1518 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
were substantially attenuated, mainly due to inclusion of the
constit utional susceptibility score, but remained significant
in each car.egory for sec and in the highest. category for
melanoma. Sunlamp usage or tanning salon attendance (ever
vs never) was a risk factor for melanoma, and the association
remained significant in the multivariate models. There was no
apparent dose- response relation between the frequency of
usage and melanoma risk with multivariate ORs of 2. 06 (95%
CJ 1.1 5- 3.68) for less than 10 times and 2.05 (95% Cl
1.08- 3.90) for 10 or more times. There were non-significant
associations of sunlamp usage or tanning salon attendance with
increased risks of SCC and BCC. Cumulative sun exposure
while wearing a bathing suit remained a significant risk factor
for the three r.ypes of skin cancers in the multivariate models,
aJld the multivariate ORs were simi lar to those iJl age-adjusted
models. This variable signi fica ntly increased the goodness-of-fit
of the model for three cancer types. Among controls, women
who had higher cumulative sun exposure while wearing a
bathing suit were more likely to use a sunlamp or attend a
tanning salon (P. Chi-square, 0.03). Women in the West and
South regions were significantly more likely to be diagnosed
with SCC or BCC compared with those in Nort heast, but
residence in the West and South was not associated with
melanoma risk in both age-adj usted and multivariate models.
OveralL there was no statistically significant difference in risks
associated with these variables for each type of skin cancer in
multivariate models, according to the heterogeneity test.
Interaction between constitutional susceptibility
score and sun exposure while wearing a
bathing suit
We eval uated interactions between the consti tutional suscep-
tibility score and sun exposure while wearing a bathing suit on
skin cancer risk. We observed a significant interaction for
melanoma risk (P, interaction, 0.03) (Table 3). Compared wi th
women with the lowest consti tutional susceptibility score and
the lowest level of sun exposure while wearing a bathing suit,
those with the highest constitutional susceptibility score and
the highest level of sun exposure while wearing a bathing suit
had a significantly increased risk of melanoma (OR, 8.37; 95%
cr 3.07- 22.84) . Controls with high constitutional susceptibility
were less likely to have prolonged su n exposure while wearing
a bathing suit compared witll those with low consti tutional
susceptibill ty (P, Chi-square, 0.04) . No statisticall y significant
interactions were found for the risks of SCC (P, interaction,
0.52) and BCC (P, interaction, 0.20).
Assessment of recall bias
We had the opportunity to examine recall bias as we had
prospectively and retrospectively obtained questionnaire data
for a subset of variables (Table 4). OveralL the reliability of the
responses on natural hair colour and childhood or adolescence
tendency to ran was high. whereas the reliability of childhood
or adolescence tendency to burn assessment was lower. We
found no notable difference in the reproducibility correlations
for the three variables between cases and controls. As shown in
Table 4, the magnit ude of absol ute shift was similar among
cases and controls, except for tendency to burn among sec and
BCC cases, for which cases retrospectively reported increased
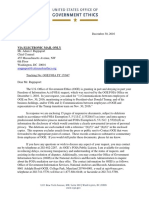
Table 3 Interaction between constituti onal susceptibility score and
sun exposure with a bathing suit on melanoma risk
Susceptibility
Sun exposure with a bathing s uit (tertile)
score (tertile)
Low Intermediate High
Low
Cases (%) 5 (20.0) 12 (48.0) 8 (32.0)
Controls (%) 62 (27.9) 70 (3 1.5) 90 (40.5)
OR (95% Cl) 1.00 1.92 0.97
(0.63- 5. 90) (0.30-3. 16)
Intermediate
Cases (%) 11 (21.2) 12 (23.1) 29 (55.8)
Controls (%) 78 (33.3) 86 (36.8) 70 (29.9)
OR (95 % C!) 1.73 1.39 4.13
(0.56- 5.32) (0.46-4.23) (1.47- J J .61)
High
Cases (%) 21 (20.4) 23 (22.3) 59 (57.3)
Controls (%) 87 (38.3) 72 (31.7) 68 (30.0)
OR (95% CI) 2 65 3.02 8.>7
(0.93-7.60) ( 1.06-8.62) (3.07-22.84)
P. interaction. 0.03.
Unconditional logistic regression adjusted for age, family his10ry of skin
cancer. rhe number of lilerime severe sunburns which blistered (none, 1- 5,
6- tl , > tt). sunlamp use or tanning salon attendance (yes/no), and geo-
graphic region. The percentages may not sum to 100 dut' to rounding.
tendency to burn to a greater extent compared with controls.
As a result, the ORs for tendency to burn based on retrospect ive
data were relatively larger than those on prospective data for
sec and BCC.
Discussion
We examined the associations of constituti onal risk factors and
sun exposure and their interactions with the risks of the three
types of skin cancer simultaneously in a nested case-comrol
st udy with in the Nurses' Hea lth Study (NHS) cohort. The risks
associated with the constitutional suscepti bility score slightly
changed but remained signi fica nt in mu ltivariate models
controlling for other exposure variables. This suggests that
the constitutional susceptibility is an independent risk factor for
all three types of skin cancer.
Sunburn at any age has been shown to be associated with an
increased risk of melanoma
14
21
22
The lifetime sunburn
variable combines exposure intensity and biological response
to sun exposure. We observed significant associations of the
number of severe sunburns with three types of skin cancer in
the age-adjusted models. The attenuation of the associations in
the multiva riate models ind icated that the skin cancer r isk
attributed to severe sunburns was partially explained by other
variables, particularly the constitutional susceptibility score.
However. even though attenuated, this association remained
significant in the multivariate models for melanoma and sec.
suggesting the number of lifetime severe sunburns may be an
independent risk factor.
The usage of indoor tanning devices was previously
associated with an increased risk of melanoma in several
studies.
23
24
Even though most of the studies, including ours,
performed retrospective assessment, it was reported recently
RISK FACTORS FOR SKIN CANCERS 1519
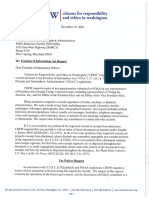
Table 4 Assessment of recall bias"
Skin tan after Skin reaction to 2
repeated s un exposure or more hours of
in childhood or s unlight in childhood
adolescence or adolescence
Natural hair colour (tendency to tan) (tendency to burn)
Kappa statistics (11) Kappa statistics (11) Kappa statistics (11)
Melanoma cases 0.84 (178) 0.61 (17 1) 0.45 ( 179)
sec cases 0.82 (244) 0.65 (238) 0.44 (243)
BCC cases 0.83 (245) 0.66 (242) 0.40 (242)
Cont rols 0.81 (682) 0.61 (668) 0.42 (679)
Mean change (SE)c Mean change (SE) Mean change (SE)
Melanoma cases 0.10 (0.03) -0.24 (0.05) 0.11 (0.07)
sec cases 0.03 (0.03) -0.1 8 (0.04) 0.21 (0.06)
BCC cases 0.09 (0.03) -0.19 (0.04) 0.26 (0.06)
Cont rols 0.04 (0.02) -0.23 (0.02) 0.09 (0.03)
Age-adjusted OR (95%Cl)d Age-adjusted OR (95%CJ) Age-adjust ed OR (95%CI)
Melanoma cases
p 2.08 (1.37-3.15) 0.55 (0. 39-0.77) 1.94 (1.38-2.71)
R 2.27 (1.53-3.35) 0.58 (0.41- 0.81) 2. 17 (1.54-3.04)
sec cases
p
1.79 (1.23-2.60) 0.61 (0.45-0.83) 1.64 ( 1.22-2.21)
R l.70 (1.18-2.44) 0.62 (0.46-0.84) 2.04 (1.51 -2.74)
BCC cases
p
1.73 (1.19-2.53) 0.68 (0.50- 0.93) ]. 55 ( 1.1 5-209)
R 1.86 ( 1.30-2.66) 0.7'5 (0.5'5-1 .00) 2.26 (1.68-3.06)
Hair colour was scored on a 5-point scale. where 1 was black and 5 was red. Tendenry to tan was scored on a 4-point scale. where 1 was practically none
and 4 was deep tan. Tendency to burn was scored on a 5-point scale. where I was practically none and 5 was painful burn with blisters.
b Kappa statistics of the responses 10 the three questions asked before and after skin cancer diagnosis in cases and in matched controls.
c Mean change was calculated as the retrospective questionnaire score minus the 1982 questionnai re score. Numbers in parentheses, standard error ol the
rnean.
d Age-adjusted OR was calculated as follows: hair colour: blonde or red vs black. dark brown. or light brown; tendency to tan: average or deep tan vs
practically none or light ta n; skin reaction: burn, painrul bum, or painful burn with blisters vs practically none or some redness only. P stands for ORs based on
the 1982 prospective data; R stands for ORs based on the 2000 retrospcctiw data.
that there was substantial reliability in reporting the usc of
sunlamps after melanoma diagnosis
2 5
A prospective study
showed that tanning device use was a significant risk factor for
melanoma with an OR for use more than once/month during
age 10-39 of 1.55 (95% CI 1.04-2.32).
21
Only a few studies
have evaluated the relationship between tanning device usc
and non-melanoma skin cancer. One population-based case-
cont rol study reported a significantly positive associat ion; the
relative risks were 2.5 (95% CI 1.7-3.8) for sec and 1.5 (95%
CI 1.1- 2.1) for BCC.
26
We simultaneously evaluated the
sunlamp use or tanning salon attendance in relation to the
three types of skin cancer. The association was strongest and
significant for melanoma compared with SCC and BCC. Most of
the previous studies only adjusted for pigmentation and
phenotype factors. In this study. after additionally controlling
for cumulative sun exposure while wearing a bathing suit,
lifetime severe sunburns. family history of skin cancer. and
geographic region. at baseli ne, the associations did not change
substantially and remained significant for melanoma risk. These
data suggest that the risks associated with sunlamp use were
not likely to be substantially confounded by sun exposure of
other kinds.
The ratio of UVB to UVA emitted by indoor tanning devices
was greatly reduced around 1980.
24
27
28
We did not differ-
ent iate age category or calendar year of the usage of indoor
tanning devices on the questionnaire. Because the age of our
study population at baseline (1976) ranged from 30 to 55, it is
possible that the majority in this study was of older
UVB-emitting devices. However, UV A has a carcinogenic effect
by causing oxidative DNA damage via reactive oxygen species
generated after the absorption of light energy by cellular
chromophores.
5
29
Additional studies are warranted to evaluate
the effect of the more contemporary UVA-emitting devices.
We used cumulati ve sun exposure whiJe wearing a bathing
suit as a measurement of recreational and intermi ttent sun
exposure; it was associated with all three types of skin cancer in
our study with the strongest risk for melanoma. The multi-
variate ORs for cumulative sun exposure while wearing
a bathing suit were not substantially confounded by other
variables.
Residence in geographic regions can be viewed as a rough
esti mation of chronic sun exposure. Vve observed that
residence in West and South regions was associated with
increased risks of sec and BCC, but not that of melanoma.
1520 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
consistent with the descriptive epidemiological evidence of a
stronger North-South gradient in the US for the risks of SCC
and BCC than that of melanoma
30
We observed a significant interaction on a mu ltiplicative
scale between the constitutional susceptibili ty score and sun
exposure while wearing a bathing suit on melanoma risk.
Women with the highest constitutional susceptibility score
and the highest level of sun exposure while wearing a bathing
suit had the highest risk for melanoma. Among controls, there
was evidence of a 'phenotype-behavior' feedback, i.e. the
controls who were more constitutionall y susceptible to sun
exposure had less sun exposure while wearing a bathing suit
compared with those who were less susceptible. In this study,
constitutional susceptibility was the combination of hair colour,
skin colour, childhood tendency to burn, and mole counts.
These identifiable phenotypic phenomena may make people
aware of their susceptibility, resulting in reduced recreat ional
sun exposure.
Few studies examined melanoma risk factors prospec-
tively3132 For retrospective studies. information on sunlight
exposure and skin cancer risk factors is potentially subject to
recall bias as it was gathered after the onset of disease. We
assessed potent ial recall bias by examining the correlations and
the difference in mean changes between the responses on the
prospective and retrospective questionnaires for the three
questions on constitutional factors and comparing odds ratios
calculated for these variables
20
The reliability of each measure
was approximately the same magnitude among the cases and
the controls and the odds ratios based on the prospective and
retrospect ive questions were similar, except for childhood
and adolescence tendency to bum, which was slightly over-
reported among sec and BCC cases retrospectively. These data
indicated tha t the retrospective assessment was not li kely to
substantiall y bias the estimate of risk in this study, at least for
these variables. Weinstock et a/.
20
examined recall bias in 143
melanoma cases with the diagnosis between June 1976 and
June 1984 in a nested case-control study conducted in 1984
and 1986 within the NHS. and the authors observed recall bias
in retrospective assessment of abili ty to tan. but not that of hair
colour. In this study, we collected the retrospective question-
nai res in 2002 among 200 melanoma cases who provided blood
samples in 1989 and 1990 and had the diagnosis between June
1990 and June 2000. We did not observe substantial recall bias
for the three variables among melanoma cases. The different
design of the two studies may help explain the discrepancy of
the results.
In summary. the nested case-control design. high follow-up
rate, and high response rate for the retrospective supplemen-
tary questiOimaire strengthen the validity of this study. The
li mitations of the study include self- reported assessment on
pigmentation phenotypes and exposures, which may lead to
misclassification. There is potential limitation in generalizability
of the results in our cohort of nurses, e.g. outdoor occupa-
tions are underrepresented. We observed sunlamp use or
tanning salon attendance remained a significant risk factor for
melanoma in multivariate models. The cumulative sun
exposure while wearing a bathing suit was an independent
risk factor from constitutional susceptibility and other exposure
variables. We observed a significant interact ion between
constitutional susceptibility and sun exposure while wearing
a bathing suit on melanoma risk, suggesting that the inter-
actions between host factors and sun exposure provide useful
itlformation for skin cancer prevention.
Acknowledgements
This work is supported by NIH CA87969 and CA 113100, and
the Harvard SPORE in Skin Cancer. We thank Gary Chase and
Nicole Williams for their help in supplementary questionnaire
admhlistration and data entry. We also thank Carolyn Guo for
her progranuning support.
References
1
Ameri can Cancer Society. Cancer Facts and Figures. Atlanta: American
cancer society, 2004.
2
Howe HL Wingo PA, Thun MJ eta/. Annual report to the nation on
the status of cancer (1973 through 1998), featuring cancers with
recent increasi ng trends. J Nat/ Cancer lrrst 2001;93:824-42.
3
AmtStrong BK, Kricker A, English DR. Sun exposure and skin cancer.
Aust J Dennato/ 1997;38:S 1-6.
4
English DR, Armstrong BK, Kricker A, Fleming C. Sunlight and
cancer. Cancer Causes Control !997;8:271-83.
5
Brash DE. Sunlight and the onset of skin cancer. Trends Genet
1997; 13:410-14.
6
Naldi L, Altieri A, lmberti GL, Gal lus S. Bosetti C. La Vecchia C. Sun
exposure, phenotypic characteristics, and cutaneous malignant
melanoma. A.n analysis according ro diUerent clinico-pathological
variants and anatomic locations (Italy). Cancer Causes Control
2005; 16:893-99.
7
Naldl L, Altieri A, Imberti GL, Giordano l, Gallus S, La Vecchia C.
Cutaneous malignant melanoma in women. Phenotypic character-
istics, sun exposure. and hormonal factors: a case-control study from
llaly. Ann Epidemic/ 2005; 15:545-50.
8
MacKie RM. Tnddence, risk fa ctors and prevention of melanoma. Eur
J Cancer 1998;34:$3- 6.
9
Osterlind A. Fair complexion and risk of malignant melanoma of the
skin based on experience from the Danish Cancer Registry. Recent
Results Cancer Res 1993; 128:91-100.
to Masback A, Westerdahl J, Ingvar C, Olsson H. Jonsson N. Cl inical
and histopathological characteristics in relation to actiological risk
factors in cutaneous melanoma: a population-bast>d study. Melanoma
Res 1999;9: 189-97.
11
Autier P, Dore JF, Gefeller 0 et a/. Melanoma risk and residence in
sunny areas. EORTC Melanoma Co-operative Group. European
Organization for Research and Treatment of Cancer. Br J Cancer
1997;76: 1521-24.
12
Dwyer T, Blizzard L, Ashbolt R, Plumb J, Berwick M, Stankovich JM.
Cutaneous melanin density of Caucasians measured by spectro
photometry and risk of malignant melanoma, basal cell carcinoma,
and squamous cell carcinoma of the ski n. Am J Eipidemio/
2002; 155:614-21.
13
Rosso S, Zanetti R. Pippione M, Sancho-Gamier H. Parallel risk
assessment of melanoma and basal cell carcinoma: skin character-
istics and sun exposure. Melanoma Res 1998;8:573- 83.
14
Elwood JM, Jopson J. Melanoma and sun exposure: an overview of
published studies. 1111 .J Cancer 1997;73: 198-203.
15
Armstrong BK. Kricker A. The epidemiology of UV induced skin
cancer. J Pltotochem Photobiol B 2001; 63:8- 18.
tt, Colditz GA. Martin P, Stampfer MJ et a/. Validation of questionnaire
info rmation on risk factors and disease outcomes in a prospective
cohort study of women. Am .l Epidemiol 1986;123:894-900.
17
NaLional Oceanic and Atmospheric Administration. Climatic Atlas of
the United States, 1983.
18
Mieninen OS. Stratification by a muhivariate confounder score. Am J
Epidemic/ 1976; 104:609- 20.
19
Marshall RJ, Ch ish olm EM. Hypothesis testing in the polychotomous
logistic model wi th an application to detecli ng gastroimesti nal
cancer. Stat Med 1985; 4:337-44.
20
Weinstock MA, Colditz GA, Willett WC, Stampfer MJ, Rosner B,
Speizer FE. Recall (report) bias a nd rel iability in th e retrospective
assessmem of melanoma risk. Am J Epidemic! 1991; 133:240-45.
2
t Veierod MB, Weiderpass E, Thorn M et a!. A prospective study of
pigmentation, sun exposure, and risk o f cutaneous malignant
melanoma in women. J Nat/ Cancer Tnst 2003;95: 1530- 38.
22
Holly EA. Aston DA, Cress RD, Ahn DK, Kristiansen .J.J. Cuta neous
melanoma in women. I. Exposure to sunlight, abilit y to ta n, and
other r isk factors related to uhraviolct light. Am J Epidemic!
1995; 141:923- 33.
23
Young AR. T.anning devices- fast track to skin cancer? Pigment Cell Res
2004; 17:2-9.
24
Gallagh er RP, Spinell i JJ, Lee TK. Ta nn ing beds. sunlamps, and risk
of cutaneous malignant melanoma. Cancer Epidemic/ Biomarkers Prev
2005; 14:562-66.
25
Beane Freeman LE. Dennis LK, Lynch CF, Lowe .JB, Clarke WR.
Test-retest of seH-reported exposure 10 a rtificial tanning devices,
RISK FACTORS FOR SKIN CANCERS 1521
self-tanning creams. and sun sensitivity showed consistency. J Clin
Epidemic/ 2005;58:430- 32.
26
r<aragas MR, Stann ard VA. Mott lA, Slattery MJ, Spencer SK,
Weinstock MA. Use of ta nn ing devices and risk of basal cell and
squamous cell skin cancers. J Nat! Ca11cer lnst 2002; 94:224-26.
27
Spencer JM, Amonette R. Tanning beds and skin cancer: artificial
sun + old sol = real risk. Clin Dermato/ 1998; 16:487- 50 I.
28
Lazovich D, Sweeney C, Weinstock MA, Berwick M. Re: a prospective
study of pigmenta tion, sun exposure. and risk of cuta neous
malignant melanoma in women. J Nat/ Cancer lmr 2004; 96:335;
author reply 7-8.
29
r<i elbassa C. Roza L, Epe B. Wavelength dependence of oxida tive
DNA damage induced by UV a nd visible light. Carcincgemsis
1997; 18:811- 16.
30
Scotto J. Fears TR. F FJ. Incidence of non-melanoma skin cancer in
t he United States. NIH Pub. No. 83-2433, 1983.
3 1
Schneide r .JS, Moore DH 2nd, Sagebiel RW. Risk factors for
melanoma incidence in prospective follow- up. The importance o f
atypical (dysplastic) nevi. Arch Dermatcl l 994; 130:1002-07.
32
Ch o E, Rosner BA, Feskanich D. Colditz. GA. Risk factors and
individual probabilities of melanoma for whites. J CTin Oncol
2005; 23:2669-75.
Annotating PDFs for eReturn
version 1.0: August 28, 2007; ful l release
1. Introduction
eProof files are self-contained PDF documents for viewing on-screen and for printing. They contain all appropriate formatting
and fonts to ensure correct rendering on-screen and when printing hardcopy. DJS sends eProofs that can be viewed, annotat-
ed, and printed using the free version of Acrobat Reader 7 (or greater). These eProofs are "enabled" with commenting rights,
therefore they can be modified by using special markup tools in Acrobat Reader that are not normally available unless using
the Standard or Professional version.
The screen images in this document were captured on a PC running Adobe Acrobat Reader version 8.1.0. Though some of the
images may differ in appearance from your platform/version, basic functionality remains similar. At the time of this writing, Ac-
robat Reader v8.1.0 is freely available and can be downloaded from: http://www.adobe.com/products/acrobat/readstep2.html
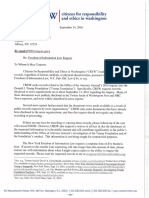
2. Comment & Markup toolbar functionality
Comment & Markup
- Sticky Note
0
,.)",Show
\.
A B c D E F G H
A. Sticky Note tool; B. Text Edits tool; C. Stamp tool; D. Highlight Text tool; E. Callout tool; F. Text Box tool ; G. Various Obj ect tools; H. Pencil tool
A. Show the Comment & Markup toolbar
The Comment & Markup tool bar doesn't appear by default. Do one of
the following:
Select View > Toolbars > Comment & Markup.
Select Tools > Comment & Markup > Show Comment
& Markup Toolbar.
Click the Review & Comment button in the Task toolbar, and choose
Show Comment & Markup Toolbar.
To add or remove tools for this too/bar, right-click the too/bar and select the tool.
Or, select Tools > Customize Too/bars.
B. Select a commenting or markup tool
Do one of the foll owing:
Select a tool from the Comment & Markup toolbar.
Select Tools > Comment & Markup > [tool].
Note: After an initial comment is made. the tool changes back to the Select tool
so that the comment can be moved, resized, or edited. (The Pencil, Highlight
Text, and Line tools stay selected.)
C. Keep a commenting tool selected
Multiple comments can be added without reselecting the tool.
Select the tool to use {but don't use it yet).
Select View > Tool bars > Properties Bar.
Select Keep Tool Selected.
More Tools [g)
0 Convnent e.: Markup Toolbat"'
0 -jii/Sh:ky Note *
< I
0 Edits
D tl! stei'Jl)Tool "'
0 .ifl HiQhfo;jht Text Tool *
0 Text Tool
0 <{] cross O<A Text Tool*
0 File as Comment
0 (' Record lwdo Conmerl *
0 E\Calout Tool*
O O cloodTool
0 )" Arcow Tool
0 / tine Tool*
0 0 Rectangle Tool "
O O ovai Tool *
0 <;' PolyQon line Tool
0 0 Polygon Tool
0 / IPeroci Tool
0 # Pendl Er&Ser Tool
0 ,.:<Show*
g !Jsend
* Only available when doC\lment ri4"lts <tre enabled.
OK j I Cancel
Choose Tools > Customize Too/bars to remove
unnecessary items from the too/bar
(see Section 7 for suggested too/bar layout)
3. The Properties bar
The Properties bar can be used to format text and select options for individual tools.
To view the Properties bar, do one of the following:
Choose View > Toolbars > Properties Bar.
Pop-Up Text Properties
Right-click the toolbar area; choose Properties Bar.
Select [Ctri-E]
T T
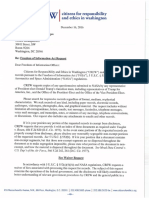
4. Using the comment and markup tools
To insert, delete, or replace text, use the Text Edits tool. Select the Text Edits tool, then select the text with the cursor (or
simply position it) and begin typing. A pop-up note will appear based upon the modification (e.g. , inserted text, replacement text,
etc.). Use the Properties bar to format text in pop-up notes. A pop-up note can be minimized by selecting theGJ button inside it.
Sticky Note t Text Edits -
~ =::: Author; klawson I More .. .
induced angiogenesis.
INTRODUCTION
Tumor-induced <mgiogenesis is the fonnation of new b
vessels from existing vasculature in response to
signals from a tumor. Angiogenesis marks
tion from benign solid tumor gro vas
a more progres:o, ivc and potent ially fatal su
beyond which cancer becomes extremely di
existing therapies become ineffecti ve and
decrease ( I). Angiogenesis is a complex
multiple time scales and intricate interplay
Cross-0312512007
ldawson Opt1c
chemical and biomechanical mechanis including cell -cell
and cell-matrix interact ions, cell tor binding,
uential mor-
Replocement Text 812512007 4 23 14 PM
ldawson Opt1ons
is des igncd to
in
understanding llllis'f
ngiogenic processes will advance
A
B
D
lopment of new therapi es for treat-
iogcnesis-dependent djseases.
~ ~ ~ ~ ~ j E
A. Attached file; B. Highlighted text; C. Crossed-out (strike-through) text; D. Inserted text; E. Replaced text
2
5. Inserting symbols or special characters
An ' insert symbol' feature is not available for annotations, and copying/pasting symbols or non-keyboard characters from Mi-
crosoft Word does not always work. Use angle brackets<> to indicate these special characters (e.g., <alpha>, <beta>).
6. Editing near watermarks and hyperlinked text
eProof documents often contain watermarks and/or hyperlinked text. Selecting characters near these items can be difficult us-
ing the mouse alone. To edit an eProof which contains text in these areas, do the following:
Without selecting the watermark or hyperlink, place the cursor near the area for editing.
Use the arrow keys to move the cursor beside the text to be edited.
Hold down the shift key while simultaneously using arrow keys to select the block of text, if necessary.
Insert, replace, or delete text, as needed.
7. Summary of main functions
Insert text- Use Text Edits tool (position cursor and begin typing)
Replace text- Use Text Edits tool (select text and begin typing)
Delete text- Use Text Edits tool (select text and press delete key)
Highlight text- Use Highlight Text tool (select text)
Attach a file- Use the Attach a File with Comment tool (select tool. position
cursor and click mouse, select fi le)
8. Reviewing changes
To review all changes, do the following:
Select the Show button on the Comment & Markup toolbar.
Select Show Comments List.
Comment & Markup
aJ Text Edits
Suggested too/bar layout
Note: Selecting a correction in the list will highlight the corresponding item in the document, and vice versa.
-t;.:::: show
~ Expand All 18 0 Next 0 PreviOUS I ~ Reply 5 ../, Sel Status - l"JJ Checkrnark I .... Show ~ Sott By ' r Search Optrons "
E3 Page I
11 '-'
I!] klawson example_resource_library.jpg
11 ...., [f!]
klawson
I! c.... [!]
klawson
IIJ L ~
klawson phases,
[!]
klawson
IJ L
~
klawson
this is a test
ll w
Use the Comments Jist to review all changes
9. The eReturn process
A. An email is received that contains a link to the eProof of the article:
http://eproofing. dartmouthjournals. com/pdfproofi ng/jou rnal1234. pdf
B. Click on the link to open the proof with the internet browser. Select "Save As" from the browser's 'File' menu to save a
copy of the PDF to the desktop or other folder.
C. Close the browser and open the saved PDF file with Acrobat.
D. Make corrections using Acrobat's Comment & Markup tools.
E. Save the PDF file, now with annotations, and return according to the instructions provided by the journal manager.
3
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
ARTICLE IN PRESS
COMMENTARY
I
Skin cancer meets vitamin D: The way forward
for dermatology and public health
Martin A. Weinstock, MD, PhD," and Arnold M. Moses, MOb
Providence, Rhode I sland, and Syracuse, New York
V
itamin D is an essential vitamin that, in recent
years, has become increasingly important to
the dermatology community because of new
evidence of its effects on health and disease and
because of the role of ultraviolet B (UVB) radiation in
its synthesis in the skin as well as in cutaneous
carcinogenesis.
1
Hence, by promoting protection of
the skin against UVB for cancer prevemion, we may
risk increasing rates or severity of other diseases.
Dermatologists should consider discussing vitamin D
with their patients when UVB exposure issues are
addressed.
Childhood rickets has been recognized for hun-
<.lreds, if not thousands, of years. Ro.man children in
the first century AD seem to have been afflicted with
rickets; it became more prevalent when people
began to dwell in crowded, smoky, and sunless
cities. In the mid-17th cemury there were multiple
publications in England on the subject of rickets.
2
In
1822, children living in \Varsaw were noted to have a
rickets more commonly than children living in the
surrounding countryside and for the first time the
idea was expressed that this disease was caused by
lack of sunshine.
3
Later in the 19th century, sun
bathing was described as being helpful in preventing
rickets. In 1921 McCollum identified a substance
found in certain fats which could prevent rickets. It
was the fourth "vitamin" identified and thus named
From the Dermatoepidemiology Unit, VA Medical Center, t he
Departments of Dermatology and Community Health, Brown
University, and the Department of Dermat ology, Rhode Island
Hospital, Providence; and the Department of Medicine, Divi
sion of Endocrinology and Metabolism, State University of New
York Upstate Medical University, Syracuse.b
Funding sources: None.
Conflicts of interest: None declared.
Reprint requests: Martin A. Weinstock, MD, PhD, Dermatoepidemiology
Unit, VA Medical Center-1 1 1D, 830 Chalkstone Ave, Providence, Rl
02908. E-mail: maw@brown.edu.
Published online .
J Am Acad Dermatol 2009;:
0190-9622/$36.00
2009 by t he American Academy of Dermatology, Inc.
doi:l o. 101 6/j.jaad.2009.04.01 6
Abbreviations used:
25(0H)D: calcidiol
1,25(0H)D: 1,25 dihyclroxyvitamin D
vitamin D. Hess and Weinstock
4
reported in 1924 that
irradiated vegetable oils could also have this etiect.
In the 1930s the chemical structure of vitamin D and
the fact that it was produced in the skin by ultraviolet
irradiation of 7-dehydrocholesterol was discovered.
Soon after, this precursor was added to milk and
some other foods that were then subjected to ultra-
violet irradiation.
Cholecalciferol (vitamin D
3
), the natural animal
vitamin D, is the form currently added to fortify foods
and is synthesized as a dietary supplement by irra-
diating 7-dehydrocholesterol extracted from lanolin
found in sheep's wool. Where animal products are
not desired, ergocalciferol (vitamin D
2
) can be made
by irradiat ing the fungal steroid ergosterol.
Ergocalciferol is approved by the Food and Drug
Administration as a pharmaceutical agent in the
United Stares, but this is not so for cholecalciferol.
There is some controversy about the relative biolog-
ical effects of ergocalciferol and cholecalciferol.
Some believe that both forms are equall y active,
5
whereas others claim that cholecalciferol has a more
favorable profile.
6
7
METABOUSM OF VITAMIN D
When obtained exogenously from food or sup-
plements, vitamin D is absorbed in the small intes-
tine. Natural food sources of vitamin D include cod,
salmon, eel, and egg yolks, but at least in the United
States, most dietary vitamin D is derived from fOJti-
fied food such as milk, orange juice, and breakfast
cereal.
8
Actually, most people in the United States
have tO resort to taking vitamin D supplements
alone, or with calcium or in a multivitamin to obtain
the recommended daily amounts. Uncommonly,
absorption from jejunum and ileum may be impaired
by diseases, such as gluten-sensitive enteropathy,
1
EDI 5.0 DTO ymjd6240 15 May 2009 5:05pm
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
ARTICLE IN PRESS
2 Weinstock and Moses
and large amounts of vitamin D are required.
Following absorption, vitamin D is transported in
the blood on a binding protein along with vitamin D
derived from the skin, to the liver where it is
QI passively 25-hydroxylated to calcidiol [25(0H)Dl.
This in turn may be stored in adipose tissue or be
transported to the kidneys and other tissues where it
is 1-hydroxylated to the active compound 1,25
dihydroxyvitamin D [1,25{0H)D]; calcitriol). This
second hydroxylation is regulated by a variety of
factors, including parathyroid hormone, phosphate,
and magnesium. Hence levels of calcitriol may not
reflect the level of calcidiol stores. Calcitriol regulates
calcium and phosphorus concentrations, which in
turn leads to proper mineralization of the skeleton to
form strong (and growing) bones and prevents
rickets in children and osteoporosis and osteomala-
cia in adults. The regulation of blood levels of
calcium and phosphorus is through directly or indi-
rectly increasing calcium and phosphorus absorp-
tion from the small intestine, decreasing urine
phosphorus excretion, and decreasing secretion of
parathyroid hormone.
CONSEQUENCES OF LOW VITAMIN D
The musculoskeletal consequences of inadequate
vitamin D have been extensively studied, although
considerable controversies remain
9
In addition to
rickets in children, and osteomalacia and osteoporo-
sis in adults (see above), falls and fractures in the
elderly are also important complications. Reduced
falls and fractures in the elderly were found in
systematic reviews of randomized trials of vitamin
D supplementationi0'
11
Other trials have failed to
confirm this finding, perhaps due in pa1t to variation
in baseline vitamin D or calcium status, or to selection
of populations studied, or other factors. Hence some
recenl systematic reviews have not found that sup-
plementation is effective for fracture reduction.
12
-
15
Among malignancies, the greatest body of evi-
dence supports a role of vitamin D in preventing
colorectal cancer,
16
although cancers of the breast
and prostate have also been prominently linked to
vitamin D.
17
However, the one large randomized trial
that has been published, which involved 36,000
women, found no difference in incidence of colo-
rectal or breasl cancer during a 7-year interven-
tion. 18 19 That trial involved supplememation with
400 IU of vitamin D plus calcium, and the 25(01-I)D
levels achieved were not reported. This trial has been
criticized because the close of vitamin supplement
and compliance may not have been sufficient to
produce a measurable effect that might have been
achieved with higher ingested doses.
J AM ACAD 0 ERMATOL
M ONTH 2009
Other malignancies have been associated with
vitamin D deficiency in observational studies, but
randomized trial evidence of a beneficial effect in
specific cancers is Jacking.
20
Ecological studies, such
as those associating malignancies with latitude of
residence, have also been published, but confound-
ing can be a major issue in these analyses, and
conflicting trends have been noted
21
One notewor-
thy randomized trial with a planned outcome of
fracture compared 1000 TU of vitamin D with 1500
mg of calcium to calcium alone and to placebo and
found a difference in the proportions of each group
that developed any cancer during the trial: 2.9%,
3.8%, and 6.9% in the calcium plus D, calcium alone,
and placebo groups, respectively.
22
The appropriate
interpretation of this finding remains unclear, partic-
ularly in the context of other studies that. have
suggested a possible role of calcium
2 3
The differ-
ences among groups were not specific with respect
to the type of cancer.
The frequency of multiple other health problems
has been shown to be inversely correlated with
vitamin D levels in some studies. These diseases
include multiple sclerosis,
24
diabetes mellitus,
25
and
infections,
26
among others. Current evidence is
insufficient. to infer a cause-and-effect relationship.
Death is not. the primary outcome in most, if not.
all, vitamin D trials published to elate. However,
mortality information is often available, particularly
since these trials are typically performed with a
substantial number of frail elderly participants. A
recently published systematic review collected 18
published randomized trials of vitamin D supple-
mentation, usually with participants who were
elderly, had low baseline vitamin D levels, or had
a history of musculoskeletal conditions consistent
with inadequate vitamin D.
27
The intervention was
usually oral ingestion of vitamin D, typically in the
400 to 880 IU range, which some view as likely to
be suboptimal. The baseline mean 25(0H)D levels
in these trials were typically less than 20 ng/ml and
increased to the 20 to 40 ng/mL range after sup-
plementation (when measured). Over 6 months to
7 years follow-up in these varied studies, no one
study found a significant difference between ran-
domized groups in mortality, but meta-analysis
revealed an overall statistically significant 7% de-
creased mortality in the vitamin D supplement
group compared to controls. We do not know the
proportion of this difference in mortality that can be
attributed to musculoskeletal, cardiovascular, neo-
plastic, or other specific causes. Although most of
these studies were of the elderly, the largest si ngle
study among them was in women 50 to 79 years of
age_zs
EDI 5.0 DTO ymjd6240 15 May 2009 5:05pm
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
ARTICLE IN PRESS
) AM ACAD DRMATOL
VOLUME NUMBER
Hence, we can conclude that vitamin D supple-
mentation appears to enhance musculoskeletal health
and reduce mortality in some groups that include a
substantial propo1tion of elderly individuals and
others at high risk of musculoskeletal problems. The
extent to which this can be applied to more general
populations with various baseline 25(0H)D levels
remains to be documented. We have evidence that
vitamin D may have an influence on cancer, cardio-
vascular disease, autoimmune disease, and infection,
but this evidence, although suggestive, is quite varia-
hie in strength and does not allow the conclusion that
any of these associations are proven.
20
These are
subjects of ongoing investigation.
OPTIMAL LEVELS OF VITAMIN D
Since 25(0H)D is the accepted marker of vitamin
D status, it is useful to estimate an optimal level.
Measures such as intestinal calcium absorption and
parathyroid hormone levels suggest that maximal
effects are attained by about 30 to 35 ng/ mL.
2930
Other outcomes, such as lower extremity function
and fractures, may be more directly relevant, and the
estimates based on these tend to be in approximately
the same range.
31
Risk of cardiovascular events in the
Framingham Offspring cohort study suggested lower
optimal levels, about 20 to 25 ng/mL.
32
The nation-
ally representative National Health and Nutrition
Examination Survey data suggested that overall
mortality was minimized at levels of about 30 to 40
ng/mL.
33
Given concerns about potential confound-
ing factors, we cannot be cettain about these esti-
mates of optimal levels, but the preponderance of
published evidence would support values of 25 to 40
ng/mL (63 to 100 nmol/L)
34
; 30 ng/ mL (75 nmol/L) is
a common estimate given current knowledge.
35
The
extent to which this estimate should va1y with age,
calcium intake, and other factors remains to be
clarified , and these estimates may be revised as
further evidence is published.
SOURCES OF VITAMIN D
ln efforts to achieve optimal vi tamin D status, the 3
sources of vitamin D must be considered. The first of
these is diet. Most dietary vitamin D intake in typical
diets is due to fortification of foods, such as mi lk and
some cereals and orange juices in the United States,
8
although this varies substantially hy country. Few
foods are naturally rich sources of this vitamin.
Photosynthesis of vitamin D in the skin requires
ultraviolet radiation in the "B" range (UVB)
36
and is
generally the largest source of vitamin D. The available
flux of UVB depends on multiple factors, including
latitude, time of day, and season of the year which
determine the angle of the sun from the horizon, and
Weinstock and Moses 3
by cloud cover and shade. Other factors that deter-
mine the ability of the skin to make vitamin D include
clothing worn, skin color, and age (there is a partic-
ularly important decline in the ability of skin ro
synthesize this vitamin with advancing age,
37
although
the elderly respond to oral supplementation
38
) . Other
factors may determine vitamin D levels as well.
39
A
series of studies has been published in a variety of
sunny, relatively equatorial locations, including
Hawaii,'
10
Santiago (Chil e),'
11
southern Arizona,
12
south Flori da,
43
and Queensland (Australia),
44
all
showing that a substantial portion of the population
has low 25(0H)D levels.
Skin cancer prevention efforts did not cause the
problem of low vitamin D levels, and abandoning
sun protection will not solve it. Dermatologists
should be aware that sun protection recommenda-
tions may impede the effectiveness of vitamin D
photosynthesis in the skin
45
and that it may be
unrealistic to presume that levels on the order of 30
ng/ mL will consistentl y be obtained from incidental
sun exposure. The vast majority of the randomized
trials that have documented the beneficial effects of
increased vitamin D have achieved that increase by
oral supplementation.
The existing Institute of Medicine guidelines rec-
ommend daily intake of 200 lU of vitamin D for
children and adults under the age of 50 years, 400 IU
for those between 50 and 70 years of age, and 600 IU
for those over the age of 70 years
46
These intake
levels may be increased in light of ongoing research. Q2
Toxicity of excess vitamin D may be manifest as
hypercalcemia or hypercalciuria; alt hough our
knowledge of the effects of high doses of vitamin
Dis limited, a recent review suggested that 10,000 IU
daily is a safe upper limit for adult intake
47
The
American Academy of Pediatrics recently increased
its recommended intake from 200 to 400 lU per clay
for all children and adolescents.
48
Some have sug-
gested that 3000 to 5000 IU daily may be required to
optimize 25(0H)D levels
4950
PREVENTION AND TREATMENT OF
HYPOVITAMINOSIS D
Although factors including obesity, bariatric sur-
gery, diabetes, skin color, dieta1y intake, dieta1y
supplements, and sun exposure may affect
25(01-I)D levels, history and physical examination
cannot reliably predict these levels.
Clinicians necessarily address low 25(0H)D levels
in individual patients. Individual levels can be
measured, and supplementation recommended.
Common recommendations include 400 or 1000 IU
daily with or without calcium or in a multivitamin;
10,000 IU weekly or eve1y 10 days; or 50,000 IU
EDI 5.0 DTO ymjd6240 15 May 2009 5:05pm
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
ARTICLE IN PRESS
4 Weinstock and Moses
monthly. Subsequent measurement of 25(0H)D
levels can be quite useful since there is great varia-
tion in the increment of 25(0H)D achieved from a
given dose of vitamin D supplement.
49
For patients with 25(0H)D levels less than
15 ng/ mL, higher doses of supplementation are
needed for a limited time to achieve the recommen-
ded levels within a reasonable period. A common,
effective, and safe method of addressing this problem
is to prescribe oral supplements of 50,000 IU vitamin
D weekl y for 8 weeks and then switch to the lower
doses mentioned above. Patients whose 25(0H)D
Q3 levels are not normalized with this approach may
have a malabsorptive syndrome and should be
referred for evaluation and alternative management.
Some have suggested that use of tanning parlors is
a recommended source of vitamin D,
51
and the
commercial indoor tanning industty has used this
for marketing purposes. However, patrons of these
facilities generally cannot determine the flux of UVB
delivered by the tanning booths and cannot deter-
mine the amount of vitamin D, if any, being gener-
ated in their skin from this exposure. It is clear,
however, that indoor tanning has been associated
with skin cancers, including squamous cell carci-
noma52 and melanoma,
53
and is a less reliable and
more expensive source of vitamin D than oral
supplementation for the general population.
For dermatologists and other clinicians whose
focus is on the patient before them, determination of
25(0H)D levels and appropriate supplementation
based on those results may be the preferred option
for managing skin cancer prevention in the context
of potentially low levels of vitamin D, panicularly
among those at high risk for future ultraviolet-
induced skin cancers, such as those whose untanned
skin color is lighter than a light to medium brown.
However, from the public health point of view,
increasing fortification of foods may be a preferable
method for management of vitamin D status that
would reach the entire population, including those
who do not have regular medical care, and fortifi ca-
tion would not require individuals to change routine
practices.
We thank Kimberly Marcolivio for her assistance.
REFERENCES
1. Lim HW, Gilchrest BA, Cooper KD, et al. Sunlight, tanning
Q4 booths, and vitamin D. J Am Acad Dermatol 2005;52:868-76.
2. O'Riordan JL. Rickets in the 17th century. J Bone Miner Res
2006;21 :1506-1 0.
3. Mozolowski W. Jedrzej Snaidecki (1768-1838) on the cure of
rickets. Nature 1939;143:121.
4. Hess AF, Weinstock M. Antirickitic imparted to inert fluids and
green vegetables by ultra-violet irradiation. J Bioi Chem 1924;
62:301-13.
J AM ACAD 0 ERMATOL
M ONTH 2009
5. Holick MF, Biancuzzo RM, Chen TC, et al. Vitamin D2 is as
effective as vitamin D3 in maintaining circulating concentra-
tions of 25-hydroxyvitamin D. J Clin Endocrinol Metab 2008;93:
677-81.
6. Trang HM, Cole DE, Rubin LA, Pierratos A, Siu S, Vieth R.
Evidence that vitamin 03 increases serum 25-hydroxyvitamin
D more efficiently t han does vitamin D2. Am J Cli n Nutr 1998;
68:854-8.
7. Armas LA, Hollis BW, Heaney RP. Vitamin D2 is much less
effective than vitamin D3 in humans. J Clin Endocrinol Metab
2004;89:5387 -91.
8. Whiting SJ, Calvo MS. Overview of the proceedings from
Experimental Biology 2005 symposium: Opt imizing Vitamin D
Intake for Populations with Special Needs: Barriers to Effective
Food Fortification and Supplementation. J Nut r 2006;136:
1114-6.
9. Wolpowitz D, Gilchrest BA. The vitamin D questions: how
much do you need and how should you get it? J Am Acad
Dermatol 2006;54:301-17.
10. Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, et al. Effect
of Vitamin D on falls: a meta-analysis. JAMA 2004;291:1999-
2006.
11. Bischoff-Ferrari HA, Willett WC, Wong JB, Giovannucci E,
Dietrich T, Dawson-Hughes B. Fracture prevention with
vitamin D supplementation: a meta-analysis of randomized
controlled trials. JAMA 2005;293:2257-64.
12. O'Donnell S, Moher D, Thomas K, Hanley DA, Cranney A.
Systematic review of the benefits and harms of calcitriol and
alfacalcidol for fractures and falls. J Bone Miner Metab 2008;26:
531-42.
13. Cranney A, Weiler HA, O'Donnell S, Puil L. Summary of
evidence-based review on vitamin D efficacy and safety in
relation to bone health. Am J Clin Nutr 2008;88:513S-9S.
14. Dawson-Hughes B. Serum 25-hydroxyvitamin D and functional
out comes in the elderly. Am J Clin Nutr 2008;88:537S-40S.
15. Bischoff-Ferrari HA, Kiel DP, Dawson-Hughes B, Orav JE, Li R,
Spiegelman D, et al. Dietary calcium and serum 25-hydrox-
yvitamin D status in relation to bone mineral density among
U.S. adults. J Bone Miner Res 2009;24:935-42.
16. Gorham ED, Garland CF, Garland FC, et al. Optimal vit amin 0
status for colorectal cancer prevention: a quantitative meta
analysis. Am J Prev Med 2007;32:210-6.
17. Garland CF, Gorham ED, Mohr SB, et al. Vitamin D and
prevention of breast cancer: pooled analysis. J Steroid
Biochem Mol Bioi 2007;103:708-11.
18. Wactawski-Wende J, Kotchen JM, Anderson GL, et al. Calcium
plus vitamin D supplementation and the risk of colorectal
cancer. N Engl J Med 2006;3S4:684-96.
19. Chlebowski RT, Johnson KC, Kooperberg C, et al. Calcium plus
vitamin D supplementation and t he risk of breast cancer.
J Natl Cancer lnst 2008;100:1581-91.
20. , International Agency for Research on Cancer. Vitami n D and
cancer Vol 5. Lyon: International Agency for Research on
Cancer; 2008.
21. Waltz P, Chodick G. Assessment of ecological regression in the
study of colon, breast , ovary, non-Hodgkin' s lymphoma, or
prostate cancer and residential UV. Eur J Cancer Prev 2008;1 7:
279-86.
22. Lappe JM, Travers-Gustafson D, Davies KM, Recker RR, Heaney
RP. Vitamin D and calcium supplementation reduces cancer
risk: results of a randomized trial. Am J Clin Nutr 2007;85:
1586-91.
23. Grau MV, Baron JA, Sandier RS, et al. Vitamin D, calcium
supplementat ion, and colorectal adenomas: results of a ran-
domized trial. J Natl Cancer lnst 2003;95:1765-71.
EDI 5-0 DTO ymjd6240 15 May 2009 5:05 pm
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
ARTICLE IN PRESS
) AM ACAD DRMATOL
VOLUME NUMBER
24. Munger KL, Levin Ll, Hollis BW, Howard NS, Ascherio A. Serum
25-hydroxyvit amin D levels and risk of multiple sclerosis.
JAMA 2006;296:2832-8.
25. Scragg R, Sowers M, Bell C. Serum 25-hydroxyvitamin D,
diabetes, and ethnicity in the Third National Health and
Nut rition Examinat ion Survey. Diabetes Care 2004;27:2813-8.
26. Cannell JJ, Viet h R, Umhau JC, et al. Epidemic influenza and
vitamin D. Epidemiol Infect 2006;134:1 129-40.
27. Autier P, Gandi ni S. Vitamin D supplementation and tot al
mortality: a met a-analysis of randomized controlled t rials. Arch
Int ern Med 2007;167: 1730-7.
28. Jackson RD, LaCroix AZ, Gass M, et al. Calcium plus vitamin D
supplementation and the risk of fractures. N Engl J Med 2006;
354:669-83.
29. Chapuy MC, Preziosi P, Maamer M, et al. Prevalence of vitamin
D insufficiency in an adult normal population. Osteoporos lnt
1997;7:439-43.
30. Heaney RP. Functional indices of vitamin D status and
ramificat ions of vitamin D deficiency. Am J Clin Nutr 2004;
80(6 Suppi):1706S-9S.
31 . Bischoff-Ferrari HA, Dietrich T, Orav EJ, et al. Higher 25-
hydroxyvitamin D concentrations are associated wit h better
lower-extremity function in both adive and inact ive persons
aged > or =60 y. Am J Clin Nutr 2004;80:752-8.
32. Wang TJ, Pencina MJ, Booth SL, et al. Vitamin D deficiency
and risk of cardiovascular disease. Circulat ion 2008;117:
503-11.
33. Melamed ML, Michos ED, Post W, Astor B. 25-Hydroxyvitamin
D levels and the risk of mortality in the general population.
Arch Intern Med 2008;168:1629-37.
34. Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T,
Dawson-Hughes B. Estimation of optimal serum concentra-
tions of 25-hydroxyvitamin D for multiple health outcomes.
Am J Clin Nutr 2006;84:18-28.
35. Vieth R, Bischoff-Ferrari H, Boucher BJ, et al. The urgent need
t o recommend an intake of vitamin D t hat is effedive. Am
J Clin Nutr 2007;85:649-50.
36. Maclaughlin JA, Anderson RR, Holick MF. Spectral charac-
t er of sunlight modulat es phot osynthesis of previtamin D3
and its photoisomers in human skin. Science 1982;216:
1001-3.
37. Holick MF, Matsuoka LV, Wortsman J. Age, vitamin D, and solar
ult raviolet. Lancet 1989;2:11 04-5.
38. Harris SS, Dawson-Hughes B. Plasma vitami n D and 250HD
responses of young and old men to supplementation with
vitamin D3. J Am Coli Nutr 2002;21 :357-62.
Weinstock and Moses 5
39. Wortsman J, Matsuoka LV, Chen TC, Lu Z, Holick MF. De-
creased bioavailability of vitami n D in obesity. Am J Clin Nut r
2000;72:690-3.
40. Binkley N, Novotny R, Krueger D, et al. Low vitamin D status
despite abundant sun exposure. J Clin Endocrinol Metab 2007;
92:213Q-5.
41. Gonzalez G, Alvarado JN, Rojas A, Navarrete C. Velasquez CG,
Arteaga E. High prevalence of vitamin D deficiency in Chilean
healthy postmenopausal women with normal sun exposure:
additional evidence for a worldwide concern. Menopause
2007;14:455-61.
42. Jacobs ET, Alberts DS, Foote JA, et al. Vitamin D insufficiency
in southern Arizona. Am J Clin Nutr 2008;87:608-1 3.
43. Levis S, Gomez A, Jimenez C, et al. Vitamin D deficiency and
seasonal variation in an adult Sout h Florida populat ion. J Clin
Endocrinol Met ab 2005;90:1557-62.
44. Kimlin M, Harrison S, Nowak M, Moore M, Brodie A, Lang C.
Does a high UV environment ensure adequate vitamin D
st atus? J Photochem Photobiol B 2007;89:139-47.
45. Mat suoka L Y, Ide L, Wortsman J, Maclaughli n JA, Holick MF.
Sunscreens ~ u p p r s s cutaneous vitamin D3 synthesis. J Clin
Endocrinol Met ab 1987;64:1 165-8.
46. Standing Committ ee on t he Scientific Evaluation of Diet ary
Reference Intakes Food and Nutrition Board. Food and
Nutrition Board. Institute of Medicine. Calcium, phosphorus,
magnesium, vitamin D and fluoride. Dietary Reference Intakes.
Washington (DC): National Academy Press; 1997. p. 250-87.
47. Hathcock JN, Shao A, Vieth R, Heaney R. Risk assessment for
vitamin D. Am J Clin Nutr 2007;85:6-18.
48. Wagner CL, Greer FR. Prevention of rickets and vitamin d
deficiency in infants, children, and adolescents. Pediat rics
2008;122:1 142-52.
49. Aloia JF, Patel M, Dimaano R, et al. Vitamin D intake to attain a
desired serum 25-hydroxyvitamin D concentration. Am J Clin
Nutr 2008;87:1952-8.
SO. Heaney RP, Davies KM, Chen TC, Holick MF, Barger-Lux MJ.
Human serum 25-hydroxycholecalciferol response to ex-
tended oral dosing with cholecalciferol. Am J Clin Nutr 2003;
77:204- 10.
51 . Holick MF. Vitamin D deficiency. N Engl J Med 2007;357:266-81.
52. Karagas MR, Stannard VA, Mott LA, Slattery MJ, Spencer SK,
Weinstock MA. Use of tanning devices and risk of basal cell and
squamous cell ski n cancers. J Nat l Cancer lnst 2002;94:224-6.
53. The association of use of sunbeds with cut aneous malignant
melanoma and other skin cancers: a systematic review. lnt
J Cancer 2007;120:11 16-22. Q5
EDI 5.0 DTO ymjd6240 15 May 2009 5:05 pm
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
540
541
542
543
544
545
546
547
548
549
550
Journal: YMJD
Article no.: 6240
Dear Author,
Author Query Form
ELSEVIER
During the preparation of your manuscript for typesetting, some questions have arisen. These are listed below. Please check your
typeset proof carefully and mark any corrections in the margin of the proof or compile them as a separate list*. This form should
then be returned with your marked proof/list of corrections to Elsevier. Please use black ink for all comments on proofs and other
documents.
Disk use
In some instances we may be unable to process the electronic file of your article and/or artwork. In that case we have, for
efficiency reasons, proceeded by usi ng the hard copy of your manuscript. If this is the case the reasons are indicated below:
r Disk damaged r Incompatible file format r LaTeX file for non-LaTeX joumal
r Virus infected r Discrepancies between electronic file and (peer-reviewed, therefore definitive) hard copy
r Other: ...... .... ........ ........ .................... ........ ........................ ........................................ ........................ ........ ....................... .
We have proceeded as follows:
r ManuSClipt scanned r Manuscript keyed in r Artwork scanned
r Files only partly used (parts processed differently: ..................... . .................... . .. .. .......................................... )
Bibliography
If discrepancies were noted between the literature list and the text references, the following may apply:
r The references listed below were noted in the text but appear to be missing from your literature list. Please complete the list or
remove the references from the text.
r Uncited references: This section comprises references that occur in the reference li st but not in the body of the text. Please
position each reference in the text or delete it. Any reference not dealt with will be retained in this section.
Queries and/or remarks
Query Details required Author's response
markers
(Ql) Note that abbreviation has been changed; thi s one appears
more frequently in the literature. OK?
(Q2) Note insertion of "intake levels"; done to clarify "These";
OK?
(Q3) Note rewording; meaning retained?
(Q4) For all references ending in "et al": please supply up to 6
authors before "eta!"; per journal style.
(Q5) Ref 53: Are there no authors for this? Please advise and
supply, if applicable.
ELSEVIER Many thanks for your assistance
*In case artwork needs revision, guidance can be found at http://authors.elsevier.com/artwork.
Page 1 of 1
I LL Docume n t De l i v e r y
REG-14714862
DCUDJG
NLM -- W1 A126 (Gen); W1 A126 (Ref ); Film S02755; E-Journal w/ILL access
US FEDERAL TRADE COMMISSION ( FTC)
US FEDERAL TRADE COMMISSION LIBRARY
600 PENNSYLVANIA AVENUE NW
WASHINGTON, DC 20580
ATTN:
PHONE : 202- 326- 2395
FAX : 202- 326- 2732
E- MAIL : library@ftc . gov
SUBMITTED:
PRINTED:
REQUEST NO. :
SENT VIA:
DOCLINE NO. :
2009-06-17 14:39:07
2009-06-18 12:35:55
REG-14714862
DOCLINE
KYB-27273266
REG Copy Journal
TITLE :
PUBLISHER/PLACE :
VOLUME/ ISSUE/PAGES :
DATE :
AUTHOR OF ARTICLE :
TITLE OF ARTICLE :
ISSN:
OTHER NUMBERS/ LETTERS :
SOURCE :
MAX COST:
COPYRIGHT COMP .:
CALL NUMBER:
NOTES:
REQUESTER INFO:
DELIVERY:
REPLY :
ARCHIVES OF INTERNAL MEDICINE
American Medical Assn. Chicago.
2009 Feb 23; 169( 4 ): 41 6-7 416-7
2009
Golomb B; Aronoff-Spencer E;Steadman M;Wu W;Yan A
A RAY OF SUNSHINE FOR THE VITAMIN D-HEART
HYPOTHES
0003-9926
Un ique ID.: 0372 44 0
KYB- 27273266
19237728
PubMed
$1 4. 00
Guidelines
W1 A126 (Gen); W1 A126 (Ref); Film S02755;
E-Journal w/ ILL access
AH
N/ A
E-mail : library@ftc.gov
Mail :
KEEP THIS RECEIPT TO RECONCILE WITH BILLING STATEMENT
For problems or questions. contact NLM a t h ttp : //wwwcf.nlm.nih.
gov/ill/ill_web_form. cfm or phone 301-496- 5511.
Include LIBID and request number.
NOTE: - THIS MATERIAL MAY BE PROTECTED BY COPYRIGHT LAW (TITLE 17, U.S. CODE)
NLM Collection Access Section . Bet hesda . MD
.I
I
I
I
'
women, respectively, but observed a similar near expo-
nential increase in hearing loss with age. In agreement with
NHANES data, hearing loss prevalence increased signifi-
cantly with age and was greater in men than in women.
Apart from hypertension, we confirm all associations be-
tween potential risk factors and any level of hearing loss
as reported by Agrawal et al.
1
Furthermore, these associa-
tions were marginally stronger (except for smoking) for
more severe levels of hearing loss. Thus, we concur with
Agrawal et al' that focusing on modifiable risks may help
to reduce the prevalence of age-related hearing loss. In con-
clusion, data from both the BMES and NHANES highlight
the burden imposed by untreated and/or underrecog-
nized hearing loss and indicate the need for possible strat-
egies to eliminate preventable hearing loss.
Bamini Gopinath, PI1D
Elena Roc1rtchina, MApplStat
Ji ejin Wang, PhD, MMed, MApplStat
Julie Sdmeider, PhD
Stephen R. Leeder, MD, PhD
Paul Mitchell, MD, PhD
Correspondence: Dr Mitchell, Centre for Vision Re-
search; University of Sydney, Westmead Hospital,
Hawkesbury Road, Westmead, New South Wales, Aus-
tralia 2145 (paul_mitchell@wmi.usyd.edu.au).
Author Contributions: Study concept and design: Gopinath,
Schneider, imd Mitchell. Acquisition of
sis and interpretation of Rochtchina, Leeder,
and Mitchell. Drafting of th'e manuscript: Gopinatl1. Criti-
cal revision of the mamucript for important intellectual con-
tent: Rochtchina, Wang, Schneider, Leeder, and Mitchell.
Statist'ical analysis: Rochtchina. Obtained funding: Mitchell.
Administrative, technical, and material support: Leeder. Study
supervision: Wang, Schneider, and Mitchell.
Financial Disclosure: None reported.
1. Agraw:tl Y, Piau EA. Nlparko JK. Prevalence of hearing loss and differences
by demographic cluractulstics among US adults: dat.t from the National Health
and Nutrition Examlrutl.on Sul'\ey, 1999-20<. Arch lnttm Mtd. 2008;168
(14):1522-1530.
2. Attebo K. Mitchell P, Smith W. Visual acuity and the a uses of \isualloss in
Australia: the Blue Mountains Study. Ophthalmology. 1996;103(3):357-
364.
3. Whitworth ) A: World Organization, International Society of H)-per-
tension Writing Group. 2003 World Health Organizat ion (WHO)/
International Society or H)-pCrtcnsion (ISH) statement on management or
hn>ertcnsion.J Hypcruns. 2003;21(ll):l983-1992.
COMMENtS AND OPINIONS
Care Quality and FraU Sublects
W
e read with interest the editorial titled "Im-
proving Care Quality and Reducing Dispari-
ties,"' and we would like to comment, add-
ing peculiar focus on "unequal treatment" given to very
old, frail subjectS.
At present, elderly persons may be considered mem-
bers of a minority population even if their numbers are
......!. '.
reaching levels much higher than other groups (eg, black,
poor, or disabled subjectS). The crucial pointS are, from
one side, clinical prejudices against old age and, from the
other side, the lack of convincing studi es transferring sci-
entific evidence to the real-world conditions of very old
subjectS, characterized by comorbidity and disability (and
very often also by a reduced cognitive function).
To overcome the gap, it could be important to pro-
duce public reports on clinical performances (starting from
the most easily demonstrable events, eg, the rate of cata-
ract removal or hip prosthesis implantation in subjectS
with dementi a), although the demonstration of out-
comes is far more difficult in elderly subjects. These re-
ports would be extremely useful for clinicians in estab-
lishing control conditions for their work and assuring a
high level of care for the most frail, elderly subjects, thus
reducing dispari ties in their access and quality of care.
Renzo Rozzini, MD
Marco Trabucd1i, MD
Corres pondence: Dr Rozzini, Department of Internal
Medicine and Geriatrics, Poliambulanza Hospital, via Ro-
manino 1, Brescia 25122, Italy (renzo.rozzini@iol.it).
1. Clancy C. lmpro,;ng care quality and reducing disparities: physici:lns' roles
Arch Inttm l\ltd. 2008; 168(11):1135-1136.
A Ray of Sunshine
for the VItamin D-Heart Hypothesis
W
e suggest that the observation by Giovan-
nucci et ai,l linki ng higher plasma 25-
hydroxyvitamin D concentrations to lower
myocardial infarction risk in men, bears fewer discrep-
ancies with existi ng literature than the authors pre-
sume. The authors note that their observational find-
ings disagr ee wi th the findings fr om the l argest
randomized trial of vitami n D, the Women's Health Ini-
tiative (WHI) study, in which the vitamin D +calcium
group exhibited no benefit-nor trend to benefit-
against myocardial infarction (hazard ratio, 1.04; 95% con-
fidence interval, 0.92-1.18).
2
We propose that this difference may arise, not pri-
marily from the relatively low vitamin D dose of 400 IU/d,
as the authors suggest, but from the inclusion of cal-
cium with vitamin D supplementation in the WHI: a re-
cent double-blind randomized controlled trial in post-
menopausal women reported an apparent increase in
myocardial infarction incidence in those randomized to
calcium .(as calcium citrate) vs placebo.
3
Moreover, in a
meta-analysis of randomized trials identifying a benefit
of vitamin D supplementation against all-cause mortal-
ity, only 2 vitamin D trials differed in the direction of effect
from the benefit found overall: both of these trials com-
bined vitamin D with calcium Thus,
the supplemental calcium in the vitamin D arm ofWHI
could be speculated to countermand its cardiac ben-
efits, rendering findings across these several studies wholly
compatible.
ARCH INTERN MED/VOL 169 (NO. 4), FEB 23, 2009
'116
Material may be protected by copyright law (Title 17, U.S. Code)
gr
th
1.
2.
3.
...
5.
I
I
I
i
l
I
. i
I
I
I
"May sunshine brighten your heart" is an Irish epi-
gram5: if a causal link is affirmed in randomized trials,
then it could become a medical prescription.
Beatrice Golomb, MD, PhD
Eli Aronoff-Spencer, MD, PltD
Midtael Steadman, MD
Winnie Wu, MS
Arthur Yan, MD
Correspondence: Dr Golomb, Department of Medicine,
University of California, San Diego, 9500 Gilman Dr, Mail
Code 0995, La jolla, CA 92093-0995 (bgolomb@ucsd
.edu).
Additional Information: At the time of the drafting of
this letter, the authors were members oflnpatient Ward
Team 3, VA San Diego Healthcare Center/UCSD School
of Medicine (June 2008).
1. Giovannucd E, Uu Y, Hollis BW, Rimm EB. 25-hydroxpi tamin D and risk
o myocardial infarction in men: a prospective study. Arch lnttrn Attd. 2008;
168(11):11741180.
2. llsia j. Heiss G. Reo II, et al. CalciumMtamin D supplementation and car
diovascular events. Circulalion. 2007;115(7):846854.
3. Bolland MJ, Barber PA, Doughty RN, etaL Vascular events In healthy older
women rccching calcium supplementation: randomised conuolled trial. BM].
2008;336(7638):262266.
4. Au tier P, Gandini S. Vitamin D supplementation and total mortality: a meta
anal)sis o randomized controlled trials. Arch InumMtd. 2007;167(16):1730-
1737.
5. Irish Culture and Customs. httpJ/www.irishcultureandcustoms.com/blessings
lbless.html. Accessed june 2008.
Hemoglobin Ate Testing,
Boarci-RecertJflcatlon Scores,-
' ancl Treatment Outcomes .
T
he publication by Holmboe et al' tilled "Asso-
ciation Between Maintenance of Certification
Examination Scores and Quality of Care for
Medicare Beneficiaries" provides a valuable insight. A
few points, however, may be added in reviewing this
matter.
The that "evidence-based processes of care"
were used in this study seems to have applied in the time
frame used, 2002 and 2003, when patient care was ex-
amined. Recent findings/
3
however, suggest an up-
dated perspective"-6 in the value of the practice exam-
ined in the study by Holmboe et al.
1
Though unknown
at the time of the study, the updated perspective in-
cludes the risk-benefit ratio of treatments that may have
resulted from extensive hemoglobin A
1
e testing. The im-
pact of effective diabetic control may have caused inad-
vertent harm despite well-intended care and stricter imple-
mentation. Even without this possibility, it supports
compliance characteristics of physicians depending on
standards of care, regardless of possible subsequent
changes in standards.
In addition, in the group examining the performance
of diabetes measures, more than 80% of patients had re-
ceived hemoglobin A
1
e tests, while other components of
the composite measure were noticeably less common. The
highest among them was lipid testing, and this was simi-
lar to the group measuring performance in cardiovascu-
lar disease, for \Vhich no difference was found \vith scores
in board recertification.
It would have been interesting to know if there were
any differences in performance for diabetic manage-
ment other than hemoglobin testing, such as the eye
examination component, in its possible correlation with
board recertification scores. Familiarity with hemoglo-
bin testing may arguably have facilitated its use more
than eye examinations, but its ease of use, when com-
pared with lipid testing, suggests a less-accepted corre-
lation between eye examination outcomes and the skills
of physicians who treat diabetes.
While Holmboe et alHP
1402
> suggest a "link between cog-
nitive skills and quality of care," it could be argued that
"skills" correlate more accurately in complying \vith stan-
dards, as far as standards can ensure quality. An impor-
tant part of physicians' cognitive skills is their ability to
assess whether the basis underlying a general standard
is sound. This may apply before changes in general stan-
dards are more widely recognized.
Simon G. Kassabian, MD
Correspondence: Dr Kassabian, Department of Medi-
cine,jewish Home Lifecare 120 W 106th St, New
York, NY 10025
1. Holmboe ES, Wang Y, Meehan TP, el at. Association between rnainterumce
or certification examination scores and quality o care for Medicare
Arch lnrern Atcd. 2008;168(13):13961403. .
2. Gerstein HC, Miller 1\t E, B)ington RP; The Action to Control Cardiovascular
Risk in Diabetes Study Group. Effects of intensi,e glucose lowering in type 2
diabetes. N Eng/} Med. 2008;358(24):25452559.
3. Patel A, MacMahon S, Chalmers]; The ADVANCE Collaborative Group.
Intensive blood glucose control and ''ascular outcomes in patients " i th type
2 diaberes. N Eng!] Med. 2008;358(24):2560-2572 .
4. Krumholz Lee Ttl. Redefining quality-implications or recent clinical
trials. N Engl} Attd. 2008;358(24):25372539.
S. Cefalu \VT. Glycemic targets and cardlo\'aSCubr disease. N Englj /lied. 2008;
358(24):2633-2635.
6. Dluhy RG, McMahon GT. Intensive glycemic control in the ACCORD and
. ADVANCE trials. N Eng/] Attd.
Is Quality of Care Only Instrume ntal?
I
read with great interest the article by Holmboe et
al' and the editorial by Landon
2
on the link be-
tween certifying examination performance and qual-
ity of care.
As these 2 articles highlight, there are substantial prac-
tical problems \"'ith collecting adequate data to demon-
strate a reliable link between paper-based cognitive as-
sessments and instrumental performance in clinical
practice. In Australia, the Bettering the Evaluation of Care
and Health (BEACH) study has shown similar links be-
tween the results of the fellowship examination and in-
strumental performance in practice.
3
However, is it sufficient to judge quality of care solely
in instrumental tenus? I would suggest that quality of
care is equally dependent on an interpersonal perfor-
mance as on doing the "right thing" in terms of disease-
specific care. \Ve should not forget that the essence of
health and health care is the personal health experience
and coping by the patient with his or her ailments-
usually multiple ailments.
4
The challenge ahead will be
ARCH INTERN MEO/VOL 169 (NO. 4), FEB 23, 2009
417
Material may be protected by copyright law (Title 17, U.S. Code)
:,
,.
,.
P E D I AT R I C S
OFFICIAL JOURNAL OF THE AMERICAN ACADEMY OF PEDIATRICS
Trends in Sunburns, Sun Protection Practices, and Attitudes Toward Sun
Exposure Protection and Tanning Among US Adolescents, 1998- 2004
Vilma Cokkinides, Martin Weinstock, Karen Glanz, Jessica Albano, Elizabeth Ward
and Michael Thun
Pediatrics 2006;118;853-864
DOl: 10.1542/peds.2005-3 109
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://www. pediatrics. org/cgil content/full/118/3/85 3
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
publication, it has been published continuously since 1948. PEDIATRICS is owned, published,
and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk
Grove Village, Illinois, 60007. Copyright 2006 by the American Academy of Pediatrics. All
rights reserved. Print ISSN: 003 1-4005. Online ISSN: 1098-4275.
American Academy of Pediatrics
DEDICATED TO THE HEALTH OF ALL CHILDREN*
Downloaded from www. pedi atrics.org by on October 21, 2009
ARTICLE
Trends in Sunburns, Sun Protection Practices, and
Attitudes Toward Sun Exposure Protection and
Tanning Among US Adolescents, 1998-2004
Vilma Cokkinides, PhD, Martin Weinstock, MD, PhDb.c, Karen Glanz, PhD, MPHd, Jessica Albano, MSPH, Elizabeth Ward, PhD,
Michael Thun, MD, MS
Department of Epidemiology and SuNeillance Research, American Cancer Society, Atlanta, Georgia; bDermatoEpidemiology Unit, VA Medteal Center Providence.
Department of Dermatology, Rhode Island Hospital, Providence. Rhode Island; <Departments of Dermatology and Community Health, Brown University, Providence,
Rhode Island; dRollins School of Public Health, Emory University, Atlanta, Georgia
The author> have indicated they have no t\nanctal relationshlpsielevant w this antcle to dtS<:Iose.
ABSTRACT ---------------------------------------------------------------------
BACKGROUND. Sun exposure in childhood is an important ri sk factor for developing
skin cancer as an adult. Despite extensive efforts to reduce sun exposure among
the young, there are no population-based data on trends in sunburns and sun
protection practices in the young. The aim of this study was to describe nationally
representative trend data on sunburns, sun protection, and attitudes related to sun
exposure among US youth.
METHODS. Cross-sectional telephone surveys of youth aged 11 to 18 years in 1998 (N
= 1196) and in 2004 (N = 1613) were conducred using a 2 -stage sampling process
to draw population- based samples. The surveys asked identical questions about
sun protection, number of sunburns experienced, and attitudes toward sun expo-
sure. Time trends were evaluated using pooled logistic regression analysis.
RESULTS. In 2004, 69% of subjects reported having been sunburned during the
summer, not significantly less than in 1998 (72%). There was a significant de-
crease in the percentage of those aged 11 to 15 years who reported sunburns and
a nonsignificant increase among the 16- to 18-year-olds. The proportion of youth
who reported regular sunscreen use increased significantl y from 31% tO 391< ..
Little change occurred in other recommended sun protection practices.
CONCLUSIONS. A small reduction in sunburn frequency and modest increases in sun
protection practices were observed among youth between 1998 and 2004, despite
widespread sun protection campaigns. Nevertheless, the decrease in sunburns
among younger teens may be cause for optimism regarding future trends. Overall,
there was rather limited progress in improving sun protection practices and
reducing sunburns among US youth between 1998 and 2004.
www.pediatrics org/cgi/doi/10. 1542/
peds.2005-3109
doi:l 0.1542/peds.2005-31 09
Other than the financial suppo11 for data
colleaion, 1he funder did not play a role in
the design and conduct of the study; data
colleaion. managemenl, analysis and
Interpretation of the data; or in the
preparation. review. or approval of the
article.
The American Cancer Sociely staff and
coinvestlgatOJs were involved in I or more
of the following: design and conduct of the
study: d<Jta colleaion management:
analysis and interpretation of the data; and
preparatiOn, I\liew, and approval of the
article.
o, Cokkinides had full access to all the data
in the study and takes responsibility for the
Integrity of the data and the accuracy of
the data analysis.The ideas and opiniom
expressed herein are those of the authors.
KeyWords
skin cancer, skin neoplasms prevention
and control. sun exposure, sun protection,
sunburn, sunscreen agents. adolescent.
epidemiology, health surveys
Abbreviations
SPF 1 5+ -sun protection factor ;;::15
Ci-confidence interval
Accepted for publication Mar 27, 2006
Address conespondence to Vilma Cokkinides.
PhD, Depanment Epidemiology and
Surveillance Research, American Glncer
Society, 1599 Clifton Rd, NE. Atlanta, GA
30329-4251. E-mail: vcokkini@Cancei.oig
PEDIATRICS OSSN Numbers: P1ir1t, 0031-4005;
Online, 11J93.4275). Copylight 2006 by the
American Academy of Pediatrics
PEDIATRICS Volume 118, Number 3, September 2006 853
Downloaded from www. pediatrics.org by on October 21 , 2009
M
ORE THAN l mi!Uon cases of basal cell or squa-
mous cell carcinoma and 62 190 cases of invasive
melanoma are expected in 2006 in the United States.' Of
these, only melanoma is included in cancer statistics
published each year by US tumor registries. Although
basal ce!J and squamous cell skin cancers (keratinocyte
carcinomas) are highly treatable, they account for con-
siderable morbidity and health care expenditures. Fur-
thermore, the incidence of both melanoma
1
-
3
and kera-
tinocyte carcinoma4-6 have been increasing.
Extensive epidemiological and biological evidence
implicates sun exposure as the principal cause of mela-
noma and keratinocyte carcinomas of the skin.
7
8
An
estimated 80% of all skin cancers are caused by UV solar
radiation.
8
Despite evidence that excessive sun exposure
in childhood contributes to the risk of skin cancers later
in life,
9
sunburns, which are markers of intense UV
exposure, remain common, especially among adoles-
cents.10-12 Several recent studies also highlight the ongo-
ing inadequacy of reported sun protection practices
among adolescentsY-
15
Most governmental and nongovernmental efforts to
prevent skin cancer in the United States have sought to
change the individual behaviors of parents and chil-
dren, ~
1 9
without a concomitant emphasis on sun pro-
tection policies, such as those used effectively in Austra-
lia.20 Furthermore, there have been no systematic efforts
to assess the effectiveness of sun protection interven-
tions in youth nationwide or to measure their changes in
attitudes toward sun protection and tanning, despite the
substantial disease burden caused by excessive sun ex-
posure. This study compared the frequency of sunburns
and attitudes and behaviors regarding sun protection in
2 nationally representative surveys of 11 - to 18-year-
olds conducted in 1998 and 2004.
METHODS
Overall Design and Study Population
The American Cancer Society conducted 2 population-
based, national cross-sectional surveys of noninstitu-
tionalized children, I I to 18 years of age, Jiving in the
continental United States. The initial Sun Survey l was
conducted from August to November L 998 and sampled
1196 boys and girls in this age range. Six years later, Sun
Survey U was conducted in August to November 2004
and sampled l 613 respondents in the same age range.
Both surveys used similar telephone-based sampling
methodology.
21
A 2-stage sampling methodology was
used to obtain a representative sample of US households
with telephones stratified by 7 US regions characterized
by levels of ultraviolet radiation.
22
At the initial contact,
an adult informant was asked if there were any children
between the ages of 11 and 18 living in the household.
Ln households with I child in this age range, he or she
was selected as the respondent. In households with > 1
854 COKKINIDES et al
eligible child, the I child with the most recent birthday
was selected. The parent or guardian having primary
caregiving responsibilities was selected as the parent re-
spondents.
Both surveys asked identical questions about sun pro-
tection behaviors, sunburn experiences, and sun protec-
tion attitudes. Trained interviewers administered the
surveys using structured telephone questionnaires. Each
interview took an average of 15 minutes to administer.
Up to 14 attempts were made to reach the eligible par-
ticipant. Initially, the interviewer spoke with the parent
or guardian to complete a parent-specific survey and
gather sociodemographic information and sun protec-
tion practices by the parent. Then the selected adolescent
completed the interview. Quality control logs were
maintained throughout the data collection period, and
data entry error rates were low (<3%). Standard re-
sponse rate formulas were used to calculate the screen-
ing, refusal, and response rates for both surveys.
23
The
screening rates were - 90% on both surveys; this indi-
cates that a high percentage of the eligible population
was successfully screened for age and household eligi-
bility. The percentage of households in which a parent
and child declined or the parent declined for both to
participate was 25% in 1998 and 27% in 2004. These
refusal rates seem high because a refusal could occur
before the screening process began or at any time during
the screening or interviewing process. The final response
rates, defined as the percentage of the (possibly) eligible
population who completed the interviews, were 58% in
1998 and 44% in 2004; the lower response rate in 2004
was affected by a larger proportion of telephone num-
bers with undetermined status (- 28%) as compared
with the proportion of telephone numbers with unde-
termined status (ie, ring, no answer) in 1998 (13%).
Participation rates in random-digit dialing surveys have
been reponed to range from 22% to 70%, with a median
of 50%. In recent years, declines in response rates in
random-digit dialing surveys have been reported.
24
Ln
this report, we focused the trend analysis only on the
youth data, whereas analysis of parent data wiU be the
subject of future reports.
Measures
Subjects were asked about their age, gender. and race,
and a series of questions related to individuals' pheno-
typic susceptibility to the sun. A validated measure of
sun sensitivity
25
was used to categorize susceptibility to
sun exposure based on 4 phenotypic characteristics: skin
reaction after 1 hour of exposure to the summer sun
(sensitivity to sunburn), skin reaction after repeated ex-
posure to the summer sun (ease of skin's tanning abil-
ity), the natural color of the skin, and the natural color
of the hair.
Subjects were asked 4 questions to determine the
average number of hours per week spent outdoors be-
Downloaded from www. pediatrics.org by on October 21, 2009
tween I 0:00 AM and 4:00 PM on weekdays during the
recent summer, the average number of hours per week
spent outdoors between I 0:00 AM and 4:00 PM on week-
ends during the recent summer, the average number of
days in the past 12 months spent. at the beach between
10:00 AM and 4:00 PM, and the number of days in the
past l2 months spent at an outdoor pool between
1.0:00 AM and 4:00 PM.
Subjects were asked whether they experienced a sun-
burn (defined as any reddening of the skin lasting 2=12
hours, received from being out in the sun) duri ng the
recent summer and, if so, the number of total sunburns
experienced during the summer. A follow-up question
asked those who experienced sunburns whether they
had taken any measures of sun protection before getting
their most serious sunburn in the sununer; response
options included: wearing protective clothing, hats, or
sunglasses; applying sunscreen; or staying in the shade.
A series of questions were used to ascertain the fre-
quency of pract.idng various recommended sun-safe be-
haviors when going outdoors on a very sunny day dur-
ing the summer for > I hour. The sun protective
practices included staying in the shade or under an
umbrella, wearing sun.glasses, wearing a wide-brimmed
hat, wearing protective clothing, such as a long-sleeved
shirt or long pants, applying sunscreen lotion, and ap-
plying a sunscreen with a sun protection factor 2=1 5 (SPF
15 +) when at the beach or pool. Response options for
these questions used a 5-point Likert scale ranging from
"always" to "never." The behavioral outcomes were di-
chotomized into regular (reported practicing the behav-
ior always or often) versus nonregular (reported prac-
ticing the behavior someti me, rarely, or never).
Subjects were asked a series of items using a 4-point
Likert scale ranging from strongly agree to strongly dis-
agree reflecting att.itudes about sun exposure and tan-
ning appeal. Attitudes toward sun protection included 4
items: "protecting my skin from the sun is an easy way
to stay healthy," "using sunscreen lotion allows me to
enjoy the outdoors with less worry," "spending time in
the sun without any protection can increase my chances
of developing cancer," and "my skin won't wrinkle as
fast if [ spend less time in the sun" (our sun protection
attitude index is a summary measure of these 4 items
and has a reliability coefficient Cronbach a = .62) . Two
other statements reflect attitudes related to outdoor sun
exposure and may be considered as separate potential
barriers against reducing sun exposure: "the sun feels
good on my skin" and "avoiding the sun takes the fun
out of being outdoors." These did not correlate with our
sun protection index and were considered separately.
The tanning preference factor reflects an underlying at-
titudina l preference for tan, and it included 2 items: "T
feel healthy when I have a nice tan" and "I look better
when l have a tan" (reliability coefficient Cronbach a =
.69).
Statistical Analysis
For both surveys, sampling weights were calculated that
take into account unequal probabilities of selection be-
cause of sample design, nonresponse, and poststratifica-
tion. Data management was conducted using SAS soft-
ware, version 9.0 (SAS Institute, Cary, NC).
26
SEs were
calculated with SLJDAAN software, version 9.0 (Re-
search Triangle Institute, Research Triangle Park, NC),
27
to account for the complex sample design; these were
applied to calculate weighted estimates to make results
representative of the noninstitutionalized population of
US youth aged 11 to l8 years old. Using the weighted
corresponding estimates and SEs in each survey year, we
present the weighted differences (change in the esti-
mates between 2004 and 1998) and 95% confidence
intervals (Cis) for the change in the estimates for the
measures of sun safe practices, sunburns, and attitudes
toward sun exposure protection and tanning. In addition
to categorical and univariate analysis of X
2
and t tests, we
also tested for the statistical significance of overall time
trends (change in the estimates between 1998 and 2004)
with pooled logistic regression analysis using dichoto-
mous outcomes, and the key predictor was time (2004 =
1 and 1998 = 0); these models also tested for significant
potential interactions between time and selected covari -
ates (age, gender, race, and sun sensitivity).
