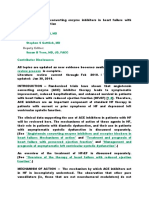
- Use of Angiotensin Converting Enzyme Inhibitors in Heart Failure With Reduced Ejection FractionDocument20 pagesUse of Angiotensin Converting Enzyme Inhibitors in Heart Failure With Reduced Ejection FractionTrung NamNo ratings yet
- Anti-Angina Drugs for Chest Pain ReliefDocument60 pagesAnti-Angina Drugs for Chest Pain ReliefPranish SawantNo ratings yet
- Skema HipertensiDocument4 pagesSkema HipertensiAndri wijayaNo ratings yet
- Anti Arrhythmic DrugsDocument91 pagesAnti Arrhythmic DrugsAlex beharuNo ratings yet
- Cardiovascular Endocrinology and Metabolism: Theory and Practice of Cardiometabolic MedicineFrom EverandCardiovascular Endocrinology and Metabolism: Theory and Practice of Cardiometabolic MedicineAndrew J. KrentzNo ratings yet
- NAPLEX Practice Question Workbook: 1,000+ Comprehensive Practice Questions (2023 Edition)From EverandNAPLEX Practice Question Workbook: 1,000+ Comprehensive Practice Questions (2023 Edition)Rating: 4.5 out of 5 stars4.5/5 (3)
- Aural Test BookDocument1 pageAural Test BookYohanes Sutrisno7% (14)
- ADA Standards of Medical Care in Diabetes 2013 PDFDocument56 pagesADA Standards of Medical Care in Diabetes 2013 PDFPatricio Moncayo DonosoNo ratings yet
- 804c Gastroenterology and Hepatology Clinic Exclusion Crit.Document1 page804c Gastroenterology and Hepatology Clinic Exclusion Crit.Yohanes SutrisnoNo ratings yet
- Potent Direct VasodilatorsDocument2 pagesPotent Direct VasodilatorsYohanes SutrisnoNo ratings yet
- Other DiureticsDocument4 pagesOther DiureticsYohanes SutrisnoNo ratings yet
- Hypertension in Pregnancy 2013-G LipkinDocument35 pagesHypertension in Pregnancy 2013-G LipkinYohanes SutrisnoNo ratings yet
- SALT Is Your Food Full of ItDocument4 pagesSALT Is Your Food Full of ItYohanes SutrisnoNo ratings yet
- Replacing MercuryDocument3 pagesReplacing MercuryYohanes SutrisnoNo ratings yet
- Potent Direct VasodilatorsDocument2 pagesPotent Direct VasodilatorsYohanes SutrisnoNo ratings yet
- Thiazide and Thiazide-Like DiureticsDocument3 pagesThiazide and Thiazide-Like DiureticsYohanes SutrisnoNo ratings yet
- Centrally Acting AgentsDocument2 pagesCentrally Acting AgentsYohanes SutrisnoNo ratings yet
- Direct Renin InhibitorsDocument2 pagesDirect Renin InhibitorsYohanes SutrisnoNo ratings yet
- Lesson 6Document1 pageLesson 6Yohanes SutrisnoNo ratings yet
- Angiotensin Receptor Blockers (ARBs) PDFDocument3 pagesAngiotensin Receptor Blockers (ARBs) PDFpriya singhNo ratings yet
- BHS Standard Operating Procedure For ABPMDocument3 pagesBHS Standard Operating Procedure For ABPMYohanes SutrisnoNo ratings yet
- Jazz XmasDocument13 pagesJazz XmasYohanes SutrisnoNo ratings yet
- Beta Adrenoceptor Antagonists (Beta Blockers)Document4 pagesBeta Adrenoceptor Antagonists (Beta Blockers)Yohanes SutrisnoNo ratings yet
- Alpha Adrenoceptor Antagonists (Alpha Blockers)Document2 pagesAlpha Adrenoceptor Antagonists (Alpha Blockers)محمدأميندماجNo ratings yet
- Lesson 1Document1 pageLesson 1Yohanes SutrisnoNo ratings yet
- Lesson 8Document1 pageLesson 8Yohanes SutrisnoNo ratings yet
- Lesson 5Document1 pageLesson 5Yohanes SutrisnoNo ratings yet
- Angiotensin Converting Enzyme (ACE) InhibitorsDocument4 pagesAngiotensin Converting Enzyme (ACE) InhibitorsPutri Mulia HasibuanNo ratings yet
- Lesson 4Document1 pageLesson 4Yohanes SutrisnoNo ratings yet
- Treatment LipidDocument6 pagesTreatment LipidYohanes SutrisnoNo ratings yet
- Lesson 3Document1 pageLesson 3Yohanes SutrisnoNo ratings yet
- What Is A Migraine With AuraDocument2 pagesWhat Is A Migraine With AuraYohanes SutrisnoNo ratings yet
- Lesson 2Document1 pageLesson 2Yohanes SutrisnoNo ratings yet
