You might also like
- Pharmacology Test 1Document39 pagesPharmacology Test 1Niki BolinNo ratings yet
- Ventricular Contraction Larger Waves OscilloscopeDocument5 pagesVentricular Contraction Larger Waves Oscilloscopeskyhigh299100% (2)
- Pharm Assign 3Document7 pagesPharm Assign 3mjamie12345No ratings yet
- My Lecture13 - Cardiovascular PhysiologyDocument16 pagesMy Lecture13 - Cardiovascular PhysiologyVivek ChaudharyNo ratings yet
- Pharm QuestionsDocument5 pagesPharm Questionsvaroon525No ratings yet
- Lecture #3Document3 pagesLecture #3yeeticusfinchlmaoNo ratings yet
- (CVS) Heart BlockDocument4 pages(CVS) Heart Blockapi-3769252No ratings yet
- Phl211 Sns 14th Lecture SFDocument10 pagesPhl211 Sns 14th Lecture SFALNAKINo ratings yet
- Effects of Ethanol and Caffeine on Crayfish Heart RateDocument1 pageEffects of Ethanol and Caffeine on Crayfish Heart Ratebroddy1No ratings yet
- Effect of Pharmacological Intervention On Frog HeartDocument2 pagesEffect of Pharmacological Intervention On Frog HeartCourtneyNo ratings yet
- Adrenergic Agonists and ReceptorsDocument90 pagesAdrenergic Agonists and ReceptorsOMAR NASSERNo ratings yet
- SympathomimeticsDocument25 pagesSympathomimeticsMirza Shaharyar BaigNo ratings yet
- Artigo - Hellen 01Document6 pagesArtigo - Hellen 01YuchungLeeNo ratings yet
- Neonatal Blood Agente Vasopresores en NeonatosDocument18 pagesNeonatal Blood Agente Vasopresores en Neonatosmdgoodangel100% (1)
- Obat SimpatomimetikDocument42 pagesObat SimpatomimetiknatinlalaNo ratings yet
- Effects of Drugs On The Frogs HeartDocument16 pagesEffects of Drugs On The Frogs HeartGreetingwedausezzt50% (2)
- Neurophysiology of Depression and Bipolar Affective DisorderDocument17 pagesNeurophysiology of Depression and Bipolar Affective DisorderShivan A.C.No ratings yet
- Human Physiology 14th Edition Fox Solutions ManualDocument16 pagesHuman Physiology 14th Edition Fox Solutions Manualoraliemaximusp474w3100% (27)
- Human Physiology 14Th Edition Fox Solutions Manual Full Chapter PDFDocument37 pagesHuman Physiology 14Th Edition Fox Solutions Manual Full Chapter PDFletitiaestheru3hnxz100% (8)
- Renalase Deficiency in Heart Failure Model of Rats-A Potential Mechanism Underlying Circulating Norepinephrine AccumulationDocument8 pagesRenalase Deficiency in Heart Failure Model of Rats-A Potential Mechanism Underlying Circulating Norepinephrine AccumulationSushmita ChaudharyNo ratings yet
- ICC Inh Peptido Natriuretico IndianJPharmacol353139-6497827 - 180258Document7 pagesICC Inh Peptido Natriuretico IndianJPharmacol353139-6497827 - 180258erickmattosNo ratings yet
- Baroreflex Control of Cardiovascular FunctionDocument6 pagesBaroreflex Control of Cardiovascular FunctionKatia KovalenkaNo ratings yet
- Frog Heart Lab Report ResultsDocument3 pagesFrog Heart Lab Report ResultsTalia AviaNo ratings yet
- ANS ReceptorsDocument14 pagesANS ReceptorsAisha AliNo ratings yet
- Inotropes: Learning ObjectivesDocument7 pagesInotropes: Learning ObjectivesOrion JohnNo ratings yet
- Table of NeurotransmittersDocument10 pagesTable of NeurotransmittersAmanda Shabrina PutriNo ratings yet
- CB1 and CB2 Are 7-Transmembrane G Protein Coupled ReceptorsDocument5 pagesCB1 and CB2 Are 7-Transmembrane G Protein Coupled ReceptorsKohatiRajasNo ratings yet
- The Physiological Effect of Smoking: IntroDocument3 pagesThe Physiological Effect of Smoking: IntroAakef WandawiNo ratings yet
- 2 Effect of Drugs On Isolated Frog HeartDocument10 pages2 Effect of Drugs On Isolated Frog HeartVidhiNo ratings yet
- Script Case StudyDocument4 pagesScript Case StudyKore ProserpinaNo ratings yet
- Synaptic Transmission: A Concise GuideDocument17 pagesSynaptic Transmission: A Concise GuidebnmjgcNo ratings yet
- Human BIology PhysioEX Assignment 1Document2 pagesHuman BIology PhysioEX Assignment 1Peilu GanNo ratings yet