RESULTS
Table I lists the characteristics of youth aged 11 to I 8
years old across the 2 survey years weighted to the US
population of adolescents. ln both surveys, participants
were mostly white, with a mean age of 14 years, and
equally divided by gender. The phenotypic characteris-
tics relevant to sun sensitivity, and the mean sun sensi -
tivity scores were comparable across survey years. With
respect to patterns of sun exposure, there was a reduc-
tion in mean number of hours per week spent outdoors
between J 0:00 Af',, and 4:00 PM on weekdays (in 1998,
I 3.0 hours vs 12 hours in 2004; P = .03). No change was
noted in the mean number of hours per week spent
outdoors between I 0:00 AM and 4:00 PM on weekends.
Between 1998 and 2004, the number of days during the
past year spent at the beach increased significantly from
6.7 days in 1998 to 10.3 days in 2004 (P = .01). You.t.h
reported spending an average of 18 days at the pool
between 10:00 AM and 4:00 PM in both 1998 and 2004.
Time trend interactions with age, gender, and sun sen-
sitivity did not reveal any significant effect.
Sunburn Trends
In 2004, 69% of youth reported having had J or more
sunburns during the past summer compared with 72% 6
years earlier {Table 2). Among those who had experi -
enced a sunburn, an average of 2.9 sunburns was re-
ported, compared with 3. I in 1998. The time-by-age
interaction effect was significant (P < .01). Among the
PEDIATRICS Volume 118, Number 3, September 2006 855
Downloaded from www. pediatrics.org by on October 21 , 2009
00
VI
TABLE 1 Characteristics of Study Population: US Adolescents, Aged 11 to 18 Years, Sun Survey 1998 and 2004
0\
Characteristics 1998 2004 Change(2004-1998)
p
r.
0
Sample Size Weighted% (95% Cl) Sample Size Weighted % (95% Cl)
Difference (95% Cl)
"' zs
z
(n = 1192) (n = 1613)
5
m
Age V>
11-13y 503 40.3 (37. 1 to 43.5) 536 35.5 (32.9 to 38.3) - 4.8 (- 9.0 to - 06) .06
!1!.
14-15 y 289 24.6 (21.8 to 27.4) 443 27.0 (24.5 to 29.5) 2.4 ( -1.3 to 6.1)
16-18y 400 35.1 (32.0 to 38 2) 624 37.5 (34.9 to 40.3) 2.4 (-1.6 to6.4)
Mean age (95% Cl mean) 14.3 (14 1 to 14.5) 14.5 (14.3 to 146) 0.2 ( -0.8 to 12)
Gender
Boys 600 50.7 (47.5 to 539) 822 51.4 (48.6 to 54.2) 0.7 (- 35 to49) .7
Girls 592 49.3 (46. 1 to 52.5) 791 48.6 (45.8 to 51.4) -0.7 ( -4.9 to 3.5)
0
Race
0
White 1016 78.2 (75.3 to 81.1) 1390 77.4 (74.6 to 800) -0.8 ( -4.7 to 31) .S
::I
0 Other 176 218 (18.9 to 24.7) 213 22.6 (19.3 to 25.4) 0.8 (- 3.1 to47)
"' Sun sensitivity index 0.
g_
l ow 316 29 8 (26.8 to 32.8) 427 30.7 (28.1 to 33.4) 0.9(- 3.1 to4.9) .9
a
Medium 589 46.6 (43.4 to 49 8) 778 46.3 (43.6 to 49.2) -0.3 ( -4.5 to 39)
3 High 287 23.6 (20.9 to 26.3) 404 23.0 (20.8 to 25.2) - 0.6 ( - 4.1 to 2 9)
Mean sun sensitivity index 0.5 (0.50 to 0.52) 0.51 (0.48 to 0.52) 0.0 ( - 0.04 to 0.02)
Phenotypic sensitivity to sun exposure
-o Skin reaction after 1-h exposure to summer sun
(b
0.
Severe sunburn with blisters 127 11.5 (9.3 to 13.7) 148 9.5 (7 9 to 112) -2.0 (-4.7 to07) .1
Severe sunburn with peeling 353 28.8 (25.9 to 31 7) 529 32.2 (29.7 to 34.9) 3.4 ( - 0.4 to 72)
::l.
n
Mild sunburn, sorne tanning 384 310 (280 to 34.0) 484 27.2 (24.9 to 29.6) - 38 (- 7.6 toO OJ
"'
0 T uming darker, no sunburn 156 14.1 (11.7 to 16.3) 207 15.6 ( 13.5 to 17.9) 1.5 ( - 1.6 to 4.6)
.....
(JQ
No sunburn or tanning 163 14.6(12.2to 17.0) 230 15.5 (13.6 to 17.7) 0.9(-2.2to4.0)
cr
'< Skin reaction after repeated exposure to surnmer sun
0
Repeated sunburns 286 237 (20.3 to 25.9) 401 25.6 (23 1 to 26.8) 19(- 1.7to5.5) .1 ::I
0 No suntan; freckles 73 6.3 (4.710 7.9) 71 4.0 (3.0 10 4.5) -2.3 (-4.1 to -0.4)
()
0
Mild tan 291 25.3 (22.4 to 28 2) 388 262 (23.6 to 27.5) 0.9 (-2.9to4.7)
cr
Moderate tan 325 27.9 (25 0 to 30.8) 425 28.0 (25.4 to 29.3) 0.1 (-3.8 to40) (b
.....
Deep tan 202 16.9 (14.5 to 19.3) 232 162 (14.0to17.3) - 0.7 (- 3.9 to 2.5)
- Natural skin color
N
Very fair 163 14.3 (11.9 to 16.5) 206 11.8(10.2 to 13.6) -2.5 (-5.3 to 0.4) .1 0
0
'-0 Fair 633 49.0 (45.910 52.3) 882 51.8 (49.0 to 54.5) 2.8 ( -1.4 to 7.0)
Olive 146 12.0 (9.8 to 14.0) 204 12.6(10.8to 14.5) 0.6 (-2.2 to 34)
Light brown 214 21.5 (18.7 to 24.3) 254 190 (16.8 to 215) - 2.5 (- 6.1to 11)
Dark brown/black 27 32 (1.9 to 4.5) 47 4.8 (3.6 to 6.5) 1.6 ( - 0.3 to 3.5)
Sun-exposure characteristics
Number of hours per week spent outdoors on 1183 13.2 (12.5 to 13.9) 1565 12.0( 11.4 to 12.6) - 1.2 (- 2.0 to -0.3) .03
weekdays, weighted mean
Number of hours per week spent outdoors on 1172 7.3 (6.8 to 7 8) 1571 7.1 (6.7 to 7.4) -0.2 (-0.6 to 0.3) .2
weekends, weighted mean
Number of days in past 12 mo spent at the beach, 1185 6.7 (5.9 to 75) 1549 10.3 (9.2 to 11.4) 3.6(2.1 to5.1} .01
weighted mean
Number of days in pasr 12 mo spent at an outdoor 1174 182 (168to 19.6) 1533 18.3 (17.0to 195) 0. 1 (- 1.6to 18) .7
pool, weighted mean
Between the hours of 10:00 1>.'A and 4:00PM.
0
0
~
::I
0
"' 0.
g_
::('
0
3
~
~
~
-o
g_
;
~
"'
~
~
0
::I
??
0"
c;rn
~ Q
~
.. - R
N '-"'
g ~
-.oc:
3
ro
90
z
3
~
~
""
"'
-o
~
~
~
00
\11
.....
TABLE 2 Trends in the Prevalence of Sunburns and Mean Number of Sunburns Experienced During the Summer in US Youth, Sun Survey 1998 and 2004
Variable Percentage Who Experienced Sunburns During the Among Those Who Experienced Sunburns
Summer
Mean No. of Sunburns Percentage Who Reported Applying Sunscreen as a
Form of Sun Protection Before Occurrence of Most
Serious Sunburn
1998,% 2004,% Change Difference 1998, 2004, Change Difference (Mean) 1998, % 2004,% Change Difference
(95% Cl Difference) Mean Mean (95% Cl Difference) (95% Cl Difference)
Overal l 72.2 68.7 - 3.5 ( -7.5 to 0.5) 3. 10 2.90 -02(-06to02) 39.2 473 8.1" (3.1 to 130)
Age,y
11-13 75.1 67.3 - 7.8 (- 14.5 to - ll)b 2.84 2.69 - 02(- 06to0.3) 47.2 58.5 1 13 (3.0 to 19.6)
14-15 78.9 69.6 -9.3(- 17.1 to - 1.5) 3.23 3.00 -0.2 (- 1.2 toO.?) 36.5 48.0 11.5 (1.9 to 21.1)
16-18 64.3 70.0 5.7 (- 1.3 to 12.7) 3.36 2.97 - 0.4 ( - 1.3 to 0.5) 30.6 36.6 6.0(- 1.9to 13.8)
Gender
Boys 72.9 66.0 - 6.9 ( - 13.8 to 0 1) 2.96 2.90 - 0.1 (- 0.7to0.6) 30.2 38.3 8.P(1.4to 14.8)
Girls 72.0 71.5 - 0.5 (- 5.8to48) 324 2.90 - 0.3 ( - 0.9 to 0.3) 48.2 56.1 7 9 (08 to 15 0)
Race
White 79.4 76.3 -3.1 (-7.1 to0.9) 3.21 3.02 -0.2 ( -0.7 to 0.3) 40.2 45.6 5.4 (0.2 to 10.6)
Nonwhite 46.8 43.0 - 3.8 ( - 14.6 to 7.0) 2.56 2. 10 - 0.5( -2.1 to 1.2) 33.6 56.0 22.4 (6.6 to 38.2)
Sun sensitivity index
Low 55.1 52.2 - 29(- 1Uto5.5) 2.53 2.20 - 0.3 (-1 OtoOA) 29.1 49.0 19.9 (9.6 to 302)
Medium 77.0 73.4 - 3.6( - 9.0to 1.8) 3.07 2.83 - 02 (- l.OtoO.S) 40.1 44.0 39(- 3.0to 10.8)
High 85.5 84.5 -1.0(- 7.8 to 58) 3.67 3.55 - 0. 1 (- 09to0.7) 46.2 52.0 5.8 (- 3.8 to 15.4)
P< .001.
b P < .01 interaction term (age by year).
16- to 18-year-olds, sunburn prevalence increased by
6% (P > .05), whereas at younger ages, sunburn prev-
alence decreased significantly by among II- to
13-year-olds and 9% in I 4- to I 5-year-olds (P < .0 l;
Table 2). ln a multivariate analysis controlling for con-
founders (age, gender, race, and sun sensitivity), we
found a positive association between having had sun-
bums and regular use of sunscreen when going outdoors
in the summer (data not shown). Among those who
sunburned, the most common reported measure of pro-
tection before experiencing the most serious sunburn of
the summer was application of sunscreen, whereas other
measures of sun protection were very infrequent
( <2%). Compared with 1998 levels, the prevalence of
wearing sunscreen before experiencing a serious sun-
bum increased significantly (overalL from 39% to 47%;
P < .00 1; Table 2). During the 6-year period, there were
larger trends that showed increases in the percentage of
youth reporting sunscreen use before getting a serious
sunburn among those aged L L to 1. 5 years, boys, and
those with more sun-resistant skin traits and of non-
white race (Table 2).
Sun Protection Practices Trends
Between 1998 and 2004, there were signifi cant increases
in the overall prevalence of regular (always/often) use of
sunscreen (8% increase, from 31% to 39%) when going
outdoors on a sunny day for > L hour. Statistically sig-
nificant increases in the regular use of sunscreen were
observed in most subgroups examined, but these in-
creases were greatest among older youth (who reponed
the least use of sunscreens) and among girls and those
who with mectium or high sun sensitivity (who had the
highest use of sunscreen). The increase was restricted to
white youth. The percentage of respondents who re-
ported regular use of sunscreen with SPF I 5 +, when at
the beach or at the pool, did not change from J 998 to
2004. Other recommended sun-safe practices, such as
wearing sunglasses, wearing protective clothing (long-
sleeve shirts or long pants), and staying in the shade
were less conunon. The regular use of wide-brimmed
hats in this population was very infrequent (- 5% in
2004). No measurable changes in these practices were
observed between 1994 and 2004, except for an increase
in the prevalence of regular use of long-sleeve shins or
long pants among white youth (P < .05; Table 3). Sim-
ilar trends were observed when comparing regular (al-
ways or often) to always use (Table 3).
Trends in Attitudes
There was a small but statistically significant increase in
the percentage of respondents who reported positive
attitudes (strongly agree or agree) toward the benefits of
sun protection (3.51<, increase; P < .05). This change in
attitude mostly involved white youth. This change was
primaril y influenced by 2 attitudinal/beli efs about the
858 COKKINIDES et al
benefits of sun protection (ie, "protecting my skin from
the sun is an easy way to stay healthy" and "spending
time outdoors without any sunscreen increases my
chances of developing cancer"; Table 4). Attitudes re-
lated to tanni ng preferences continued to be common in
2004: 67.8% of youth strongly agree or agree with the
statement "I look better when I have a tan" and 55% of
youth strongly agree or agree with the statement "I feel
healthy when I have a nice tan," and across youth
characteristics, slight declines in trends for these single
items were observed between 1998 and 2004. As mea-
sured by an overall index of these items (tanning pref-
erence), there was a signifi cantly modest decrease in the
prevalence of positive (strongly agree or agree) attitudes
(from 56.5% to 51.4%; 5.1% decrease; P < .05; Table 4).
In 2004, the proportion of youth who reponed strongly
agreeing or agreeing with the statement "the sun feels
good on my skin" significantly increased (11.6%; P <
.001) compared with 1998 levels, and this pattern of
change was consistent across all of the subgroups (Table
4).
DISCUSSION
There have been extensive efforts by government agen-
cies, foundations, and other organizations in recent
years to promote sun protection behaviors among chil-
dren and adults in the United States for the purpose of
preventing future melanomas and other skin cancers.
1
&-
2
s
Unfortunately, there has been little systematic effort to
assess the effect of these initiatives on trends in behavior.
Particularly lacking are repeated surveys of population-
based samples with consistent methodology to allow
systematic assessment of trends. Most studies have been
cross-sectional surveys.
12
13
-
15
29
-
31
Some of these studies
have been regional in scope,
12
29
30
others were based on
nationally representative samples,
and 1 had a large
nonpopulation-based sample.
15
Despite the varied meth-
odology, these surveys have shown that adolescents
have low levels of sun protection behaviors and high
levels of sun exposure and sunburns. Although findings
of these studies have been i11formative, they do not
address the issue of how much change there has oc-
curred in US youths' sun protection and sun exposure.
Our study collected data from 2 time periods on mul-
tiple behavioral and attitudinal end points. We found
that. trends in US youth sun protection were mixed
during the interval of 1998 to 2004. The prevalence of
youth experiencing sunburns during the summer was
high and generally stable between 1998 and 2004
in 2004). However, there were significant trends
of decreasing prevalence of sunburns among younger
teens. Tt is li kely that this age -specific trend may relate in
part to greater parental influence in younger adolescents
(as well as children), because several studies indicate
that parental vigilance and parent's sun protection be-
haviors are related to greater sun protection practices
Downloaded from www. pediatrics.org by on October 21 , 2009
TABLE 3 Trends in the Prevalence of Sun-Safe Behavior Practices When Going Outdoors on a Sunny Day During the Summer for> 1 Hour in US
Youth, Sun Survey 1998 and 2004
Sun Protection Apply Sunscreen When Going Apply Sunscreen With SPF 15 + Wear Wide-Brimmed Hat
Measures Outdoors in Summer at the Beach/Pool
1998, 2004, Change, % 1998, 2004, Change,% 1998, 2004, Change, %
% % (Change, 95% Cl) % % (Change, 95% Cl) % % (Change, 95% Cl)
Total (often/always) 31.4 39.4 8.0 (4.0 to 12.0) 58.4 56.4 - 2 0 (- 6.5 to 2.5) 3.8 4.9 1.1 ( - 0.7 to 2.9)
T oral {always) 9.7 15.8 6. Jd (3.3 to 88) 32.2 29.0 - 3.2( - 7.40 10) 0.4 2.3 1.9 ( - 0.7 to 3.0)
Age,y
11-13 41.9 48.1 6.2 ( -0.7 to 13.1) 63.4 64.6 1.2 {-5.9 to 8.3) 5.0 5.0 0.0 (-3.1 to3.1)
14-15 26.5 35.5 901>(1.2to 168) 586 53.0 -56(- 14.5 to3.3) 2.0 4.9 2.9{-0.3to6.1)
16-18 22.9 330 10 1 (4.0 to 16.2) 52.0 51.1 -09(-8.6to68) 3.5 4.8 1.3 ( -1.7 to 4.3)
Gender
Boys 25.1 30.0 49{- 0.4to 10.2) 56.0 53.1 - 2.9 ( - 9.6 to 38) 3.8 6.5 2.7 (0.1to 5.3)
Girls 37.9 48.6 10.7" (4.9to 16.5) 60.6 59.8 -0.8 (-6.8 to 5.2) 3.8 3.3 -o.s (-2.9 to 1.9)
Race
White 33.5 430 9.5 (5. 1 to 13.9) 60.3 62. 1 18{-2.9to6.5) 32 4.9 1.7 ( -0.2 to 3.6)
Nonwhite 25.2 25.3 0.1 { -9.5to 9.7) 509 36.8 -14.1 (-26.3 to -1.8) 5.7 53 -0.4 (-5.5 ro4.7)
Sun sensitivity index
Low 21.0 23.6 2.6 { - 4.1 to 9.3) 50.8 42.9 - 79( -1 7.0 to 1.2) 5.1 4.5 - 0.6 ( - 4.4 to 3.2)
Medium 30.7 41.4 10.7 (5.0 to 16.4) 57.1 57.2 0.1 (-6.3 to6.5) 2.9 4.9 2.0 ( -0.3 to4.4)
High 46 1 55.6 9.5 {0.9 to 18.6) 69.0 74.9 5.9 (- 2.4 to 14.2) 3.8 5.8 2.0 ( -1.7 to 5.7)
Wear Sunglasses Wear Clothing Stay in Shade or Under Umbrella
(Long Pants or Long-Sleeve Shirt)
1998, 2004, Change,% 1998, 2004, Change, % 1998, 2004, Change,%
% % (Change, 95% Cl) % % (Change, 95% Cl) % % (Change, 95% Cl)
Total (often/always) 32.2 321 -0.1 (-40to3.8) 21.7 22.8 1.1 (-2.5to4.7) 21.8 21.7 -0.1 {-3.7to3.5)
Total {always) 13.2 16.1 2.9(-0.01 !05.8) 7.3 10.8 3.5 {1.0 to 5.0) 2.8 2.2 -0.6 (-2.1 to 0.9)
Age,y
11-13 23.5 25.4 1.9{- 4.1 to 7.8) 21.2 21.0 - 0.2 ( - 6.0 to 5.6) 23.9 25.6 1.7 ( - 4.3 to 7.7)
14-15 30.4 27.3 -3.1 (-10.6to4.4) 18.9 24.3 5.4(- 1.8to 12.6) 19.4 20.6 1.2 ( -6.0 to 8.4)
16-18 43.4 41.8 -1.6 ( -8.5 to 5.4) 24.1 23.4 - 0.7 {-6.9to 5.6) 20.8 19.0 -1.8 (-7.6 to4.0)
Gender
Boys 26.2 24.4 -1.8 { -6.9 to 3.3) 23.9 21.9 -20(-71 to3.1) 21.5 20.5 - 1.0 (-6.0 to4.0)
Girls 38.2 40.1 1.9{ - 4.1to 7.8) 19.4 23.7 4.3 {- 0.8to9.4) 21.9 230 1.1 ( - 4.2to6.4)
Race
White 32.9 32.9 0.0 {-4.3 to 4.3) 18.8 22.7 3.9b {0.2 to 7.6) 18.6 18.8 0.2 (-3.4 to 3.8)
Nonwhite 30.5 290 - 1.5 {- 11.s to 8.5) 32.8 22.7 -10.1b { - 19.8 to - 0.3) 33.3 31.8 - 1.5 (- 11.8 to 8.8)
Sun sensitivity index
Low 34.4 28.7 -5.7 ( -13.4 to 1.9) 261 24.7 -1.4 (-8.7 to 5 9) 22.7 21.4 -1.3 (-8.5 to 5.9)
Medium 31.5 313 - 02 {- 5.7 to 5.3) 20.5 20.4 - 0.1 (- 51 to4.9) 20.6 20.2 - 0.4{- 5.4 to46)
High 30.4 38.1 7.7 ( - 0.3 to 15.7) 18.5 25.3 6.8( - 0.4!0 14.0) 22.7 25.6 2.9 ( - 4.4 to 10.3)
Prevalence of regular sun-safe behavior practiced as always or often.
P< .001.
bf< .05
and reduced likelthood of sunburn experiences in their The beach setting, in particular, provides a greater op-
children.
13
32
-
35
Between 1998 and 2004, the prevalence portunity for exposure to intense (intermittent) UV ex-
of regularly practicing measures of sun protection were posure and is associated with extended time of UV radi-
low, whereas opportunities for high (intermittent) UV ation exposure. J(>.37
exposure seem to have increased (ie, increased number We also found increasing trends in the proportion of
of days spent at the beach). rnterestingly, among older youth who reported wearing sunscreen before getting
youth, we found a larger trend increase in the numbers their most serious sunburns and that regular use of
of days spent at the beach than in younger youth (data sunscreen was independently associated with experienc-
not shown). However, we lack the information to deter- ing sunburn in the past summer, after adjusting for
mine whether the trend increase in the numbers of days confounders. These findings, in parallel to our findings
spent at the beach is related to proximity to the beach, of an increasing trend in regular sunscreen use as de-
popularity of the beach as family vacation, or more scribed next. may suggest that sunscreen use is marker
affordable and frequent travel to beach by older youth. of excessive UV exposure and that, whereas intending to
PEDIATRICS Volume 118. Number 3, September 2006 859
Downloaded from www. pediatrics.org by on October 21 , 2009
00
01
0
r.
0
"' zs
z
TABLE4 Trends in Attitudes Toward Sun Exposure and Tanning Appeal in US Youth, Sun Survey 1998 and 2004
5
Proport ion of Youth Who Total Age,y m
V>
"Strongly Agree or "Agree"
11-13 14-15 16--18
!1!.
1998, 2004, Change 1998, 2004, Change 2004-1998, 1998, 2004, Change 2004- 1998, 1998, 2004, Change 2004-1998,
% % 2004- 1998, % % %(95%( 1) % % %(95%(1) % % %(95%CI)
%(95%(1)
Attitudes on benefits of sun protection
Protecting my skin from the sun is an easy 87.8 92.8 5.0 (2.2 to 7.8) 87.2 92.4 5.2b (0.5 to 9.8) 89.3 93.6 4.3 (-1.1 to 96) 87.4 92.8 5.4b (0.5 to I 0.2)
0 way to stay healthy
0
Using sunscreen allows me to enjoy the 84.8 84.7 - 0.1 (-3.4 to 3.2) 90.4 89.2 - 1.2(- 5.7to3.3) 83.4 85.1 1.7(-4.7 to8.1) 78.9 79.9 1.0 (- 5.3 to 73)
::I outdoors with less worry
0
Spending time outdoors without any sun 91.0 95.1 4.1" (1.6 to 6.6) 90.9 94.8 3.9" (0.0 to 7.8) 90.4 95.5 5. 1"(0.1 to 10.1) 91.4 95.1 3.7 (- 0.4 to 7.8)
"' 0. protection can increase my chances of
g_
developing cancer
a
My skin won't wrinkle as fast if I spend less 73.0 65.0 - s.o(- 12.4 to - 3.6) 68.8 58.0 - 10.8" (- 18.4 to - 3.2) 77.8 68.0 - 9.8(- 18.0to - 1.6) 74.2 69.3 -4.9( - 11.9 to2.1)
3
time in the sun
Sun protection index (1) values s2 86.3 89.8 3.5b (0.5 to 6.5) 87.8 90.2 2.4 (- 2.2 to 7.0) 87.0 913 4.3 (-1.1 to9.6) 84.0 88.3 4.3 (- 1.1 to9.7)
Attitudes on outdoor sun exposure
The sun feels good on my skin 71.7 83.3 11 6 (7.5 to 1 5.6) 66.0 80.0 14.0 (7.0 to 20.7) 73.8 86.5 12.7< (5.0 to 20.4) 76.4 84.6 8.2 (1.7to 14.6)
-o
(b Avoiding the sun takes the fun out of 44.8 50.0 5.2" (0.7 to 9.7) 42.9 51.1 8.2b (0.8 to 15.5) 51.4 46.6 - 48(-13.7 !04.1) 42.4 51.3 8.9b (1.6 to 161)
0.
being outdoors
::l.
Tanning preferences
n
I look better when I have a tan 71.2 67.8 - 3.4( - 7.7100.9) 64.1 618 - 2.3 (-9.7 to 5.1) 76.7 69.0 - 77( - 161 100.8) 75.3 72.4 -2.9(-9.6to38)
"'
0 I feel healthy when I have a nice tan 53.4 55.0 1.6(- 3. 1 to63) 48.2 50.7 2.5( -5.1 to 10.1) 57.8 57.0 - 08 ( - 10.2 to 8.6) 56.4 57.0 06(- 7 t to8.6)
.....
(JQ
Tanning preference index (2) values s2 56.5 51.4 -5.1b (-9.5 to -0.7) 49.5 45.6 - 39(-11.1 to 3.3) 630 52.1 - 10.9b(-19.6to -22) 60.2 56.2 -4.0(- 11.2 to32)
cr
'<
0
::I
Gender Race
0
()
Boys Girls White Nonwhite
0
cr
(b
1998, 2004, Change 2004-1998, 1998, 2004, Change 2004-1998, 1998, 2004, Change 2004- 1998, 1998, 2004, Change 2004- 1998, .....
% o/o %(95%CI) % % %(95%(1) o/o o/o %(95%(1) % % % (95%CI)
-
N
0 Attitudes on benefits of sun protection
0
'-0 Protecting my skin from the sun is an easy 85.6 913 5.7 (1.3 to 10.0) 89.9 94.4 4.5(0.8 to 8.1) 87.9 95.3 7.4 (4.5 to 102) 86.7 84.3 -2.4 (- 10.5 to 57)
way to stay healthy
Using sunscreen allows me to enjoy the
outdoors with less worry
80 l 82.2 2.1 (-2.9to 7.1) 89.5 87.5 - 2.0(-6.1 to2.1) 853 881 28( - 0.4 to60) 82.1 72.7 -9.4 (-18.9to01)
Spending time outdoors without any sun
protection can increase my chances of
89.6 94.9 5.3" (1.6 to 8.9) 92.4 95.3 2.9 ( -0.4 to 6.2) 92.1 97.0 4.9 (2.5 to 7.2) 86.2 890 2.8(- 4.8 to 10.4)
developing cancer
My skin won't wrinkle as fast 1f J spend less 63.5 59.5 - 4.0 (-10.7to 2.7) 79.2 70.6 - 8.6"(- 14.2 to -2.9) 74.8 68.9 - 5.9( - 10.4to - 1.3) 67.0 51.7 - ISJb (- 26.8 to - 3.7)
time in the sun
Sun protection index (1) values s2 83.0 86.8 3.8 ( -0.7 to 8.3) 89.6 92.8 32 (-0.5 to 7.0) 87.9 93.3 5.4 (2.7 to 8.1) 79.5 77.7 - 1.8(- ll.Oto 73)
Attitudes on outdoor sun exposure
The sun feels good on my skm 726 82.6 1 o.oa (4.2 to 15 7) 70.9 841 13.2 (7.5 to 18.8) 76.5 86.0 9.5 (5.5 to 13.5) 54.7 74.6 19.9 (8.8 to 30.9)
0
0
::I
0
"' 0.
g_
::('
0
3
-o
g_
;
"'
0
::I
??
0"
c;rn
.. - R
N '-"'
-.oc:
3
ro
90
z
3
""
"'
-o
00
TABLE 4 Continued
Proportion of Youth Who
"Strongly Agree or "Agree"
Avoiding the sun takes the fun out of
being outdoors
Tanning preference
I look better when I have a tan
l feel healthy when I have a nice tan
Tanning preference index(2) values s2
Attitudes on benefits of sun protection
Protecting my skin from the sun is an easy
way to stay healthy
Using sunscreen allows me to enjoy the
outdoors with less worry
Spending time outdoors without any sun
protection can increase my chances of
developing cancer
My skin won't wrinkle as fast if I spend less
time in the sun
Sun protection index (1) values S2
Attitudes on outdoor sun exposure
The sun feels good on my skin
Avoiding the sun takes the fun out of
being outdoors
Tanning preference
I look better when I have a tan
I feel healthy when I have a nice tan
Tanning preference index (2) values S2
1998,
%
43.0
73.3
57.9
61.1
1998,
%
83.4
77.5
85.9
65.5
77.4
72.2
47.4
72.2
58.0
59.6
Gender
Boys
2004, Change 2004-1998, 1998,
% %(95%( 1) %
51.7 8. 7" (2.4 to 15.Q) 46.7
70.6 -2.7(-8Sto31) 69.2
57.2 -0.7 ( - 7.3 to 5.9) 49.0
532 - 1.8) 52.0
Low Sun Sensitivity
2004, Change 2004-1998, 1998,
o/o %(95%(1) o/o
87.0 3.6 (- 3.0 to 1 0.2) 88.6
75.2 -2.3 (-9.8to52) 86.2
92.5 6.6b (0.8 to 12.3) 93.2
59.7 -5.8(-14.61030) 77.0
82.4 5.0 (- 2.0 to 12.0) 89.1
82.9 107- (2.8to 18.5) 73.9
54.6 7.2 (-1.3 to 15.7) 46.6
69.2 -30(-11.2to52) 74.6
56.4 -1.6 ( - 10.5 to 7.3) 54.5
53.5 -6.1 (- 14.5to2.3) 58.5
Race
Girls White Nonwhite
2004, Change 2004-1998, 1998, 2004, Change 2004- 1998, 1998, 2004, Change 2004-1998,
% %(95%(1) o/o % % (95%CI) % % %(95%(1)
48.3 1.6(-4.7to7.9) 43.4 51.0 7.6b (2.7 to 12.3) 49.3 47.0 -2.3 (- 13.7 to 9.1)
65.0 -4.2(- 10Sto20) 76.0 73.6 -24 ( -6.7 to 19) 530 47.8 -5.2 (-16.9 to6.5)
52.5 3.5 (- 31 to 10.1) 58.0 59.0 1.0(-4.0to6.0) 37.8 40.5 2.7 ( - 8.6 to 14.0)
49.5 -2.5 ( -8.7 to 3.7) 60.7 56.7 - 4.0(-8.6to06) 50.5 33.4 - 64)
--
Medium Sun Sensitivity High Sun Sensitivity
2004, Change 2004-1998, 1998, 2004, Change 2004- 1998,
o/o % (95% en o/o o/o o/o (95% Cl)
95.0 6.4 (2.7 to 1 O.O) 91.2 97.0 5.8 (1.6 to 1 O.O)b
86.9 0.7 (-36to50) 905 93.4 2 9 (-1.9to 7.7)
95.5 2.3 ( -0.8 to 5.4) 92.5 98.2 57" (1.7to 9.6)
67.7 - 9.3 (-15.1 to - 3.4) 74.7 67.9 - 6.8(-15.7 to 2.1)
92.2 3.1 (- O.Sto6.7) 91.7 95.8 4.1 ( -0.3 to 8.5)
85.3 11.4(5.9!0 16.9) 66.4 81.0 14.6 (5.7 to 23.4)
482 1.6(-4.8to8.0) 37.9 48.0 IO.Ob (I I to 18.9)
71.7 -29(-8.7to29) 62.2 58.2 -40(-136to 5.6)
57.3 2.8 (- 3.8 to 9.4) 44.5 48.0 3.5( - 6.3 to 13 1)
54.6 -3.9 (-10.0 to 2.3) 48.5 41.8 - 6.7 (-15.6 to 2.3)
( 1) indicates percentage prevalence score :s2 for benefits of sun protection attitudes index consisting of four items: ' protecting my skin from the sun is an easy way to stay healthy; using sunscreen allows me to enjoy the outdoors with less worry; 'spending time
outdoors without any sun protection can increase my chances of developing cancer.' and 'my skin won't wrinkle as fast if I spend less time in lhe sun'; measured on a 4point Likert these were 1 = strongly agree, 2 = agree, 3 = disagree, and 4 = strongly disagree
(reliabihtycoefficiem Cronbach a =.62). {2) indicates percentage prevalence score :s2 for tanning appeal attitudes index consisting of two nerns: 'I look better when I have a tan and "I feel healthy when I have a nice tan"; measured on a 4point Likert scale these were
1 = strongly agree. 2 = agree. 3 = disagree. and 4 = strongly disagree (reliability coefficient Cronbach a = .69).
P<.OOI.
bf<.OS.
protect themselves from the sun, inadequate application
of sunscreen (ie, not enough appl ied or certain areas of
the body missed) or sunscreens degraded or washed off
from swimming, sweating, or other activities may un-
dennine the sunscreen efficacy for prevention of sun-
burns.38-40 Our findings showed very few improvements
in trends for the regular (routine) practice of sun pro-
tection behaviors and in attitudinal preferences to tan-
ning, whereas some trends in barriers to reduced sun
exposure increased. Specifically, between 1998 and
2004, the only positive increases were for the regular use
of sunscreens, and there was a slight and nonsignificant
reduction (2%) in the prevalence of regular tJse of sun-
screen with SPF 15 + when at the beach or pool (58% vs
56%). Sunscreen use continues to be the main form of
protection from the sun practiced by youth. Our study
found no changes, and the regular use of other sun
protection measures (ie, protective clothing, seeking
shade, and wearing sunglasses) was less prevalent. In
particular, the regular use of wide-brimmed hats in this
population was very infrequent. Research is needed to
understand the reasons or barriers (eg, attitudes, norms,
or contextual settings) related to the low adoption of
such practices.
Modest but significant increases in the prevalence of
youths' attitudes related to benefits of sun protection
occurred between J 998 and 2004; youth in general seem
to hold largely positive attitudes (knowledge-related
benefits) toward sun protection (with the exception that
knowledge levels about the effect of UV exposure and
skin photograph-aging effects were moderate). Educa-
tional skin cancer prevention efforts in schools, outdoor
aquatic settings, and media campaigns may have con-
tributed to these improvements in attitudes/knowledge
during the 6-year petiodY''s
19
In addition, although
trends showed modest decreases, youths' tanning pref-
erences cont.inued to be prevalent, and barriers related
to sun exposure ("sun feels good on my skjn" and
"avoiding the sun takes the fun out of being outdoors")
increased during this period. Tms may suggest that skin
cancer prevention efforts to change such attitudes may
been (somewhat) less effective in youth or that other
factors, such as social norms toward tanrung, fashion
trends, peer pressure, and the lack of policies to support
sun-safe environments, may have been more influential
so as to preclude changes in attitudes.
41
-4
5
Because such
attitudes are determinants of sun exposure and sun pro-
tection behaviors, LO.n-
15
.4
6
-4
8
it is important to develop
better educational messages and strategies targeted at
youth.
There were several strengths and limitations in this
study. The surveys used the same instruments, which
include questions for multiple behavior and attitude end
points, and tbe same probability sampling methodology
to allow for generalizing estimates to the entire popula-
tion of US youth aged l1 to 18 years. However, the
862 COKKINIDES et al
telephone survey methodology limited the generalizabil -
ity of results to persons with a telephone ( ~ 9 5 of US
bouseholds).
49
Particularly in the most recent survey, a
substantial proportion of households were not reached
despite multiple attempts, or selected subjects did not
complete the telephone interview, and, thus, a potential
for unmeasured bias may be present. The sampling de-
sign allowed for a representative sample of the US pop-
ulation, but certain low-frequency population subgroups
were not well represented, because cost issues did not
permit oversampling. We note that skin cancer is mgher
among the white-skinned population, a group that is
well represented in these surveys. Data used in this
study were based on self-reports and possibly subject to
recall bias or social desirability bias. However, surveys
were conducted in an anonymous fashion, and ques-
tions gathered information about recent events and ex-
periences occurring either during the past summer (2- 4
months before the date of interview) or within the last
year.
Internationally, Australia has served as a model of a
national (in scope) comprehensive skin cancer preven-
tion program, which has used systematic ongoing pop-
ulation-based tracking of disease and behavioral end
points.'s
50
5 1
Early in the 1970s, Australia developed a
national health care policy that made skin cancer pre-
vention a public health ptiority; the Australian public
educational campaigns known as Slip! Slop! Slap! (slip
on a shirt, slop on some sunscreen, and slap on a hat)
and the SunSma.rt program, the most recent national
program, involved multipronged approaches in various
settings (schools, worksites, and health care systems), as
well as environmental supports and policies.
20
In the
United States, several broad-based national, state, and
private skin cancer primary prevention efforts have been
initiated, and most target primarily chi ldren.
18
1
9
52
-
55
In
light of our findings of mixed results on sun protection
among US youth, there is a need to further expand
efforts in targeting youth a11d to improve the effective-
ness of these programs. In addition to the assessment of
skin cancer disease trends, there is a need for concomi -
tant surveillance activities to monitor sun protection
practices and sunburn rates in youngsters (and in sus-
ceptible high-risk populations), thereby allowing the
United States to measure success in skin cancer preven-
tion and reduction in disease burden as incorporated in
Objective 3.9 of the Healthy People 2010 goals.
56
CONCLUSIONS
Despite moderate increases in the regular use of sun-
screens among US youth between 1998 and 2004, there
has not been adequate adoption of regular use of other
recommended sun protection practices. Moreover, al-
though the decreasing trends in sunburns among
younger teens may give some cause for optimism re-
garding future trends in skin cancer, there was little
Downloaded from www. pediatrics.org by on October 2 1, 2009
overall change in sunburn trends during this period;
thus, summer sunburns experiences among youth re-
main high. The findings suggest that current efforts in
the United States toward skin cancer prevention have
not been sufficienr to have a major impact on overall sun
protection among youth.
19
Thus, there is a need to
strengthen the implementation of skin cancer preven-
tion programs and interventions along with environ-
mental structural supports and policies
16
18
19
42
41
that
may help shape the social and physical environment and
promote sustainability or these programs. To strengthen
implementation or skin cancer prevention, research is
needed on effective mechanisms to broadJy diffuse skin
cancer prevention intervention and sun-safety policies
in communities
57
and in schools
1
6
17
and for effective
ways to increase the role of pediatri cians and health care
providers wi th their patients
5
R about sun safety practices
to minimize risks associated with excessive UV exposure.
ACKNOWLEDGMENTS
Data collection for the 1998 Sun Survey I was funded by
the American Cancer Society as an intramural research
project. Data collection for the 2004 Sun Survey n was
financially supported by Neutrogena Corporation.
REFERENCES
I. American Cancer Sodety. Cancer Facts and Figures. Atlanta, GA:
American Cancer Sodety; 2006
2. Jemal A, Devesa S, llartge P, Tucker M. Recent trends in
cutaneous melanoma incidence among whites in the United
States. J Nat/ Cancer lnst. 2001;93:678-683
3. Howe H, Wingo P, Thun M, et al. Annual report to the nation
on the status of cancer ( 1973 through 1998), featuring cancers
with recent increasing trends. J Nat/ Cancer lnst. 2001;93:
824-842
4. Christenson L, Borrow111 an T, Vachon C, et al. Incidence of
basa l cell and squamous cell carcinomas in a population
younger than 40 years. JAM/I. 2005;294:681- 690
5. Harris R, Griffith K, Moon T. Trends in the incidence of non-
melanoma skin cancers in southeastern Arizona, 1985- 1996.
JAm Acad Dmuatol. 2001;45:528-536
6. Karagas M, Grccnl>c.:rg E. Spencer S. Stukd T, Molt L. New
Skin Cancer Study Group. Increase in incidence
rates of basal cell and squamous cell skin cancer in New Hamp-
shire. USA. lnt J Cancer. 1999;81:555-559
7. International Agency for Research on Cancer. Monograph on the
Evaluation of Carcinogmic Risks to Humans; Ultraviolet Radiation,
vol. 55. Lyon, France: Int ernational Agency for Research on
Cancer; t 992
8. B, Kricker A. The epidemiology of UV induced skin
cancer. J Phoroclrmr Plrotobiol B. 2001;63:8-18
9. Whiteman D. Whiteman C, Green A. Childhood sun exposure
as a risk factor for melanoma: a systematic review of epidemi -
ologic studies. Cancer Causes Control. 2001;12:69- 82
ro. Davis K, Cokkinidcs V, Weinstock M, O'Connell M, Wingo P.
Summer sunburn and sun exposure among US youths ages 11
to 18: national prevalence and associated factors. Pediatrics.
2002; 110:27- 35
I I. Mermelstein R, Riesenberg L. Changing knowledge and att i-
tudes about ski n cancer risk factors in adolescents. Health Psy-
cho/. 1992;1 1:37 1-376
12. Robinson J, Rademaker A, Sylvester J. Cook B. Summer sun
knowledge, attitudes. and behaviors of Midwest ad-
olescents. Pm Med. I 997;26:364-372
13. Cokkinides V, Johnston-Davis K. Weinstock M, et al. Sun
exposure and sun-protection behaviors and attitudes among
U.S. youth, II to 18ycarsofage.PrMJMed.2001;33:141-15l
14. Alberg A, Herbst R, Genkinger J. Duszynski K. Knowledge.
allitudes, and behaviors toward skin cancer in Maryland
youths. J Ado/esc Health. 2002;31:372-377
15. Geller A, Colditz G, Oliveria S, et al. Use of sunscreen, sun-
burning rates. and tanning bed usc among more than I 0 000
US children and adolescents. Pediatrics. 2002; t09:1009-l 014
16. Glanz K, Saraiya M. Wechsler H. Guiddines for school pro-
grams to prevent skin cancer. MNIWR Recomm Rep. 2002;51 (RR-
4):1- 18
17. Saraiya M, Glanz I<. Briss P, et al. Preventing skin cancer:
findings of the Task Force on Community Preventive Services
On reducing Exposun: tO Ultravioletl.ight. NL'viWR Recomm Rep.
2003;52(RR- I 5): 1- 12
18. Edl ich R. Wimers K, Cox M, et al. National health strategies to
reduce sun exposure in Australia and the United States. J Long
Tenu Eff Med Imp/allis. 2004; 14:215-224
19. Geller A, Cantor M, Miller D, et al. The Environmental PrOtec-
tion National SunWise School Program: sun protec-
tion education in US (1999-2000). JAm Acad Dermato/.
2002;46:683-689
20. Montague M, Borland R. Sinclair C. Slip! Slop! Slap! and
SunSman, 1980-2000: Skin cancer control and 20 years of
population-based campaigning. Health Educ Behav. 2001;28:
290-305
21. Waksberg J. Sampling methods for random digit dialing. JAm
Stat Assoc. 1978:73:40- 46
22. National Weather Service. UV Index Forecast. Available at:
www .cpc. nce1). noaa .gov /prod ucts/st ra tOsphere/u v _index /uv _
current.htrnl. July 30, 2004
23. The American Association for Public Opinion Research. Stan-
dard Definitions: Final Disposition of Case Codes and Outcome Rates
and Otucome Rates for Surveys. Ann Arbor, MI: American Asso-
ciation for Publ ic Opinion Research (AAPOR); 2004
24. Massey J. O'Connor D, J<rokt i K. Response Rates in Random Digit
Dialing (RDD) Telephone Surveys. Alexandxia, VA: American Sta-
tist ical Association; 1997
25. Weinstock MA. Assessment of sun sensitivity by questionnaire:
validity or items and formulation of a prcdicrion rule . .! Clin
Epidemic/. 1992;4 5:5117-552
26. SAS Institute, Inc. SAS Procedure Guide. Cary, NC: SAS Insti tute,
Inc; 1999
27. SUDAAN Usa's Manual. Professional Software for Survey Data
Analysis !computer program]. Version 9.0. Research Triangle
Park, NC: ReS('arch Triangle Institute; 2003
28. Saraiya M. Glanz K. Briss P, et at. Interventions to prevem skin
cancer by reducing exposure to ultraviolet radiation: a system-
atic review. Am J Prrv Med. 2004;27:422-466
29. Banks B. Silvennan R. Schwanz R, Tunnessen W. Attitudes of
teenagers toward sun exposure and sunscreen use. Pediatrics.
I 992;89:40-4 3
30. Reynolds K, Blaum J, Je5ter P, Webs H. Soong S, Didememe R.
Predictors of sun exposure in adolescents in a southeastern
U.S. population. J Ado/esc Health. 1996;19:409-41 5
31. Hall H, Jones S, Saraiya M. Pn:valcncc and correlates of sun-
screen use among US high school students. J Sch Health. 200 L;
71:453-457
32. Hall H, Jurgensen C. McDavid K. Kraft J, Breslow R. Protection
from sun exposure in US white children ages 6 months to I I
years. Public Henltlr Rep. 2001;116:353-361
33. Johnson K. Dnvy L. Boyett T, Weathers L, Roetzhcim R. Sun
PFDIATRICS Volume 118, Number 3, September 2006 863
Downloaded from www.pediatrics.org by on October 2 1, 2009
protection practices for children: knowledge, atti tudes. and
parent behaviors. Arch Pediatr Ado/esc Med. 2001; 155:891- 896
34. O'Riordan D, Geller A, Brooks D, Zhang Z, Miller D. Sunburn
reduction through parental role modeling and sunscreen vigi-
lance. J Pediatr. 2003; 142:67-72
35. Turrisi R, Hillhouse J, Heavin S, Robinson J, Adams M, Berry
J. Exami.nation of the short- term effi cacy o[ a parent-based
intervention to prevent skin cancer. J Behav Med. 2004;27:
393- 412
36. Buller D, Borland R. Skin cancer prevention for children: a
critical review. Heallh Educ Behav. 1999;26:317- 343
37. Thieden E, Philipsen P, Sandby-Moller J, Wuil H. Sunburn
related to UV radiation exposure. age, sex. occupation. and sun
bed usc based on time-stamped personal dosimetry and sun
behavior diaries. Arch Derma to/. 2005; 141:482- 488
38. Diffey B. Grice J The influence of sunscreen t ype on photopro-
tection. Br J Dermato/. 1997; 137:103-105
39. Wul H. Sender 1. Lock-Andersen J . Sunscreens used at the
beach do not protect against. erythema: a new defini tion of SPF
is proposed. Photodermatol Photoimmunol Photomed. 1997; 13:
129- 132
40. Autier P, Boniol M, Severi G. Dore J, European Organization
for Research and Treatment of Cancer Melanoma Co-operative
Group. Quantity of sunscreen used by European students. Br J
Derma/of. 2001;144:288-291
41. Hill D. Dixon H. Promoting sun protection in children: ratio-
nale and challenges. Health Educ Behav. 1999;26:409- 4 17
42. Hill D. Skin cancer prevention. Am J Prev Med. 2004;27:
482- 483
43. Erru11ons K. Colditz G. Preventing excess sun exposure: it is
time for a nat ional poli cy. J Nat/ Cancer lnst. 1999;9 1:
1269-1270
44. Lower T, Girgis A, Sanson-Fisher R. The prevalence and pre-
dictors of solar protection use among adolescents. Prev Med.
1998;27:391-399
45. Livingston P, White v, Hayman J. Dobbinson S. Sun exposure
and sun protection behaviours among Australian adolescents:
t rends over time. Prev Med. 2003;37:577-584
46. Branstrom R. Brandberg Y, Holm L, Sjoberg L. Ullen H. Beliefs,
knowledge and attitudes as predictors of sunbathing habits and
use of sun protection among Swedish adolescents. Bur J Cancer
Prev. 2001;10:337- 345
47. Lowe J. Borland R, Stanton W, Baade P, White V. Balanda K.
864 COKKINIDES et al
Sun-sa fe behaviour among secondary school students in Aus-
tralia. Health Educ Res. 2000;15:271- 281
48. Wichstrom L. Predictors of Norwegian adolescents' sunbathing
and use or sunscreen. Health f>sychol. I 994; I 3:412- 420
49. US Bureau of the Census. Phone/ess in America. Washington,
DC: US Department of Commerce Economics and Statistics
Administration . .Bureau of the Census; I 994. Statistical brief
94-1 6
50. Hill D. White V. Marks R. Borland R. Changes in sun-related
attitudes and behaviours. and reduced sunburn prevalence in a
population at high risk of melanoma. Eur J Cancer Prev. 1993;
2:447-456
51. Staples M, Marks R. Giles G. Trends in the incidence of non-
melanocytic skin cancer (NMSC) t r ea ted in Au st rali a
1985-1995: arc p rimary prevent ion programs starting to have
an effect? lnt J Cancer. 1998;78:144- 148
52. Jorgensen C. Wayman J, Green C, CA. G. Using health com-
munications for primary prevent ion o f skin cancer: CDC's
Choose Your Cover campaign. J Womens Health Gend Based Med.
2000;9:471- 475
53. American Cancer Society. Skin Cancer. Atlanta, GA: American
Canct:r Society. Available at: www.cancer.org. Accessed Octo-
ber 10, 2005
54. Lim H. Cooper l<. The health impact of solar radiation and
prevention strategies: Report of the Environment CounciL
American Academy of Dermatology. JAm Acad Dennatol. I 999;
41 :8 1-99
55. Skin Cancer Foundation. Sun and Skin News. New York. NY:
Skin Cancer Foundation; 2002:19.
56. Healthy People 2010 (HP2010)- Volume I. Focus Area: Cancer. Ob-
jective .3- 9: Sun Exposure and Skin Cancer. Rockville. MD: Office
of Disease Prevention and Health Promotion. U.S. Department
oi Health and Human Services; 2000. Available at: www.
health ypeople. gov I document/ htmlfvolLu11e 1 I 0 3ca ncer.htm # _
Toc490540737. Accessed November 30. 2005
57. l ~ n z K, Steffen A. Elliott T, O'Riordan D. Diffusion or an
effective skin cancer prevention program: design. theoretical
foundations, and first-year implementation. Health Psycho/.
2005;24:477-487
58. Gritz ER. Tripp MK, de Moor CA. Eicher SA. Spedale JH. Skin
cancer prevention counseling and cl inical practices or pediatri-
cians. Pediatr Derma to/. 2003;20: I 6 -24
Downloaded from www. pediatrics.org by on October 21, 2009
Trends in Sunburns, Sun Protection Practices, and Attitudes Toward Sun
Exposure Protection and Tanning Among US Adolescents, 1998-2004
Vilma Cokkinides, Martin Weinstock, Karen Glanz, Jessica Albano, Elizabeth Ward
and Michael Thun
Updated Information
& Services
Refer ences
Citations
Subspecialty Collections
Permissions & Licensing
Reprints
Pediatrics 2006; 118;853-864
including high-resolution figures, can be found at:
http://www.pediatrics.org/cgi/content/full/ 118/3/853
This article cites 47 articles, 13 of which you can access for free
at:
http://www. pediatrics.org/cgi/content/full/ 118/3/853#BIBL
This article has been cited by 7 High Wire-hosted articles:
http://www.pediatrics.org/cgi/content/full/118/3/853#otherarticle
s
This article, along with others on similar topics, appears in the
following collection(s):
Allergy & Dermatology
http://www.pediatrics.org/cgi/collection/allergy_and_dermatolog
y
Information about reproducing this article in parts (figures,
tables) or in its entirety can be found online at:
http://www.pediatrics.org/misc/Permissious.shtml
Information about ordering reprints can be found online:
http://www.pediatrics.org/rnisc/reprints.shtml
American Academy of Pediatrics
DEDICATED TO T H E HEALTH OF ALL CHILDREN*
Downloaded from www.pediatrics.org by on October 21, 2009
A Prospective Study of Pigmentation, Sun Exposure, and
Risk of Cutaneous Malignant Melanoma in Women
Marit Bragelien Veierd, Elisabete Weiderpass, Magnus Thorn, Johan Hansson,
Eiliv Lund, Bruce Armstrong, Hans-Olov Adami
Background: Although sun exposure is au established cause
of cutaneous malignant melanoma, possible interactions with
host factors remain incompletely understood. Here we re-
port the first results from a large prospective cohort study of
pigmentation factors and sun exposure in relation to mela-
noma risk. Methods: The Women's Lifestyle and Health Co-
hort Study included 106 379 women from Norway and Swe-
den who were aged 30-50 years in 1991 or 1992 when they
completed an extensive questionnaire on personal character-
istics and exposures. Linkages to national registries ensured
complete follow-up through December 31, 1999. Poisson re-
gression models were used to estimate relative risks (RRs).
All statistical tests were two-sided. Results: During an aver-
age follow-up of 8.1 years, 187 cases of melanoma were di-
agnosed. Risk of melanoma was statistically significantly as-
sociated with increasing body surface area (RR for ;:.1.79 m
2
versus m
2
= 1.60, 95% confidence interval [CI] = 1.03
to 2.48; Ptrend = .02), number of large asymmetric nevi on the
legs (RR for ;:.7 nevi versus 0 nevi= 5.29, 95% CI = 2.33 to
12.01; Ptrend<.001), hair color (RR for red versus dark
brown or black= 4.05, 95% CI = 2.11 to 7.76; Ptrend<.001),
sunburns per year at ages 10-19, 20-29, and 30-39 years
cPtrend<.001, Ptrend = .03, and Ptrend = .05, respectively), and
use of a device that emits artificial light (solarium) one or
more times per month (P = .04). Conclusions: Our results
confirm previous findings that hair color, number of nevi on
the legs, and history of sunburn are risk factors for mela-
noma and suggest that use of a solarium is also associated
with melanoma risk. Adolescence and early adulthood ap-
pear to be among the most sensitive age periods for the
effects of sunburn and solarium use on melanoma risk. How-
ever, it may be too early to see the full effect of adult expo-
sures in this cohort. [J Natl Cancer lnst 2003;95:1530-8]
Cutaneous malignant melanoma (hereafter called melanoma)
imposes a considerable public health burden. The incidence of
melanoma va1ies more than 150-fold around the world, with the
highest rates occurring among white or predominantly white
populations in Australia, New Zealand, North America, and
northern Europe ( 1 ). Rates of melanoma in Norway and Sweden
have more than tripled since 1958- 1962, the first years that
Affiliations of authors: M. B. Section of Medical Statistics, Univer-
sity of Oslo, Oslo, Norway; E. Weiderpass, Department of Medical Epidemiol-
ogy and Biostatistics, Karolinska lnstitutet, Stockholm, Sweden, and Interna-
tional Agency for Research on Cancer, Lyon, France; M. Th<im. Department of
Surgery, South Stockholm General Hospital , Stockholm; J. Hansson, Depart-
ment of Oncology and Pathology, Karolinska Institute!; E. Lund, Institute of
Conununity Medicine, University of Troms0, Norway; B. Armstrong,
School of Publ ic Health, University of Sydney, Sydney, Australia; H.-0. Adami,
Department of Medical Epidemiology and Biostatistics, Karol inska Institute!.
and Department of Epidemiology, Harvard University, Boston, MA.
Correspondence ro: Marit B. Veier!ild, PhD, Section of Medical Statistics,
University of Oslo, P.O. Box 1122 Blindern, N-0317 Oslo, Norway (e-mail:
marit.veierod@basahned.uio.no).
See "Notes" following "References."
DOl : 10.1 093/jnci/djg075
.Journal of the National Cancer l nsrilute, Vol. 95, No. 20, Oxford University
Press 2003, all rights reserved.
1530 ARTICLES Joumal of the National Cancer Institute, Vol. 95, No. 20, October 15, 2003
0
0
::::
g
c.
"' c.
a
3
0
::::
reliable information was available from cancer registries; rates
are now higher there than they are elsewhere in Europe (2) and
are predicted to increase (3 ).
Although sun exposure is the major established risk factor for
melanoma (4,5), geographic differences in melanoma incidence
cannot be attributed solely to differences in the intensity of solar
exposure. Within Europe, for example, the incidence of mela-
noma is higher at northern latitudes, which generally have lower
solar intensities, than at southern latitudes, which generally have
higher solar intensities (2), although in both Norway and Swe-
den, an inverse relationship between melanoma incidence and
latitude has been noted (6,7). Hence, the etlect of UV light on
melanoma risk may be strongly modified by other factors, such
as differences in sun sensitivity and the nature of the exposure to
the sun (8).
A number of studies have examined factors that influence the
association between sun exposure and the risk of melanoma. An
intermittent pattern of sun exposure, which is typically assessed
by measures of sun-intensive activities, such as outdoor recre-
ation or vacations, is associated with increased risk of melanoma
(9). In addition, many studies (4,5,9,10) have reported that sun-
burn, which is an indicator of an intermittent pattern of sun
exposure, is positively associated with the risk of melanoma.
Results of many studies have suggested that childhood is a criti-
cal period for sun exposure (9), and ecologic studies have shown
more consistent associations than case-control studies between
childhood sun exposure and melanoma risk ( 11 ). Host factors
such as eye color, hair color, skin color, the number of nevi, and
skin reaction to chronic and acute sun exposure have also been
associated with the risk of melanoma (4, 12).
Most of what is known about the association between sun
exposure and melanoma risk comes from results of case-control
studies. The Nurses' Health Study is, as far as we know, the only
cohort study to examine the association between sun exposure
and malignant melanoma; however, a case- control design within
the cohort was used in these analyses ( 13,14 ). Case-control
studies are limited by the potential for differential bias in recall
of sun exposure between case patients and control subjects
(15, 16). Prospective cohort studies can overcome such limita-
tions because the exposure information is collected prior to dis-
ease occurrence. Here we report the first results from the Nor-
wegian-Swedish Women's Lifestyle and Health Cohort Study,
which was initiated in 1991. This study is the first prospective
cohort study, to our knowledge, to examine the associations
between pigmentation factors and sun exposure and the risk of
malignant melanoma.
SUBJECTS AND METHODS
Study Population
For practical reasons, women were enrolled in the Norwegi-
an- Swedish Women's Lifestyle and Health Cohort Study in
both 1991 and 1992.ln Norway, a nationwide random sample of
100000 women who were born between 1943 and 1957 (i.e.,
aged 34-49 years at inclusion) was drawn from the National
Population Register at Statistics Norway (Oslo, Norway). In
Sweden, a random sample of 96 000 women who were born
between 1943 and 1962 (i.e., aged 30-50 years at inclusion) and
were residing in the Uppsala Health Care Region (which com-
prises about one-sixth of the Swedish population) was drawn
from the National Population Register at Statistics Sweden
(Stockholm, Sweden).
All women received a letter inviting them to participate in the
study. The letter also requested that they provide written in-
formed consent and contained a comprehensive questionnaire
that was to be completed and returned in a prepaid envelope.
Identical questions relevant to the analysis presented here were
included in the questionnaires sent to women in the two coun-
tries. The study was approved by the Data Inspection Boards in
both countries and by the regional Ethical Committees, and all
women gave written informed consent to participate.
Host Factors and Exposure Information
In the questionnaires, study participants were asked to cat-
egorize their natural hair color (dark brown/black, brown, blond,
or red) and their eye color (brown, gray/green, or blue) and to
categorize the number of asymmetric nevi larger than 5 mm on
their legs from toes to groin (0, 1, 2- 3,4- 6,7- 12, 13- 24, or ;;.25
nevi). A brochure that was included with the questionnaire pro-
vided color pictures with three examples of asymmetric nevi.
Participants recorded their sun sensitivity according to their
reactions to both acute and chronic exposure to the sun. Regard-
ing acute sun exposure, the questionnaire asked the women to
choose from among four categories to describe how their skin
reacts to heavy sun exposure at the beginning of the summer: the
skin turns brown without first becoming red, the skin turns red,
the skin turns red with pain, or the skin turns red with pain and
blisters. The women were asked to describe how their skin reacts
to long-lasting or chronic sun exposure according to four cat-
egories: the skin turns deep brown, brown, or light brown, or the
skin never turns brown.
Participants were asked to report their histories of sunburn
and sunbathing vacations and on the frequency of their use of a
solarium (i.e., a sun bed or a sunlamp that emits artificial UV
light) when they were aged 10-19, 20-29, 30-39, or 40-49
years. For each age period, the participant was asked to report
the number of times per year she had been burned by the sun so
severely that it resulted in pain or blisters that subsequently
peeled by choosing from among five categories: never, one time
per year at most, two or three times per year, four or five times
per year, or six or more times per year. Participants reported the
average number of weeks per year spent on sunbathing vacations
in southern latitudes (typically southern Europe, e.g., Spain or
Greece) or within Norway or Sweden for each age period by
choosing from among five categories: never, I week per year,
2-3 weeks per y e a r ~ weeks per year, or ;;.7 weeks per year.
Participants reported their average use of a solarium during each
age period by choosing from among six categories: never, rarely,
one time per month, two times per month, three or four times per
month, or more than one time per week. The questionnaires also
contained questions about the participant' s current height and
weight, current and past contraceptive use, reproductive history,
prevalent diseases, and lifestyle.
Follow-up and Endpoints
Start of follow-up was defined as the date of receipt of the
returned questionnaire. Person-years were calculated from the
start of follow-up to the date of diagnosis of primary melanoma,
to the date of emigration or death, or to the end of follow-up
(December 31, 1999), whichever occurred first. Each resident of
Norway and Sweden is assigned a unique national registration
number that includes the person's date of birth; those registra-
tion numbers are entered into the nationwide databases that were
Journal of the National Cancer Institute, Vol. 95, No. 20, October 15, 2003 ARTICLES 1531
0
0
~
::::
g
c.
"' c.
a
3
0
::::
used in this study. By linkage of cohort data to the national
cancer registries in Norway and Sweden, this national registra-
tion number allowed us to identify cancer cases. Information on
death and emigration was gathered by linkage to Statistics Nor-
way and Statistics Sweden.
A total of 57 584 (57.6%) of the Norwegian women and
49 259 (51.3%) of the Swedish women returned completed ques-
tionnaires; the overall response rate was 54.5%. We excluded
four women because of the lack of vital status information in the
available register files, 18 women who had emigrated or died
before the start of follow-up, 198 women who did not adequately
answer the questions regarding sun exposure or personal char-
acteristics (i.e., sun sensitivity of skin, hair color, eye color, and
number of asymmetric nevi), and 244 women who were diag-
nosed with melanoma prior to the start of follow-up.
Statistical Analysis
Participants' geographic regions of residence were defined
according to four categories: the southern region of Norway, the
middle region of Norway, the northern region of Norway, and
the Uppsala Health Care Region in Sweden. The latitudes of the
population center of mass within each Norwegian county, which
were provided by the Norwegian Mapping Authority, together
with the observed number of melanoma cases in those counties,
formed the basis for our definitions of the three Norwegian
regions. The southem region of Norway includes Vest-Agder,
Aust-Agder, Rogaland, Vestfold, 0stfold, and Telemark coun-
ties, with population centers of mass located at 5824' - 5931'
N; the middle region of Norway includes Oslo, Akershus, Bus-
kerud, Hordaland, Oppland, Hedmark, and Sogn og Fjordane
counties, with population centers of mass located at 5958' -
61 30' N; the northern region of Norway includes Ms:6re og
Romsdal, Ss:6r-Trndelag, Nord-Trs:6ndelag, Nordland, Troms,
and Finnmark counties, with population centers of mass located
at 6244'- 7022' N. The Uppsala Health Care Region in Swe-
den has the population center of mass located at 5986' N.
Body surface area was calculated according to the formula (17)
weight
0
425
x height
0 725
x 71.84 and categorized by guartiles.
We combined the upper two categories of the variables concern-
ing acute and chronic exposures to sun because of the small
numbers in each category and analyzed nevus counts in three
categories: 0, 1, 2-6, and ~ 7 (only two categories, 0 and ~ 1
were used when testing interaction effects). In the age period-
specific analyses of sunburns, sunbathing vacations, and so-
larium use, we combined the upper categories of these variables
because of small numbers. For each of the variables (sunburns,
sunbathing vacations, and solarium use), new variables were
constructed to combine the exposure during the three age peri-
ods that were recorded for all women (i .e., 10-19,20-29, 30-39
years).
We used Poisson regression analysis to estimate the associa-
tion between sun exposure or personal characteristics and the
risk of melanoma. The statistical significance of independent
variables and interaction effects was tested by using the likeli-
hood ratio test. We tested for trends across categories of vari-
ables by assigning equally spaced values (e.g., I , 2, 3, or 4) to
the categories and treating the variables as continuous variables
in the Poisson regression analysis. All analyses were adjusted for
attained age (i.e., age at study entry plus the duration of follow-
up), which was categorized by 5-year intervals (for analyses of
women aged 40 years or older, we used only two age categories,
<50 years and 50-60 years), and all multivariable models also
included geographic region of residence. The analyses of per-
sonal characteristics included mutual adjustments for statisti-
cally significant variables. The multivariable models used in the
analyses of sunburn, sunbathing vacations, and use of a solarium
included hair color. In addition, each age-specific model for use
of a solarium included the corresponding numbers of age-
specific sunburns and sunbathing vacations. Results are pre-
sented as relative risks (RRs) with 95% confidence intervals
(Cis). All P values are two-sided, and a 5% level of statistical
significance was used.
RESULTS
The final study sample consisted of 106 379 Norwegian and
Swedish women. Dming an average 8.1 years of follow-up (me-
dian = 8.3 years, range = 0.01- 8.6 years) corresponding to
866 668 person-years of observation, 187 incident cases of mela-
noma were reported to the Cancer Registries in Norway and
Sweden. These incident cases occurred among 183 women for
whom melanoma was their first cancer diagnosis and four
women for whom melanoma was their second cancer diagnosis.
All incident cancer cases were histopathologically confirmed as
invasive melanoma. Characteristics of the study cohort and of
the incident cases of malignant melanoma and their frequencies
are summarized in Table 1. Melanomas on the lower limbs were
observed most frequently, followed by melanomas on the trunk.
Classification of subtypes was less frequently performed in Swe-
den than in Norway. Seventy-one percent of the Norwegian cases
were classified as superficial spreading melanoma (Table 1).
Table 2 summarizes the associations between personal char-
acteristics and the risk of melanoma. Calculated body surface
area was positively associated with the risk of melanoma (Ptrend
= .02), as was hair color (P trend<.OO I). Compared with women
who had dark brown or black hair, women with blond hair had
an approximately twofold higher risk of melanoma, whereas
women with red hair had an approximately foUifold higher tisk.
Eye color was not associated with melanoma risk. We also found
no statistically significant association between tanning of the
skin after heavy or repeated sun exposure and the risk of mela-
noma, although an indication of a trend was seen for skin color
after repeated sun exposure. The number of large asymmetric
nevi on the legs was a strong predictor of melanoma risk: women
with seven or more nevi had an approximately fivefold higher
risk of melanoma than women with no nevi (Ptrend<.OO I ). Mu-
tual adjustment for all statistically signi ficant variables li sted in
Table 2 did not appreciably change any of the multivariable
relative risks presented in the table (data not shown).
Risks of melanoma increased with increasing numbers of
sunburns women reported having during the second, third, and
fourth decade of life (Table 3). The estimated risk of melanoma
was highest for women who reported having sunburns during
adolescence (i.e., the 10-19-year age period), whereas no asso-
ciation between risk and sunburns during the fifth decade of life
(i.e., the 40-49-year age period) was observed. Next, we com-
bined the information about the number of sunburns at ages
10-19, 20-29, and 30-39 years into one new variable. Women
who had one or no sunburns per year during these three periods
were used as the reference category. The other categories were
sunburns two or more times per year during the adult years (i.e.,
20-29 years and/or 30-39 years), sunburns two or more times
1532 ARTICLES Joumal of the National Cancer Institute, Vol. 95, No. 20, October 15, 2003
0
0
~
::::
g
c.
"' c.
a
3
0
::::
Table 1. Characteristics of participants in the Norwegian-Swedish Women's Lifestyle and Health Cohort Study and of the incident cases
of cutaneous malignant melanoma during follow-up from 1991- 1992 through 1999
Characteristics
Mean age at study entry, y (range)
Person-years of follow-up
Number of incident cases of melanoma
Mean age at diagnosis of melanoma, y (range)
Site of melanoma, No. (%)
Tlllnk
Upper limb
Lower limb
Othert
Histologic type of melanoma, No. (%)
Superficial spreading melanoma
Nodular melanoma
Lentigo malignant melanoma
Malignant melanoma, not othenvise specified
Body surface area in m
2
t No. (%) (n = 103 333)
~ 1 6 1
1.62- 1.69
1.70-1.78
:;. ).79
Norway
(n = 57 3 ll )*
41. I (34--49)
468982
121
45.7 (35.4-54.0)
32 (26)
12 (10)
60 (50)
17 (14)
86 (71)
16 (13)
2 (2)
17(14)
13 985 (25)
13 929 (25)
14361 (26)
13 896 (25)
Sweden
(n = 49 068)*
39.6 (30-50)
397 686
66
45.3 (31.9- 57.5)
19 (29)
10 ( IS)
29 (44)
8 (12)
5 (8)
2 (3)
0 (0)
59 (89)
I I 696 (25)
I I 680 (25)
II 802 (25)
I I 984 (25)
Total
(N = 106 379)*
40.4 (30-50)
866668
187
45.6 (31.9- 57.5)
51 (27)
22 ( 12)
89 (48)
25 (13)
91 (49)
18 ( 10)
2 (I)
76 (41)
25 681 (25)
25 609 (25)
26 163 (25)
25 880 (25)
Skin color after heavy sun exposure in the beginning o f the summer, No. (%) (n = 105 595)
Brown 14 856 (26)
27 584 (49)
11 342 (20)
I 1532 (24)
23 243 (48)
11421 (23)
26 388 (25)
50 827 (48)
22763 (22)
Red
Red with pain
Red with pain and blisters
Skin color after repeated sun exposure, No. (%) (n = 103 31 2)
Deep brown
Brown
Light brown
Never brown
Hair color, No. (%) (n = 103 027)
Dark brown, black
Brown
Blond
Red
Eye color, No. (%) (n = J 02 710)
Brown
Gray, green, or mi x
Blue
Total No. of asymmetric nevi >5 mm on legs, No.(%) (n = 100980)
0
1
2-3
4- 6
:;.7
2999 (5)
8797 ( 16)
31394 (58)
13 453 (25)
900 (2)
9348 (17)
21 500 (39)
22241 (41)
1495 (3)
6345 ( 12)
2 1 062 (39)
27 170 (50)
47 704 (89)
3438 (6)
1595 (3)
416 (I)
324 (I)
261 8 (5)
7979 (16)
30029 (62)
10129 (2 1)
631 ( I)
13813(29)
20939 (43)
12 185 (25)
1506 (3)
6738 (14)
17 130 (36)
24 265 (50)
38 997 (82)
4842 (10)
2424 (5)
713 (2)
527 (l)
5617(5)
16776 ( 16)
61423 (59)
23 582 (23)
1531 ( I )
23 161(23)
42439 (41)
34426 (33)
3001 (3)
13 083 (13)
38 I 92 (37)
5 I 435 (50)
86 701 (86)
8280 (8)
4019 (4)
I 129 (I)
851 (I)
*Because of missing values. the number of women wil l d iffer in the presentation of personal characteristics below. The total number of women (n) is presented
for each personal characteristic.
t Head/neck and skin unspecitied.
*Calculated according to the followi ng formula {17): weight
0
..
25
x height
0
725
x 71.84.
per year dming adolescence (i.e., l0- 19 years), and sunburns
two or more times per year during all three age decades (i.e.,
10-19, 20-29, and 30-39 years). We observed increased risk of
melanoma for the upper two categories of this new variable and
a statistically significant positive trend (Table 3). Collapsing the
upper three categories into one gave a multi variable relative risk
of 1.70 (95% CI = 1.23 to 2.34; P = .002) for sunburns two or
more times per year for at least one of the three age decades as
compared with a maximum of one sunburn per year in all three
decades. No statistically significant interaction was found be-
tween this dichotomous sunbum variable and the number of nevi
on the legs (P = .84).
We found suggestive evidence for an association between
increasing risk of melanoma and increasing number of weeks
women spent on sunbathing vacations at ages 30- 39 years
(Table 4). Although most of the point estimates and all of the
trends pertaining to this association were not statistically signifi-
cant, we consistently observed a risk increase of approximately
60%- 70% for the hi ghest compared with the lowest exposure
category for women who took sunbathing vacations between the
ages of I 0 and 39 years. Increased risk, albeit not statisticall y
significant and with no appreciable trend, was also observed
when inforn1ation on sunbathing vacations from these three de-
cades of life was combined into a new variable in a way analo-
Journal of the National Cancer Institute, VoL 95, No. 20, October 15, 2003 ARTICLES 1533
0
0
~
::::
g
c.
"' c.
a
3
0
::::
Table 2. Relative risks (RRs) and 95% confidence intervals (Cis) of cutaneous malignant melanoma according to personal characteristics*
Characteristic
Body surface area, m
2
:j: (n = I 03 333)
1.62- 1.69
1.70--1.78
;;> 1.79
Skin color after heavy sun exposure at the beginning of sunuuer (n = 1 OS 595)
Brown
Red
Red with pain/red with pain and blisters
Skin color after repeated sun exposure (11 = 103 312)
Deep brown
Brown
Light brown/never brown
Hair color (n = 103 027)
Dark brown, black
Brown
Blond
Red
Eye color (n = I 02 710)
Brown
Gray, green, or mix
Blue
Total No. of asymmetric nevi >5 mm on legs (n = 100 980)
0
I
2--6
;;>7
*Poisson regression analysis. All statistical tests were two-sided.
t Multivariable models included attained age and region of residence.
No. of cases
32
44
57
52
36
100
51
21
107
51
26
57
82
14
18
63
97
128
26
16
6
Age-adjusted RR (95% Cl) Multivariable RRt (95% Cl)
1.00 (referent) 1.00 (referent)
1.38 (0.87 to 2. 17) 1.37 (0.87 to 2.17)
1.74 (1.13 to 2.68) 1.73 ( 1.12 to 2.66)
1.60 (1.03 to 2.49) 1.60 ( 1.03 to 2.48)
Puend = .02 P.,,.od = .02
1.00 (referent) 1.00 (referent)
1.45 (0.99 to 2.12) 1.45 (0.99 to 2.13)
1.34 (0.88 to 2.06) 1.36 (0.89 to 2.08)
plr<Od = .21 P.,,.od = .19
1.00 (referent) 1.00 (referent)
1.39 (0.87 to 2.22) 1.40 (0.87 to 2.23)
1.62 (0.97 to 2.69) 1.60 (0.96 to 2.67)
ptrcnd = .07 Pcrcnd = .07
1.00 (referent) 1.00 (referent)
1.18 (0.74 to 1.88) 1.16 (0.73 to 1.84)
2.10 (1.35 to 3.26) 1.96 ( 1.25 to 3.07)
4.13 (2.16to7.9l) 4.05 (2.11 to 7.76)
P.,..,, d<.OOl ptrend<.OOI
1.00 (referent) 1.00 (referent)
Ll8 (0.70 to 1.99) 115 (0.68 to 1.94)
1.36 (0.82 to 2.25) 1.33 (0.80 to 2.20)
P,,..," = .17 P,.en<l = .19
1.00 (referent) 1.00 (referent)
2.15 ( 1.41 to 3.28) 2.29 ( 1.50 to 3.49)
2.14 (1.27 to 3.60) 2.30 ( 1.36 to 3.87)
4.92 (2.17 to 1l.l5) 5.29 (2.33 to 12.01)
P""""<.OOI
:j:Calcu1ated acc-ording to the following formula ( 17): weight
0
..
25
x height
0
725
x 7 1.84.
gous to that described above for sunburns (Table 4). Collapsing
the upper three categories of this new vatiable gave a multi vari -
able relative risk of 1.51 (95% CI = 0.95 to 2.40; P = .07) for
sunbathing vacations one or more weeks per year in at least one
of the three age decades as compared with never going on sun-
bathing vacations in any of the three decades. No statistically
significant interaction was found between this dichotomous vari-
able for sunbathing vacations and the number of nevi on the legs
(P = .58).
We had limited power to examine the association between the
use of a solarium during adolescence and melanoma risk be-
cause only 2% of the women in the study reported having such
exposure. However, we found that compared with women who
never used a solarium at ages 20-29 years, women who reported
using a solarium once or more per month during that age period
had a relative risk of melanoma of 2.58 (95% CI = 1.48 to 4.50;
Ptrend = .006) (Table 5). Use of a solarium at ages 30- 39 years
and 40-49 years also appeared to be associated with a risk,
although not a statistically significantly increased risk, of mela-
noma (Table 5). In a multivariable analysis of the combined
variable for solarium use duri ng the 10- 39-year age period,
women who used a solatium one or more times per month jn at
least one of the three decades between ages 10 and 39 had a
statistically significantly higher risk of melanoma than women
who had never or rarely used a solarium during those three
decades (RR = 1.55, 95% CI = 1.04 to 2.32; P = .04) (Table 5).
The multivariable models in Tables 3-5 include hair color as
a measure of sun sensitivity. Additional adjustment for skin
color after repeated sun exposure gave similar results and did not
affect the conclusions (data not shown).
DISCUSSION
Results of our prospective analysis suggest that hair color, the
number of large asymmetric nevi on the legs, and body surface
area are important personal characteristics that contribute to the
risk of melanoma. The number of sunburns was also an impor-
tant predictor of melanoma risk, and the strongest effects were
associated with the number of sunburns women experienced
during adolescence; there was similar, albeit weaker, evidence
for an associat.ion between the number of sunbathing vacations
taken in Norway, Sweden, or more southern latitudes and mela-
noma risk. Using a solarium one or more times per month,
particularly during the 20-29-year age period, adjusted for num-
bers of sunburns and sunbathing vacations, was statistically sig-
nificantly associated with melanoma risk.
The incidence of melanoma observed in our study was higher
among the Norwegian women than among the Swedish women.
The crude incidence rates of melanoma, which we calculated
from the data presented in Table 1, were 25.8 cases per 100000
person-years of follow-up for the Norwegian women and 16.6
cases per 100000 person-years of follow-up for the Swedish
1534 ARTICLES Joumal of the National Cancer Institute, VoL 95, No. 20, October 15, 2003
0
0
::::
g
c.
"' c.
a
3
0
::::
Table 3. Relative risks (RRs) and 95% confidence intervals (Cis) of cutaneous malignant melanoma according to annual number of
sunburns during different age periods*
Frequencies,
Age period and number of sunburns No.(%) No. of cases Age-adjusted RR (95% Cl) Multivariable RRt (95% Cl)
I 0-19 years (n = 95 472)
0 2 1 747 (23) 22 1.00 (referent) 1.00 (referent)
52452 (55) 94 1.80 (1. 13 to2.86) 1.64 ( 1.03 to 2.62)
21273 (22) 55 2.70 ( 1.65 to 4.44) 2.42 ( 1.46 to 4.02)
P,rend<.001 P.,
0
,w<.00 I
20-29 years (n = 97 442)
0 20346 (21) 28 1.00 (referent) 1.00 (referent)
58 458 (60) 102 1.29 (0.85 to 1.96) 1.24 (0.81 to 1. 88)
18638 (19) 43 1.76 (1.09 to 2.84) 1.69 (1.04 to 2.76)
p<rcnd = .02 p<rcnd = .03
30- 39 years (n = 94 850)
0 30 588 (32) 48 1.00 (referent) 1.00 (referent)
54 199 (57) 99 1.15 (0.82 to 1.63) 1.15 (0.81 to 1.62)
10 063 (11) 27 1.71 (1.07 to 2.74) 1.71 (J.06to 2.76)
p<rend = .04 P,rend = .05
40-49 years:t: (n = 45 269)
0 20031 (44) 43 1.00 (referent) 1.00 (referent)
22 260 (49) 44 0.92 (0.61 to 1.41) 0.92 (0.61 to 1.41)
2978 (7) 6 0.94 (0.40 to 2.21) 0 96 (0.41 10 2.27)
p<rcnd = .74 P,rend = .77
Combined, 10-39 years (n = 90633)
1/ycar, I 0- 39 years 64807 (72) 99 1.00 (referent) 1.00 (referent)
20- 29 years and/or 30-39 years 5873 (6) 13 1.4 7 (0.82 to 2.62) 1.54 (0.86 to 2.75)
10-19 years 7357 (8) 20 1.82 (1.13 to 2.95) 1.66 ( 1.02 to 2.70)
10- 39 years 12 595 (14) 34 1.83 (1.24 to 2.70) 1.79 ( 1.20 to 2.68)
Ptrerld<.OOl P, rend = 002
*Poisson regression analysis. All statistical tests were two-sided.
tMultivariable models included attained age, region of residence, and hair color.
*Included only women who were aged 40 years or older when answering the questionnaire.
women. These incidence rates are in accordance with crude in-
cidence rates reported for Norwegian and Swedish women for
1993 through 1997 (23.3 cases per 100000 person-years for
Norwegian women and 17.3 cases per 100000 person-years for
Swedish women) (3). Age-adjusted incidence rates of melanoma
have been consistently hi gher among Norwegian than among
Swedish women since the 1960s.
We observed a strong association between hair color and
melanoma risk but not between eye color and melanoma risk.
These results are consistent with results of a pooled analysis of
data derived from published case-control studies, in which the
reported relative risks were 2.38 (95% CI = 1.90 to 2.97) for
individuals who have red hair compared with those who have
black or dark brown hair and 1.55 (95% CI = 1.35 to 1.78) for
individuals who have blue eyes compared with those who have
brown eyes (12). However, the association we observed between
cutaneous sensiti vi ty to the sun (i. e., burning or tanning) and
melanoma risk was much weaker than that reported in a retro-
spective Australian study (I 8). Our findings, that hair color but
not eye color was statistically significantly associated with mela-
noma risk, agree with those of two Danish case-control studies
(19,20): in addition, the association between melanoma risk and
cutaneous sun sensitivity reported in those two studies was also
much weaker than that for hair color. A Swedish case-control
study (21) also found that hair and eye color and skin type were
statistically signi ficantly associated with melanoma risk, al-
though the associations were considerably weaker for eye color
and skin type than for hair color, whereas an early Norwegian
case-control study (22) that used hospital-based control subjects
found that tolerance to sun exposure, but not hair or eye color,
was associated with melanoma risk. We speculate that hair color
may be the best measure (combining accuracy of measurement
and predictive capacity) of sun sensitivity in homogeneous fair-
skinned populations, such as those of Scandinavia. By contrast,
reported sun sensitivity may be a less reliable measure of sun
sensitivity in these populations because it depends on an indi-
vidual's experience with repeated and quite heavy sun exposure,
which many Scandinavian subjects may not have.
