You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Medicare Guide United HealthcareDocument64 pagesMedicare Guide United HealthcarescottgurveyNo ratings yet
- Environment Protection Act in Relation To Health LawDocument25 pagesEnvironment Protection Act in Relation To Health LawNandini TarwayNo ratings yet
- Avandia - The Intimidation of Dr. John BuseDocument12 pagesAvandia - The Intimidation of Dr. John BuseVaccineInformation100% (1)
- Stewarship in Mental HealthDocument18 pagesStewarship in Mental HealthRon Joshua ImperialNo ratings yet
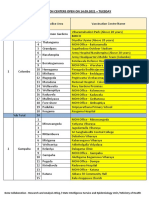
- Vaccination Centers On 14.09.2021Document8 pagesVaccination Centers On 14.09.2021Chanu On CTNo ratings yet
- ZULKIFLI - Premier SkillsDocument7 pagesZULKIFLI - Premier SkillsPuan PermaisuriNo ratings yet
- Glossary: Agency - Certified Home Health Care Agencies. Certified Home Health AgenciesDocument8 pagesGlossary: Agency - Certified Home Health Care Agencies. Certified Home Health AgenciesLinda RodriguezNo ratings yet
- Environmental HealthDocument22 pagesEnvironmental Healthhjl35057No ratings yet
- Observership ApplicationDocument5 pagesObservership ApplicationPratiksha KapartiwarNo ratings yet
- FOrensic Case Digest ExampleDocument2 pagesFOrensic Case Digest ExampleJoseph OcampoNo ratings yet
- The Philippine Nursing Act of 2002Document7 pagesThe Philippine Nursing Act of 2002sabduraupNo ratings yet
- Grant of Drug and Cosmetic Manufacturing Licence in OwnDocument4 pagesGrant of Drug and Cosmetic Manufacturing Licence in Owngo2pakadeNo ratings yet
- Application FormAFMSD DELHIDocument3 pagesApplication FormAFMSD DELHIAbhay SharmaNo ratings yet
- NEW: Customize Your Professional Certificate To Your HR Career GoalsDocument2 pagesNEW: Customize Your Professional Certificate To Your HR Career GoalsAriane VergaraNo ratings yet
- Timetable For wwc2 FinalDocument2 pagesTimetable For wwc2 Finalapi-240430967No ratings yet
- List of Products (Pigeon, India)Document17 pagesList of Products (Pigeon, India)hemantNo ratings yet
- Clinton Foundation MOUDocument5 pagesClinton Foundation MOUZerohedge100% (1)
- Eiu Democracy Index 2021Document85 pagesEiu Democracy Index 2021pberegoiNo ratings yet
- CA - Nov'21 (Date Wise)Document970 pagesCA - Nov'21 (Date Wise)MEHAK MALIKNo ratings yet
- The Tendering ProcessDocument18 pagesThe Tendering ProcessMohamed IrfanfmNo ratings yet
- Collapse of The NATM Tunnels at Heathrow AirportDocument3 pagesCollapse of The NATM Tunnels at Heathrow AirportOana Mihaela BanuNo ratings yet
- Tele MedicineDocument12 pagesTele MedicineNoorul Faedzah RosliNo ratings yet
- Abbott Laboratories Pakistan LimitedDocument2 pagesAbbott Laboratories Pakistan LimitedDanyalNo ratings yet
- 2Document43 pages2guluNo ratings yet
- Teva AR 2017 - PharmaceuticalIndustriesLtdDocument805 pagesTeva AR 2017 - PharmaceuticalIndustriesLtdBhushanNo ratings yet
- Historical Development of Social Work in UKDocument58 pagesHistorical Development of Social Work in UKIsrael James PacificoNo ratings yet
- Ra 9710 Magna Carta Women Irr 0Document131 pagesRa 9710 Magna Carta Women Irr 0ritchiemanaNo ratings yet
- Warehouse Startup ChecklistDocument3 pagesWarehouse Startup Checklistasgbalaji67% (3)
- Otda Foil Request 2Document4 pagesOtda Foil Request 2sammyschwartz08No ratings yet
- As 4457.1-2007 - Part I - Wheel and RimsDocument7 pagesAs 4457.1-2007 - Part I - Wheel and RimsjorgegachaNo ratings yet