- Caffeine PharmacologyDocument8 pagesCaffeine PharmacologyRodrigo MaranhãoNo ratings yet
- Nihms 181336Document6 pagesNihms 181336Giulia AndreeaNo ratings yet
- Sympathetic Modulation by Antihypertensive DrugsDocument3 pagesSympathetic Modulation by Antihypertensive Drugsthomas albertNo ratings yet
- The Sympathetic Nervous System in Obesity Hypertension: Adrenal and Nervous System Mechanisms (S Oparil, Section Editor)Document8 pagesThe Sympathetic Nervous System in Obesity Hypertension: Adrenal and Nervous System Mechanisms (S Oparil, Section Editor)Caesar Catalin CaratasuNo ratings yet
- PCOL CHP 4-6 (Situational Analysis)Document2 pagesPCOL CHP 4-6 (Situational Analysis)Sunshine_Bacla_4275No ratings yet
- LP Cardio 1 Part 2Document50 pagesLP Cardio 1 Part 2Cristina SariNo ratings yet
- Autonomic Nervous SystemDocument8 pagesAutonomic Nervous SystemBobet Reña50% (2)
- Shimizu 2020Document9 pagesShimizu 2020Caesar Catalin CaratasuNo ratings yet
- Problem Set 3 Neuro 214 2022Document4 pagesProblem Set 3 Neuro 214 2022Zakaria ShenwariNo ratings yet
- Autonomic Nervous System PharmacologyDocument13 pagesAutonomic Nervous System PharmacologySam BotNo ratings yet
- Atrial Natriuretic PeptideDocument12 pagesAtrial Natriuretic Peptidesaad1qNo ratings yet
- Cardiovascular Pleiotropic Effects of NUPDocument18 pagesCardiovascular Pleiotropic Effects of NUPВладимир ДружининNo ratings yet
- Frog Heart Action Potential Lab 9 AssignmentDocument4 pagesFrog Heart Action Potential Lab 9 AssignmentNicky WieczorekNo ratings yet
- Epilepsy and Seizures: PathophysiologyDocument11 pagesEpilepsy and Seizures: PathophysiologyAbrizan HassanNo ratings yet
- Epinephrine Drug Interaction With Nonselective Beta Blocker in Local Anesthetic SolutionDocument2 pagesEpinephrine Drug Interaction With Nonselective Beta Blocker in Local Anesthetic SolutionabdugrafitiNo ratings yet
- Somatosensory FaalDocument1 pageSomatosensory Faalamalia khusnaNo ratings yet
- Chapter 12 Drugs and The Autonomic Nervous System PDFDocument10 pagesChapter 12 Drugs and The Autonomic Nervous System PDFMaha KhanNo ratings yet
- Lab08 Frog HeartDocument4 pagesLab08 Frog HeartAbie CaponponNo ratings yet
- Characteristics and Treatment of Hypertension in PheochromocytomaDocument17 pagesCharacteristics and Treatment of Hypertension in PheochromocytomaJunior TorresNo ratings yet
- Peer Review Process: Author: Section Editor: Deputy EditorDocument14 pagesPeer Review Process: Author: Section Editor: Deputy EditorLuis Enrique Caceres AlavrezNo ratings yet
- Adrenal Medulla HormonesDocument57 pagesAdrenal Medulla HormonesnikkitingNo ratings yet
- CHFDocument11 pagesCHFGwendolyn Talahiban LusaraNo ratings yet
- CHOLINERGIC AGONIST AND ANTAGONISTDocument4 pagesCHOLINERGIC AGONIST AND ANTAGONISTstephanienwafor18No ratings yet
- Assignment On Adrenergic ReceptorDocument13 pagesAssignment On Adrenergic ReceptoryannaingNo ratings yet
- Role of acetylcholine at the neuromuscular junctionDocument7 pagesRole of acetylcholine at the neuromuscular junctionSTelaNo ratings yet
- Questions From Exam 08.09.22Document12 pagesQuestions From Exam 08.09.22Ismo SNo ratings yet
- Cerebral blood flow increases after adrenaline due to blood-brain barrier dysfunctionDocument8 pagesCerebral blood flow increases after adrenaline due to blood-brain barrier dysfunctionSupu VeeturiNo ratings yet
- Phill Rasnick Resume 2 May 2014Document1 pagePhill Rasnick Resume 2 May 2014api-253602935No ratings yet
- Irg FinalDocument12 pagesIrg Finalapi-253602935No ratings yet
- FFR 2Document9 pagesFFR 2api-253602935No ratings yet
- The Emergence of Feathers in Theropods and The Evolution of Avian FlightDocument6 pagesThe Emergence of Feathers in Theropods and The Evolution of Avian Flightapi-253602935No ratings yet