In agreement with the results of several case-control studies
(23- 25), the results of our cohort study show that the number of
asymmetric nevi larger than 5 mm on the legs was the strongest
host risk factor for melanoma. The participants self-reported
such nevi on their legs, guided by color pictures of dysplastic
nevi in a brochure that was encl osed with the questionnaire. The
method we used for this self-reporting has been shown to have
limited accuracy for the diagnosis of one or more dysplastic
nevi, with an estimated sensitivity of 29% and a specificity of
85% (26). Hence, the relative risk of 5.3 for melanoma in the
presence of seven or more large nevi on the legs that we ob-
served in our study may underestimate the excess risk. Increased
surveillance and more frequent excision of suspected lesions
might, on the other hand, spuriously inflate the risk of melanoma
among subjects with asymmetric nevi. However, such an effect
seems unlikely because all incident cases were histopathologi-
cally confirmed invasive malignant melanomas.
Our results confirm the positi ve association between past his-
tory of sunburn and melanoma reported previously by the ma-
jority of case-control studies (9,10). Our effect estimates were
higher for sunburns that occurred during adolescence than for
those that occurred later in life; however, it may be too early to
Journal of the National Cancer Institute, Vol. 95, No. 20, October 15, 2003 ARTICLES 1535
0
0
::::
g
c.
"' c.
a
3
0
::::
Table 4. Relative risks (RRs) and 95% confidence intervals (Cis) of cutaneous malignant melanoma according to the average number of
weeks per year spent on sunbathing vacations to southern latitudes or within Norway or Sweden during different age periods*
Frequencies,
Age period and annual weeks on sunbathing vacation No.(%) No. of cases Age-adjusted RR (95% Cl) Multivariable RRt (95% C1)
10-19 years (n = 93418)
0 45 298 (48) 77 1.00 (referent) 1.00 (referent)
I week/year 19 921 (21) 35 1.10 (0.74 to 1.65) 1.21 (0.80 to 1.83)
2- 3 weeks/year 20086 (22) 32 1.02 (0.67 to 1.54) 1.09 (0.71 to 1. 65)
;;;.4 weeks/year 8113 (9) 20 1.56 (0.95 to 2.55) 1.67 (1.01 to 2.74)
ptrend = .22 P,,.,," = .12
20-29 years (n = 96 029)
0 26460 (28) 41 1.00 (referent) I .00 (referent)
I week/year 28 723 (30) 55 1.28 (0.85 to 1.92) 1.36 (0.90 to 2.05)
2-3 weeks/year 32 997 (34) 53 I .08 (0.7 1 to I .62) I . 13 (0.74 to I .70)
;;;.4 weeks/year 7849 (8) 19 1.67 (0.96 to 2.88) 1.79 ( Ul3 to 3. I 1)
P,,..,J = .26 P., .. ," = .18
30-39 years (n = 93 845)
0 24 293 (26) 33 1.00 (referent) 1.00 (referent)
I week/year 28 858 (3 I) 56 1 .42 (0.93 to 2. 19) 1 .49 (0.97 to 2.30)
2- 3 weeks/year 33 144 (35) 65 I .43 (0.94 to 2.18) 1.45 (0.95 to 2.21)
;;;.4 weeks/year 7550 (8) 16 1.56 (0.86 to 2.84) 1.63 (0.89 to 2.97)
pttend = .10 P,,.,," = .08
40-49 years:t: (n = 45 21 1)
0 13806(31) 23 I .00 (referent) 1.00 (referent)
l week/year 12801 (28) 36 1.70 (1.01 to 2.87) 1.87 ( 1.11 to 3.18)
;;;.2-3 weeks/year 18 604 (41) 31 1.01 (0.59 to 1.73) 1.06 (0.61 to 1.81)
ptrend = .87 pto-end = .98
Combined, 10-39 years (n = 88 450)
0, 10-39 years 15799(18) 2 1 1.00 (referent) 1.00 (referent)
;;;. I week/year, 20-29 and/or 30- 39 years 27851 (31) 53 1.42 (0.86 to 2.36) 1.45 (0.87 to 2.40)
;;;. I week/year, I 0-19 years 1751 (2) 3 1.37 (0.4 I tO 4.59) 1.46 (0.43 to 4.92)
;;;. I week/year, I 0-39 years 43 049 (49) 79 1.44 (0.89 to 2.34) 1. 56 (0.95 to 2.56)
P,,..," = .27 P trend = .13
*Poisson regression analysis. All statistical tests were two-sided.
t Multivariable models included attained age, region of residence, and hair color.
*Included only women who were aged 40 years or older when answering the questionnaire.
Table 5. Relative risks (RRs) and 95% confidence intervals (Cls) of cutaneous malignant melanoma according to solarium usc during different age periods*
Frequencies,
Age period and solarium use No.(%) No. of cases Age-adjusted RR (95% CJ) Multivariable RRt (95% CJ)
10-19years(n = 85 847)
Never 84 182 (98) 152 1.00 (referent) 1.00 (referent)
Rarely or ;;;. I time/month 1665 (2) 4 1. 65 (0.61 to 4.47) 1. 52 (0.56 to 4. 1 2)
p = .36 p = .44
20-29 years (n = 89 142)
Never 71 133 (80) 123 1.00 (referent) 1.00 (referent)
Rarely 11618 (13) 19 1.16 (0.70 to 1.92) Ill (0.67 to 1.85)
;;;. I time/month 6391 (7) 18 2.32 ( I .35 to 3.99) 2.58 ( 1 .48 to 4 50)
P,,..,"" = .009 P,,...
0
= .006
30-39 years (n = 87 890)
Never 44338 (50) 78 1.00 (referent) 1.00 (referent)
Rarely 28 383 (32) 51 I .03 (0.72 to 1.48) 0 93 (0.64 to 1 .34)
;;;. I time/month 15169(17) 36 1.40 (0.93 to 2.10) 1.42 (0.93 to 2.16)
P<rend = .15 Ptr<nJ = .19
40-49 yearst (n = 41 409)
Never 17 345 (42) 27 1.00 (referent) 100 (referent)
Rarely 145 14 (35) 33 1.46 (0.88 to 2.43) 1 .39 (0.82 to 2.33)
;;;. I time/month 9550 (23) 22 1.48 (0.84 to 2.60) 1.67 (0.93 to 2.99)
P., . .,, = .14 pmmd = .08
Combined, 10-39 years (n = 79 616)
Never/rarely. 10-39 years 65239 (82) 111 1.00 (referent) 100 (referent)
;;;. I time/month I 0-19, 20-29, or 30-39 years 14 377 ( 18) 34 1.45 (0.98 to 2.14) 1.55 ( 1.04 to 2.32)
p = .07 p = .04
*Poisson regression analysis. All statistical tests were two-sided.
t Multivariable models included attained age, region of residence, hair color, and the corresponding number of age-specific sunburns and weeks on annual summer
vacations.
only women who were aged 40 years or older when answering the questionnaire.
1536 ARTICLES Joumal of the National Cancer Institute, Vol. 95, No. 20, October 15, 2003
0
0
::::
g
c.
"' c.
a
3
see the full effect of sunburns later in tife in our cohort of
women. Systematic reviews of case-control studies ( 10,11) have
not found evidence of an overall stronger effect of sunburns in
early life than in later life. Furthe1more, the rep011ed dose-
response gradients of melanoma risk with frequency of sunburn
were comparable during childhood and adulthood in a recent
large multicenter case-control study from Europe (27). How-
ever, it is possible that the case- control studies have underesti-
mated the effects of sunburn during childhood and adolescence
because of high recall error from the very long recall period for
most subjects. All of our study subjects were younger than 50
years when they answered the questionnaire, giving a shorter
recall period than in many case-control studies (9) that include
subjects up to 70 years old or older.
Sun exposure during sunbathing vacations is usually intense
and intermittent, and results of previous case-control studies
( 10) suggest that there is a positive association between the
incidence of melanoma and hi gh levels of intermittent sun ex-
posure. We recorded the number of sunbathing vacations in
Norway and Sweden (at latitudes higher than 58 N, where UV
levels are low, even in summer) and those in southern latitudes
in the same variable, which may explain the lack of a strong
association between sunbathing vacations and melanoma in our
study. Previous Scandinavian studies show inconsistencies in
their results on sunbathing and melanoma risk. One Swedish
study (21) and a Danish study (28) found associations between
vacations spent in sunny places and melanoma risk, whereas
another Swedish study (29) did not.
Our results provide stronger evidence than those of other
studies that solarium use is associated with an increased risk of
melanoma; we found that overall, regular (i.e., one or more times
per month) solarium use at any age was associated with a sta-
tistically significant 55% increase in risk of melanoma after
adjustment for sun sensi tivity and measures of sun exposure.
Although other studies (30-34) have reported positive associa-
tions between melanoma risk and exposure to artificial UV light,
these associations often apply to specific subgroups of the study
population (e.g. the youngest subjects with melanoma), or they
have not been adjusted for possible confounding with sun ex-
posure. A recent review (35) concluded that there was insuffi-
cient evidence to determine whether or not tanning lamps cause
melanoma. The more consistent and overall statistically signifi-
cant association between melanoma risk and solarium use ob-
served in our study, which may be due to the relative youth of
our cohort, adds substantially to the existing evidence that arti-
ficial UV light for recreational tanning increases fisk of melanoma.
Our study has several important strengths. First, because aU
physicians, hospital departments, and histopathologic laborato-
ries in Norway and Sweden are obliged to report malignant
diseases to the cancer registries, and the cancer registries match
regularly against the death registers at Statistics Norway and
Statistics Sweden, respectively, we had a complete follow-up
and histopathologic confirmation of all incident cases of mela-
noma. Second, our study had a prospective design, such that
detailed infonnation on host factors and sun exposure was col-
lected prior to melanoma diagnosis. Error in measurement of
these factors is inevitable in epidemiologi c studies of skin cancer
(26,36,37) but can be assumed to be non-differential in the pres-
ent study. By contrast, measurement error in case-control stud-
ies may be intluenced by a diagnosis of skin cancer and therefore
may differ in degree between cases and controls (15,16).
Among the limitations of our study were the comparatively
small number of cases, the limited detail about the exposure
measurements, and the relatively short follow-up petiod for solar
and artificial UV light exposure during midlife. In addition, we
did not adjust for the multiple comparisons made in this study.
Instead, we chose to eval uate the individual associations on their
own merits and with respect to results from prior studies. Fi-
nally, because our cohort included only women, our results may
not be generalizable to both sexes. In Norway and Sweden,
incidence rates of melanoma tend to be slightly higher among
women than among men (3). However, previous case- control
studies (9) have not focused on whether there are sex differences
in the associations between pigmentation characteristics or sun
exposure and the risk of melanoma.
The results of our cohort study suggest that public health
recommendations for melanoma prevention should include a
combination of information on inherent predisposition and the
effects of exposure to UV radiation. Hair color and large asym-
metric nevi on the legs were the most important host factors
associated with ri sk, and our results for sunbum, sunbathing
vacations, and use of a solarium support current recommenda-
tions for the avoidance of UV exposure, especially intermittent
exposure, either from natural or from artificial sources. Al-
though our smdy cohort is still too young to fully assess whether
UV exposure during adolescence is more critical than UV ex-
posure during adulthood for melanoma risk, there is great po-
tential to explore this question and the important issue of inter-
actions between risk factors in future follow-up studies of these
Norwegian and Swedish women.
REFERENCES
(1) Parkin MD, Pisani P, Ferlay J. Estimates of the worldwide incidence of 25
major cancers in 1990 Tnt J Cancer 1999;80:827-41.
(2) Ferlay J, Bray F, Pisani P, Parkin DM. GLOBOCAN 2000: cancer inci-
dence, mortality and prevalence worldwide. Version 1.0. lARC Cancer-
Base No. 5. Lyon (France): IARC Press; 2001.
(3) B, Fekjaer H, Hakulinen, T, Tryggvad6ttir L, Storm HH, Talback
M, et al. Prediction of cancer incidence in the Nordic countries up to the
year 2020. Eur J Cancer Prev 2002; I I Suppl I :S 1-96.
(4) Armstrong BK, English DR. Cutaneous malignant melanoma. ln: Schot-
tenfeld D. Fraumeni IF Jr, editors. Cancer epidemiology and prevention.
2nd ed. New York (NY): Oxford University Press; 1996. p. 1282-312.
(5) Green A, Trichopoulos D. Skin cancer. In: Adami HO, Hunter D, Tricho-
poulos D. Textbook of cancer epidemiology. New York (NY): Oxford
University Press; 2002. p. 281- 300.
(6) Eklund G, Malec E. Sunlight and incidence of cutaneous malignant mela-
noma. Effect of latitude and domicile in Sweden. Scaod J Plast Recoostr
Surg
(7) Magnus K. Incidence of malignant melanoma of the skin in Norway,
1955- 1970. Variations in time a11d space and solar radiation. Cancer 1973;
32:1275-86.
(8) Armstrong BK. Melanoma of the skin. Br Med Bull 1984;40:346-50.
(9) International Agency for Research on Cancer (IARC). !ARC monographs
on the evaluation of carcinogenic risks in humans. Vol. 55. Solar and
ultraviolet radiation. Lyon (France): IARC; I 992.
{10) Elwood JM, Jopson 1. Melanoma and sun exposure: an overview of pub-
lished srudies. Tnt J Cancer 1997;73: 198-203.
(II) Whiteman DC, Whiteman CA, Green A C. Childhood sun exposure as a
risk factor for melanoma: a systematic review of epidemiologic studies.
Cancer Causes Control 200 I; 12:69- 82.
{12) Bliss JM. Ford D, Swerdlow AJ, Armstrong BK, Cristofolini M, Elwood
JM, et al. Risk of cutaneous melanoma associated with pigmentation char-
acteristics and freckling: systematic overview of I 0 case-control studies. Int
J Cancer 1995;62:367- 76.
Journal of the National Cancer Institute, Vol. 95, No. 20, October 15, 2003 ARTICLES 1537
0
0
::::
g
c.
"' c.
a
3
0
::::
(13) Weinstock MA, Colditz GA, Willett WC, Stampfer MJ, Bronstein BR,
Mihm MC, et al. Moles and site-specific risk of nonfamilial cutaneous
malignant melanoma in women. J Natl Cancer Inst 1989:81:948-52.
(14) Weinstock MA, Colditz GA, Willett WC, Stampfer MJ, Bronstein BR,
Mihm MC, et al. Nonfamilial cutaneous melanoma incidence in women
associated with sun exposure before 20 years of age. Pediatrics 1989:84:
199- 204.
( I 5) Weinstock MA, Colditz GA, Willett WC, Stampfer MJ, Rosner B, Speizer
FE. Recall (report) bias and reliability in the retrospecti ve assessment of
melanoma risk. Am J Epidemiol 1991;133:240-5.
( 16) Cockburn M, Hamilton A, Mack T. Recall bias in self-reported melanoma
risk factors. Am J Epidemiol 2001;153: 1021-6.
(17) Geigy scientific tables. Vol. I. Units of measurement, body fluids. com-
position of the body, nutrition. 8th ed. Basel (Switzerl and): Ciba-Geigy;
1981. p. 227.
(18) Holman CD, Armstrong BK. Pigmentary traits, ethnic origin, benign nevi,
and family history as risk factors for cutaneous malignant melanoma. J Nat!
Cancer Inst 1984;72:257-66.
(19) 0sterli nd A, Tucker MA. Hou-Jensen K, Stone BJ, Engholm G. Jensen
OM. The Danish case-control study of cutaneous malignant melanoma. I.
Importance of host factors. lnt J Cancer 1988;42:200-6.
(20) Lock-Andersen J. Drzewiecki KT. WulfHC. Eye and hair colour. skin type
and constituti ve skin pigmentation as risk factors for basal cell carcinoma
and cutaneous malignant melanoma. A Danish case-control study. Acta
Derm Venereol 1999;79:74-80.
(21) Beitner H, Norell SE, Ringborg U, Wennersten G, Mattson B. Malignant
melanoma: aetiological importance of individual pigmentation and sun ex-
posure. Br J Dermatol I 990; I 22:43-51.
(22) Klepp 0, Magnus K. Some environmental and bodily characteristics of
melanoma patients. A case-control study. lnt J Cancer 1979;23:482- 6.
(23) Augustsson A, Stiemer U, Rosdahl I, Suurkula M. Common and dysplastic
naevi as risk factors for cutaneous malignant melanoma i.n a Swedish
population. Acta Derm Venereol 1991;71:518-24.
(24) Tucker MA, Halpern A, Holly EA, Hartge P, Elder DE, Sagebiel RW, et al.
Clinically recognized dysplastic nevi. A central risk factor for cutaneous
melanoma. JAMA 1997;277:1439-44.
(25) Bataille V, Grulich A, Sasieni P. Swerdlow A. Newton Bishop J. McCarthy
W, et al. The association between naevi and melanoma in populations with
different levels of sun exposure: a joint case-control smdy of melanoma in
the UK and Australia. Br J Cancer 1998;77:505- 10.
(26) Titus-Ernstoff L, Thorn M, Tosteson TD, Brahme EM, Yuen J, Baron JA,
et al. The accuracy of skin self-examination for atypical nevi. Epidemiol-
ogy 1996;7:619-23.
(27) Pfahlberg A, Kolmcl KF, Gcfeller 0 ; FEBlM Study Group. Timing of
excessive ultraviolet radiation and melanoma: epidemiology docs not sup-
port the existence of a critical period of high susceptibility to solar ultra-
violet radiation-induced melanoma. Br J Dermatol 2001 ;144:471-5.
(28) 0sterl ind A, Tucker MA, Stone BJ, Jensen OM. The Danish case-control
study of cutaneous malignant melanoma. II. Importance of UV -light expo-
sure. Lnt J Cancer 1988;42:319- 24.
(29) Westerdahl J. Olsson H, Ingvar C. At what age do sunburn episodes play
a crucial role for the development of malignant melanoma. Eur J Cancer
1994;30A: 1647-54.
(30) Swerdlow AJ, Engl ish JS, MacKie RM. O' Doherty CJ, Hunter JA, Clark J,
et al. Fluorescent lights, ultraviolet lamps, and risk of cutaneous melanoma.
BMJ 1988;297:647-50.
(3 I) Walter SD, Marrett LD, From L, Hertzrnan C. Shannon HS. Roy P. The
association of cutaneous mal ignant melanoma with the use of snnbeds and
sunlamps. Am J Epidemiol 1990;131:232-43.
(32) Autier P, Dore JF, Lejeune F, Koehne! KF, Geffeler 0, Hille P, et al.
Cutaneous malignant melanoma and exposure to sunlamps or sunbeds: an
EORTC multicenter case-control study in Belgium, France and Germany.
lnt J Cancer 1994;58:809-13.
(33) Westerdahl J, Olsson H, Masback A, lngvar C, Jonsson N, Brandt L, et al.
Use of sunbeds and sunlamps and malignant melanoma in southern Swe-
den. Am J Epidemiol 1994;140:69.1-9.
(34) Westerdahl J, Tngvar C. ~ s b a c k A. Jonsson N, Olsson H. Risk of cuta-
neous malignant melanoma in relation to use of sunbeds: further evidence
for UV-A carcinogenicity. Br J Cancer 2000:82:1593- 9.
(35) Swerdlow AJ, Weinstock MA.. Do tarming lamps cause melanoma? An
epidemiologic assessment JAm Acad Dermatol 1998;38:89- 98.
(36) Westerdahl J, Anderson H. Olsson H, l ngvar C. Reproducibility of a self-
administered questionnaire for assessment of melanoma risk. lnt J Epidc
miol 1996:25:245- 51.
(37) English DR. Armstrong BK. Kricker A. Reproducibility of reported mea-
surements of sun exposure in a case-control study. Cancer Epidemiol Bio-
markers Prev 1998;7:857-63.
NOTES
In Norway, the sur vey was s upported by Public Health Service grant CA-
52449 (to Professor E. Lund) from the National Cancer Institute. National In-
stitutes of Health. U.S. Department of Health and Human Services; granLS 90050
and E 00065 from the Norwegian Cancer Society; and grants from the Aakre
Foundation. ln Sweden, the survey was supported by the Swedish Counci l for
Planning and Coordination of Research, the Swedish Cancer Society. Organon,
Pharmacia. Medical Products Agency. and Scheri ng-Piough.
Manuscript received February 20, 2003; revised May 20, 2003; accepted
August 21,2003.
1538 ARTICLES Joumal of the National Cancer Institute, Vol. 95, No. 20, October 15, 2003
0
0
~
::::
g
c.
"' c.
a
3
..
nt' the Amenun C.:.llg nf Co.rdinlng:r
It) hr thr A:nctjc:tn C..U9.<u af Caul.inltlgy Fc:w.dation
t'uhll.<hcd hy Eln.-vior bl<!.
Vitamin D Deficiency
An Important, Common
7
and Easily
Treatable Cardiovascular Risk Factor?
Vol 52, Na. 21, 200l!
ISSN 07351097/081$34.00
doi:lO. 1016(j,j3cc.1008.09.050
John H. Lee, MDt James H. O'Keefe, MD, David Bell, MD,t Donald D. Hensrud, l\IID, MPH,:f:
Michael F. Holick, MD, PHD
Kansas City. Missottri, Birmingham, Alabama; Rochester, l'V!irmcsota.: and Boston, Massachuutts
Vitamin 0 deficiency Is s highly prevalent condition, prosont in approximately 30% to 50% of lha ganerol popula-
tion. A growing body of dotn suggests !hill low 0 lovols may
health. Vitamin D deficiency activates the system and can predispose to hyperten
slon and left vontrloulilr hypertrophy. Additionally. vitamin D deficiency cousos on inercilSO In pornthyrold hor-
mone, which increases insulin raslstoneo ond is ossociotod with diilbotos, hypertension, ond in-
cardiovascular risk. Epidemiologic studies hOve iJSSOclated low 0 levels with coronary
rnctors and adverse cardiovascular outcomes. Vitamin 0 svpplementlltlon Is simple, safe, and IneXPensive.
Lurgorundomized controlled trials are needed to firmly establish the relev<Jnce of vltnmln 0 status tl;) oardlovas
c:ular health. In tha moilnwhllo, monitoring serum 25hyaroxyvltamin o lovols Md correction of vtttlmin o dofJ-
clency Is Indica tad tor optlmlz;.,tlon of musculoskeletal and general (J Am Col! 2008;52:
1949-56) 2008 by tho Am orlean College of Cardiology Found!ltlon
Traditionally, vltamin D has been associated
bone healrh, and it is well tmdcrstood that vitamin D
deficiency lends to rldcct.c; in children nnd osteomalacia and
osteoporosis in adults (l). Howeve.r, it i.s now known
adequate vitamin D status is important for optimal function
of many organs and tissues throughout rhe body, including
the cardiovascular (CV) system (2). Vimmin D receptors
(VDRs) arc present on :1 L'trge variety of cell types, including
myocyret;, ca.rdioroyocytcs, pnncrc<ttic vuscular
e'ndothelial cells, neurons, immune cells, and osteoblast:; (1).
Vitamin D deficiency or insufficiency prevalent in prac-
tically every segment of the U.S. populacioflt including
children and young adults (f). This worldwide pandemic
. remains generally Wliccogn i.7.e.d and untreated.
Evolving dttt:.\ indicate that vltamin D deficiency is
playing an important role in the: genesis of coronary risk
and CV disease:. Vitamin D deficiency seems to
predispose: to hypertension, cliahetes and the metabolic
syndrome, left ventricular hypertrophy, congestive heart
fiillure, and chronic vascular inflammation (1,2). Epidemi-
Vro"l the MJd lkut ln;titutr uml uf Mi..auri, K.1m1 City,
Mi>IJ,lllri: Emlocrinofnc;y, AJp\r.lmr.; Clinic, Roch-
<tcr,IIMinn"r.ot..; 2nd !iB<,."tt>n University Mcdic:\1 Center, ilonon, Mnmchuscm.
Dr. O'Keefe is nn unpnid 5cic:ntitlc COtHultant tu C""ilii)Tb. Fulldl derived from tllis
comp:111y Ate \l!cd for tnarkcring :md potlr.nr CRrdinvuculr Con.,.ltunt<,
tbe I;IOUp vrJCUCC ><ith which Or. O' Kectc lt Dr.. Holi,;lc i p
fur thr Nut:ional Dairy C<luncU me UV 1-'oundntiQn.
Mltnwt:ript receit ... d Jup. 4, 7.006; rc:viaed 111111\llctipr recdl'td 6, 20011,
=.prr,.d Augur 13, '-OOS.
ologic :;cudi!!s have also recently linked vitamin D deficiency
with incrensed risk of mu.jor adverse CV cvco.ts (3). A study
of male health professionals showed a 2-fold risk of myo-
cardial infi\rction (Ml) in t>ubjects who were: vitnolin D
deficient compared with those in the range (4).
Similarly, a rc:cent prospectiw cohort study measured the
vitanlin D levels in 3,258 German adults who were under-
going elective cardiac cathe[en7.ation. During a mean
follow-up of7.7 years, indiv.idullls in the lowest quartile for
baseline serum 25-hydroxyv.ita.rnin D [25(0H)D) had a
risk-adjusted 2-fold increased risk of death, especially CV
death, cornpar.ed with those in the highest of
vit11.mi.n D (5).
This review focuses on the relatlonship between 2 wide-
spread problems: v.itanlin D deficiency and CV disease. The
i.ssues addressed will include:: 1) the: role of vitamin D
deficiency in the genesis of coronary risk factors and adverse
CV 2) how repletion of v.immi n D stores may
improve CV health and prognosis; and 3) practical :tnd
specific for restoring i\nd maintaining a
healthy vi.tumin D in pnticnts, because no
guidelines have been published on this topic yet.
VItamin D Baslc:s
Vitamin. D comes in 2 forms: vita.min D
2
(ergocalciferol)
nnd D
3
(cholecnlciferol). Vitamin Dz, found in
plants
1
is the propuct ofuhraviolct B (UVB) (290 ro 315
mm) irradiation of and cnn. be consumed as
19so
Vltlmln D Doficiency and CV Risk
Abbrc:vJ;:,tJons
:u1d Acronyms
:Z$-
0
c::v .. catdrava. culJtr
Ml = III)GC8 rdllll Jnlatetlan
IIV8 Ultnlllfalat 9
11tm 1.4tamln D >c:captor
a supplement or in fortified
foods (1). Vitamin D
3
, a prod-
uct of UVB irradiation of 7-
is synthe-
in the human epidermis or
consumed in the form of oily
fish, fortified foods, or a :;upplc-
mc:nt. Excessive sunlight
sure c:mnot vitamin D tox-
icity because UVB
ccccss virom.i.n to biologically
ioen isomers (l); ho\vcver, QCccs-
sive oml \':it:unin D intake can cnuse toxicity at very high
doses (6).
Vitamin 0 is converted in the liver to 2S(OH)D, which
is t:he major circulating metabolite of vit:un.in D. Serum
25(0H)D concentrations, which reflect both vitamin D
inrnke nnd endogenous producti.on, should be measured to
clinic:illy :tsscss vitamin D status (1). In the kidney,
25(0H)D is by lcr-hydroxylase to its active form,
1,25-dihydroxyvit:unin D [1,25(0H)
2
D], which n
vit-.11 role in maintnining boac and health by regu-
lating calcium metabolism. Although 1,25(0HhD is the
active form of vitamin D, it& serum level docs not cortelate
with over:ill vitamin D stntus and thus is generally not
clinically lL<ieful. (1).
Vitamin D in the form of 1,2S(OH)p is a hormone,
because it ic; produced primarily in 1 orgnn (the kidney) and
chen circuhttc.c; throughout the body, where it c.xerts wide-
ranging effects. The VDR is present in mosr: til;sues,
including endodtelium, vasc:nl:lr smooth mut;de, :tnd myo
C.'U'dium (2). In nddition, both vasc:ulM smooth muscle and
endothc.li:U cells may have the ability to convert 25(0H)D
to 1,25(0HhD (7). Circulatory 1,2S(OH)
2
D crosses the
cell and cytoplasm tU1d reaches the nucleus,
where it to the VDR. The VDR-bound 1,25(0H)
2
D
in turn binds to the retinoic acid x-rcceptor and serves u.s a
nuclear tronscription fuctor, altering gene function and
inducing protein synthesis (1). Directly or indirectly,
1,25(0H)
2
D regulates over 200 genes, including those
involved in renin production in the kidney, in!\ulin produc
cion in the: p:mcn:as, release of cytokincs .&om lymphocytes,
production of cathclicidin in and growth nnd
proliferation of both vascular smooth muscle cell!1 and
cardiomyocytes (1).
Definition and Prevalence of Vrtamln D Deficiency
Although a consensus regarding the optimal level of serum
25(0H)D has not yet been established, most e.\.-pe.tts define
vitamin D deficiency a 25(0H)D level of <20 nglml (50
nmoVl) and -+itarnin D in:;ufficiency as 21 to 29 ng/ml.
(Table 1). For all studied end points to d11.te, the optimal
concentncion of .lS(OH)D is at lenst 30 ng/ml (8).
A rapidly evolving knowledge base indicates that vitamin
D deficiency is mucl1 more prcvnlcnt thlln previously rec:-
JACC Vol. 52, No. 24, 2008
December 9,
ognizcd and is prese.tu in up tc> SO% of young adult!l (9) and
a.pparemly healthy childrer'l (1), 'lhe Third Nation:U. Health
and Nutrition Examination Survey (NHANES In) re-
ported the prevalence of vitamin D deficiency in the U.S; to
be between 25% and 57% of adults (10).
The prevalence of vitamin D deficiency increases in
proportion to distance from the equ.'\tor because of increased
atmospheric filtering of UVB radiation caused by the
oblique :mgles of the lt-un's rays at higher latitudes. Addition-
ethnic groups with slcin require proportionally mon:
!>1Jn o..-po!>urc to equiV'..tl.cnt :J..!llOWlt<; of vitun.in D
compared with people with lighter skin (11).
Modern humnn cultures produce less vitamin D cutane:-
ously, in part because of increasingly indoor lifestyles and
cffons to minimize sun c::.:>..-po:;u.rc by using and
other sua avoidance strategies. Sunscreen with u sun pro-
tection fac:ror of 15 blocks 99% of the
cut:IJ\eous vimmin D production (12). AdcUtiontill.y, obesity
is associated with vifll.mjn () deficiency (13), probably
because of a dec:rcascd bioav.Wability of vitamin D that is
sequestered in the fat of indivi duals \vith C."<CeSS adipose
(14). After equivalent to UVB radiation or a
do!'e of vitamin D:
11
obese individuals showed 50%
lower blood levels of vitamins D
3
und D
2
compared with
nonobesc individuals, probably because of scque<;tcring of
25(0H)D in adipose tissue (14). Older age also reduces the
capacity for U\fB-induced cutaneous syntheSis of vitamin
D. After equal doses of runl.ight C);posure, a 70-year-old
person produces 75% less vitamin D
3
than a 20-yeru:-old
person (15). Other risk factors for vit:u:n.in D deficiency arc
listed in Table 2.
VItamin D Deficiency and cv Disease
.Epidemiological studies report that the rates of coronary
heart diabetes, nnd
like vitamin D
deficiency, increase in proportion to increasing dist:mcc
from the equator (16). Defi.cienr or insuf!icitnr serum
25(0H)D lcvcls have been .documented in patients with
myocardial infarction (17)_. stroke (18), heart fiillure (2),
diabetic CV disease {19), and peripheral arterial disease
(20). Recendy, the rcL'\tionship between CV risk and
25(0H)D levels was explored among the 15,088 subject!:
from the NHANES Til national cohort registry. In this
study, 25(0H)D levels were: inversely asso-
ciated with hypertension, diabetes mdlirus, hypcrtriglycer-
idemia, and obesity (21). Other cross-sectional studies have
:ZS.Hydrol(Y'<twnln 0 (nVml)
lD-20
:U.-29
:::::30
>1!10
Vltllmln D S13hn
S1>\'l>n: ddicflongy
Toxic ley
JAC
De<
I
E
COl
hYJ
dcl
ccl
Or
D
red
stu
of
CXf
ens
fin,
So
J
seq
1,7
: . We!
obs
. bas
. yea
. nor.
. to!
. . 11lCI
; wa:;
.: Wit)
v
t, 2003
):and
ealth,
) re-
.S. to
:s .in
:ased
the
tion-
more
inD
::we-
and
:md
pro-
. the
: esity
>ably
at is
. ora
50%
with
Jg of
; the
unin
' -old
: -old
r are
. nary
nD
ance
.rum
wi.th
: (2),
case
and
jccts
tlus
sso-
cer-
lave
\D$
ney
' .
.. ; t ; . ... : . .. ; ... : ; . . t ' : ;.. .. .
Factors . .for Vltamln o.:nencroncy .: : .... , .. ; : .. .... ,
. ' f- '!: .... .,..\; .. ... .. .... . . ... ,.. . ' '
)motllutlon"lh:rd at homebound
? dist:once lrotn :<:qulllat
.....
WloterseMM
. >: C<>vcMJP cl otnlniC nnll/o;,,un&cre&n
... Aft ooltu\lon
::.-
""'!l+"" l ...
':. Mn!absol'l'tiD<I
Ronal dl5<:;>$0
.' llvOf df5Cl!SO
Me<lleatlons.: ,tllueocoi'\Jeold,, enllrejectlon, om! tillman
vfrus moctlcgtlon'
:corrfirmed the links bcrween vitamio D deficiency and b<1th
hypertension and diabetes (22,23). Additionally, vitrunin D
deficiency predisposes to insulin rt!Sistance, pancreatic beta
cell dyofunction (24), and the: metabolic :l)'lldrome (24,25) .
One reported that n daily intake of 800 ill of vitamin
D compared with a dailyintake of <400 JU of vitamin D
reduced the rilik of type 2 diabetes by cue-third (26). A
study of 10,366 Finnish children who were given 2,000 IU
of vitamin per day thr.oughout che first year of life
ocpccicncc:d a 78% reduced risk of type 1 diabetes over the
ensuing 31 years of follow-up (27). Subsequently, this
finding has been confirmed by a meta-analysis performed on
5 stuclies by t\ group in England (2S).
A co.rcd.ation between vitamin D deficiency and
sequent rn:1jor adverse CV events was found among the
1,739 Framingham Offspring Study participants- who
were free of CV di!iease at baseline: (3). In this prospective
ob!ien'lttional study, 25(0H)D levels were mca.-:urcd at
baseline and subjects were followed up for u rnenn of 5.4
years. The rate of a composite CV end point (fatal or
nonfntal MI, ischemia, stroke:, or heart f.lllure) was 53%
to 80% higher in people with low vitamin D levels. The
CV risk associated with vi. mmin D deficiency
w:1s m:1gnilied in the cohort of Frarningh1ttn offspring
.with hypertension (Figs. 1 and 2).
Vitamin D deficiency predisposes co up-regulation of the
rcnln-gngiotensin-aldosterone l>Y,item .il!ld hrpertrophy of
both the left ventricle and vascular smooth muscle cells {2)
(Fig. 3). In vitamin D- deficient anirnnls there is an in-
creased incidence of hypertc:n. 1on, left vc:ntricul\\r hypertro-
phy, and athetosc.lerosis (29). Human studies indic:\te that
1,25(0H)
2
D inhibits renin synthesis,, which may
blood pressure (30). Krause et al. (31} showed that incre:\sed
c:."Posurc to UVB radi.ation in a tanning bed 3 times per
week for 3 months led to a 18Ql!;b increase in 25(0H)D
levels and a 6-mm Hg reduction in both systolic and
diastolic A small, randomized, placebo-controlled
t;tudy of patients with type 2 diabetes and low baseline
25(0H)D levels showed thac a single dose of 100,000 IU of
vitamin D
2
reduced systolic blood pressure: by a mean of 1.4
Lee et al. .1951
Vlt11mln D Deficiency CV Rlsk
nun Hg and signifiumtly improved endothelial function as
measured hy forearm blood flow (32). J n the NHANES ill
study, the mean blood was about 3 mm Hg
lower in those in the individuals in the hlghest quincile of
serum 25(0H)D levels compnred with those in the lowest
quintilc (22) .
Hyperparathyroidism Increases CV
Chronic vitamin D deficiency causes secondary hyperpara-
thyroidism, which in turn may mediate many of the detri-
mental CV dfects of inadequate vitamin D lcvcb. The
A o.s r------------
0.251------------C.
Years
B o.a 1""'"""'----------
0 0.25 1---------------
t;
0
0.2 1----------------
j
Q.
'Iii
:;
E
::J
(.)
0.151--------------
26-(0HJ D !ovals< 'IS nglmL j ..
0.05 1-....;_....;.._ ___
2 3 4 5 6 7
Years
. D .. ':\
, .. . ': :: , . ,. . .. '\ t , . :;:,,. . . : . ,:
Vit:lmin D dllficlancy CV rlsk. CUM!& show 1110 orobabll
lty of m!l]or OCllhlrse CV ownts In partleloant& wlttl 2.!1(0H)O teii81S :::.1.5 nc:/mt
(lll'llon ttnoo) eno 2!S(OHJD l evets <15 ng,tmt (red nnea). Tile tncmesed cv
rtsk was more sppStent In pattanl!. wnn (A) In plstients wllhlllit (8) nype,..
tllnBIOil. Reprlnlt:d, With rtom Wang el. (3), 25(0H)O - 2.S.hy-
Ciroy;ttaonln o: cv =- CVD :o c:.ofdiov=,.cutor dlzc::osc:.
,.
1952
40
1.0
0
"" <D 1.2
a:
'0
5
0.8
"
:I:
OA
0.0
lee etsl,
V'lbmin D und CV Risk
10<15ngfmL
25 (OH) D Level
1.80
< 10 nglmL
. 1or: bvo.br. Vitimln:o
. . : . ,; . . . I . . . : . I: . . . .. ... : .. ..
odjustod hiiUII'II ratloa tor m'1)or udvors!t
CV Oom from wan, e1 al. (:l). Mlbrovliltloll!l as In Fi!lurc 1.
threshold for elevation of parathyroid hormone (PTH) is a
25(0H)D level of <30 ng/ml. Furcher decreases in
25(0I-I)D levels will rc.crult in proportionally higher PTH
levels to m:llnt:Un strum and total body calcium (Fig. 4).
Vimrnin D ddiciency reduces intestinal cnlcium nbsorption
by more than 5()1.){, (1). The attend'lT'It decrease in serum
calcium triggers PTI-I releasr;:, which quickly corrects
the calcium levd by mobili1.ati.on of cnlcium from bone,
renal tubular calcium reabsorption, t\ncl
rennl production of 1,25(0H)J).
JACC Vol. 52, No. 24, 2008
Oecemt>et 9, 2000:1949-56
The effects of prim:uy hypc:rparathyroidism on CV out-
come& were shown in a study th:tt reported approximately
40% lower relative rlsks of MJ
1
stroke, and death in patientS
who had surgic:U parathyroidectomy compared with obser-
vation (33). 'I11i:; UoJ.: between inCJ:e:tsc:d PTH and CV
disease was further corroborated by a. srudy of with
renal failure and necondnry hyperp:u-achyroidism by
decreltSed conversion of25(0H)D to 1,25(0HhDJ. In this
study, patients with a PTH levd 2::250 pg/mJ had a 2-fold
risk of CV compared with those with PTH
<250 pg/ml (34). Additionally, a recent obscrvntionnl study
found that c:lcv:ttcd PTH level-; in elderly individuals was
associated with a doubling of mortality during follow-up
compared with those with norm:U PTH levels (35),
An increased PTH level is with increases in
both blood pressure (36) and myocardial contractility, which
eventually lew to hypertrophy, apoptosis, and fibrosis of
both the left ventridc: nml vascular mcdinl smooth muscle
(2). Vit:\min D deficiency and/or increased P11-i also
prt:dib-posc to calcification of hel\rt v:tlvell, mitral annulus,
:md myocardium, especirllly in paticnt'l; wirl1 moderate or
severe chronic kidney (37).
Chronic kidm:y dilicasc is with markedly in-
creased CV risk (38), which may in part be mediated by
inlldequatc vitamin D lcvck Vitamin D deficiency is asso-
ci:ltcd wid1 increased mortality mtes in d1e Retting of chronic
kidney (39), and rcplcting vimmin D in such
parients improves outcomes. Recent observational srudies of
patients wich chronic lcidney dise-.1sc and
ism fo11nd that the oral admioisrration of 1,25(0H):J):l
- --------- -- - ----
:: _ .. .. ' :., j
r------t Vlremin.o t----..,
. ' . , .....
' ., .. \ .
- . \ .: , : , , ; , . I; , : ' ,; , ..1 , .'' ;: : ,
0 !' .... . . . .. . ' .. . :: . .
Po:;:;lblc m<!Cil&nl9nl' or tCVI nsl< rrcnt viu.mln 0 oonc1ency, PTH = pnruthyroid hormone: RM!:i - renin -'tl!!iotons/n;lldostr.ronc sy51om.
..
(:
<':
p.
p
tr
d:
OJ
tc
b(
(3
tit
ar
1,
rc,
0(
sy.
tic
of
m;
wi
Ot
A
COt
mt
det
bt]l
SUF
SUf
UlC
I, 200S
!49-56
.out-
.atcly
:icnts
bser-
CV
with
:d by
1 this
-fold
:rudy
W:J.S
H-up
'hich
is of
usele
.
ulu:;,
te or
'jt in-
d by
:\SSO-
:onic
such
es of
:oid-
)zD3
Jt<CC Vel. 52. No. 24. 2008
[)ecembcr 9, 2008:1949-56
.s
Ill
c
E
'tJ
0
l;;.
100
90
80
70
60
so
40
30
20
05 6-10 11-15 ll-2.5 26-30 >30
25-Hydro1tyv1Uimln D (ng/ml)
I!P. -o; < ::" :: :' :
. or a!l'd : : : . ! ..
The ln-..:rso: relotlonsnlp !l9twel!fl 5erurn o levels and serum
p=thylolo hcumone 1"--eH. Reprinto<l, wnn permission. ftOrn Z\ttr:w.,., ct ol. (2).
(also known liS activated vitamin D or cnldtriol) was
associated with signilicandy itnprovcd survival ( 40). A
placebo-controUed study of: 30 pre-dialysis renal fuilure
patients with !;econdacy hyperparathyroidism showed that
treatment with 1,25(0HhD
3
improved left vontrkul.nr
diastolic function (41). Vitunin D :malogs used in patients
on dialysis b1we been shown to improve survival at all
tested thus far { 42). ..
Low 25(0H).D level:; and incre:tSed PTH lcvdll increase
both inilammation and the risk of adverse CV events
(36). Vit:unin D deficiency increases systemic iofinrolmt-
tion, :lli documl!nted by elevated levels of C-rcactivc protein
and intcrlc:ulcin-10 (2). Furthermore, adnJinlstracion of
1,25(0HhD to vitamin D-deficic:nt individuals down-
regulated inflammatory markers (C-reaccive prorein, nnd so
on) and conferred an anti.prolifecative effect (43). E:rtr:u-cnnl
of 1,25(0HhD occurii through cytokinc stimula-
tion (7) and is locally important in the: paracrine regulation
of cellula.r growth, d.i1fcrentinrion, :md function {44). This
may explain why vitamin D deficiency has been assochtted
with type 1 di:lbcrc.s, cartcer, and multiple sclerosi.o; (45).
Out come Studies
A recent meta-analysis of 18 randomized controlled trials
comprising 57,000 individuals showed that a vitamin D
intake >500 ill/day improved all-cnusr: mort:1lity, in part by
decreasing CV dctlths (46). Moreover, the dati. rcg:u-cling
both efficacy and CV s:tfcty for vit.'U'Tl)n D nppellC to be
to thnt fur calcium supplements. Indeed, calcium
supplemeottltion ha.<; recently been implicated ns possibly
increasing d1e risk of adverse CV c:vents, particularly in
LM atl. 1953
Vlbmin D Dt!ficie"cy und C:V Risk
patients with chronic kidney clisense (47,48). Calcium sup-
plements acutely increa.c;e &rum calcium levels, which might
accelerate c.alcification (49). In cont:rMt, serum
vitamin D lc:vds arc inversely nssociated with coronRry
artery calcific.ation (50).
Ostl!oporosis and ad1crosclerotic CV disease share many
common risk factol'l>, and \1 pathologic link between these 2
highly prevalent age-related cliHeascs been suggested
{51). A latgc! number of midcllc-ngcd to elderly individuals
at risk for both CV disc:!Sc nnd osteoporosis may benefit
from therapies that nrc likely to improve both conclitions,
such as an anti-inflarnmarory diet, daily c:xc.rcise (especiallr
weight-bearing fu.rrm), avoidance of both tobacco :md heavy
alcohol inmke, and possibly vittmin D supplementation.
Vltantin D Myopathy
o.re genc:rnlly the fir.it manifestation of vitnmin D
deficiency. Severe: vir.mun D deficiency with correl>ponding
elevations of PTH were reported in 88% of 'women who
presented \vith muscle pams :md weakness (52). Another
study investigated 150 padenn; \vlth nonspecific musculo-
skeletal pains and reported that 25(0H)D levels were
insufficient in of individuals and severely deficient in
28% (53). A metn-malysis of 5 randomi7..ed clinical trials
reported that vitamin D supplementation reduced the risk
of .fitlls, mosr likely from improved muscle function and
strength (54). Mynlgia, the most common complaint
ported by patients on statin therapy, may be at in put
caused by undedying vitamin D dc.ficicncy. Anecdotally, we
have observed that repletion of 25(0H).I) levels predictably
improves or resolves statin-reh\ted myalgias.
Supplementing Vitamin D
Traditionally, up to 95% of the body's vitamin D
ment comes from the synthesis in the c:piderml!; on sun
exposure, with the remainder ingelited from dictaty sources
(Ta]Jlc: 3) (55). The U.S. government's current rccommen.-
dation for ornl '<itamin Dis 200 IU daily for individuals age
<50 years, 400 ru d.-illy for .between age 50 and
70 yeart>, [Uld 600 ru for those older than age 70
Studies indicate that the average U.S. adult consumes o.bout
230 ill vir:unin D pt!r. ch1y (56). However, ic has been
Food
Cod llnr oil, 1
illl mon, 3 oz
Farmed ""lmon, 3 oz
MQCICG!el, cooked, 3 o.
Tuna nSII, eennod In o!l, 3 w
San!lneJ (Willi on. 1 cu
Mllk. non!:Jt. lat. ana Ylllol&,
\Ol1;:tmfn o.fonlnad .L eul)
Oolol lrom Holick (1) tho tlollonnlln&dMe of H .. lth
IU per &crvf111i!
l 00-250
l4!S
:100
250
98.
'
l9S4 Lee et al.
Vitamin D DeficienCy and CV Risk
5(i
4l!
4(\
31
C'
.
"'
:!.! ...
16
R
0
0
l
Durutlnn ofVJ<mln D rupplcmaut.tdon (tnonlh.o)
,.: .. : .. . ::, .. .: .. !
-: .i: :;. ;d:, !
ttect or do9& ena dursuon or D supplomoounlon on tM mean
serum 25-llyarol<)"'il;ornio D [25(0HJDJ ooncontrauon acllleved. from Vieth
et st. (62),
estimated that 1,000 to 2,000 IU is oecc:ss:uy to satisfy the
needs for people (8). Mwy experts in the ficld
suggest the recommended daily intnkc: of vitn.min D be
incrc:ascd to at least 800 ro .2,000 IU of vitamin D daily,
doses that are difficult ro achic:ve without rupplemenmtion,
pa.rcicularly in higher latitudes and in of c:xtrc:mc:
winter climate. A dose of vitamm D
3
up to 2,000 IU daily
has been deemed by the: U.S. Food and Drug Adm..inistra-
tion's nutritional. guidelines to be genernl.l.y recognized as
sue. A rect:nt review concluded that the safe upper limit for
vitamin D consumption is 10,000 IU per dn.y (57); doses
JACC Vol. 51, No. 24, 2008
9, 2008:1949-56
above this increase of renal calculi formati.on, ' c:specially
in with absorptive hypc:rcalc:uria nnd end-stage
renal dise:I.Se patients on dialysis (SS).
A study of 340 children ages 10 to 17 years found that
increasing cl1e intake of oral vitamin D 10-fold, from the:
cw-rcntly recommended dose of 200 to 2,000 IU daily, \-r.\S
required to reach a 25(0H)D lc:vel of 30 ng/m.l (the lower
end of the optimal range) (59). Tho investigators concluded
that doses equivalent to 2,000 IU of vitamin D
3
daily were
not only sue for adolc::;cents, bur also necessary for nchiev-
ing the: desirable vitamin D lcvc:ls.
The most poten.t 5ourceA Dare sunllght (about
3,000 IU vitamin D
3
per 5 to 10 min of mid-day, midyc:u.r
exposure of arms legs for n light-skinned C<lucashm) or
prescription oral supplements of 50,000 IU C!lpsule of either
vitumin D
2
or D
3
every 2 weeks (1). Among foods, oily fish
have: the highest content of vitamin D
3
, which mnges from
100 to 1,000 IU per 3.5 (1,60), wherens other sources
such as milk or orange juice forri.6.ed wich vitamin D con min
up to 100 IU per
As a general rule, every 100 IU vitamin D ingested daily
incrca . .c;es the 25(0H)D level by about 1 ng/ml (61,62) (Fig.
5). Over-the-counter dietary supplements of vitamin D
2
D
3
typically comain 400 ro 5,000 ID pc.r capsule. Oral
supplementation with either vitamin D
2
or D
3
initially will
increase v.itrunin D lcvds cqu:illy well (63), although the
incrc:uscs in serum 25(0H)D lc:vcls to persist
after a bolus dose ofvitamin D
3
than (64).
Treatment of vitamin D-defictent individuals should be
initiated "vith 50,000 IU of vitamin D
2
or D
3
weekly for a
period of 8 to 12 weeks. Once the initial repletion phase is
complete, maintenance thcrnpy can be continued in 1 of 3
1) 50,000 IU vitamin D
2
or D
3
every 2 weeks; 2)
25(0H)D In 31o 6 months
:Z5(0H)O "' 2&1Jydf'OX)N1tamln o.
J'7nr'7 C'tar. nTift
'
J,
c
c
r
r
..A
1
ri
B
4.
E
R
G
B
10.
11.
.:, .. . 12.
13.
,., : : 15,
. ..
..
16.
(about
aid year
:ian) or
f either
ily fish
'!S from
iourccs
d daily
. ') o-
. 'lg.
1in D
2
:. Oral
lly will
the
longer
uld be
1 for a
1ase is
1 of3
ks; 2}
... ... .
;, .. : ...
-: ,,.; :.
to 2,000 IU vitamin D:! daily; and 3) $Untight
for 5 to 10 min for Caucasians (longer times
........ for people with increased skin pigmentation) be-
the hours of 10 AM to 3 l'M (spring, summer, nnd f.ill)
(F;g. 6).
authors thank Lori J. vVJbon for hc:r help in pt'epara-
of this article.
-----------.. .... .. . .... .. .
requests nnd correspondence: Dr. J:unes H. O'Keefe,
Woi'Il!l!l Road, Suite 2000, City, Mi,;souri 64111.
Jholceefe@cc-pc.com.
. Holick MF. Vitnmm D deficiency. N EnglJ Mc.d
Zirn:rmnnn A. Yi=in D prevention with specinl refer-
. ence m ordlov:uu:uhr Ptog Mol Blol2006;92:39-49.
W1111g TJ, Pencion .!VJJ, Booth SL, et ul. Viblmin D ri'k
of ordiov:u<:Ulu Cl.rcuhtion 2008;117!503-11.
4. Gio .... .tnnucci E, Liu Y, BW, Rimm B. 25-hydtoxyvitAmin D
:md risk of myocnn:lial ioEw:tion in men: prospective kch
': Jnrctn Mc:d 2008;1GS:ll74-SO.
::: '5 . .Dohnig H, Pili. S, Sch:un3g1 H, et 11l. Independent :wac.i3clon of low
sctum 25-hydt(l).'}"'lt;ltl'lin d 11cd 1,25-cf.hydtuxyvitRmin D hwcb with
ill-omse 1\od c.1ttdioYUSGUlnr mart'ility. Arch lntem Med 2008;16S:
1340-9. .
6. Koutkin P, Cbcn TC, HolicklV1F. Vl=in D intoocication as6ociJlted
with an over-the-counter ropplcmcnr. N Eng! J Med 2001;345:66-7.
7. Zchndc( D, :BJ;1.od R, Chima RS, et Ill. o.f J.,2S-
dihydroxyvitllmin D(3) by humnn cndothcli:Ll cell! is rc:gubrc:d by
infl:lmmntory cytokincs: n novelnul'OeriOI! cd1
ndbe:.ion. J Am Soc Ncphrol2002;13:621-9.
8. Bischolf-Fcrr:u-1 H:A, P., Willen: WC, Dic:ttich T,
B. R,tim;ltion of optimnl vcrum c.cmcentrllliOtl$ of
D for multiple health outcomes, Am J Clio Nutr
2006;84:18-28.
9. Tnogpricha V, Pcuce EN, Chen TC, HoUck 1\IIF. Vitamin D
inrufiicicncy :unoog freeUving young :tdults. Am J M.:d
2002;11.2:659-62.
10. [..,okcr 1\.C, B, Calvo MS, Guntt:t F.:W,
NR. Serum 25-hydro:cyvit:uni.n D of wd 3dults in
two RUbpopul:nioM from NHANES m. Bone 2002;30:
77\-7.
11. Clcmem TL, Ad:uns JS, Heodc.rnon SL, Hollcl: MF. lncrcued skin
pigment the ap:tclty of to vimmin D3. Lancet
12. lVJ!Ir>uok.:l J:.Y, ldt L, Wort:imao J, M:teLnughlin JA, Holick
. &uppral cutaneous vit:Unln D:l synthcsu.J Clin Endoai-
nol Meub 1987;64:1165-8.
13. Wortsm:mJ, LY, Chen TC, Z, Holick MF.
of vitumin D in obesity. Am J Clio Nutr 2000;72:
690-3.
14, Blwn M, Dolniko\l'llki C, Scyouu1 E, tt 1\.1. Vitnmin D(3) in
Endoc.rinr: 20011;33:90-4.
15. Holick lv!F, Su>lligbt and \it.unin D for bonc-bc:.'llth nnd prrn:acion of
uutoimmune dm::ises, CIUlCcr.l, cwioV':l!CUW cfueuc. Am I Clio
Nutr 2004;80:16785-885.
16. Rostnnd SG, Ultmviolct light may contribute: to wd racial
blood pressure diFcrcnc:cn. Hyp<:rtension '997:30:150-6.
17. S=gg R, R, Ho.ldaWity IM, Lim T, Beuglehole R.
. infi1tctioa is invcmdy wid1 25-hydroX}".oit:unin DJ
11 study. lntJ Epidemio11990;19:559-63.
lB. Poole KE, Lo1eridgc N, B:uker PJ, c:t :U. Reduced viumin Din acute:
stroke. Stroke 2006;37!243-S .
19. Cigolln.i M, hgu11i Mll, Miami V, Gnliotto M, L<lmhunH S, 'fnrWter
C. Serum D3 cooceacr:ttions nnd prenlem:C o(
dhelt:;e nmong type 2 diabetic Clll1:
2006;29:722- 4,
1o:rno:r oac nT<.
Lno et 1955
Vltllmin D Defit:iency and CV Risk
:w. Mcl;&rottl ML, MvntMr P, ED. et nl. Serum 25-
hydroxyviromin D lo:vch and the pri!Vn!ence of peripher.U :mcrbl
from NHANES 2001 to 2004. Anc:dooclcr Thromh
Vase 'Hiol2008;28:1179-85.
21. M:urin$ D, Wolf M, P-111 D. ct Pti:V:Ilcnce of risk
f.lc:rora a.nd the serum levels of 25-hydroxyviuml.n D In the: United
Stutes; dnt:1 &om the Thittl Nutionul He1Uth und Nutrition E.-uuninn-
tion Survey. Arcl\ Intern Mcd 2007;167:1159-65. ,
22. Scragg R., Sow= M, Bc:ll C. S=un 25-hydroxyvitamin D, etbnicity,
blood in che TIW:d Health nnd N11trition
Survey. Am J HypcrtCll5 2007;20:713-9.
13. S=gg R, S.lwcr' M, Bell C. SctUtn 25-hydroxyviwrun D,
cthnicity in the 'Third Nutionul He1tlth 11nd Nutrition &'Ounina-
clon Survey. C:u-e 2004;27:2813-8.
24. Ri:tchy R. V:llldcwu!lc B, Moennun E, ct uL 1,25-Dihyd.roX)"-it&min
D3 humnn e:ywl:inc-induc:cd '-popto-
si.!i via downregul.1tion of the F:IS receptor. Apoprosi.5 2006;11:151-9.
25, Chiu KC, ChuA, Go VT.., MF. D
with inbulin resill'tltncc: llnd bent cell Am J Clin Nutr
2004;79:820-S.
26. Pittns AG, Dnwson-Hughe& B, Li T, et al. Vit1min D ruid alcium
ln cc:l:ttinn ro cypc: 2 dio.b<:tc.1 In womc:n. DbhctcR C:trc
2006;29;650-6
27. Hypponeu E, Lnar-<1 E, Reun:tneo. A, ]iltvdin MR, Vlttanen SM.
Int1ke of 0 and ri!lk of type l n bi.rth-(ohort study.
Lmcc:c 2001;'!5S:1500-3.
28. Zipitis cs, Akobeng AI<, Vinunin D 1Uppl=cntation m early
childhood and dsk of type 1 &alx:te&: :1 li)llltc:m:ldc ce\'lew :1nd
mctu-unul)'!'u. Arch ))j, Child 2008;93:517.-7
29. Slmpsaa RU, Hc:nhc:y SH, Nlbbcllnk KA. Clur.u:tcri.:t:ltion ofheut
1111d bloJotl in che vito'lmin .D knocko11c J
Steroid Biochcm Mol Bioi 2007;103:521-4.
30. Ll YC. Vi1:1min D regui:J.tion of che "}'Stem. J Cell
iochcm 2003;88;327-31.
3).. R, Buhri.ng M, Hopfenmullet W, Holick MF, Sb1\tm!1 AM.
Ultr:Iviolct B nnd blood prCRrurc. Lltncet 1998;352:709-10.
32. Sugden JA, Davies jl, With:un MD, N!orris AD, Struthc:n AD.
Vilttmin D c:ndothelilll function in p1ttients '"oitb type: 2
di:tbc:tcJ mclliDJ.q nnd low tif.:lmln D lcvciR. DubctcR Mc:d 2008;25:
320-5.
33. P, Moaddldc L Cohort study on &co; of p:u:lthyrold
on Jnul.riple outcomtl> in prim:>.')' hypcrpolt;othyroidi.1m, BMJ
2003;327;530-4.
34. Soub:uei LP, Chi= TC, ED, c:r :U. Incider.c:e
fitetuno of' curonucy benrt discwsc in elderly p11tic:nts on chronic:
hemodi3lysi,;. T.nt Uml Ncphro1 2006;38:795-SOO.
35. Bjork:mtln MP, Sol'\'!!. AJ, Tuvis RS. sc:rum p:uuthyroid
hormone: prcdic;tl; impaired )'\lrvi"u in 1\ g.:ncnu t1gcd
popubtion. Eur J Endocrinoi2008;1SS:7-19-S3.
36. Ogmd CG, J::cgehrumo MD, Kisturp C, Nichcn SL, Yestcrgitard H.
lncrc:w:d. N-tctminn.l pro-B-typc: peptide
mnrkcn; of inflrurunntion rcbtcd to utherosclcrosili in paticntl; with
prim:l!y hypc.rp:u:tthyroldiam. Clin Endocrinol (Ox) 2005;63:493-S.
37. AnclcMoo P, RydbctJ; E;Willcnheimcr R. hyperpmthyroid-
ism and hClLit rc:view. Eur Hem J 2004;25:1776-87.
38. S11rnnk MJ, Ltm:y AS, Schoohvcnh AC, t!t 111. Kidney diseuse tu 11 risk
flctar for dc:vclopmc:nt of disclll!e: rn:atc:mc:nt from the
Amcric11n H= Associntion Councils on Kidney in Cud.iovuscubr
High Blood PrCM\Il'c Clinic::U C:ll'dio1ogy,
Epidcmiolo;;y Mnd Prevention. Citcullltion 2003;108:2154-69.
39. Wolf M, Shalt A, Gucicnc:-t 0, et :U. Vit:1mln D Jcvdr. wd
mortAlity t\rtiOilg ineitl(:l'lt JllltientJ. Kidney lnt 2007;72:
1004-13.
40. CP, Ahm3d7.3dcli S, JE, K:shnta:-Z:.dch K.
Association of a<:tivutcd vitumin D tn:utment and mortnlity in chronic
k:dncy 1\reh Intern Med 2008:168:397-403.
41. Singh NP, V, 0, Nair M. Elfcct of
of Reeond:uy on c::udiav:lS<:uhr he
modymunics in prc:diuly.;is CKD pnticnts: 11 preliminllt')'
Hemodiallnt 2007;11:417-23.
42. Le': GH, Bennet D, Regidor DL, Knlnnttr-ZRdch K. Imp3ct of
lcidno:J' boac disezc wd ito lllll.'1llgcment on rurvivnl of pKticnts on'
dlnl)'!lis. J Rc:1t Nutr 2007;17!3\l-44.
'
t lO. d 'TVJ.O.L
1956 lee et 111.
V"rbntin D Dofldoncy lltld CV IUsk
43. S::hldtholfSS, Zittmmum A, C. ll=ha!p HK, Stdlle P,
Komer R. D supplcmc:nutlon improves cytokinc ht
with congestive hem f.tilUK: a double-blitd, t:Uldomiud,
pbccbocontrollcd triaL Am J Clin Nutt .. 1:754-9.
44. T, Morris RC Jr., J\'C.I HE. 1,25-dihydroxy;itnm.in D3
of v:ISculu &mooth muscle L-dls. J Clin I nvut
1991;87:1899-95.
45. P. Vit:unin D pbyzlology. Frog Mol Biul 2006;?2!4-R.
46. Auticr P, G11ndini !:i. Vitumin D :md tot:U morn.liry:
of r:mdonuua controlled tri.Js. Arch l ntc:rn Mcd
2007i167:1730-7.
47, Jone' C, W.M.cnbccz T. C:udiov:ucu!M risks of cnlcium
in women. BMJ 2005;336:226-7.
4S. Bolland .Mj
1
.l:larbc:r P A, Doughty RN, ct V eve no; in healthy
older women nndomi.scd con-
rtollerl cnal. BMJ 200S;336:262-6.
49, &mu HG, Broun J, Kr.u"'r. R, .t Tw11 yc".lt COlllpariaon of
o.nd urboonte c:.fi'eas on c:udiovo.sculnr cu.lciicl!tiun
and hone dcmity. Nephrol Dial ' l'nm"Plunt :!005;20:1 65:1-lll.
SO. Wnn:ul'l K,F., Ahrobt 1\fi., MAlone LL, ct :al.. Active sc:rum. vitamin D
levels uc: in\crsely correlated with coruni\C)'
19?7;?6:j 755-60.
51. JR, IWnaiacr CM, IUUr.vatu DL. c:r Ill. bone mineral
density is com:llllt<i with subdink:d in olrlcr, but not
)'DWlt,OU, Meactn AmcriCin women fl)gl: rhc Sn Anronio F:i:nily
Sturl). lm ::!007;81:430-41.
52. ClctUp H, Mikkd5c:n K, Poul!c:n L, et aL Commonly rccommc:nded
dilly lnt'lke of viwnin V is not sufficient if $llnligbt c.'q'OMC i..;
limited. J .lnt m1 Med 2001T,247:260B.
53. PlomikoffGA, Qltiglcy ]1\lt. Prc:v21ena: of bypovh:uninos.ls Din
with pcni5lc:nt, nonspecific muKUlosla:kllll pnin. Muyo Clin
Ptve 2003;78:1163-70.
JACC Vol. 52, tlo. 24, 2008
2008:1949-55
54. Bischoff-Fcrt:Lrl HA, :B, WJ..IJ.ert we. Ct :11. Elfecr
of vit'.tmin D 011 fo.IL\: :1. meta. :uulyals. JAMA 2004;291:199?-
2006.
SS. Diebt) Supplement Fact Sbtct; Vittunin D. Office of Dieooy Sup-
NIH CUnic::ll Center, Io.-titutes of Hetlth. 2007.
AvnilAble http:/ldlctaty-ilnpplemcnts.lnfo.nlh.gov/f:!.CuhcetJ/
vit:lmiod.asp. July 30, 2()0!l.
SF.. Moore C, Murphy MM, DR, HulickMF. Viumin D in
the United Sutc&, J Am Diet Anoc 2004;104:980-3.
57. Huthc:oek JN, A. Vieth R, Heaney R. for
vittrmin D. Am] Clln Nutr 2007;85:6-18.
58. Dnudun M. Jungc:rA P. Drug-induced renal cnlculli epidemiology,
prcvtntion Knd tn01>1agcmr:m. Drugs 2004:64:245-75.
59. M:uloufj, Nubuai M, Vieth R, cr al. Shorc-rc:rm :md long rerm
of wctlcly highdofic viumin DJ in school children.
J Clln Endoc::rinol Melilb
60. Chcl TC, Chlmch F, Lu Z, ct Foctot3 tl.mr inllucnc:c the cuti\DCOU>
and dlcr.uy su11rt:o.:!l c>f' (). Atcb Biochcm Biophy:i
2007;460:213- 7. .
61. He11t1c:y RP, DavicA KM, Chen TC, Holick MF, .MJ.
Human serum response co extended onl
doai.ng with Am J Clln Nutc 2003;77:204-10.
62. Vieth R. Vitamln D nrpplcmcnt:.tion, 25-hydtoxyviwnin D cunCI:TI-
tnuions, :u1d WCt)'. Am J Clin Nurr 1'J!l9;69:842-5G.
63. Holick Ml?, BiRncu;:7.o RM, Chen TC, ct :U. Vitamin 02 in ;u
cJFtcrivc :u1 viwnin 03 in cireul:lting conccn=cions of
25-hydroxyviu.rnit 1). J Clin Endocriool 2008;93:677-Sl.
64. Arm:u LA, Hollis 'OW, RP. Vltamln 02 j ,; much
than vir:unin D3 in huml\ns. J Clin 'Endocrinol Met\b
2004;89:5387-91.
Key Wo(d.: viumln D 25- hydro.-t)'vinmin 'D c::Uclwu coron:tty
plcvcntiOr\ " hypcr.:cnsion
I
Th
tie1
rcn
tria
Fn.r.
trto
. : Ql=
,CJ-
bncl.
l emma/ ofGerontolog\: MEDICALSC/E/IlC.4)
Cite journal as: J Grromol A Bioi Sci Med Sd
2009. Vol. 64A. No. :\, 5:\9-56 7
The Awhor 2009. Publishetl by O.iford Uni\ersiry Pre.o;s ou belwlj of The Cit'rtllllOiogical Society ofAmerit.'a.
All riglus rtsen-ed. For pamissions. p/e((St e-mail: joumals.permissions@oxjordjoumals.org.
Admm.:t> A<.ce,\S publlt;ation ()II February 16, 2009
doi: I 0.1 093/gerono/glp006
Calcium Plus Vitamin D Supplementation and Mortality in
Postmenopausal Women: The Women's Health Initiative
Calcium-Vitamin D Randomized Controlled Trial
Andrea Z. LaCroix,
1
Jane Kotchen,2 Gamet Anderson,
1
Robe1t Brzyski,
3
Jane A. Cauley,
4
Steven R. Cummings,5 Margery Gass,6 Karen C. Johnson,
7
Marcia Ko,8 Joseph Larson,
1
JoAnn E. Manson,9
Marcia L. Stefanick, IO and Jean Wactawski-Wende
11
1
Division of Public Health Sciences, WHl Clinical Coordinating Center, Fred Hutchinson Cancer Research Center, Seattle, Washington.
2
Division of Epidemiology, Department of Population Health, Health Policy Institute, Medical College of Wisconsin, Milwaukee.
3Department of Obstetrics and Gynecology, Division of Reproductive Endocrinology and Infertility, University of Texas,
Health Science Center, San Antonio.
4
Department of Epidemiology, University of Pittsburgh, Pennsylvania.
5
Department of Medicine, Epidemiology and Biostatistics, University of California at San Francisco.
6
Department of Medicine, University of Cincinnati, Ohio.
7
Department of Medicine, Health Science Center, University of Tennessee, Memphis.
8Department of Internal Medicine, Women's Health, Mayo Clinic Scottsdale, Arizona.
9
Department of Epidemiology, Division of Preventive Medicine, Brigham and Women's Hospital, Harvard Medical School,
Boston, Massachusetts.
10
Stanford Prevention Research Center, School of Medicine, Stanford University, California.
11
Department of Social and Preventive Medicine, University at Buffalo, New York.
Background. Calcium and vitamin D (CaD) supplementation trials including the Women's Health Initiative (WHI)
trial of CaD have shown nonsignificant reductions in total monality. Tlus report examines intervention effects Oil total and
cause-specific mortality by age and adherence.
Methotls. The WHJ CaD trial w a ~ a randomized, double-blind, placebo-controlled trial that enrolled 36,282 post-
menopausal women aged 51- 82 years from 40 U.S. clinical centers. Women were assigned to 1,000 mg of elemental
calcium carbonate and 400 IU of vitamin D3 daily or placebo with average follow-up of7.0 years.
Results. The hazard ratio (HR} for total mortalily was 0.91 (95% confidence interval [CI], 0.83-1.01} with 744
deaths in women randomized to CaD versus 807 deaths in the placebo group. HRs were in the direction of reduced risk
but nonsignificant for stroke and cancer mortality, but ncar unity for coronary heart disease and other causes of death.
HRs for total mortality were 0.89 in the 29,942 women younger than 70 years (95% CI, 0.79- 1.01) and 0.95 in the
6,340 women aged 70 and older (95% CI, 0.80-1 . 12; p value for age i.nteraclion= .10). No statistically significant in-
teractions were observed for any baseline characteri stics. Treatment effects did not vary significantly by season.
Couclusions. In the WHI CaD trial. supplementation did not have a statistically significant effect on mortality rates but the
findings support the possibility that these supplements may reduce lllOltality rates in postmenopausal women. These data can
neither support nor refute recommendation.s for higher dose vitamin D supplemenlation to reduce cancer or total mortality.
Key Words: Calcium-Vitamin D-Mortality-Cause-specific mortality-Women' s Health Initiative.
D
ESPITE predictions that some types of micronutri-
ent supplementation might prevent cancer and car-
diovascular disease (CVD) and reduce mortality, the
results of large intervention trials of chemoprevention
have been largely disappointing to date. Several random-
ized controlled trials have shown nonsignificant reduc-
tions in total mortality among women assigned to vitamin
D
3
, calcium carbonate alone, or the combination of cal-
cium plus vitamin D (1-4). Among the 36,282 women
who participated in the Women's Health Initiative (WHI)
calcium plus vitamin D (CaD) supplementation trial, the
intention-to-treat hazard ratio (HR) for total mortality
was 0.91 (95% confidence interval [CI], 0.83-1.0 1) (1). A
recent meta-analysis, in which WHI women contributed
nearly two thirds of the data, reported a significant reduc-
tion in mortality among nine trials (4) based only on pre-
viously published data.
We report here the first thorough evaluation of the possi-
ble effects of CaD supplementation on total and cause-
specific mortality in the WHI CaD trial. This repott also
assesses the impact of adherence to CaD supplementation
on treatment effect estimates and determines whether HRs
for total mortality differed according to levels of selected
baseline characteristics, including age.
559
560 IACROJX ET AL.
METHODS
Design Overview
The WHI CaD trial is a randomized, double-blind, place-
bo-controlled trial designed to determine whether supple-
mentation with calcium (1,000 mg/d) plus vitamin D (400
IU/d) would prevent hip fracture (the primary outcome), other
fractures, or colorectal cancer (designated secondary out-
come). These findings have been previously published (1,5).
Setting and Participants
Between 1993 and 1998, postmenopausal women aged
~ 7 9 years were enrolled in the WHI randomized clinical
trials designed to assess the 1isks and benefits of hormone
therapy (HT) and dietary modification (DM) (6). One year
later, participants in either the HT or the DM trial were in-
vited to enroll in the CaD trial. Exclusion criteria for the CaD
trial included a predicted survival of less than 3 years; a his-
tory of renal calculi or hypercalcemia; or current use of oral
corticosteroids or calcitriol, or daily use of 600 IU or more of
supplemental vitamin D (7). Personal use of calcium supple-
ments up to 1 ,000 mg/d or vitamin D up to 600 IU/d wa<;
permitted. The protocol and consent fonns were approved by
the institutional review board at each pa1ticipating institution.
All women provided written informed consent.
Randomization and Intervention
Details regarding execution of the trial have been de-
scribed previously (I ,6). Briefly, using a permuted-block
algorithm stratified by clinical center and age, 18,176 women
were randomly assigned to receive one tablet of 500 mg of
elemental calcium as calcium carbonate combined with 200
JU of vitamin D3 (GiaxoSmithKline. Pittsburgh, PA) twice
daily, totaling I ,000 mg of elemental calcium and 400 IU of
vitamin D. A total of 18,106 women were randomized to
receive an identical-appearing placebo tablet twice daily.
Blinding of the study was achieved by bottle labeling.
Outcomes and Follow-Up
Participants were contacted semiannually thereafter to
ascertain self-reported medical history updates. When they
could not be contacted, information on vital status was sought
from previously identified proxy informants, National Death
Index searches, and obituary notices. Regardless of adher-
ence, participants were followed up until they died, were lost
to follow-up, requested no further contact, or until the study
ended. Ninety-seven percent of participants were followed to
study completion. Causes of death were determined based on
available medical records, autopsy reports, and the death cer-
tificate in a blinded fashion by local and central physician
adjudicators. For 352 deaths (22.7%), the death certificate
was the only available source of information for determining
cause of death. Ninety-six percent of reported deaths were
centrally adjudicated, 2.5% were locally adjudicated, and
1.5% could not be adjudicated.
Study pills were discontinued if women reported kidney
stones, hypercalcemia, dialysis, or the use of calcitriol or
daily supplements of more than 1,000 IU of vitamin D dur-
ing semiannual contacts. During the study, adherence was
assessed by weighing returned pill bottles.
An independent data and safety monitoring board reviewed
the trial data semiannually. Closeout visits occmTed as
planned between October 1, 2004, and March 31,2005, with
final outcomes assessed before the treatment assignment was
revealed. WHI investigators and National Institutes of Health
sponsors all contributed to the study design and execution.
Nested Case-Control Study of Vitamin D Levels
Baseline serum measurements of 25-hydroxyvitamin D
were available for 323 women who died and I ,962 living
controls in the CaD trial from previous nested case-control
studies (I ,5). Levels of 25-hydroxyvitamin D were mea-
sured using the DiaSorin Liaison chemiluminescent immu-
noassay system at Diasorin headquarters (Stillwater, MN)
as previously described (I ,5).
Statistical Analysis
Primary analyses used time-to-event methods, according
to the intention-to-treat principle. Mortality rates were com-
pared in the two groups with the use of HRs (with 95 per-
cent Cis) and stratified logrank tests from Cox proportional
hazards models (8), stratified according to baseline age and
treatment assignment in the HT and DM uials.
In addition, HRs were calculated by categories of causes
of death (cardiovascular, cancer, other, and for CVD, coro-
nary heart disease (CHD), and cerebrovascular cause of
death separately). Because mortality rates tise markedly
with age, treatment effects were examined separately for
women younger and older than 70 years, the cut point pre-
specified in the protocol for defining older women. Analy-
ses according to adherence to study medication were also
conducted, with participants censored 6 months after first
detection of becoming less than 80% adherent. Inverse
probability weighting methods were used to estimate full-
adherence HRs adjusting for covariates found to be associ-
ated with nonadherence (1,9).
Potential differential effects across categories of important
risk factors for mortality were also tested individually with
the use of a likelihood ratio test for interaction between the
risk factor and the treatment assignment after including both
as main effects. Twenty-three subgroup comparisons were
tested; thus, about one test would be expected to be statisti-
cally significant at the .05 level by chance alone. All reported
p values are two sided and were not adjusted for multiplicity.
Odds ratios for CaD supplementation were estimated using
logistic regression across tertiles of serum 25-hydroxyvitarnin
D. The model stratified by randomization assignment in
CALCIUM PLUS VITAMIN D AND MORTALITY 561
!:::!
0
AU ages !:::! Ages ;::70
0
0
HR=0.91
0
HR =0.95
(95% Cl. 0.83-1.0 I) (95% Cl, 0.80 1.1 2)
00
0
0
00
0
0
g
8
0
0
0
N
c:
0
s
0
c:
0
Time (years) 0 Time (years)
0
0 2 4 5 6 7 8 0 2 3 4 5 6 7 8
CaD: CaD:
Event;;. 33 58 89 96 118 131 103 19 33 E\'COL."i II 23 32 37 44 so 3S 29 16
Nat risk 1817618072 17975 17839 17676 17331 14768 9213 4+14 Na1 3173 3155 3129 3087 3038 2940 2327 1262 570
Placebo: Placebo:
Evcms 48 74 98 114 126 114 74 25 18 36 41 31 39 46 42 24 10
N 18106 17993 17872 17720 17541 17174 14617 9105 4385 Na1risk 3167 3145 3103 3056 3012 2921 2317 1262 565
Ages<70
HR=0.89
(95%CI, 0.79-1.01)
CaD:
Evcnb
N Ql ri&k
Placebo:
Events
N ul ris.k
.....
0
0
0
0
0
22 35
15003 14917
30 38
14939 I4R4R
2
57
14846
57
1471\Q
Figure I. Cumulative mortality Kaplan-Meier curves by age group.
3 4 5 6 7 8
59 74 81 68 50 17
14752 14638 1244 1 7951 3874
83 87 81 72 50 15
141\1\4 14253 12100 7R4l 3R20
Note: CaD = calcium and vitamin D; Cl = confidence interval; HR =hazard ratio.
another WHI trial and age group, and adjusted for age, ethnic-
ity, and latitude of clinical center. An interaction p value was
calculated for treatment by continuous serum level.
RESULTS
Baseline characteristics were well balanced between the
treatment groups (Table 1). Twenty-nine percent of study
participants were taking at least 500 mg/d of supplemental
calcium on their own. Low calcium intakes ( <800 mg/d)
were noted in approximately one third of study participants.
The mean (SD) duration of follow-up was 7.0 (1.4) years.
At time of closeout, 1,551 deaths had occurred, 744 in the
CaD intervention group and 807 in the placebo group. The
final HR for total mortality was 0.91 (95% Cl, 0.83- 1.01)
(Table 2). CaD HRs were in the direction of reduced risk but
nonsignificant for stroke and cancer mortality, whereas HRs
were close to unity for CHD and other causes of death.
Intention-to-treat HRs by age at baseline ( <70 vs ?:.70
years) suggested lower HRs among younger women for to-
tal, stroke, and other causes of death. The HRs for total mor-
tality were 0.89 in women younger than 70 (95% CI,
0.79- 1.01) compared with 0.95 in women of ages 70 and
562 IACROJX ET AL.
Table I. Characteristics of WHl CaD Participants at WHI Screening by Randomization Arm
CaD (N= 18,176) Placebo (N = 18, I 06)
N Mean (SD) or % N Mean (SD) or % p Value
Age at screening, y
Mean (SD) 18,176 62.4 (7.0) 18,106 62.4 (6.9) .97
50-54 2.594 14.3 2.563 14.2
55-59 4,134 22.7 4, 131 22.8
~ 9 8.275 45.5 8,245 45.5
70-79 3,173 17.5 3, 167 17.5
Race/ethnicity .45
White 15.047 82.8 15.106 83.4
Black 1.682 9.3 1,635 9.0
Hispanic 789 4.3 7 18 4.0
American Indian/Native American 77 0.4 72 0.4
Asian/Pacific Islander 369 2.0 353 1.9
Unknown 212 1.2 222 1.2
Education at screening .98
High school or less 4,286 23.6 4,289 23.7
Some school after high school 5,30 1 292 5,248 29.0
College graduate 1,862 10.2 1,856 10.3
Graduate school 4,693 25.8 4,687 25.9
Hormone use at annual visit I .23
Never used 5,814 32.0 5.690 3!.4
Past user 3,004 16.5 2,932 16.2
Current user 9,358 51.5 9,484 52.4
Dai ly supplemental calcium use
Mean (SD) 18,176 322.6 (479.2) 18,106 326.2 (482.4) .48
None. mg 8.009 44.1 7,871 43.5
<500 4.975 27.4 4,922 27.2
>500 5.192 286 5,3 13 29.3
Dai ly iota! calci um (supplements+ diet). mg
Mean (SD) 17,821 1,148.4 (654.2) 17,753 1.154.3 (658.0) .40
<800 6.104 33.6 6.003 33.2
800 to <l ,200 4,715 25.9 4.655 25.7
2: 1.200 7.002 38.5 7.095 39.2
Daily vitami n D (supplements+ diet), IU
Mean (SD) 17.821 365.3 (265.5) 17.753 367.9 (266.0) .36
<200 6,827 37.6 6,671 36.8
200 to <400 3.379 18.6 3.423 18.9
400 to<600 4.188 23.0 4.295 23.7
<:600 3,427 18.9 3,364 18.6
History of hypertension .88
Never hypertensive 6,944 38.2 6,925 38.2
Untreated hypertensive 6.686 36.8 6,692 37.0
Treated hypertensive 4,546 25.0 4.489 24.8
Systolic blood pressure 18.176 127.4 (l7 .I) 18.106 127.5 (17.2) .48
Diastolic blood pressure 18,175 75.9 (9.1) 18,101 75.9 (9.1)) 56
Smoking .50
Never smoked 9,428 52.1 9,325 51.3
Past smoker 7,133 39.4 7,255 39.9
Current smoker 1,356 75 1,405 7.7
Alcohol use 88
Nondrinker 1,863 10.2 1,891 10.4
Past drinker 3,192 17.6 3,209 17.7
<I drink per mo 2.529 13.9 2,520 13.9
<I drink per wk 3.863 21.3 3.758 20.8
I to <7 drinks per wk 4.683 25.8 4,706 260
<:7 drinks per wk 1.910 10.5 .1.900 10.5
Physical activity
Mean (SD) METs/wk 16.546 10.7 ( 12.7) 16.448 10.6 (12.4) .60
0-3.00 5,517 30.4 5,478 30.3
>3.00 to <11.75 5.463 30.1 5.477 30.2
:0:11. 75 5.566 30.6 5,493 30.3
CALCIUM PLUS VITAMIN D AND MORTALITY 563
Table I. (Continued)
CaD (N= 18,176) Placebo (N= 18, 106)
N Mean (SD) or% N Mean (SD) or % pYalue
Body mass index. kg!Jn2
Meao (SD)
<25
25-29.9
;:.:30
No. of CVD risk factors
None
J-2
>3
History ofCVD
History of treated diabetes
OM trial arm
Placebo
Intervention
Not randomized
HTtrial arm
Placebo
Active
Not randomized
No. of chronic conditions at screening
Depressive symptoms score
Physical function score
18,084
4,745
6,472
6,867
5.544
12,337
295
1, 173
&85
7,827
4.767
5,582
4,015
4,039
10,122
18,176
18,135
18,127
29.1 (5.9) 18.011
26.1 4,833
35.6 6.4&3
37.8 6,695
30.5 5.579
67.9 12. 195
1.6 332
6.5 1.221
4.9 &75
43.1 7,738
26.2 4.878
30.7 5.490
22.1 3,957
22.2 4.078
55.7 10.071
1.2 (0.9) 18.106
2.30 (2.55) 18,057
81.5 (20.1) 18,061
29.0 (5.9)
267
35.8
37.0
30.8
67.4
1.8
6.7
4.8
42.7
26.9
30.3
21.9
22.5
55.6
1.2 (0.9)
2.33 (2.59)
81.4 (20.3)
.24
.23
.27
.87
.30
.74
.93
.18
.50
Note: CaD = calcium and vitamin D; CVD = cardiovascular disease; DM = dietary modification; HT = hormone therapy; MET = metabolic equivalent;
WHI = Women's Health Initiative.
older (95% CI, 0.80-1.12; p value for age interaction= .1 0).
