You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Dwell Prefab Sourcebook Summer 2013Document172 pagesDwell Prefab Sourcebook Summer 2013Sara Loureiro da Luz100% (4)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- A Guide For International Post UsersDocument16 pagesA Guide For International Post UsersSara Loureiro da LuzNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Dental X-Ray ExamsDocument2 pagesDental X-Ray ExamsSara Loureiro da LuzNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Zinc Oxide Eugenol2012Document18 pagesZinc Oxide Eugenol2012Sara Loureiro da LuzNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Bioactive Glass-Published ArticleDocument4 pagesBioactive Glass-Published ArticleSara Loureiro da LuzNo ratings yet
- National Rail Operators MapDocument1 pageNational Rail Operators MapSara Loureiro da LuzNo ratings yet
- ExciTE F - ExciTE F DSCDocument6 pagesExciTE F - ExciTE F DSCSara Loureiro da LuzNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Maintaining StandardsDocument90 pagesMaintaining StandardsSara Loureiro da LuzNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
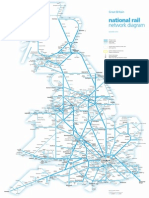
- National Rail Network Diagram: Great BritainDocument1 pageNational Rail Network Diagram: Great BritainSara Loureiro da LuzNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- London Rail Tube MapDocument1 pageLondon Rail Tube MapSara Loureiro da LuzNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Patient ConsentDocument8 pagesPatient ConsentSara Loureiro da LuzNo ratings yet
- Cold Testing Through Full-Coverage RestorationsDocument6 pagesCold Testing Through Full-Coverage RestorationsSara Loureiro da LuzNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Dental Pulp Testing - A ReviewDocument12 pagesDental Pulp Testing - A ReviewSara Loureiro da LuzNo ratings yet
- EP7 Final Programme WebDocument99 pagesEP7 Final Programme WebSara Loureiro da LuzNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Forensic BallisticsDocument23 pagesForensic BallisticsCristiana Jsu DandanNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- 2nd Quarter Exam All Source g12Document314 pages2nd Quarter Exam All Source g12Bobo Ka100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- January Payslip 2023.pdf - 1-2Document1 pageJanuary Payslip 2023.pdf - 1-2Arbaz KhanNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Propht William Marrion Branham Vist IndiaDocument68 pagesPropht William Marrion Branham Vist IndiaJoshuva Daniel86% (7)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Internship Report On A Study of The Masterbranding of Dove: Urmee Rahman SilveeDocument45 pagesInternship Report On A Study of The Masterbranding of Dove: Urmee Rahman SilveeVIRAL DOSHINo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Jesus Hold My Hand EbDocument2 pagesJesus Hold My Hand EbGregg100% (3)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Anglicisms in TranslationDocument63 pagesAnglicisms in TranslationZhuka GumbaridzeNo ratings yet
- Trainee'S Record Book: Technical Education and Skills Development Authority (Your Institution)Document17 pagesTrainee'S Record Book: Technical Education and Skills Development Authority (Your Institution)Ronald Dequilla PacolNo ratings yet
- GMAT Sentence Correction Practice Test 03Document5 pagesGMAT Sentence Correction Practice Test 03krishnachivukulaNo ratings yet
- Construction Agreement SimpleDocument3 pagesConstruction Agreement Simpleben_23100% (4)
- Waldorf Curriculum ChartDocument1 pageWaldorf Curriculum Chartplanetalingua2020100% (1)
- Comparing ODS RTF in Batch Using VBA and SASDocument8 pagesComparing ODS RTF in Batch Using VBA and SASseafish1976No ratings yet
- Seminars - 09-12-2022 - Vanessa AQUINO CHAVESDocument3 pagesSeminars - 09-12-2022 - Vanessa AQUINO CHAVESVanessa AquinoNo ratings yet
- 2011 06 13-DI-PER8-Acoustic Insulation Catalogue-Rev 01Document12 pages2011 06 13-DI-PER8-Acoustic Insulation Catalogue-Rev 01Tien PhamNo ratings yet
- Modul9 VPNDocument34 pagesModul9 VPNDadang AbdurochmanNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Kindergarten Report Card SampleDocument3 pagesKindergarten Report Card Sampleapi-294165063No ratings yet
- 755th RSBDocument32 pages755th RSBNancy CunninghamNo ratings yet
- Grade 10 Science - 2Document5 pagesGrade 10 Science - 2Nenia Claire Mondarte CruzNo ratings yet
- Research On Goat Nutrition and Management in Mediterranean Middle East and Adjacent Arab Countries IDocument20 pagesResearch On Goat Nutrition and Management in Mediterranean Middle East and Adjacent Arab Countries IDebraj DattaNo ratings yet
- SOLO FrameworkDocument12 pagesSOLO FrameworkMaureen Leafeiiel Salahid100% (2)
- Project CharterDocument10 pagesProject CharterAdnan AhmedNo ratings yet
- Listening Fill in The Gaps and ExercisesDocument4 pagesListening Fill in The Gaps and ExercisesAdriano CamargoNo ratings yet
- E F Eng l1 l2 Si 011Document2 pagesE F Eng l1 l2 Si 011Simona ButeNo ratings yet
- E-Governance Horizon Report 2007 PDFDocument240 pagesE-Governance Horizon Report 2007 PDFtouhedurNo ratings yet
- Chapter 14ADocument52 pagesChapter 14Arajan35No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cotton Pouches SpecificationsDocument2 pagesCotton Pouches SpecificationspunnareddytNo ratings yet
- Robot 190 & 1110 Op - ManualsDocument112 pagesRobot 190 & 1110 Op - ManualsSergeyNo ratings yet
- Ancient Egyptian TimelineDocument5 pagesAncient Egyptian TimelineMariz Miho100% (2)
- Syllabus For Final Examination, Class 9Document5 pagesSyllabus For Final Examination, Class 9shubham guptaNo ratings yet
- Tax Strategies: The Essential Guide to All Things Taxes, Learn the Secrets and Expert Tips to Understanding and Filing Your Taxes Like a ProFrom EverandTax Strategies: The Essential Guide to All Things Taxes, Learn the Secrets and Expert Tips to Understanding and Filing Your Taxes Like a ProRating: 4.5 out of 5 stars4.5/5 (43)