You might also like
- First InjuryDocument1 pageFirst InjuryNarayanaNo ratings yet
- First Notice of Loss PDFDocument1 pageFirst Notice of Loss PDFAnonymous cu4yJhhLRNo ratings yet
- DD 2527Document2 pagesDD 2527Paul MilesNo ratings yet
- Doctor'S First Report of Occupational Injury or IllnessDocument1 pageDoctor'S First Report of Occupational Injury or IllnessAdmin MedheroNo ratings yet
- Injury Report Instructions: Worker DetailsDocument5 pagesInjury Report Instructions: Worker DetailsAfzal ImamNo ratings yet
- Employer'S Report OF Occupational Injury or Disease: Employer Instructions and Wage Information On Reverse SideDocument2 pagesEmployer'S Report OF Occupational Injury or Disease: Employer Instructions and Wage Information On Reverse SidePete CNo ratings yet
- OCR 104A: Application For Mediation or Hearing - Form ADocument4 pagesOCR 104A: Application For Mediation or Hearing - Form AjohnNo ratings yet
- Form VBA 21-2680 AREDocument4 pagesForm VBA 21-2680 AREJane DoeNo ratings yet
- Employer'S Work Accident Illness Report: Dole/Bwc/Ohsd/Ip-6Document1 pageEmployer'S Work Accident Illness Report: Dole/Bwc/Ohsd/Ip-6ellaNo ratings yet
- BMS Virtual Claim Form Fill-In Version 0320Document1 pageBMS Virtual Claim Form Fill-In Version 0320shane ragerNo ratings yet
- Liability Claim FormDocument3 pagesLiability Claim FormJonathan StrongNo ratings yet
- Alleged Safety or Health Hazards: How Does DOSH Define A "Representative of Employees?"Document6 pagesAlleged Safety or Health Hazards: How Does DOSH Define A "Representative of Employees?"jhoniNo ratings yet
- Labor DigestsDocument20 pagesLabor DigestsKelvin ZabatNo ratings yet
- Tugas Ke 3Document4 pagesTugas Ke 3R. Brian99No ratings yet
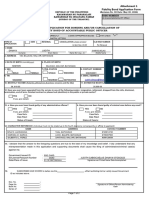
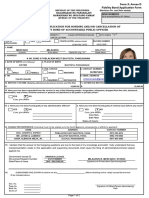
- Form 3: Annex D Fidelity Bond ApplicationDocument2 pagesForm 3: Annex D Fidelity Bond ApplicationMark Idaloy0% (1)
- Module 1 - Appendix 3BDocument9 pagesModule 1 - Appendix 3BPhanankosi DubeNo ratings yet
- Fidelity Bond Application Form FBAFDocument2 pagesFidelity Bond Application Form FBAFREYES-DEVILLA LAW OFFICENo ratings yet
- Oliver Byrd Records Only WC 092311Document5 pagesOliver Byrd Records Only WC 092311Oliver ByrdNo ratings yet
- Https WWW - Sss.gov - PH Sss Uploaded Images Forms Editable b301 Fill inDocument4 pagesHttps WWW - Sss.gov - PH Sss Uploaded Images Forms Editable b301 Fill inEricka GaganNo ratings yet
- Makati Haberdashery CaseDocument2 pagesMakati Haberdashery CaseAtheena Marie PalomariaNo ratings yet
- Electrical Permit (Front Page)Document2 pagesElectrical Permit (Front Page)Lan BalakalNo ratings yet
- Claim City of SD FinalDocument13 pagesClaim City of SD FinalRob NikolewskiNo ratings yet
- Vba 20 0996 AreDocument3 pagesVba 20 0996 AreJaster Da GreatNo ratings yet
- Accident FormDocument7 pagesAccident FormMihaela MikaNo ratings yet
- WorkCover Register of Injuries formDocument1 pageWorkCover Register of Injuries formArun MajumderNo ratings yet
- t1lt (RT: Tort ClaimsDocument3 pagest1lt (RT: Tort Claimsbarzilay123No ratings yet
- SIC - 01252 Sickness NotificationDocument3 pagesSIC - 01252 Sickness NotificationJeannylyn BurgosNo ratings yet
- Claim FormDocument5 pagesClaim FormAnchal katiyarNo ratings yet
- Petitioner Vs.. Respondents Angara, Abello, Concepcion, Regala & Cruz Dominador MaglalangDocument5 pagesPetitioner Vs.. Respondents Angara, Abello, Concepcion, Regala & Cruz Dominador MaglalangAlexandra Nicole CabaelNo ratings yet
- Liberty Mutual Avibra AME FormDocument2 pagesLiberty Mutual Avibra AME FormClorry PerryNo ratings yet
- Vba 21 4192 AreDocument2 pagesVba 21 4192 AreGene GloverNo ratings yet