HRs for cancer death were similar across age categories.
At trial closure, 76% of women enrolled were still taking
study medications and 59% were taking at least 80% of
study pills. When participants were censored 6 months after
first detection of adherence less than 80%, HRs were 0.87
for total mortality (95% Cl, 0.73-1.04), 0.85 for cancer
mortality (95% CI, 0.66-1.09), and 0.57 (95% Cl, 0.30-
L09) for stroke mortality. HRs suggested greater benefit for
adherent women younger than 70 years, as compared with
older adherent women (data not shown). Tests for age inter-
action were statistically significant for total mortality
(p = .02) but not for the cause-specific categories. Estimated
full-adherence HRs based on the inverse probability weight-
ing method were similar to those for adherent women and
all Cis included 1.0.
Intention-to-treat HRs did not vary significantly for any
of the 23 baseline risk factors examined for mortality. In
addition to the subgroups shown in Table 3, no significant
differences were observed by subgroups of education, al-
cohol intake, history of diabetes, depressive symptoms,
physical function score, and disability in activities of
daily living, or randomization in the dietary modification
trial. In models adjusting for season as a time-dependent
variable, risk of mortality was increased during winter
months, with a HR of 1.14 (95% CI, 0.99-1.32). Treat-
ment effects did not vary significantly by season at time
of death (p value for interaction= .20), although HRs were
observed to be reduced iJJ winter (HR =0.81; 95% CI,
0.66-0.98), summer (HR=0.87; 95% Cl, 0.71-1.06), and
autumn (HR =0.93; 95% CI, 0.77-1.13), but not in spring
(HR= 1.10; 95% Cl, 0.89-1.36).
In the nested case-control study, CaD intervention effects
did not vary significantly by baseline levels of serum 25-
hydroxyvitamin D (p= .66), although the odds ratio was in
the direction of benefit for women in the lowest tertile
(Table 4). Compared with women in the highest tertile of
serum 25-hydroxyvitamin D, there was a significantly in-
creased risk for death for women in the middle and low ter-
tiles. The odds ratio for serum 25-hydroxyvitamin D level
analyzed as a continuous variable was 0.80 (95% CI, 0.67-0.95)
for a difference of 29.9 nmol/L (the interquartile range).
DISCUSSION
In this large randomized trial of women aged 50-79, CaD
supplementation for an average of 7 years was associated
with a nonsignificant reduction in the risk of death (9% with
95% Cl, 17% reduction to a 1% increase in risk). The evi-
dence was most consistent for a decrease in cancer mortality.
Among the 23 interactions tested, none was statistically
significant. Age, as the strongest predictor of mortality in
the general population, was of particular interest. Among
the women younger than 70 years, CaD supplementation
appeared to reduce risks of total, CVD, and cancer death.ln
older women, only cancer mortality appeared to be reduced.
The interaction between CaD supplementation and age was
not statistically significant for total mortality overall but
was so among adherent women (p = .02).
Because the majority of statistical tests repotted herein
are not significant at the .05 level, a viable explanation for
564 IACROJX ET AL.
Table 2. Effect of Calcium With Vitamin D Supplementation on Total, CVD, Cancer, and Other Mortality, According to Randomly Assigned
Group
CaD Placebo
Cases (am1ualized %) Cases (annualized%) HR(95% Cl)
Follow-up time, y (mean SDl 7.01.4 7.01.4
Total monality 744 (0.58) 807 (0.63) 0.91 (0.83- 1.01 )
CVDdeath 226 (0.18) 244 (0.1 9) 0.92 (0.77- 1.10)
CHD death 130 (0.1()) 128 (0.1 0) 1.01 (0.79-1.29)
Cerebrovascular death 54 (0.04) 60 (0.05) 0.89 (0.62-1.29)
Cancer death 344 (0.27) 382 (0.30) 0.89 (0.77-1.03)
Other/unknown death 174 (0.14) 181 (0.14) 0.95 (0.77-1. 17)
Participants younger than 70 years
Follow-up time, y (mean SD) 7.1 1.4 7.1 1.4
Total mortality 466 (0.44) 517 (0.49) 0.89 (0.79-t.OJ)
CVDdcath 115 (0.11) 135 (0.13) 0.85 (0.66-1.08)
CHDdeath 70 (0.07) 70 (0.07) 0.99 (0.71- 1.38)
death 21 (0.02) 33 (0.03) 0.62 (0.36-1 08)
Cancer death 245 (0.23) 268 (0.25) 0.9 1 (0.76-1.08)
Other/unknown death 106 (0.10) I 14 (0. 11) 0.92 (0.70-1.20)
Participants 70 or older
Follow-up time, y (mean SO) 6.7 1.4 6.7 1.5
'lbtal mortality 278 ( 1.30) 290 (137) 0.95 (0.80-1.12)
CVDdeath I l l (0.52) 109 (0.51) 1.01 (0.78-1.32)
CHD death 60 (0.28) 58 (0.27) 1.02 (0.71- 1.47)
Cerebrovascular death 33 (0.15) 27 (0.13) 1.20 (0.72- 2.01)
Cancer death 99 (0.46) 114 (0.54) 0.86 (0.65-1.12)
Other/unknown death 68 (0.32) 67 (0.32) 1.01 (0.72-1.42)
Note: CaD= calcium and vitami n D: CHD =coronary heart disease; Cl =confidence interval: CVD =cardiovascul ar disease; HR = hazard ratio.
these results is chance alone. Among the younger women,
there was a difference favoring intervention for reduced
mortality within the first year, which is difficult to attribute
to intervention. A trial designed to confirm this association
would require more than 90,000 women aged 50 and older
followed for 5 or more years to detect a statistically signifi-
cant reduction in mortality rates of 9%-10%.
Nonetheless, previous randomized controlled trials, most
of which enrolled only older women, have also shown non-
significant reductions in total mortality. A recent meta-
analysis of nine trials testing vitamin D supplementation
reported an overall HR of 0.93 (95% CI, 0.87-0.99); how-
ever, this point estimate largely reflects the contribution of
WHI women who contributed a majority of the person-time.
Six of the remaining eight smaller uials showed nonsignifi-
cant reductions in total mortality ( 4 ). Cause-specific mortal-
ity was examined in only one previous trial and showed
nonsignificant reductions in cardiovascular, total cancer,
and colorectal cancer mortality with very wide Cis (3).
If the results did not occur by chance, multiple pathways
could be involved including any elements of the supple-
ments tested: calcium, vitamin D
3
, or carbonate, or all. Cal-
cium supplementation has been shown in small experimental
studies to lower blood pressure ( 1 0) and reduce cholesterol
levels (11-13). Observational epidemiological studies have
shown an association of calcium intake with reduced stroke
incidence and mortality ( 14-16) and inconsistent associa-
tions with reduced risk of coronary disease (16, 17). Lower
bone density has been associated with increased mortality
risks (18,19). In the WH1 CaD trial, the intervention group
had statistically significant but small reductions in low-
density lipoprotein, weight, and waist circumference, whereas
blood pressure change was slightly increased compared
with placebo (20). Although the intervention improved hip-
bone density by about 1 %, it produced no significant differ-
ences in CHD or stroke incidence.
Vitamin D insufficiency has now been linked to a broad
spectrum of human diseases from cancer to cardiovascular
to autoimmune conditions (21). A recent ecological study
showed consistently elevated death rates from cancer sites
among U.S. women with less solar ultraviolet-B exposure
(22). Vitamin D receptors are present in many cell types and
1,25-dihydroxyvitami.n D bas been shown to favor cell dif-
ferentiation over proliferation and to inhibit potential for me-
tastasis and invasiveness (23). Serum vitamin D levels were
inversely associated with colon cancer risk in the Nurses'
Health Study (24), in the WHI CaD trial (6), and with colon
cancer mortality in National Health and Nutrition Examina-
tion Survey (25). Supplementation with 1,100 IU of vitamin
D
3
reduced the risk of cancer in a recent small trial of healthy
postmenopausal women (26). Two recent prospective studies
link levels of serum 25-hydroxyvitarnin D below 44.4 nmol/L
(27) or 25.2 nmol/L (28) to increased risk of total mortality.
The emerging optimism over vitamin D supplementation
for the prevention of cancer (29) is occurring in the absence
of confirmation from large prevention trials that can deter-
mine the benefits and any currently unknown risks. Proponents
argue that the necessary levels of vitamin D supplementation
CALCIUM PLUS VITAMIN D AND MORTALITY 565
Table3. HRs Re lating CaD to Ri sk of Total Mortality St ratified by Selected Baseline Characteristics
CaD (N= 18.176) Placebo(N= 18,106)
No. of Dea1hs % No. of Deaths % HR (CI)' p Value for Interaction
Ethnicity .30
White 607 0.57 679 0.64 0.89 (0.80-0.99)
Black 79 0.68 89 0.78 0.91 (0.67-1.23)
Hispanic 23 0.42 11 0.22 2.28 ( 1.07-4.87)
American Indian 0.93 4 0.79 0.84 (0.16-4.48)
Asian/Pacific Islander 18 0.73 12 0.51 1.60 (0.75- 3.43)
Otber/Unk.oown 12 0.83 12 0.81 0.90 (0.45- 1.80)
HT use at annual visit I . 14
Never used 280 069 275 0.69 100 (0.84- 1.18)
Past user 118 0.56 155 0.75 0.74 (0.58-0.94)
Currem user 346 0.52 377 0.57 0.93 (0.80-1.07)
Calcium supplementation. mg .64
None 366 0.64 369 0.66 0.97 (0.84-1.12)
<500 199 0.57 226 0.66 0.86 (0.71-1.04)
::::soo 179 0.50 212 0.58 0.8710.71-1.06)
Baseline total calcium (supplements) .20
<800 282 0.65 313 0.74 0.88 (0.75- 1.04)
800 to <1,200 186 0.56 204 0.63 0.88 (0.72- 1.08)
2: 1,200 259 0.53 269 0.54 0.98 (0.83- 1.17)
Baseline total vitamin D (supplemems) .59
<200 275 0.56 303 0.64 0.88 (0.74-!.03)
200 to <400 144 0.60 150 0.62 0.98 (0.78-1.23)
400 to <600 170 0.58 189 0.63 0.92 (0.75-1.14)
::-600 138 0.58 144 0.62 0.93 (0.73-1.17)
Latitude of clit1ical center .70
Southern: <35 north 232 0.60 255 0.67 0.8910.74-1.06)
Middle: 35-40 north 209 060 238 0.69 0.86 (0.71- 1.03)
N())1hern: >40 north 303 0.55 314 0.57 0.96 (0.82- 1.13)
Blood prc.<sure .39
Treated 237 0.77 278 0.92 0.84 (0.70- 1.00)
;::: 140/90 305 0.64 307 0.65 0.98 (0.84-1.15)
Normal 202 0.40 222 0.45 0.90 (0.75-!.09)
Smoking .20
Never smoked 326 0.49 322 0.48 1.0 I (0.86-1.17)
Past smoker 300 0.59 355 0.7 1 0.83 (0.71-0.97)
CmTent smoker 108 1.11 120 1.28 0.87 (0.67-1.13)
Pbysical activity IMETs/wk) .06
53.00 237 063 278 0.75 0.85 (0.71- 1.01)
>3.00 to <11.75 2 18 058 249 0.66 088 (0.73- 1.06)
2: 11.75 188 0.49 179 0.47 1.03 (0.84- 1.26)
No. of CVD risk factors .59
None 130 0.32 153 0.38 0.85 (0.67-1.08)
1-2 596 0.69 616 0.73 0.95 (0.85-1.07)
;:::3 18 0.89 38 1.70 0.49 (0.27-0.87)
Body mass index. kgtm2 .49
<25 197 0.58 216 0.63 0.93 (0.76-1.12)
25 to <30 232 0.51 261 0.57 0.89 (0.74- 1.06)
::::30 3 15 066 328 0.70 0.93 (0.80- 1.09)
History of CVD .90
No 645 0.54 694 0.58 0.92 (0.82- 1.02)
Yes 99 1.25 113 1.38 0.91 (0.70- 1.20)
Number of chronic conditions* .67
None 95 0.32 107 0.36 0.86 (0.65-1.14)
300 0.52 298 0.52 1.00 (0.86-1.18)
2 244 0.72 283 0.84 0.86 (0.72-1.02)
3 or more 105 1.49 119 1.73 0.87 (0.66-1.13)
Self-reported health status . 13
Excellent 84 0.39 79 0.36 1.14 (0.83- 1.55)
Very good 296 0.52 305 0.54 0.93 (0.79- 1.09)
Good 273 067 304 0.75 0 89 (0.76- 1.05)
Fair 79 0.99 106 1.28 0 79 (0.59- 1.06)
Poor 12 231 13 3.07 051 (0. 18- 1.43)
Notes: ~ t D =calcium and vitamin D: CJ = coniidenc.: interval; CYD =cardiovascular disease; HR = hazard ratio; HT = h(nmone therapy; MET= metabolic equivalent.
HRs and 95% Cis are derived from Cox proportional hazards models suatified by age and randomization in the WH! dietary modification or HT trial, or both.
t 1> values are for the interaction between the subgroup variable and treatment assignment.
t Number of chronic conditions includes self-report of coronary heart disease. congestive heart failure. treated diabetes. hypertension (treated or untreated). hip
fracture. emphysema. cancer, or artluitis. HT at annual visit J includes randomized treatment assignment in the WHI HT trial aod personal use of HT.
566 IACROJX ET AL.
Table 4. ORs* for Total Mortality According to Tertile of Serum 25-Hydroxyvitamin D Level and CaD Study Group, as Determined in a Nested
Case-Control Study
Main Effect ORI (95% Cl) CaD. Cases/Controls Placebo. Cases/Controls OR(95%CD p Value for Interaction
Tertile of serum 25-hydroxy 65
vitamin D, nmoi/L
!::52.5 1.00 53/404 50/425 1.04 (0.69-1.59)
35.4-52.4 1.42 (1.06-1.91) 57/301 59/296 0.96 (0.64-1.45)
<35.4 1.46 ( 1.07- 1.99) 47/270 571266 0.79 (0.51 - 1.23)
Notes: CaD= calcium and vitamin 0; CI = c.onfidence interval; OR =odds ratios.
* ORs were derived from logi stic regressioo 01odels stratified by age group and randomization assignment io the hormone therapy or dietary ruodificarioo trial, or
both, and further adjusted for age. ethniciry (white, black, Hispanic, other), latitude of clinical center, and season of blood draw.
t Serum 25-hydroxyvitamin D main effects models are also adjusted for CaD treatment assignment.
to exert anticancer effects might be 1,500-2,000 IU/d based
on selective findings from observational studies (30,31).
The optimum dose of vitamin D for reducing cancer or mor-
tality is unknown and, if it exists, can only be deteiTnined
from future large randomized trials.
The trends toward reductions in risks of both cardiovascular
and cancer mortality in this trial, if real, suggest mechanisms
that may have broad physiological effects. Vitamin D supple-
mentation has been shown experimentally to increase levels of
the anti-inflammatory cytokine interleukin-10, while prevent-
ing increases in tumor necrosis factor alpha (32). Calcium and
vitamin D supplementation both lower parathyroid h01mone
levels (PTH), and PTH levels have been associated with an
increased risk of mortality in a vitamin D-<leficient cohort of
the very old age (33). Chronic metabolic acidosis increases
with age and declining kidney function even when plasma
measures of acid-base balance are normal. Administration of
bicarbonate has been shown to reverse acidosis (34,35). Ben-
eficial effects of CaD supplementation on cytokine profiles,
PTH, or acidosis might be expected to produce greater bene-
fits in older women, whereas the opposite trend was observed
in this trial. However, it is also possible that mo11ality could be
delayed by improvements in these parameters and eventually
benefits diminish with disease progression in later life.
Strengths of this trial include its large size, diversity, long
duration, excellent retention, and reasonably good adher-
ence for an average of 7 years of follow-up. This study is
limited by Jack of statistical power for detecting interven-
tion effects on mortality, as it was not designed for this pur-
pose. We did not collect postintervention serwn specimens
for exploring potential intermediate effects of the interven-
tion that might have influenced mortality. We cannot distin-
guish between effects of calcium, vitamin D, or carbonate
because the intervention combined these ingredients. We do
not know whether higher supplement doses of vitamin D
would have produced different results.
In conclusion, the WHI CaD tiial supports the hypothesis
that CaD supplementation provides a modest reduction in rates
of total and categories of cause-specific mortality, but the re-
sults are too imprecise to be definitive. Moreover, these data
can neither support nor refute recommendations for higher
dose vitamin D supplementation to reduce cancer or total
mortality. This hypothesis merits further consideration by test-
ing altemative underlying mechanisms and possibly by testing
higher dose supplements in even larger randomized trials.
SUPPLEMENTARY MATERIAL
Supplementary material can be found at: http://biomed.
gerontology j ournals. org/.
ACKNOWLEDGMENTS
The autJJOrS thank the WHJ investigators, staff. and study participants for
their outstanding dedication and commitment. A list of key investigators in-
volved in this research follows: A full listing of WHI investigators can be
found at the following Web site: bttp://www.whi.org. A.Z.L. affinns that ev-
etyone who significantly contributed to this work has been listed in the Ac-
The WHI investigaton; and National Institutes of Health
sponsors all contributed to the design and execution of the study. This work
was supported by the National Heart, Lung, and Blood Institute of the U.S.
Department of Health and Human Services. The active study drug and pla-
cebo were suppl ied by GlaxoSmithKii ne Consumer Healthcare (Pittsburgh).
Clinical Trials Registration: ClinicaiTrials.gov identifier: NCf00000611
CORRESPONDENCE
Address correspondence to Andrea z. LaCroix, PhD, WHJ Clinical Co-
ordinating Center, Fred Hutchinson Cancer Research Center, J 100 Fairview
Avenue North. M3-A410, P.O. Box 19024. Seattle, WA 9RI09-1024.
Email : alacroix@wbi.org
REFERENCES
L Jackson RD. LaCroix AZ, Gass .M, eta! for tbe Women's Health Ini-
tiative Investigators. Calcium plus vitamin D supplementation and
the risk of fractures. N Eng/ J Med. 2006;354:669-683.
2. Prince RL, Devine A. Dhaliwal SS, Dick lM. Effects of calcimn
supplementation on clinical fracture and bone structure: results of a
5-year, double-blind, placebo-controlled ttial in elderly women. Arch
Intern Med. 2006;166:869-875.
3. Trivedi DP, Doll R. Khaw KT. Effect of four monthly oral vitamin D3
{cholecalciferol) supplementation on fractures and mortality in men
and women living in the community: randomized double blind con-
trolled trial. BMJ. 2003;326:1 - 6.
4. Autier P. Gandini S. Vitamin D supplementation and total mottalit.y:
a meta-analysis of randomized controlled trials. Arch Intern Med.
2007;167: 1730-1737.
5. Wactawski-Wende J. Kotchen JM. Anderson GL et al. For the Women's
Health Initiative Investigators. Calcium plus vitamin D supplementation
and the risk of colorectal cancer. N Eng/ J Med. 2006;354:684-696.
6. The Women's Health Initiative Study Group. Design of the Women's
Health Initiative clinical trial and observational study. Control Clin
Trials. 1998;19:61-109.
7. Jackson RD, LaCroix AZ, Cauley JA, et al. The Women' s
Health Initiative Calcium-Vitamin D Trial: overview and baseline
CALCIUM PLUS VITAMIN D AND MORTALITY 567
characteristics of participants. Ann Epidemio/, (suppl9) 2003; 13:
598-106.
8. Cox DR. Regression analysis and life tables. J R Stat Soc. 1972;
34: 187-220.
9. Robins JM, Finkelstein DM. Correcting for noncompliance and depen-
dent censoring in an AIDS clinkal trial with inverse probability of cen-
soring weighted (IPCW) log-rank tests. Biometrics. 2000; 56:779-781.
10. Appel LJ, Moore TJ, Obarzanek E, eta!. A clinical trial of the effects
of dietary pmterns on blood pressure. DASH Collaborative Research
Group. N Eng/ J Med. 1997;336: 11 17- 1124.
11. Groot PHE, Grose WFA, Dijkbuis-Stoffelsma R, Fernandes J,
Ambagtshcer JJ. The effect of oral calcium carbonate administration
on serum lipoproteins of children with famil ial hypercholesterolae-
mia (type II-A). Eur J Pediatr. 1980:135:81-84.
12. Denke MA, Fox MM, Schulte MC. Short-term dietary calcium forti-
fication increases fecal saturated fat content and reduces serum lipids
in men. J Nutr. 1993;123: 1047-1053.
13. Bell L, Halstenson CE, Halstcnson CJ, Macrcs M, Keane WF.
Cholesterol-lowering effects of calcium carbonate in patients with
mild to moderate hypercholesterolemia. Arch Imem Med. 1992; 152:
2441-2444.
14. Abboll RD. Curb JD, Rodrigues BL. Sharp DS, Burch lie! CM, Yano K.
Effect of dietary calcium and milk consumption on risk of thromboem-
bolic stroke in older middle-aged men. Stroke. 1996;27:813-818.
15. lso H, Stampfer MJ, Manson JE, et al. Prospective study of calcium,
potassium and magnesium intake and risk of stroke in women. S1roke.
1999;30: 1772-1779.
16. Umesawa M, lso H, Date C, et al. For the JACC Study Group.
Dietary intake of calcium in relation to mortality from cardiovascular
disease: the JACC Study. Stroke. 2006;37:20-26.
17. Bostick RM, Kushi LH, Wu Y, Meyer KA, Sellers TA, Folsom AR.
Relation of calcium. Vitamin D. and dairy food intake to ischemic
heart disease mortality among postmenopausal women. Am J Epide-
miol. 1999;149: 151-161.
18. Yonder Recke P, Hansen MA, Hassager C. The association between
low bone mass at the menopause and cardiovascular mortality. Am .T
Med. 1999:106:273- 278.
19. Browner WS, Seeley DG. Yogt TM, Cummings SR. Non-trauma
mo1tality in elderly women with low bone mineral density. Study of
Osteoporotic Fractures Research Group. Lancet. 1991 ;338:355-358.
20. Hsia J, Heiss G. Ren H, et al. For the Women's Health Initiative In-
vestigators. Calcium/vitamin D supplementation and cardiovascular
events. Circulation. 2007;1 15:846- 854.
21. Grant WB. Epidemiology of disease risks in relation to vitamin D
insufficiency. Prog Biophys Mol Bioi. 2006;92:65-79.
22. Boscoe FP, Schymura MJ. Solar ultraviolet-B exposure and cancer
incidence and mortality in the United States. 1993-2002 BMC
Cancer. 2006;6:264-272.
23. GiovarulUcci E. The epidemiology of vitamin D and cancer incidence
and mortality: a review (Uni ted States). Cancer Causes Control.
2005:16:83-95.
24. Feskanich D, Ma J, Fuchs CS, et al. Plasma vitamin D metabolites
and risk of colorcctal cancer in women. Cancer Epidemiol Biomark-
ers Prev. 2004: 13:1502-1508.
25. Freedman DM. Looker AC, Chang SC, Graubard BI. Prospective
study of serum Vitamin D and cancer mortality in the United States.
J Nat/ Cancer fnst. 2007;99:1594-1602.
26. Lappe JM. Travers-Gustafson D, Davies KM, Recker RR. Heaney
RP. Vitamin D and calcium supplementat ion reduces cancer risk:
results of a randomized trial. Am J Clin Nuir. 2007;85:
1586- 1591.
27. Melamed ML, Michos ED, Post W, Astor B. 25-Hydroxyvitamin D
levels and the risk ofmoltality in the general population. Arch lntem
Med. 2008;168: 1629- 1637.
28. Dobnig H. Pilz S, Schamagl H, et at. Independent association of low
serum 25-IJydroxyvitamin D and 1,25-dihydroxyvitamin D levels
with all-cause and cardiovascular mortality. Arch Intern Med. 2008;
168:1340- 1349
29. Vieth R, Bischoff-Ferrari H, Boucher BJ, et a!. The urgent need to
recommend an intake of vitamin D that is effective [Editorial]. Am J
Clin Nutr. 2007;85:649-650.
30. Bischoff-Ferrari HA. The 25-hydroxyvitamin D threshold for better
health. J Steroid Biochem Mol Bioi. 2007;103:614-619.
31 . Giovannucci E. Liu Y, Rimm EB, et al. Prospective study of predic-
tors of vitamin D status and cancer incidence and mortality in men.
J Nat/ Cancerlnst. 2006;98:451-459.
32. Schleithoff SS. Zittermann A. Tenderich G. Berthold HK. Stehle P.
Koerfcr R. Vitamin D supplementation improves cytokine profiles in
patients with congestive heart fai lure: a double-blind, randomized,
placebo-controlled trial. Am J Clin Ntar. 2006:83:754-759.
33. Sambrook PN, Chen JS, March LM, et al. Serum parathyroid
hormone is associated with increased mortality independent of
25-hydroxy vitamin D status, bone mass. and renal function in the
frai l and very old: a cohort study. J Clin Endocrirwl Metab. 2004;
89:5477-5481.
34. Frassetto LA. Morris RC, Sebastian A. Effect of age on blood acid-
base composition in adult humans: mle of age-related renal functional
decline. Am J Physiol. 1996;271 (6 Pt 2):FII I4-Fl 122.
35. Frassetto L. Morris RC. Jr. Sebastian A. Potassium bicarbonate
reduces urinary nitrogen excretion in postmenopausal women. J Clin
Endocrinol Mewb. 1997;82:254-259.
Received July 6, 2008
Accepted December 23, 2008
Decision Editor: Luigi Ferrucci, MD, PhD
THE WALL STREET JOURNAL
Date:
l ocation:
Friday. April 18, 2008
NEW YORK, NY
302,393 (1)
Newspaper (D)
Circul ation (DMA):
Type (Frequency):
Page: 611
Keyword: dermatology
Researcher Received Industry Funds
Medical-JournalAuthor
Was Backed by Group
Tied to Indoor Tanning
BY DAVID ARMSTRONG
A Boston University researcher who
authored an article in the New England
Journal of Medicine last year recom-
mending the moderate use of tanning
beds as a way to treat or avoid vita-
min-D deficiency has received research
funding from an organization funded
and controlled by the tanning-bed in-
dustry.
The link to researcher Michael Hol-
ick's work and the tanning industry
wasn't made clear in the article. A
note at the end of the article dis-
closed that Dr. Holick's research was
funded, in part, by the UV Founda-
tion. No information about the foun-
dation was provided.
The nonprofit foundation, accord-
ing to its Web site, is funded by the In-
door Tanning Association as well as
the makers of tanning-bed equipment.
The board of directors is composed en-
tirely of tanning-bed -industry offi-
cials. Boston University was the top re-
cipient of grants from the foundation
from 2004 through 2006, the most re-
cent three years oft he group's Internal
Revenue Service filings. In total, the
university received $162,014 during
that period.
On its Web site, the UV Foundation
said it "has made a commitment of
$150,000 over three years to Boston
University, to continue the efforts of
Dr. Michael Holick, a Vitamin D expert."
The site said the foundation "is dedi-
cated to exploring the positive effects
of UV light and to increasing public
awareness about those benefits."
Dr. Holick said in an interview that
the money was an unrestricted grant
that he used for vitamin-D research.
A report on the funding arrange-
ment was to appear in Friday's edition
of the Cancer Letter, a Washington-
based trade publication.
A spokeswoman for the New Eng-
landJownalsaid "wewereawareofthe
source of funding and disclosed it. We
looked at the Web site and saw that the
inf01mation was available and felt the
inf01mation was publicly available."
Copyrigh12008
Please contl'let lhe poblisher lOt reprints.
Dr. Holick said he complied with all dis-
closure requests from the journal.
Questions over disclosures of poten-
tial conflicts have been growing at med-
ical journals. Two weeks ago, the New
England Journal corrected the record
on a lung-cancer-screening study pub-
lished in 2006 to show some of the au-
thors were receiving previously undis-
closed royalties from General Electric
Co., a big scanner make1; and also get-
ting research funding from tobacco
company Vector Group, the parent of
Liggett Group LLC.
The current NEJM policy for review
articles requires that authors "not
have major research support" from rele-
vant companies. Dr. Holick said the
funds were about 2% of his total re-
search budget. The NEJM spokes-
woman said that amount was within
the jow'Jlal's guidelines.
Dr. Holick's article didn't repmt new
research but made recommendations
based on a review of published studies.
Tanning beds were cited as a "recom-
mended" source of vitamin D when
used in moderation.
That concerned some cancer spe-
cialists, who note that ultraviolet rays
used in indoor tanning have been
linked to an increased risk of cancer in
some studies.
"I was surprised that the New Eng-
land Journal, a very prestigious jow-
nal, would run the article this way,"
said Ma1tin Weinstock, a Brown Univer-
sity professor. He said he
was surprised t e journal would run a
piece by an industry-funded author.
-> The Situation: A Boston University
researcher authored an article last year
recommending moderate use of
tanning beds for vitamin-D deficiency.
-:. Industry Funding: The author has
received research funding from an
organization controlled by the
tanning-bed industry.
-:. Disclosure Issues: Questions over
disclosures of potential conflicts have
been growing at medical journals.
Account: 7470NX (3159)
NY-472
Page 1 of 1
Vitamin D in the prevention and treatment of coronary heart
disease
Armin Zittermann and Reiner Koerfer
Department of Thoracic and Cardiovascular Surgery,
Heart and Diabetes Center North-Rhine Westfali a,
Ruhr University Bochum, Bad Oeynhausen, Germany
Correspondence to Armin Zittermann, PhD, Associate
Professor, Department of Thoracic and Cardiovascular
Surgery, Heart and Diabetes Center North-Rhine
Westfalia, Ruhr University Bochum, Georgslra6e 11,
32545 Bad Oeynhausen, Germany
Tel: +49 573 1 97 1912; fax: +49 5731 97 2020;
e-mail: azit1ermann@hdz-nrw.de
Current Opini on In Clinical Nut rition and
Met abol ic Care 2008, 11 :752-757
Introduction
Purpose of review
The pathogenesis of coronary heart disease is of multifactorial origin. Probably, not all
risk factors are satisfactorily understood. This article outlines beneficial vitamin D effects
on cardiac function and the vasculature. In addition, human data associating serum
vitamin D metabolite levels or oral vitamin D dosages or both with coronary heart disease
outcome parameters are reviewed.
Recent findings
There is accumulating evidence that the vitamin D hormone calcitriol exerts important
physiological effects in cardiomyocytes, vascular smooth muscle cells, and the vascular
endotheli um. Low levels of the calcitriol precursor 25-hydoxyvitamin D are associated
with myocardial infarction, congestive heart fail ure, and calcific aortic stenosis. Deficient
calcitriol concentrations probably contribute to the massive vascular calcification seen
in chronic kidney disease. In patients with end-stage renal disease and end-stage heart
failure, very low-circulating calcitriol levels or nonuse of active vitamin D or both are
independently associated with high mortality rates.
Summary
Despite these exciting data, it is still too early to recommend exact dosages for the
prevention or therapy of coronary heart disease. Prospective, randomized controlled
trials with different amounts of vitamin D and probably with its active form calcitriol are
needed to determine whether vitamin D can prevent coronary heart disease events and
mortality.
Keywords
calcitriol, coronary heart disease, mortality, survival, vascular calcification, vitamin D
Curr Opin Clin Nutr Metab Care 11:752- 757
2008 Wolters Kluwer Health I Lippincott Williams & Wilkins
1363-1 950
Coronary heart disease (CHD), also called coronary artery
disease or ischemic heart disease, is the result of the
accumul ation of atheromatous plaques within the walls of
the arteries that supply the myocardium with oxygen and
nutri ents. After decades of progression, some atheroma-
tous plaques may rupture and may thus severel y restri ct
the flow of oxygen carrying blood to the myocardium. As a
consequence, a heart arrack can occur. l\llyocardial infarc-
tions are the most common cause of sudden death in
western countries. In the USA and Germany, CHD is
responsible for one in fi ve deaths. The WHO estimated
that in 2002, 12.6% of deaths worldwide were from CHD
[1]. CHD is also one of the major causes of congestive
heart failure, another prevalent disease in western
countries that is characterized by fai lure of the heart to
supply adequate blood flow and therefore oxygen deliv-
ery co peripheral ti ssues and organs or co do so only from
elevated filling pressures. The prevalence of congestive
heart failure is 2.0% in patients aged 40- 59 years and
rises to 12.0% in patients who are 80 years and older [2].
This review summarizes recent experimental and epide-
mi ological evidence for a role of vitamin D in the pre-
vention of CHO. In additi on, available data concerning
the effect of vitamin D on cardiovascular and total
mortality are presented.
Vitamin D and the heart
The active form of vitamin D, 1,25-dihydroxyvitamin D
or calcitriol, is the end product of two hydroxylation steps
of vitamin 0: a hepatic 25-hydroxylation and a sub-
sequent renal !a-hydroxylation. Calcitriol exerts geno-
mic and nongenomic effects through a cytosolic vitamin
D receptor (VDR) and a membrane bound receptor.
VDRs have been found in almost all human tissues
and cells, among them cardiomyocyces, endothelial
cells, and vascular smooth muscle cells. Several tissues
also possess an enzymatically active 25-hydroxyvitamin
o-la-hydroxylase system, among them vascular smooth
muscle cells [3]. However, cardiomyocytes do not possess
1363 1950 2008 Wolters Kluwer Heal th ! Lippi ncott W illiams & W ilkins 001:10.1 097/MCO.Ob013e328312c33f
Copyright Lippincott Willi ams & Wilkins. Unauthorized reproduction of this article is prohibited.
such a 1-a-hydroxylase activity [4). Therefore, the car-
diac muscle strongly depends on the circulating blood
concentration of calcitriol. It is noteworthy that renal
calcitriol synthesis and thus circulating calcitriol concen-
trations become substrate dependent, that is, dependent
on the circulating 25-hydroxyvitamin D [25(0H)D] con-
centration, in case of vitamin D deficiency/insufficiency.
lt is therefore an important finding that in postmenopau-
sal women, calcitriol concentrations were reduced by
approximately one-third in patients with deficient
25(0H)D levels ( < 25 nmol/1) compared with adequate
levels (>80 nmol/1) [5]. Moreover, in severely obese
patients (BMI > 40 kg/m
2
), 25(0H)D levels were
20 nmol/1 lower compared with patients with a BMI less
than 25 kg/m
2
[6]. These two subgroups also differed
significantly in serum calcitriol levels (by 20 pmol/l). Data
are in line with the fact that both, some postmenopausal
women and obese patients, have an enhanced risk for
CHD.
Experimental vitamin D effects on cardiomyocytes
Calcitriol affects the growth, proliferation, and morpho-
logy of murine cardiomyocytes (Fig. 1). In detail, treat-
ment with calcitriol increased the expression of the
cardiac muscle protein myotrophin. Calcitriol treatment
also decreased expression of atrial natriuretic peptide, a
biochemical risk marker that is inversely related to car-
diac function. In addition, calcitriol treatment increased
expression and nuclear localization of the VDR in these
cells [7]. Murine cardiomyocytes isolated from VDR
knockout mice show accelerated rates of contraction
and relaxation as compared wi th wild type mice, and
calcitriol directly affected contractility in the wild type
but not the knockout cardiomyocyte [8]. Thus, calcitriol
is an important hormone involved in modulating and
maintaining heart cell structure and function. The afore-
mentioned study group [9] has also demonstrated that
the heart of VOR knockout mice is hypertrophied
because of cellular hypertrophy of heart myofibrils.
Microarray analysis revealed tissue inhibitors of metallo-
proteinases were significantly underexpressed in VDR
knockout mice compared with wi ld type mice [10].
Matrix metalloproteinases (MMPs) are connective tissue
enzymes that are involved in remodeling of the vascular
wall and myocardium. They function to destabilize athero-
matous plaques to cause rupture and thrombosis within
the lumen. Extracellular matrix remodeling mediated by
MMPs contributes to progressive left ventricular remo-
deling, dilation, and heart failure. Experimental data
suggest that calcitriol may prevent the development of
cardiac hypertrophy. In spontaneously hypertensive
heart fai lure rats, calcitriol treatment resulted in lower
heart weight, myocardial collagen levels, left ventricular
diameter, and cardiac output compared with untreated
rats [111.
Vitamin D in the prevention of CHD Zittermann and Koerfer 753
Vitamin D and cardiac events
During the last decade, it became clear that deficient
serum concentrations of vitamin D metabolites are preva-
lent not only in specific patient groups but also in the
general population in western countries and throughout
the world [121. The by far most important reason for this
phenomenon is an inadequate skin exposure ro solar
ultraviolet B radiation, as ultraviolet B-induced skin
synthesis is the major source of vitamin D for humans.
Ecological studies have reported hi gher rates of CHD
with increasing distance from the equator, a phenomenon
that can be attributed to the higher prevalence of vitamin
D deficiency in regions with less exposure to sunlight.
In a nonrandomized prospective study in 1739 Framing-
ham Offspring Study participants, individuals with low
25(0H)O levels ( <37.5 nmol/1) had a multivariable-
adjusted hazard ratio of 1.62 for incident cardiovascular
disease such as myocardial infarction, coronary insuffi-
ciency, and heart failure compared with those with
25(0H)D levels of at least 37.5 nmol/1 [13.]. In the
Women's Health Initiative study, however, myocardial
infarction, ischemic attack, hospitalization rate for heart
failure, and cardiovascular death could not be prevented
by supplementation with 1000 mg calcium and 10 fl-g
vitamin D daily compared with the placebo group [14].
But several li mitations such as the low daily vitamin D
dose and the lack of measurements of serum 2S(0H)D
levels or of calcitriol or of both of the vitamin D arm of
this srudy makes data interpretation difficult [15]. In a
nested case- control study among male participants of the
Health Professionals Follow-up Study [1 6.], men with
low 25(0H)D levels ~ 3 7 . 5 nmol/1) had a relative risk of
2.09 [95% confidence interval (Cl) 1.24- 3.54] of myo-
cardial infarction compared with those considered to
be sufficient (:;75 nmol/1), after adjustment for various
lifestyle and other risk factors. Very recently, data on all-
cause and cardiovascular mortality in association with
vitamin 0 status have been published from a prospective
cohort study of 3258 consecutive male and female
patients scheduled for coronary angiography [171.
During a median follow-up period of 7.7 years, 737
patients (22.6%) died, including 463 deaths from cardio-
vascular causes. Multivariate-adjusted hazard ratios for
patients in the lower two ZS(OH)D quartiles (median,
19.0 and 33.3 nmol/1) were higher for all-cause mortality
(hazard ratio 2.08; 95% CI 1.60-2.70; and hazard ratio
1.53, 95% CI 1.17 -2.01, respectively) and for cardiovas-
cular mortality (hazard ratio 2.22; 95% CI 1.57 - 3.13; and
hazard ratio 1.82, 95% CI 1.29- 2.58, respectively) com-
pared with patients in the highest 25(01-I)O quartile
(median, 71.0 nmol/1). Similar results were obtained for
patients in the lowest calcitriol quartile. A trend toward
lower mortality was already observed in a British vitamin
D intervention trial [18]. T he vitamin D group recei ved
one capsule containing 2500 fl-g vitamin 0
3
every
Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
754 Functional foods
Figure 1 Biochemical and clinical effects of low calcitriol availability on cardiac and vascular function
Low serum levels of Chronic kidney
25-hydroxyvitamin D disease
t t
Low cellular availabi lity of calcitriol
/
}
Enhanced synthesis andjor Reduced synthesis of Disturbed cardiomyo- Reduced synthesis
enhanced deleterious effects MGP, osteopontin, cyte contraction of inhibitors of MMPs
of MMPs, TNF- ex, IL-1, IL-6, IL-10, and type IV Enhanced synthesis of and cardiac muscle
contracting factors, and AGEs collagen natriuretic peptides protein
Vascular calcifi cation Cardiac hypertrophy
Coronary heart disease
!
Myocardial infarction Heart fail ure
!
I
Death
I
I
AGEs, advanced glycation end products; IL-1, interleukin-1; IL-2, interleukin-2; MGP, matrix Gla protein; MMP, matrix metalloproteinases; TNF, tumor
necrosis factor.
4 months over 5 years (equivalent w 211-Lg vitamin D per
day). In subgroup analysis, serum 25(01-I)D concen-
trations were 21 nmol/1 higher in the active vi tamin 0
group compared with the placebo group. The rare ratios
for cardiovascular diseases, cancers, and coloreccal can-
cers incidences were 0.90 (0. 77 -1.06), 1.11 (0.86- 1.42),
and 1.02 (0.60-1.74), respectivel y. For mortality, these
ratios were 0.84 (0.65-1.20), 0.86 (0.61 - 1.20), and 0.62
(0.24- 1.60), respectively. Hence, though statistical sig-
nificance was not achieved, incidence rate ratios were
always close to 1.0, whereas mortality rate ratios were
always lower, suggesting that the protective effect of
vitamin D on cardiovascular and cancer mortality is more
effective than irs effect on disease incidence. In line with
this suggestion, a metaanalysis of controlled clinical trials
came co the conclusion that vitamin 0 supplementation
reduced total mortality in middle aged to elderly adul ts
by 7% during a trial size-adj usted mean of 5. 7 years [19 ].
In the vitamin 0 -suppl emented patients and controls,
mean serum 25(0H)O concentrations increased by
40 nmol/1 and decreased by 6.5 nmol/1, respectively.
Although the authors could not evaluate cause-specific
mortality, the relatively immediate effect of a large
enough magni tude co influence coca! mortality would
suggest a preventive effect on Cl-IO morcalicy.
Vitamin D and congestive heart failure
The aforementioned experimencal data and several
clinical results indicate that adequate vitamin 0 metab-
olite levels may contribute to the prevention of conges-
tive heart failure (CHF). In a recent study in 43 men and
17 women \Vith left ventricular ejection fraction of 40%
or less, longer 6 min walk distance was correlated with
higher 25(0H)D levels [20.]. The 6 min walk distance is
a frequently used cest in heart fai lure patients to assess
functi onal cardiac outcome. Other independent vari ables
of the 6 min wal k distance were age, sex, and hi ghly
sensi ti ve C-reactive protein levels. A case-controlled
study [21] showed that lifestyle factors associated with
adequate vi tamin D status such as membership in a sports
club, frequent summer holidays, and li ving in rural areas
were less frequently reported for the period of childhood,
Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
adolescence, and young adulthood by CHF patients
compared with healthy controls. Data indicate that
vitamin D insufficiency/deficiency is a causal factor of
CHF and not just the result of disease-related alterations.
Very low serum calci triol levels ( <37.5 pmol/1) have fre-
quently been found in end-stage heart failure patients
[22""]. In this study, patients in the highest calcitriol
tertile had a hazard ratio for an event (death or cardiac
transplantation) of only 0.506 (95% CI 0.334- 0. 767)
compared with patients in the lowest calcitriol tertile,
after adjustment for potential confounders. Data
support the assumption that low vitamin D metabolite
levels are a risk factor for survival and that vitamin D
seems to be a very important protective factor for
cellular health.
Vitamin D and the vasculature
Classical risk factors in the pathogenesis of CHD are
smoking, dyslipoproteinemia, hypertension, disturbed
glucose metabolism, and proinfiammatory processes.
Until recently, vascular calcification was considered to
be a passive process that occurred as a nonspecific
response to vascular damage without clinical significance.
However, there is no-..v accumulating evidence that vas-
cular calcificat ion is an acti ve process [23""]. Almost all
angiographically atherosclerotic lesions are calcified [24].
Vascular calcification can cause thrombosis, arterial rup-
ture, and myocardial infarction. In general, the develop-
ment of tissue calcification requires a preexisting injury as
an inducer, whereas further progression requires the
presence of other promoter factors such as hyperpho-
sphatemia and hypercalcemia or a deficiency in calcifica-
tion repressor factors or both [251.
Experimental vitamin D effects on the vasculature
Beside the heart, the vasculature is an important target
tissue for vitamin D. Available data concerning protective
effects of vitamin 0 on the vasculature have recently
been summarized [23""]. These effects include calcitriol-
mediated downregulation of MMPs and proinflammatory
cytokines such as IL-l, IL-6, and TNF-a (Fig. 1). The
effects also include upregulation of the anti-inflammatory
cytokine IL-10 and of inhibitors of vascular calcification
such as matrix Gla protein (MGP), osteopontin, and
type IV collagen in vascular smooth muscle cells and
osteoblast-like cells. In addition, calcitriol blunts the
deleterious impact of advanced glycation end products
(AGEs) on endothelial cells [26"). AGEs are believed
to induce vascular dysfunct ion in diabetic and uremic
patients and may explain the link between hyper-
glycemia and the development of vascular complications.
In experimental studies with rings of spontaneously
hypertensive rats aorta, calcitriol treatment reduced the
Vitamin D in the prevention of CHD Zittermann and Koerfer 755
acetylcholine-induced and ATP-induced endothelium-
dependent contractions [27"]. Moreover, the acetyl-
choline-induced release of prostacyclin was reduced by
the acute administration of calcitriol. Calcitriol also
reduced the increase in cytosolic free calcium concen-
tration caused by acetylcholine. These data demonstrate
that calcirriol modulates vascular cone by reducing
calcium influx into the endothelium and hence decreas-
ing the production of endothelium-derived contracting
factors.
Vitamin D deficiency and vascular calcification
in chronic kidney disease
Obviously, chronic kidney disease (CKD) can be con-
sidered as a human model for the effects of calcitriol
deficiency on vascular calcification and Cl-IO mortality.
In CKD, both calcitriol deficiency and vascular calcifica-
tion are extremely common. DistUrbances in mineral
homeostasis such as hyperphosphatemia and hyperpar-
athyroidism seem to be secondary to calcitri ol deficiency
and are obviously key factors for medial calcification
[23""]. End-stage renal disease (stage 5 CKD) results
in glomerular filtration rates below 15 ml/min/1.73 m
2
.
As a consequence, circulating calcitriol levels fall below
37.5 pmol/1 (reference range 40- 150 pmol/1). In end-stage
renal disease, the age-standardized risk for cardiovascular
events and mortality is 37 times and 10-20 times,
respectively, higher than in the general population [23""].
Children on dialysis with calcitriollevels helow 40 pmol/1
or ahove 150 pmol/1 had significantly higher cardiac cal-
cification score than controls and patients wi th calcitriol
levels in the reference range [28""]. A mouse model of
CKD-stimulated atherosclerotic cardiovascular mineral-
ization demonstrated that treatment with calcitriol and
one of its analogs, paricalcitol, was protective against
aortic calcification at dosages sufficient to correct second-
ary hyperparathyroidism. However, higher dosages
stimulated aortic calcification [29"]. Data support the
assumption that both inadequately low and high vitamin
D concentrations are associated with deleterious effects
on the vasculature [30"]. In non-CKD patients, lower
serum 25(0H)D levels and higher serum parathyroid
hormone (PTH) levels were independentl y associated
with calcific aortic stenosis [31"]. In patients with type 2
diabetes and low vitamin D status [25(0H)D levels
<50 nmol/1], vitamin D treatment with a single oral
vitamin 0
2
bolus of 100000 JU (1500J.Lg vitamin 0
2
)
improved endothelial function, measured by flow medi-
ated vasodilatation, in a double-blind, parallel group,
randomized trial [.32"].
Treatment with active vitamin D and total mortality
in chronic kidney disease
Wolf eta/. [33."] reported that in CKD, serum 25(0H)D
levels of at least 25 nmol/1 or serum calcitriol levels of at
Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
756 Functional foods
least 37.5 pmol/1 were associated with reduced risk of
early mortality compared with patients who were
untreated and had 25(0H)D and calcitriol levels below
these respective values. Some studies indicate that treat-
ment of CKD with active vitamin D (0.25-0.75 !J..g/d)
reduces all -cause mortality by 16- 24% and cardiovascular
mortality by 70% (30"]. Data also indicate that the differ-
ences in survival between patients treated with different
forms of active vitamin D (calcitriol, doxercalciferol,
and paricalcitol) are small [34] . In a recent study
[35"], patients receivi ng treatment with calcit riol , 0.25-
0.5 !J..g/day, for a median duration of 2.1 years, had a
significantly lower incidence rate ratio [adjusted relative
risk (RR) 0.35, 95% CI 0.23- 0.54] for predialysis
mortality chan untreated patients. Although calcitriol
appears co be associated with greater survival, results
have to be confirmed by the use of prospect ive, rando-
mized tri als.
Conclusion
Several experimental studies demonstrate that the vita-
min D hormone calcitriol plays a pivotal role for normal
physiology of cardiomyocytes and the vasculature. Low
vitamin D metabolite levels are associated with vari ous
CHD outcome parameters such as myocardial infarction,
congestive heart fai lure, and cardiovascular mortality.
There are also exciting data that vitamin D may reduce
total mortality, especially in patients with deficient calci-
triol levels. However, it is still too earl y to recommend
exact dosages for the prevention or therapy of CHD, as
prospective, randomized controlled trials with adequate
amounts of vitamin D are Jacking.
References and recommended reading
Papers of particular interest, published within the annual period of review, have
been highlighted as:
of special interest
of outstanding interest
Additional references related to this topic can also be found in the Current
World Literature section in this issue (p. 8 18).
World Health Organization. The World Health Report 2004 - Changing
History, 2004, 1204. ISBN 924 156265X.2.
2 Parikh Nl, Vasan RS. The epidemiology of heart failure. In: Colucci WS, editor.
Atlas of heart failure, 5th ed. Philadelphia, Pennsylvania: Springer; 2008. pp.
1-1 4.
3 Somjen D, Weisman Y, Kohen F, et at. 25-hydroxyvi tamin 031 alpha-hydro
xylase is expressed in human vascular smooth muscle cells and is upregulated
by parathyroid hormone and estrogenic compounds. Circulation 2005;
111:1666-1671.
4 Hewison M, Zehnder D, Chakraverty R, Adams JS. Vitamin D and barrier
function: a novel role for extra-renal 1 alpha-hydroxylase. Mol Cell Endocrinol
2004; 215:31- 38.
5 Rejnmark L, Vestergaard P, Heickendorff L, et at. Plasma 1,25(0H)2D levels
decrease in postmenopausal women with hypovitaminosis D. Eur J Endocrinol
2008; 158:571-576.
The above is a crosssectional study in 315 healthy postmenopausal women
selected from the local background population. This study demonstrated
that circulating calcitriol levels depend on the availability of its substrate
25-hydroxyvitamin D in case of pl asma 25-hydroxyvitamin D levels below
80nmolll.
6 Konradsen S, Ag H, Lindberg F, et at. Serum 1,25-dihydroxy vitamin D is
inversely associated with body mass index. Eur J Nutr 2008; 47:87- 91.
This cross-sectional study investigated the dependency of serum 25-hydroxyvi-
tamin D and calcitriol levels on BMI in 21 87 patients. Obesity was associated with
lower 25-hydroxyvitamin D and calcitriol levels.
7 Nibbelink KA, Tishkoff DX, Hershey SO, eta/. 1,25(0H)2vitamin 03 actions
on cell proliferation, size, gene expression, and receptor localization, in the
HL-1 cardiac myocyte. J Steroid Biochem Mol Bioi 2007; 103:533- 537.
8 Tishkoff OX, Nibbelink Ka, Holmberg KH, eta/. Functional vi tamin D receptor
(VDR) in the ! tubules of cardiac myocytes: VDR knockout cardiomyocyte
contractility. Endocrinology 2008; 149:558 - 564.
This study investigated the subcellular localization of the functional VDR in adult rat
cardiomyocytes.
9 Simpson RU, Hershey SH, Nibbelink KA, eta/. Characterization of heart size
and blood pressure in the vitamin D receptor knockout mouse. J Steroid
Biochem Mol Bioi 2007; 103:521 - 524.
This study demonstrated that ablation of the VDR signaling system results in
cellul ar hypertrophy. This model supports the assumption that the vitamin D
hormone calci triol may contribute to the prevention of congestive heart failure.
1 0 Rahman A, Hershey S, Ahmed S, et a/. Heart e<tracellular matrix gene
expression profile in the vitamin D receptor knockout mice. J Steroid Biochem
Mol Biol 2007; 103:416-419.
11 Mancuso P, Rahman A, Hershey SO, el a/. 1,25DihydroxyvitaminD3 treat
ment reduces cardiac hypertrophy and left ventricular diameter in sponta
neously hypertensive heart failure-prone (cp/ +} rats independent of changes
in serum leptin. J Cardiovasc Pharmacol 2008; 51 :559-564.
Another experimental study demonstrating the pivotal role of calcitriol for normal
cardiac function.
12 Holick MF. Vitamin D deficiency. N Engl J Med 2007; 357:266 -
281.
A comprehensive overview about the reasons and consequences of vitamin D
deficiency.
13 Wang TJ, Pencina MJ, Booth SL, et at. Vitamin D deficiency and risk of
cardiovascular disease. Circulation 2008; 117:503-511.
In 17 39 Framingham Offspring Study participants, the multivariableadjusted
hazard ratio lor cardiovascular disease was 1 .62 (95% Cl 1.11 - 2.36} for
individuals with 25-hydroxyvitamin 0 levels of less than 37.5 nmol/1 compared
with those with 25hydroxyvitamin D levels of at least 3 7.5 nmol/1. This effect was
evident in patients with hypertension (hazard ratio 2.13, 95% Cl 1.30-3.48} but
not in those without hypertension (hazard ratio 1.04, 95% Cl 0.55- 1.96). Mean
follow-up was 5.4 years.
14 Hsia J, Heiss G, Ren H, et a/. Calcium/vitamin D supplementation and
cardiovascular events. Circulation 2007; 115:846- 854.
15 Zittermann A, Schleitholl SS, Koerfer R. Letter by Zitterman et at. regarding
article, 'Calcium/vitamin D supplementation and cardiovascular events'. Cir
culation 2007; 116:e85.
A letter to the editor that addresses the problems of appropriate study design and
data interpretation in vitamin D research.
16 Giovannucci E, Liu Y, Hollis BW, Rimm EB, et at. A prospective study of
25hydroxyvitamin D in relation to risk of myocardial infarction in men. Arch
Intern Med 2008; 168:1 174- 1180.
In a nested case- control study among male participants of the Health Proles
sionals Follow-up Study, the multivariableadjusted relative risk l or myocardial
infarction was 2.42 (95% Cl 1.53-3.84) lor individuals with 25-hydroxyvitamin D
levels of less than 37.5 nmol/1 compared with those with 25hydroxyvitamin D
levels of at least 75 nmol/ 1. Follow up was 1 0 years.
17 Dobnig H, Pilz S, Scharnagl H, el a/. Independent association of low serum
25-hydroxyvitamin D and 1,25-dihydroxyvi tamin D levels wi th all-cause and
carduiovascular mortality. Arch Intern Med 2008; 168:1340- 1349.
This large prospective cohort study adds further evidence l or an association of low
vitamin D status with total and cardiovascular mortality.
18 Trivedi DP, Doll R, Khaw KT, et at. Effect of four monthly oral vitamin 03
(chol ecalciferol) supplementation on fractures and mortality in men and
women living in the community: randomised double blind controlled trial.
BMJ 2003; 326:469-472.
19 Autier P, Gandini S. Vitamin D supplementation and total mortality: a meta
analysis of randomized controlled trials. Arch Intern Med 2007; 167: 1730-
1737.
A metaanalysis of 1 8 randomized controlled trials demonstrating that vi tamin
supplementation reduced the relati ve risk for total mortality to 0.93 (95% Cl
0.87 - 0.99) in middle-aged and early patients. Mean dose of daily vitamin D was
13.21'-g (ranging from 7.5 to
20 Boxer RS, Dauser OA, Walsh SJ, el at. The association between vitamin D and
inflammation with the 6min walk and frailty in patients with heart failure. Am
Geriatr Soc 2008; 56:454- 461 .
This cross-sectional study was performed in 60 patients with heart failure. Aerobic
capacity was reduced in patients with low 25-hydroxyvitamin D levels.
Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
21 Zittermann A, Fischer J, Schleithoff SS, et al. Patients with congestive heart
failure and healthy controls differ in vitamin D-associated lifestyle factors. tnt J
Vitam Nutr Res 2007; 77:280- 288.
A case- control study that investigated lifestyle factors of congestive heart failure
patients before onset of the disease. Results of 1 50 patients were compared with
150 apparently heal thy controls.
22 Zittermann A, Schleithoff SS, Gotting C, el a/. Poor outcome in end-stage
heart failure patients with low circulating calcitriol levels. Eur J Heart Fail 2008;
10:321-327.
A very large investigation on 389 congestive heart failure patients i ndicating that
low calcitriollevels are a risk factor for poor outcome (death or cardiac transplanta-
tion). This study supports the assumption that adequate circulating calcitriol levels
play a pivotal role for survival.
23 Zittermann A, Koerfer R. Protective and toxic effects of vitamin D on vascular
calcification: clinical implications. J Mol Aspects Med 2008. [Epub ahead of
print).
A comprehensive review that summarizes available data of vitamin D effects on the
vasculature and on vascular calcification.
24 Margolis JR, Chen JT, Kong Y, et a/. The diagnostic and prognostic sig-
nificance of coronary artery calcification. A report of 800 cases. Radiology
1980; 137:609- 616.
25 Grases F, Sanchis P, Perello J, et a/. Effect of crystallization i nhibitors on
vascular calcifications induced by vitamin D - A pilot study in Sprague-Dawley
rats. Circ J 2007; 71: 1152-1 156.
26 Tal mor Y, Golan E, Benchetrit S, eta/. Calcitriol blunts the deleterious impact
of advanced glycation end products (AGEs) on endothel ial cells. Am J Physiol
Renal Physiol 2008; 294:F1059-F1064.
In this experimental study, calcitriol administration blunted several metabolic
pathways in endothelial cells that are associated with the adverse effects of AGEs.
27 Wong MS, Delansorne R, ManRY, er al. Vi tamin D deri vatives acutely reduces
endothelium-dependent contractions in the aorta of the spontaneously
hypertensive rat. Am J Physiol Heart Circ Physiol 2008; 295:H289-H296.
This study adds further evidence for an important role of vitamin D in the
vasculature.
28 Shroff R, Egerton M, Bride! M, eta/. A Bimodal Association of Vi tamin D Levels
and Vascular Disease in Children on Dialysis. J Am Soc Nephrol 2008;
19:1239- 1246.
An important investigation in children on dialysis supporti ng the assumption of a
bimodal association of calcitriol levels with vascular calcification.
Vitamin D in the prevention of CHD Zittermann and Koerfer 757
29 Mathew S, Lund RJ, Chaudhary LR, el a/. Vitamin D receptor activators can
protect against vascular calcification. J Am Soc Nephrol 2008; 19:1509-
1519.
Another important study, performed in a mouse model of CKD, supporti ng the
assumption of a bimodal association of circulating calcitri ol levels with vascular
calcification.
30 Zittermann A, Schleithoff SS, Koerfer R. Vi tamin D and vascular calcification.
Curr Opinion Lipidol 2007; 18:41 - 46.
A comprehensive review of experimental and clinical data about the association of
vitamin D with vascular calcification.
31 Linhartova K, Veselka J, Sterbakova G, eta/. Parathyroid hormone and vitamin
D levels are independentl y associated with calcific aortic stenosis. Circ J
2008; 72:245 - 250.
This cl ini cal study, performed on 122 consecutive patients, showed that
low 2 5-hydroxyvi tamin D level s were an i ndependent predictor of aortic
stenosis.
32 Sugden JA, Davies Jl, Witham MD, et a/. Vitamin D improves endothelial
function in patients with type 2 diabetes mellitus and low vitamin D levels.
Diabet Med 2008; 25:320-325.
This is one of the first prospective, randomized, placebo-controlled, double-blind
studies demonstrating that vitamin D supplementation can improve endothelial
function i n humans.
33 Wolf M, Shah A, Gutierrez 0 , et a/. Vitamin D level s and early mortality
among i ncident hemodialysis patients. Kidney l nt 2007; 72: 1004-
1013.
This is a large cross-sectional analysis on 825 incident US hemodialysis patients.
The investigation demonstrated an association of baseline vitamin D levels with
90-day mortality.
34 Tentori F, Hunt WC, Stidley CA, et a/. Mortality risk among hemodialysis
patients receiving different vitamin D analogs. Kidney tnt 2006; 70:1858-
1865.
35 Kovesdy CP, Ahmadzadeh S, Anderson JE, et al. Association of acti vated
vitamin D treatment and mortality in chronic kidney disease. Arch Intern Med
2008; 168:397-403.
This investigation was performed on 520 male US veterans with CKD stages 3 - 5
not yet receiving dial ysis. The study supports the hypothesis that calcitriol may
improve survival.
Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
WORLD HEALTH ORGANIZATION
INTERNATIONAL AGENCY FOR RESEARCH ON CANCER
I ARC
Working Group Reports
Volume 1
EXPOSURE TO
ARTIFICIAL UV RADIATION
AND SKIN CANCER
This report represents the views and expert opinions of an IARC Working
Group that met in Lyon, France
27 - 29 June 2005
IARC Library Cataloguing in Publication Data
IARC Working Group on Risk of Skin Cancer and Exposure to Artificial Ultraviolet Light (2005 : Lyon,
France)
Exposure to artificial UV radiation and skin cancer I views and expert opinions of an IARC Working
Group that met in Lyon, France 27- 29 June 2005.
(IARC Working Group Reports ; 1)
1. Skin Neoplasms - epidemiology 2. Skin Neoplasms- etiology 3. Ultraviolet Rays
4. Risk Assessment I. Title II. Series
ISBN 92 832 2441 8 (NLM Classification: W1)
Contents
List of participants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v
List of abbreviations ... . ...... . .. . . . ....... . ... .. . . ....... . ......................... vii
Preamble ...... . ... . . . . . . . . .. . .. .... . . .. . ..... . .......... . ....... . ........... . .... . ix
Executive summary ...... . .. . .......... . ............... . ... . .............. . ..... . ... xi
Physical characteristics and sources of exposure to artificial UV radiation .. ................ 1
Physical characteristics of UV radiation . .......... . .......... .. ........................ 1
Units and measurements of UV radiation ..... . .... . ............... . . ................... 1
Measurement of ambient solar UV radiation . . . ........... . ........ . .. . ...... . . . . .... . .. 1
Standard erythemal dose (SED) and minimal erythemal dose (MED) ........... .. ........ . .. 2
UV index . ... . .. . .... . .... . ................ . ... . ...... . ...... ... . . .......... . . .. 2
Limit values .... . .... . .... . ...................................... . ........ . ...... 2
Sources of natural and artificial UV radiation . . ................................. . ............ 2
Solar radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Artificial UV radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Comparison of UV spectrum from sunlight and indoor tanning appliances .... . .............. . 5
European and international positions regarding artificial sources of UV radiation ... .. ........ 5
Standard for appliances designed specifically for tanning purposes .. . . . ... . . . ............... 5
National and international scientific policies .............. . . ...... . ...... . . . ............. 6
Regulations . . ... . . . .... . ........................ . ........... .. ........ . ......... 6
Biological effects of exposure to UV radiation relevant to carcinogenesis . . ...... . . .. . ...... 7
Biological lesions induced by UVA and UVB radiation ....................... . .. . ......... 7
DNA damage ......... .. .................... . ........... ... .. . ....... . .. . ........ 7
Cell damage ..... .. ... . .... . ....................... . .. . ........ . ................. 7
UVA, UVB and human skin ................. . ............. . .......... . ... . .......... 8
Differential effect of UVA and UVB on skin cancers ...... . ... . ....... . ............. . ..... 8
Experimental systems ........... . .............................. . .. . , .......... . ... 8
Relevance of experimental data to human skin cancers .. . .... . . . ... . . . ........... . ....... 8
Changes in immune response ...... . ...... . .......... . .... . ........... . .. . ........ . . . 9
Experimental systems ......... . ........... . ........... . ............ .. ... . ......... 9
Studies in humans ............. .. ... . . .. . . .. . .... . ...... . ... .. . . .......... . . . ..... 9
Effects of natural and artificial UV radiation on human skin .... . .................. .. ...... 9
Variety of skin types . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Sunburn .. . ..... . ............ . . .. ..... . .............. . . . .......... . ... . ......... 10
Tan acquisition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 0
Prevalence of exposure to artificial UV radiation for tanning purposes ....... . .. . .. . .. . ..... 11
Prevalence of exposure by region/country ... . .. . .................... . . . . . . . .... . . . . . ... 11
Time trends . ... . ..... . .... . . . .. . ........... . .... . . . ....... . .... .. . .. . . . ........... 11
Personal characteristics of adult users ........................ . .. . .. . .... . ...... . . . ... 13
Sex ..... . ........... . .... . .. . ........ . ........... . . . ........... . . . .... . . . .. . . . . 13
Age ... . .... . . . ........ . ... . .... . .... . ............ . ........ . ........... . ........ 14
iii
Exposure to Artificial UV Radiation and Skin Cancer
Skin type .................... . ....... . ............. . . . . .... ......... . ... . ....... 14
Other factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Personal characteristics of adolescent and children users . ...... ... ........... ... ........ 15
Studies of compliance to regulations and recommendations . .. . .... . .... .... ......... ... . 15
Compliance of operators . . . . .... . . .. . .... . ..... . .. . . . . . .. .... . .............. .. . .... 15
Compliance of customers ................ .. .................. . . . .. . ............ . ... 18
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and
skin cancers ..... . ... . ........ .... ................... ... ... . .. .. . . . .... . . .... . . .. .. 20
Methodology for literature search ............ . ...... ... . .. . .. . ............ .. . .. . ... .. . 20
Melanoma ............................. ........ ......................... .... ....... 21
Description of studies .................. . ......... . ... . . .. . .. . ... . ........ . . .... ... 21
Quantitative approach: meta-analysis ............................................. . . .. 25
Discussion .... . ......... . ................................. . ..................... 33
Basal cell and squamous cell carcinomas .................. . ........................... 38
Description of studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Meta-analysis ............. .. ......... ............... . . ... . . ... . ............. . ........ 40
Quality of studies ................ ..... .' .................... . ...................... 40
Other sources of exposure to artificial UV radiation ............ .... ...................... 41
Medical use ..... . .. . ... .................. . ... .. . ........ . . .. . .... . ....... . .. .. .. 41
Lighting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Effects of artificial UV radiation not relevant to skin carcinogenesis ........... ..... . ..... .. 44
Cutaneous diseases ............. . .. .. .. . . ..... .. . .. . ................... .. .......... 44
Skin ageing .......... ...... ... . ................... . .. . .. .. .. . ......... . . .. . . .... 44
Other skin diseases caused or exacerbated by exposure to UV radiation ..................... 44
Drug-induced photosensitivity .. . .... . .. . ...................... . ..................... 45
Effects on the eyes .. . . ....... . . .............. . ......... .. ..... . .................. . . 45
Cataract ...... . .......... . . . ......... . ..... . .. . .. . .. . ............... . ... .. ...... 45
Intraocular melanoma . . .... . ... ....... . .. . . . . .............. . . .... . .. .... . . . .. . .... 46
UV exposure and vitamin D ...... . .. . . .... .. . .. ... . ............................. . .. . . 46
Vitamin D formation by photosynthesis ........... . .. . . .. . . .. . . ... . . ..... ........... . . . 46
Dietary sources of vitamin D ........ . .... . .. . .. . ...... . . .... . . . . .... . .. . .... . . . .. . .. 46
Vitamin D and exposure to artifical UV radiation for tanning purposes . .............. . .... ... . 48
Vitamin D and xeroderma pigmentosum patients ..... .... . .. . . . ....... .. ....... ... .. .. .. 48
Summary and Conclusion
Summary ............... . ....... . ........ . ..... . . .. . ........ ...... ................ 49
Conclusion . ...... . .......... . . .. . ....................... .. ................... . .... 50
References ..... . ..... ... .. .... .... . ......... ................ . ..... . . . . ........... . 51
Appendix: European and international positions regarding artificial sources of UV radiation ... 61
Establishment of a standard for appliances designed specifically tor tanning purposes ....... 61
National and international scientific policies ....... . ........ . . . .... ................. . .. . 62
Regulations .... .... . .. . . ............... .. ...... . ....... . .... .. ....... . .. . ... . . . .. . 63
iv
LIST OF PARTICIPANTS
Dr Philippe Autier
I ARC
150 cours Albert Thomas
69008 Lyon
France
Dr Mathieu Boniol
I ARC
150 cours Albert Thomas
69008 Lyon
France
Dr Peter Boyle
I ARC
150 cours Albert Thomas
69008 Lyon
France
Mr J. Daniel (Technical Editor)
I ARC
150 cours Albert Thomas
69008 Lyon
France
Dr Jean-Francais Dore
INSEAM U590
Centre Leon Berard
28 rue Laennec
69008 Lyon
France
Dr Sara Gandini
Division of Biostatistics and Epidemiology
European Institute of Oncology
Milan
Italy
Professor Adele Green (Chair)
Queensland Institute of Medical Research
PO Royal Brisbane Hospital
Brisbane 4029, Queensland
Australia
Professor Julia Newton-Bishop
Cancer Research UK Genetic Epidemiology Div.
St James's University Hospital
Beckett Street
Leeds LS9 7TF
United Kingdom
Professor Martin A. Weinstock
Dermatoepidemiology Unit
Department of Dermatology
Brown University Medical School
VA Medical Center- 111 D
Providence, Rl 02908
USA
Dr Johan Westerdahl [unable to attend]
Department of Surgery
Lund University Hospital
22185 Lund
Sweden
Dr M. Beatrice Secretan (Coordinator)
I ARC
150 cours Albert Thomas
69008 Lyon
France
Dr Stephen D. Walter
Visiting Scientist at IARC until mid-July 2005
Clinical Epidemiology and Biostatistics
McMaster University
1200 Main Street West
Hamilton, Ont. L8N 3Z5
Canada
v
vi
ACGIH
sec
Cl
CIE
OF
GVHD
GP
I ARC
ICNIRP
IPO
ISO
MED
NRPB
NTP
OR
PUVA
RR
sec
SED
UNEP
uv
WHO
LIST OF ABBREVIATIONS
American Conference of Governmental Industrial Hygienists
Basal cell carcinoma
95% confidence interval
Commission lnternationale de I'Eclairage
Degrees of freedom
Graft versus host disease
General practitioner (family doctor)
International Agency for Research on Cancer
International Commission of Non-Ionising Radiation Protection
Immediate pigment darkening
International Organization for Standardization
Minimal erythemal dose
National Radiation Protection Board
National Toxicology Program
Odds ratio
Psoralen photochemotherapy
Relative risk
Squamous cell carcinoma
Standard erythemal dose
United Nations Environment Programme
Ultraviolet
World Health Organization
vii
PREAMBLE
The concern that there may be an association between exposure to artificial UV radiation and skin
cancer was reactivated in 2003-4 when the 1Oth Report on Carcinogens published by the National
Toxicology Program in the USA classified UVA radiation as a "Known Carcinogen to Humans".
In October 2004, the French Ministry of Health contacted the Director of the International Agency
for Research on Cancer (IARC) , Dr Peter Boyle, raising a particular concern about the
continuous increase in incidence of melanomas in France and in the world. Since the last IARC
Monograph on ultraviolet (UV) radiation in 1992, a large number of epidemiological and
experimental studies have been conducted on the risks associated with exposure to UV radiation. The
Ministry therefore requested IARC to investigate the possibil ity of reevaluating the carcinogenic risk
associated with this radiation, particularly concerning artificial UV sources and the use of indoor
tanning facilities.
A Working Group and a Secretariat were gathered by Dr Peter Boyle to this end. The Secretariat
met in January to prepare for the meeting of the Working Group in June 2005. The Working Group
met on 27-29 June 2005 to compile the present document.
ix
EXECUTIVE SUMMARY
We have assessed the available evidence relating to possible detrimental health effects of expo-
sure to artificial ultraviolet radiation through use of indoor tanning facilities, in particular whether their
use increases the risk for skin cancer. Epidemiologic studies to date give no consistent evidence that
use of indoor tanning facilities in general is associated with the development of melanoma or skin can-
cer. However, there was a prominent and consistent increase in risk for melanoma in people who first
used indoor tanning facilities in their twenties or teen years.
Limited data suggest that the risk of squamous cell carcinoma is similarly increased after first use
as a teenager. Artificial tanning confers little if any protection against solar damage to the skin, nor
does use of indoor tanning facilities grant protection against vitamin D deficiency. Data also suggest
detrimental effects from use of indoor tanning facilities on the skin's immune response and possibly
on the eyes (ocular melanoma) .
Knowledge of levels of UV exposure during indoor tanning is very imprecise. Moreover, early
studies published had low power to detect long-term associations with artificial UV exposure that
become evident only following a prolonged lag period. Although the available findings are therefore
not conclusive, the strength of the existing evidence suggests that policymakers should consider
enacting measures, such as prohibiting minors and discouraging young adults from using indoor
tanning facilities, to protect the general population from possible additional risk for melanoma and
squamous cell carcinoma.
xi
Physical characteristics and sources of exposure to artificial UV radiation
For most individuals, the main source of
exposure to ultraviolet (UV) radiation is the sun.
Nevertheless, some individuals are exposed to
high doses of UV through artificial sources.
Sunbeds and sunlamps used for tanning purposes
are the main source of deliberate exposure to
artificial UV radiation.
Physical characteristics of UV radiation
UV radiation belongs to the non-ionizing part of
the electromagnetic spectrum and ranges
between 100 nm and 400 nm; 100 nm has been
chosen arbitrarily as the boundary between non-
ionizing and ionizing radiation. UV radiation is
conventionally categorized into 3 regions: UVA
(>315-400 nm), UVB (>28Q-315 nm) and UVC
(> 100-280 nm) (Figure 1 ).
These categories have been confirmed by
the Commission lnternationale de I'Eclairage
(CIE, 1987), although there is variation in usage.
In the medical and biological fields, for example,
320 nm is used as the limit between UVA and
UVB. More recently, it was proposed to
distinguish between UVA-1 (>340-400 nm) and
UVA-2 (320-340 nm).
Units and measurements of UV radiation
Measurement of ambient solar UV radiation
Measurement of ambient solar UV radiation has
been performed worldwide for many years.
However, UV radiation detectors for research or
individual use have been developed only recently.
There are two principal types of instruments:
steady spectroradiometers, which screen the
entirety of the UV spectrum (1 00-400 nm) within
a few minutes, and broad-spectrum dosimeters,
which can measure solar irradiance within a few
seconds. Individual dosimeters, which can easily
be placed at strategic places on individuals, are
of the second type.
Broad-spectrum instruments often include a
weighting factor representative of a given
biological spectrum (e.g. skin erythema). In
current practice, the margin of error for the
measurement is relatively high, around 30%.
The biologically relevant UV radiation dose at
a given wavelength corresponds to the measured
UV radiation multiplied by a weighting factor
specific to the biological endpoint considered
(e.g. erythema, pigmentation, carcinogenesis,
etc.) at that wavelength. For the overall dose (Eeff
Figure 1. Ultraviolet (UV) region of the electromagnetic spectrum
---- Vacuum UV
________ u_v_c _______ _.
1
uvs u ~ ~
100
Extreme UV
10 100
Adapted from IARC (1992)
280
FarUV Middle UV
180
Wavelength (mn)
315 400
Near UV
300 380
Exposure to Artificial UV Radiation and Skin Cancer
Table 1. Specifications of relative erythemal
effectiveness
Wavelength (>..; nm)
A.< 298
298 <A< 328
328 <A::;; 400
Relative erythemal
effectiveness
(SA.) (weighting factor)
1
1 0
o.o94(298-A.)
1 0
o.o15(139-A.>
From McKinlay & Diffey (1987); International Electrotech-
nical Commission (1989)
expressed in watts per square meter (W.m-2)),
the weighted components are added for all the
wavelengths included in the interval considered.
The specifications of the relative erythemal
effectiveness are defined by the parameters
described in Table 1 .
Standard erythemal dose (SED) and minimal
erythemal dose (MED)
The standard erythemal dose (SED) is a
measure of UV radiation equivalent to an efficient
erythemal exposure of 100 joules per square
meter (J.m-
2
).
The clinically observed minimal erythemal
dose (MED) is defined as the minimal amount of
energy required to produce a qualifying
erythemal response, usually after 24h. The
erythemal responses that qualify can be either
just-perceptible reddening or uniform redness
with clearly demarcated borders, depending on
the criterion adopted by the observer.
Since 1997, the Erythemal Efficacy Spectrum
of human skin has become an International
Organization for Standardization/International
Commission on Illumination (ISO/CIE) standard
that allows, by integration with the emission
spectrum of any UV source, calculation of the
erythemal output of this source.
UVindex
The UV index is a tool designed for communication
with the general public. It is the result of a common
effort between the World Health Organization
(WHO), the United Nations Environment
2
Programme (UNEP), the World Meteorological
Organization and the International Commission
on Non-Ionising Radiation Protection (ICNIRP),
and is standardized by ISO/CIE. The UV index
expresses the erythemal power of the sun: UV
index = 40 x Eett W.m-
2
(Table 2).
Limit values
The American Conference of Governmental
Industrial Hygienists (ACGIH) and ICNIRP have
determined the maximal daily dose that a worker
exposed to UV would be able to receive without
acute or long-term effects on the eyes. This dose
has been established at 30 J.m
2
(eft), which cor-
responds to a little less than 1/3 of SED. The
value takes into account an average DNA repair
capacity in the cells.
There are currently no recommendations for
safe doses for human skin.
Sources of natural and artificial UV
radiation
Solar radiation
The sun is the main source of exposure to UV for
most individuals. Sunlight consists of visible light
(40Q-700 nm), infrared radiation (>700 nm) and
UV radiation. The quality (spectrum) and quantity
(intensity) of sunlight are modified during its pas-
sage through the atmosphere. The stratosphere
stops almost all UV radiation <290 nm (UVC) as
well as a large proportion of UVB (70-90%).
Therefore, at ground level, UV radiation
represents about 5% of solar energy, and the
radiation spectrum is between 290 and 400 nm.
An individual's level of exposure to UV varies
with latitude, altitude, time of year, time of day,
clouding of the sky and other atmospheric com-
ponents such as air pollution.
Artificial UV radiation
Artificial sources of UV radiation emit a spectrum
of wavelengths specific to each source. Sources
of artificial UV radiation include various lamps
used in medicine, industry, business and
research, and for domestic and cosmetic purposes.
Physical characteristics and sources of exposure to artificial UV radiation
(Pjrek et a/., 2004), sleep disorders and the
behavioural/activity disorders in dementia
(Skjerve et a/., 2004). The light boxes used for
such treatment can emit light levels up to approxi-
mately 10,000 lux (Pjrek et a/., 2004; Skjerve et
a/., 2004), an intensity 5 to 10 times lower than
that of bright sunlight. The emission spectrum is
variable, and some lamps may contain a small
but non-negligible proportion of UVA and UVB
(Reme et a/., 1996), which however is largely
inferior to that of indoor tanning appliances. It is
noteworthy that the UV component of the light
emitted is not involved in the therapy.
(c) Occupational exposures: Artificial sources of
UV are used in many different ways in the
working environment: some examples include
welding, industrial photoprocesses (e.g. polymer-
ization), sterilization and disinfection (sewage
effluents, drinking water, swimming pools,
operating theatres and research laboratories), pho-
totherapy, UV photography, UV lasers, quality insur-
ance in the food industry, and discotheques. For
some occupations, the UV source is well
contained within an enclosure and, under normal
circumstances, presents no risk of exposure. In
other applications, workers are exposed to some
radiations, usually by reflection or scattering from
adjacent surfaces. Of relevance, indoor tanning
facilities may comprise 20 or more UVA tanning
appliances, thus potentially exposing operators to
high levels (>20W/m
2
) of UVA radiation (Diffey,
1990).
Comparison of UV spectrum from sunlight
and from tanning appliances
During a sunny day on the Mediterranean coast,
the solar UV spectrum at noon contains 4-5% of
UVB and 95-96% of UVA.
When UV output is calculated in terms of
biological activity, as estimated by the erythema-
effective irradiance, the emission of many tanning
appliances is equivalent to or exceeds the emis-
sion of the midday sun in the Mediterranean
(Wester eta/. , 1999; Gerber eta/., 2002). The UV
intensity of powerful tanning units may be 10 to
15 times higher than that of the midday sun
(Gerber et al., 2002) , leading to UVA doses per
unit of time received by the skin during a typical
tanning session well above those experienced dur-
ing daily life or even sunbathing. As a result, the
annual UVA doses received by frequent indoor
tanners may be 1.2 to 4.7 times those received
from the sun, in addition to those received from the
sun (Miller eta/., 1998). This widespread repeated
exposure to high doses of UVA constitutes a new
phenomenon for human beings.
In the 1990s, regulations in some countries
(e.g. Sweden, France) limited to 1.5% the maxi-
mum proportion of UVB in the UV output of
tanning appliances. However, in practice, the UV
output and spectral characteristics of tanning
appliances vary considerably. Surveys in the
United Kingdom on tanning appliances operated
in public or commercial facilities revealed sub-
stantial differences in UV output, mainly for UVB,
for which up to 60-fold differences in output have
been observed (Wright et a/., 1996; McGinley et
a/., 1998). The proportion of UVB in total UV out-
put varied from 0.5 to 4%, and thus emission
spectra similar to that of the sun in the UVB range
were sometimes attained (Gerber eta/., 2002).
These differences are due to tanning appliance
design (e.g. type of fluorescent tubes used as
sources, materials composing filters, distance
from canopy to the skin), tanning appliance
power and tube ageing. Tanning appliances in
commercial facilities may have a greater output in
the UVB range than those used in private prem-
ises (Wright et a/., 1997). With tube ageing, the
output of fluorescent lamps decreases, and the
proportion of UVB decreases more rapidly than
that of UVA.
European and international positions
regarding artificial sources of UV radiation
Full details are given in the Appendix and are
summarized below.
Standard for appliances designed specifically
for tanning purposes
Appliances designed specifically for tanning pur-
poses are defined according to an international
standard prepared by the International
Electrotechnical Commission (IEC 60 335-2-27).
5
Exposure to Artificial UV Radiation and Skin Cancer
This standard was first established in 1985 and
further modified in 1990, in 1995 and in 2002. A
first amendment was added in 2004 and a
second amendment is currently being voted on
internationally. This standard regulates all
appliances sold worldwide, except for the USA
who are regulated by the Food and Drug
Administration (FDA).