- Root of Samsung Galaxy Tab 10Document5 pagesRoot of Samsung Galaxy Tab 10Yohanes SutrisnoNo ratings yet
- ADA Standards of Medical Care in Diabetes 2013 PDFDocument56 pagesADA Standards of Medical Care in Diabetes 2013 PDFPatricio Moncayo DonosoNo ratings yet
- Top 10 prescribed drugs dental interactionsDocument14 pagesTop 10 prescribed drugs dental interactionsAnubhuti SabhlokNo ratings yet
- Pharmacology - Cardiovascular DrugsDocument113 pagesPharmacology - Cardiovascular DrugsBenjamin Joel BreboneriaNo ratings yet
- Problems in Oxygenation HPNDocument13 pagesProblems in Oxygenation HPNRoshin TejeroNo ratings yet
- Affordable medicines price listDocument172 pagesAffordable medicines price listMolka BellasfarNo ratings yet
- 11. 201909 抗高血压 antihypertensionDocument72 pages11. 201909 抗高血压 antihypertensionShanon LimNo ratings yet
- Lista preturi medicamenteDocument936 pagesLista preturi medicamenteCristina Elena NicuNo ratings yet
- Amdocal Final PDFDocument5 pagesAmdocal Final PDFSaifur Rahman SuzonNo ratings yet
- Case Presentation of Bipolar Affective Disorder, Current Episode, Manic With Psychotic DisorderDocument37 pagesCase Presentation of Bipolar Affective Disorder, Current Episode, Manic With Psychotic DisorderEarl John Natividad89% (9)
- Tutorial Report 1 Pharmacology and Therapy: Lecturer: Nurmawati Fatimah DR., M.SiDocument34 pagesTutorial Report 1 Pharmacology and Therapy: Lecturer: Nurmawati Fatimah DR., M.SiGitaaNo ratings yet
- Drugs 3Document43 pagesDrugs 3IonuțHerpeșNo ratings yet
- Amlodipine - Drug StudyDocument2 pagesAmlodipine - Drug StudyAcads useNo ratings yet
- Drug StudyDocument21 pagesDrug StudyRemedios Bandong100% (1)
- Pathophysiology Raynauds Phenomenon Schematic DiagramDocument6 pagesPathophysiology Raynauds Phenomenon Schematic DiagramEerie Era0% (1)
- MecamylanimeDocument15 pagesMecamylanimeNoor HaiderNo ratings yet
- Amlodipine CPDocument2 pagesAmlodipine CPRose EchevarriaNo ratings yet
- Amniodarone (Norvasc) Drug SummDocument1 pageAmniodarone (Norvasc) Drug SummWarrenNo ratings yet
- AHA Hypertension Guidelines 2017Document22 pagesAHA Hypertension Guidelines 2017Anonymous elSqPhzKNo ratings yet
- DIURETICS AND UPPER RESPIRATORY DRUGSDocument40 pagesDIURETICS AND UPPER RESPIRATORY DRUGSNiña Jean Tormis AldabaNo ratings yet
- Amlodipine-10mg TabletDocument7 pagesAmlodipine-10mg TabletMd. Abdur RahmanNo ratings yet
- Empr Prescriber's EditionDocument420 pagesEmpr Prescriber's EditionPatel Pratyk100% (1)
- Classifications of Pharmaceutical DrugsDocument31 pagesClassifications of Pharmaceutical DrugsDeepankar Srigyan100% (30)
- Scholarship ExamDocument16 pagesScholarship ExamRicky Vanguardia IIINo ratings yet
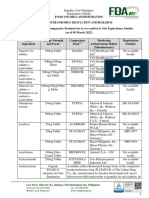
- Food and Drug Administration Center For Drug Regulation and R Food and Drug Administration Center For Drug Regulation and Research EsearchDocument141 pagesFood and Drug Administration Center For Drug Regulation and R Food and Drug Administration Center For Drug Regulation and Research EsearchJha JhaNo ratings yet
- Lercanidipine Drug StudyDocument16 pagesLercanidipine Drug StudylenecarglbnNo ratings yet
- Rovers - CH - 3 - Patient DataDocument27 pagesRovers - CH - 3 - Patient DataKhalid Bin AliNo ratings yet
- Cardiovascular Agents ReviewerDocument18 pagesCardiovascular Agents ReviewerJoycel CeñidozaNo ratings yet
- Case Study-Congestive Heart FailureDocument71 pagesCase Study-Congestive Heart FailureKentTangcalagan92% (13)
- Diabetes Treatment Plan for 78-Year-Old WomanDocument4 pagesDiabetes Treatment Plan for 78-Year-Old WomanShazaan NadeemNo ratings yet
- Drug Study - AmlodipineDocument1 pageDrug Study - AmlodipineDhanNie Cenita100% (6)
- HTN Topic DiscussionDocument7 pagesHTN Topic Discussionapi-668844754No ratings yet