- Incident Report FormDocument1 pageIncident Report FormPolycarp Danson SigaiNo ratings yet
- Editable FilesDocument5 pagesEditable FilesJholly JumadayNo ratings yet
- The National Insurance Board Funeral Grant Application NI8: (Please Use Capitals Letters)Document4 pagesThe National Insurance Board Funeral Grant Application NI8: (Please Use Capitals Letters)Allison Nadine MarchandNo ratings yet
- Fidelity Bond Application Form BT2024Document2 pagesFidelity Bond Application Form BT2024jomarNo ratings yet
- Cambridge Village ID FormDocument1 pageCambridge Village ID FormRamiro RamirezNo ratings yet
- Boiler & Pressure Plant Insurance Claim FormDocument2 pagesBoiler & Pressure Plant Insurance Claim Formhappy39No ratings yet
- Apply for AGR PositionDocument2 pagesApply for AGR PositionMike KeilNo ratings yet
- Merged 1Document24 pagesMerged 1api-317193133No ratings yet
- SF95 Equifax TortFormDocument2 pagesSF95 Equifax TortFormcamwills2100% (2)
- Vba 21 2680 AreDocument3 pagesVba 21 2680 AreAhmad Gamal Elden MAhanyNo ratings yet
- M PL E: Please Print or TypeDocument4 pagesM PL E: Please Print or TypeAnderson Jesús Romero MarchánNo ratings yet
- AEP New Application FormDocument1 pageAEP New Application Formcamille samsonNo ratings yet
- Skidmore Statement of Position With Appendices A-D and RFM Notice of AppearanceDocument21 pagesSkidmore Statement of Position With Appendices A-D and RFM Notice of AppearanceWendy LiberatoreNo ratings yet
- Dole FormDocument3 pagesDole FormAsh HamiltonNo ratings yet
- Kiten Elle 2 6 To 10Document14 pagesKiten Elle 2 6 To 10ChristineNo ratings yet
- Application For Identification Card/Deers Enrollment: Section I - Sponsor/Employee InformationDocument2 pagesApplication For Identification Card/Deers Enrollment: Section I - Sponsor/Employee InformationAlisto Darryl100% (1)
- New Revised Fidelity Bonding Application Form in ExcelDocument4 pagesNew Revised Fidelity Bonding Application Form in ExcelHad Sebuan88% (26)
- WC-1 Submitted Template - a0i53000001Du92AACDocument3 pagesWC-1 Submitted Template - a0i53000001Du92AACnga23sem33300No ratings yet
- Personal Data SheetDocument11 pagesPersonal Data SheetGeofrey Sy BajeNo ratings yet
- FIDELITY BONDING Attachment 3 Annex D TC No. 02 2019 2Document4 pagesFIDELITY BONDING Attachment 3 Annex D TC No. 02 2019 2Seven De Los ReyesNo ratings yet
- Labor Dispute Ruling on Demotion, AbandonmentDocument9 pagesLabor Dispute Ruling on Demotion, AbandonmentRamon DyNo ratings yet
- CPM Claim Form (SGI)Document2 pagesCPM Claim Form (SGI)sumitsinghNo ratings yet
- ESI Notice of Accident FormDocument3 pagesESI Notice of Accident FormOm Prakash100% (2)
- Fidelity Bond Application Form (FBAF)Document2 pagesFidelity Bond Application Form (FBAF)noeljarabata3No ratings yet
- Log of Work-Related Injuries and Illnesses: OSHA's Form 300Document3 pagesLog of Work-Related Injuries and Illnesses: OSHA's Form 300bioarquitecturaNo ratings yet
- Department of Labor and Employment: Republic of The Philippines Intramuros, ManilaDocument2 pagesDepartment of Labor and Employment: Republic of The Philippines Intramuros, ManilaLeowell John RapaconNo ratings yet
- Medical Device Complaint FormDocument2 pagesMedical Device Complaint FormJEYA KUMARANNo ratings yet
- Statcon Case 3 Tamayo V GsellDocument1 pageStatcon Case 3 Tamayo V GsellRap Macalino50% (2)
- The Telephone Answering Service Industry: Preparing for the FutureFrom EverandThe Telephone Answering Service Industry: Preparing for the FutureNo ratings yet
- Field TripsDocument4 pagesField Tripscorrina088314No ratings yet
- Unit Plan DAY 4Document4 pagesUnit Plan DAY 4corrina088314No ratings yet