Appliances emitting UV radiation must
belong to one of four types of such appliances,
determined by their wavelength spectrum and
irradiance efficiency (see Appendix for detail).
National and international scientific policies
Several national and international authorities
(ICNIRP, WHO, EUROSKIN, the National
6
Radiological Protection Board [United Kingdom]
and the National Toxicology Program [USA]) have
adopted explicit positions regarding the use of
UV-emitting appliances for tanning purposes.
These positions are almost invariably accompa-
nied by recommendations targeting the safety of
the customers.
Regulations
Regulations and recommendations by health
authorities exist in a dozen countries, predomi-
nantly in Western and Northern Europe and the
USA. Details of the regulations for each country
are given in the Appendix.
Biological effects of exposure to UV radiation relevant to carcinogenesis
A large body of literature documents the effects
of UV radiation on different living organisms,
including humans, animals and bacteria.
Experimental as well as epidemiological data
strongly indicate that the spectrum of UV
radiation reaching the Earth's surface is involved
in the development of melanoma (IARC, 1992).
The biological effects of exposure to UV
radiation were described in detail in an IARC
Monograph on UV radiation (IARC, 1992), and
the molecular effects in recent review articles
(Griffiths eta/., 1998; Pfeifer et at., 2005). In this
section, we summarize the aspects most relevant
to the understanding of the biological issues
associated with exposure to artificial sources of
UV radiation.
Biological lesions induced by UVA and UVB
radiation
DNA damage
(a) Experimental systems: UVB is a complete
carcinogen that is absorbed by DNA and can
directly damage DNA. DNA damage induced
by UVB irradiation typically includes the
formation of cyclobutane pyrimidine dimers
(CPD) and 6-4 photoproducts (6-4P). If repair
mechanisms fail to restore genomic integrity,
mutations are likely to occur and persist through
subsequent cell divisions. These mutations are
C ~ T and CC ~ TT transversions, commonly
referred to as "UVB fingerprint" or "UVB
signature" mutations. UVB can also induce the
formation of singlet oxygen species (Oi), an
oxidative compound that is highly reactive and
can cause DNA damage indirectly (Griffiths eta/.,
1998).
UVA is not readily absorbed by DNA and thus
has no direct impact on DNA. Instead, UVA
induces DNA damage indirectly through the
absorption of UVA photons by other cellular
structures (chromophores), with formation of
reactive oxygen species (such as singlet oxygen
and hydrogen peroxide [H
2
0
2
]) that can transfer
the UVA energy to DNA via mutagenic oxidative
intermediates such as 8-hydroxydeoxyguanosine
(8-0HdG). DNA damage by UVA radiation typi-
cally consists ofT transversions, called "UVA
fingerprint" or "UVA signature" lesions (Dobretsky
et at., 1995).
One study in hamster fibroblasts showed that
UVB produces numerous immediate mutations,
whereas UVA produces fewer immediate muta-
tions and more delayed mutations than UVB
(Dahle & Kvam, 2003).
(b) Effects on humans: The mutagenic properties
of UVA in humans have been confirmed in several
studies (Robert et at. , 1996; see Pfeifer et a/.,
2005; Halliday, 2005 for reviews). The possibility
that indirect DNA damage induced by UVA could
play a major role in melanoma occurrence is
underlined by reports of multiple cutaneous
melanomas developing in patients genetically
highly susceptible to oxidative agents (Pavel et
at., 2003).
Experiments in human volunteers conducted
during the last decade have shown that commer-
cial tanning lamps produce the types of DNA
damage associated with photocarcinogenesis in
human cells. Volunteers whose skin was exposed
to UVA lamps used in tanning appliances show
DNA damage, p53 mutations induced by oxida-
tive damage, and alterations of the p53 protein
similar to those observed after sun exposure or
after UV exposure of experimental animals
(Woollens et a/., 1997; Whitmore et a/., 2001;
Persson et at., 2002).
Studies in humans show that a pre-vacation
artificially-induced tan offers little or no protection
against sun-induced DNA damage (Hemminki et
a/., 1999; Bykov eta/., 2001; Ruegemer eta/., 2002).
Cell damage
UVA and UVB radiation can cause cell damage
through different mechanisms: both UVA and
UVB lead to differential expression of p53 and
7
Exposure to Artificial UV Radiation and Skin Cancer
bcl-2 proteins, which may play an important role
in regulating UV-induced apoptosis (Wang eta/. ,
1998). DNA repair and apoptosis protect the
cell's integrity against UV-induced damage. One
study conducted in cells from medaka fish sug-
gested that different apoptotic pathways exist
depending on the wavelength, i.e. for long- (UVA)
and for short- (UVB or UVC) wavelength radia-
tions (Nishigaki et al., 1999). Irradiation of
melanocytes with UVA or UVB leads to alter-
ations of different intracellular proteins, suggesting
that UVA and UVB may induce initiation of
melanoma via separate intracellular pathways
(Zhang & Rosdahl, 2003).
UVA, UVB and human skin
In humans UVA penetrates deeper into the skin
than does UVB. Because UVA represents the
majority of the UV spectrum of tanning appli-
ances and of solar radiation reaching the Earth's
surface, far more UVA than UVB reaches the
basal layers of the epidermis, where skin
keratinocytic stem cells and melanocytes are
located. DNA analysis of human squamous cell
carcinoma (SCC) and solar keratosis showed
that UVA fingerprint mutations are mostly detect-
ed in the basal germinative layer of these lesions,
whereas UVB fingerprint mutations are found
predominantly more superficially in these lesions
(Agar eta/., 2004).
Differential effects of UVA and UVB on skin
cancers
Experimental systems
Several studies showed that UVA could induce
squamous cell cancers in nude mice, but the abil-
ity of UVA alone (without exogenous photosensi-
tizers such as those used in PUVA therapy -
see Page 41) to induce squamous cell skin can-
cers was about 5000 to 1 0000 times lower than
that of UVB alone {IARC, 1992; de Laat et al.,
1997; Griffiths et al., 1998). Both in-vitro experi-
ments and epidemiological studies have demon-
strated that long-lasting, chronic exposure to
UVB is the main cause of sec of the skin (see
IARC, 1992; Brash et al., 1996 for reviews).
8
Accordingly, before 1990, only UVB, and not
UVA, was considered to be carcinogenic.
In the 1990s, studies in newborn rodents and
on human foreskin grafted on immunosup-
pressed nude mice have provided compell ing
evidence that high UVB doses were required in
the genesis of melanoma or of melanocytic
tumours considered to be precursor lesions of
melanoma (Mintz & Silvers, 1993; Atillasoy eta/.,
1998; Robinson eta!., 1998; Sauter eta/., 1998;
Robinson et al. , 2000a; Noonan eta/., 2001; van
Schanke et al. , 2005). At the same time, several
in-vivo studies showed that UVA can induce
melanoma in backcross hybrids of freshwater
fishes of the genus Xiphophorus (platyfish and
swordtail; Setlow et a/. , 1993) and melanocytic
tumours in the South American opossum
Monodelphis domestica (Ley, 1997, 2001 ).
However, UVA was less efficient than UVB for the
induction of melanocytic tumours in Monodelphis
domestica (Ley 2001 ), and experiments with UVA
on newborn rodents and on human foreskin could
not reproduce the results obtained with UVB
(Robinson eta/., 2000b; Berking et al. , 2002; de
Fabo et al., 2004; van Schanke eta/. , 2005).
Other studies showed that radiation emitted
by lamps used in tanning appliances (mainly
UVA) could significantly increase the carcino-
genic effect of broad-spectrum UV radiation
(Bech-Thomsen et a/., 1991 , 1992), indicating
the possibil ity of a complex interplay between
UVA and UVB radiation in human skin.
Relevance of experimental data to human
skin cancers
To date, evidence obtained from experimental
studies on the involvement of high UVB doses in
the causation of sec is consistent with observa-
tions in humans. In contrast, experimental studies
provide conflicting results on an implication of
UVB and UVA in the induction of melanoma in
humans. The same uncertainties hold true for
basal cell carcinoma (BCC), a type of tumour that
shares many of the epidemiological characteris-
tics of melanoma.
The relevance of animal models for elucidating
the biological mechanisms involved in the
development of melanoma and BCC remains
Biological effects of exposure to UV radiation relevant to carcinogenesis
questionable, as even engineered mice with
multiple deficiencies in key genes involved in cell
cycle regulation and growth factor synthesis do
not represent a model equivalent to the human
skin. In addition, experiments on animals cannot
reproduce the complex relationship existing in
individuals between highly variable natural sus-
ceptibilities to UV radiation, different sun exposure
behaviours, and exposure to various sources of
UV radiation. In the case of indoor tanning, such
relationships may be critical, as users are more
inclined than the average population to engage in
outdoor tanning activities (Autier et al., 1991 ), and
indoor tanning sessions often precede or follow
active sun exposure or outdoor tanning.
Changes in immune response
Several reports (IARC, 1992, 2001; Ullrich, 2005)
have extensively reviewed the studies on the
effects of UV on the immune system and of the
underlying mechanisms. This section only refers
to studies relevant to UVA and use of indoor
tanning facilities.
Experimental systems
Both UVA and UVB radiation can affect the
immune response that may be involved in the
promotion of melanoma (Kripke, 1974; Singh et
al. , 1995), but the two types of radiation seem to
act differently. UVB can induce immune suppres-
sion at both local and systemic levels whereas
UVA does not induce systemic immune suppres-
sion. However, studies have shown that a number
of local responses induced by UVB radiation on
the skin could be suppressed by a UVB filter, but
the melanoma growth stimulation effect could not
be suppressed (Donawho eta/., 1994; Wolf et al.,
1994). This result suggests that UVA may influ-
ence local immune responses different from
those influenced by UVB.
Studies in humans
Observations in human volunteers have
demonstrated that UV exposure suppresses the
induction of immunity (Cooper eta/., 1992; Tie et
al., 1995; Kelly et a/., 1998). Few studies have
specifically investigated the effects of exposure to
tanning appliances on the systemic and local
immune systems. UV lamps similar to those used
in tanning appliances are used without concomi-
tant use of photosensitizer for treating skin
conditions such as dermatitis and sun allergies,
illustrating the effect of that radiation spectrum on
the skin immune system.
Studies in volunteers have shown that expo-
sure to tanning appliances induces reductions in
blood lymphocyte counts, changes in proportion
of lymphocyte subpopulations, immune response
to known carcinogens applied to the skin, and
changes in the skin immune system (Hersey et
al., 1983, 1988; Rivers et al. , 1989; Clingen et al.,
2001 ). These studies also indicated that UVA and
UVB would affect the immune system via inter-
acting and overlapping mechanisms, depending
on the amount of UVA and UVB emitted (Ciingen
et a/., 2001 ), which would then lead to the
suppression of known immune reactions
(Nghiem et al., 2001, 2002). Hence, these stud-
ies indicate that UVA can suppress established
immune reactions at the skin level, but it remains
to be established how these effects relate to the
induction of neoplastic processes.
Effects of natural and artificial UV radiation
on human skin
Variety of skin types
There is a considerable range of susceptibility of
the human skin to the carcinogenic effects of UV
radiation, and in humans, there is an estimated
1 000-fold variability in DNA repair capacity after
UV exposure (Hemminki et a/., 2001 ).
Susceptibil ity to sun-induced skin damage is
closely related to pigmentary traits, and subjects
having the following characteristics are at
increased risk for developing a skin cancer
(melanoma, SCC and BCC):
Red hair, followed by blond hair, followed by
light brown hair.
Skin phototype (Fitzpatrick, 1988): subjects
who always burn and never tan when going
9
Exposure to Artificial UV Radiation and Skin Cancer
unprotected in the sun (skin phototype I) have
a much higher risk for skin cancer than sub-
jects who never burn and always develop a
deep tan (skin phototype IV). Intermediate
risk categories are subjects who always burn
then develop a light tan (skin phototype II),
and subjects who sometimes burn and always
develop a tan (skin phototype Ill). Subjects of
skin phototypes V and VI belong to popula-
tions with natural brown or black skin, and are
resistant to sunlight.
Freckles (ephelides) on the face, arms or
shoulders. The skin cancer risk increases with
increasing sensitivity to freckling.
Skin colour: pale colour, followed by
increasing depth of pigmentation.
Eye colour: blue, followed by grey/green eyes,
then by brown eyes.
Subjects with red hair, many freckles and
who never tan are at particularly high risk for skin
cancer.
Sunburn
Sunburn is the occurrence of painful erythemal
reaction after exposure to UV radiation. Sunburn
during childhood or during adulthood is a risk fac-
tor for melanoma, and the risk increases with
increasing number of sunburns (IARC, 1992).
Skin erythema or sunburns are reported by
18- 55% of users of indoor tanning facilities in
Europe and North America (reviewed in Autier,
2004). Although UVB is more potent than UVA for
triggering sunburn, high fluxes of UVA are capa-
ble of inducing skin erythemal reactions after 1 0
to 20 minutes in subjects susceptible to sunlight
and having moderate tanning ability (Fitzpatrick
skin phototype II}.
10
Tan acquisition
The production of melanin (tanning) accounts for
part of the protection against UV radiation, but
there is mounting scientific evidence that faculta-
tive tan is triggered by UV-induced DNA damage
in the skin (Pedeux eta/., 1998; Gilchrest & Eller
1999 for a review}. Facultative tanning is now
considered a better indicator of inducible DNA
repair capacity than of efficient photoprotective
skin reaction. Inducible DNA repair capacity
rather than pigmentation itself could result in the
lower incidence of skin cancer observed in
darker-skinned individuals (Young et a/. , 1998;
Agar & Young, 2005; Bohm eta/., 2005}.
In subjects who tan easily, exposure to
tanning appliances will first lead to the oxidation
of melanin already present in superficial
keratinocytic layers of the skin (i.e. immediate
pigment darkening [IPD]). IPD is essentially trig-
gered by UVA (Young, 2004). It develops rapidly
after exposure during an indoor tanning session,
and fades away after a few hours. A more
permanent tan is acquired with accumulation of
exposure, depending on tanning ability and on
the amount of UVB present in the UV spectrum of
the lamps. The permanent tan conferred by
"UVA-tanning" has a uniform and less deep
brown appearance than the tan acquired in the
sun.
IPD has no photoprotective effect against
UV-induced erythema (Black et a/., 1985}. A
UVA-induced permanent tan provides practically
no photoprotection either (Gange et a/. , 1985;
Rivers et a/., 1989), and UVA-induced moderate
skin thickening would afford even less photopro-
tection than tanning (Seehan eta/., 1998).
Prevalence of exposure to artificial UV radiation for tanning purposes
The indoor tanning industry developed in Europe
and the USA in the early 1980s, a time when UVA
radiation was thought to be harmless, with the
introduction of tanning applances emitting UVA at
levels similar to or even exceeding those from nat-
ural sunlight. In the USA, indoor tanning is now a
more than $5 billion industry that employs
160,000 persons (Indoor Tanning Association,
2004), and in the United Kingdom the turnover in
the indoor tanning industry exceeds an estimated
100 million per annum (source: www.ray-
watch.co.uk; accessed on 15/06/2005).
Prevalence of exposure by region/country
Indoor tanning is a widespread practice in most
developed countries, particularly in Northern
Europe and the USA, and is gaining popularity
even in sunny countries like Australia.
Few surveys have estimated specifically the
prevalence of indoor tanning among adult popu-
lations. In 1996, a telephone survey was carried
out among white adults (18 to 60 years old) from
the two most densely populated regions
(Montreal and Quebec) of the Province of
Quebec, Canada (Rhainds et a/., 1999). Of the
1 003 respondents, 20% reported having used a
tanning appliance in a commercial tanning facility
at least once during the last 5 years before the
survey. The prevalence of use during the last 12
months before the study was 11 %.
Recently, a brief report describing prevalence
of indoor tanning in Minnesota, USA, derived
from a telephone interview (45% response rate)
concerning quality of life, employment and health
of 802 randomly selected adults, showed that in
2002, 38% of adults had ever used indoor
tanning facilities (Lazovich eta/., 2005).
The prevalence of use of indoor tanning facil-
ities can be estimated from the proportion of
exposed controls in population-based case-con-
trol studies on risk factors for melanoma and
basal and squamous cell skin cancers (Table 3).
The prevalence varies greatly with country,
gender and age. Prevalence of ever having used
indoor tanning facilities ranges from 5% in
Northern Italy to 87% in Swedish women, and is
currently very high in Northern European coun-
tries, particularly in Sweden and the Netherlands.
Prevalence of exposure to tanning appliances
may still be low in some European countries or
populations. In a survey conducted among
33,021 adults older than 30 years attending
health check-up centres in France, only 2% of
subjects reported use of indoor tanning facilities
(Stoebner-Delbarre eta/., 2001 ).
Time trends
The prevalence of indoor tanning is currently
increasing in many countries, and current avail-
able estimates may therefore be rapidly outdated.
In studies conducted approximately 20 years
ago, the practice of indoor tanning was generally
low: 7% in Germany, 18% in Denmark.
Prevalence of exposure to tanning appliances by
the controls included in case-control studies is
higher in the most recent studies than in studies
conducted before 1990 (Table 3).
A survey in Minnesota (Lazovich eta/., 2005)
indicated that prevalence of use has increased
over the last decades. Few men and women had
used a tanning appliance before 1980. Women
were almost twice as likely as men to report
tanning indoors during the 1980s (19% versus
1 0%), but in the following decade, the proportion
of men using indoor tanning facilities approached
that of women (15% versus 17% in the 1990s).
The fact that the prevalence of indoor tanning
has increased during the 1990s can be demon-
strated by comparing prevalence of use as
reported in studies conducted by the same inves-
tigators in the same countries at intervals of
several years.
A case-control study conducted in 1991 in
five centres in Belgium, France and Germany
11
li\)
m
Table 3. Prevalence of use of indoor tanning facilities by popul ation controls from epidemiological studies
X
'8
IJ)
c
Reference Location Inclusive years Disease Type of No. of Source of c ontrols Age range Prevalence of ever use (il
of recruitment Study controls (years)
0
Number %
)>
::l.
Holman el a/. Western Australia 1980 1981 M Case-control 511 Population, electoral roll, NR NR NR
:::;.;
C>
(1986) matched on age, sex ~
c
Osterlind et a/. East Denmark Oct. 1982 Mar. 1985 M Case-control 926 Population, National 20-79 168 18
<
(1988) Population Register
::u
Q)
a.
iii'
Zanetti eta/. (1988) Torino, Italy May 1984 Oct. 1986 M Population, from the National Case-control 416 NR 21 5 d:
0
Health Service ::1
Q)
::I
Walter et a/. (1990 Southern Ontario, Oct. 1984 Sep. 1986 M Case-control 608 Population, Property tax 20-69 109 18
a.
and 19g9) Canada assessment rolls
(f)
a.
::I
Autier el a/. (1994) Germany, France, Jan. 1991 onwards M Case-control 447 Population, door to door ~ 2 120 27
(')
Q)
Belgium
::I
Westerdahl et a/. Sweden July 1966 June 1990 M Case-control 640 Population, National 15-75 159 25 ~
(1994) Population Registry
Holly et al. (1995) San Francisco, Jan. 1961 Dec. 1966 M Case-control 452 Population, random digit 25-59 NR NR
USA telephone dialling
Bajdik el a/. (1996) Alberta, Canada 1983 1984 BCC I SCC Case-control 406 Population, health insurance 25-79 33 8. 1
plan subscriber list
Chen et a/. (1998) Connecticut, USA Jan. 1987 May 1989 M Case-control 512 Population, telephone NR 95 19
random digit dialling
Westerdahl el al. South Health Care Jan. 1995 June 1997 M Case-control 913 Population, National NR 372 4 1
(2000) region, Sweden Populati on Registry
Karagas et a/. New Hampshire, July 1993 June 1995 BCC I SCC Case-control 539 Population, Dept. of 25-74 75 14
(2002) USA Transportation, medicare
medicaid
Veier0d eta/. Norway and 1991 1992 M Cohort 79616 Population, prospective 10-39 14 377
2
18
(2003) Sweden cohort
Bataille eta/. (2004) North East Aug. 1989 July 1993 M Case-control 416 Hospital and general 16-75 110 26
Thames, UK practice, excluding skin
disease
Bataille el a/. {2005) Belgium, France, Dec. 1998 July 2001 M Case-control 622 Sweden, population-based; 18- 50 354 57
Netherlands, France & Belgium. door to
Sweden & UK door; UK & Netherlands, GP
NR. not reported; GP, general practitioner
' BCC, basal cell carcinoma; M, melanoma; SCC, squamous cell carcinoma
2
<: 1 time/month
Prevalence of exposure to artificial UV radiation for tanning purposes
(Autier eta!., 1994) showed that 19% of controls
had ever exposed themselves to a sunlamp or a
sunbed, this proportion being higher in Germany
(25%) than in Belgium (20%) or in France (6%) .
Of the recorded exposures, 84% had started
after 1979. In a more recent case-control study
conducted by the same investigators between
1998 and 2000 in Belgium, France, Sweden, the
Netherlands and the United Kingdom among
persons younger than 50 years (mean age of
controls, 37 years), 57% of controls had ever
exposed themselves to artificial UV tanning, with
the highest prevalence of use being found in
Sweden (87%) (Bataille eta!., 2005).
According to two studies conducted within the
same population in the south of Sweden in
1988-1990 and in 1995- 1997, the prevalence of
exposure doubled in 7 years. In 1988-1990, 46%
of individuals younger than 30 years had ever
exposed themselves to sun lamps or solaria (56%
of women and 12% of men, these figures being
higher in the group aged 15-24 years) while this
proportion was only 24% among individuals older
than 30 years (31% of women and 16% of
men)(Westerdahl et a!., 1994). After 1995, the
prevalence of solarium use in the population aged
16-80 years was 41 %, but 70% of women and
50% of men aged 18-50 years reported having
ever used a solarium (Westerdahl eta!., 2000).
Personal characteristics of adult users
Sex
Use of indoor tanning facilities is more prevalent
among women, particularly among younger age
groups and in Northern countries.
A survey of tanning appliances in commercial
use in Scotland was conducted in 1997 to measure
the spectal irradiance of the different models and
compare this irradiance with UV doses received
during sunbathing (McGinley eta!., 1998). As part
of the study, a questionnaire was distributed to
sunbed users, seeking information about their age,
sex, skin type, frequency of use, attitudes and rea-
sons for use. A total of 205 questionnaires were
collected. The majority of users were women (170
versus 35 men).
A significantly higher proportion of women
and young people (18-34 years old) was found
among tanning bed users in the Montreal-
Quebec survey (Rhainds et a!. , 1999). In the
Minnesota survey (Lazovich eta!., 2005), indoor
tanning was also more prevalent among women
than among men: 45% versus 30%. Among
users, the median number of times used was 1 0
for men and 20 for women (range, 1-600), and
21% of women reported frequent use (defined as
more than 30 times) .
In Europe, a recent case-control study found
use of indoor tanning facilities to be more preva-
lent among women (61 %) than among men
(43%) (Bataille et al., 2005). Another recent
survey explored exposure to tanning appliances
and sun exposure behaviour in a cohort of adult
volunteers. In 2001, a self-administered question-
naire was specifically developed and addressed
to 12 741 adult volunteers in France enrolled in
the SU.VI.MAX cohort (a cohort recruited in 1994
and followed for 8 years, which included men
aged 45-60 years and women aged 35-60
years). Over 60% of the questionnaires were
returned, of which 97% were useable. Among the
7 359 individuals who answered the question-
naire, 1 179 (16%) - 953 women (22%) and 226
men (8%) - reported having ever experienced
indoor tanning. Men and women reported similar
prevalences for regular use (6% and 7%, respec-
tively) and for a duration of at least five years
(1 0% for men and women). Among women, 44%
of users belonged to the youngest age group at
recruitment (35-44 years), versus 33% in non-
users (in rnen, data were not available for this age
group); 48% of female users lived in the North or
in lle-de-France, versus 39% of non-users (45%
and 36% for men, respectively) (Ezzedine eta!. ,
2005) (Table 4).
Bataille et a!. (2005) recently observed that
indoor tanning is becoming more frequent in men
and in younger age groups, with important varia-
tions by country: exposure of men is highest in
Sweden (78%) and Netherlands (60%), while
39% of men in the United Kingdom and 13% in
France reported ever having used indoor tanning
facilities.
13
Exposure to Artificial UV Radiation and Skin Cancer
Table 4. Lifetime use of indoor tanning facilities and sun exposure behaviour among 7 359
healthy adults (SU.VI.MAX cohort)
Women Men
Use of indoor tanning facilities Users Non-users Users Non-users
N = 953 (22%) N = 226 (8%)
Regular use 7%
5 years 10%
Residence North of France or lle-de-France 48%
Sunbathing between 11 a.m. and 4 p.m. 56%
Regular sunscreen use during sunbathing 39%
Progressive sun exposure 54%
Nudism 13%
Sunburns in adulthood 93%
Important or extreme tan seeking behaviour 37%
From Ezzedine et at. (2005)
Age
Younger age (<35 years) is significantly associated
with higher likelihood of using indoor tanning
facilities among both men and women.
In an early case-control study conducted in
several countries in Europe (Autier eta/., 1994),
indoor tanning was more prevalent in younger
age groups (31 % among controls < 40 years). In
a more recent case-control study in Europe
(Bataille eta/., 2005), exposure before the age of
15 years was reported in 3% of all controls, but
reached 20% in Sweden. The mean age at first
exposure was 20 years in Sweden, 23 years in
the United Kingdom and 27 years in France.
In the survey conducted in Scotland (McGinley
et a/. , 1998), 73% of users were under 35 years
old, with 32% of users being under 25 years old.
In the Minnesota survey (Lazovich et a/.,
2005), 13% of men and 22% of women reported
first tanning indoors as adolescents.
Skin type
Few studies have analysed specifically the use of
indoor tanning facilities as a function of skin type.
Since most studies have been conducted primari-
ly in relation to skin cancer risk factors, use by skin
type cannot be derived from the reported results.
In the survey conducted in Scotland
(McGinley et a/., 1998), 38% of users described
14
6%
10%
45% 36%
37% 53% 38%
24% 17% 7%
43% 53% 38%
6% 19% 8%
88% 93% 89%
20% 26% 11 %
their skin phototype as type I or II , and 38% also
indicated that they had experienced an adverse
reaction when using indoor tanning facilities; 31%
of users had more than 1 0 courses of over 5 ses-
sions in a year, and for 16% this amounted to
over 1 00 sessions per year.
In several case--control studies, use of indoor
tanning facilities was more frequent among
controls with a poor ability to tan: for example, 27%
and 31% among controls with blond or red hair,
respectively, in a European study (Autier eta/., 1994).
In the SU.VI.MAX cohort, individuals wi th a
pale complexion were more likely to use indoor
tanning facilities (Ezzedine eta/. , 2005). This was
not the case among controls from a recent
case-control study conducted in Europe, where
approximately one third of controls using indoor
tanning facilities were of phototype I or II (Bataille
et a/., 2005) (Table 5). However, it must be
stressed that in this study, phototype was declared
by participants and it is likely that few of them
perceived themselves as sun-sensitive, as exem-
plified by the very low proportion of persons with
self-reported phototype I in the Swedish popula-
tion.
Other factors
Higher education levels or income are significantly
associated with a higher li kelihood of using
indoor tanning facilities among men.
Prevalence of exposure to artificial UV radiation for tanning purposes
Table 5. Prevalence of indoor tanning according
to skin type among controls in a European
case-control study (Bataille et a/., 2005)
Country Phototype (%)
II Ill IV
Belgium 13.3 23.3 43.3 20.0
France 6.4 38.7 25.8 29.0
Sweden 1.2 24.7 64.2 9.8
The Netherlands 6.0 17.9 53.0 23.1
United Kingdom 12.7 32.1 39.0 6.9
Data courtesy of V. Bataille.
The most common reasons given for use of
indoor tanning faci lities is to develop a "base tan"
before a holiday and to feel more relaxed
(McGinley eta/. , 1998).
In the SU.VI.MAX survey, the most frequently
report ed motivations tor using artificial tanning
were aesthetic (35%) and skin preparation before
sun exposure (34%) (Ezzedine et a/. , 2005) . In
this cohort, there was a clear link between use of
indoor tanning faci lities and sun-seeking
behaviour (Table 4).
Personal characteristics of adolescent and
children users
Since 1989, a total of 16 studies (18 reports)
have examined indoor tanning among children
and adolescents aged 8-19 years. These studies
are summarised in Table 6 (see Lazovich &
Forster, 2005 for review). Studies were conducted
in Europe (Norway, Sweden and the United
Ki ngdom) , in various locations throughout the
USA (including two nationally representative
samples) and in Australia. Adolescents were
identified through paediatric clinics, schools, as
offspring of adult cohort study participants, or
through random selection of defined populations.
Sample size ranged from 96 to over 15,000. Use
of indoor tanning facilities was defined either as
ever use, or use in the past 6 or 12 months. Given
the differences in the study populations and in
the definition of indoor tanning between studies,
it is not surprising that prevalence estimates vary
greatly. However, all these studies show frequent
use by adolescents and chi ldren, sometimes at a
very young age. According to the most recent
studies, 30% of adolescents in Sweden and 24%
of adolescents in the USA aged 13-19 years
reported ever use of indoor tanning faci lities, and
8% and 12% respectively were frequent users
(1 0 times per year or more). In a recent survey in
the United Kingdom, while 7% of children aged
8- 11 years reported exposure to a sunbed in the
last 6 months, as many as 48% expressed a
desire to use a sunbed (Hamlet & Kennedy,
2004) .
The earl iest studies in Sweden and in the
USA tended to find indoor tanning to be more
prevalent among adolescents with fair skin types
who are more prone to sunburn (Mermelstein &
Riesenberg, 1992; Boldeman et a/., 1996;
Robinson eta/. , 1997). More recent studies in the
USA found either the opposite (Cokkinides eta/.,
2002; Geller eta/., 2002; Demko eta/., 2003) or
no association (Lazovich eta/., 2004).
Studies of compliance to regulations and
recommendations
Few studies have assessed the compliance of
indoor tanning facility operators or consumers
with recommendations and regulations. In this
section, studies are first summarised and then
data are presented according to each regulation.
Compliance of operators
(a) Study descriptions - overall compliance rates:
In 1991, Oliphant et a/. (1994) surveyed over
1 000 high school students aged 13 to 19 years in
suburban Minnesota (USA) via a self-adminis-
tered questionnaire regarding use of indoor tan-
ning facilities and knowledge about risks of
indoor tanning. The survey assessed compliance
of staff with regulations and recommendations as
reported by the users.
In 1998, Culley et a/. (2001) quantified the
level of compliance by indoor tanning facility
operators with selected federal and state regula-
tions and recommendations. A person posing as
a potential customer visited 54 tanning facilities in
15
Exposure to Artificial UV Radiation and Skin Cancer
Table 6. Studies of adolescent use of Indoor tanning facilities
Reference Year of Location Population N Age range Prevalence (%)
1
Characteristics
survey source (years)
assessed In relation to
Boys Girls All
use of indoor tanning
facilities
Banks eta/. 1989 Vienna, Adolescents 96 16-19 16 33 23 Gender, age, frequency
(1992) VA, USA seen at nine
pediatrics
clinics
Mermelstein 1990 Chicago, 10 schools 1 703 9th and 7 19 NR Gender, age, skin type
& Riesen IL, USA participating
1oth
berg (1992) in skin
graders
cancer inter
vention
study
Oliphant et 1991 St. Paul, One high 1 008 13-19 15 51 34
Gender, age, frequency,
a/. (1994) MN, USA school knowledge of risks,
practice, symptoms
Wichstrom 1992 Norway 56 randomly 15 169 17.3
35
752 NR
Gender, age, frequency
(1994) selected (mean)
high schools
Boldeman et 1993 Stockholm, 60 randomly 1 252 14-19
32 68 57
Gender, age, knowledge
a/. (1996, Sweden selected of risks, smoking,
1997) classes frequency, skin type,
symptoms, sunbathing,
skin disease, perceived
attractiveness, attitudes
Robinson et 1994 Chicago, Population- 658 11-19
16 8
Gender, age, skin type,
a/. (1997) IL, USA based ran- socio-economic status
dom sample
Brandberg et 1996 Sweden Population 2 615 13, 15, 17
4 16 10
Gender, age, satisfaction
a/. (1998) based ran- with self
dom sample
Boldeman et 1999 Stockholm, Population- 4 060 13-19
19 40 30
Gender, age, frequency,
a/. (2001) Sweden based ran symptoms
dom sample
Lucci eta/. 1999 Dallas & Junior and 210 14-19
NR NR 183 None
(2001) Houston, senior high
Texas, students
USA
Cokkinides 1998
USA Population- 1 192 11-18 5 16 102 Gender, age, race,
eta/. (2002)
based ran- parent education and
dom sample income, residence, sun
sensitivity, skin type,
sunbathing, sun
protection, health-
provider advice,
attitudes, parent tans
16
Prevalence of exposure to artificial UV radiation for tanning purposes
Table 6 c o n t d ~
Reference Year Location Population N Age range
Prevalence (%)
1
Characteristics
of source (years) assessed in relation to
survey
Boys Girls All
use of indoor tanning
facilities
Geller eta/. 1999 USA Prospective 10 079 12-18 2 14 102 Gender, age, skin type,
(2002) cohort of social factors, sun pro-
off-springs tection, attitudes
of Nurses
Health
Study
Knight et a/. 1999 Bloomington, College 489 ~ 17 38 70 62 Gender, age, frequency,
(2002) Indiana, students 402 17- 22
NR NR 522
skin type, geographical
USA attending
region, reason for using
student tanning bed, believes
health about tanning,
centre
knowledge of risks
Demko eta/. 1996 USA 132 6 903
13-19 11 37 24 Gender, age, frequency,
(2003) schools in sun sensitivity, geogra-
80 commu- phical region, school
nities location, student income,
maternal education,
sunbathing, substance
use, diet, obesity, body
image, physical activity,
body piercing, psycho-
social factors
Hamlet & NR Wish ow 23 primary 1 405 8-11 NR NR 7 Age, frequency, atti-
Kennedy Local schools tudes, exposure at home
(2004) Health or on commercial
Care, UK premises.
Lazovich et 2000 Minneapolis/ Random 1 273
14-17 12 42 30
Gender, age, smoking,
a/. (2004); St. Paul, MN sample of
satisfaction with looks,
Stryker et a/. and Boston, households
depression, sun protec-
(2004) MA. USA likely to
tion, skin cancer risks,
have
parent and teen
adolescents
knowledge of risks,
parent and teen atti
tudes, social factors,
parent tans, parent
education, parent con-
cern, parental influence
score
Paul eta/. 2000 New South Population- 1 509 ~ 15 5 14 10 Gender, age, attitudes,
(2004) Wales,
based
78
15-17 4
use of sunscreen
Australia
random 18-29 11
sample 30-39 19
Adapted from Lazovich & Forster (2004)
NR, not reported.
1
Prevalence of ever use, unless otherwise noted.
2
Past 12 months
3
Past 6 months
17
Exposure to Artificial UV Radiation and Skin Cancer
the San Diego, USA metropol itan area.
Compliance with 13 regulations/recommenda-
tions was assessed by either direct query or
observation of the presence/absence of signs and
warning labels. No facility was in compliance with
all 13 selected regulations. The mean number of
regulations complied with was 8.33.
In another study conducted in the San Diego
area, in 2000, Kwon et al. (2002) assessed the
compliance of 60 tanning facilities with recom-
mended exposure schedules by means of a tele-
phone enquiry made by a supposedly prospective
customer.
One study, conducted in Australia in 2005,
explored compliance with international recom-
mendations on solarium use in an unregulated
setting: simulated customers visited 176 solaria
in two face-to-face visits for each establishment
and one telephone contact. Few (16%) establish-
ments were compliant with more than 1 0 of the
13 recommendations. Compliance was particu-
larly poor for those recommendations with the
greatest potential for minimising harm: i.e. to dis-
courage or exclude persons at high risk from UV
exposure (Paul et al. , 2005).
(b) Duration/frequency of exposure: In the survey
assessing compliance of staff as reported by the
users (Oliphant eta/., 1994), 26% said they were
never told to limit their time per session.
In a later study from the USA (Culley et al. ,
2001 ), compliance was found to be relatively high
for maximum duration allowed to tan (98%) but was
relatively low for presence of and compliance with
an appropriate shut-off switch (57%). Frequency
allowed to tan had the lowest compliance at 6%;
one facility even allowed two consecutive tanning
sessions.
In the most recent study from the USA (Kwon
et al. , 2002), only 4 out of 58 tanning salons (7%)
recommended less than 3 sessions in the first
week, and therefore were compliant with the reg-
ulations. All responded with a duration of expo-
sure of less than 30 minutes, but all reported
offering unlimited tanning packages, and less
than 30% limited the exposure to once a day.
(c) Wearing of goggles: In the high school student
survey cited above (Oliphant et al., 1994), less
18
than half of the customers interviewed (42%) had
always been told to wear goggles, and 28% had
never been.
In a more recent study from the USA (Culley
et al., 2001 ), compliance was found to be high for
provision and sanitation of protective eyewear
(1 00%) and for requirement to use it (89%).
(d) Age restriction: Very few studies have looked
at compliance with age restriction. One study
observed a low compliance (43%) with the
requirement for parental permission for adoles-
cent users aged 14-18 years (Culley et a/.,
2001 ). Low levels of compliance with recommen-
dations relating to age restriction were also found
in a more recent study (Paul eta!., 2005).
(e) Warning of health risks: In the survey assess-
ing compliance of staff as reported by users
(Oliphant et a/., 1994), 50% reported that they
had never received a warning about the health
risks of indoor tanning, and less than half (48%)
had ever noticed a warning sign at the facility. In
another study in the USA (Culley et a/:, 2001 ),
compliance was found to be relatively high for
presence of labels on warning of UV danger and
of exposure (85%) and legibility, accessibility and
correctness of these labels (74%); lower compli -
ance (15-20%) was observed for warning signs
in the tanning area.
(f) Other regulations: In the Australian study (Paul
et al. , 2005), 1% of operators refused access to a
pretending customer with skin phototype I, and
1 0% recommended against solarium use. In the
same study, low levels of compliance were also
found for using a sunbed while taking medica-
tions, for provision of consent forms and for
discussing safety procedures.
Compliance of customers
(a) Study descriptions: The 1991 high school stu-
dent survey in the USA (Oliphant et al. 1994) has
been described above.
McGinley eta/. (1998) conducted a survey of
the output of tanning appliances in use in 1997 in
Scotland. At the same time, questionnaires were
distributed by the indoor tanning facilities to
Prevalence of exposure to artificial UV radiation for tanning purposes
users, seeking information on patterns of expo-
sure and reasons for using sunbeds.
In 1996, a telephone survey was carried out
among adults from the two most densely popu-
lated regions of Quebec, Canada, as described
above (Rhainds et al., i 999). The final sample
included i 003 white persons i 8-60 years old.
Interviewers used a standardised questionnaire
to document exposure habits to artificial UV
radiation sources.
One study was conducted in North Carolina
(USA) to assess adherence of indoor tanning
clients to FDA-recommended exposure limits.
A community-based survey was administered
during routine state inspections of 50 indoor
tanning facilities. At each facility, users' records
were randomly selected (n = 483) for a survey of
exposure (Hornung et al., 2003).
To gain anecdotal evidence that primary
school children were using sunbeds in
Lanarkshire (United Kingdom), school nurses
conducted a short questionnaire in 23 primary
schools in 2003. Children 8-11 years old took part
in the classroom surveys. Positive responses
were counted by a show of hands by the children
(Hamlet & Kennedy, 2004). [This small study was
based on a "hands up" survey, which may have
biased answers through copying of friends'
actions.]
{b) Duration/frequency of use: In the high school
student survey, 1 i% of users reported tanning
indoors for more than 30 minutes. Those who
reported longer usual tanning sessions were
more likely to tan frequently (Oliphant et a/.,
1994).
A user survey demonstrated that 31% of 205
responders had more than 1 0 courses of over
five tanning sessions in a yeaF and, for 16% of
them, this amounted to over i 00 sessions per
year (McGinley eta/., 1998).
In the study by Hornung et al. (2003), out of
483 users, 95% were exceeding the recommended
exposure times. Also, 33% of users started their
first tanning session at or above exposure times
recommended for users in the maintenance
phase of tanning (>4.0 MED). The average dura-
tion of exposure on the first visit was 14.3 min-
utes (range, 3-30 minutes). Compilation of 15
common exposure schedules listed a suggested
range of 2- to 15-minute sessions (average, 5.76
minutes) for the first week of tanning, with
gradual increases over a 4-week or longer period
to a range of 8- to 30-minute maintenance ses-
sions (average, 20.5 minutes). The average peri-
od of tanning for each user was 6.3 weeks. Users
spent approximately 43 minutes per week (range,
5-135 minutes) during an average of 2.4 ses-
sions per week (0.25-7 sessions) (Hornung et
at., 2003).
(c) Wearing of goggles: In the i 991 study of high
school students (Oliphant et al., 1994), 59%
reported always wearing goggles and 17%
reported never wearing them. Those who reported
longer usual tanning sessions were less likely to
use goggles.
In the Scottish survey (McGinley eta/., 1998)
35% of users stated that they never or hardly ever
wore protective goggles.
In the Canadian study (Rhainds eta/., 1999),
70% of 203 tanning bed users wore protective
goggles during tanning sessions.
(d) Age restriction: In the US high school survey,
almost 20% of those aged 14 years or younger
reported using indoor tanning facilities, and half
of the users had had their first session before age
15 years (Oliphant et al. , 1994).
Among 1405 adolescents under 16 years
surveyed in the United Kingdom (Hamlet &
Kennedy, 2004), 7% had used a sunbed in the
last 6 months, of whom sixteen (17%) agreed
that they used a sunbed regularly, i.e. twice a
month or more. Of these 96 adolescent recent
users, 61 (64%) reported using a sunbed in
someone's house, and 23 (24%) had used a
sunbed in a shop or salon.
19
Epidemiological data on exposure to artificial UV radiation for cosmetic
purposes and skin cancers
As no valid animal model of human melanoma or
other skin cancers exists, evidence of an associ-
ation between indoor tanning facility exposure
and skin cancer must be sought predominantly
from epidemiological studies. Few studies have
addressed this topic specifically, but most skin
cancer studies have included one or more items
about use of indoor tanning facilities. We system-
atically analysed the summary statistics compiled
from the relevant studies in a meta-analysis. The
results have also been discussed qualitatively, to
allow for the large differences in study popula-
tions and study quality.
Since melanoma and other skin cancers
differ somewhat in their aetiology, studies of
melanoma were analysed separately from those
of basal and squamous cell cancers.
Epidemiological evidence from studies investigating
other sources of exposure to artificial UV
radiation has also been presented.
Methodology for literature search
The literature to April 2005 was searched using
the following databases: Pubmed, lSI Web of
Science (Science Citation Index Expanded),
Embase, Pascal, Cochrane library, Lilacs and
Medcarib. The following keywords and their cor-
responding French translations were used for
search in the PASCAL database: "skin cancer",
"squamous cell carcinoma", "SCC", "basal cell
carcinoma", "BCC", "melanoma" for diseases. To
define exposure, the following keywords were
used: "sunbed", "sunlamp" , "artificial UV",
"artificial light", "solaria", "solarium", "indoor tan-
ning", "tanning bed", "tanning parlour", "tanning
salon" and "tanning booth".
We searched for keywords in the title and in
the abstract, when available. We also performed
a manual search of references cited in the selected
articles, and in selected reviews or books on
20
melanoma and skin cancer. All participants of the
working group and some IARC staff were asked
to report any additional published or submitted
study. No language restriction was applied.
Primary inclusion criteria were developed for
the selection of relevant articles, which were:
case-control, cohort or cross-sectional studies
published as an original article. Ecological
studies, case reports, reviews and editorials were
not considered eligible.
For the meta-analysis, we selected the
articles fulfilling both of the following two criteria:
1 . The article contained sufficient information to
estimate the relative risk and 95% confidence
intervals (odds ratios [OR], relative risks or
crude data and corresponding standard errors,
variance, confidence intervals or P-values of
the significance of the estimates); and
2. The article reported an independent study (in
order to avoid giving additional weight to some
studies).
The selected articles were reviewed and data
abstracted by means of a standardized data-
collection protocol. When another article on the
same study was published simultaneously,
additional relevant or missing information was
retrieved from the companion paper. For each
study the following information was retrieved:
General information: year of publication,
recruitment years, study design, study loca-
tion and latitude of the region;
Exposure information: definition of type of
exposure, age at first exposure, duration of
exposure, year of exposure, place of exposure;
Case-control information: inclusion or exclusion
of specific histological types of melanoma,
number and source of cases and controls,
matching design, blinding of interviewers;
Statistical information: statistical methods
used, adjustment for confounding variables
(demographic factors such as age and sex,
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
baseline host characteristics such as hair, eye
and skin colour, inherent tendency to burn or
tan easily, naevi, sunburns or sun exposure)
and type of effect estimates (odds ratio,
relative risk, standardized incidence ratio)
with corresponding measures of precision,
according to specific exposure category.
The minimal common information about exposure
to indoor tanning devices for all studies was "ever
exposed". For those studies where the
definition of exposure "ever versus never exposed
to indoor tanning facilities" was not present, we
used the information closest to this category.
Since it has been suggested that age at
exposure may influence the relative risk for skin
cancer associated with UV exposure (Whiteman
eta/. , 2001 ), we extracted relative risks associated
with use of indoor tanning facilities before the age
of 35 years where available. Studies used
different age categories for classifying age at first
exposure, so odds ratios for the "young expo-
sure" category were pooled without correction.
Melanoma
We identified 23 studies of use of indoor tanning
facilities and melanoma (Kiepp & Magnus, 1979;
Adam eta/., 1981 ; Gallagher eta/., 1986; Holman
et a/., 1986; Holly et a/., 1987; Swerdlow et a/.,
1988; Osterl ind eta/. , 1988; Zanetti eta/., 1988;
MacKie eta/. , 1989; Beitner eta/., 1990; Walter et
a/., 1990 (and 1 999); Dunn-Lane et a/., 1993;
Garbe eta/., 1993; Westerdahl eta/., 1994; Autier
eta/., 1 994; Holly eta/., 1 995; Chen eta/., 1998;
Westerdahl eta/., 2000; Naldi eta/., 2000; Kaskel
et a/., 2001; Veiemd et a/., 2003; Bataille et a/.,
2004; Bataille et a/., 2005). All studies were
case-control studies, except for one cohort study
(Veier0d eta/., 2003). No cross-sectional studies
were identified. A case-control study was
considered population-based when cases were
derived from a population-based cancer registry
and controls selected from the general population.
Description of studies
(a) Cohort study- Veiered eta/. {2003): The only
published prospective cohort study was conducted
in Norway and Sweden, where 106 379 women
aged 30-50 years at inclusion were recruited
between 1991 and 1992. This population was
selected from the National Population Register
and followed for an average of 8.1 years. Among
these, 187 cases of invasive melanoma were
diagnosed during follow-up. The analysis was
stratified by age at the time of exposure to
sunbeds. Thirty-four cases occurred among the
14 377 women who were exposed at least once
a month during one of three age periods (1 0-19,
20-29 or 30-39 years). The corresponding risk
for melanoma for the entire cohort was 1.55 (con-
fidence interval (CI), 1.04-2.32) when adjusting
for age, region, hair colour, age-specific sunburns
and annual number of weeks of summer vaca-
tions. For the age group 20-29 years, the risk for
melanoma associated with solarium use more
than once a month compared with rarely or never
was 2.58 (CI, 1.48-4.50).
(b) Population-based case-control studies -
Adam eta/. (1981): A case-control study was
conducted in Oxford and the south-western
region of the United Kingdom between 1971 and
1976, recruiting 111 incident cases and 342 con-
trols to study the association between the oral
contraceptive and melanoma in women. Cases
were selected from two cancer registries and
when identified, were contacted through their
General Practitioner (GP) ; controls were selected
from the G P practice lists and matched to cases
for age, marital status and GP practice. Nine
cases and 1 0 controls had ever used sunlamps.
The crude odds ratio calculated [by the Working
Group] was 2.93 (CI, 1.16-7.40). [No estimate was
reported for the exposure to sunlamps. The working
group noted that 169 cases and 507 controls were
selected from the registry, but only 111 cases and
342 controls completed questionnaires.]
Holman eta/. (1986): A case-control study was
conducted in Western Australia between 1 980
and 1981 to evaluate constitutional traits, sunlight
exposure, hormones, diet and other possible risk
factors for cutaneous melanoma. This study
recruited 511 incident cases and 511 controls,
selected from the electoral roll and matched to
cases for age and sex. Past use of sunlamps was
21
Exposure to Artificial UV Radiation and Skin Cancer
recorded, but only 9% of subjects had used them.
The crude odds ratio for "ever use" compared to
"never use" of sunlamps was 1.1 (CI, 0.6-1.8).
Osterlind eta/. (1988}: A case-control study con-
ducted in East Denmark between October 1982
and March 1985 recruited 474 incident cases and
926 controls aged 2Q-79 years selected from the
National Population Register to study risk factors
for melanoma. Sixty-six cases and 168 controls
had ever used sunbeds, and 50% of controls had
used sunbeds less than 1 0 times. The crude odds
ratio for ever versus never use [calculated by the
Working Group] was 0.73 (CI, 0.53-1.01 ), and no
trend was observed with number of sessions.
Regarding exposure to sunlamps, 45% of cases
and 42% of controls had used sunlamps, with
40% of both cases and controls having used sun-
lamps less than 1 0 times. [No estimate was
reported for the use of a sunlamp.]
Zanetti et a/. (1988): A case-control study inves-
tigating melanoma risk factors was conducted in
Torino, Italy between May 1984 and October
1986. The authors identified 208 incident cases in
the "Registro Tumori Piemonte" registry and
selected 416 controls from National Health
Service files. Of these, 15 cases and 21 controls
had used UVA lamps for tanning purposes. The
risk for melanoma from this exposure was 0.9
(CI , 0.4-2.0) after adjustment for age, hair colour,
skin reaction, sunburn in childhood and educa-
tion level. The use of sunlamp for tanning was
very rare in Italy during the study period, and the
authors warned about the consequent lack of
power of the study.
Walter et a/. (1990): A case-control study,
designed specifically to investigate the
melanoma risk associated with artificial UV expo-
sure, was conducted in southern Ontario,
Canada between October 1984 and September
1986. Recruitment included 583 incident cases
identified from pathology reports and 608 con-
trols selected from property tax assessment rolls.
Controls were matched to cases for sex, age and
place of residence; 152 cases and 109 controls
had ever been exposed to sunlamps or sunbeds.
The risk for melanoma, adjusted for skin reaction
22
to initial summer exposure, was 1.54 (CI,
1.16-2.05). The relative risk in the youngest age
group (2Q-34 years) was 1.51 (CI, 0.82-2.77).
When duration of exposure to tanning appliances
was analysed by category (never; <12 months;
12 months), a significant trend was observed
both for men (p < 0.01) and for women (p = 0.04).
[This study was initially published in 1990 (Walter
et a/., 1990). Further calculations with new
adjustments were published in 1999 (Walter et
a/. , 1999).]
Westerdahl et a/. (1994}: A case-control study
was conducted in Sweden between July 1988
and June 1990. The authors recruited 400 inci-
dent cases selected from the regional tumour
registry, and 640 controls selected from the
National Population Registry, aged 15 to 75
years. Controls were matched to cases for age,
sex and place of residence. Of these, 111 cases
and 159 controls had ever used sunbeds or sun-
lamps. The relative risk, adjusted for sunburns,
hair colour, naevi number and sunbathing habits
during summer, was 1.3 (CI, 0.9- 1.8). Among
individuals aged $ 30 years, the relative risk was
2.7 (CI, 0.7-9.8). When exposure exceeded 10
sessions per year, the risk for melanoma was
significantly increased over that of never-users
(OR, 1.8; Cl, 1.0-3.2).
Holly et a/. (1995): A case-control study on
melanoma risk factors was conducted in San
Francisco, USA between January 1981 and
December 1986. The study was restricted to
women aged 25-59 years. The authors recruited
452 incident cases ascertained through the
SEER Registry for the San Francisco Bay area
and 452 controls ascertained using telephone
random digit dialling. Controls were frequency-
matched to cases for age in 5-year categories.
Exposure to sunlamps was investigated. No
association was observed for ever using a sun-
lamp (crude OR, 0.94; Cl , 0.74- 1.2). [The
Working Group noted that use of sunlamps by
63% of cases and 62% of controls, as presented
in the text, would result in an odds ratio of 1.05
(CI, 0.79-1.38). Despite this inconsistency, it was
decided to use the estimate given in the table.)
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
Chen et a/. (1998): A case-control study was
conducted in Connecticut, USA between January
1987 and May 1989. Using the population-based
Rapid Case Ascertainment System, 624 incident
cases were identified and 512 controls ascer-
tained using telephone random digit dialling. Of
these, 141 cases and 95 controls had ever used
a sunlamp or sunbed. The risk for melanoma
associated with sunlamp or sunbed exposure
was 1.13 (CI, 0.82-1.54) after adjustment for
age, sex, cutaneous phenotype index and recre-
ational sun exposure index. In a stratified analy-
sis, the relative risk associated with first exposure
before age 25 years was 1.35 (CI, 0.88-2.08). No
trend was observed in relation to duration of
exposure to sunlamps-or sunbeds.
Westerdahl et a/. (2000): A case-control study
was conducted in the South Health Care region
of Sweden between January 1995 and June
1997. The authors recruited 571 incident cases
identified in the regional tumour registry, and 913
controls matched for age and sex ascertained
from the National Population Registry. Of these,
250 cases and 372 controls had ever used
sunbeds. The risk for melanoma associated with
sunbed exposure was 1.2 (CI, 0.9- 1.6) after
adj ustment for age, sex, history of sunburn, hair
colour, skin type and number of raised naevi. No
change in the estimate was observed after
adjustment for sunbathing habits. In a stratified
analysis, there was a significant increase in risk
when exposure took place before the age of 35
years (OR, 2.3; Cl, 1.2-4.2). No trend relating to
total duration of exposure was observed.
(c) Hospital- or clinic-based case-control studies
Klepp & Magnus (1979): A hospital-based
case-control study was conducted in Oslo,
Norway between January 1974 and May 1975.
The authors enrolled 89 cases and 227 controls
aged 20 years or more to evaluate possible etio-
logical factors for melanoma. Cases were incident
cutaneous melanomas from the Norwegian
Radium Hospital; controls were other cancer
patients in the same hospital. The self-adminis-
tered questionnaire included a question about
use of artificial UV lamps. No estimates were
derived from the results because exposure to UV
lamp was very rare, and there was no difference
between cases and controls.
Gallagher eta/. (1986): A case-control study was
conducted in western Canada between April
1979 and March 1981. To study risk factors for
melanoma, including host factors, sun exposure,
and the use of oral contraceptive for women, 595
incidence cases from dermatology practice and
595 controls from provincial medical plans were
recruited. Controls were matched to cases for
age and sex. The recruitment was limited to indi-
viduals 20-79 years old. No estimate of the risk
was presented. The study showed no association
between sunlamp use and subsequent risk for
melanoma (X
2
=6.1; 5 df; p=NS), including after
stratifying by sex or by anatomical site exposed to
the sunlamp.
Holly eta/. (1987): A hospital-based case-control
study was conducted in San Francisco (USA)
between April1984 and October 1987. To assess
melanocytic naevi (dysplatic and non-dysplastic
naevi) as risk factor for melanoma, 121 incident
cases were recruited from a melanoma clinic at
the University of California, San Francisco, and
139 controls were recruited among patients in
another clinic at the same university. No estimate
of the risk for melanoma associated with sunbed
use was presented. The patients with cutaneous
melanoma were similar to those in the control
group with respect to their use of tanning salons.
Swerdlow et a/. (1988): A hospital-based case-
control study was conducted in Scotland (United
Kingdom) between 1979 and 1984 to evaluate
the role of fluorescent light and UV lamps on
cutaneous melanoma risk. The authors recruited
180 incident cases from dermatology and plastic
surgery units and 197 hospital inpatients and out-
patients as controls excluding those with malig-
nant disease. Analysis for exposure to tanning
appliances was restricted to 120 controls without
dermatological disease. Only 38 cases and 1 0
controls had ever used UV lamps or sunbeds
(crude OR, 2.94; Cl , 1.40-6.17). Data by age at
first use (before and after age of 30 years) and by
total number of hours of exposure (1-19 hours;
20 hours within the 5 years before presentation)
23
,.
Exposure to Artificial UV Radiation and Skin Cancer
were also presented. A significant linear trend for
duration of use was observed (p<0.01 ).
Adjustment for hair colour, eye colour, skin type
or sun exposure did not substantially change the
estimates, while a small decrease was observed
when adjusting for number of naevi.
MacKie eta/. (1989): A hospital-based case-control
study of melanoma was conducted in Scotland,
United Kingdom in 1987. The authors identified
280 incident cases (99 men and 181 women)
through the Scottish Cancer Registry; 280 con-
trols (99 men and 181 women) were recruited at
a hospital, excluding patients with dermatological
illness. Controls were matched to cases for age
and sex. In the questionnaire, one item investi-
gated exposure to artificial UV radiation and use
of sunbeds; 33 cases and 8 controls had been
exposed to such sources. The odds ratio was
stratified by sex and adjusted for total number of
naevi, atypical naevi, freckling tendency, history
of severe sunburns, tropical residence for more
than 5 years and skin type. The adjusted odds
ratios were 1.3 (CI, Q.2-7.9) for men and 1.2 (CI,
0.5-3.0) for women. Only 26 cases and 6 controls
had used "modern sunbeds" once or twice weekly
for at least 12 weeks. [Due to stratification by sex,
two estimates from this study were used in the
analysis.]
Beitner et al. (1990): A case-control study was
conducted in Stockholm, Sweden between
February 1978 and December 1983. The authors
recruited 523 incident cases from the
Department of Oncology at Karolinska Hospital
and 505 controls selected from population reg-
istries. Controls were matched to cases for age
and sex. No estimate of the risk was presented.
No increase in the risk for developing cutaneous
malignant melanoma was associated with fre-
quent exposures to solaria.
Dunn-Lane et a/. (1993): A hospital-based
case-control study was conducted in Dublin,
Ireland between 1985 and 1986. The authors
recruited 100 incident cases from seven Dublin
hospitals and 100 controls, admitted for limb
injuries in the accident and emergency and
orthopaedic departments, were recruited.
24
Controls were matched to cases for age (within 5
years), sex and health broad area of residence.
Seventeen cases and 15 controls had ever used
sunbeds. The crude odds ratio [calculated by the
Working Group] was 1.16 (CI, 0.54-2.47). [No
estimates were reported by the authors.]
Garbe eta/. {1993): A hospital-based case-con-
trol study evaluating risk factors for melanoma
was conducted in Germany between 1984 and
1987. The authors studied 856 cases selected
from the Central Malignant Melanoma Registry of
the German Dermatology Society and 705
controls selected from outpatients presenting at
dermatology clinics. Of these, 66 cases and 50
controls had ever used sunbeds. The relative risk
for melanoma, adjusted for number of naevi, hair
colour, skin type, age and study centre, was 1.5
(CI, 0.9-2.4). [The Working Group noted that the
Central Malignant Melanoma Registry is a volun-
tary registry.]
Autier et a/. (1994): A case-control study of
melanoma was conducted in Europe (Germany,
France, Belgium) from January 1991 onwards.
The authors recruited 420 incident cases from
dermatology practices and cancer centres; 447
controls were selected from neighbourhood by
door-knock. Of these, 11 0 cases and 120 con-
trols had ever been exposed to sunlamps or
sunbeds. While there was no crude association
with melanoma (OR, 0.97; Cl, 0.71-1.32) , in a
stratified analysis total exposure to sunlamp or
sun bed for tanning purposes for more than 1 0
hours and before 1980 showed an increased risk
(OR, 2.12; Cl, 0.84-5.37) after adjustment for
age, sex, hair colour and number of holiday
weeks per year. The risk for melanoma associated
with sunlamp or sunbed use was significantly
increased if exposures for more than 10 hours
were accompanied by a burn to the skin (OR,
7.35; Cl, 1.67-32.3).
Naldi eta/. (2000}: A hospital-based case-control
study of melanoma was conducted in Italy
between June 1992 and February 1995. The
authors recruited 542 incident cases from oncol -
ogy and dermatology centres, and 528 controls
admitted to the hospital for a non-dermatologic or
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
non-neoplastic illness. Of these, 30 cases and 36
controls were ever exposed to sunbeds or sun-
lamps. The risk for melanoma, adjusted for age,
sex, marital status, education, eye and skin
colour, number of naevi , freckles density, sun-
burns and number of sunny vacations, was 0.78
(CI, 0.45-1.37).
Kaskel eta/. (2001): A hospital-based case-con-
trol study of melanoma was conducted in Munich,
Germany between June 1996 and April 1997.
The authors recruited 271 prevalent cases (diag-
nosed from 5 years to 6 months before inclusion)
from the Tumour Centre in Munich, and 271 con-
trols from hospital departments of general surgery
and ophthalmology. Controls were matched to
cases for age (in 5-year categories), sex and
place of residence. Among the 56 factors
explored, one item investigated exposure to UV
radiation or UV beds more than 5 times per year
compared with 5 times per year or less. In the
analysis of discordant pairs, the crude risk for
artificial UV exposure was 1.0 (CI, 0.6-1.8).
Bataille eta/. (2004): A hospital-based case-con-
trol study of melanoma was conducted in the
North East Thames region (United Kingdom)
between August 1989 and July 1993. The authors
recruited 413 cases and 416 controls aged 16 to
75 years old. Incident cases of histologically con-
firmed melanomas were recruited from hospitals
and general practices. Controls were also recruited
through hospitals and general practices, excluding
patients attending for a skin disease. One hun-
dred cases and 11 0 controls had ever been
exposed to sunbeds. The risk for melanoma
associated with sunbed use was 1.19 (CI,
0.84-1.68), after adjusting for age and sex.
Further adjustment for skin type and other sun
exposure measures did not affect the results. In a
stratified analysis, if sunbed exposure took place
before the age of 45 years, the relative risk was
1.2 (CI, 0.76-1.90). No trend toward increased
risk was observed with increasing lifetime dura-
tion of exposure.
Bataille et a/. {2005) : A case-control study
designed specifically to investigate melanoma
risk associated with sunbed exposure was con-
ducted in Belgium, France, the Netherlands,
Sweden and the United Kingdom between
December 1998 and July 2001. The authors
recruited 597 incident cases from dermatology or
oncology clinics or identified through pathology
laboratories. The method of recruitment of 622
controls differed according to each centre: popu-
lation register in Sweden, neighbourhood
controls in Belgium and France, and general
practices in the Netherlands and the United
Kingdom. Of these, 315 cases and 354 controls
had ever used sunbeds. The risk for melanoma
associated with sunbed use was 0.9 (CI,
0. 71-1 .14) when adjusting for age, sex and skin
type. If exposure to tanning appliances occurred
before age 15 years, the relative risk was 1.82
(CI, 0.92-3.62) . No trends in risk for melanoma
were observed with increasing lifetime exposure
or with increasing time since first exposure. No
association was observed when stratifying by
type of sunbed. [A companion paper warned
about potential biases that could have occurred
in this study: selection bias of controls and mis-
classification of cases who tended to underreport
their exposure (de Vries eta/. , 2005)].
Of these 23 studies, 4 studies were excluded-
in accordance with the selection criteria-
because they did not include estimates of the
relative risk for cutaneous melanoma associated
with exposure to tanning appliances (Kiepp &
Magnus, 1979; Gallagher eta/., 1986; Holly eta/.,
1987; Beitner eta/., 1990).
Another study (Walter eta/., 1990) which pre-
sented an evaluation of "ever" versus "never"
exposed to artificial UV radiation was excluded
because it involved the same population as a later
publication (Walter eta/., 1999); moreover, it pre-
sented crude rather than adjusted relative risks.
However, the estimate for "first exposure before
age 35 years" from the early publication (Walter et
a/. , 1990) was included in the relevant section.
Quantitative approach: meta-analysis
(a) Evaluation of exposure: Four types of expo-
sure to indoor tanning appliances were evaluated:
"ever" versus "never";
"first exposure before age 35 years" versus "never".
25
Exposure to Artificial UV Radiation and Skin Cancer
In addition, another concept was considered in
order to make a comparison between recent and
distant exposures:
"exposure distant in time" versus "never";
"exposure recent in time" versus "never".
A dose-response model was not considered
for this meta-analysis because of the hetero-
geneity among the categories of duration and
frequency of exposure used by different authors.
(b) Study characteristics: Table 7 provides an
overview of all the studies retrieved, including the
19 studies reporting estimates that could be
included in the meta-analysis (for a total of 7 355
cases). The first (publ ished in 1981) and the last
(published in 2005) studies included were pub-
lished more than 20 years apart. Three
case-control studies presented a time lag
between first recruitment year and publication of
1 0 years or more.
Fifteen studies were carried out in European
countries, four of which were in Scandinavian
countries; two were conducted in the United
States, one in Canada and one in Australia. The
mean latitude of the study centres was 50
(range 25!L59
2
) ; eight studies were conducted in
countries with average latitude below 50.
(c) Types of estimate presented: Since melanoma
is a rare disease, we ignored the distinction
between the various estimates of relative risk (i.e.
odds ratio, rate ratio, risk ratio), and all measure-
ments were interpreted as odds ratios.
Except for the studies by Kaskel eta/. (2001)
and by Veierod eta/. (2003) , all studies presented
estimates for "ever" versus "never" exposed to
artificial UV radiation (Table 8). Thirteen of 19
studies presented positive estimates for "ever"
versus "never" exposed to sunbed/sunlamps, but
only four were statistically significant. For seven of
these studies it was possible to obtain only crude
relative risks, one adjusted for age and sex only.
The cohort study (Veiemd eta/., 2003) pre-
sented an estimate for the widest age interval
included (1 Q-39 years) , only for the comparison
":?: 1 time per month" versus "never/rarely" . One
study (Kaskel eta/., 2001) presented an estimate
only for the comparison ">5 times per year"
26
versus "::;: 5 times per year".
Five studies (Swerdlow eta/., 1988; Walter et
a/., 1990; Chen et a/., 1998; Westerdhal et a/.,
2000; Bataille eta/. , 2005) also presented an esti-
mate for first exposure at age s 35 years (Table
9). Veierod eta/. (2003) presented relative risks
for ":?: 1 time per month" versus "never" in the age
period 2Q-29 years; Westerdhal et a/. (1994)
presented estimates of "ever" versus "never" for
individuals younger than 30 years. All relative
risks were adjusted for confounders related to
sun exposure or sun sensitivity, except in the
study by Walter eta/. (1990). All these estimates
were considered for the evaluation of "first expo-
sure before age 35 years" versus "never".
Five studies investigated time since exposure
(Table 1 O) and reported estimates that allowed
comparisons between recent and distant expo-
sure: number of years of exposure before pres-
entation (Swerdlow et a!., 1988; Bataille et a!.,
2005), number of years since last exposure
(Walter et a/., 1990) and age at first exposure
(Autier eta!. , 1994; Chen eta/., 1998).
(d) Selection of data and methods of analysis:
Every measure of association adjusted for the
maximum number of confounding variables and
corresponding confidence interval were trans-
formed into log RR, and the corresponding vari-
ance was calculated using the formula proposed
by Greenland (1987). Where no estimates were
given, crude estimates were calculated from tab-
ular data, using Asymptotic Mantei-Haenszel
estimates to evaluate the 95% Cl of the log odds
ratio.
Most estimates included all subjects, combining
sexes. One study presented results separately for
women and men with no combined data; both
estimates were included (MacKie eta/., 1989).
The homogeneity of the effects across studies
was assessed using the large sample test based
on the Chi-square statistic (Chi). Since the Chi-
square test has limited power, we considered
statistically significant heterogeneity at the
P=0.1 0 level of association. A further measure of
heterogeneity, H (the square-root of Chi-square
divided by its degrees of freedom), has been con-
sidered in order to make comparisons between
heterogeneities of pooled estimates summarizing
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
Table 7. Characteristics of studies considered for the meta-analysis on melanoma
Reference Country First Year Number Histological di agnosis Participation
of controls {%)
Cases Controls
Cohort study
1
Veier0d eta/. (2003) Norway, Sweden 1992 187 106 379
2
HC invasive M 54.5
3
Populatlonbased studies
'Adam eta/. (1981) UK 1971 169 207 HCM 68
Gallagher eta/. (1986) Western Canada 1979 595 595 M excluding LMM and ALM 48
'Holman eta/. (1986) Australia 1982 511 511 HC pre-invasive/ invasive M 69
'Osterlind eta/. (1988) Denmark 1985 474 926 HCM excluding LMM 81.7
'Zanetti eta/. (1988) Italy 1984 208 416 M in situ and all other 68.2
histology
Beitner eta/. (1990) Sweden 1978 523 505 HCM (SSM, NM. LMM, 96.2
unclassif. MM)
Walter eta/. (1990) Canada 1984 583 608 HCM in situ and Hutchinson's 81
freckle, LMM
'Westerdahl el a/. (1994) Sweden 1990 400 640 Invasive M 77.4
'Holly el a/. ( 1995) USA 1986 452 930 HCM 77
'Chen eta/. (1998) USA 1969 624 512 HC fi rst primary invasive M 70
'Walter eta/. (1999) Canada 1966 583 608 HCM in situ and Hutchinson's 81
freckle, LMM
'Westerdahl at a/. (2000) Sweden 1997 571 913 HC first primary invasive M 68
Other studies
Klepp & Magnus (1979) Norway 1974 78 131 M NR
Holly el a/. ( 1987) USA 1984 121 139 NMorSSM NR
1
Swerdlow eta/. ( 1988) UK 1988 160 120 PrimaryM NR
'MacKie eta/. (1989) UK 1987 280 180 Invasive M NR
' Dunn-Lane et a/. (1993) UK 1986 100 100 M excluding LMM and ALM NR
' Garbe eta/. (1993) Germany 1987 280 280 M NR
'Autier eta/. (1994) Belgium, France & 1991 420 447 HCM 78
Germany
' Naldi eta/. (2000) Italy 1993 542 538 M NR
' Kaskel eta/. (2001) Germany 1996 271 271 HCM NR
' Bataille eta/. (2004) UK 1993 413 416 M including in situ and LMM NR
' Bataille eta/. (2005) UK 1998 597 622 HC first primary invasive M NR
excluding LMM
included in the meta-analysis; cohort size: response rate.
ALM, acral lentiginous melanoma; HC, histologically confirmed: LMM, lentigo maligna melanoma; M, melanoma; MM. malignant
melanoma; NM, nodular melanoma; NR, not reported; SSM, superficial spreading melanoma.
27
Exposure to Artifici al UV Radiation and Skin Cancer
Table 8. Estimates included in the evaluation of an association of ever use of indoor tanning
facilities and risk for melanoma
Reference Exposure comparison Adjustment
Adam eta/. (1981) Ever use of sunlamps vs never Crude
Holman et a/. ( 1986) Ever use of sunlamps vs never 1.1 (0.6-1. 8) Cnude
Osterlind et a/. (1988) Ever use of sun beds vs never 0.73 (0.53-1.01) Cnude
Swerdlow eta/. (1988) Ever use of UV lamps/ sunbeds vs 2.94 (1.41-6.17) Cnude
never
Zanetti et a/. (1988) Use of UVA lamp for tanning 0.9 (0.4-2.0) Age, hair colour, skin reaction,
purpose: yes/no sunburn in childhood, education
level
MacKie et al. (1989) Ultraviolet use: some vs none 1.3 (0.2- 7.9) Naevi, freckles, sunburns, tropical
(men) residence, phototype
MacKie et al. (1989) Ultraviolet use: some vs none 1.2 (0.5--3.0) Naevi, freckles, sunburns, tropical
(women) residence, phototype
Dunn-Lane eta/. Ever use of sun beds vs never 1.16 (0.54- 2.47) Cnude
(1993)
Garbe et a/. (1993) Use of sunbeds: yes/no 1.5 (0.9-2.4) Age, naevi, hair colour, phototype,
study cent re
Autier et al. (1994) Ever exposed to 0.97 (0.71-1.32) Crude
sunl amps/sunbeds vs never
Westerdahl eta/. (1994) Ever exposed to 1.3(0.9- 1.8) Sunburns, hair colour, naevi,
sunbedslsunlamps vs never sunbathing
Holly et al. (1995) Ever use of sunlamps vs never 0.94 (0.74-1.2) Crude
(women)
Chen et al. (1998) Ever use of sunlamps vs never 1.13 (0.82- 1.54) Sex, age, phenotype, recreational
sun exposure
Walter et al. (1999) Ever use of sunbeds/sunlamps vs 1.54 (1.16-2.05) Sex, age, skin reaction to initial
never summer sun exposure
Naldi et al. (2000) Ever use of sunbeds/sunlamps vs 0.78 (0.45-1 .37) Sex, age, skin, hair, eye, naevi,
never freckles, sunburn, number of sunny
vacations
Westerdahl et al. (2000) Ever use of sunbeds vs never 1.2 (0.9-1.6) Sunburns, hair colour, skin type,
raised naevi
Kaskel et al. (2001) Artificial UV radi ation/UV beds: 1.00 (0.6-1 .8) Crude
>5/year vs :s5/year
Veier0d et al. (2003) Solarium use : 2:1/month vs 1.55 (1 .04-2.32) Age. region of residence. hair
(women) never/rarely colour, sunburns, summer vacations
Bataille et al. (2004) Ever use of sun beds vs never 1.19 (0.84- 1.68) Sex, age
Bataille eta/. (2005) Ever use of sunbeds or sunlamps 0.90 (0.71-1.14) Sex, age, skin phototype
vs never
28
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
Table 9. Estimates included in the evaluation of an association of first use of indoor tanning
facility in youth and risk for melanoma
Reference Definition
Swerdlow eta/. (1988) Age at first exposure <30 years vs
never
Relative risk
(95% Cl)
3.8 (0.9--16.5)
Adjustment
Naevi, skin type, hair and
eye colour, sun exposure
Walter eta/. (1990) Age at first use <30 years vs never 1.67 (1.17-2.39) Age
Westerdahl eta/. (1994) Ever use of sunbed at age younger 2.7 (0.7- 9.8) Sunburns, hair colour,
naevi , sunbathing than 30 years
Chen eta/. (1998) Age at first use of sunlamp < 25
years vs never
1 .35 (0.88-2.08) Sex, age, phenotype index,
recreational sun exposure
Westerdahl et a/. (2000) Age at first exposure s; 35 years vs 1 .6 {0.9--2.9) Sunburns, hair colour,
skin type, naevi
Veiemd et al. (2003)
Bataille et at. (2005)
never
Exposure at age 2D-29:
~ 1 time/month vs never
Ever sunbed use before age
15 years vs never
2.58 (1.48-4.50)
1 .82 {0.92- 3.62)
Age, region of residence,
sunburns, summer
vacations
Age, sex, skin type
Table 10. Estimates included in the evaluation of an association of distant and recent exposure
and risk for melanoma
Reference
Swerdlow et a/.
(1988)
Walter eta/. {1990)
Autier eta/. (1994)
Chen eta/. (1998)
Bataille et a/. (2005)
Definition
Less than 5 years before
presentation vs never
More than 5 years before
presentation vs never
Less than 5 years since last use
vs never
More than 5 years since last use
vs never
First use in 1980 or later ~ 1 0 hr
of exposure for tanning purposes)
First use before 1980 ~ 1 0 h r of
exposure for tanning purposes)
First use after 1970
First use before 1970
< 6 years between first sunbed use
and interviews
;:: 15 years between first sunbed use
and interviews
Relative risk
(95% Cl)
1.9 (0.6-5.6)
9.1 (2.0-40.6)
Men, 1.52 (0.56-4.25)
Women, 1.24 (0.67-2.31)
Men, 2.00 (1 .21-3.34)
Women, 1.53 {0.96-2.46)
0.99 (0.49--2.00)
2.12 (0.84-5.37)
1.15 {0.64-2.07)
1.33 (0.84-2.12)
0.91 (0.58-1.42)
0.97 (0.70-1.34)
Adjustment
Age, sex,
residence
Age
Age, sex, hair
colour, holiday
weeks spent in
sunny resorts
Sex, age,
phenotype index,
recreational sun
exposure
Sex, age, skin
type
29
Exposure to Artificial UV Radiation and Skin Cancer
different numbers of studies. Greater values of H
indicate larger heterogeneity (Higgins &
Thompson, 2002).
The summary relative risk was estimated by
pooling the study-specific estimates by random
effects models even when heterogeneity was
found to be not significant and H was very low, in
order to be conservative and to enable generali-
zation of the results. For mixed effects models,
SAS was used (SAS Institute Inc. SAS Windows
version 8.02, 1999, Cary, NC) with PROC MIXED
(van Houwelingen et a/., 2002). These models
allowed taking into account between-study vari-
ability and non-independence of estimates origi-
nating from the same study.
Subgroup analyses and meta-regressions
were carried out to investigate inter-study hetero-
geneity (Colditz eta/., 1995). Heterogeneity was
investigated by looking at all factors concerning
the type of study, analysis, exposure and features
of the population that could influence the esti-
mates. Studies conducted in different populations
living at substantially different latitudes were not
included in the heterogeneity analysis that evalu-
ated latitude.
A sensitivity analysis was conducted to eval-
uate the stability of the pooled estimates and the
influence of individual studies. To verify whether
publication bias might affect the validity of the
estimates, funnel plots were plotted using Copas
and Shi's method (Copas & Shi , 2001) and the
funnel plot regression of Ln(RR) on the sample
size, weighted by the inverse of the pooled vari-
ance (Macaskill eta/., 2001 ).
Table 11. Meta-analysis of all studies included
(e) Pooled estimates: Results of the meta-analy-
sis of all studies included are shown in Table 11
and Figure 2. Between-study heterogeneity was
found significant for being "ever" versus "never"
exposed to artificial UV (Chi=35.40, degrees of
freedom (d.f.) =19, P=0.013). The pooled
estimate indicated a borderline-significant posi-
tive association between "ever" versus "never"
use of sunlamps/sunbed and melanoma (RR,
1.15; Cl, 1.00-1 .31 ).
When "first exposure before age 35 years"
was analysed, a significant 75% increase in risk
was detected (Table 11; Figure 3) and the Chi-
square testing heterogeneity was non-significant
(Chi= 4.95, d.f. = 6, P = 0.55) and H (= 0.91) was
smaller than the value obtained for "ever" versus
"never" (H = 1.37).
The number of studies presenting an
assessment of time since exposure was low
(n = 5); however all studies presented greater
estimates for exposures more distant in time com-
pared to more recent exposures. Heterogeneity was
greater for "distant exposure" (H = 1.65 and Chi
=13.63, d.f. = 5, P = 0.018) than for "recent expo-
sure" (H = 0.67 and Chi = 2.52, d.f. = 5, P = 0.81 ).
It is interesting to note that exposures more
distant in time led to an increased risk compared
with recent exposures, consistently with the higher
risk for "first exposure before age 35 years"
versus "never'' compared to "ever" versus "never".
In order to decrease the influence of biases,
estimates were calculated including only the
cohort and population-based case-control studies
(Table 12). The pooled relative risks were very
similar apart from wider confidence intervals.
Exposure Number of Summary relative risk (95% Cl) Heterogeneity
1
studies P-value x
2
H
Ever use of indoor tanning facility 19 1.15 (1.0G-1.31) 0.013 1.37
First exposure in youth 7 1. 75 (1.35-2.26) 0.55 0.91
Exposure distant in ti me 5 1.49 (0.93-2.38) 0.018 1.65
Exposure recent in ti me 5 1.10 (0.76-1.60) 0.81 0.67
1
The degrees of freedom for the Chi-square are given by the number of databases included minus one, not by the
number of studies.
30
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
Figure 2. Relative risk for cutaneous melanoma associated with ever use of indoor tan-
ning equipment: estimates of 19 studies and summary estimate
Studies
Adameta/.(1981)
Holman eta/.(1986)
o.terlind eta/. ( 1988)
Swerdlow et a/.(1988)
Zanerti., al. (1988)
Mackie eta/.(1989, Men)
Mackie eta/(1989, Women)
Dunn-Lane c/a/.(1993)
Garbe et a/.(1993)
Au tier et a/. ( 1994)
Westerdnhlet al. (1994)
Holly et al (1995)
Cheneta/.(1998)
Wal!eret al. (1999)
Nldi eta/. (2000)
Wes!erdah.l eta/. (2000)
Kaslccl et a/. (2001)
Veierod et a/.(2003)
Bataille I a/. (2004)
Dnta.ille eta/. (2005)
Summary relative risk
0.5
--
-II 1--
---
-
<>
1.15 (1.00, 1.31)
1.0 1.5 2.0 2.5 3.0 5.0 7.0
Relative risk
Figure 3. Relative risk for cutaneous melanoma associated with first use of indoor tanning
equipment at age <35 years: estimates of 7 studies and summary estimate
Studies
Swerdlow eta/. (1988)
Westerdnbl et al. (1994)
Chen eta/. (1998)
Walter eta/. ( 1999)
Westerdahl eta/. (2000)
Veierod et al. (2003)
Bataille el al. (2005)
Summary relative risk
I
0.5
-
-
-
<>
1. 75 (1.35-2.26)
l.O 1.5 2.0 2.5 3.0 5.0 7.0
Relative risk
31
Exposure to Artificial UV Radiation and Skin Cancer
Table 12. Meta-analysis of the cohort and population-based case-control studies included
Exposure Number of Summary relative risk Heterogeneity
studies (95% Cl)
P-value X
2
H
Ever use of indoor tanning facility 10 1.17 (0.96-1.42) 0.011 1.540
Age at first exposure in youth 5 1.71 {1.25-2.33) 0.435 0.973
Exposure distant in time 2 1.58 (0.25-9.98) ' 0.502 0.830
Exposure recent in time 2 1.24 (0.52- 2.94) 0.762 0.521
'The confidence interval is very wide because this analysis includes only 2 studies, one of which has two estimates.
(f) Heterogeneity analysis: For the comparison of
"ever" versus "never", which included the largest
number of studies, several factors that could
influence the variability among estimates were
investigated. This analysis revealed that studies
with a longer time lag between the first year of
recruitment and 10 years) presented
higher estimates (Table 13). (The cohort study
was excluded from this analysis because of the
nature of the study design.)
Studies carried out in countries at higher
latitudes presented higher relative estimates than
did studies carried out at lower latitudes (Table 13
and Figure 4).
Adjustment for confounders related to sun
exposure and sun sensitivity led to a higher
pooled estimate compared with studies considering
only crude relative risks or relative risks adjusted
only for age and sex (Table 13). In the analysis
restricted to the eight studies that adjusted for
Table 13. Heterogeneity analysis
confounders related to sun exposure and sun
sensitivity, the pooled relative risk remained simi-
lar to the summary estimate for all 19 studies but
the confidence interval widened (RR, 1.19; Cl,
0.33--4.30). The difference between adjusted and
crude pooled relative risks may not be due to the
adjustment in itself but to the fact that well-con-
ducted studies usually adjust for sun exposure
and sun sensitivity, which could be an indicator of
the quality of the analysis.