- Bio 473 Reproductive Endocrinology Lab Compiled LabDocument10 pagesBio 473 Reproductive Endocrinology Lab Compiled Labapi-253602935No ratings yet
- Column Chromatography As A Chemical Purification Technique FinalDocument3 pagesColumn Chromatography As A Chemical Purification Technique Finalapi-253602935No ratings yet
- Clayton & Willihnganz: Basic Pharmacology For Nurses, 17th EditionDocument4 pagesClayton & Willihnganz: Basic Pharmacology For Nurses, 17th EditionabsianoNo ratings yet
- Overcoming Emotional Eating: Practical Methods To Gain ControlDocument40 pagesOvercoming Emotional Eating: Practical Methods To Gain ControlElena Vlasceanu100% (1)
- ScenarDocument41 pagesScenarwizard1111iam100% (7)
- Adrenoceptor Antagonists Classification & Clinical UsesDocument23 pagesAdrenoceptor Antagonists Classification & Clinical UsesMirza Shaharyar BaigNo ratings yet
- The Endocrine Pancreas: Regulation of Carbohydrate MetabolismDocument61 pagesThe Endocrine Pancreas: Regulation of Carbohydrate MetabolismFatima OngNo ratings yet
- 327-1659-1-PB YogaaDocument4 pages327-1659-1-PB YogaaikaNo ratings yet
- IELTS Official Guide For Reading - 2018Document69 pagesIELTS Official Guide For Reading - 2018Sanaullah Shar100% (1)
- AdrenalineDocument14 pagesAdrenalineOmar AyoubNo ratings yet
- Autonomic Practice Questions MEDPHARM 501/801 FALL, 2004Document16 pagesAutonomic Practice Questions MEDPHARM 501/801 FALL, 2004suresh yadavNo ratings yet
- 1102 OBJECTIVE 2 PBL 2 Cardiac Cycle .Document3 pages1102 OBJECTIVE 2 PBL 2 Cardiac Cycle .brennan12345No ratings yet
- Ch. 45 (Milan Manchandia p.5)Document3 pagesCh. 45 (Milan Manchandia p.5)Nikpreet SinghNo ratings yet
- 8 IsoproterenolDocument8 pages8 IsoproterenolSilvia RNo ratings yet
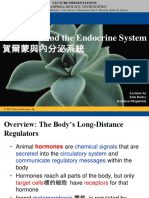
- Hormones and the Endocrine System 內分泌系統: For Campbell Biology, Ninth EditionDocument116 pagesHormones and the Endocrine System 內分泌系統: For Campbell Biology, Ninth EditionJirlyn Asoy GumilidNo ratings yet
- Adrenaline PDFDocument8 pagesAdrenaline PDFkarpanaiNo ratings yet
- Lecture 7: Chapter 4 Carbohydrates (Continued) Artificial SweetenersDocument5 pagesLecture 7: Chapter 4 Carbohydrates (Continued) Artificial SweetenersNikhil TutejaNo ratings yet
- Recommendations To Use Vasoconstrictors in Dentistry and Oral SurgeryDocument30 pagesRecommendations To Use Vasoconstrictors in Dentistry and Oral SurgeryAnonymous i7fNNiRqh2No ratings yet
- HormonesDocument25 pagesHormonesapi-309893409No ratings yet
- Chapter 2 AlkanesDocument50 pagesChapter 2 AlkanesAndreea ElenaNo ratings yet
- Key Terms and DefinitionsDocument257 pagesKey Terms and DefinitionslaurafultanoNo ratings yet
- Cathecolamine, Sympathomimetic DrugsDocument24 pagesCathecolamine, Sympathomimetic DrugsEric AryantoNo ratings yet
- Four Major Chemicals in The Brain That Influence Our HappinessDocument12 pagesFour Major Chemicals in The Brain That Influence Our HappinessHariBabuNo ratings yet
- ANS Physiology and PharmacologyDocument79 pagesANS Physiology and PharmacologyMarc Imhotep Cray, M.D.100% (1)
- Natural Muscle - April 2008Document33 pagesNatural Muscle - April 2008alfortlan100% (1)
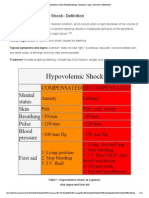
- Hypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarDocument15 pagesHypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarKaloy KamaoNo ratings yet
- 16 Metabolic DiseasesDocument34 pages16 Metabolic DiseasesLarisa RamonaNo ratings yet
- PharmacologyDocument236 pagesPharmacologyyalahopa100% (2)
- PharmacologyDocument25 pagesPharmacologygregNo ratings yet
- Emergency DrugsDocument40 pagesEmergency Drugsmattheus101No ratings yet
- The DeadDocument837 pagesThe DeadLee Keeron86% (7)
- Book Report "Why Zebra's Don't Get Ulcer's"Document7 pagesBook Report "Why Zebra's Don't Get Ulcer's"api-242679829No ratings yet