- Unit Plan DAY 2Document4 pagesUnit Plan DAY 2corrina088314No ratings yet
- Unit Plan DAY 3Document4 pagesUnit Plan DAY 3corrina088314No ratings yet
- Unit Plan DAY 1Document5 pagesUnit Plan DAY 1corrina088314No ratings yet
- PlannerDocument2 pagesPlannercorrina088314No ratings yet
- Confirmation LetterDocument1 pageConfirmation LetterNirali RupareliyaNo ratings yet
- Martin Jephcote Jane SalisburyDocument7 pagesMartin Jephcote Jane SalisburyBernardita BrainNo ratings yet
- C Channel Catalogue PDFDocument109 pagesC Channel Catalogue PDFMalek al hawamdehNo ratings yet
- Non Teaching Performance Evaluation ToolDocument4 pagesNon Teaching Performance Evaluation ToolKathrynAlcantaraMagnaye100% (4)
- Employment - Body LanguageDocument4 pagesEmployment - Body LanguageIulia DobrescuNo ratings yet
- D - Lapanday V NLRC - Eve1Document2 pagesD - Lapanday V NLRC - Eve1WiMaeNo ratings yet
- Maula v. Ximex Delivery Express, Inc., G.R. No. 207838, January 25, 2017, 816 SCRA 1Document3 pagesMaula v. Ximex Delivery Express, Inc., G.R. No. 207838, January 25, 2017, 816 SCRA 1Katrina Pamela AtinNo ratings yet
- General Social Survey 2010 Worklife SectionDocument19 pagesGeneral Social Survey 2010 Worklife Section'RahmaT' ANdesjer Lcgs CuyyNo ratings yet
- Andrew Mycak v. Honeywell, Inc. and Honeywell Federal Systems, Inc., 953 F.2d 798, 2d Cir. (1992)Document8 pagesAndrew Mycak v. Honeywell, Inc. and Honeywell Federal Systems, Inc., 953 F.2d 798, 2d Cir. (1992)Scribd Government DocsNo ratings yet
- CH 13Document81 pagesCH 13Parth Goyal100% (3)
- Primus Dasotobleave FormDocument4 pagesPrimus Dasotobleave Formoldanpaulo5No ratings yet
- DTR FormDocument1 pageDTR FormkennethNo ratings yet
- Problems and prospects of technical college teachersDocument7 pagesProblems and prospects of technical college teachersমৃদুল তালহাNo ratings yet
- Notes Industrial ManagmentDocument44 pagesNotes Industrial ManagmentAftab Alam100% (1)
- General Qualifications For Appointment To Fire Officer 1 RankDocument1 pageGeneral Qualifications For Appointment To Fire Officer 1 RankMinalin FireStationNo ratings yet
- Interview AnswersDocument3 pagesInterview AnswersREACTION COPNo ratings yet
- 6 - Human Resources ManagementDocument47 pages6 - Human Resources ManagementMinh NguyệtNo ratings yet
- Activity of IbhrmDocument23 pagesActivity of IbhrmAnoop SainiNo ratings yet
- Improving relations and productivity at a struggling sawmillDocument7 pagesImproving relations and productivity at a struggling sawmilltjones51002100% (2)
- BM410 Sales Management & PracticesDocument52 pagesBM410 Sales Management & PracticesG JhaNo ratings yet
- Iktva 2021 - V2Document40 pagesIktva 2021 - V2Hassan Al EidNo ratings yet
- Untitled DocumentDocument14 pagesUntitled DocumentBrynn Enriquez IINo ratings yet
- Moya v. First Solid Rubber Industries, G.R. No. 184011Document3 pagesMoya v. First Solid Rubber Industries, G.R. No. 184011Rennah Jane YonsonNo ratings yet
- Case Study: The Vision FailedDocument2 pagesCase Study: The Vision FailedMary Gold Mosquera Espartero50% (2)
- DBA 303: Organisational Behaviour: DR Moses Otieno 0721246929 Moses - Otieno@uonbi - Ac.keDocument96 pagesDBA 303: Organisational Behaviour: DR Moses Otieno 0721246929 Moses - Otieno@uonbi - Ac.kefatma jaffarNo ratings yet
- Community Focal PointDocument6 pagesCommunity Focal PointHabibullah HekmatNo ratings yet
- PF Challan of Central Railway 107 Nos.Document1 pagePF Challan of Central Railway 107 Nos.Sukrut MayekarNo ratings yet
- MPA - Lameck John - 2015Document81 pagesMPA - Lameck John - 2015Lweli LupondoNo ratings yet
- Human Resource Management Job DescriptionDocument6 pagesHuman Resource Management Job DescriptionJam BongNo ratings yet