(g) Sensitivity analysis: A series of analyses were
performed to test the stability and sensitivity of
the analysis (Table 14). Inclusion criteria were
tested by including the estimates reported by
Walter and colleagues in 1990 instead of those
reported in 1999. Also, the studies that did not
report any relative risk (Kiepp & Magnus, 1979;
Gallagher eta/., 1986; Holly eta!. , 1987; Beitner
et a!., 1990) were included by imputing the
Number of Pooled relative risk Heterogeneity
Parameter analysed
studies (95% Cl)
P-value X
2
Number of years between recruitment and 3 1.38 (0.25- 7.46) 0.16
pub I ication 1 0
Number of years between recruitment and 15 1.06 (0.50-2.27) 0.14
publication <1 0
Estimate adjusted for phototype/sun 10 1.19 (0.45-3.12) 0.17
exposure/sunburns
Crude estimate or estimate adjusted for age 9 1.03 {0.31-3.40) 0.018
and sex only
Latitude of study centre <50 8 1.08 (0.31 - 3. 78) 0.73
Latitude of study center >50 o 11 1.20 (0.41-3.46) 0.003
32
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
Figure 4. Correlation between latitude of study centre and relative risk for melanoma
associated with use of indoor tanning facilities
1.5
-0.5 +------.,.--- - -----..,r-------.------1
20 30 40 50 60
Latitude (in degrees) for the region of each study
m1ss1ng estimates from data available in the
reports. Where no data at all were presented but
an indication of non-significant effect was given,
a relative risk of 1 and a standard error equal to
the mean standard error of the other studies was
considered. The pooled relative risks did not
change considerably (Table 14).
In order to verify the stability of the results, a
new analysis was carried out taking out the
estimate from the cohort study (Veiemd et a/.,
2003) . The pooled relative risk showed a wider
confidence interval.
The definitions used to evaluate the risk for
"first exposure before age 35 years" differed for
two studies: one study presented an estimate of
"ever" versus "never" for individuals aged 30
years (Westerdahl et a/. , 1994); the other study
(Veiemd et a/., 2003) presented two estimates:
"ever" versus "never" at age 1 0-19 years and ";;::: 1
time/month" versus "never" at age 20-29 years.
For the latter study, the estimate including a larger
number of individuals (age group 20-29 years) was
used for the main analysis of "first exposure before
age 35 years" (only 4 cases were in the exposed
group for the estimate at age 10-19 years). When
both studies were excluded, the pooled estimate did
not change considerably (Table 14).
For the evaluation of recent and distant expo-
sures, Autier et al. ( 1994) reported estimates by
several substrata; for the main analysis we selected
the adjusted relative risk evaluating exposure for
tanning purposes and for a duration of 10 hr or
more. Crude relative risks obtained by merging all
categories were: for "distant exposure" , 1.22
(CI, 0.79-1 .88) and for "recent exposure", 0.82
(CI, 0.56-1 .19). Thus the pooled relative risk for
"distant exposure" remained greater than that for
"recent exposure" (data not shown).
Analysis by Funnel plot regression gave no indi-
cation of publication bias ("ever used sunbed/sun-
lamps", P = 0.80; "first exposure before age 35
years", P = 0.1 0). In addition, analysis by the Copas
and Shi method of trends in the funnel plots
(Figures 5 and 6) gave an indication of non-signifi-
cant asymmetry ("ever used sunbed/sunlamps",
P = 0.37; "first exposure before age 35 years", P =
0.15).
Discussion
To establish a causal link between exposure to tan-
ning appliances and melanoma occurrence, studies
should show whether there are dose-effect rela-
tionships and whether exposures distant in time are
33
Exposure to Artificial UV Radiation and Skin Cancer
Table 14. Sensitivity analysis
Parameter
analysed
Inclusion criteria Number of
Ever use of indoor
tanning facility
Including study by
Walter eta/. (1990)
studies
19
Including all studies 23
First exposure in
youth
considered
Excluding the
cohort study by
Veier0d eta/. (2003)
Excluding the
cohort study by
Veier0d et a/. (2003)
Including only
those studies with
a specific definition
of first exposure
(studies by Veiered
et a/. 2003 and
Westerdahl eta/.,
2000 excluded)
more strongly associated with melanoma than are
recent exposures. The latter point is important, as
there is most probably a latency period between
exposure and melanoma, thus the carcinogenic
effect of more recent exposures would not yet be
detectable. Also, since the fashion of using indoor
tanning facilities has been increasing steadily, a
lack of distinction between distant and recent expo-
sures may mask an actual increase in risk.
Experimental and epidemiological studies
provide evidence that susceptibility to UV radia-
tion is greater at younger ages (mainly in child-
hood and adolescence) than at older ages (see
page 8; Autier & Dare 1998; Whiteman et at.,
2001). Hence, data analysis should identify
whether exposure to tanning appliances starting at
younger ages was more strongly associated with
melanoma than exposure starting at older ages.
The UV emission spectrum of UV lamps in
indoor tanning appliances has changed over
time: before 1980, many UV lamps produced
large amounts of UVC and UVB, whereas most
UV tanning appliances used after 1985 mainly
emitted in the UVA range (see page 3).
34
18
6
5
Summary relative
P-value X
2
risk (95% Cl)
Heterogeneity
1.15 (1.00-1.32) 0.007
1.14 (1.00-1.30)
0.045
1.11 (0.97-1.26) 0.019
1.64 (1.22-2.20)
0.743
1.65 (1.17-2.32) 0.709
(a) Case-control studies: Case-control studies of
melanoma providing results on use of indoor tan-
ning facilities have been of variable study design,
and many of them only included one question on
exposure to tanning appliances. Some positive or
negative associations between exposure to tan-
ning appliances and risk for melanoma may have
been due to statistical fluctuations (i.e. alpha or
beta errors) or to design effects.
In some studies, melanoma patients (i.e.
cases) were derived from a small number of der-
matologic clinics, and subjects without melanoma
(i.e. controls) were derived from hospital wards or
outpatient clinics. This way of selecting cases and
controls is prone to many biases: for instance,
control subjects could suffer from a disease asso-
ciated with higher or lower propensity to engage
in indoor or outdoor tanning.
Users of indoor tanning facilities have been
shown to have a greater-than-average propensity
to engage in intentional sun exposure (Autier et
a/., 1991 ), and may have characteristics of
inherited sun sensitivity different from the rest of
the population (see page 9). Hence, a possible
association between exposure to tanning
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
Figure 5. Investigation by Funnel plot representation of a possible publication bias in the
studies of risk for melanoma associated with use of indoor tanning facilitites included in the
meta-analysis
0
....
0
0.1
E
.. !
.c:
-
., 'i:
*
ca
0)
0.2
0
....
0
'-
t
0
0.3
'-
'-
i
Q)
"C
'-
ca
"C
0.4
r:::
ca
-
(,/)
0.5
-0.5 0 0.5 1 1.5
Logarithm of RR
Figure 6. Investigation by Funnel plot representation of a possible publication bias in the
studies of risk for melanoma associated with first use of indoor tanning facilities in youth
....
0
0
0.2
-
'i:
"'
0)
0
-
0 0.4
s..
e
'-
Q)
0.6
"C
r:::
(,/)
0.8 +------......-------,--------,
0 0.5 1 1.5
Logarithm of RR
35
Exposure to Artificial UV Radiation and Skin Cancer
appliances and risk for melanoma could in fact be
due to greater sun exposure than average, or to
greater use of indoor tanning facilities by subjects
naturally more prone to melanoma. To reduce the
effect of these confounding factors on risk
estimates, it was necessary to adopt statistical
methods (e.g. a multivariate logistic regression
model) allowing the calculation of estimated risks
adjusted for both sun exposure history and host
characteristics.
In order to examine the consistency of the
data on exposure to tanning appliances and risk
for melanoma provided by case-control studies,
we selected those studies among the 19 studies
included in the meta-analysis (see Tables 7 and
8) that had a section specifically exploring
exposure to tanning appliances and results
adjusted for (intermittent) sun exposure and
sun sensitivity (Autier eta/., 1994; Westerdahl et
a/., 1994; Chen et a/., 1998; Westerdahl et a/.,
2000).
Table 15 presents adjusted relative risks for
melanoma associated with exposure to tanning
appliances, showing some statistically significant
dose-effect relationship for two studies (Autier et
a/. , 1994; Westerdahl et a/., 1994), a borderline
statistically significant dose-effect relationship in
one study (Chen eta/., 1998), and one study with
a non-significant dose-effect relationship
(Westerdahl eta/., 2000).
Two of the four studies (Autier et a/. , 1994;
Chen et al. , 1998) showed that the highest risk
for melanoma was associated with exposure to
tanning appliances more distant in time (Table
1 0). Three studies (Westerdahl eta/., 1994; Chen
eta/., 1998; Westerdahl et al., 2000) showed that
melanoma risk was highest when exposure to
tanning appliances started at younger ages, i.e.
before approximately 35 years old (Table 9).
However, most associations with exposure dis-
tant in time and with younger age at start did not
reach statistical significance because of the low
number of subjects in the relevant categories of
exposure. Statistical significance first emerged
when all data were combined in a meta-analysis,
resulting in a greater number of subjects in
relevant categories of exposure and thus higher
statistical power (see page 30).
36
(b) Prospective study: The Norwegian-Swedish
study (Veiemd eta/., 2003) is the only published
prospective cohort study of environmental risk
factors for melanoma. Women in Norway and
Sweden (N=106 379) were followed for an average
of 8.1 years from 1991 until 1999. The study
showed consistent associations between host
characteristics of inherited sun susceptibility,
sunburn history, sun exposure, exposure to tan-
ning appliances and cutaneous melanoma.
During follow-up, 187 cases of melanoma were
diagnosed. After adjustment for intermittent sun
exposure and host characteristics, the adjusted
relative risk for melanoma was 1.55 (CI ,
1 .04-2.32) among the 18% of women aged
1 0-39 years who reported having used sun beds
at least once a month when they were 10-19,
20-29 or 30-39 years old. Twelve sunbed
sessions per year correspond to the typical tan-
ning programme proposed by many commercial
tanning facilities. Thus the 55% increase in
melanoma risk was related to 40 hours or more
of exposure to tanning appliances, assuming an
average of 20 minutes per session. In that
respect, the levels of exposure to tanning
appliances reported in this prospective study
were more comparable with levels reported in
surveys carried out in European countries than
those reported in case-control studies.
In the Scandinavian countries, use of indoor
tanning facilities has been popular since the late
1970s, and the prevalence of use of indoor tanning
facilities in those countries is the highest in the
world. In the Norwegian-Swedish prospective
study, the highest risk for melanoma was found in
women who used indoor tanning faci lities at least
once per month when they were 20 to 29 years old
(RR, 2.58; Cl, 1.48-4.50), and the lowest risks
were found for exposure to tanning appliances at
least once a month during the third (RR, 1.42; Cl,
0.93-2.16) or the fourth decade of life (RR, 1.67;
Cl, 0.93-2.99). These results support the hypo-
thesis by which a latency period is needed before
the impact of exposure to tanning appliances on
melanoma incidence becomes apparent. It also
underlines the greater vulnerability of younger sub-
jects to harmful effects of sunbeds.
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
Table 15. Duration of exposure to indoor tanning facilities and risk for melanoma in selected
case-control studies
1
Reference Duration of Cases Controls Estimated 95% Cl
Place & years of study exposure risk
Numbers of cases/control
Autier et a!. ( 1 994) Never used 310 327 1.00 Ref.
Belgium, France, Germany, Exposure starts < 10 hours 36 45 0.75 0.46-1.25
1991- 92 1980 10 hours 19 18 0.99 0.49-2.00
420/447
2
Exposure starts < 10 hours 16 15 1.00 0.47- 2.13
< 1980 10 hours 18 7 2.12 0.84-2.12
Westerdahl eta/. (1994) Never used 282 479 1.0 Ref.
Sweden, 198890 1- 3 sessions/year 44 67 1.1 0.7-1.9
400/640 4-1 0 sessions/year 30 55 1.1 0.7-1.9
> 1 0 sessions/year 41 33 1.8 1.0-3.2
Chen et a/. ( 1998) Never used 483 417 1.00 Ref.
Connecticut, USA, 1987-89 < 10 sunlamp uses 76 50 1.25 0.84-1.84
624/512 1 0 sunlamp uses 63 40 1.15 0.60-2.20
Westerdahl eta!. (2000) Never used 319 538 1.0 Ref.
Sweden, 1995-97 1-125 uses 22 32 2.8 1.0-7.8
571/913 126-250 uses 34 31 3.1 1.3-7.1
> 250 uses 31 37 1.5 0.7-3.2
1
Duration of exposure, relative risk, and 95% confidences as in published reports. All estimated risks are adjusted for
age, sex, natural sun sensitivity and recreational sun exposure.
2
The 21 cases and 35 controls who were exposed to sunlamp or sunbed for non-tanning purposes are not reported in
this Table.
(c) Methodological aspects of case-control and
prospective cohort studies: Case-control studies
are prone to two biases inherent in the design.
First, since data are collected retrospectively
(when cases already know they have a
melanoma}, the associations found could be the
result of recall bias, as melanoma patients might
have been more likely to remember past expo-
sures to artificial UV sources (Walter et al. ,
1990). Second, the selection of controls may
have included subjects more (or less) inclined to
have had more frequent exposure to tanning
appliances than average (selection bias).
Among the four case-control studies selected
in Section (a) of this section, three studies (Autier
et al. , 1994; Westerdahl et al., 1994, 2000) used
measures to control for recall bias. Autier et al.
(1994) focused on recall bias in the training of the
interviewers: neither interviewers nor subjects
were informed of the study's objective.
Westerdahl et al. (1994) used a questionnaire
with many variables and stated that at the time of
the interview (1988 to 1990), the population was
unaware of the relationship between exposure to
artificial UV radiation for tanning purposes and
malignant melanoma. Westerdahl et al. (2000)
used identical procedures of data collection for
cases and controls, and collected information
from melanoma patients shortly after diagnosis.
Selection bias of controls was not likely to
have occurred in any of the four selected
case-control studies: three studies (Westerdahl
eta!., 1994, 2000; Chen eta/., 1998) were based
on population-based melanoma registries and
sampling of control subjects. The study by Autier
et a/. (1994) selected cases from multiple
sources (hospital, clinics and melanoma regis-
tries), and controls were chosen in the neigh-
bourhood of cases according to rigorous contact
procedures (Grimes & Schulz, 2005).
The prospective cohort study assessed
exposure to tanning appliances retrospectively
37
Exposure to Artificial UV Radiation and Skin Cancer
but before diagnosis of melanoma. Thus, this
study was less prone to interview and selection
biases at the inception of the cohort.
Taken together, the four case-control studies
selected and the prospective study offer the con-
clusion that the increased melanoma risk was
associated with exposure to tanning appliances
(mainly when exposure started before the age of
approximately 35 years) and the observed positive
associations are not entirely due to recall or selec-
tion biases.
(d) Type of artificial UV light: Only one study
(Chen et al., 1998) collected information con-
cerning the type of appliance used by showing
subjects pictures of various types of indoor
tanning appliances (e.g. desktop models, floor
models, beds, walk-in booths). The study found a
non-significant elevated risk for melanoma asso-
ciated with the use of desktop sunlamps and
heavyweight floor-model sunbeds and a statisti-
cally significant tripled risk associated with use of
more than two types of sunlamps, compared with
no use of sunlamps.
Before 1980, exposure to artificial UV radia-
tion was more likely to take place at home with
appliances that emitted large amounts of UVB
radiation, whereas exposure in the 1980s
increasingly occurred in commercial salons using
appliances that emitted mainly UVA. The
prospective study provided evidence that the
increased melanoma risk associated with expo-
sure to tanning appliances was not due to the
type of UV lamps used before 1983 (Veiemd et
a/., 2004).
Basal cell and squamous cell carcinomas
Description of studies
Nine case-control studies have addressed the
possible association of artificial UV exposure with
either BCC or SCC of the skin. All studies reported
a risk estimate, except one (Boyd et al., 2002),
which was therefore excluded. A further three
studies that did not distinguish between these
two major types of skin cancer (O'Loughlin et al.,
1985; Herity eta!., 1989; Hogan eta!., 1991) were
also excluded from review because BCCs and
sees have different aetiologies, thus leaving five
studies under consideration (Table 16).
Aubry & MacGibbon (1985): The earliest
case-control study that addressed the possible
Table 16. Characteristics of case-control studies included in the meta-analysis on non-
melanoma skin cancers
Reference Country Number of
cases
Aubry & McGibbon Canada sec: 92
(1985)
Bajdik eta/. (1996) Canada BCC: 226
SCC: 180
Corona eta/. (2001) Italy BCC: 166
Karagas et af. (2002) USA BCC: 601
SCC:292
Walther et af. (2004) Germany BCC: 213
BCC, basal cell carcinoma; SCC, squamous cell carcinoma
38
Number of
controls
174
404
158
539
411
Cases
Hospital
Cancer
registry
Hospital
Source
Controls
Hospital
Population, health
insurance
Hospital
Dermatology Population, Dept.
department of Transportation,
Medicare
Hospital Hospital
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
association of artificial UV exposure and
squamous cell carcinoma was conducted in
Montreal, Canada. Its overall aim was to assess
risk factors for sec of the skin with a particular
focus on potential carcinogenic occupational expo-
sures. Eligible cases were histologically diagnosed
with primary invasive cutaneous sec in 1977-78
in 12 hospitals in the Montreal region; 2 controls
per case with no known history of skin cancer,
matched for sex, age and hospital of case diagno-
sis, were selected from those diagnosed in the
same period with specified dermatologic
conditions. Data on standard risk factors for skin
cancer were collected including skin type, occu-
pational and nonoccupational sun exposure as
well as ever-use of long- and round-tube sun-
lamps. The final study population, aged 65 years
on average, comprised 30% of all eligible
patients. There were 92 SCC cases, 4 of whom
reported any exposure to a long-tube sunlamp,
and 17 4 dermatological controls, one of whom
was so exposed, giving an odds ratio of 13.4 after
adjusting for age, sex, eye and hair colour, eth-
nicity, and nonoccupational sun exposure (p <
0.008). (Round-tube sunlamp results were not
reported.) [This study was conducted almost 30
years ago among elderly people; the Working
Group noted major drawbacks, including a hospital-
based study population, controls with skin conditions
and a very low response rate. The risk estimates
were based on a single exposed control, and no
details of artificial UV exposure were obtained.]
Bajdik et a/. (1996): Another study carried out in
Canada that aimed to assess phenotypic, solar
and non-solar risk factors for BCC and SCC of
the skin in men in the province of Alberta also
asked about exposure to non-solar UV light.
Cases were men with a first BCC or SCC histo-
logically diagnosed in 1983-84 and ascertained
through the Alberta Cancer Registry. Controls
were matched for age within 2 years from the
Alberta health insurance plan subscriber list.
Through personal interviews, information about
non-solar UV exposure such as exposure to weld-
ing torches, UV lights and sunlamps was
obtained, as well as standard risk factors. Results
were based on 226 BCC cases (72% of those
ascertained) , 180 sec cases (80%), and 406
eligible controls (71 %). Ever-use of a sunlamp
was reported by 8% of controls (33 of 404) and
9% of BCC cases (23 of 226), giving an odds
ratio of 1.2 (CI , 0.7-2.2); ever-use was reported
by 10% of sec cases (18 of 180), with odds ratio
of 1.4 (CI, 0.7-2.7). Risk estimates were adjusted
for age, skin and hair colour, ethnicity and lifetime
occupational sun exposure. [While this study was
population-based, it was conducted 20 years
ago, was restricted to men of unreported but likely
older ages, and no details of artificial UV expo-
sure were available.]
Corona eta/. (2001): A more recently conducted
hospital-based case-control study of causes of
BCC in Italy assessed non-solar factors as well
as phenotypic and solar factors. Cases of histo-
logically-confirmed BCCs diagnosed in
1995-1997 were ascertained on random days of
the week through a hospital for skin diseases in
Rome. Controls diagnosed with minor skin disor-
ders (e.g. warts, naevi) were drawn from the
same hospital but excluded if they had a history
of skin cancer or UV therapy. Questionnaire data
collected face-to-face included artificial UV expo-
sure as well as standard risk factors regarding
phenotype and patterns of sun exposure. Ever-
use of a sunbed or sunlamp was reported by 20%
of controls (31 of 158) and 11% of BCC cases
(17 of 166). After adjustment for age, sex, family
history of skin cancer, outdoor work and beach
exposure in youth, the relative risk estimate for
BCC was 0.6 (CI, 0.3-1 .2). [This study, carried out
1 0 years ago, had major shortcomings through its
design, namely a convenience sampling frame of
adult dermatologic patients. No details of expo-
sure to tanning appliances were obtained.]
Karagas eta/. (2002): A case-control study con-
ducted in the USA among New Hampshire resi-
dents assessed risk for BCC and SCC in relation
to exposure to artificial UV tanning appliances,
among other factors. Cases of skin cancer diag-
nosed in 1993-1995 were ascertained through a
network of dermatologists and pathology labora-
tories. Controls were a frequency-matched
sample of residents drawn from the Department
of Transportation listing (< 65 yrs) or Medicare
program list (> 65 yrs). Sunlamp/tanning bed use
39
Exposure to Artificial UV Radiation and Skin Cancer
and age at first and last use as well as standard
skin-cancer risk factor data were obtained
through personal interviews. The study popula-
tion comprised 603 sec cases and 293 sec
cases (78% of those eligible) and 540 (60%) eli-
gible controls. Fourteen percent of controls (75 of
539), 21% (127 of 601) of BCC cases and 22%
(63 of 229) of sec cases reported any exposure
to tanning appliances. After adjustment for age,
sex and sun sensitivity, risk estimates associated
with ever-use of a sunlamp in relation to BCC
were 1.5 (CI, 1.1-2.1) and to SCC, 2.5 (1.7-3.8),
and were similar in men and women. There was
a non-significant trend toward increased risk with
younger age at first use for SCC. Risks were
increased for both BCC (OR, 1.6; Cl, 1.1- 2.3)
and SCC (OR, 2.9; Cl, 1.8-4.7) for first use more
than 20 years previous to enrolment (before
1975). [The strengths of this study conducted 10
years ago were its population-based design and
its availability of some quantitative data regarding
sunlamp use. It lacked power to explore the asso-
ciations with age at first use versus years since
first exposure, and no data were available about
frequency of use.]
Walther et a/. (2004): The most recently pub-
lished study of the association of artificial UV
radiation and BCC was conducted in Germany,
based on 213 patients with sec diagnosed in the
previous 5 years and 411 controls from the same
dermatology department as the cases or the gen-
eral surgery department of the same hospitals.
During an interview patients were asked about
number of times a year they used indoor tanning
faci lities. On crude analysis there was no associa-
tion between recent history of BCC and use of
indoor tanning facilities more than 5 times a year
(OR, 0.7; Cl , 0.3-1 .5).
Meta-analysis
The meta-analysis was based on the five studies
reporting type-specific risk estimates (Table 17).
Chi-squared test and random effect models were
used to assess heterogeneity, as described on
page 26. Pooled relative risks suggested a signifi-
cant effect of exposure to indoor tanning facilities
for SCC, but not for BCC (Table 18).
40
The effect estimate seen for BCC was not
much influenced by the estimate reported by
Corona et a/. (2001 ), which indicated a protective
effect of artificial UV radiation for BCC (the weight
of this study was the lowest [w = 8.0]). As above,
this study was not specifically designed to investi-
gate exposure to artificial UV radiation, thus radia-
tion exposure data were not detailed. Excluding
this publication from the analysis changed the
pooled relative risk for BCC, although not substan-
tially (pooled RR, 1.39; Cl , 0.14-13.51).
Regarding SCC as an outcome, the study by
Aubry & MacGibbon (1985) reported findings for
only one type of sunlamp (long-tube type) and
was hospital-based. The weight of this study was
the lowest of this group (w=0.74); nevertheless,
the pooled relative risk for sec excluding this
study was neither stronger not more significant
(pooled RR, 2.16; Cl , 0.24- 19.53).
Funnel plot regression gave indication of no
publication bias (P=0.77 and 0.26 for BCC and
sec, respectively) but results based on so few
estimates are not reliable.
The study by Karagas et a/. (2002) gave the
most detai led results and the trends were
consistent with the results reported for
melanoma. The weight of this study was the high-
est (w = 23.8 for SCC and w = 36.8 for BCC) and
therefore its results were the most influential.
Quality of studies
Only one case-control study (Karagas et a/.,
2002) had a section designed specifically to
explore sunlamp/sunbed use in more detai l than
never/ever use. Results were adjusted for sun
sensitivity but not for sun exposure since adjust-
ment for sun exposure did not change the risk
estimates. Study participants who reported using
sunlamps or sunbeds were more likely to be
women, to be aged under 50 years, to have
sun-sensitive skin, more painful sunburns and a
history of frequent sunbathing (> 4 times per year)
than non-users. Based on age at first use, the rela-
tive risks for BCC and SCC were found to
increase by 10% (OR, 1.1; Cl , 0.9-1 .5) and 20%
(OR, 1.2; Cl, 0.9-1.6) respectively, for each decade
younger the person was at first use of an indoor
tanning facility. The effects of age at first use could
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
Table 17. Estimates included in the evaluation of an association of ever use of indoor
tanning facilities and risk for non-melanoma skin cancers
Reference Exposure Diagnosis
Aubry & McGibbon Long-tube sunlamp SCC
(1985) use
Bajdik et a/. (1996) Ever use of sun- BCC
lamps sec
Corona et a/.
(2001) Sun bed or sun- BCC
lamp use
Karagas et a/. Any tanning device BCC
(2002) use sec
Walther et a/. Exposure <! 5 BCC
(2004) times/year to artifi-
cial UV radiation/-
UV sunbeds
BCC, basal cell carcinoma; SCC, squamous cell carcinoma
not be distinguished from years since first use
because of the relatively small number of cases in
the study, and there were no semi-quantitative
measurements of artificial UV exposure (e.g. num-
ber of sessions per month, duration of use).
Other sources of exposure to artificial UV
radiation
Medical Use
Light treatment has been used for a large number
of medical conditions (see page 4), most
particularly for psoriasis.
(a) PUVA therapy in psoriasis patients: Most
long-term studies looking at risk for skin cancer
resulting from exposure to UV treatment collected
data from a significant number of psoriasis
patients treated with PUVA (see page 4 (b)).
Relative risk
(95% Cl)
13.4 (1.4-130.5)
1.2 (0.7-2.2)
1.4 (0.7-2.7)
0.6 (0.3-1.2)
1.5 (1.1-2.1)
2.5 (1.7-3.8)
0.7 (0.3-1.5)
Adjustment
Age, sex, eye and
hair colour, ethnicity,
non-occupational
sun exposure
Age, ethnic origin,
skin and hair
colour, occupational
sun exposure
Age, sex, pigmen-
tary traits, family
history skin cancer,
outdoor work, num-
ber of weeks spent
at beach before age
20 years
Age, sex, sun
sensitivity
Crude
There is clear evidence that PUVA increases the
risk for sec with a relatively short latency period,
although it is difficult to distinguish the contribu-
tion of PUVA from other factors, given that treated
patients have usually received multiple
carcinogenic treatments. For example, SCC in
psoriatic patients treated with PUVA commonly
have UV signature mutations rather than PUVA
signature mutations (Kreimer-Erlacher et a/.,
2003), suggesting that PUVA may act as a
promoter rather than an initiator.
Two large cohorts of psoriasis patients have
been followed up since the 1970s: one of 4799
patients in Sweden (Lindelof et a/., 1999) and
another of 1380 patients in the USA (Stern,
2001 ). In the Swedish cohort the relative risk for
sec was 5.6 in men (CI , 4.4-7.1) and 3.6 in
women (CI, 2.1-5.8). In the cohort in the USA,
one fourth of patients who received more than
2000 J/cm
2
developed an SCC (Stern & Laird,
41
Exposure to Artificial UV Radiation and Skin Cancer
Table 18. Meta-analysis of studies of exposure to artificial UV radiation and risk for non-
melanoma skin cancers
Diagnosis Number of
studies
Summary relative risk
(95% Cl)
P-value X
2
Heterogeneity
sec
BCC
3
4
2.25 (1.08-4.70)
1.03 (0.56-1.90)
BCC, basal cell carcinoma; sec, squamous cell carcinoma
1994). The same authors subsequently carried
out a meta-analysis of their own data and all pub-
lished studies with more than 150 patients (Stern
& Lunder, 1998), and found that patients exposed
to high doses of PUVA (more than 200 treat-
ments or more than 2000 J/cm
2
) had a 14-fold
higher risk for sec than those with <1 00 treat-
ments or <1 000 J/cm
2
exposure. The risk is
further increased when the patients have also
received methotrexate at some time (Stern &
Laird, 1994) and is greater still with the use of
cyclosporine (Marcil & Stern, 2001 ). There is no
evidence to date that bath PUVA increases the
risk for SCC (Hannuksela-Svahn eta!., 1999) but
the data available relate to only 944 patients who
received relatively low total PUVA doses.
The risk for melanoma after PUVA treatment
is more controversial. In the cohort in the USA,
discussed above, an increased risk for melanoma
has been reported (Stern, 2001 ). Of the 822 par-
ticipants with long-term follow-up, 44% had at
least 200 PUVA treatments and therefore are
called high exposure patients. Sixteen of the
1380 patients developed an invasive melanoma
and 6 developed a melanoma in situ. The authors
reported a 1 0-fold increase in the incidence of
invasive melanoma compared with population
rates in the 27 months prior to publication of the
article. Within the cohort, the risk for melanoma
was greater in those with fair skin (Fitzpatrick skin
type) and those who received high doses of
PUVA (incidence rate ratio, 2.6; Cl, 1.0-.6) for
more than 200 treatments compared with less
than 200. The risk also appeared to have a long
latency in that an elevation in risk appeared only
after 15 years. There did not appear to be any
increased risk in patients who were also treated
with ionizing radiation or methotrexate.
The Swedish cohort (Lindelof et al., 1999)
42
0.10
0.06
reported no increased risk for melanoma. This
study was much larger than the study in the USA
and the patients were tracked using the Swedish
Cancer Registry, thereby allowing "complete"
follow-up. Of the 2343 men in the cohort, 8
developed a melanoma compared with the 7.3
expected, and of the 2456 women, 7 developed a
melanoma compared with the 6.3 expected. The
length of follow-up was impressive in this cohort,
as the average length was 16 years and 1 038
patients had been followed for more than 19 years.
Given the considerable size and the duration
of follow-up of the Swedish cohort, the findings
from this cohort are the more persuasive of the
two studies. The difference in findings, however,
remains unexplained. In the Swedish cohort a
proportion of patients had had bath PUVA, which
tends to be associated with lower UVA doses.
There were differences in the treatment protocols
as well (Honigsmann, 2001 ), in that in Europe
schedules are individualized after light testing,
more commonly resulting in reduced time to
clearing and lower doses per treatment course.
These differences may explain the discrepant
risk estimates, but it cannot be excluded that the
data from the study in the USA are subject to
bias, not least because follow-up was substan-
tially incomplete.
Overall, there is a postive association
between PUVA and risk for SCC and there
appears to be a dose-response effect. The risk
was greater for fair-skinned people. The risk for
melanoma is much less clear, even in
fair-skinned populations. The positive dose-
response relationship in the study in the USA
supports the interpretation that the association is
causal. It seems likely, however, that the risk is
associated with high doses of PUVA, is relatively
small and is observed after a long latency.
Epidemiological data on exposure to artificial UV radiation for cosmetic purposes and skin cancers
The data from PUVA studies are important in
that they include large numbers of people who
were studied prospectively. They cannot however
be extrapolated to exposure to tanning appli-
ances because of the presence of psoralen.
Furthermore, the total UV dose received by
psoriasis patients is considerably less than that
received by long-term users of indoor tanning
facilities.
(b) Broadband and narrow-band UVB in psoriasis
patients: The evidence relating to long-term risk
for skin cancer after UVB therapy is scanty. In the
PUVA cohort study from the United States, there
was no discernible additional effect of exposure
to UVB (Stern & Laird, 1994}. In a study of psori-
atics treated with coal tar and UVB in the 1950s
followed up for 25 years, there was no demon-
strable increased risk for skin cancer, though the
numbers treated were relatively small (n = 280)
(Pittelkow et a/., 1981 ). In a small study of 195
German psoriatics treated with broadband
(n = 69) or narrow-band UVB (n =126) from 1994
to 2000 only one skin cancer had occurred by
2004. This was an in-situ melanoma which devel-
oped in the same year that narrow-band UVB
therapy was begun (Weischer et a!., 2004}.
Though these data are reassuring they cannot
exclude a small increased risk nor a large
increased risk in patients treated with high doses.
(c) UV treatment of other skin diseases: The
immunomodulatory effects of UV radiation are
utilized in the treatment of a variety of skin dis-
eases other than psoriasis. Many of the patients
treated are at increased risk for skin cancer even
without PUVA because of the nature of their
dermatosis (e.g. viti ligo). Others are at further
increased risk because of immunosuppression
which may both characterize the skin disease
and its treatment, such as graft versus host
disease (GVHD) (Furlong eta/., 2002) or cuta-
neous T-cell lymphoma.
A series of 1 03 patients with steroid-resistant
GVHD treated with PUVA received a mean dose
of 41 J/cm
2
between 1994 and 2000. Only one
sec has developed in this cohort to date
(Furlong eta!., 2002).
PUVA is also very useful, although not cura-
tive, in the treatment of cutaneous T cell lym-
phoma (CTCL) when it is commonly used as part
of multi-modality treatment programmes with
other drugs contributing to risk such as cytotoxi-
cs (McGinnis et at., 2003). Narrow-band UVB has
been reported to be as effective as PUVA in the
treatment of early CTCL in one retrospective
study (Diederen et at., 2003). There is no doubt
that in this patient population there was an
increased risk for sec but it is difficult to appor-
tion risk to PUVA. The risk for melanoma was
reported in a very small series of patients and
therefore cannot be assessed (McGi nnis et a/.,
2003).
Lighting
(a) Fluorescent tubes: Household lights emit
significant amounts of UV radiation (Sayre eta/.,
2004) and several case-control studies have
addressed risk for melanoma associated with
such exposure. The earl iest study suggested an
elevated risk associated with exposure to fluores-
cent lights at work (Beral et at., 1982) but alt sub-
sequent studies failed to identify such a risk
(Rigel et at., 1983; Osterlind et a/., 1988; Walter
et at., 1992; Holly eta/., 1995).
(b) Full spectrum lamps: No data were available
to the Working Group regarding exposure to full-
spectrum lamps intended for domestic and public
use and risk for skin cancer.
43
Exposure to Artificial UV Light and Skin Cancer
Effects of artificial UV radiation not relevant to skin carcinogenesis
Cutaneous diseases
Skin ageing
Skin ageing is a phenomenon comprising intrin-
sic processes that are largely genetically deter-
mined and extrinsic ageing (or photo-ageing) that
is largely related to sun exposure (Jenkins,
2002) . Both UVB (Del Bino eta/., 2004) and UVA
(Marrot eta/. , 2004) are held to be mediators of
these effects. Intrinsic ageing is characterized by
thinning of the skin accompanied by reduction in
collagen levels. These changes are thought to
result at least in part from diminished cellular pro-
liferative activity in the skin (inevitable cellular
senescence) and from increased expression of
enzymes that degrade the collagen, such as the
metallo-proteinases (Jenkins, 2002). The process
is undoubtedly complex, and one of the drives to
cellular senescence may be chronic exposure to
oxidative stress.
The changes resulting from sun exposure
that are perceived as ageing are loss of elastici-
ty, pigmentary change and deep wrinkling
(Leyden, 1990). Most of these changes result
from damage to the dermis, which is visible his-
tologically as elastotic material. This material is
comprised of degenerate elastic fibres and newly
synthesized dysfunctional elastotic material.
Similarly there appears to be a reduced amount
of collagen I in the dermis and increased
amounts of degenerate collagen. The metallo-
proteinases mediate this degradation, at least in
part, and their activity appears to be increased
both by age and by sun exposure. Increased age
is associated with a diminished ability to repair
damage induced by exposure to UV radiation
(Takahashi et at., 2005).
Comparatively few epidemiological studies
have addressed photo-ageing of the skin, not
least because of the difficulties of measuring it
accurately. Some authors have suggested that
ultrasound measurement is of value (Gniadecka
& Jemec, 1998); others have used silicone
(Green, 1991; Fritschi et a/., 1995) to create
44
moulds to allow an estimate of the topography of
the skin, a method which appears to be better
evaluated. A large study performed in
Queensland, Australia demonstrated premature
ageing of the skin in a population excessively
exposed to the sun (Green, 1991 ). This was more
marked in men who reported outdoor work or
leisure, and especially those with fair skin. The
presence of photo-ageing was correlated with
skin cancer. The relationship between non-
melanoma skin cancer and solar keratoses is
held to be clear and straightforward (Green et at.,
1999). Experimental studies on UV exposure and
photo-ageing have been reviewed (IARC, 1992).
Very few studies have investigated the rela-
tionship of artificial UV exposure to ageing in
humans. Lentigos similar to PUVA freckles have
been reported to be induced by exposure to tan-
ning appliances (Roth et at., 1989; Kadunce et
at. , 1990), which is of concern given the evidence
that the risk for skin cancer is increased in PUVA
patients. A number of case reports have
described an extreme form of cutaneous ageing
which resulted from very frequent exposure to
tanning appliances in fair-skinned people (Poh-
Fitzpatrick & Ellis, 1989). There have been no
informative epidemiological studies of the role of
indoor tanning facilities in the induction of photo-
ageing.
There is some evidence that cigarette smoke
exacerbates photo-ageing of the skin (IARC,
2004; Placzek eta/., 2004).
Other skin diseases caused or exacerbated
by exposure to UV radiation
A wide variety of dermatoses are exacerbated by
sun exposure, such as atopic eczema or psoria-
sis if sunburn occurs. Some skin diseases are
directly provoked by sun exposure, the most
common of which is polymorphic light eruption,
which is common in women. It has been reported
in around 20% of healthy women (Millard et at.,
Effects of artificial UV radiation not relevant to skin carcinogenesis
2000). Variants occur, such as a blistering erup-
tion seen on the ears in childhood or actinic
prurigo, where itchy papules and nodules devel-
op after sun exposure. Such photodermatoses
are a nuisance but otherwise relatively trivial
problem. Exposure to tanning appliances may
precipitate such dermatoses (O'Toole & Barnes,
1995). Medical use of artificial UV radiation may
be used to control polymorphic light eruption if
used carefully as a means of desensitization.
Photosensitivity is usual in patients with
lupus even in the absence of a history of a sun-
evoked eruption (Sanders eta/., 2003), and light
testing reveals that the majority of patients react
to both UVA and UVB (Sanders eta/., 2003). The
cutaneous manifestations of lupus are also com-
monly precipitated by exposure to the sun. Photo-
testing with artificial UV radiation sources has
been reported to provoke cutaneous lupus
(Marguery et a/., 2005), and therefore it seems
likely that it may also be provoked by other
sources of artificial radiation such as tanning
appliances.
More significant photodermatoses occur
more rarely, such as chronic actinic dermatosis,
in which persistent sun-induced eczema occurs.
It is a rare condition, usually seen in elderly men.
It may develop from an allergic dermatitis for
example to pollen or fragrances.
Much more significant are the porphyrias in
which sun exposure may trigger photosensitivity.
The varieties that induce photosensitivity are
variegate porphyria (Mustajoki, 1980) (most
common in South Africans of Dutch descent),
erythropoietic porphyria (Goerz, 1979) and
porphyria cutanea tarda (PCT) . PCT is the most
common and in 80% of cases occurs because of
exposure to estrogens or alcohol. Use of indoor
tanning facilities or other artificial UV sources -
even fluorescent lights - by patients with latent
porphyria is potentially very serious as a result of
the possible induction of sunburn.
The overall dose of UVB and UVA incurred
by most people using bright light therapy is likely
to be considerably less than that received by pso-
riasis patients treated with PUVA. Exposure is
also likely to be limited to the face. It seems likely
therefore that the theoretical risk will relate to
non-melanoma skin cancer rather than
melanoma, but there are no relevant data from
epidemiological studies at present to inform. It
would seem very reasonable however to con-
clude that lamps emitting low levels of UVA would
be preferred to those emitting higher levels.
Case reports also suggest that use of indoor
tanning facilities is associated with development
of drug-induced photodermatoses and exacerba-
tion of lupus erythematosus (Spencer &
Amonette, 1995).
Drug-induced photosensitivity
A variety of commonly used drugs increase cuta-
neous sensitivity to the sun and to artificial UV
sources, and are predicted therefore to increase
the risk for skin cancer. Most drugs have a pho-
totoxic effect rather than a photo-allergenic one
(Moore, 2002). Oral photosensitisers include
tetracyclines, amioderone, diuretics, non-steroidal
anti-inflammatory drugs (NSAIDs) and chlorpro-
mazine (Moore, 2002). Diuretics, antibiotics and
NSAIDs are very widely used drugs, and their
phototoxic effects therefore have the potential to
affect a significant proportron of the population.
Topical agents include plant-derived photosensi-
tisers (psoralens) such as bergamot, widely used
in perfumed products. Use of perfumes has the
potential to increase the photo-damaging effects
of indoor tanning appliances.
Effects on the eyes
Cataract
Conditions linked to sub-chronic and chronic
exposure to solar uv include pterygium and sec
affecting the cornea; cataract, affecting the ocular
lens; and acute macular degeneration affecting
the retina (Tomany et a/., 2004). Of these,
cataracts of the nuclear and cortical types are the
most widespread and serious UV-related eye
conditions. There is an inverse association
between latitude of residence and cataract sur-
gery in Medicare program data from the USA
(Javitt & Taylor, 1994), and epidemiological studies
conducted in Australia, China, and the USA (see
Taylor, 1994, for review) support a role of UV
exposure in cataract development. Risk for
45
Exposure to Artificial UV Radiation and Skin Cancer
cortical cataract (opacity of the outer lens) is
related to increasing cumulative UVB exposure,
while risk for nuclear cataract (opacity of the cen-
tral lens) has been shown to be significantly
increased with increasing UV exposure in young
adulthood, consistent with the successive laying
down with age of outer lens fibres on the cortical
layer exposed in earlier life (Neale eta/., 2003).
With regard to artificial UVB, there is sufficient
experimental evidence that exposure causes
cortical lens opacity in the eyes of laboratory ani-
mals (IPCS, 1994).
Intraocular melanoma
Early-life exposure to sunlight may be important
in the development of intraocular melanoma
(Tucker eta/., 1985; Seddon eta/., 1990), more
specifically of choroidal melanoma (Moy, 2001 ).
This is consistent with the observation that after
childhood most UV radiation is screened by the
lens (Zigman, 1983; Lerman, 1984).
Welding equipment and tanning appliances
are sources of intense UV radiation. Five out of
eight epidemiologic studies found a significantly
increased risk for ocular melanoma with welding
exposure, with relative risks ranging from 1.9 to
10.9 (Tucker et a/., 1985; Holly et a/., 1990;
Seddon et a/., 1990; Siemiatycki, 1991 ; Ajani et
a/. , 1992; Holly eta/., 1996; Guenel eta/., 2001 );
in contrast , one study conducted in nine
European countries found an increased risk only
in one country (Lutz eta/., 2005) .
Four case-control studies have examined
the risk for intraocular melanoma in relation to
exposure to UV radiation from sunlamps (Table
19). Whi le the earliest study only found a non-sig-
nificant trend in risk according to frequency of
sunlamp use (Tucker eta/., 1985), the three more
recent studies consistently found an increased
relative risk, ranging from 1.7 to 3.6 (Holly eta/.,
1990; Seddon eta/. , 1990; Vajdic eta/., 2004) .
UV exposure and vitamin D
Vitamin D is an essential nutrient, generally
quantified by measuring circulating levels of 25-
hydroxyvitamin D. There are three major sources
46
of vitamin D: photosynthesis in the skin, ingestion
in the diet and oral supplementation. Worldwide,
photosynthesis from sunlight is the most common
source of vitamin D.
Vitamin D formation by photosynthesis
Previtamin D3 is produced from 7-dehydroxycho-
lesterol (provitamin D
3
) by the direct photolytic
action of UVB. The precursor, 7-dehydroxycho-
lesterol, is abundant in human skin although lev-
els decrease with age (Holick et a/., 1989). On
exposure of the skin to sunlight, 7-dehydroxycho-
lesterol in epidermal and dermal cells absorbs
UVB radiation to form previtamin D
3
. Previtamin
D
3
is thermodynamically unstable and is rapidly
transformed by rearrangement of its double
bonds to form vitamin D
3
{here called vitamin D)
before entering the circulation. Vitamin Dis a pro-
hormone that is converted by 25-hydroxylation in
the liver to the intermediate metabolite 25-
hydroxyvitamin D, which is the main ci rculating
and storage form. With physiological demands for
calcium and phosphorus, 25-hydroxyvitamin D
undergoes 1 a-hydroxylation in the kidney to form
the active hormone, 1 ,25-dihyroxyvitamin D.
Blood levels of 25-hydroxyvitamin D reflect the
availability of vitamin D (Osborne & Hutchinson,
2002).
Main target organs for 1 ,25-dihydroxyvitamin
D include the intestine, kidney and bone, but
nuclear receptors have been found in over 30 dif-
ferent tissues, reflecting its many other actions
besides parathyroid activity and serum calcium
homeostasis, analogous to those of classical
steroid hormones. 1 ,25-dihydroxyvitamin D is
also an antiproliferative, prodifferentiation and
proapoptotic agent (Osborne & Hutchinson,
2002).
Dietary sources of vitamin 0
There are only a few foods (cod liver oil , oily fish
such as salmon, mackerel and sardines) that are
naturally rich in vitamin D, so in many countries
where oily fish are not widely consumed, food
fortification or vitamin supplements may be needed.
In a global review of vitamin D intake, wide varia-
tions were found in food fortification
practices and contributions from supplement use
Table 19. Case-control studies of exposure to artificial UV radiation and risk for intraocular melanoma
Reference Location, Cases and Controls Age Adjusted Relative Characteristics Comments
Period of (years) Risk Assessed
Recruitment
Tucker era/. Philadelphia, PA, 444 intraocular melanoma NR 1.4 (0.9-2.2); Eye colour, complexion Telephone interview (45 min.); estimates
(1985) USA, January (1 hospital) with cataract: and hair colour, adjusted for history of cataract; sunlight
197 4- June 1979 424 hospital controls with 2.3 (0.9- 5.9) corrective lenses, sun exposure is an important risk factor for
detached retina, matched without cataract: exposure during leisure intraocular melanoma (persons born in the
on age, sex and period of 1.2 (0.7-2.0) time, sun protection, South: RR 2.7 (1.3-5.9). Trend in RR
diagnosis years lived in the South according to frequency of sunlamp use
rising to twofold for frequent use (P=0.10)
Holl y eta/. (1990) 11 Western 407 cases (Ocular 20--74 Exposure to UV or Eye and hair colour, Telephone interview; adjustment on eye
States. USA. Oncology Unit, UCSF); blacklight: naevi, freckles, tendency colour, coffee, effect of 0.5 h exposure to
January 1978-- 870 controls (random digit 3.59 (1.57-8.70) to sunburn, other eye midday summer sun, other UV exposure.
February 1987 dialling in the same Welding burn, conditions, tobacco,
geographic area as the sunburn to eye, coffee. tea. alcohol
patients), snow blindness:
2 age/sex matched 7.17 (2.5-20.57) m
controls per patient
1if
f}
Seddon et a/. New England, 197 cases 17--88 Use of sunlamps: Ancestry from Northern Only choroid and ciliary body melanomas.
a
Ol
(1990) USA 385 matched population 3.4 (1.1-10.3); or Southern latitudes, 2 independent comparisons. Occasional or
3i
(")
controls (random digit with random digit latitude of residence, skin frequent versus never use. ![
dialling) dialled controls colour, naevi
c
<
2.3 (1.2--4.3) with
iil
337 cases; sibling controls
c..
5[
all USA 800 sibling controls
()'
::;)
::;)
Vajdic eta/. (2004) Australia, 290 cases (246 with 19--79 Use of sunlamps: Eye colour, host Population-based prospective recruitment
g_
Cil
1996-1998 melanoma of choroid or 1. 7 (1.0--2.8) characteristics. lifetime of cases (all ophthalmologists and cancer
(i)
ciliary body); Welding: residence, work calendar, registries). Telephone interview. Risk
::!.
893 population controls 1.2 (0.8--1 .7) sun exposure, sun increases with increasing duration of use 0
(electoral rolls) protective wear and is greater for exposures begun before
(/)
:;><"
the age of 21 years and after 1980.
;:;-
(")
Sunlamp use or welding not associated
Ol
n
with iris or conjunctival melanoma.
::;
0
<0
NR, not reported.
<t>
::;)
<t>
en
-...J
c;;
Exposure to Artificial UV Radiation and Skin Cancer
(Calvo et a/., 2005). In Canada and the USA,
where fortification is mandatory for staple foods
such as milk and margarine and optional for other
classes of food, vitamin D intake was generally
2-3 f.!g higher than in either Australia, Ireland,
Scotland or the United Kingdom where fortifica-
tion of staples like margarine and breakfast cere-
als is optional, or European and other countries
where food fortification is restricted. Mean daily
vitamin D intakes were reported to be highest in
young adult Caucasian men and women in North
America (8.1 and 7.3 f.!g/d) due to milk fortifica-
tion and in Japanese women (7.1 f.!g/d) due to
high fish consumption. Norwegian men and
women, who also have high fish consumption,
had higher levels (6.8 and 5.9 mg/d) than their
British counterparts (4.2 and 3.7 f.,lg/d).
Contributions by dietary supplements to mean
daily vitamin D intakes ranged from 49% in
Norwegian women to 12% in British men, and on
average contributions from supplements
increased with age and were more common in
women (Calvo eta/., 2005) .
Vitamin D and exposure to artificial UV radia-
tion for tanning purposes
Available data are inadequate to assess the
effect of exposure to UV in indoor tanning facili-
ties on vitamin D status. Our current understanding
of the photosynthesis of vitamin D in the skin
would suggest that this type of artificial UV expo-
sure would be effective in induction of vitamin D
photosynthesis only to the extent that it contains
UVB, as opposed to UVA radiation. Practically
speaking, the usefulness of these facilities for
correcting vitamin D insufficiency is limited by the
inability of consumers to ascertain the UVB flux
to which they are being exposed in a tanning
session, the expense and inconvenience of these
sessions compared with oral vitamin D supple-
mentation, and the other health consequences of
using these facilities, as outlined in the other
chapters of this document.
The nature of the network of photo- and ther-
moreactions that are involved in vitamin D syn-
thesis in vitro is well established. As measured in
vitro the greatest sensitivity of the conversion of
7-dehydroxycholesterol to previtamin D lies in the
48
UVB part of the solar spectrum, 280-320 nm. It is
therefore similar to the erythema action spec-
trum, except for a sharper downturn in provitamin
D absorptivity in the UVA spectral region from a
maximum at 282 nm (Galkin & Terenetskaya,
1999).
Seasonal and latitude variations in UVB
intensity markedly affect vitamin D synthesis,
with lowest relative production occurring at high lat-
itudes during winter months. Also, ageing
decreases the capacity of skin to produce vitamin
D (Holick et al., 1989). Finally, compared with fair-
skinned people, those with darkly pigmented skin
are less efficient at producing vitamin D and
require 10-50 times the level of sun exposure to
produce the same amount (Clemens et al.,
1982). In addition to season, latitude, ageing, and
skin pigmentation, vitamin D photosynthesis may
be influenced by factors that affect the intensity of
skin exposure to UVB.
For light-skinned adults, a few minutes per
day with the face and hands in bright sunshine is
sufficient to cover daily needs in vitamin D.
Intense UVB exposure may generate little vitamin
D beyond that achieved by more modest expo-
sure because previtamin D and vitamin D can
readily convert to other photoproducts that have
little or no vitamin D action.
Vitamin D and xeroderma pigmentosum patients
A further indication that necessary amounts of
vitamin D may be provided through dietary
sources comes from a study of patients suffering
from xeroderma pigmentosum, a rare disease
associated with a deficiency in UV-induced DNA
lesion repair (Setlow eta/., 1969), and character-
ized by extreme sensitivity to sunlight (Kraemer
et al., 1994). To prevent the development of skin
cancers at an early age, these patients wear
protective clothing and use sunscreens when
outdoors. A six-year follow-up study of eight
children with xeroderma pigmentosum showed a
normal vitamin D intake and that normal vitamin
D levels can be maintained in ambulatory
patients despite rigorous sun protection (Sollitto
et al., 1997).
Summary and conclusion
Summary
UV radiation wavelengths range between 100 nm
and 400 nm and are broadly categorised into UVA
(>315-400 nm), UVB (>28Q-315 nm) and UVC
(1 OQ-280 nm). The portion of solar UV radiation
that reaches the earth's surface is composed pre-
dominantly of UVA and less than 5% UVB.
The sun is the main source of UV for most
individuals. Sources of artificial UV radiation are
used during indoor tanning, for medical appl ica-
tions and in some occupations. Indoor tanning
facilities in general deliver higher relative intensi-
ties and higher proportions of UVA compared
with solar UV radiation, but there are wide varia-
tions.
Several national and international organisa-
tions have presented recommendations regard-
ing the use of indoor tanning facilities, but few
countries regulate access and use.
The few studies that have addressed the bio-
logical changes in the skin induced by indoor
tanning have shown that they are similar to those
induced by sunlight.
Many studies have substantiated the carcino-
genic effects of UV radiation. Experimental stud-
ies in humans have shown that in the basal lay-
ers of the epidermis, where melanocytes are
located, UVA induces more DNA damage than
does UVB.
Both UVA and UVB radiation can affect the
immune system: while UVB induces immunosup-
pression at both the local and systemic levels,
UVA does not induce systemic immune suppres-
sion. Exposure to tanning appliances has also
been shown to induce changes in the skin
immune system, including reduced skin test
responses, changes in lymphocyte populations,
and depression of NK cell activity.
Prevalence of indoor tanning varies greatly
between countries; it is widespread in Northern
Europe and North America, particularly among
women and young people. Indoor tanning has
increased considerably since the early 1980s.
Several studies show common use by adoles-
Exposure to Artificial UV Light and Skin Cancer
cents, and sometimes by children. The most fre-
quent motivations for indoor tanning are the
acquisition of a so-called "safe" tan and skin
preparation before sun exposure. Limited evi-
dence suggests that compliance with recommen-
dations and regulations by indoor tanning facility
operators and customers is poor.
Twenty-three published studies (22
case-control, one cohort) in light-skinned popu-
lations investigated the association between
indoor tanning and risk for melanoma, and 7
case-control studies for keratinocytic skin can-
cers. Characterisation of exposure was highly
variable across reports.
The summary relative risk for ever versus
never use of indoor tanning facilities from the 19
informative studies was 1.15 (1.0Q-1.31 ). When
the analysis was restricted to the nine population-
based case-control studies and the cohort study,
the summary relative risk was 1.17 (0.96-1 .42).
There was no consistent evidence for a
dose-response relationship between indoor tan-
ning exposure and risk for melanoma.
All studies that examined age at first expo-
sure found an increased risk for melanoma when
exposure started before approximately 30 years
of age, with a summary relative risk estimate of
1.75 (1.35-2.26).
Studies on exposure to indoor tanning appli-
ances and squamous cell carcinoma found some
evidence for an increased risk for squamous cell
carcinoma, especially when age at first use was
below 20 years. Studies on basal cell carcinoma
did not support an association with use of indoor
tanning faeilities.
Investigation of the association between
indoor tanning and skin cancers poses challeng-
ing problems, as the fashion of indoor tanning is
still very recent. Associations after long latency
periods, such as may be expected for melanoma
and basal cell carcinoma, may not yet be
detectable.
Artificial UV sources are used to treat a
variety of skin conditions, predominantly psoriasis.
49
Exposure to Artificial UV Radiation and Skin Cancer
Broadband UVB has been used for many years
and, more recently, narrow-band UVB, but there
are few data on which to base estimates of risk
for skin cancer. PUVA therapy increases the risk
for squamous cell carcinoma. Data concerning
the risk for melanoma as a result of PUVA thera-
PY are conflicting, but to date it seems likely that
any increased risk for melanoma is small and that
the latency is in excess of 20 years.
Case reports suggest that use of indoor tan-
ning facilities is associated with the development
of drug-induced photodermatoses and exacerba-
tion of lupus erythematosus.
UV exposure is related to eye damage,
including cataracts, corneal squamous cell carci-
noma and ocular melanoma. Several epidemio-
logical studies have shown an association
between artifiCial UV exposure and ocular
melanoma, especially if exposure occurred in
adolescence or young adulthood.
Sources of vitamin D include photosynthesis
in the skin in response to exposure to UVB radi-
ation, oral intake from consumption of food and
dietary supplements. In cases of insufficiency,
supplementation through oral intake is recom-
mended. Indoor tanning may produce vitamin D
photosynthesis in the skin depending on the
amount of UVB radiation, if any, in their emission
spectrum, although the emission spectrum is
generally unknown to consumers and operators.
Conclusion
The use of indoor tanning facilities is widespread
in Europe and North America, and this impels con-
sideration of the risk for adverse health conse-
quences, particularly melanoma. Consideration is
hampered by the relative recency of widespread
use and the limitations of available studies.
Our systematic review of published studies,
conducted mainly in North America and Europe,
of the association of indoor tanning facility use
with melanoma revealed an association of early
age at first use (less than approximately 30
years) with melanoma risk. These studies consis-
tently indicated a moderate strength of associa-
tion, with a summary relative risk of 1.75
(1 .35-2.26). The association with ever use of
50
these facilities, or use more than 15 to 20 years
prior to diagnosis of melanoma, was weak, and
evidence regarding a dose-response relation-
ship was scanty. The evidence is limited by varia-
tion in characterization of exposure, potential
confounding by sun exposure or other variables,
and the low power to detect associations that
become evident only following a prolonged lag
period after exposure.
The association between indoor tanning facility
use and melanoma risk is consistent with the
knowledge that melanoma is caused by exposure
to solar radiation. Exposure to sunlight in child-
hood has been established as an important
contributing factor for melanoma risk in adults.
Although the contexts of exposure to sun and of
indoor tanning differ, both deliver UV radiation,
and the health effects would therefore be expected
to be similar. The limited evidence for an associ-
ation between indoor tanning and squamous cell
carcinoma is consistent with the known associa-
tion of sun exposure with that cancer. In light of
the known effects of UV radiation on the skin, the
biological plausibility of a causal association
between use of indoor tanning facilities and risk
for melanoma and squamous cell carcinoma is
strong.
On balance, the evidence pertaining to the
strength, consistency, dose-response and tem-
poral sequence of the association of the use of
indoor tanning equipment with melanoma risk,
and of the coherence and biologic plausibility of
the association, leads us to conclude that there is
convincing evidence to support a causal relation-
ship, particularly with exposure before the age of
35 years. This evidence is strongly suggestive
and further studies could clarify our understand-
ing of this association and allow more definitive
conclusions.
We are cognizant of the importance of this
issue for the health of light-skinned populations.
The strength of the existing evidence suggests
that policymakers should consider enacting
measures, such as prohibiting minors and dis-
couraging young adults from using indoor tanning
facilities, to protect the general population from
possible additional risk for melanoma.
References
Adam SA, Sheaves JK, Wright NH, et al. (1981) . A
case-control study of the possible association
between oral contraceptives and malignant
melanoma. Br J Cancer, 44:45-50.
AFSSE (2005) [Ultraviolet radiation - Current
knowledge relating to exposure and health
risks], Report, Maisons-Aifort, France (in
French).
Agar N, Young AR (2005) . Melanogenesis: a photo-
protective response to DNA damage? Mutat
Res, 571 :121-132.
Agar NS, Halliday GM, Barnetson RStC, et al.
(2004). The basal layer in human squamous
tumors harbors more UVA than UVB fingerprint
mutations: A role for UVA in human skin car-
cinogenesis. Proc Natl Acad Sciences USA,
101:4954-4959.
Ajani UA, Seddon JM, Hsieh CC, et al. (1992).
Occupation and risk of uveal melanoma: an
exploratory study. Cancer, 70:2891-2900.
Atillasoy ES, Seykora JT, Soballe PW, et al. (1998).
UVB induces atypical melanocytic lesions and
melanoma in human skin. Am J Pathol,
152:1179-1 186.
Aubry F, MacGibbon B (1985). Risk factors of squa-
mous cell carcinoma of the skin. Cancer,
55:907- 911.
Autier P (2004). Perspectives in melanoma preven-
tion: the case of sunbeds. Eur J Cancer,
40:2367-2376.
Autier P, Dore JF (1998) . 1nfluence of sun exposures
during childhood and during adult hood on
melanoma risk. lnt J Cancer, 77:533-537.
Autier P, Joarlette M, Lejeune F, et al. (1991).
Cutaneous malignant melanoma and exposure
to sunlamps and sunbeds: a descriptive study in
Belgium. Melanoma Res, 1:69-74.
Autier P, Dore JF, Lejeune F, et al. (1 994), for the
EORTC Melanoma Cooperative Group.
Cutaneous malignant melanoma and exposure
to sunlamps or sunbeds: an EORTC multicenter
case-control study in Belgium, France and
Germany. lnt J Cancer, 58:809-813.
Bajdik CD, Gallagher RP, Astrakianakis G, et al.
( 1996) . Non-solar ultraviolet radiation and the
risk of basal and squamous cell skin cancer. Br
J Cancer, 73:1612-1614.
Exposure to Artificial UV Light and Skin Cancer
Banks BA, Silverman RA, Schwartz RH, et al.
(1992). Attitudes of teenagers toward sun expo-
sure and sunscreen use. Pediatrics, 89:40--42.
Bataille V, Winnett A, Sasieni P, et al. (2004).
Exposure to the sun and sun beds and the risk of
cutaneous melanoma in the UK: a case-control
study. Eur J Cancer, 40:29-435.
Bataille V, Boniol M, DeVries E, et al. A multicentre
epidemiological study on sunbed use and cuta-
neous melanoma in Europe. Eur J Cancer 2005,
41 : 2141-2149.
Bech-Thomsen N, Wulf HC, Poulsen T, et al. (1991) .
Photocarcinogenesis in hairless mice induced
by ultraviolet A tanning devices with or without
subsequent solar-simulated ultraviolet irradia-
tion. Photodermatol Photoimmunol Photomed,
8:139-145.
Bech-Thomsen N, Poulsen T, Christensen FG, et al.
(1992). UVA tanning devices interact with solar-
simulated UV radiation in skin tumor develop-
ment in hairless mice. Arch Dermatol Res,
284:353-357.
Beitner H, Norell SE, Ringborg U, et al. (1990).
Malignant melanoma: aetiological importance of
individual pigmentation and sun exposure. Br J
Dermatol, 122:43-51.
Beral V, Evans S, Shaw H, Milton G (1982).
Malignant melanoma and exposure to fluores-
cent lighting at work. Lancet, 2:29Q-293.
Berking C, Takemoto R, Binder RL, et al. (2002).
Photocarcinogenesis in human adult skin grafts.
Carcinogenesis, 23: 181-187.
Black G, Matzinger E, Gange RW (1985). Lack of
photoprotection against UVB-induced erythema
by immediate pigmentation induced by 382 nm
radiation. J Invest Dermatol, 85:448-449.
Bohm M, Wolff I, Scholzen TE, et al. (2005). Alpha-
Melanocyte-stimulating hormone protects from
ultraviolet radiation-induced apoptosis and DNA
damage. J Bioi Chem, 280:5795-5802.
Boldeman C, Beitner H, Jansson B, Nilsson B, Ullen
H (1996) . Sunbed use in elation to phenotype,
erythema, sunscreen use and skin diseases. A
questionnaire survey among Swedish adoles-
cents. BrJ Dermatol, 135:712-716.
Boldeman C, Jansson B, Nilsson B, Ullen H (1997).
Sunbed use in Swedish urban adolescents relat-
ed to behavioral characteristics. Prev Med,
26:114-119.
51
...
Exposure to Artificial UV Radiation and Skin Cancer
Boldeman C, Branstrom R, Dal H, et al. (2001).
Tanning habits and sunburn in a Swedish popu-
lation age 13-50 years. Eur J Cancer,
37:2441-2448.
Boyd AS, Shyr Y, King LE (2002). Basal cell carci-
noma in young women: An evaluation of the
association of tanning bed use and smoking. J
Am Acad Dermatol, 46:706-709.
Brandberg Y, Ullen H, Sjoberg L, Holm LE (1998) .
Sunbathing and sunbed use related to self
image in a randomized sample of Swedish ado-
lescents. Eur J Cancer Prev, 7:321-329.
Brash DE, Ziegler A, Jonason AS, et al. (1996).
Sunlight and sunburn in human skin cancer:
p53, apoptosis, and tumor promotion. J Jnvestig
Derma to/ Symp Proc, 1:136-142.
Bykov VJ, Marcusson JA, Hemminki K (2001 ).
Protective effects of tanning on cutaneous
melanoma. Dermatology, 202:22-26.
Calvo MS, Whiting SJ, Baron CN (2005). Vitamin D
intake: A global perspective of current status. J
Nutr, 135:31 Q-316.
Chen YT, Dubrow R, Zheng T, et al. (1998). Sunlamp
use and the risk of cutaneous malignant
melanoma: a population-based case-control
study in Connecticut, USA. tnt J Epidemiol,
27:758-765.
Clemens TL, Adams JS, Henderson SL, et al.
(1982) . Increased skin pigment reduces the
capacity of skin to synthesise vitamin D
3
.
Lancet, 319:74-76.
Clingan PH, Berneburg M, Petit-Frere C, et al.
(2001). Contrasting effects of an ultraviolet B
and an ultraviolet A tanning lamp on interleukin-
6, tumour necrosis factor-alpha and intercellular
adhesion molecule-1 expression. Br J Oermatol,
Cokkinides VE, Weinstock MA, O'Connell MC, Thun
MJ (2002). Use of indoor tanning sunlamps by
US youths, ages 1118 years, and by their par-
ents or guardian caregivers: prevalence and cor-
relates. Pediatrics, 1 09:1124-1130.
Colditz GA, Burdick E, Mosteller F (1995).
Heterogeneity in meta-analysis of data from epi-
demiologic studies: a commentary. Am J
Epidemiol, 142:371-382.
Commission Internationals de I'Eclairage
52
(International Commission on Illumination)
(1987). Vocabulaire International de I'Eclairage
[International Lighting Vocabulary] (CI E
Publication No. 17.4), 4th ed., Geneva, Bureau
Central de Ia Commission Electrotechnique
lnternationale, p. 3.
Cooper KD, Oberhelman L, Hamilton TA, et al.
( 1992). UV exposure reduces immunization
rates and promotes tolerance to epicutaneous
antigens in humans: relationship to dose, CD1 a
DR+ epidermal macrophage induction, and
Langerhans cell depletion. Proc Nat/ Acad Sci
USA, 89:8497-8501.
Copas JB, Shi JQ (2001). A sensitivity analysis for
publication bias in systematic reviews. Stat
Methods Med Res, 10:251-265.
Corona R, Dogliotti E, D'Errico M, et al. (2001 ). Risk
factors for basal cell carcinoma in a
Mediterranean population. Arch Dermatol,
137:1162-1168.
Culley CA, Mayer JA, Eckhardt L, et al. (2001 ).
Compliance with federal and state legislation by
indoor tanning facilities in San Diego. JAm Acad
Dermatol,
Dahle J, Kvam E (2003). Induction of delayed muta
tions and chromosomal instability in fibroblasts
after UVA, UVB, and X-radiation. Cancer Res,
63:1464-1469.
De Fabo EC, Noonan FP, Fears T, Merlino G (2004).
Ultraviolet B but not ultraviolet A radiation initi
ates melanoma. Cancer Res,
Del Sino S, Vioux C, Rossio-Pasquier P, et al.
(2004). Ultraviolet B induces hyperproliferation
and modification of epidermal differentiation in
normal human skin grafted on to nude mice. Br
J Dermatol,
Dellavalle RP, Parker ER, Cersonsky N, et al.
(2003). Youth access laws: in the dark at the tan-
ning parlor? Arch Dermato/, 139:443-448.
Demko CA, Borawski EA, Dehanne SM, et al.
(2003). Use of indoor tanning facilities by white
adolescents in the United States. Arch Pediatr
Ado/esc Med, 157:854-860.
DeVries E, Boniol M, Severi G, et al. Public aware-
ness about risk factors could pose problems for
case-control studies: the example of sun bed use
and cutaneous melanoma. Eur J Cancer 2005,
in press.
De Winter S, Pavel S (2000). [Tanning beds: effect
on skin cancer risk unclear]. Ned Tijdschr
Geneeskd, 144:467-470 (in Dutch).
Diederen PV, van Weelden H, Sanders CJ, et al.
(2003). Narrowband UVB and psoralen-UVA in
the treatment of early-stage mycosis fungoides:
A retrospective study. J Am Acad Dermatol,
48:215-219.
Diffey BL (1990). Human exposure to ultraviolet
radiation. Semin Dermatol, 9:2-10.
Diffey BL, Langley FC (1986). Evaluation of
Ultraviolet Radiation Hazards in Hospitals
(Report No. 49), London, Institute of Physical
Sciences in Medicine.
Diffey BL, Farr PM, Ferguson J, et al. (1990). Tanning
with ultraviolet A sun beds. Br Med J, 301: 773-774.
Donawho CK, Wolf P, Kripke ML (1994). Enhanced
development of murine melanoma in UV-irradiat-
ed skin : UV dose response, waveband depend-
ence, and relation to inflammation. Melanoma
Res, 4:93-100.
Drobetsky EA, Turcotte J, Chateauneuf A (1995). A
role for ultraviolet A in solar mutagenesis. Proc
Nat/ Acad Sci USA, 92:2350-2354.
Dunn-Lane J, Herity B, Moriarty MJ, Conroy R
(1993). A case control study of malignant
melanoma. lr Med J, 86:57-59 (Erratum in lr
Med J (1993), 86:135).
Ezzedine K, Guinot C, Mauger E, et al. (2005) . Use
of tanning devices: attitudes, beliefs and behav-
iour in 1,179 French adults. EuroSkin workshop,
Lyon, 19-20 May 2005 (meeting abstract).
Fitzpatrick TB (1988). The validity and practicality of
sun-reactive skin types I through VI. Arch
Dermatol, 124:869-871.
Francis SO, Burkhardt DL, Dellavalle RP (2005).
2005: A banner year for new US youth access
tanning restrictions. Arch Dermatol, 141 :524-525.
Fritschi L, Battistutta D, Strutton GM, Green AA
(1995). A non-invasive measure of photoageing.
lnt J Epidemiol, 24: 150-154.
Furlong T, Leisenring W, Storb R, et al. (2002).
Psoralen and ultraviolet A irradiation (PUVA) as
therapy for steroid-resistant cutaneous acute
graft-versus-host disease. Bioi Blood Marrow
Transplant, 8:206-212.
Galkin ON, Terenetskaya IP (1999). Vitamin D bio-
dosimeter: Basic characteristics and potential
applications. J Photochem Photobiol B:Biology,
53:12-19.
Gallagher RP, Elwood JM, Hill GB (1986). Risk fac-
tors for cutaneous malignant melanoma: the
Western Canada Melanoma Study. Recent
Results Cancer Res, 1 02:38-55.
Gange RW, Blackett AD, Matzinger EA, et al. (1985).
Comparative protection efficiency of UVA- and
UVB-induced tans against erythema and forma-
tion of endonuclease-sensitive sites in DNA by
UVB in human skin. J Invest Oermatol,
85:362-364.
Garbe C, Weiss J, Kruger S, et al. (1993). The
German melanoma registry and environmental
risk factors implied. Recent Results Cancer Res,
128:69-89.
References
Geller AC, Colditz GA, Oliveria S, et al. (2002). Use
of sunscreen, sunburning rates, and tanning bed
use among more than 10,000 US children and
adolescents. Pediatrics, 109:1009-1 014.
Gerber B, Mathys P, Moser M, et al. (2002).
Ultraviolet emission spectra of sunbeds.
Photochem Photobiol, 76:664-668.
Gilchrest BA, Eller MS (1999). DNA photodamage
stimulates melanogenesis and other photopro-
tective responses. J Invest Oermatol Symp Proc,
4:35-40.
Gniadecka M, Jemec GB (1998). Quantitative eval-
uation of chronological ageing and photoageing
in vivo: studies on skin echogenicity and thick-
ness. BrJ Oermatol, 139:815-821.
Goerz G (1979). [Erythropoietic protoporphyria].
Fortschr Med, 97:1625-1630 (in German).
Green AC (1991). Premature ageing of the skin in a
Queensland population. Med J Aust,
155:473-474, 477-478.
Green A, Whiteman D, Frost C, Battistutta D (1999).
Sun exposure, skin cancers and related skin
conditions. J Epidemio/, 9:S7-13.
Greenland S (1987) . Quantitative methods in the
review of epidemiologic literature. Epi Reviews,
9:1-30.
Greinert R, McKinlay A, Breitbart EW (2001 ). The
European Society of skin cancer prevention -
EUROSKIN: towards the promotion and harmo-
nization of skin cancer prevention in Europe.
Recommendations. Eur J Cancer Prev,
10:157-162.
Griffiths HR, Mistry P, Herbert KE, et al. (1998).
Molecular and cellular effects of ultraviolet light-
induced genotoxicity. Grit Rev Clin Lab Sci,
35:189-237.
Grimes DA, Schulz KF (2005). Compared to what?
Finding controls for case-control studies. Lancet,
365:1429-1433.
Guenel P, Laforest L, Cyr D, et al. (2001 ).
Occupational risk factors, ultraviolet radiation,
and ocular melanoma : a case-control study in
France. Cancer Causes Control, 12:451-459.
Halliday G (2005). Inflammation, gene mutation and
photoimmunosuppression in response to UVR-
induced oxidative damage contributes to photo-
carcinogenesis. Mut Res, 571:107-120.
Halliday GM, Agar NS, Barnetson AS, et al. (2005).
UV-A fingerprint mutations in human skin can-
cer. Photochem Photobiol, 81:3-8.
Hamlet N, Kennedy K (2004). Reconnaissance
study of sunbed use by primary school children
in Lanarkshire. J Public Health, 26:31-33.
53
Exposure to Artificial UV Radiation and Skin Cancer
Hannuksela-Svahn A, Sigurgeirsson B, Pukkala E,
et al. (1999). Trioxsalen bath PUVA did not
increase the risk of squamous cell skin carcino-
ma and cutaneous malignant melanoma in a joint
analysis of 944 Swedish and Finnish patients
with psoriasis. Br J Dermatol, 141:497-501.
Hefferren JJ, Cooley RO, Hall JB, et al. (1971 ). Use
of ultraviolet illumination in oral diagnosis. JAm
dent Assoc, 82:1353-1360.
Hemminki K, Bykov VJ, Marcussen JA (1999). Re:
Sunscreen use and duration of sun exposure: A
double-blind, randomised trial. J Nat/ Cancer
lnst, 91:2046-2047.
Hemminki K, Xu G, Le Curieux F (2001). Ultraviolet
radiation-induced photoproducts in human skin
DNA as biomarkers of damage and its repair.
IARC Scientific Publications, 154:69-79.
Henseler T, Wolff K, Honigsmann H, et at. (1981).
Oral 8-methoxypsoralen photochemotherapy of
psoriasis. The European PUVA study: A cooper-
ative study among 18 European centres. Lancet,
1:853-857.
Herity B, O'Loughlin C, Moriarty MJ, Conroy R
(1989). Risk factors for non-melanoma skin can-
cer. J Irish Med, 82:151-152.
Hersey P, Bradley M, Hasic E, et al. (1983).
Immunological effects of solarium exposure.
Lancet, 1 :545-548.
Hersey P, MacDonald M, Henderson C, et at. (1988) .
Suppression of natural killer cell activity in
humans by radiation from solarium lamps
depleted of UVB. J Invest Dermatol,
90:305-310.
Higgins JP, Thompson SG (2002). Quantifying het-
erogeneity in a meta-analysis. Stat Med,
15:1539-1558.
Hogan DJ, ToT, Wilson ER, et al. (1991 ). A study of
acne treatments as risk factors for skin cancer of
the head and neck. Br J Dermatol, 125:343-348.
Holick MF, Matsuoka LY, Wortsman J (1989). Age,
vitamin D, and solar ultraviolet. Lancet,
334:1104-1105.
Holman CD, Armstrong BK, Heenan PJ, et al.
(1986). The causes of malignant melanoma:
results from the West Australian Lions
Melanoma Research Project. Recent Results
Cancer Res, 102:18-37.
Holly EA, Kelly JW, Shpall SN, et al. (1987). Number
of melanocytic nevi as a major risk factor for
malignant melanoma. J Am Acad Dermatol,
17:459-468.
Holly EA, Aston DA, Char DH, et at. (1990). Uveal
melanoma in relation to ultraviolet light exposure
and host factors. Cancer Res, 50:5773-5777.
54
Holly EA, Aston DA, Cress RD, et al. (1995).
Cutaneous melanoma in women. I. Exposure to
sunlight, ability to tan, and other risk factors
related to ultraviolet light. Am J Epidemiol,
141 :923-933.
Holly EA, Aston DA, Ahn DK, et al. (1996).
Intraocular melanoma linked to occupations and
chemical exposures. Epidemiology, 7:55-61.
Honigsmann H (2001). Phototherapy for psoriasis.
Clin exp Dermatol, 26:343-350.
Hornung RL, Magee KH, Lee WJ, et al. (2003).
Tanning facility use: are we exceeding Food and
Drug Administration limits. JAm Acad Dermatol,
49:655-661.
IARC (1992). /ARC Monographs on the Evaluation
of Carcinogenic Risks to Humans, Vol. 55, Solar
and ultraviolet radiation, Lyon, International
Agency for Research on Cancer.
IARC (2001). !ARC Handbooks of Cancer
Prevention, Vol. 5, Sunscreens, Lyon, IARC
Press.
IARC (2004). /ARC Monographs on the Evaluation
of Carcinogenic Risks to Humans, Vol. 83,
Tobacco smoke and involuntary smoking, Lyon,
International Agency for Research on Cancer.
ICNIRP (2002). General approach to protection
against non-ionizing radiation. Health Physics,
82:540-548.
ICNIRP (2004). Guidelines on limits of exposure to
ultraviolet radiation of wavelengths between 180
nm and 400 nm (incoherent optical radiation).
Health Physics, 87:171-186.
Indoor Tanning Association (2004). Statistics and
facts, Sep 30, 2004. Available at: http://www.thei-
ta.com/client_files/news/estimates.pdf (accessed
26 July 2005).
International Electrotechnical Commission (1987).
Safety of Household and Similar Electrical
Appliances, Part 2, Particular Requirements tor
Ultraviolet and Infrared Radiation Skin
Treatment Appliances tor Household Use, IEC
60335-2-27, Geneva, International Electro-
technical Commission.
International Electrotechnical Commission (1989).
Amendment, Geneva, International Electro-
technical Commission.
International Electrotechnical Commission (1995).
Household and similar electrical appliances -
Safety - Part 2-27: Particular requirements for
appliances for skin exposure to ultraviolet and
infrared radiation, IEC 60335-2-27, 3rd edition,
Geneva, International Electrotechnical Com-
mission.
International Electrotechnical Commission (2003).
Household and similar electrical appliances -
Safety - Part 2-27: Particular requirements for
appliances for skin exposure to ultraviolet and
infrared radiation, IEC 60335-2-27, 4th edition,
Geneva, International Electrotechnical
Commission.
IPCS (1994). Ultraviolet radiation, Environmental
Health Criteria 160, Geneva, International
Programme on Chemical Safety, World Health
Organisation, United Nations Environment
Programme.
Javitt JC, Taylor HR (1994). Cataract and latitude.
Doc Ophtha!mol, 88:307-325.
Jenkins G (2002). Molecular mechanisms of skin
ageing. Mech Ageing Dev, 123:801-810.
Kadunce DP, Piepkorn MW, Zone JJ (1990).
Persistent melanocytic lesions associated with
cosmetic tanning bed use: 'Sunbed lentigines'. J
Am Acad Dermato!, 23:1029-1031.
Karagas MR, Stannard VA, Mott LA, et al. (2002).
Use of tanning devices and risk of basal cell and
squamous cell skin cancer. J Nat! Cancer lnst,
94:224-226.
Kaskel P, Sander S, Kron M, et al. (2001 ). Outdoor
activities in childhood: a protective factor for
cutaneous melanoma? Results of a case-control
study in 271 matched pairs. Br J Dermatol,
145:602-609.
Kelly DA, Walker SL, McGregor JM, Young AR
(1998). A single exposure of solar simulated
radiation suppresses contact hypersensitivity
responses both locally and systemically in
humans: quantitative studies with high-frequency
ultrasound. J Photochem Photobiol 8,
44:130-142.
Klepp 0, Magnus K (1979). Some environmental
and bodily characteristics of melanoma patients.
A case-control study. lnt J Cancer, 23:482-486.
Knight JM, Kirincich AN, Farmer ER, Hood AF
(2002). Awareness of the risks of tanning lamps
does not influence behavior among college stu-
dents. Arch Dermatol, 138:1311-1315.
Kraemer KH, Lee MM, Andrews AD, Lambert WC
(1994). The role of sunlight and DNA repair in
melanoma and non-melanoma skin cancer: The
xeroderma pigmentosa paradigm. Arch
Dermatol, 130:1018-1021.
Kreimer-Erlacher H, Seidl H, Back B, et al. (2003).
High frequency of ultraviolet mutations at the
INK4a-ARF locus in squamous cell carcinomas
from psoralen-plus-ultraviolet-A-treated psoria-
sis patients. J invest Dermatol, 120:676-682.
References
Kripke ML (1974) . Antigenicity of murine skin tumors
induced by UV light. J Nat! Cancer lnst,
53:1333-1336.
Kwon HT, Mayer JA, Walker KK, et al. (2002).
Promotion of frequent tanning sessions by
indoor tanning facilities: two studies. JAm Acad
Dermato!, 46:700-705.
de Laat A, van der Leun JC, de Gruijl FR (1997).
Carcinogenesis induced by UVA (365-nm) radia-
tion: the dose-time dependence of tumor forma-
tion in hairless mice. Carcinogenesis,
18:1013-1020.
Lazovich D, Forster J (2005). Indoor tanning by ado-
lescents: prevalence, practices and policies. Eur
J Cancer, 41 :20-37.
Lazovich D, Forster JL, Sorensen G, et al. (2004).
Characteristics associated with adolescents
intention to initiate or continue indoor tanning
use. Arch Pediatr Ado/esc Med, 158:918-924.
Lazovich D, Sweeney C, Forster J (2005).
Prevalence of indoor tanning use in Minnesota,
2002. Arch Dermatol, 141:523-524.
Lerman S (1984). Biophysical aspects of corneal
and lenticular transparency. Curr Eye Res,
3:3-14.
Ley RD (1997). Ultraviolet radiation A-induced pre-
cursors of cutaneous melanoma in Monodelphis
domestica. Cancer Res, 57:3682-3684.
Ley RD (2001 ). Dose response for ultraviolet radia-
tion A-induced focal melanocytic hyperplasia
and nonmelanoma skin tumors in Monodelphis
domestica. Photochem Photobiol, 73:20-23.
Leyden JJ (1990). Clinical features of ageing skin.
Br J Dermato!, 122 (Suppl. 35):1-3.
Lim HW, Cyr WH, DeFabo E, et al. , for the American
Academy of Dermatology Association, American
Society for Photobiology, US Food and Drug
Administration (2004). Scientific and regulatory
issues related to indoor tanning. J Am Acad
Dermatol, 51:781-784.
Lindelof B, Sigurgeirsson B, Tegner E, et al. (1999) .
PUVA and cancer risk: The Swedish follow-up
study. Br J Derma to/, 141 : 1 08-112.
Lucci A, Citro HW, Wilson L (2001). Assessment of
knowledge of melanoma risk factors, prevention,
and detection principles in Texas teenagers.
J Surg Res, 97:179-183.
Lutz JM, Cree I, Sabroe S, et al. (2005).
Occupational risks for uveal melanoma results
from a case-control study in nine European
countries. Cancer Causes Control, 16:437-447.
Macaskill P, Walter SO, lrwig L (2001 ). A comparison
of methods to detect publication bias in meta-
analysis. Stat Med, 20:641-654.
55
J
Exposure to Artificial UV Radiation and Skin Cancer
MacKie RM, Freudenberger T, Aitchison TC (1989).
Personal risk-factor chart for cutaneous
melanoma. Lancet 2:487-90.
Marcil I, Stern RS (2001 ). Squamous-cell cancer of
the skin in patients given PUVA and cyclosporin:
Nested cohort crossover study. Lancet,
358:1 042-1 045.
Marguery MC, Lamant L, Bayle P, et al. (2005).
Lupus-like phototriggering in a young woman
with benign summer li ght eruption.
Photodermatol photoimmunol Photomed,
21:53-55.
Marrot L, Belaidi JP, Lejeune F, et al. (2004).
Photostability of sunscreen products influences
the efficiency of protection with regard to UV-
induced genotoxic or photoageing-related end-
points. Br J Dermatol, 151:1234-1244 .
McGinley J, Martin CJ, MacKie RM (1998). Sunbeds
in current use in Scotland: a survey of their out-
put and patterns of use. Br J Dermatol,
139:428-438.
McGinnis KS, Shapiro M, Vittorio CC, et al. (2003).
Psoralen plus long-wave UV-A (PUVA) and
bexarotene therapy: An effective and synergistic
combined adjunct to therapy for patients with
advanced cutaneous T-cell lymphoma. Arch
Dermatol, 139:771- 775.
McKinlay AF, Diffey BL (1987). A reference action
spectrum for ultraviolet induced erythema in
human skin. CIE (Commission lnternationale de
I'Eclairage) J, 6:17-22.
Mermelstein RJ, Riesenberg LA (1992). Changing
knowledge and attitudes about skin cancer risk
factors in adolescents. Health Psycho/,
11 :371-376.
Millard TP, Bataille V, Snieder H, et al. (2000). The
heritability of polymorphic light eruption. J invest
Dermatol, 115:67-70.
Miller SA, Hamilton SL, Wester UG, Cyr WH (1998).
An analysis of UVA emissions from sunlamps
and the potential importance for melanoma.
Photochem Photobiol, 68:63-70.
Mintz B, Silvers WK (1993). Transgenic mouse
model of malignant skin melanoma. Proc Nat/
Acad Sci USA, 90:8817-8821.
Moore DE (2002). Drug-induced cutaneous photo-
sensitivity: Incidence, mechanism, prevention
and management. Drug Sat, 25:345-372.
Moy CS (2001). Evidence for the role of sunlight
exposure in the etiology of choroidal melanoma.
Arch Ophthalmol, 119:430-431.
Mustajoki P (1980). Variegate porphyria. Twelve
years' experience in Finland. Q J Med,
49:191-203.
56
Naldi L, Gallus S, lmberti GL, et al. , for the Italian
Group for Epidemiological Research in
Dermatology (2000). Sunlamps and sunbeds
and the risk of cutaneous melanoma. Eur J
Cancer Prev, 9:133-134.
National Radiation Protection Board (NRPB)
(2002). Statement by the advisory group on non-
ionizing radiation, use of sunbed and cosmetic
tanning. In : Health Effects from Ultraviolet
Radiation, 13:279-282.
National Toxicology Program (2002). Report on
Carcinogens, 10th Edition, Substances Profiles,
National Toxicology Program, Research Triangle
Park, NC.
Neale RE, Purdie JL, Hirst LW, Green AC (2003).
Sun exposure as a risk factor for nuclear
cataract. Epidemiology, 14:707-712.
Nghiem OX, Kazimi N, Clydesdale G, et al. (2001).
Ultraviolet A radiation suppresses an estab-
lished immune response: implications for sun-
screen design. J lnvestDermatol, 117:1193-99.
Nghiem OX, Kazimi N, Mitchell DL, et al. (2002).
Mechanisms underlying the suppression of
established immune responses by ultraviolet
radiation. J Invest Dermatol, 119:600-608.
Nishigaki R, Mitani H, Tsuchida N, Shima A (1999).
Effect of cyclobutane pyrimidine dimers on
apoptosis induced by different wavelengths of
UV. Photochem Photobio/, 70:228-35.
Noonan FP, Recio JA, Takayama H, et al. (2001 ).
Neonatal sunburn and melanoma in mice.
Nature, 413:271-272.
Oliphant JA, Forster JL, McBride CM (1994). The
use of commercial tanning facilities by suburban
Minnesota adolescents. Am J Public Health,
84:476-478.
O'Loughlin C, Moriarty MJ, Herity B, et al. (1985) . A
Re-appraisal of risk factors for skin carcinoma in
Ireland. lr J med Science, 154:61-65.
Osborne JE, Hutchinson PE (2002). Vitamin D and
systemic cancer: is this relevant to malignant
melanoma? BrJ Dermatol, 147:197-213.
Osterlind A, Tucker MA, Stone BJ, et al. (1988) . The
Danish case-control study of cutaneous malig-
nant melanoma. II. Importance of UV-Iight expo-
sure. tnt J Cancer, 42:319-24.
O'Toole E, Barnes L (1995). Sun-bed-induced
vesiculobullous polymorphic light eruption. Br J
Dermatol, 132:171 .
Paul CL, Girgis A, Tzelepis F, Walsh R (2004).
Solaria use by minors in Australia: is there a
cause for concern? Aust N Z J Public Health,
28:90.
Paul CL, Stacey F, Girgis A, et al. (2005). Solaria
compliance in an unregulated environment: The
Australian experience. Eur J Cancer, 41:
1178-1184.
Pavel S, Smit NP, Van Der Meulen H, et al. (2003).
Homozygous germline mutation of
CDKN2A/p16 and glucose-6-phosphate dehy-
drogenase deficiency in a multiple melanoma
case. Melanoma Res, 13:171-178.
Pedeux A, Al-lrani N, Marteau C, et al. (1998) .
Thymidine dinucleotide induce S phase cell
cycle arrest in addition to increased melanogen-
esis in human melanocytes. J Invest Dermatol,
111:472-477.
Persson AE, Edstrom DW, Backvall H, et al. (2002).
The mutagenic effect of ultraviolet-A 1 on human
skin demonstrated by sequencing the p53 gene
in single keratinocytes. Photodermatol
Photoimmunol Photomed, 18:287-293.
Pfeifer GP, You YH, Besaratinia A {2005). Mutations
induced by ultraviolet light. Mutat Res,
571:19-31.
Pittelkow MR. Perry HO, Muller SA, et al. (1981).
Skin cancer in patients with psoriasis treated
with coal tar. A 25-year follow-up study. Arch
Dermatol, 117:465-468.
Pjrek E, Winkler D, Stastny J, et al. (2004). Bright
light therapy in seasonal affective disorder-
Does it suffice? Eur Neuropsychopharmacol,
14:347-351 .
Placzek M, Kerkmann U, Bell S, et al. (2004).
Tobacco smoke is phototoxic. Br J Dermatol,
150:991- 993.
Poh-Fitzpatrick MB, Ellis DL (1989). Porphyrialike
bullous dermatosis after chronic intense tanning
bed and/or sunlight exposure. Arch Dermatol,
125:1236-1238.
Reme CE, Rol P, Grothmann K, et al. {1996). Bright
light therapy in focus: lamp emission spectra and
ocular safety. Techno/ Health Care, 4:403-413.
Rhainds M, De Guire L, Claveau J (1999). A popu-
lation-based survey on the use of artificial tan-
ning devices in the province of Quebec, Canada.
JAm Acad Dermatol, 40:572- 576.
Rigel DS, Friedman RJ, Levenstein MJ, et al. {1983).
Relationship of fluorescent lights to malignant
melanoma: another view. J Dermatol Surg
Oncol, 9:836-838.
Rivers JK, Norris PG, Murphy GM, et al. {1989).
UVA sunbeds: tanning, photoprotection, acute
adverse effects and immunological changes. Br
J Dermatol, 120:767- 777.
Robert C. Muel B, Benoit A, et al. (1996). Cell sur-
vival and shuttle vector mutagenesis induced by
Exposure to Artificial UV Light and Skin Cancer
UVA and UVB radiation in a human cell line.
J Invest Dermatol, 106:721-728.
Robinson ES, Hubbard GB, Colon G, et al. (1998).
Low-dose ultraviolet exposure early in develop-
ment can lead to widespread melanoma in the
opossum model. tnt J Exp Patho/, 79:235-244.
Robinson ES, Hill RH Jr, Kripke ML, et al. (2000a).
The Monodelphis melanoma model: initial report
on large ultraviolet A exposures of suckling
young. Photochem Photobiol, 71:743-746.
Robinson ES, Hubbard GB, Dooley TP (2000b).
Metastatic melanoma in an adult opossum
(Monodelphis domestica) after short-term inter-
mittent UVB exposure. Arch Dermatol Res,
292:469-471 .
Robinson JK, Rademaker AW, Sylvester JA, Cook B
(1997). Summer sun exposure: knowledge, atti-
tudes and behaviours of midwest adolescents.
Prev Med, 26:364-372.
Roenigk HH Jr (1979). Photochemotherapy for
mycosis fungoides: Long-term followup study.
Cancer Treat Rep, 63:669-673.
Roth DE, Hodge SJ, Callen JP (1989). Possible
ultraviolet A-induced lentigines: A side effect of
chronic tanning salon usage. J Am Acad
Dermatol, 20:950-954.
Ruegemer J, Schuetz B, Hermann K, et al. (2002).
UV-induced skin changes due to regular use of
commercial sunbeds. Photodermatol
Photoimmunol Photomed, 18:223-227.
Sanders CJ, Van Weelden H, Kazzaz GA, et al.
(2003). Photosensitivity in patients with lupus
erythematosus: A clinical and photobiological
study of 1 00 patients using a prolonged pho-
totest protocol. Br J Derma to/, 149:131-137.
Sauter EA. Klein-Szanto AJ, Atillasoy E, et al.
{1998). Ultraviolet B-induced squamous epithe-
lial and melanocytic cell changes in a xenograft
model of cancer development in human skin.
Mol Carcinog, 23:168-174.
Sayre AM, Dowdy JC, Poh-Fitzpatrick M (2004).
Dermatological risk of indoor ultraviolet expo-
sure from contemporary lighting sources.
Photochem Photobiol, 80:47- 51.
Seddon JM, Gragoudas ES, Glynn RJ, et al. (1990).
Host factors, UV radiation, and risk of uveal
melanoma. A case-control study. Arch
Ophtalmol, 1 08:127 4-1280.
Sheehan JM, Patten CS, Young AR (1998). Tanning
in human skin types II and Ill offers modest pho-
toprotection against erythema. Photochem
Photobiol, 68:588-592.
Setlow AB, Regan JD, German J, et al. (1969).
Evidence that xeroderma pigmentosum cells do
57
Exposure to Artificial UV Radiation and Skin Cancer
not periorm the first step in the repair of ultravi
olet damage to their DNA. Proc Nat/ Acad Sci
USA, 64:1035-1041 .
Setlow RB, Grist E, Thompson K, et al. (1993).
Wavelengths effective in induction of malignant
melanoma. Proc Nat/ Acad Sci USA, 90:
6666-6670.
Siemiatycki J (1991 ). Risk factors for cancer in the
work place. Vol. 1, Boca Raton, CRC Press.
Singh RK, Gutman M, Reich R, et al. (1995).
Ultraviolet 8 irradiation promotes tumorigenic
and metastatic properties in primary cutaneous
melanoma via induction of interleukin-8. Cancer
Res, 55:369-374.
Skjerve A, Holsten F, Aarsland D, et al. (2004).
Improvement in behavioral symptoms and
advance of activity acrophase after short-term
bright light treatment in severe dementia.
Psychiatry clin Neurosci, 58:343-347.
Sellitto RB, Kraemer KH, DiGiovanna JJ (1997).
Normal vitamin D levels can be maintained
despite rigorous photoprotection: six years'
experience with xeroderma pigmentosum. JAm
Acad Dermatol, 37:942-947.
Spencer JM, Amonette RA (1995). Indoor tanning:
risks, benefits, and future trends. J Am Acad
Dermatol, 33:288-298.
Stern AS (2001 ). The risk of melanoma in associa-
tion with long-term exposure to PUVA. J Am
Acad Dermatol, 44:755-761.
Stern RS, Laird N (1994). The carcinogenic risk of
treatments for severe psoriasis.
Photochemotherapy Follow-up Study. Cancer,
73:2759-2764.
Stern AS, Lunder EJ (1998) . Risk of squamous cell
carcinoma and methoxsalen (psoralen) and UV-
A radiation (PUVA). A meta-analysis. Arch
Dermatol, 134:1582-1585.
Stoebner-Delbarre A, Thezenas S, Kuntz C, et al.
(2001 ). Connaissances, attitudes et comporte-
ments des adultes vis-a-vis de !'exposition
solaire en France. In: Aubin F. Humbert P (eds)
Rayonnement ultraviolet et peau. Paris, John
Libbey Eurotext, pp 135-140 (in French).
Stryker JE, Lazovich D, Forster JL, et al. (2004).
Maternal/female caregiver influences on adoles-
cent indoor tanning. J Ado/esc Health,
35:528e1-528e9.
Swerdlow AJ, English JS, MacKie RM, et al. (1988).
Fluorescent lights, ultraviolet lamps, and risk of
cutaneous melanoma. Br med J, 297:647-650.
Takahashi Y, Moriwaki S, Sugiyama Y, Endo Y, et al.
(2005). Decreased gene expression responsible
for post-ultraviolet DNA repair synthesis in
58
aging: A possible mechanism of age-related
reduction in DNA repair capacity. J Invest
Dermatol, 124:435-442.
Taylor HR (1994). Ocular effects of UV-8 exposure.
Doc Ophthalmol, 88:285-93.
Tie C, Golomb C, Taylor JR, Streilein JW (1995).
Suppressive and enhancing effects of ultraviolet
B radiation on expression of contact hypersensi-
tivity in man. J Invest Dermatol, 104:18-22.
Tomany SC, Cruickshanks KJ, Klein R, et al. (2004).
Sunlight and the 1 0-year incidence of age-relat-
ed maculopathy: the Beaver Dam Eye Study.
Arch Ophtha/mol, 122:750-757. Erratum in:
Arch Ophtha/mol (2005), 123:362.
Tucker MA, Shields JA, Hartge P, et al. (1985).
Sunlight exposure as risk factor for intraocular
malignant melanoma. N Eng/ J Med,
313:789-792.
Ullrich SE (2005). Mechanisms underlying UV-
induced immune suppression. Mut Res,
571:185-205.
US FDA (1985) Code Fed. Regul., 21 CFR Part
1040 (Docket No. 82N-0188). Sunlamp
Products; Periormance Standard - Final Rule.
Federal Register, Vol. 50, No. 173, US
Department of Health and Human Services.
Food and Drug Administration.
US FDA (2004) Code Fed. Regul., 21 CFR 1040.20.
Sunlamps and sunlamp products; Periormance
standards. Revised as of April 1, 2004, US
Department of Health and Human Services,
Food and Drug Administration.
Vajdic CM, Kricker A, Giblin M, et al. (2004). Artificial
ultraviolet radiation and ocular melanoma in
Australia. /nt J Cancer, 112:896-900.
van Houwelingen HC, Arends LA, Stijnen T (2002).
Advanced methods in meta-analysis: multivari-
ate approach and meta-regression. Stat Med,
21:589-624.
van Schanke A, Jongsma MJ, Bisschop R, et al.
(2005). Single UVB overexposure stimulates
melanocyte proliferation in murine skin, in con-
trast to fractionated or UVA-1 exposure. J Invest
Dermato/, 124:241-247.
Veiemd MB, Weiderpass E, Thorn M, et al. (2003).
A prospective study of pigmentation, sun expo-
sure, and risk of cutaneous malignant
melanoma in women. J Nat/ Cancer lnst,
95:1530-1538.
Veierod MB, Weiderpasss E. Lund E, et al. (2004).
Re: prospective study of pigmentation, sun
exposure, and risk of cutaneous malignant
melanoma in women. J Nat/ Cancer lnt,
96:337-338.
Walter SD, Marrett LD, From L, et al. (1990) . The
association of cutaneous malignant melanoma
with the use of sunbeds and sunlamps. Am J
Epidemiol, 131:232-243.
Walter SD, Marrett LD, Shannon HS, et al. (1992).
The association of cutaneous malignant
melanoma and fluorescent light exposure. Am J
Epidemio/, 135:749--762.
Walter SD, King WD, Marrett LD (1999). Association
of cutaneous malignant melanoma with intermit-
tent exposure to ultraviolet radiation: Results of
a case-control study in Ontario, Canada. lnt J
Epidemiol, 28:418-427.
Walther U, Kron M, SanderS, et al. (2004). Risk and
protective factors for sporadic basal cell carcino-
ma: results of a two-centre case-control study in
southern Germany. Clinical actinic elastosis may
be a protective factor. Br J Dermatol,
151 :170-178.
Wang Y, Rosenstein B, Goldwyn S, et al. (1998) .
Differential regulation of P53 and Bcl-2 expres-
sion by ultraviolet A and B. J Invest Dermatol,
111 :380-384.
Weischer M, Blum A, Eberhard F, et al. (2004). No
evidence for increased skin cancer risk in psori-
asis patients treated with broadband or narrow-
band UVB phototherapy: A first retrospective
study. Acta Derm Venereal, 84:370-374.
Wester U, Boldemann C, Jansson B, Ullen H (1999).
Population UV-dose and skin area -Do sunbeds
rival the sun? Health Physics, 77:436-440.
Westerdahl J, Olsson H, Masback A, et al. (1994).
Use of sunbeds or sunlamps and malignant
melanoma in southern Sweden. Am J Epidemiol,
140:691-699.
Westerdahl J, lngvar C, Masback A, et al. (2000).
Risk of cutaneous malignant melanoma in rela-
tion to use of sunbeds: Further evidence for UV-
A carcinogenicity. Br J Cancer, 82:1593-1599.
Whiteman DC, Whiteman CA, Green A (2001).
Childhood sun exposure as a risk factor for
melanoma: A systematic review of epidemiologic
studies. Cancer Causes Control, 12:69-82.
Whitmore SE, Morison WL, Patten CS, et al. (2001).
Tanning salon exposure and molecular alter-
ations. JAm Acad Dermatol, 44:775-780.
References
WHO (2003). Artificial tanning sunbeds - risks and
guidance, Geneva, World Health Organisation.
Wichstrom L (1994). Predictors of Norwegian ado-
lescents' sunbathing and use of sunscreen.
Health Psycho/, 13:412-420.
Wolf P, Donawho CK, Kripke ML (1994). Effect of
sunscreens on UV radiation-induced enhance-
ment of melanoma growth in mice. J Nat/ Cancer
lnst, 86:99--105.
Woollens A, Clingen PH, Price ML, et al. (1997).
Induction of mutagenic damage in human fibrob-
lasts after exposure to artificial tanning lamps. Br
J Dermatol, 137:687-692.
Wright AL, Hart GC, Kernahan E, et al. (1996).
Survey of the variation in ultraviolet outputs from
ultraviolet A sunbeds in Bradford. Photodermatol
Photoimmunol Photomed, 12:12-16.
Wright A, Hart G, Kernahan L (1997). Dangers of
sun beds are greater in the commercial sector. Br
Med J, 314:1280-1281.
Young AR, Patten CS, Nikaido 0 , et al. (1998).
Human melanocytes and keratinocytes exposed
to UVB or UVA in vivo show comparable levels
of thymine dimers. J Invest Dermatol,
111:936-40.
Young AR (2004). Tanning devices-Fast track to
skin cancer? Pigment Cell Res, 17:2-9.
Zanetti R, Rosso F, Faggiano F, et al. (1988). A
case-control study on cutaneous malignant
melanoma in the province of Torino, Italy. Rev
Epidemiol Sante Publique, 36:309-317 [in
French].
Zhang H, Rosdahl I (2003). Ultraviolet A and B dif-
ferently induce intracellular protein expression in
human skin melanocytes - A speculation of
separate pathways in initiation of melanoma.
Carcinogenesis, 24:1929--1934.
Zigman S (1983). Effects of near ultraviolet radiation
on the lens and retina. Doc Ophtatmol,
55:375-381.
59
'
Appendix: European and international positions regarding artificial
sources of UV radiation
Establishment of a standard for appliances
designed specifically for tanning purposes
Appliances designed specifically for tanning pur-
poses are defined in the international standard
prepared by the International Electrotechnical
Commission (IEC 60 335-2-27). This standard
was first established in 1985 (IEC, 1987) and
slightly modified in 1989 (2nd edition; IEC, 1989),
in 1995 (3rd edition; IEC, 1995) and in 2002 (4th
edition; IEC, 2003). The USA follow the recom-
mendations of the Food and Drug Administration
(US FDA, 1985), which were recently updated
(Lim et al., 2004; US FDA, 2004).
According to the 3rd edition of the IEC stan-
dard, appliances emitting UV radiation must
belong to one of the types described below:
Type UV-1 appliance: appliance with a UV
source such that the biological effect is trig-
gered by radiation wavelengths >320nm, and
which is characterized by relatively high irra-
diance efficiency in the range 32D-400nm.
Type UV-2 appliance: appliance with a UV
source such that the biological effect is trig-
gered by radiation wavelengths above or
below 320nm, and which is characterized by
relatively high irradiance efficiency in the
range 320-400nm.
Type UV-3 appliance: appliance with a UV
source such that the biological effect is
triggered by radiation wavelengths above or
below 320nm and which is characterized by
restricted irradiance over the entire range of
UV radiation.
Type UV-4 appliance: appliance with a UV
source such that the biological effect is
triggered primarily by radiation wavelengths
<320nm.
Table I shows the physical characteristics of the
appliances.
According to the standard, "the appliances
must not be toxic or represent similar hazard. The
appliances emitting UV radiation must not emit
radiation in dangerous amounts and their irradi-
ance efficiency must be within the values
specified in Table [1]". In addition, the standard
states that the verification of conformity must be
performed by 1) determining the ageing of the
appliance before measurement and 2) respecting
a distance of 0.3m.
The guidelines recommend that the exposure
time for the first session on untanned skin should
correspond to an effective dose not exceeding
1 00 J/m
2
; this is approximately equivalent to 1
MED for subjects with sun-reactive skin type I.
The annual exposure should not exceed an effec-
tive dose of 25 kJ/m
2
(IEC, 1989).
Although these guidelines form the basis of
several national standards on the use of tanning
appliances, it should be noted that variations
exist; for example, in the Netherlands, Norway
Table I. Type of UV appliances according to their irradiance efficiency
Type of UV
appliance
lrradlance efficiency In W/m
250 nm < A. < 320 nm 320 nm < A. < 400 nm
2
3
4
< 0.0005
0.0005 to 0.15
< 0.15
2: 0.15
A., radiation wavelength
2: 0.15
2: 0.15
< 0.15
< 0.15
61
Exposure to Artificial UV Radiation and Skin Cancer
and Sweden, certain UV appliances are not per-
mitted. Regulations concerning the use of
tanning appliances are in force in only a few
countries, but many others have published advice
on their use, including information on adverse
effects, as well as guidelines on manufacturing
standards.
In 2004, amendment 1 (2004-2007) to the
4th edition of the standard (2002-2009) added
type-5 appliances to the standard: appliance with
a UV source such that the biological effect is trig-
gered by radiation wavelengths above or below
320nm and which is characterized by a relatively
high irradiance efficiency over the entire range of
UV radiation.
The second amendment is currently being
voted internationally. This amendment would sup-
press the current classes and distinguish only
two classes: appliances for sale to the general
public (formerly type-3 appliances) and appli-
ances for professionals making UV available to
the public.
National and international scientific policies
Several international authorities have adopted a
defined position regarding specifically the use of
UV-emitting appliances for tanning purposes.
These positions are almost invariably accompa-
nied by recommendations targeted at the safety
of customers.
ICNIRP
The International Commission on Non-Ionizing
Radiation Protection (ICNIRP) is an independent
group of experts convened to evaluate available
data on the effects of non-ionizing radiation to
humans. ICNIRP proposes exposure limits to UV
radiation for the general population and in occu-
pational settings for the eye and for the skin, for
an 8-hour exposure period (ICNIRP, 2004).
In its statement relating to UV-emitting
appliances for tanning purposes, ICNIRP, after
considering the effects of UV radiation on the
skin and the different types of existing
appliances, concluded that use of UV-emitting
appliances for tanning and other non-medical
purposes should be discouraged. High-risk
individuals must be particularly warned against
62
the use of tanning appliances. These include:
individuals with skin phototypes I and II;
children and adolescents under the age of 18
years;
individuals with a large number of naevi;
individuals with a tendency to have freckles;
individuals who had frequent sunburns during
childhood;
individuals with pre-malignant and malignant
skin tumours;
individuals with actinic skin ageing;
individuals who have applied cosmetics on
their skin; and
individuals who are taking medication must
seek advice from their doctor to determine
whether their medication renders them more
sensitive to UV.
If, in spite of the above-mentioned recommenda-
tions, individuals decide to use tanning
appliances, a number of measures must be
implemented to minimize the risk. These
measures apply specifically to skin phototype I
and II, children, individuals with increased sensi-
tivity due to the use of medication or cosmetics,
or individuals with a skiR cancer-related pathology.
World Health Organization (WHO)
In 2003, WHO published a document entitled:
"Artificial tanning sunbeds: risks and guidances"
in the framework of the INTERSUN program
(WHO, 2003). This document is based on recom-
mendations cited by other organisations such as
ICNIRP, EUROSKIN and the National
Radiological Protection Board (NRPB), among
others. Specifically, WHO recommends that cos-
tumers carefully read the recommendations and
sign the consent form before each tanning ses-
sion, so as to make them fully aware of their
responsibilities.
EUROSK/N
EUROSKIN dedicated an international meeting
to the problems arising from the use of tanning
appliances. The outcome of the conference was
published in the European Journal of Cancer
Prevention (Greinert eta/. , 2001 ). The document
presents general statements about individuals
,
.i
who should avoid such practices, and makes
specific recommendations on the information to
be given to customers and on how to use UV-
emitting appliances.
National Radiological Protection Board
(NRPB)
In 2002, a group of public health scientists in the
United Kingdom published a report through the
National Radiological Protection Board on the
health effects of UV radiation (NRPB, 2002). The
document advises against the use of UV-emitting
appliances for tanning purposes and recom-
mends that the potential risks for detrimental
health effects be clearly outlined to the users and
to the general population at large.
National Toxicology Program (NTP)
In 2002, the National Toxicology Program in the
USA published the 1Oth Report on Carcinogens
(NTP, 2002) in which UVA, UVB and UVC
radiations were included in the list of "known car-
cinogens to humans". One chapter of the docu-
ment is dedicated to solar radiation and exposure
to UV-emitting appliances. In fact, the American
Medical Association had asked in 1994 for a
complete ban of exposure to UV for non-medical
purposes. In the USA, 27 states have a regulation
regarding availability of indoor tanning facilities to
the general population.
Regulations
Regulations and recommendations of health
authorities from those countries where they are
available are listed in Table II. The following find-
ings can be highlighted:
For consumer safety reasons, Scandinavian
countries authorise only type-3 appliances with
an emission limit of 0.15 w.m
2
for both UVA and
UVB, i.e. a total UV intensity of 0.3 W.m
2
. Some
countries specify that these appl iances may also
be sold to individuals.
The organisations responsible for radiopro-
tection and the health authorities of five
Scandinavian countries (Denmark, Finland,
Iceland, Norway and Sweden) released a joint
Appendix
public health advice recommending that more
stringent safety procedures be adopted regarding
the use of UV tanning appliances. This advice is
in line with the position of international (WHO,
ICNIRP), European (EUROSKIN) and national
organisations.
The countries that produce the majority of
UV tubes and UV tanning appliances (Germany,
Italy and the Netherlands) have no legislation
limiting the manufacturers.
The USA has its own restrictive regulation
imposed by the FDA.
The European Commission has raised a
concem about the lack of upper limits for the
dose rate of type-1 and type-2 appliances (Type-
4 appliances are not concerned).
The legislation in Spain requires that each
individual sign a book, a registry and a consent
form, and be given a tanning booklet specifying
the details of the sessions in accordance with the
characteristics of the UV appliance. This initiative
corresponds to the recommendations of WHO
(WHO, 2003).
The maximal cumulative annual dose of UV
radiation currently established at 15 kJ.m-2 is cal-
culated from the standard IEC 60 335-2-27. This
cumulative dose by far exceeds the dose
received from ambient natural UV. Finland
wishes to set a maximal annual cumulative dose
of 5 kJ.m2. In fact, the maximal annual cumula-
tive dose should be adjusted to the phototype, i.e.
9 kJ.m-2 (NMSC) for phototype II, 15 kJ.m-2
(NMSC) for phototype Ill and 21 kJ.m-2 (NMSC)
for phototype IV.
It is noteworthy that few countries regulate
indoor tanning, and when they do, regulations are
mostly silent on use of these appliances by ado-
lescents. According to a recent review by
Dellavalle et al. (2003), only France has adopted
the age of 18 years as the legal minimum age for
indoor tanning. In the USA, only 6 states have in
place minimum age limits for tanning patrons:
California, Illinois, New Hampshire and North
Carolina restrict access to individuals younger
than 14 years old, while Texas and Wisconsin
restrict access to adolescents younger than 13 and
16 years old, respectively (Francis eta/., 2005).
In France, technical controls are performed
periodically in all registered tanning
63
Exposure to Artificial UV Radiation and Skin Cancer
Table II. Regulations and recommendations from health authorities in those countries where
information is available
Austria
Belgium
Canada
Germany
Finland
France
Italy
Netherlands
Norway
Spain
Sweden
USA
Presnorme 6norm S 1132 : "Safety rules during the use of solaria emitting UV radiations'
(1 January 2002)
"Royal decision on requirements for exploiting solaria" (2000)
Territory, Province and State Committee on radioprotection : "Guidelines to owners, operators and
users of tanning salons". Enforcement of regulations enacted to implement the" law relating to
appliances emitting radiations - RED Act : Regulations of sun lamps , (2002-2003)
Bundesamt fUr Strahlenschutz, Munich : ' Certification of solaria" (proposal)
Currently, UV exposure in solaria must respect the German standard DIN 5050-2 (June 1998)
Decree on the limitation of public exposure to non-ionising radiation (294/2002) chapter 4,
"Ultraviolet radiation"; SS 9.1 "Safety of solaria" (1989); SONT 9.1 "Safety and control conditions
of solaria" (project) (2003)
Decree no 97-617 (30 May 1997) and regulations of 10 September 1997, 09 December 1997 and
16 September 2002 enacted to implement the law
lstituto Superiore di Sanita "Devices must conform to the technical norm IEC 60335-2-27"
(1995-2003); detailed information available at http://www.iss.iVsitp/sole/abbrarVIeggi.html
No formal regulation.
Several reports from the Dutch Health Council (1987, 1994)
Regulations of 8 April 1983 for solaria/alpine sun. Delegation of authority regulation fixing by royal
decree the usage of UV radiations for cosmetic purposes (01 July 1983)
19574 Royal decree 100212002: "Regulation of sale and use of tanning appliances emitting
UV radiations" (27 September 2002)
Regulatory code concerning sunbeds (SSI FS 1998:2) "The regulation of tanni ng appliances
used by the public fulfils the criteria of the standard EN 60335-2-27." (28 September 1998 and
03 November1 998)
FDA Sunlamp Performance Standard 21CFR1040.20 combined wi th a guide (1986) on timers
and frequency of exposure (updated 01 April 2004)
establishments since 1999. The proportion of
establishments 90mpliant with the technical
requirements increased from 51% in 1999 to
72% in 2003. Periodic visits in 2002 and 2003 to
additional establishments showed a compliance
of 85% and 81%, respectively. Non-compliance
was mainly for minor infractions (AFSSE, 2005).
tanning facilities in 2002 and 2003. The following
comments were noted: the facility operators are
well informed of the regulations in place; the
compulsory declaration was generally satisfactory;
in most places, at least one person had the
required qualifications, but the need for
continuing education was not perceived clearly;
information to the customers were usually
available to the users, but information on risks
was often lacking (AFSSE, 2005).
In addition, the Direction Generale de Ia
Concurrence, de Ia Consommation et de Ia
Repression des Fraudes (DGCCRF) proceeded
to a series of controls and enquiries about indoor
64
WORLD HEALTH ORGANIZAflON
INTERNATIONAL AGENCY FOR RESEARCH ON CANCER
IARC MONOGRAPHS
ON THE
EVALUATION OF CARCINOGENIC
RISKS TO HUMANS
Solar and Ultraviolet Radiation
VOLUME 55
This publication represents the views and expert opinions
of an IARC Working Group on the
Evaluation of Carcinogenic Risks to Humans,
which met in Lyon,
11-18 February 1992
1992
IARC MONOGRAPHS
In 1969, the International Agency for Research on Cancer {IARC) initiated a programme
on the evaluation of the carcinogenic risk of chemicals to humans involving the production of
critically evaluated monographs on individual chemicals. In 1980 and 1986, the programme
was expanded to include the evaluation of the carcinogenic risk associated with exposures to
complex mixtures and other agents.
The objective of the programme is to elaborate and publish in the form of monographs
critical reviews of data on carcinogenicity for agents to which humans are known to be
exposed, and on specific exposure situations, to evaluate these data in terms of human risk
with the help of international working groups of experts in chemical carcinogenesis and
related fields; and to indicate where additional research efforts are needed.
This project is supported by PHS Grant No. 2-UO 1 CA33193- 10 awarded by the US
National Cancer Institute, Department of Health and Human Services. Additional support
has been provided since 1986 by the Commission of the European Communities.
International Agency for Research on Cancer 1992
ISBN 92 832 1255 X
ISSN 0250-9555
All rights reserved. Application for rights of reproduction or translation, in part or in t ~
should be made to the International Agency for Research on Cancer.
Distributed for the International Agency for Research on Cancer
by the Secretariat of the World Health Organization
PRINTED IN THE UNITED KINGDOM
I
I
I
I
I
I
I
I
I
I
I
CONTENTS
I
I
I
NO'fE TO THE READER . ... . . .. ..... . .... .. . ... .... .. .... . . ... .. ...... . 11
I
I
UST OF PARTICIPANTS . . .. .. ..... .. . . . ... . . . . . . . . ... .. . ... .. . . .. . . .. .. . 13 I
PREAMBLE
I
Background ... . ... . . . ..... . ...... . ... . .... . ... . .. ... . ...... . .... . . . . 19
Objective and Scope .. .... .. ... ... ..... . ....... .... .. . . . . ..... . . ..... . 19
Selection of Topics for Monographs ... .. .. ... . . .... .... . .. . .... . .... .. .. . 20
Data for Monographs . . ... ..... .. . ..... . . . . ... . . . ... . . . . . . ... . ... . .. . . 21
The Working Group . . .. .... . . .. . . . . . . ... . . .... .. .. .. . ... . ... .. .. .... . 21
Working Procedures . ..... .. .. . .. . .. . ... . . .. . . . . . .. ... . ... ...... . . .. . . 21
Exposure Data ... . .. ..... . .. . . . ... . . . ... .... . . .. .. .. . ........ . . .. .. . . 22
Evidence for Carcinogenicity in Humans ... ... . . . . .... . .. . .. . . . . . ... . . . . . . 23
Studies of Cancer in Experimental Animals . .. .. . .. .. .. .. .. .......... ... . . 27
Other Relevant Data .. ... . .. .... . . ....... ... ... ... .. . .... .. . .. ... .. . . 29
Summary of Data Reported . .. . .. ... .. .. .... ... . . .. .. .. .. . ... ... . . .. .. . 30
Evaluation .... . . .. .... .. . ... . . ... . . . ..... . .. . .. .. .. .. . . ..... . . .. .. . . 32
References . . .... ....... . .... .. .. .. .......... . . ... .. . .. . . . . ... . .. . .. . 36
GENERAl. REMARKS .. ... .. .. .. .. .. . . ... .. . . . .. .. .. ........ . .. . . .. .. . . 39
SOLAR AND ULTRAVIOLET RADIATION
1. Exposure data ... ..... . .. . . ..... . . ...... . .. ... . .. .... .. . .... . .. . .. ... . 43
1.1 Nomenclature . .. ... . . . . . . .. . . . ...... . . . .. ... .. .. ... .. ... . . . . . .. . 43
1.1.1 Optical radiation ... . .. . .. ... ... . ....... . . . ........ . . .. .. ... . 43
1.1.2 Quantities and units ... . . .. . .. .. . ........ . . .... ...... . .. ... . . 45
1.1.3 Units of biologically effective ultraviolet radiation ...... . .. .. .... . 46
1.2 Methods for measuring ultraviolet radiation ..... .. ...... ... . . . .. . .. .. . 47
1.2.1 Spectroradiometry .. . ..... .. .. . ...... . . .. . . ...... .. .. .. .. . . . 47
1.2.2 Wavelength-independent (thermal) detectors . ..... .. ... . ... ... . . . 48
1.2.3 Wavelength-dependent detectors . ... . ... .. ... .. .... ... . ...... . . 48
1.3 Sources and exposures . . .... . ... . .... .... . .... . . ... . ..... .... .. ... . 49
1.3.1 Solar ultraviolet radiation ....... . . . . . . ... . ........ . ..... .. .. . 50
(a) Measurements of terrestrial solar radiation ... . . . . .. .. . . . .. . . 54
(b) Personal exposures ... . ... . . ... .. . .. ... .. . ... . .. . .. .. .. . . 57
1.3.2 Exposure to artificial sources of ultraviolet radiation . . . . . .. . . . . .. . 58
(a) Sources ... .. ... ... . . . ... .. .. . . .. .. ...... . ..... . .. . .. .. . 58
(i) Incandescent sources .... . ... .... . . .. .. .. . .. ... . ... .. . 58
. (ii) Gas discharge lamps . . . .. ... ... . .. ... .. ... . ... .. .. . . . 59
CONTENTS
(iii) Arc lamps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
(iv) Fluorescent lamps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
(v) Metal halide lamps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
(vi) Electrodeless lamps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
(b) Human exposure ...... .. .... . ...................... .. .. . 60
(i) Cosmetic use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
(ii) Medical and dental applications . . . . . . . . . . . . . . . . . . . . . . . . 63
(iii) Occupational exposures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
(iv) General lighting ..................... .. . . . . . . . . . . . . . 70
(c) Regulations and guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
(i) Cosmetic use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
(ii) Occupational exposure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
2. Studies of cancer in humans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
2.1 Solar radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
2.1.1 Nonmelanocytic skin cancer ... . .. . . . . .......... . . . . . ... ....... 73
(a) Case reports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
(i) Studies of xeroderma pigmentosum patients . . . . . . . . . . . . . . 73
(ii) Studies of transplant recipients . . . . . . . . . . . . . . . . . . . . . . . . 73
(b) Descriptive studies . .. .... . ......... .. .. ........ ... .. ..... 74
(i) Host factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74
(ii) Anatomical distribution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74
(iii) Geographical variation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
(iv) Migration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
(v) Occupation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
(c) Cross-sectional studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77
(d) Case-control studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
(e) Cohort studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
(j) Collation of results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
2.1.2 Cancer of the lip . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
(a) Descriptive studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
(i) Geographical variation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
(ii) Occupation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
(b) Case-control studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
2.1.3 Malignant melanoma of the skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
(a) Case reports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
(b) Descriptive studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
(i) Sex distribution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
(ii) Age distribution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
(iii) Anatomical distribution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
(iv) Ethnic origin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
(v) Geographical variation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
(vi) Migration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 99
(vii) Socioeconomic status and occupation . . . . . . . . . . . . . . . . . 99
--------
CONTENfS
(c) Case-control studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100
(i) Australia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100
(ii) Europe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102
(iii) North America . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
(d) Collation of results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113
(i) Total sun exposure: potential exposure by place of residence 113
(ii) Biological response to total sun exposure . . . . . . . . . . . . . . . 113
(iii) Total sun exposure assessed by questionnaire . . . . . . . . . . . . 115
(iv) Short periods of residence implying high potential exposure 115
(v) Occupational exposure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 115
(vi) Intermittent exposure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 115
(vii) Sunburn . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122
2.1.4 Malignant melanoma of the eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122
(a) Case reports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122
(b) Descriptive studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 125
(i) Ethnic origin . . . . . . .. . . . . .. .. . . . . . . . .. . . . .. . .. . .. . . 125
(ii) Place of birth and residence . . . . . . . . . . . . . . . . . . . . . . . . . . 125
(iii) Occupation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 127
(iv) History of skin cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 127
(c) Case-control studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 127
2.1.5 Other cancers . . . . . . . . . . . . . . . . . . . . . . . . . . ... . . . . . . . . . . . . . . . . . 130
2.2 Artificial sources of ultraviolet radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 130
2.2.1 Nonmelanocytic skin cancer. . .. .......... . . . . . . . . . . . . . . . . . . . . 130
2.2.2 Malignant melanoma of the skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 130
2.2.3 Malignant melanoma of the eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134
2.3 Premalignant conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134
2.3.1 Basal-ceH naevus syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134
2.3.2 Dysplastic naevus syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134
2.4 Molecular genetics of human skin cancers . . . . . . . . . . . . . . . . . . . . . . . . . . . 135
2.4.1 ras Gene mutations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 135
2.4.2 p53 Gene mutations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 135
3. Studies of cancer in animals. . ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 139
3.1 Experimental conventions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 139
3.1.1 Species studied . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 139
3.1.2 Wavelength ranges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 139
3.1.3 Measured doses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 140
3.1.4 Protocols . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 140
3.2 Broad-spectrum radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
3.2.1 Sunlight ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
3.2.2 Solar-simulated radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142
3.2.3 Sources emitting UVC, UVB and UVA radiation . . . . . . . . . . . . . . . . 142
3.3 Sources emitting mainly UVB radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 144
3.3.1 Mouse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 144
I
I
I
I
I
I
I
I
I
I
I
I
I
I
CONTENfS
3.3.2 Rat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
3.3.3 Hamster . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
3.3.4 Guinea-pig. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
3.3.5 Fish . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
3.3 .6 Opossum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
3.4 Sources emitting mainly UVC radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 147
3.4.1 Mouse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 147
3.4.2 Rat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 148
3.5 Sources emitting mainly UVA radiation . . . . . ... ..... . ... . .......... . 148
3.6 Interaction of wavelengths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 150
3.6.1 Interaction of exposures given on the same day . . . . . . . . . . . . . . . . . . 150
3.6.2 Long-term interactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151
3.7 Additional experimental observations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151
3.7.1 Tumour types . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151
3.7.2 Dose and effect . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
3.7.3 Dose delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154
3. 7.4 Action spectra . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154
3.7.5 Pigmentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155
3.8 Administration with known chemical carcinogens . . . . . . . . . . . . . . . . . . . . . 155
3.8.1 Administration with polycyclic aromatic hydrocarbons . . . . . . . . . . . . 156
(a) 3,4-Benzo[a]pyrene ........ ... . . ..... .. ... . .... ... ...... 156
(b) 7,12-Dimethylbenz[a]anthracene ... . ..................... . 156
3.8.2 Administration with other agents with promoting activity . . . . . . . . . . 157
(a) Croton oil . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 157
(b) 12-0-Tetradecanoylphorbol 13-acetate . . . . . . . . . . . . . . . . . . . . . 158
(c) Benzoyl perm<ide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 158
(d) Methyl ethyl ketone peroxide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 159
3.9 Interaction with immunosuppressive agents . . . . . . . . . . . . . . . . . . . . . . . . . . 160
3.10 Molecular genetics of animal skin tumours induced by ultraviolet radiation 161
4. Other relevant data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163
4.1 Transmission and absorption in biological tissues . . . . . . . . . . . . . . . . . . . . . . 163
4.1.1 Epidermis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163
(a) Humans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163
(b) Experimental systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 164
(c) Epidermal chromophores . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 165
(d) Enhancement of epidermal penetration of ultraviolet radiation . 166
4.1.2 Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166
(a) Humans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166
(b) Experimental systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166
4.2 Adverse effects (other than cancer) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167
4.2.1 Epidermis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167
(a) Humans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167
(i) Erythema and pigmentation (sunburn and suntanning) . . . . 167
CONTENTS
(ii) Pigmented naevi . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 169
(iii) Ultrastructural changes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 170
(iv) Keratosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172
(v) Photosensitivity disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172
(b) Experimental systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173
(c) Comparison of humans and animals . . . . . . . . . . . . . . . . . . . . . . . 174
4.2.2 Immune response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175
(a) Humans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175
(i) Contact hypersensitivity (allergy) . . . . . . . . . . . . . . . . . . . . . . 175
(ii) Lymphocytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 176
(iii) Infectious diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 177
(iv) Photosensitive diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 177
(b) Experimental systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 177
(i) Contact hypersensitivity ..... ........... . . .'. . . . . . . . . . 177
(ii) Delayed hypersensitivity to injected antigens . . . . . . . . . . . . 179
(iii) Immunology of ultraviolet-induced skin cancer . . . . . . . . . . 180
(iv) Transplantation immunity . . . . . . . . . . . . . . . . . . . . . . . . . . . . 180
(v) Infectious diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181
(vi) Human lymphocytes in vitro ......... . . .. . .............. 182
(c) Comparison of humans and animals . . . . . . . . . . . . . . . . . . . . . . . 182
4.2.3 Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183
(a) Humans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183
(i) Anterior eye (cornea, conjunctiva) . . . . . . . . . . . . . . . . . . . . . 183
(ii) Lens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183
(iii) Posterior eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183
(b) Experimental systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184
(i) Anterior eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184
(ii) Lens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184
(iii) Posterior eye .. ... ...... . . . . . . . . . . . . . . . . . . . . . . . . . . . 184
(c) Comparison of humans and animals . . . . . . . . . . . . . . . . . . . . . . . 184
4.3 Photoproduct formation ........... . ................ .. .... ; . . . . . . . 185
4.3.1 DNA photoproducts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 185
(a) Cyclobutane-type pyrimidine dimers . . . . . . . . . . . . . . . . . . . . . . . 185
(b) Pyrimidine- pyrimidone (6-4) photoproducts . . . . . . . . . . . . . . . . . 186
(c) Thymine glycols . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 187
(d) Cytosine damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 188
(e) Purine damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 188
(/) DNA strand breaks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 188
(g) DNA-protein cross-links. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 189
4.3.2 Other chromophores and targets. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 189
(a) Chromophores . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 189
(b) Membranes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 190
CONTENTS
4.4 Human excision repair disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 191
4.4.1 Xeroderma pigmentosum ................................. ... 191
4.4.2 Trichothiodystrophy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192
4.4.3 Cockayne 's syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 193
4.4.4 Role of immunosuppression. . ......... . . . . . . . . . . . . . . . . . . . . . . . 193
4.5 Genetic and related effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 194
4.5.1 Humans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 194
(a) Epidermis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 195
(i) Broad-spectrum ultraviolet radiation, including solar
simulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 195
(ii) UVA radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 196
(iii) UVB radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 196
(iv) UVC radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 197
(b) Lymphocytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 198
(i) Broad-spectrum ultraviolet radiation . . . . . . . . . . . . . . . . . . . 198
(ii) UVA radiation ..................... . .............. . 199
(iii) UVB radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 199
4.5.2 Experimental systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 199
(a) DNA damage ... ... ............... .. ... .. . .... ... .. .. . . 199
(b) Mutagenicity . ........ . .... . .. . ... . ......... . . .. ..... .. 200
(c) Chromosomal effects .. ....................... . .......... 202
(d) Transformation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203
(e) Effects of cellular and viral gene expression . . . . . . . . . . . . . . . . . 204
5. Summary of data reported and evaluation ..................... -. . . . . . . . . . . 217
5.1 Exposuredata . . . . . . .... .. ... . . ...... ............. ... ........... 217
5.2 Human carcinogenicity data ....... . .... . ........ .. .... .... . .. ... . . 218
5.2.1 Solar radiation ......................... . . . ..... . ... .. . . . .. 218
(a) Nonmelanocytic skin cancer . ......... . . .. .... .... ........ 218
(b) Cancer of the lip ........................ . ... ........... 219
(c) Malignant melanoma of the skin ...... .. .. ....... . ... ..... 219
(d) Melanoma of the eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2ZO
(e) Other cancers .............. . ........ . .. .............. .. 220
5.2.2 Artificial sources of ultraviolet radiation . . . . . . . . . . . . . . . . . . . . . . . 220
5.2.3 Molecular genetics of human skin cancers . . . . . . . . . . . . . . . . . . . . . . 221
5.3 Carcinogenicity in experimental animals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221
5.4 Other relevant data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222
5.4.1 Transmission and absorption ........ . .. . ..... .. ... ....... .. .. 222
5.4.2 Effects on the skin ................ . ..... . ..... ... .. ... . . ... 222
5.4.3 Effects on the immune response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222
5.4.4 DNA photoproducts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223
5.4.5 Genetic and related effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223
5.5 Evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 227
6. References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 229
CONTENTS
SUMMARY OF FINAL EVALUATIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 281
GLOSSARY OF TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 283
Appendix 1. Topical sunscreens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285
1. General . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285
2. Protective effects . .... . ... . . ..... . .. .. .. . . ..... . . . ..... .. .. . .. : . . . . . . . 286
2.1 Against DNA damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 286
2.2 Against acute and chronic actinic damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . 286
2.3 Against immunological alterations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 286
2.4 Against tumour formation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 286
3. Adverse effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
3.1 Acute toxicity . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
3.2 Chronic toxicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
3.3 Reduced vitamin D synthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
4. References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 288
CUMULATIVE INDEX TO THE MONOGRAPHS SERIES . . . . . . . . . . . . . . . . . . . 291 ~ - - - - - - ' __________________________ _
NOTE TO THE READER
The term 'carcinogenic risk' in the /ARC Monographs series is taken to mean the proba-
bility that exposure to an agent will lead to cancer in humans.
Inclusion of an agent in the Monographs does not imply that it is a carcinogen, only that
the published data have been examined. Equally, the fact that an agent has not yet been
evaluated in a monograph does not mean that it is not carcinogenic.
The evaluations of carcinogenic risk are made by international working groups of in-
dependent scientists and are qualitative in nature. No recommendation is given for regu-
lation or legislation.
Anyone who is aware of published data that may alter the evaluation of the carcinogenic
risk of an agent to humans is encouraged to make this information available to the Unit of
Carcinogen Identification and Evaluation, International Agency for Research on Cancer,
150 cours Albert Thomas, 69372 Lyon Cedex 08, France, in order that the agent may be
considered for re-evaluation by a future Working Group.
Although every effort is made to prepare the monographs as accurately as possible,
mistakes may occur. Readers are requested to communicate any errors to the Unit of
Carcinogen Identification and Evaluation, so that corrections can be reported in future
volumes.
-11-
Members
1
IARC WORKING GROUP ON THE EVALUATION
OF CARCINOGENIC RISKS TO HUMANS
VOLUME 55: SOLAR AND ULTRAVIOLET RADIATION
Lyon, 11-18 February 1992
LIST OF PARTICIPANTS
C. Arlett, MRC Cell Mutation Unit, University of Brighton, Falmer, Brighton BNl 9RR,
United Kingdom
B. Bridges, MRC Cell Mutation Unit, University of Brighton, Falmer, Brighton BNl 9RR,
United Kingdom (Chairman)
A Br!ISgger, Department of Genetics, Institute for Cancer Research, Montebello, 0310 Oslo
3, Norway
B.L. Diffey, Regional Medical Physics Department, Dryburn Hospital, Durham DHl 5TW,
United Kingdom
J .M. Elwood, Hugh Adam Cancer Epidemiology Unit, University of Otago Medical School,
PO Box 913, Dunedin, New Zealand
E.A. Emmett, Worksafe Australia, National Occupational Health and Safety Commission,
92 Parramatta Road, Camperdown, NSW 2050, Australia
D. English, NHMRC Research Unit, The Queen Elizabeth II Medical Centre, University of
Western Australia, Nedlands, WA 6009, Australia
P.D. Forbes, Temple University, Biohazards Control Office, Environmental Health and
Safety Offices, 3307 North Broad Street, Philadelphia, PA 19140, USA
R.P. Gallagher, British Columbia Cancer Agency, 600 West lOth Avenue, Vancouver, BC
V52 4E6, Canada
J.W. Grisham, Department of Pathology, University of North Carolina, Brinkhous-Bullitt
Building CB# 7525, Chapel Hill, NC 27599, USA
1
Unable to attend: J. Marshall, Department of Ophthalmology, Block 8, UNDS, StThomas's Hospital,
London SEl 7EH, United Kingdom
-13-
14 IARC MONOGRAPHS VOLUME 55
K. Kraemer, National Cancer Institute, Division of Cancer Etiology, Laboratory of
Molecular Carcinogenesis, Building 37, Room 3D-06, Bethesda, MD 20892, USA
J.C. van der Leun, Institute of Dermatology, University Hospital Utrecht, Heidelberglaan
100, 3584 CX Utrecht, The Netherlands
T. Mack, University of Southern California, School of Medicine, Department of Preventive
Medicine, Parkview Medical Building, 1420 San Pablo Street, Los Angeles, CA
90033-9987, USA (Vice-Chairman)
W.L. Morison, Johns Hopkins University, Baltimore, MD 21205, USA
S. Olin, ILSI Risk Science Institute, 1126 Sixteenth Street NW, Washington DC 20036, USA
A 0sterlind, Danish Cancer Registry, Rosenvaengets Hovedvej 35, Box 839, 2100
Copenhagen, Denmark
D.H. Sliney, Laser Branch, US Army Environmental Hygiene Agency, Aberdeen Proving
Ground, MD 21010-5422, USA
F. Stenbiick, Department of Pathology, University of Oulu, Kajaanintie 52 D, 90220 Oulu 22,
Finland
R.M. 1}rrrell, Swiss Institute for Experimental Cancer Research, 1066 Epalinges-sur-
Lausanne, Switzerland
AR. Young, Photobiology Department, StJohn's Institute of Dermatology, StThomas's
Hospital, London SE1 7EH, United Kingdom
Representative of the US Food and Drug Administration
J.Z. Beer, US Food and Drug Administration, Center for Devices and Radiological Health,
12709 Twinbrook Parkway, Rockville, MD 20852, USA
Observers
R.C. Burton, Department of Surgery, John Hunter Hospital, Locked Bag #1, Newcastle Mail
Centre, Newcastle, NSW 2310, Australia
C.J. Portier, National Institute of Environmental Health Sciences, PO Box 12233, Res.earch
Triangle Park, NC 27709, USA
Secretariat
B. Armstrong, Deputy Director
H. Bartsch, Unit of Environmental and Host Factors
P. Boffetta, Unit of Analytical Epidemiology
J .R.P. Cabral, Unit of Mechanisms of Carcinogenesis
E. Cardis, Director's Office
M. Friesen, Unit of Environmental and Host Factors
M.-J. Ghess, Unit of Carcinogen Identification and Evaluation
J. Hall, Unit of Mechanisms of Carcinogenesis
E. Heseltine, Lajarthe, St Leon-sur-Vezere, France
A Kricker, Unit of Descriptive Epidemiology
PARTICIPANTS
V. Krutovskikh, Unit of Multistage Carcinogenesis
D. McGregor, Unit of Carcinogen Identification and Evaluation
D. Mietton, Unit of Carcinogen Identification and Evaluation
H. M0ller, Unit of Carcinogen Identification and Evaluation
R. Montesano, Unit of Mechanisms of Carcinogenesis
T. Nakazawa, Unit of Multistage Carcinogenesis
I. O'Neill, Unit of Environmental and Host Factors
M. Parkin, Unit of Descriptive Epidemiology
C. Partensky, Unit of Carcinogen Identification and Evaluation
I. Peterschmitt, Unit of Carcinogen Identification and Evaluation, Geneva, Switzerland
D. Shuker, Unit of Environmental and Host Factors
L. Tomatis, Director
H. Vainio, Unit of Carcinogen Identification and Evaluation
1. Wilbourn, Unit of Carcinogen Identification and Evaluation
H. Yamasaki, Unit of Multistage Carcinogenesis
Secretarial assistance
1. Cazeaux
M. Lezere
S. Reynaud
15
PREAMBLE
IARC MONOGRAPHS PROGRAMME ON THE EVALUATION
OF CARCINOGENIC RISKS TO HUMANS
1
PREAMBLE
1. BACKGROUND
In 1969, the International Agency for Research on Cancer (IARC) initiated a pro-
gramme to evaluate the carcinogenic risk of chemicals to humans and to produce mono-
graphs on individual chemicals. The Monographs programme has since been expanded to
include consideration of exposures to complex mixtures of chemicals (which occur, for
example, in some occupations and as a result of human habits) and of exposures to other
agents, such as radiation and viruses. With Supplement 6 (IARC, 1987a), the title of the series
was modified from /ARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals
to Humans to /ARC Monographs on the Evaluation of Carcinogenic Risks to Humans, in order
to reflect the widened scope of the programme.
The criteria established in 1971 to evaluate carcinogenic risk to humans were adopted by
the working groups whose deliberations resulted in the first 16 volumes of the /ARC
Monographs series. Those criteria were subsequently updated by further ad-hoc working
groups (IARC, 1977, 1978, 1979, 1982, 1983. 1987b, 1988, 199la; Vainio eta/., 1992).
2. OBJECTIVE AND SCOPE
The objective of the programme is to prepare, with the help of international working
groups of experts, and to publish in the form of monographs, critical reviews and evaluations
of evidence on the carcinogenicity of a wide range of human exposures. The Monographs may
also indicate where additional research efforts are needed.
The Monographs represent the first step in carcinogenic risk assessment, which involves
examination of all relevant information in order to assess the strength of the available
evidence that certain exposures could alter the incidence of cancer in humans. The second
step is quantitative risk estimation. Detailed, quantitative evaluations of epidemiological
data may be made in the Monographs, but without extrapolation beyond the range of the data
1
This project is supported by PHS Grant No.2 UOI CA33193-10 awarded by the US National Cancerlnstitute,
Department of Health and Human Services. Since 1986, the programme has also been supported by the Com-
mission of the European Communities.
-19-
20 IARC MONOGRAPHS VOLUME 55
available. Quantitative extrapolation from experimental data to the human situation is not
undertaken.
The term ' carcinogen' is used in these monographs to denote an exposure that is capable
of increasing the incidence of malignant neoplasms; the induction of benign neoplasms may
in some circumstances (seep. 28) contribute to the judgement that the exposure is carcino-
genic. The terms 'neoplasm' and 'tumour' are used interchangeably.
Some epidemiological and experimental studies indicate that different agents may act at
different stages in the carcinogenic process, and several different mechanisms may be
involved. The aim of the Monographs has been, from their inception, to evaluate evidence of
carcinogenicity at any stage in the carcinogenesis process, independently of the underlying
mechanisms. Information on mechanisms may, however, be used in making the overall eval-
uation (IARC, 1991a; Vainio eta/., 1992; see also pp. 33-34).
The Monographs may assist national and international authorities in making risk
assessments and in formulating decisions concerning any necessary preventive measures.
The evaluations of IARC working groups are scientific, qualitative judgements about the
evidence for or against carcinogenicity provided by the available data. These evaluations
represent only one part of the body of information on which regulatory measures may be
based. Other components of regulatory decisions may vary from one situation to another and
from country to country, responding to different socioeconomic and national priorities.
Therefore, no recommendation is given with regard to regulation or legislation, which are the
responsibility of individual governments and/or other international organizations.
The /ARC Monographs are recognized as an authoritative source of information on the
carcinogenicity of a wide range of human exposures. A users' survey, made in 1988, indicated
that the Monographs are consulted by various agencies in 57 countries. Each volume is
generally printed in 4000 copies for distribution to governments, regulatory bodies and
interested scientists. The Monographs are also available via the Distribution and Sales
Service of the World Health Organization.
3. SELECTION OF TOPICS FOR MONOGRAPHS
Topics are selected on the basis of two main criteria: (a) there is evidence of human
exposure, and (b) there is some evidence or suspicion of carcinogenicity. The term 'agent' is
used to include individual chemical compounds, groups of related chemical compounds,
physical agents (such as radiation) and biological factors (such as viruses). Exposures to
mixtures of agents may occur in occupational exposures and as a result of personal and
cultural habits (like smoking and dietary practices). Chemical analogues and compounds
with biological or physical characteristics similar to those of suspected carcinogens may also
be considered, even in the absence of data on a possible carcinogenic effect in humans or
experimental animals.
The scientific literature is surveyed for published data relevant to an assessment of
carcinogenicity. The IARC surveys of chemicals being tested for carcinogenicity (IARC,
1973-1990) and directories of on-going research in cancer epidemiology (IARC, 1976-
1991) often indicate those exposures that may be scheduled for future meetings. Ad-hoc
working groups convened by IARC in 1984, 1989 and 1991 gave recommendations as to
which agents should be evaluated in the /ARC Monographs series (IARC, 1984, 1989, 1991b ).
PREAMBLE 21
As significant new data on subjects on which monographs have already been prepared
become available, re-evaluations are made at subsequent meetings, and revised monographs
are published.
4. DATA FOR MONOGRAPHS
The Monographs do not necessarily cite all the literature concerning the subject of an
evaluation. Only those data considered by the Working Group to be relevant to making the
evaluation are included.
With regard to biological and epidemiological data, only reports that have been
published or accepted for publication in the openly available scientific literature are
reviewed by the working groups. In certain instances, government agency reports that have
undergone peer review and are widely available are considered. Exceptions may be made on
an ad-hoc basis to include unpublished reports that are in their final form and publicly
available, if their inclusion is considered pertinent to making a final evaluation (see pp. 32
et seq.). In the sections on chemical and physical properties, on analysis, on production and
use and on occurrence, unpublished sources of information may be used.
5. THE WORKING GROUP
Reviews and evaluations are formulated by a working group of experts. The tasks of the
group are: (i) to ascertain that all appropriate data have been collected; (ii) to select the data
relevant for the evaluation on the basis of scientific merit; (iii) to prepare accurate summaries
of the data to enable the reader to follow the reasoning of the Working Group; (iv) to
evaluate the results of experimental and epidemiological studies on cancer; (v) to evaluate
data relevant to the understanding of mechanism of action; and (vi) to make an overall
evaluation of the carcinogenicity of the exposure to humans.
Working Group participants who contributed to the considerations and evaluations
within a particular volume are listed, with their addresses, at the beginning of each publi-
cation. Each participant who is a member of a working group serves as an individual scientist
and not as a representative of any organization, government or industry. In addition,
nominees of national and international agencies and industrial associations may be invited as
observers.
6. WORKING PROCEDURES
Approximately one year in advance of a meeting of a working group, the topics of the
monographs are announced and participants are selected by IARC staff in consultation with
other experts. Subsequently, relevant biological and epidemiological data are collected by
IARC from recognized sources of information on carcinogenesis, including data storage and
retrieval systems such as BIOSIS, Chemical Abstracts, CANCERLIT, MEDLINE and
TOXUNE-including EMIC and ETIC for data on genetic and related effects and
teratogenicity, respectively.
For chemicals and some compJex mixtures, the major collection of data and the
preparation of first drafts of the sections on chemical and physical properties, on analysis, on
production and use and on occurrence are carried out under a separate contract funded by
22 IARC MONOGRAPHS VOLUME 55
the US National Cancer Institute. Representatives from industrial associations may assist in
the preparation of sections on production and use. Information on production and trade is
obtained from governmental and trade publications and, in some cases, by direct contact
with industries. Separate production data on some agents may not be available because their
publication could disclose confidential information. Information on uses may be obtained
from published sources but is often complemented by direct contact with manufacturers.
Efforts are made to supplement this information with data from other national and
international sources.
Six months before the meeting, the material obtained is sent to meeting participants, or
is used by IARC staff, to prepare sections for the first drafts of monographs. The first drafts
are compiled by IARC staff and sent, prior to the meeting, to all participants of the Working
Group for review.
The Working Group meets in Lyon for seven to eight days to discuss and finalize the texts
of the monographs and to formulate the evaluations. After the meeting, the master copy of
each monograph is verified by consulting the original literature, edited and prepared for
publication. The aim is to publish monographs within nine months of the Working Group
meeting.
The available studies are summarized by the Working Group, with particular regard to
the qualitative aspects discussed below. In general, numerical findings are indicated as they
appear in the original report; units are converted when necessary for easier comparison. The
Working Group may conduct additional analyses of the published data.and use them in their
assessment of the evidence; the results of such supplementary analyses are given in square
brackets. When an important aspect of a study, directly impinging on its interpretation,
should be brought to the attention of the reader, a comment is given in square brackets.
7. EXPOSURE DATA
Sections that indicate the extent of past and present human exposure, the sources of
exposure, the people most likely to be exposed and the factors that contribute to the exposure
are included at the beginning of each monograph.
Most monographs on individual chemicals, groups of chemicals or complex mixtures
include sections on chemical and physical data, on analysis, on production and use and on
occurrence. In monographs on, for example, physical agents, biological factors, occupational
exposures and cultural habits, other sections may be included, such as: historical pers-
pectives, description of an industry or habit, chemistry of the complex mixture or taxonomy.
For chemical exposures, the Chemical Abstracts Services Registry Number, the latest
Chemical Abstracts Primary Name and the IUPAC Systematic Name are recorded; other
synonyms are given, but the list is not necessarily comprehensive. For biological agents,
taxonomy and structure are described, and the degree of variability is given, when applicable.
Information on chemical and physical properties and, in particular, data relevant to
identification, occurrence and biological activity are included. For biological agents, mode of
replication, life cycle, target cells, persistence and latency, host response and description of
nonmalignant disease caused by them are given. A description of technical products of
chemicals includes trades names, relevant specifications and available information on
.._ ______________ - - - - - - - - ------
----
PREAMBLE 23
composition and impurities. Some of the trade names given may be those of mixtures in
which the agent being evaluated is only one of the ingredients.
The purpose of the section on analysis is to give the reader an overview of current
methods, with emphasis on those widely used for regulatory purposes. Methods for moni-
toring human exposure are also given, when available. No critical evaluation or recommen-
dation of any of the methods is meant or implied. The !ARC publishes a series of volumes,
Environmental Carcinogens: Methods of Analysis and Exposure Measurement (IARC, 1978-
91), that describe validated methods for analysing a wide variety of chemicals and mixtures.
For biological agents, methods of detection and exposure assessment are described, inclu-
ding their sensitivity, specificity and reproducibility.
The dates of first synthesis and of first commercial production of a chemical or mixture
are provided; for agents which do not occur naturally, this information may allow a reaso-
nable estimate to be made of the date before which no human exposure to the agent could
have occurred. The dates of first reported occurrence of an exposure are also provided. In
addition, methods of synthesis used in past and present commercial production and different
methods of production which may give rise to different impurities are described.
Data on production, international trade and uses are obtained for representative
regions, which usually include Europe, Japan and the USA It should not, however, be
inferred that those areas or nations are necessarily the sole or major sources or users of the
agent. Some identified uses may not be current or major applications, and the coverage is not
necessarily comprehensive. In the case of drugs, mention of their therapeutic uses does not
necessarily represent current practice nor does it imply judgement as to their therapeutic
efficacy.
Information on the occurrence of an agent or mixture in the environment is obtained
from data derived from the monitoring and surveillance of levels in occupational envi-
ronments, air, water, soil, foods and animal and human tissues. When available, data on the
generation, persistence and bioaccumulation of the agent are also included. In the case of
mixtures, industries, occupations or processes, information is given about all agents present.
For processes, industries and occupations, a historical description is also given, noting
variations in chemical composition, physical properties and levels of occupational exposure
with time. For biological agents, the epidemiology of infection is described.
Statements concerning regulations and guidelines (e.g., pesticide registrations, maximal
levels pennitted in foods, occupational exposure limits) are included for some countries as
indications of potential exposures, but they may not reflect the most recent situation, since
such limits are continuously reviewed and modified. The absence of information on regula-
tory status for a country should not be taken to imply that that country does not have
regulations with regard to the exposure. For biological agents, legislation and control,
including vaccines and therapy, are described.
8. EVIDENCE FOR CARCINOGENICI1Y IN HUMANS
(a) Types of studies considered
Three types of epidemiological studies of cancer contribute to the assessment of carcino-
genicity in humans-cohort studies, case-control studies and correlation studies. Rarely,
24 IARC MONOGRAPHS VOLUME 55
results from randomized trials may be available. Case reports of cancer in humans may also
be reviewed.
Cohort and case-control studies relate individual exposures under study to the occur-
rence of cancer in individuals and provide an estimate of relative risk (ratio of incidence in
those exposed to incidence in those not exposed) as the main measure of association.
In correlation studies, the units of investigation are usually whole populations (e.g., in
particular geographical areas or at particular times), and cancer frequency is related to a
summary measure of the exposure of the population to the agent, mixture or exposure
circumstance under study. Because individual exposure is not documented, however, a causal
relationship is less easy to infer from correlation studies than from cohort and case-control
studies. Case reports generally arise from a suspicion, based on clinical experience, that the
concurrence of two events- that is, a particular exposure and occurrence of a cancer-has
happened rather more frequently than would be expected by chance. Case reports usually
lack complete ascertainment of cases in any population, definition or enumeration of the
population at risk and estimation of the expected number of cases in the absence of exposure.
The uncertainties surrounding interpretation of case reports and correlation studies make
them inadequate, except in rare instances, to form the sole basis for inferring a causal
relationship. When taken together with case- control and cohort studies, however, relevant
case reports or correlation studies may add materially to the judgement that a causal
relationship is present.
Epidemiological studies of benign neoplasms, presumed preneoplastic lesions and other
end-points thought to be relevant to cancer are also reviewed by working groups. They may,
in some instances, strengthen inferences drawn from studies of cancer itself.
(b) Quality of studies considered
The Monographs are not intended to summarize all published studies. Those that are
judged to be inadequate or irrelevant to the evaluation are generally omitted. They may be
mentioned briefly, particularly when the information is considered to be a useful supplement
to that in other reports or when they provide the only data available. Their inclusion does not
imply acceptance of the adequacy of the study design or of the analysis and interpretation of
the results, and limitations are clearly outlined in square brackets at the end of the study
description.
It is necessary to take into account the possible roles of bias, confounding and chance in
the interpretation of epidemiological studies. By 'bias' is meant the operation of factors -in
study design or execution that lead erroneously to a stronger or weaker association than in
fact exists between disease and an agent, mixture or exposure circumstance. By 'confounding'
is meant a situation in which the relationship with disease is made to appear stronger or to
appear weaker than it truly is as a result of an association between the apparent causal factor
and another factor that is associated with either an increase or decrease in the incidence of
the disease. In evaluating the extent to which these factors have been minimized in an
individual study, working groups consider a number of aspects of design and analysis as
described in the report of the study. Most of these considerations apply equally to
case-control, cohort and correlation studies. Lack of clarity of any of these aspects in the
L---------------- - ---
PREAMBLE 25
reporting of a study can decrease its credibility and the weight given to it in the final
evaluation of the exposure.
Firstly, the study population, disease (or diseases) and exposure should have been well
defined by the authors. Cases of disease in the study population should have been identified
in a way that was independent of the exposure of interest, and exposure should have been
assessed in a way that was not related to disease status.
Secondly, the authors should have taken account in the study design and analysis of other
variables that can influence the risk of disease and may have been related to the exposure of
interest. Potential confounding by such variables should have been dealt with either in the
design of the study, such as by matching, or in the analysis, by statistical adjustment. In cohort
studies, comparisons with local rates of disease may be more appropriate than those with
national rates. Internal comparisons of disease frequency among individuals at different
levels of exposure should also have been made in the study.
Thirdly, the authors should have reported the basic data on which the condusions are
founded, even if sophisticated statistical analyses were employed. At the very least, they
should have given the numbers of exposed and unexposed cases and controls in a case-
control study and the numbers of cases observed and expected in a cohort study. Further
tabulations by time since exposure began and other temporal factors are also important. In a
cohort study, data on all cancer sites and all causes of death should have been given, to reveal
the possibility of reporting bias. In a case-control study, the effects of investigated factors
other than the exposure of interest should have been reported.
Finally, the statistical methods used to obtain estimates of relative risk, absolute rates of
cancer, confidence intervals and significance tests, and to adjust for confounding should have
been clearly stated by the authors. The methods used should preferably have been the
generally accepted techniques that have been refined since the mid-1970s. These methods
have been reviewed for case-control studies (Breslow & Day, 1980) and for cohort studies
(Breslow & Day, 1987).
(c) Inferences about mechanism of action
Detailed analyses of both relative and absolute risks in relation to temporal variables,
such as age at first exposure, time since first exposure, duration of exposure, cumulative
exposure and time since exposure ceased, are reviewed and summarized when available. The
analysis of temporal relationships can be useful in f9rmulating models of carcinogenesis. In
particular, such analyses may suggest whether a carcinogen acts early or late in the process of
carcinogenesis, although at best they allow only indirect inferences about the mechanism of
aCtion. Special attention is given to measurements of biological markers of carcinogen
exposure or action, such as DNA or protein adducts, as well as markers of early steps in the
carcinogenic process, such as proto-oncogene mutation, when these are incorporated into
epidemiological studies focused on cancer incidence or mortality. Such measurements may
allow inferences to be made about putative mechanisms of action (IARC, 199la; Vainio et al.,
1992).
(d) Criteria for causality
After the quality of individual epidemiological studies of cancer has been summarized
and assessed, a judgement is made concerning the strength of evidence that the agent,
26 IARC MONOGRAPHS VOLUME 55
mixture or exposure circumstance in question is carcinogenic for humans. In making their
judgement, the Working Group considers several criteria for causality. A strong association
(i.e., a large relative risk) is more likely to indicate causality than a weak association,
although it is recognized that relative risks of small magnitude do not imply lack of causality
and may be important if the disease is common. Associations that are replicated in several
studies of the same design or using different epidemiological approaches or under different
circumstances of exposure are more likely to represent a causal relationship than isolated
observations from single studies. If there are inconsistent results among investigations,
possible reasons are sought (such as differences in amount of exposure), and results of studies
judged to be of high quality are given more weight than those from studies judged to be
methodologically less sound. When suspicion of carcinogenicity arises largely from a single
study, these data are not combined with those from later studies in any subsequent
reassessment of the strength of the evidence.
If the risk of the disease in question increases with the amount of exposure, this is
considered to be a strong indication of causality, although absence of a graded response is
not necessarily evidence against a causal relationship. Demonstration of a decline in risk
after cessation of or reduction in exposure in individuals or in whole populations also
supports a causal interpretation of the findings.
Although a carcinogen may act upon more than one target, the specificity of an asso-
ciation (i.e., an increased occurrence of cancer at one anatomical site or of one morpho-
logical type) adds plausibility to a causal relationship, particularly when excess cancer
occurrence is limited to one morphological type within the same organ.
Although rarely available, results from randomized trials showing different rates among
exposed and unexposed individuals provide particularly strong evidence for causality.
When several epidemiological studies show little or no indication of an association
between an exposure and cancer, the judgement may be made that, in the aggregate, they
show evidence of lack of carcinogenicity. Such a judgement requires first of an that the
studies giving rise to it meet, to a sufficient degree, the standards of design and analysis
described above. Specifically, the possibility that bias, confounding or misclassification of
exposure or outcome could explain the observed results should be considered and excluded
with reasonable certainty. In addi.tion, all studies that are judged to be methodologically
sound should be consistent with a relative risk ofunityfor any observed level of exposure and,
when considered together, should provide a pooled estimate of relative risk which is "at or
near unity and has a narrow confidence interval , due to sufficient population size. Moreover,
no individual study nor the pooled results of all the studies should show any consistent
tendency for relative risk of cancer to increase with increasing level of exposure. It is
important to note that evidence of lack of carcinogenicity obtained in this way from several
epidemiological studies cap. apply only to the type(s) of cancer studied and to dose levels and
intervals between first exposure and observation of disease that are the same as or less than
those observed in all the studies. Experience with human cancer indicates that, in some cases,
the period from first exposure to the development of clinical cancer is seldom less than 20
years; latent periods substantially shorter than 30 years cannot provide evidence for lack of
carcinogenicity.
PREAMBLE 27
9. STUDIES OF CANCER IN EXPERIMENTAL ANIMALS
For several agents (e.g., aflatoxins, 4-aminobiphenyl, bis(chloromethyl)ether, diethyl-
stilboestrol, melphalan, 8-methoxypsoralen (methoxsalen) plus ultraviolet radiation, mus-
tard gas and vinyl chloride), evidence of carcinogenicity in experimental animals preceded
evidence obtained from epidemiological studies or case reports. Information compiled from
the first 41 volumes of the IARC Monographs (Wilbourn et al. , 1986) shows that, of the 44
agents and mixtures for which there is sufficient or limited evidence of carcinogenicity to
humans (seep. 32), all37 that have been tested adequately produce cancer in at least one
animal species. Although this association cannot establish that all agents and mixtures that
cause cancer in experimental animals also cause cancer in humans, nevertheless, in the
absence or adequate data on humans, it is biologically plausible and prudent to regard
agents and mixtures for which there is sufficient evidence (see p. 33) of carcinogenicity in
experimental animals as if they presented a carcinogenic risk to humans. The possibility that
a given agent may cause cancer through a species-specific mechanism which does not operate
in humans (see p. 34) should also be taken into consideration.
The nature and extent of impurities or contaminants present in the chemical or mixture
being evaluated are given when available. Animal strain, sex, numbers per group, age at start
of treatment and survival are reported.
Other types of studies summarized include: experiments in which the agent or mixture
was administered in conjunction with known carcinogens or factors that modify carcinogenic
effects; studies in which the end-point was not cancer but a defined precancerous lesion; and
experiments on the carcinogenicity of known metabolites and derivatives.
For experimental studies of mixtures, consideration is given to the possibility of changes
in the physicochemical properties of the test substance during coJlection, storage, extraction,
concentration and delivery. Chemical and toxicological interactions of the components of
mixtures may result in nonlinear dose-response relationships.
An assessment is made as to the relevance to human exposure of samples tested in
experimental systems, which may involve consideration of: (i) physical and chemical charac-
teristics, (ii) constituent substances that indicate the presence of a class of substances, (iii) the
results of tests for genetic and related effects, including genetic activity profiles, DNA adduct
profiles, proto-oncogene mutation and expression and suppressor gene inactivation. The
relevance of results obtained with viral strains analogous to that being evaluated in the
monograph must also be considered.
(a) Qualitative aspects
An assessment of carcinogenicity involves several considerations of qualitative im-
portance, including (i) the experimental conditions under which the test was performed,
including route and schedule of exposure, species, strain, sex, age, duration of follow-up;
(ii) the consistency of the results, for example, across species and target organ(s); (iii) the
spectrum of neoplastic response, from preneoplastic lesions and benign tumours to mali-
gnant neoplasms; and (iv) the possible role of modifying factors.
As mentioned earlier (p. 21}, the Monographs are not intended to summarize all
published studies. Those studies in experimental animals that are inadequate (e.g., too short
a duration, too few animals, poor survival; see below) or are judged irrelevant to the
28 IARC MONOGRAPHS VOLUME 55
evaluation are generally omitted. Guidelines for conducting adequate long-term carcino-
genicity experiments have been outlined (e.g., Montesano et a/. , 1986).
Considerations of importance to the Working Group in the interpretation and eva-
luation of a particular study include: (i) how clearly the agent was defined and, in the case of
mixtures, how adequately the sample characterization was reported; (ii) whether the dose
was adequately monitored, particularly in inhalation experiments; (iii) whether the doses and
duration of treatment were appropriate and whether the survival of treated animals was
similar to that of controls; (iv) whether there were adequate numbers of animals per group;
(v) whether animals of both sexes were used; (vi) whether animals were allocated randomly to
groups; (vii) whether the duration of observation was adequate; and (viii) whether the data
were adequately reported. If available, recent data on the incidence of specific tumours in
historical controls, as well as in concurrent controls, should be taken into account in the
evaluation of tumour response.
When benign tumours occur together with and originate from the same cell type in an
organ or tissue as malignant tumours in a particular study and appear to represent a stage in
the progression to malignancy, it may be valid to combine them in assessing tumour inci-
dence (Huff eta/., 1989). The occurrence of lesions presumed to be preneoplastic may in
certain instances aid in assessing the biological plausibility of any neoplastic response
observed. If an agent or mixture induces only benign neoplasms that appear to be end-points
that do not readily undergo transition to malignancy, it should nevertheless be suspected of
being a carcinogen and it requires further investigation.
(b) Quantitative aspects
The probability that tumours will occur may depend on the species, sex, strain and age of
the animal, the dose of the carcinogen and the route and length of exposure. Evidence of an
increased incidence of neoplasms with increased level of exposure strengthens the inference
of a causal association between the exposure and the development of neoplasms.
The form of the dose-response relationship can vary widely, depending on the particular
agent under study and the target organ. Since many chemicals require metabolic activation
before being converted into their reactive intermediates, both metabolic and pharmaco-
kinetic aspects are important in determining the dose-response pattern. Saturation of steps
such as absorption, activation, inactivation and elimination may produce nonlinearity in the
dose-response relationship, as could saturation of processes such as DNA repair (Hoe] et al.,
1983; Gart et al . 1986).
(c) Statistical analysis of long-term experiments in animals
Factors considered by the Working Group include the adequacy of the information given
for each treatment group: (i) the number of animals studied and the number examined
histologically, (ii) the number of animals with a given tumour type and (iii) length of survival.
The statistical methods used should be clearly stated and should be the generally accepted
techniques refined for this purpose (Peto eta/. , 1980; Gart eta/., 1986). When there is no
difference in survival between control and treatment groups, the Working Group usually
compares the proportions of animals developing each tumour type in each of the groups.
Otherwise, consideration is given as to whether or not appropriate adjustments have been
- - ---------------- - - - - - - - -
PREAMBLE 29
made for differences in survival. These adjustments can include: comparisons of the
proportions of tumour-bearing animals among the effective number of animals (alive at the
time the first tumour is discovered), in the case where most differences in survival occur
before tumours appear; life-table methods, when tumours are visible or when they may be
considered 'fatal' because mortality rapidly follows tumour development; .and the Mantel-
Haenszel test or logistic regression, when occult tumours do not affect the animals' risk of
dying but are 'incidental' findings at autopsy.
In practice, classifying tumours as fatal or incidental may be difficult. Several survival-
adjusted methods have been developed that do not require this distinction (Gart et al., 1986),
although they have not been fully evaluated.
10. OTHER RELEVANT DATA
(a) Absorption, distribution, metabolism and excretion
Concise information is given on absorption, distribution (including placental transfer)
and excretion in both humans and experimental animals. Kinetic factors that may affect the
dose-response relationship, such as saturation of uptake, protein binding, metabolic activa-
tion, detoxification and DNA repair processes, are mentioned. Studies that indicate the
metabolic fate of the agent in humans and in experimental animals are summarized briefly,
and comparisons of data from humans and animals are made when possible. Comparative
information on the relationship between exposure and the dose that reaches the target site
may be of particular importance for extrapolation between species.
(b) Toxic effects
Data are given on acute and chronic toxic effects (other than cancer), such as organ
toxicity, increased cell proliferation, immunotoxicity and endocrine effects. The presence
and toxicological significance of cellular receptors is described.
(c) Reproductive and developmental effects
Effects on reproduction, teratogenicity, fetotoxicity and embryotoxicity are also sum-
marized briefly.
(d) Genetic and related effects
Thsts of genetic and related effects are described in view of the relevance of gene
mutation and chromosomal damage to carcinogenesis (Vainio eta/., 1992).
The adequacy of the reporting of sample characterization is considered and, where
necessary, commented upon; with regard to complex mixtures, such comments are similar to
those described for animal carcinogenicity tests on p. 28. The available data are interpreted
critically by phylogenetic group according to the end-points detected, which may incJude
DNA damage, gene mutation, sister chroJTlatid exchange, micronucleus formation, chromo-
somal aberrations, aneuploidy and celJ 1 msformation. The concentrations employed are
given, and mention is made of whether use of an exogenous metabolic system affected the
test result. These data are given as listings of test systems, data and references; bar graphs
(activity -profiles) and corresponding summary tables with detailed information on the
preparation of the profiles (Waters et a/., 1987) are given in appendices.
30 IARC MONOGRAPHS VOLUME 55
Positive results in tests using prokaryotes, lower eukaryotes, plants, insects and cultured
mammalian cells suggest that genetic and related effects could occur in mammals. Results
from such tests may also give information about the types of genetic effect produced and
about the involvement of metabolic activation. Some end-points described are clearly
genetic in nature (e.g., gene mutations and chromosomal aberrations), while others are to a
greater or lesser degree associated with genetic effects (e.g., unscheduled DNA synthesis).
In-vitro tests for tumour-promoting activity and for cell transformation may be sensitive to
changes that are not necessarily the result of genetic alterations but that may have specific
relevance to the process of carcinogenesis. A critical appraisal of these tests has been
published (Montesano et al., 1986).
Genetic or other activity manifest in experimental mammals and humans is regarded as
being of greater relevance than that in other organisms. The demonstration that an agent or
mixture can induce gene and chromosomal mutations in whole mammals indicates that it
may have carcinogenic activity, although this activity may not be detectably expressed in any
or all species. Relative potency in tests for mutagenicity and related effects is not a reliable
indicator of carcinogenic potency. Negative results in tests for mutagenicity in selected
tissues from animals treated in vivo provide less weight, partly because they do not exclude
the possibility of an effect in tissues other than those examined. Moreover, negative results in
short-term tests with genetic end-points cannot be considered to provide evidence to rule out
carcinogenicity of agents or mixtures that act through other mechanisms (e.g., receptor
mediated effects, cellular toxicity with regenerative proliferation, peroxisome proliferation)
(Vainio et al., 1992). Factors that may lead to misleading results in short-term tests have been
discussed in detail elsewhere (Montesano eta!., 1986).
When available, data relevant to mechanisms of carcinogenesis that do not involve
structural changes at the level of the gene are also described.
The adequacy of epidemiological studies of reproductive outcome and genetic and
related effects in humans is evaluated by the same criteria as are applied to epidemiological
studies of cancer.
(e) Structure-activity considerations
This section describes structure-activity relationships that may be relevant to an evalua-
tion of the carcinogenicity of an agent.
11. SUMMARY OF DATA REPORTED
In this section, the relevant epidemiological and experimental data are summarized.
Only reports, other than in abstract form, that meet the criteria outlined on p. 21 are
considered for evaluating carcinogenicity. Inadequate studies are generally not summarized:
such studies are usually identified by a square-bracketed comment in the preceding text.
(a) Exposures
Human exposure is summarized on the basis of elements such as production, use,
occurrence in the environment and determinations in human tissues and body fluids.
Quantitative data are given when available.
PREAMBLE 31
(b) Carcinogenicity in humans
Results of epidemiological studies that are considered to be pertinent to an assessment
of human carcinogenicity are summarized. When relevant, case reports and correlation
studies are also summarized.
(c) Carcinogenicity in experimental animals
Data relevant to an evaluation of carcinogenicity in animals are summarized. For each
animal species and route of administration, it is stated whether an increased incidence of
neoplasms or preneoplastic lesions was observed, and the tumour sites are indicated. If the
agent or mixture produced tumours after prenatal exposure or in singledose experiments,
this is also indicated. Negative findings are also summarized. Dose-response and other
quantitative data may be given when available.
(d) Other data relevant to an evaluation of carcinogenicity and its mechanisms
Data on biological effects in humans are of particular relevance are summarized.
These may include toxicological, kinetic and metabolic considerations and evidence of DNA
binding, persistence of DNA lesions or genetic damage in exposed .humans. Toxicological
information, such as that on cytotoxicity and regeneration, receptor binding and hormonal
and immunological effects, and data on kinetics and metabolism in experimental animals are
given when considered relevant to the possible mechanism of the carcinogenic action of the
agent. The results of tests for genetic and related effects are summarized for whole mammals,
cultured mammalian cells and nonmammalian systems.
When available, comparisons of such data for humans and for animals, and particularly
animals that have developed cancer, are described.
Structure-activity relationships are mentioned when relevant.
For the agent, mixture or exposure circumstance being evaluated, the available data on
end-points or other phenomena relevant to mechanisms of carcinogenesis from studies in
humans, experimental animals and tissue and cell test systems are summarized within one or
more of the following descriptive dimensions:
(i) Evidence of genotoxicity (i.e., structural changes at the level of the gene): for
example, structure-activity considerations, adduct formation, mutagenicity (effect on speci-
fic genes), chromosomal mutation/aneuploidy
(ii) Evidence of effects on the expression of relevant genes (i.e., functional changes at
the intracellular level): for example, alterations to the structure or quantity of the product of
a proto-oncogene or tumour suppressor gene, alterations to metabolic activation/inacti-
vation/DNA repair
(iii) Evidence of relevant effects on cell behaviour (i.e . morphological or behavioural
changes at the cellular or tissue level): for example, induction of mitogenesis, compensatory
cell proliferation, preneoplasia and hyperplasia, survival of premalignant or malignant cells
(immortalization, immunosuppression), effects on metastatic potential
(iv) Evidence from dose and time relationships of carcinogenic effects and interactions
between agents: for example, early/late stage, as inferred from epidemiological studies;
initiation/promotion/progression/malignant as defined in animal carcinogeni-
city experiments; toxicokinetics
32 IARC MONOGRAPHS VOLUME 55
These dimensions are not mutually exclusive, and an agent may fall within more than one
of them. Thus, for example, the action of an agent on the expression of relevant genes could
be summarized under both the first and second dimension, even if it were known with
reasonable certainty that those effects resulted from genotoxicity.
12. EVALUATION
Evaluations of the strength of the evidence for carcinogenicity arising from human and
experimental animal data are made, using standard terms.
It is recognized that the criteria for these evaluations, described below, cannot
encompass all of the factors that may be relevant to an evaluation of carcinogenicity. In
considering all of the relevant data, the Working Group may assign the agent, mixture or
exposure circumstance to a higher or lower category than a strict interpretation of these
criteria would indicate.
(a) Degrees of evidence for carcinogenicity in humans and in experimental animals and
supporting evidence
These categories refer only to the strength of the evidence that an exposure is carcino-
genic and not to the extent of its carcinogenic activity (potency) nor to the mechanisms
involved. A classification may change as new information becomes available.
An evaluation of degree of evidence, whether for a single agent or a mixture, is limited to
the materials tested, as defined physically, chemically or biologically. When the agents
evaluated are considered by the Working Group to be sufficiently closely related, they may
be grouped together for the purpose of a single evaluation of degree of evidence.
(i) Carcinogenicity in humans
The applicability of an evaluation of the carcinogenicity of a mixture, process, occu-
pation or industry on the basis of evidence from epidemiological studies depends on the
variability over time and place of the mixtures, processes, occupations and industries. The
Working Group seeks to identify the specific exposure, process or activity which is considered
most likely to be responsible for any excess risk. The evaluation is focused as narrowly as the
available data on exposure and other aspects permit.
The evidence relevant to carcinogenicity from studies in humans is classified into one of
the following categories:
Sufficient evidence of carcinogenicity: The Working Group considers that a causal
relationship has been established between exposure to the agent, mixture or exposure
circumstance and human canGer. That is, a positive relationship has been observed between
the exposure and cancer in studies in which chance, bias and confounding could be ruled out
with reasonable confidence.
Limited evidence of carcinogenicity: A positive association has been observed between
exposure to the agent, mixture or exposure circumstance and cancer for which a causal
interpretation is considered by the Working Group to be credible, but chance, bias or
confounding could not be ruled out with reasonable confidence.
----------- ------- - - - -- --
PREAMBLE 33
Inadequate evidence of carcinogenicity: The available studies are of insufficient quality,
consistency or statistical power to permit a conclusion regarding the presence or absence of a
causal association, or no data on cancer in humans are available.
Evidence suggesting lack of carcinogenicity: There are several adequate studies covering
the full range of levels of exposure that human beings are known to encounter, which are
mutually consistent in not showing a positive association between exposure to the agent,
mixture or exposure circumstance and any studied cancer at any observed level of exposure.
A conclusion of 'evidence suggesting lack of carcinogenicity' is inevitably limited to the
cancer sites, conditions and levels of exposure and length of observation covered by the
available studies. In addition, the possibility of a very small risk at the levels of exposure
studied can never be excluded.
In some instances, the above categories may be used to classify the degree of evidence
related to carcinogenicity in specific organs or tissues.
(ii) Carcinogenicity in experimental animals
The evidence relevant to carcinogenicity in experimental animals is classified into one of
the following categories:
Sufficient evidence of carcinogenicity: The Working Group considers that a causal
relationship has been established between the agent or mixture and an increased incidence of
malignant neoplasms or of an appropriate combination of benign and malignant neoplasms
in (a) two or more species of animals or (b) in two or more independent studies in one species
carried out at different times or in different laboratories or under different protocols.
Exceptionally, a single study in one species might be considered to provide sufficient
evidence of carcinogenicity when malignant neoplasms occur to an unusual degree with
regard to incidence, site, type of tumour or age at onset.
Limited evidence of carcinogenicity: The data suggest a carcinogenic effect but are limited
for making a definitive evaluation because, e.g., (a) the evidence of carcinogenicity is
restricted to a single experiment; or (b) there are unresolved questions regarding the
adequacy of the design, conduct or interpretation of the study; or (c) the agent or mixture
increases the incidence only of benign neoplasms or lesions of uncertain neoplastic potential,
or of certain neoplasms which may occur spontaneously in high incidences in certain strains.
Inadequate evidence of carcinogenicity: The studies cannot be interpreted as showing
either the presence or absence of a carcinogenic effect because of major qualitative or quan-
titative limitations, or no data on cancer in experimental animals are available.
Evidence suggesting lack of carcinogenicity: Adequate studies involving at least two
species are available which show that, within the limits of the tests used, the agent or mixture
is not carcinogenic. A conclusion of evidence suggesting lack of carcinogenicity is inevitably
limited to the species, tumour sites and levels of exposure studied.
(b) Other data relevant to an evaluation of carcinogenicity
Other evidence judged to be relevant to an evaluation of carcinogenicity and of
sufficient importance to affect the overall evaluation is then described. This may include data
on preneoplastic lesions, tumour pathology, genetic and related effects, structure-activity
relationships, metabolism and and physicochemical parameters.
34 IARC MONOGRAPHS VOLUME 55
Data relevant to mechanisms of the carcinogenic action are also evaluated. The strength
of the evidence that any carcinogenic effect observed is due to a particular mechanism is
assessed, using terms such as weak, moderate or strong. Then, the Working Group assesses if
that particular mechanism is likely to be operative in humans. The strongest indications that
a particular mechanism operates in humans come from data on humans or biological
specimens obtained from exposed humans. The data may be considered to be especially
relevant if they show that the agent in question has caused changes in exposed humans that
are on the causal pathway to carcinogenesis. Such data may, however, never become
available. because it is at least conceivable that certain compounds may be kept from human
use solely on the basis of evidence of their toxicity and/or carcinogenicity in experimental
systems.
For complex exposures, including occupational and industrial exposures, chemical com-
position and the potential contribution of carcinogens known to be present are considered by
the Working Group in its overall evaluation of human carcinogenicity. The Working Group
also determines the extent to which the materials tested in experimental systems are related
to those to which humans are exposed.
(c) Overall evaluation
Finally, the body of evidence is considered as a whole, in order to reach an overall eval-
uation of the carcinogenicity to humans of an agent, mixture or circumstance of exposure.
An evaluation may be made for a group of chemical compounds that have been eval-
uated by the Working Group. In addition, when supporting data indicate that other, related
compounds for which there is no direct evidence of capacity to induce cancer in humans or in
animals may also be carcinogenic, a statement describing the rationale for this conclusion is
added to the evaluation narrative; an additional evaluation may be made for this broader
group of compounds if the strength of the evidence warrants it.
The agent, mixture or exposure circumstance is described according to the wording of
one of the following categories, and the designated group is given. The categorization of an
agent, mixture or exposure circumstance is a matter of scientific judgement, reflecting the
strength of the evidence derived from studies in humans and in experimental animals and
from other relevant data.
Group 1- The agent (mixture) is carcinogenic to humans.
The exposure circumstance entails exposures that are carcinogenic to humans.
This category is used when there is sufficient evidence of carcinogenicity in humans.
Exceptionally, an agent (mixture) may be placed in this category when evidence in humans is
less than sufficient but there is sufficient evidence of carcinogenicity in experimental animals
and strong evidence in exposed humans that the agent (mixture) acts through a relevant
mechanism of carcinogenicity.
Group 2
This category includes agents, mixtures and exposure circumstances for which, at one
extreme, the degree of evidence of carcinogenicity in humans is almost sufficient, as well as
those for which, at the other extreme, there are no human data but for which there is evidence
of carcinogenicity in experimental animals. Agents, mixtures and exposure circumstances are
PREAMBLE 35
assigned to either group 2A (probably carcinogenic to humans) or group 2B (possibly
carcinogenic to humans) on the basis of epidemiological and experimental evidence of
carcinogenicity and other relevant data.
Group 2A-The agent (mixture) is probably carcinogenic to humans.
The exposure circumstance entails exposures that are probably carcinogenic to humans.
This category is used when there is limited evidence of carcinogenicity in humans and
sufficient evidence of carcinogenicity in experimental animals. In some cases, an agent
(mixture) may be classified in this category when there is inadequate evidence of carcino-
genicity in humans and sufficient evidence of carcinogenicity in experimental animals and
strong evidence that the carcinogenesis is mediated by a mechanism that also operates in
humans. Exceptionally, an agent, mixture or exposure circumstance may be classified in this
category solely on the basis of limited evidence of carcinogenicity in humans.
Group 2B-The agent (mixture) is possibly carcinogenic to humans.
The exposure circumstance entails exposures that are possibly carcinogenic to humans.
This category is used for agents, mixtures and exposure circumstances for which there is
limited evidence of carcinogenicity in humans and less than sufficient evidence of carcino-
genicity in experimental animals. It may also be used when there is inadequate evidence of
carcinogenicity in humans but there is sufficient evidence of carcinogenicity in experimental
animals. In some instances, an agent, mixture or exposure circumstance for which there is
inadequate evidence of carcinogenicity in humans but limited evidence of carcinogenicity in
experimental animals together with supporting evidence from other relevant data may be
placed in this group.
Group 3-The agent (mixture or exposure circumstance) is not classifiable as to its carcino-
genicity to humans.
This category is used most commonly for agents, mixtures and exposure circumstances
for which the evidence of carcinogenicity is inadequate in humans and inadequate or limited
in experimental animals.
Exceptionally, agents (mixtures) for which the evidence of carcinogenicity is inadequate
in humans but sufficient in experimental animals may be placed in this category when there is
strong evidence that the mechanism of carcinogenicity in experimental animals does not
operate in humans.
Agents, mixtures and exposure circumstances that do not fall into any other group are
also placed in this category.
Group 4-The agent (mixture) is probably not carcinogenic to humans.
This category is used for agents or mixtures for which there is evidence suggesting lack of
carcinogenicity in humans and in experimental animals. In some instances, agents or mixtures
for which there is inadequate evidence of carcinogenicity in humans but evidence suggesting
lack of carcinogenicity in experimental animals, consistently and strongly supported by a
broad range of other relevant data, may be classified in this group.
36
IARC MONOGRAPHS VOLUME 55
References
Breslow, N.E. & Day, N.E. (1980) Statistical Methods in Cancer Research, Vol. 1. The Analysis of Case-
control Studies (!ARC Scientific Publications No. 32), Lyon, IARC
Breslow, N.E. & Day, N.E. (1987) Statistical Methods in Cancer Research, Vol. 2, The Design and
Analysis of Cohort Studies (IARC Scientific Publications No. 82), Lyon, !ARC
Gart, J.J., Krewski, D., Lee, P.N., Tarone, R.E. & Wahrendorf, J. (1986) Statistical Methods in Cancer
Research, Vol. 3, The Design and Analysis of Long-term Animal Expenments (IARC Scientific
Publications No. 79), Lyon, !ARC
Hoe!, D.G., Kaplan, N.L. & Anderson, M.W. (1983) Implication of nonlinear kinetics on risk
estimation in carcinogenesis. Science, 219, 1032-1037
Huff, J.E., Eustis, S.L. & Haseman, J.K. (1989) Occurrence and relevance of chemically induced
benign neoplasms in long-term carcinogenicity studies. Cancer Metastasis Rev., 8, 1-21
!ARC (1973-1990) Information Bulletin on the Survey of Chemicals Being Tested for Carcinogenicity/-
Directory of Agents Being Tested for Carcinogenicity, Numbers 1- 14, Lyon
Number 1 (1973) 52 pages
Number 2 (1973) 77 pages
Number 3 (1974) 67 pages
Number 4 (1974) 97 pages
Number 5 (1975) 88 pages
Number 6 (1976} 360 pages
Number 7 (1978) 460 pages
Number 8 (1979) 604 pages
Number 9 (1981) 294 pages
Number 10 (1983) 326 pages
Number 11 (1984) 370 pages
Number 12 (1986) 385 pages
Number 13 (1988} 404 pages
Number 14 (1990) 369 pages
!ARC (1976-1991)
Directory of On-going Research in Cancer Epidemiology 1976. Edited by C.S. Muir & G. Wagner,
Lyon
Directory of On-going Research in Cancer Epidemiology 1977 (IARC Scientific Publications
No. 17). Edited by C.S. Muir & G. Wagner, Lyon
Directory of On-going Research in Cancer Epidemiology 1978 (IARC Scientific Publications
No. 26). Edited by C.S. Muir & G. Wagner, Lyon
Directory of On-going Research in Cancer Epidemiology 1979 (IARC Scientific Publications
No. 28). Edited by C.S. Muir & G. Wagner, Lyon
Directory of On-going Research in Cancer Epidemiology 1980 (IARC Scientific Publications
No. 35). Edited by C.S. Muir & G. Wagner, Lyon
Directory of On-going Research in Cancer Epidemiology 1981 (!ARC Scientific Publications
No. 38). Edited by C.S. Muir & G. Wagner, Lyon
Directory of On-going Research in Cancer Epidemiology 1982 (!ARC Scientific Publications
No. 46). Edited by C.S. Muir & G. Wagner, Lyon
Directory of On-going Research in Cancer Epidemiology 1983 (IARC Scientific Publications
No. 50). Edited by C.S. Muir & G. Wagner, Lyon
PREAMBLE 37
Directory of On-going Research in Cancer Epidemiology 1984 (IARC Scientific Publications
No. 62). Edited by C.S. Muir & G. Wagner, Lyon
Directory of On-going Research in Cancer Epidemiology 1985 (IARC Scientific Publications
No. 69). Edited by C.S. Muir & G. Wagner, Lyon
Directory of On-going Research in Cancer Epidemiology 1986 (IARC Scientific Publications
No. 80). Edited by C.S. Muir & G. Wagner, Lyon
Directory of On-going Research in Cancer Epidemiology 1987 (IARC Scientific Publications
No. 86). Edited by D.M. Parkin & J. Wahrendorf, Lyon
Directory of On-going Research in Cancer Epidemiology 1988 (IARC Scientific Publications
No. 93). Edited by M. Coleman & J. Wahrendorf, Lyon
Directory of On-going Research in Cancer Epidemiology 1989/90 (IARC Scientific Publications
No. 101). Edited by M. Coleman & J. Wahrendorf, Lyon
Directory of On-going Research in Cancer Epidemiology 1991 (IARC Scientific Publications
No. 110). Edited by M. Coleman & J. Wahrendorf, Lyon
IARC (1977) !ARC Monographs Programme on the Evaluation of the Carcinogenic Risk of Chemicals to
Humans. Preamble (IARC intern. tech. Rep. No. 77/002), Lyon
IARC (1978) Chemicals with Sufficient Evidence of Carcinogenicity in Experimental Animals-IARC
Monographs Volumes 1-17 (IARC intern. tech. Rep. No. 78/003), Lyon
IARC (1978-1991) Environmental Carcinogens. Methods of Analysis and Exposure Measurement:
Vol. 1. Analysis ofVolatile Nitrosamines in Food (IARC Scientific Publications No. 18). Edited by
R. Preussmann, M. Castegnaro, E.A. Walker & A.E. Wasserman (1978)
Vol. 2. Methods for the Measurement of Vinyl Chloride in Poly(vinyl chloride), Air; Water and
Foodstuffs (IARC Scientific Publications No. 22). Edited by D.C.M. Squirrell & W. Thain
(1978)
Vol. 3. Analysis of Polycyclic Aromatic Hydrocarbons in Environmental Samples (IARC Scientific
Publications No. 29). Edited by M. Castegnaro, P. Bogovski, H. Kunte & E.A. Walker(1979)
Vol. 4. Some Aromatic Amines and Azo Dyes in the General and Industrial Environment (!ARC
Scientific Publications No. 40). Edited by L. Fishbein, M. Castegnaro, I.K. O'Neill & H.
Bartsch (1981)
Vol. 5. Some Mycoto.xins (IARC Scientific Publications No. 44). Edited by L. Stoloff, M.
Castegnaro, P. Scott, I.K. O'Neill & H. Bartsch (1983)
Vol. 6. N-Nitroso Compounds (IARC Scientific Publications No. 45). Edited by R. Preussmann,
I.K. O'Neill, G. Eisenbrand, B. Spiegelhalder & H. Bartsch (1983)
Vol. 7. Some Volatile Halogenated Hydrocarbons (IARC Scientific Publications No. 68). Edited by
L. Fishbein & I.K. O'Neill (1985)
Vol. 8. Some Metals: As, Be, Cd, Cr. Ni, Pb, Se, Zn (IARC Scientific Publications No. 71). Edited
by I.K. O'Neill, P. Schuller & L. Fishbein (1986)
Vol. 9. Passive Smoking (IARC Scientific Publications No. 81). Edited by I.K. O'Neill, K.D.
Brunnemann, B. Dodet & D. Hoffmann (1987)
Vol. 10. Benzene and Alkylated Benzenes (IARC Scientific Publications No. 85). Edited by L.
Fishbein & I.K. O'Neill (1988)
Vol. 11. Polychlorinated Dioxins and Dibenzofurans (IARC Scientific Publications No. 108) ..
Edited by C. Rappe, H.R. Buser, B. Dodet & I.K. O'Neill (1991)
IARC (1979) Criteria to Select Chemicals for IARC Monographs (IARC intern. tech. Rep. No. 79/003),
Lyon
38 IARC MONOGRAPHS VOLUME 55
IARC (1982) /ARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans,
Supplement 4, Chemicals, Industrial Processes and Industries Associated with Cancer in Humans
(/ARC Monographs, Volumes 1 to 29), Lyon
IARC (1983) Approaches to Classifying Chemical Carcinogens According to Mechanism of Action
(!ARC intern. tech. Rep. No. 83/001), Lyon
IARC (1984) Chemicals and Exposures to Complex Mixtures Recommended for Evaluation in IARC
Monographs and Chemicals and Complex Mixtures Recommended for Long-term Carcinogenicity
Testing (IARC intern. tech. Rep. No. 84/002), Lyon
IARC (1987a) !ARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Supplement 6,
Genetic and Related Effects: An Updating of Selected !ARC Monographs from Volumes 1 to 42,
Lyon
IARC (1987b) /ARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Supplement 7,
Overall Evaluations of Carcinogenicity: An Updating ofiARC Monographs Volumes 1 to 42, Lyon
!ARC (1988) Report of an /ARC Working Group to Review the Approaches and Processes Used to
Evaluate the Carcinogenicity of Mixtures and Groups of Chemicals (IARC intern. tech. Rep.
No. 88/002), Lyon
!ARC (1989) Chemicals, Groups of Chemicals, Mixtures and Exposure Circumstances to be Evaluated in
Future /ARC Monographs, Report of an ad hoc Working Group (!ARC intern. tech. Rep. No.
89/004), Lyon
IARC (1991a) A Consensus Report of an IARC Monographs Working Group on the Use of Mechanims
of Carcinogenesis in Risk Identification (!ARC intern. tech. Rep. No. 91/002), Lyon
!ARC (199lb) Report of an Ad-hoc !ARC Monographs Advisory Group on Viruses and Other Biological
Agents Such as Parasites (IARC intern. tech. Rep. No. 911001), Lyon
Montesano, R., Bartsch, H., Yainio, H., Wilbourn, J. & Yamasaki, H., eds (1986) Long-term and
Slwrt-term Assays for Carcinogenesis-A Critical Appraisal (IARC Scientific Publications No. 83),
Lyon, !ARC .
Peto, R., Pike, M.C., Day, N.E., Gray, R.G., Lee, P.N., Parish, S., Peto, J., Richards, S. & Wahrendorf,J.
(1980) Guidelines for simple, sensitive significance tests for carcinogenic effects in long-term
animal experiments. In: /ARC Monographs on the Evaluation of the Carcinogenic Risk of Chem-
icals to Humans, Supplement 2, Long-term and Short-term Screening Assays for Carcinogens: A
Critical Appraisal, Lyon, pp. 311-426
Vainio, H., Magee, P., McGregor, D. & McMichael, A., eds (1992) Mechanisms of Carcinogenesis in
Risk Identification (IARC Scientific Publications No. 116), Lyon, IARC
Waters, M.D., Stack, H.F., Brady, A.L., Lohman, P.H.M., Haroun, L. & Yainio, H. (1987) Apendix 1.
Activity profiles for genetic and related tests. In: !ARC Monographs on the Evaluation of
Carcinogenic Risks to Humans, Suppl. 6, Genetic and Related Effects: An Updating of Selected
!ARC Monographs from Volumes 1 to. 42, Lyon, !ARC, pp. 687-696
Wilbourn, J., Haroun, L., Heseltine, E., Kaldor, J., Partensky, C. & Yainio, H. (1986) Response of
experimental animals to human carcinogens: an analysis based upon the IARC Monographs
Programme. Carcinogenesis, 7, 1853- 1863
---------- ----- ---- -- - - -- - -
GENERAL REMARKS
This fifty-fifth volume of /ARC Monographs contains evaluations of carcinogenic risks
associated with human exposure to solar and ultraviolet (UV) radiation from medical and
cosmetic devices, general illumination and industrial sources. Ultraviolet radiation (UVR)
was considered previously (IARC, 1986) in a volume in which furocoumarins were evaluated.
Since some of these compounds are used clinically in conjunction with ultraviolet A (UVA)
radiation, information on the carcinogenic effects of UVR alone was provided in an
appendix; however, no evaluation was made at that time.
Solar radiation is largely optical radiation (UV. visible and infrared), although both
shorter wavelength (ionizing) and longer wavelength (microwaves and radiofrequency)
radiation is present. UVR lies in the interval 100-400 nm and is further subdivided into UVA
(315-400 nm), UVB (280-315 nm) and UVC (100-280 nm). The UV component of
terrestrial radiation from the sun comprises about 95% UVA and 5% UVB; UVC is removed
from extraterrestrial radiation by stratopheric ozone. Before the beginning of this century,
the sun was essentially the only source of UVR; with the advent of artificial sources, the
opportunity for additional exposure, not only to UVA and UVB but also to UVC, has
increased. It should be stressed that the distinction of UVR into UVA, UVB and UVC ranges
has no biological basis, and the potential of UVR for causing damage to biomolecules, cells,
tissues and organisms varies enormously over the spectral region from 250 to 400 nm.
UVA raqiation is one of the components of solar emissions and of emissions from
medical lamps and lamps used for cosmetic purposes. UVB radiation is present in solar
emissions, from lamps used in medicine and for cosmetic purposes and in certain lamps used
for general illumination, such as unshielded fluorescent and tungsten-halogen lamps. It
causes sunburn relatively easily and is immunosuppressive; it can cause ocular cataracts. The
possibility that the UVB component of solar radiation will increase as a result of depletion of
the ozone layer is a matter of concern. This question was not addressed in the present
volume.
Human exposure to UVC radiation is uncommon and is related to the use of germicidal
and tungsten-halogen lamps, phototherapy and welding arcs. Thus, very little is known about
the effects ofUVC on humans, although a great deal of information is available on the effects
of radiation in this range on biomolecules, cells and viruses.
In the USA. skin melanoma has been second only to lung cancer in its rate of increase in
incidence over the last 40 years: the incidence has been increasing by about 5% per year. The
major sites have been male trunk and female leg. Mortality from melanoma may now be
falling in younger generations (at least in the USA) due, possibly, to changes in sun exposure
(Scotto et al., 1991). There is also evidence that the incidence of nonmelanocytic skin cancer
is increasing in some white-skinned populations (Gallagher et al., 1990). Constitutional risk
-39-
40 IARC MONOGRAPHS VOLUME 55
factors, e.g., skin type, hair and eye colour and specific subtypes of exposure (for example,
occupational and recreational), have been assessed in individual studies or sections of the
monographs but have not been included in the evaluations.
UYR is ubiquitous and cannot be totally avoided. An appendix to this volume presents a
discussion on the use of topical sunscreens, taking into consideration both potentially
beneficial, protective effects and possible adverse reactions. The biological effects of
combinations of psoralens and UYR were not considered since these were the subjects of
separate monographs (IARC, 1980, 1986, 1987) in the !ARC Monographs series.
References
Gallagher, R.P., Ma, B., McLean, DJ., Yang, C.P., Ho, V., Carruthers, J.A. & Warshawski, L.M. (1990)
Trends in basal cell carcinoma, squamous cell carcinoma, and melanoma of the skin from 1973
through 1987. J. Am. Acad. Dermatol., 23, 413-421
IARC (1980) !ARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans,
Vol. 24, Some Pharmaceutical D r u ~ Lyon, pp. 101-124
!ARC (1986) /ARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans,
Vol. 40, Some Naturally Occurring Synthetic Food Components, Furocoumarins and Ultraviolet
Radiation, Lyon, pp. 317-371
IARC (1987) /ARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Suppl. 7, Overall
Evaluations of Carcinogenicity: An Updating of IARC Monographs Volumes 1 to 42, Lyon,
pp. 242-245
Scotto, J ., Pitcher, H. & Lee, J.A.H. (1991) Indications of future decreasing trends in skin-melanoma
mortality among whites in the United States. Int. 1. Cancer, 49, 490-497
SOLAR AND ULTRAVIOLET RADIATION
1.1 Nomenclature
1.1.1 Optical radiation
1. Exposure Data
Optical radiation is radiant energy within a broad region of the electromagnetic
spectrum that includes ultraviolet (UV), visible (light) and infrared radiation. Ultraviolet
radiation (UVR) is characterized by wavelengths between 10 and 400 nm- bordered on the
one side by x rays and on the other by visible light (Fig. 1 ). Solar .radiation is largely optical
radiation, although ionizing radiation (i.e. , cosmic rays, gamma rays and x rays, which have
wavelengths less than approximately 10 nm) and radio-frequency radiation (i.e., wavelengths
greater than 1 mm: microwaves and longer radio waves) are also present in the spectrum.
The optical radiation spectrum is generally considered to fall between 10 nm and 1 mm,
and several different conventions have been developed to describe different bands within
this spectrum. It is important to recognize that no single convention is uniquely 'correct' but
that each may be useful for a particular branch of science and technology. For example, in
optics, it is convenient to separate the spectrum into different bands on the basis of the
transmission and absorption properties of optical materials (e.g., glass and quartz). In one
optical convention, shown in Figure 1, UVR is divided into vacuum UV, extending from 10 to
180 nm; middle UV, from 180 nm to 300 nm; and near UV, from 300 nm to 380 or 400 nm.
Meteorological scientists typically define optical spectral regions on the basis of atmospheric
windows. Some spectral designations are based on uses, e.g., 'germicidal' and 'black-light'
regions.
For the purposes of this monograph, the photobiological designations of the Com-
~ s s o n Internationale de l' Eclairage (CIE, International Commission on Illumination) are
the most relevant and are used throughout to define the approximate spectral regions in
which certain biological absorption properties and biological interaction mechanisms may
dominate (Commission Internationale de l'Eclairage, 1987). The CIE bands are: UVC
(100-280 nm), UVB (280-315 nm) and UVA (315-400 nm). Visible light is the region
between 400 nm and 780 nm.
It is important to recognize that these spectral band designations are merely short-hand
notations and cannot be considered to designate fine dividing lines below which an effect is
present and above which it does not occur. The reader should also be alerted to the fact that
the CIE nomenclature is not always followed rigorously and that some authors introduce
slight variations; for example, distinguishing b.etween UVB and UVA at 320 rather than
315 nm (frequently used in the USA) and defining UVC as200-280 nm(Moseley, 1988). The
German Industrial Standard (DIN 5031) defines UVA as radiation between 315 and 380 nm
(Mutzhas, 1986).
-43-
44 IARC MONOGRAPHS VOLUME 55
Figure 1. Electromagnetic spectrum with enlargement of ultraviolet (UV) region
Visible
Violet Red
Cosmic rays, gamma rays, x rays
Ultra-
violet
Infrared Radio waves
X rays -.J
100 180
I
Vacuum UV
,
I
uvc
100
Extreme UV FarUV
300
I UVB
280 315
Black
light
UVA
Middle uv Near UV
400
400
I I
I I ,
10 100 180
Wavelength (nanometres)
Adapted from WHO (1979), Morison (1983a), Sylvania (undated)
300 380
VIsible
From the viewpoint of photochemistry and photobiology, interactions of optical
radiation with matter are considered to occur when one photon interacts with one molecule
to produce a photochemically altered molecule or two dissociated molecules (Phillips, 1983;
Smith, 1989). In any photochemical interaction, the energy of the individual photon is
important, since this must be sufficient to alter a molecular bond. The photon energy is
generally expressed in terms of electron volts (eV). A wavelength of 10 nm corresponds to a
photon energy of 124 eV, and 400 nm to an energy of 3.1 eV (WHO, 1979). The number of
altered molecules produced relative to the number of absorbed photons is referred to as the
'quantum yield' (Phillips, 1983). The efficacy of photochemical interaction per incident
quantum and the photobiological effects per unit radiant exposure typically vary widely with
wavelength. A quantitative plot of such spectral variation, usualJy normalized to unity at the
most effective wavelength, is referred to as an 'action spectrum' (Jagger, 1985).
- - --- - - - - -
EXPOSURE DATA 45
1.1.2 Quantities and units
1\vo systems of quantities and units are used to describe the characteristics of light and
light sources: the radiometric and the photometric systems. Radiometry can be applied to all
optical sources and to all exposures to optical radiation (including solar radiation and UVR).
Photometry can be used only to describe visible light sources, and photometric quantities are
used in illumination engineering. The basic photometric unit is the lumen, which is defined in
terms ofthe spectral response of the human eye (specifically, the spectral response ofthe CIE
'standard observer'), i.e., the action spectrum of vision, which is initially a photochemical
process. It is important to recognize that radiometric quantities and units are absolute, while
photometric quantities and units are related to standardized human perception; the
relationship between the two sets of units varies significantly with the spectrum of radiation.
The effects of optical radiation (including light), other than vision, must therefore be
measured and quantified in terms of radiometric units and spectral characteristics rather
than photometric units. This is particularly important in relation to the photobiological
effects of UVR. Most lamps used for illumination are rated by manufacturers only in
photometric terms (e.g., lumen output) and not in terms of UVR emission (Phillips, 1983).
The most important radiometric quantities and units commonly used to describe optical
radiation are given in Table 1. Certain terms are used primarily to describe source charac-
teristics, e.g., radiance, radiant intensity; whereas other terms are generally used to describe
exposure (irradiance, radiant exposure). The term 'spectral' placed before any of the quan-
tities implies restriction to a unit wavelength band, e.g., spectral irradiance (watts per square
metre per nanometre) (Moseley, 1988). For a more detailed discussion of these parameters,
see various standard textbooks on radiometry, such as Boyd (1983).
The quantities of radiometry are expressed in terms of absolute energy (Jagger, 1985).
Radiant intensity is the power emitted per unit solid angle of a source. Radiance is the radiant
intensity per unit area of source. Thus, a fluorescent lamp does not have very high radiance in
comparison to the filament of a flashlight bulb, even though it has a high radiant power
output. The radiometric term expressed in units of watts per square metre (dose rate) is
irradiance, which is also the power striking a unit area of surface.
The energy of UVR falling on a unit surface area of an object was defined in 1954 by the
First International Congress of Photobiology as the 'dose'; it has also been referred to as
'exposure dose'. The equivalent radiometric quantity is radiant exposure, expressed in joules
per square centimetre or per square metre. Radiant exposure has been referred to as 'energy
fluence' in some texts; however, fluence is a radiometric quantity, with the same units as
radiant exposure, but referring to energy arriving at a plane of unit area from all directions,
including backscatter. Thus, fluence is quite correctly of value in describing an exposure dose
at a depth inside tissue; it has, however, seldom been calculated in photobiological studies of
the effects of UVR, in which the radiant exposure incident upon the skin is normally
measured. Radiant exposure is the amount of energy crossing a unit area of space normal to
the direction of propagation of a beam of UVR. If the radiant energy arrives from many
directions, as from the sky, then the fluence at one point is the sum of all the component
fluences entering a unit sphere of space. The energy fluence rate is the power that crosses a
unit area normal to the direction of propagation, or the energy per unit area per unit time
46 IARC MONOGRAPHS VOLUME 55
Table 1. Some basic terminology used to quantify optical radiation
Term International Definition SI unit Synonyms and comments
symbol
Wavelength >.. nm Nanometre = tQ-
9
m (also called
millimicron, mJJ.)
Radiant energy
Oe l: (Pe X dt) J Joule; 1 joule = 1 watt x second;
total energy contained in a radiation
field or total energy delivered to a
given receiver by such a radiation
field
Radiant flux Pe dQe/dt w Watt; rate of delivery of radiant
energy ('radiant power'); also
expressed as q,
lrradiance
Ee dPe/dA
Wfm2 Radiant flux arriving over a given
area ('fluence rate', ' dose rate',
'intensity', 'radiant incidence'). In
photobiology, has also been
expressed in W/cm2, mW/cm2 and
JJ.W/cm2
Radiant intensity Ie dPeld.n W/sr Watt/steradian; radiant flux emitted
by source into a given solid angle
(solid angle expressed in steradians)
Radiance dPeldA X d.n Wfm2 x sr Watt/m 2 X steradian; radiant flux
per unit solid angle per unit area
emitted by an extended source
Radiant exposure He Ee X t
Jt m2 Radiant energy delivered to a given
area (' fluence', 'exposure dose' ,
'dose'); t = time in seconds. Has
also been expressed as J/cm2,
m.J/cm2 and J.l]/cm2
Adapted from WHO (1979), Boyd (1983), Jagger (1985), Hoffman (1987) and Weast (1989)
(J/m
2
/s or W/m
2
) . The terms dose (J/m
2
) and dose rate (W/m
2
) pertain to the energy and
power, respectively, striking a unit surface area of an irradiated object (Jagger, 1985).
In terms of visible light perceived by humans, the photometric analogue of the radiance
of a source is luminance (brightness), and irradiance is illuminance (measured in 'lux' or
lumen per square metre). In photometry, the lumen is the unit of luminous power (Jagger,
1985).
1.1.3 Units of biologically effective ultraviolet radiation
In addition to general radiometric quantities, specialized quantities of effective irra-
diance relative to a specified photochemical action spectrum are used in photochemistry and
photobiology. Effective radiant exposures to produce erythema (Jagger, 1985) or photo-
keratitis are examples. Effective irradiance or radiant exposure is not limited to photo-
biology, and a similar approach has been used to quantify the photocuring of inks, in photo-
polymerization (Phillips, 1983) and in assessing the hazards of UVR. In order to weight a
EXPOSURE DATA 47
source spectrally, the general formula involves an action spectrum and a spectral radiometric
quantity. The effective irradiance of a given photobiological process is defined as:
~
I EA X SA X fl.l
lt
expressed in W/m
2
, where Ex. is the spectral irradiance (W/m
2
x nm) at wavelength A. (nm)
and Ax. is the wavelength interval 0\.
1
-A.
2
) used in the summation (in nm). Sx. is a measure of
the effectiveness of radiation of wavelength A. (nm), relative to some reference wavelength, in
producing a particular biological end-point. As it is a ratio, Sx. has no units {American
Conference of Governmental Industrial Hygienists, 1991).
Effective irradiance is equivalent to a hypothetical irradiance of monochromatic radia-
tion with a wavelength at which Sx. is equal to unity. The time integral of effective irradiance is
the effective radiant exposure (also called the ' effective dose').
A unit of effective dose commonly used in cutaneous photobiology is the 'minimal
erythema dose' (MED). One MED has been defined as the lowest radiant exposure to UVR
that is sufficient to produce erythema with sharp margins 24 h after exposure (Morison,
1983a). Another end-point often used in cutaneous photobiology is a just-perceptible
reddening of exposed skin; the dose of UVR necessary to produce this 'minimal perceptible
erythema' is sometimes also referred to as an MED. In unacclimatized, white-skinned
populations, there is an approximately four-fold range in the MED of exposure to UVB
radiation (Diffey & Fdrr, 1989). When the term MED is used as a unit of exposure dose,
however, a representative value is chosen for sun-sensitive individuals. If, in the above
expression for effective irradiance, Sx. is chosen as the reference action spectrum for
erythema (McKinlay & Diffey, 1987) and a value of200 11m
2
at wavelengths for which Sx. is
equal to unity is assumed for the MED, the dose (expressed in MED) received after an
exposure period oft seconds is
t X I: E.t X Sl X fl.J200.
Notwithstanding the difficulties of interpreting accurately the magnitude of such an
imprecise unit as the MED, it has the advantage over radiometric units of being related to the
biological consequences of the exposure.
1.2 Methods for measuring ultraviolet radiation
UVR can be measured by chemical or physical detectors, often in conjunction with a
monochromator or band-pass filter for wavelength selection. Physical detectors include
radiometric devices, which depend for their response on the heating effect of the radiation,
and photoelectric devices, in which incident photons are detected by a quantum effect such as
the production of electrons. Chemical detectors include photographic emulsions,
actinometric solutions and UV-sensitive plastic films.
1.2.1 Spectroradiometry
The fundamental way of characterizing a source of UVR is on the basis of its spectral
power distribution in a graph (or table) which indicates the radiated power as a function of
wavelength. The data are obtained by a technique known as spectroradiometry. Spectral
48 IARC MONOGRAPHS VOLUME 55
measurements are often not required as ends in themselves but are used to calculate
biologically weighted radiometric quantities. A spectroradiometer comprises three essential
components (Gibson & Diffey, 1989):
(i) input optics, such as an integrating sphere or Teflon diffuser, which collects the
incident radiation and conducts it to
(ii) the entrance slit of a monochromator, which disperses the radiation by means of
one or two wavelength dispersive devices (either diffraction grating or prism). The
monochromator also incorporates mirrors to guide the radiation from the entrance
slit to the dispersion device and on to the exit slit, where it is incident on
(iii) a radiation detector, normally a photodiode or, for higher sensitivity, a
photomultiplier tube.
Spectroradiometry is generally considered to be the best way of specifying UV sources,
although the accuracy of spectroradiometry, particularly with respect to the UVB waveband
of terrestrial radiation, is affected by a number of parameters including wavelength cali-
bration, band width, stray radiation, polarization, angular dependence, linearity and
calibration sources. It is therefore essential to employ a double monochromator for accurate
characterization of terrestrial UVR and particularly UVB (Garrison et al., 1978; Kostkowski
eta/., 1982; Gardiner & Kirsch, 1991).
1.2.2 Wavelength-independent (thermal) detectors
General-purpose radiometers incorporate detectors that have a flat response over a
wide range of wavelengths. Such thermal detectors operate on the principle that incident
radiation is absorbed by a receiving element, and the temperature rise of the element is
measured, usually by a thermopile or a pyroelectric detector. A thermopile, which comprises
several thermocouples connected in series for improved sensitivity, must have a window
made of fused silica for measuring UVR at wavelengths down to at least 250 nm. Pyroelectric
detectors rely on a voltage generated by temperature changes in a lithium tantalate crystal.
Thermal detectors are normally used to measure the total radiant power of a source rather
than just the UV component (Moseley, 1988).
Instruments for measuring broad-band solar radiation fall into three categories: pyro-
heliometers, pyranometers and pyranometers with a shading device (Iqbal, 1983). These
types of instrument find their applications in meteorology rather than in UV photobiology.
1.2.3 Wavelength-dependent detectors
Detectors of this type have a spectral response that varies widely depending on the types
of detector and filters that may be incorporated. Detectors can be designed to have a spectral
response that matches a particular action spectrum for a photobiological end-point. The
success with which this is achieved is variable. The most widely used device, particularly for
measuring solar UVR, has been the Robertson-Berger meter (Robertson, 1972; Berger,
1976), which incorporates optical filters, a phosphor and a vacuum phototube or photo-
voltaic cell. This device measures wavelengths of less than 330 nm in the global spectrum with
a spectral response that rises sharply with decreasing wavelength. It has been used to monitor
natural UVR continuously at several sites throughout the world (Berger & Urbach, 1982;
Diffey, 1987a).
---------------- - - -- --
EXPOSURE DATA 49
Detectors incorporating a photodiode or vacuum photocell in conjunction with optical
filter(s) and suitable input optics (e.g., a quartz hemispherical detector) have been produced
to match a number of different action spectra. One such detector is the International Light
Model -730 UV Radiometer, which has a spectral response close to the action spectrum
designated by the American Conference of Governmental Industrial Hygienists for eval-
uating the hazard to health of exposure to UVR, and has been used to measure irradiance
over different terrains (Sliney, 1986).
Wavelength-dependent detectors with spectral responses largely in the UVAwaveband
are used, for example, in measuring the output of irradiation units for the treatment of
psoriasis by psoralen photochemotherapy (Morison, 1983a).
A different yet complementary approach is the use of various photosensitive films as UV
dosimeters. The principle is to relate the degree of deterioration of the films, usually in terms
of changes in their optical properties, to the dose of incident UVR. The principal advantages
of the film dosimeter are that it provides a simple means of integrating exposure continuously
and allows simultaneous comparison of numerous sites that are inaccessible to bulky,
expensive instruments (Diffey, 1987a). The most widely used photosensitive film is polymer
polysulfone (Diffey, 1989a). Personal dosimeters of polysulfone film have been developed
and used in a number of dosimetric studies (Challoner et al., 1976, 1978; Leach eta/., 1978;
Holman et al., 1983a; Larko & Diffey, 1983; Diffey, 1987a; Schothorst et al., 1987a; Slaper,
1987; Rosenthal et al., 1990).
It is difficult to achieve a prescribed UVR spectral response with wavelength-dependent
detectors. Accurate results can be achieved only if the detectors are calibrated against the
appropriate source spectrum using a spectroradiometer (Gibson & Diffey, 1989). Unless this
is done, severe dosimetric errors can arise, particularly with measurements of solar UVR
(Diffey, 1987a; Sayre & Kligman, 1992).
Accurate measurement of UVB radiation is far more difficult than would appear
initially. The primary problem is that the UVB produced by most optical sources- the sun as
. well as incandescent and fluorescent lamps used for illumination-is only a very small
fraction (i.e., less than 0.3%) of the total radiant energy emitted. Additionally, biological
action spectra (e.g., for erythema and photokeratitis) typically decrease dramatically within
the same waveband in which the source spectrum increases (Diffey & Farr, 199la). This
means that either a spectroradiometer or a direct-reading filtered 'erythemal' or 'hazard'
meter must reject out-of-band radiant energy to better than one part in 10
4
or even 10
5
The
spectral band-width of a monochromator can also greatly affect measurement error: too
large a band-width can reduce the steepness of reported action spectra.
1.3 Sources and exposures
In the broadest sense, UVR may be produced when a body is heated (incandescence) or
when electrons that have been raised to an excited state return to a lower energy level, as
occurs in fluorescence, in an electric discharge in a gas and in electric arcs (optical plasma)
(Sliney & Wolbarsht, 1980; Phillips, 1983; Moseley, 1988). The characteristics of exposures
to both terrestrial solar radiation (an incandescent source) and artificial light sources are
discussed in the following sections.
50 IARC MONOGRAPHS VOLUME 55
1.3.1 Solar ultraviolet radiation
Optical radiation from the sun is modified significantly as it passes through the Earth's
atmosphere (Fig. 2), a1though about two-thirds of the energy from the sun that impinges on
the atmosphere penetrates to ground level. The annual variation in extra-terrestrial
radiation is less than 10%, but the variation in the modifying effect of the atmosphere is far
greater (Moseley, 1988). Measurements corrected for atmospheric absorption show that the
visible portion comprises approximately 40% of the total radiation received at the surface of
the Earth. While UVR comprises only a small proportion of the total radiation (approxi-
mately 5% ), this component is extremely important in various biological processes. The
principal effect of infrared radiation is to warm the earth; approximately 55% of the solar
radiation received at the surface of the earth is infrared (Foukal. 1990).
Fig. 2. p ~ t r a l irradiance from the sun outside the Earth's atmosphere (upper curve) and at
sea level (lower curve)
......
E
c
)( 0 2
.. E
(J
-
......
~
E
Q)
g 01
I1S
'6
I1S
...
. !::
ni
...
-0
Q)
Q.
(/)
From Moseley (1988}
1000 2000
Wavelength (nm)
On its path through the atmosphere, solar radiation is absorbed and scattered by various
constituents of the atmosphere. It is scattered by air molecules. particularly oxygen and
nitrogen (Rayleigh scattering), which produce the blue colour of the sky. It is also scattered
by aerosol and dust particles (Mie scattering) and is scattered and absorbed by atmospheric
pollution. Total solar irradiance and the relative contributions of different wavelengths vary
with altitude. Clouds attenuate solar radiation, although their effect on infrared radiation is
greater than on UVR. Reflection of sunlight from certain ground surfaces may contribute
significantly to the total amount of scattered UVR. An effective absorber of solar UVR is
ozone in the stratosphere (Moseley, 1988). An equally important absorber in the longer
wavelengths (infrared) is water vapour (Diffey, 1991); a secondary absorber in this range is
carbon dioxide. These two filter out much of the solar energy with wavelengths longer than
1000 nm (Sliney & Wolbarsht, 1980).
EXPOSURE DATA 51
The quality (spectral distribution) and quantity (total UV irradiance) of UVR reaching
the Earth's surface depend on the radiated power from the sun and the transmitting
properties of the atmosphere. Although UVC exists in the extra-terrestrial solar spectrum, it
is filtered out completely by the ozone layer in the atmosphere. UVB radiation, which
represents about 5% of the total solar UVR that reaches the Earth (Sliney & Wolbarsht,
1980), has been considered to be the most biologically significant part of the terrestrial UV
spectrum. The levels of UVB radiation reaching the surface of the Earth, although heavily
attenuated, are also largely controlled by the ozone layer.
Ozone (03) is a gas which comprises approximately one molecule out of every two
million in the atmosphere. It is created by the reaction of molecular oxygen (0
2
) with atomic
oxygen (0), formed by the dissociation of 0
2
by short-wavelength UVR ( < 242 nm) in the
stratosphere at altitudes between about 25 and 100 km. Absorption of UVR at wavelengths
up to about 320 nm converts the ozone back to 0
2
and 0, and it is this dissociation of ozone
that is responsible for preventing radiation at wavelengths less than about 290 nm from
reaching the Earth's surface (Moseley, 1988; Diffey, 1991). Molina and Rowland (1974) first
proposed that chlorofluorocarbons and other gases released by human activity could alter
the natural balance of creative and destructive processes and lead to depletion of the stra-
tospheric ozone layer. Substantial reductions, of up to 50%, in the ozone column observed in
the austral spring over Antarctica were first reported in 1985 and may continue. There arc,
however, serious limitations in our current understanding of and ability to quantify ozone
depletion at the present levels of contaminant release and in our ability to predict the effects
on stratospheric ozone of any further increases (United Nations Environment Programme,
1989; United Kingdom Stratospheric Ozone Review Group, 1991).
A number of factors influence terrestrial UVR levels:
- Vilriations in stratospheric ozone with latitude and season (United Nations Environ-
ment Programme, 1989)
- Time of day: In summer, about 20-30% of the total daily amount of UVR is received
between 11:00 and 13:00 hand 75% between 9:00 and 15:00 h (Diffey, 1991; Table 2
and Fig. 3). Although the amount of visible light falling on the ground in the summer
may vary by only 30% between 12:00 and 15:00 h (local solar time), the short-
wavelength component of the UVB spectrum undergoes a dramatic change during
Table 2. Percentage of daily UVB and UVA radiation received during
different periods of a clear summer's day. Solar noon is assumed to
be at 12:00 h, i.e., no allowance is made for daylight saving time
Latitude ("N} UVB UVA
11:00-13:00 h 9:00-15:00 h 11:00-13:00 h 9:00-15:00 h
20 30 78 27 73
40 28 75 25 68
60 26 69 21 60
From Diffey (1991)
52 IARC MONOGRAPHS VOLUME 55
Fig. 3. Daily variation in ultraviolet radiation: erythemal effective irradiance falling on a
horizontal earth surface at Denver, CO, USA, on one summer's day
8 100
c
as
--,.._,
as] .. 10
e ... e
0
.J::. ......
>. 1.0
... - :1..
w--
o
G)
-
-
Clear day
--.... 7
-..
Low dense
cloud cover _/
06.00 08.00 1.0.00 12DO 14.00 16.00 18.00
Standard time (h)
From Machta et at. (1975)
this period. At a wavelength of 300 nm, the spectral irradiance decreases by 10 fold,
from approximately 1.0 to 0.1
x nm) (Sliney, 1986).
- Season: Seasonal variation in terrestrial UV irradiance, especially UVB, at the
Earth's surface is significant in temperate regions but much less nearer the equator
(Table 3).
Table 3. 'JYpical values for ambient daily and annual UVB
radiation expressed in minimal erythema dose (MED)
Latitude ("N) Diurnal UVB (MED)
Winter Spring/ Autumn Summer Annual
20 (Hawaii, USA) 14 20 25 6000
30 (Florida, USA) 5 12 15 4000
40 (Spain) 2 7 12 2500
50 (Belgium) 0.4 3 10 1500
From Diffey (1991)
- Geographical latitude: Annual UVR exposure dose decreases with increasing distance
from the equator (Table 3).
- Clouds: Clouds reduce UV ground irradiance; changes in UVR are smaller than those
of total irradiance because water in clouds attenuates solar infrared radiation much
more than UVR. Even with heavy cloud cover, the scattered UVB component of sun-
light (often called skylight) is seldom less than 10% of that under clear sky; however,
very heavy cloud cover can virtually eliminate UVB even in summer. light clouds
scattered over a blue sky make little difference in sunburning effectiveness unless they
directly cover the sun. Complete light cloud cover prevents about 50% of UVB
energy, relative to that from a clear sky, from reaching the surface of the Earth
(Diffey, 1991}.
EXPOSURE DATA
53
- Surface reflection: The contribution of reflected UVR to a person's total UVR expo-
sure varies in importance with a number of factors {Thble 4). A grass lawn scatters
about 3% of incident UVB radiation. Sand reflects about 10-15%, so that sitting
under an umbrella on the beach can lead to sunburn both from scattered UVB from
the sky and reflected UVB from the sand. Fresh snow has been reported to reflect up
to 85- 90% of incident UVB radiation, although reflectance of about 30-50% is
probably more typical. Ground reflectance is important, because parts of the body
that are normally shaded are exposed to reflected radiation {Diffey, 1990a).
Table 4. Representative terrain reflectance factors for horizontal
surfaces measured with a UVB radiometer at 12:00 h (290-315 nm)
in the USA
Material
Lawn grass, summer, Maryland, California and Utah
Lawn grass, winter, Maryland
Wild grasslands, Vail Mountain, Colorado
Lawn grass, Vail, Colorado
Flower garden, pansies
Soil, clay/humus
Sidewalk, light concrete
Sidewalk, aged concrete
Asphalt roadway, freshly laid (black)
Asphalt roadway, two years old (grey)
House paint, white, metal oxide
Boat dock, weathered wood
Aluminium, dull, weathered
Boat deck, wood, urethane coating
Boat deck, white fibreglass
Boat canvas, weathered, plasticized
Chesapeake Bay, Maryland, open water
Chesapeake Bay, Maryland, specular component of reflection
at Z = 45 N
Atlantic Ocean, New Jersey coastline
Sea surf, white foam
Atlantic beach sand, wet, barely submerged
Atlantic beach sand, dry, light
Snow, fresh
Snow, two days old
From Sliney (1986)
Reflectance
(%)
2.0- 3.7
3.0- 5.0
0.8-1.6
1.0--1.6
1.6
4.0--6.0
10- 12
7.0--8.2
4.1- 5.0
5.0- 8.9
22
6.4
13
6.6
9.1
6.1
3.3
13
8.0
25-30
7.1
15- 18
88
50
- Altitude: In general, each 300-m increase in altitude increases the sunburning
effectiveness of sunlight by about 4%. Conversely, places on the Earth's surface
below sea level have lower UVB exposures than nearby sites at sea level (Diffey,
1990a).
54 IARC MONOGRAPHS VOLUME 55
- Air pollution: Tropospheric ozone and other pollutants can decrease UVR, parti-
cularly in urban areas (Frederick, 1990).
(a) Measurements of te"estrial solar radiation
Since UVR wavelengths between about 295 and 320 nm (UVB radiation) in the terres-
trial solar spectrum are thought to be those mainly responsible for adverse health effects, a
number of studies have concentrated on measuring this spectral region (Sliney, 1986}.
Accurate measurements of UVR in this spectral band are difficult to obtain, however,
because the spectral curve of terrestrial solar irradiance increases by a factor of more than
five between 290 and 320 nm (Fig. 4). Nevertheless, extensive measurements of ambient
Fig. 4. Action spectrum designated by the American Conference of Governmental Industrial
Hygienists (ACGIH) for assessing the hazard of ultraviolet radiation (very similar to erythe-
mal action spectrum from 300-230 nm) and the solar spectrum. The ACGIH action spec
trum, which is unitless, is closely tit by some radiometers; however, because of the small over-
lap of the terrestrial solar spectrum with the action spectrum, problems of stray light must
be dealt with by constant checks with a filter that blocks wavelengths of less than 320 nm
10
3
1o2
'E
c
)(
10
1
'E
2.
~
CD
:::1
::I. lG
CD
1cf
>
0 CD
c:
~
"'
'5
"'
"'
Qi
. ~
16
1
...
J:
~
a ...
0
(,.)
<D <
Q.
.,
1 ~
a;
0
en
1&
~ ~ ~ ~ ~ ~ ~ ~ 1 i f
300 320 340 360 380 400
Wavelength (nm)
Adapted from Sliney et a/. (1990)
EXPOSURE DATA 55
UVR in this spectral band have been performed worldwide (Schulze, 1962; Schulze & Grafe,
1969; Henderson, 1970; Sundararaman eta/., 1975; Garrison el a/., 1978; Doda & Green,
1980; Mecherikunnel & Richmond, 1980; Kostkowski eta/., 1982; Ambach & Rehwald,
1983; Blumthaler eta/., 1983; Uvingston, 1983; Blumthaler et al., 1985a,b; Kolari et al., 1986;
Hietanen, 1990; Sliney eta/., 1990). Longer-wavelength UVR (UVA) was measured at the
same time in many of these studies. Measurements of terrestrial solar UVA radiation are less
subject to error than measurements of UVB, since the spectrum does not vary widely with
zenith angle and the spectral irradiance curve is relatively flat.
Maps of annual UVR exposure, such as that shown in Figure 5, have been compiled for
epidemiological studies of skin cancer and other diseases (Schulze, 1962, 1970; Scotto eta/.,
1976). Despite the large numbers of measurements, their interpretation in relation to human
exposure has been complicated by three factors: (i) the considerable variation in UVB
spectral irradiance with solar position throughout the day and with ~ e a s o n (ii) the effect of
the geometry of exposure of individuals; and (iii) variation between humans in outdoor
exposure and the parts of their bodies that are exposed.
Fig. 5. Global distribution of ultraviolet radiation
From Schulze (1970); WHO (1979)
The total solar radiation that arrives at the Earth's surface is termed 'global radiation',
and measurements of terrestrial UVR most frequently pertain to this quantity, i.e., the
radiant energy falling upon a horizontal surface from all directions (both direct and scattered
radiation). Global radiation comprises two components, referred to as ' direct' and 'diffuse'.
56 IARC MONOGRAPHS VOLUME 55
Approximately 70% of the UVR at 300 nm is in the diffuse component rather than in the
direct rays of the sun (Fig. 6). The ratio of diffuse to direct radiation increases steadily from
less than 1.0 at 340 nm to at least 2.0 at 300 nm (Garrison eta/., 1978).
Fig. 6. Diffuse and direct solar spectral irradiance (solar zenith angle, 45)
From Garrison et al. (1978)
"'
0
0
""
0
"'
w
w
0
0
0
0
Spectral irradiance IJWI(cm'x nm)
..... .. .
t .. : ... .:
':: :t .. : .
.. :. ..
}('
/
...
..
8
.,
8
0
8
Ratio diffuse: direct
;;;
0
0
"'
0
0
"' 0
"'
...
;;;
...
"'
0
...
...
0
UVR reflected from the terrain (the albedo) may also be important; however,essentially
all measurement programmes have been limited to the direct and total diffuse components
of sunlight. While such measurements are of interest in calculating the exposure dose of
UVR of a prone individual, they are of very limited value in estimating exposure of the eye
and shaded skin surfaces (e.g., under the chin), where the UVB radiation incident upon the
body from terrain reflectance and horizon sky is of far greater importance. Sliney (1986) and
Rosenthal eta/. (1988) reported measurements of outdoor ambient UVR that included the
reflected component to the eye. Exposure data for different anatomical sites is of value in
developing biological dose- response relationships (Diffey eta/., 1979). The fact that ocular
exposure differs significantly from cutaneous exposure is emphasized by the finding that
photokeratitis is seldom experienced during sunbathing yet the threshold for UV photo-
keratitis is less than that for erythema of the skin (Sliney, 1986).
EXPOSURE DATA 57
Measurements of the angular distribution of UVR relative to solar position and cloud
distribution have been reported (Sliney, 1986; Fig. 7). A cloud obscuring the sun had no
effect upon the UV radiance of open blue sky or the horizon sky; however, when the sun was
'out' (i.e., in an open sky), clouds near the horizon opposite the sun apparently reflected more
UVR than would otherwise be present from the blue sky. This confirms the findings of
studies of photographs of the sky taken through a narrow-band filter at 320 nm (Livingston,
1983), which revealed that the sky looks almost uniformly bright even when clouds are
present and the clouds disappear into a uniformly hazy sky. Only the sun stands out, as would
be expected from the plots on Figure 7. When the sun is near the horizon and can be looked
at without great discomfort (i.e., at Z = 75- 90 ), the effective UV irradiance is again of the
order of 0.3 J!W/cm2, e.g., about 0.08-1.1 JlW/cm
2
at an elevation angle of 12-15 (Sliney,
1986).
Fig. 7. Semilogarithmic plots of the angular dependence of skylight for 290-315 nm
ultraviolet radiation (UVR) with the sun at zenith angle of about 45 o. A narrow field-of-view
detector was scanned from zenith to the horizon. Uppermost curves show that direct UVR
from the sun is more than 10 times greater than scattered UVR normally incident upon the
eye at near-horizon angles where the zenith angle Z = 70-90 o . Most surprising is the simi
larity of blue sky and cloudy sky UV irradiances at zenith or near the horizon.
-
N
E
0
'
~
~
- 10 -
Q)
0
c
(U
'6
(U
...
=
~ 10 -
7
:;::
0
Sun' s position
Hazy- ,.. .... - ... .., Sunny-
toward / . .,_toward
sun ' '. sun
' , .
Q)
::: Clear sky-away.
UJ from sun
I
Cloudy bright-toward sun
' .
1 0
8
~ ~ ~ ~ ~ ~ ~ ~ ~ ~
0 30 60 90
Zenith angle (degrees)
Adapted from Sliney (1986)
(b) Personal exposures
The exposure of different anatomical sites to solar UVR depends not only on ambient
UVR and orientation of sites with respect to the sun but also on cultural and social
behaviour, type of clothing arid whether spectacles are worn.
58 lARC MONOGRAPHS VOLUME 55
Measurements of ambient UVR are useful in that they provide upper limits on human
exposure (Scotto et al . 1976), They are of lesser value for assessing exposure doses received
by groups of individuals. Polysulfone film has been used to monitor personal exposure to
solar UVR (see p. 49). The wide variations in recorded exposure doses reflect diversity of
behaviour and. in most cases. the small numbers ( < 30) of subjects monitored. Nevertheless.
it can be estimated that recreational (excluding vacations) exposure to the sun of people in
northern Europe (where most of these studies were carried out) results in an annual solar
exposure dose to the face of 20-100 MED. depending on the propensity for outdoor pursuits.
The annual weekday UV exposure dose of indoor workers is around 30 MED; as a two-week
outdoor vacation can result in a further 30- 60 MED. the total annual exposure dose to the
face of most indoor workers is probably in the range 40-160 MED. Outdoor workers at the
same latitudes receive about two to three times these exposure doses, typically around 250
MED (Diffey, 1987b; Slaper, 1987).
An alternative approach to estimating personal exposure is to combine measured data
on ambient UVR with a behavioural model of exposure. This approach was applied to a
group of more than 800 outdoor workers in the USA (40 oN) by Rosenthal et al. (1991).
These investigators estimated annual facial exposure doses of 30-200 MED, which are
considerably lower than those estimated for outdoor workers in northern Europe, perhaps
because Rosenthal et al. assumed facial exposure to be about 5-10% of ambient. A number
of researchers have used polysulfone film badges on both human subjects (Holman et a/.,
1983a; Rosenthal et al., 1990) and mannequins (Diffeyet al., 1977, 1979; Gies et al., 1988) to
measure solar UVR exposure on the face relative to ambient exposure. The results vary
considerably, reflecting factors such as positioning of film badges, behaviour of individuals,
solar l t i t u e and the influence of shade. Examination of the data suggests, however. that the
exposure of an unprotected face is probably close to 20% of the ambient. Using this estimate,
the annual facial exposure doses in the outdoor worker group studied by Rosenthal et a/.
(1991) would be about 80- 500 MED. These data demonstrate clearly the current
uncertainties associated with estimates of population exposure doses.
1.3.2 Exposure to artificial sources of ultraviolet radiation
(a) Sources
Six artificial sources that often produce UVR incidental to the production of visible light
(Sliney & Wolbarsht, 1980; Phillips. 1983; Moseley, 1988) are described below.
(i) Incandescent sources
Optical radiation from an incandescent source appears as a continuous spectrum. Incan-
descent sources are usually ascribed a certain 'colour temperature', defined as the tempe-
rature of a black body that emits the same relative spectral distribution as the source. UVR is
emitted in significant quantity when the colour temperature exceeds 2500 OK (2227 oc).
Thngsten-halogen lamps in a quartz envelope (colour temperature, 3000 K (2727 C]) may
emit significant UVR, whereas the UVR emission of an ordinary tungsten light bulb is
negligible.
EXPOSURE DATA 59
(ii) Gas discharge lamps
Another method of producing optical radiation is to pass an electric current through a
gas. The emission wavelengths are determined by the type of gas present in the lamp and
appear as spectral lines. The width of the lines and the amount of radiation in the interval
between them (the continuum) depend on the pressure in the lamp. At low pressures. fine
lines with little or no continuum are produced; as pressure is increased, the lines broaden and
their relative amounts alter. Low-pressure discharge lamps, commonly containing mercury,
argon, xenon, krypton or neon, are useful for spectral calibration. Medium-pressure mercury
lamps operate at an envelope temperature in the region of 600-800 o C.
(iii) Arc lamps
Arc lamps operate at high pressures (20-100 atm (2020-10133 kPa]) and are very
intense sources of UVR. Commonly available lamps contain xenon, mercury or a mixture of
the two elements, which are effective sources of UVR. Xenon arc lamps operate at a colour
temperature of 6000 oK (5727 oC); they are often used as the light source in solar simulation
or are combined with a monochromator in spectral illumination systems. Deuterium arc
lamps provide a useful source of UVC radiation and find their main use in spectro-
photometers and as a calibration source for spectroradiometers.
(iv) Fluorescent lamps
The primary source of radiation in a fluorescent lamp arises from a low-pressure
mercury discharge, which produces a strong emission at 254 nm, which in turn excites a
phosphor-coated lamp to produce fluorescence. By altering the composition and thickness of
the phosphor and the glass envelope, a wide variety of emission spectral characteristics can
be obtained. The output is thus chiefly the fluorescent emission spectrum from the coating,
with a certain amount of breakthrough of UVB mercury lines at 297, 303 and 313 nm, as well
as those in the UVA and visible regions (WHO, 1979).
(v) Metal halide lamps
The addition of other metals (as halide salts) to a mercury discharge lamp allows for the
addition of extra lines to the mercury emission spectrum. Most such tubes are basically
medium-pressure discharge lamps with one or more metal halide additives, usually iodide.
Advantage has been taken of the strong lead emission lines at 364, 368 and 406 nm in the lead
iodide lamp, in which there is a 50% increase in output in the region between 355 and 380 nm
compared to a conventional mercury lamp. Antimony and magnesium halide lamps provide
spectral lines in the UVB and UVC regions.
(vi) Electrodeless lamps
A type of lamp recently introduced on a large scale is the electrodeless lamp. In this
design, the discharge tube absorbs microwave energy fed, via waveguides, irito a microwave
chamber containing the tube. TWo 1500-W magnetrons generate microwave energy at 2450
MHz. The life of such lamps is longer than that of electrode lamps, and a greater range of
metal halides is available. Electrodeless lamps are used extensively for UV curing of inks and
coatings, particularly when a short lamp length is adequate for the area to be irradiated. They
have often been the first choice for curing prints on containers such as two-piece cans, plastic
pots and bottles, and tubes.
60 IARC MONOGRAPHS VOLUME 55
(b) Human exposure
Although the sun remains the main source of UVR exposure for humans, the advent of
artificial UVR sources has increased the opportunity for both intentional and unintentional
exposure.
Intentional exposure is most often to acquire a tanned skin, frequently using sunbeds
and solaria emitting principally UVA (315-400 nm) radiation (Diffey, 1987c). Another
reason for intentional exposure to artificial UVR is the treatment of skin diseases, notably
psoriasis.
Unintentional exposure is most often the result of occupation, and workers in many
industries (see p. 66) may be exposed to UVR from artificial sources. The general public is
exposed to low levels of UVR from sources such as fluorescent lamps used for indoor lighting
and may be exposed in shops and restaurants where UVA lamps are employed in traps to
attract flying insects.
(i) Cosmetic use
To some individuals, a tanned skin is socially desirable. A 'suntanning industry' has
grown up, particularly in northern Europe and North America, in which artificial sources of
UVR supplement exposure to sunlight.
Description of UVR sources used for tanning: Prior to the mid-1970s, the source of UVR
was usually an unfiltered, medium- or high-pressure mercury arc lamp which emitted a broad
spectrum of radiation, from UVC through to visible and infrared radiation (Diffey & Farr,
1991b). The units often incorporated one or more infrared heaters and were commonly
called 'sunlamps' or 'health lamps' (Anon., 1979). One disadvantage of this type of unit was
that the area of irradiation was limited to a region such as the face and so whole-body tanning
was tedious. By incorporating several mercury arc lamps into a 'solarium', whole body
exposure was achieved. Tanning devices based on mercury arc lamps emit relatively large
quantities of UVB and UVC radiation, resulting in a significant risk of burning and acute eye
damage. Solaria that incorporate unfiltered mercury arc lamps are therefore now less
popular (Diffey, 1990a).
So-called UVB fluorescent lamps (e.g., Westinghouse FS Sunlamp, Philips TL12) emit
approximately 55% of their UV energy in the UVB and approximately 45% in the UVA
regions (Diffey & Langley, 1986). They were often used in tanning booths, more commonly
in the USA than in Europe.
Sunbeds, incorporating high-intensity UVA fluorescent lamps, were developed in the
1970s. These devices consist of a bed and/or canopy incorporating 6- 30 fluorescent lamps
150-180 em in length. The earliest type of UVA lamp used in sun beds is typified by the Philips
TL09, Wotan Ll00/79 and Wolff Solarium lamps (Diffey, 1987c). The spectral power
distribution from this type of lamp is shown in Figure Sa. The emission spectrum comprises
the fluorescence continuum, extending from about 315 to 400 nm and peaking at 350-355
nm, together with the characteristic lines from the mercury spectrum down to 297 nm (UVB)
(Diffey & McKinlay, 1983). The UVA irradiance at the skin surface from a typical sunbed or
suncanopy containing these lamps is between 50 and 150 W/m
2
(Bowker & Longford, 1987;
Bruyneel-Rapp et al., 1988).
---- ------- - ----- - - -- --
EXPOSURE DATA 61
Fig. 8. Spectral emissions of different lamps used for cosmetic tanning: (a) Philips TL09
(Diffey, 1987c); (b) Philips TLlOR (Diffey, 1987c); (c) Wolff BelJarium S (B.L. Diffey,
unpublished data); (d) optically filtered high-pressure metal halide lamp (Diffey, 1987c)
0.1
0.01 -
.. 0.001
Q)
~
g_ 0.0001
<U
...
0
<I)
Cl.
(J)
280
0.1
0.01
0.001
0.0001
310 340 370 400
Wavelength (nm)
(c)
280 310 340 370 400
Wavelength (nm)
..
Q)
0.1
0.01
0.001
~ 0.0001 .
Cl.
(b)
tii
!::
0 280
Q)
Cl.
(J)
~ (d)
(; 0.1
Qj
cr
0.01
0.001
0.0001
310 340 370 400
Wavelength (nm)
280 310 340 370 400
Wavelength (nm)
In the mid-1980s, another type of UVA fluorescent lamp (Philips TLIOR) was
introduced especially for cosmetic tanning. The principal features of this type of lamp were a
reflector intrinsic to the lamp envelope and a fluorescence spectrum extending from about
340 to 400 nm, peaking at 370 nm (Fig. 8b ); note also the presence of characteristic mercury
lines in the UVB region. The skin surface irradiance from a sunbed or suncanopy
incorporating Philips TLlOR lamps is typically around 250 W/m2 (Diffey, 1987c).
Another type of UV fluorescent lamp that has been used in sunbeds is the so-caJJed 'fast
tan' tube. This type of lamp is typified by the Wolff Bellarium S, the spectral power
distribution of which is shown in Figure 8( c). The spectrum extends from about 290 to 400 nm
and peaks at around 350 nm (Diffey & Farr, 1987).
Optically filtered, high-pressure mercury lamps doped with metal halide additives are
also used in cosmetic tanning. The spectral emission lies entirely within the UVAwaveband
(Fig. 8d), and irradiances at the skin surface of more than 1000 W 1m
2
can be achieved. The
best known of this type of unit is probably the UVASUN (Mutzhas, 1986).
A summary of the physical and photobiological emissions from these different types of
lamps is given in Table 5 (Diffey & Farr, 1991a).
62
IARC MONOGRAPHS VOLUME 55
Table 5. Characteristics of different ultraviolet (UV) lamps used for tanning
Lamp Radiation emission (%)
Mercury arc sunlamp
Simulated sunlight lamp
l}'pe I UV A lamp
Type II UVA lamp
Optically filtered high-pressure lamp
0
Summer UV sunlightb
UVA
40
95
99
> 99.9
100
95
UVB
40
5
1
< 0.1
0
5
From Diffey & Farr (199lb) unless otherwise specified
OFrom Mutzhas (1986)
bFrom Sliney & Wolbarsht (1980)
uvc
20
0
0
0
0
0
Contnbution to tanning(%)
UVA UVB uvc
0 35 65
20 80 0
60 40 0
>90 < 10 0
100 0 0
20 80 0
Exposure to UVR sources used for tanning: Telephone surveys carried out in the
Netherlands (Bruggers et al., 1987) and in the United Kingdom (Anon., 1987) in the
mid-1980s showed that 7-9% of the adult population in each country had used sunbeds in the
previous one to two years. A more recent market survey in the United Kingdom
(R. McLauchlan, personal communication), with a sample size of 5800, gave a slightly higher
figure, with 10% of the population having used a sun bed during the previous year (1988) and
19% of the sample admitting to having used a sunbed at some time in the past. In these and
other surveys in the United Kingdom (Diffey, 1986) and the USA (Dougherty eta/., 1988),
women accounted for 60-85% of users, about half of the subjects being young women aged
between 16 and 30. The commonest reason given for using tanning equipment was to acquire
a pre-holiday tan (Anon., 1987; R. McLauchlan, personal communication); other reasons
included perceived health benefits, reduction of stress and improved relaxation, protection
of the skin before going on holiday, sustaining a holiday tan and treatment of skin diseases
such as psoriasis and acne (Diffey, 1986; Dougherty eta!., 1988).
In the Dutch survey (Bruggers et a!., 1987), about half of the users interviewed used
tanning equipment at home and the other half used facilities at commercial premises, such as
tanning salons, hairdressers, sports clubs and swimming pools. Most people had used UVA
equipment; 24% had used either UVB mercury arc sunlamps or solaria incorporating these
lamps. A more recent survey in the United Kingdom (McLauchlan, 1989) confirmed the
Dutch finding that the amount of use at home and at commercial premises was approximately
the same. A survey carried out at commercial establishments in the United Kingdom
indicated that all the equipment used emitted primarily UVA radiation, mostly from
fluorescent UVA lamps and 10% from optically filtered high-pressure metal halide lamps
(Diffey, 1986). Sales of tanning appliances in the United Kingdom increased rapidly during
the 1980s, but by the end of the decade there appeared to be a steady, or possibly reduced,
level of sales (Diffey, 1990a).
The mean number of tanning sessions per year in the Dutch study was 23 (Bruggers eta/.,
1987). In the United Kingdom, half-hour sessions were the most popular (Diffey, 1986). Each
tanning session with UVA equipment normally results in an erythemally-weighted exposure
EXPOSURE DATA 63
of about 0.8 MED (150 J/m
2
), whereas exposure to mercury arc lamps results in about
2 MED per session ( 400 J/m
2
). In the Dutch survey, it was estimated that the median annual
exposure was 24 MED (4.8 kJ/m
2
) (Bruggers et al., 1987).
(ii) Medical and dental applications
UVR has both diagnostic and therapeutic applications in medicine and dentistry. The
diagnostic uses are confined largely to fluorescing of skin and teeth, and the UVR source is
normally an optically filtered medium-pressure mercury arc lamp producing radiation
mainly at 365 nm (so-called 'Wood's lamps') (Caplan, 1967). Radiation exposure is limited to
small areas ( < 15 em in diameter), and the UVA radiation dose per examination is probably
no more than 5 J/cm
2
. The therapeutic uses of UVR, which result in considerably higher
doses, are mainly in the treatment of skin diseases and occasionally the symptomatic relief of
pruritus.
Phototherapy: The skin diseases that are most frequently treated with UVR are psoriasis
and eczema. Phototherapy of psoriasis at hospital may include the use of tar and related
derivatives and other substances, such as anthralin, on the skin (Morison, 1983a; see also
IARC, 1987a).
The first treatment of psoriasis with an artificial source of UVR is credited to
Sardemann, who used a carbon arc lamp of the type developed by Finsen at around the turn
of the century. These lamps were unpopular in clinical practice because they emitted noise,
odour and sparks, and they were superseded by the development of the medium-pressure
mercury arc lamp. In the 1960s, a variety of metal halides were added to mercury lamps to
improve emissions in certain regions of the UV and visible spectra. Fluorescent lamps were
developed in the late 1940s; since then, a variety of phosphor and envelope materials have
been used to produce lamps with emissions in different regions of the UV spectrum, such
that, today, there exists a wide range oflamps for the phototherapy of skin diseases (Diffey &
Farr, 1987).
Lamp systems can be classified into one of five categories in terms of suitability for
phototherapy (Diffey, 1990b):
Type A: a single, medium-pressure mercury arc or metal halide lamp;
Type B: one or more vertical columns containing five or six optically filtered
high-pressure metal halide lamps;
Type C: a canopy or cubicle containing fluorescent sunlamps which emit predominantly
UVB but also significant amounts of radiation at wavelengths below 290 nm
(e.g., Westinghouse FS sunlamp, Philips TL12 and Sylvania UV21lamps);
TypeD: a canopy, sunbed or cubicle incorporating fluorescent lamps which emit
predominantly UVB radiation and negligible amounts of radiation at wave-
lengths below 290 nm (e.g., the Wolff Helarium);
Type E: a newly developed fluorescent lamp that emits a narrow band of radiation
around 311- 312 nm (Philips TLOl).
The spectral power distributions characteristic of each of these five types of lamp are
shown in Figure 9. The therapeutic radiation for psoriasis lies principally within the UVB
waveband (Parrish & Jaenicke, 1981), and the cumulative UVB dose required for clearing
64
IARC MONOGRAPHS VOLUME 55
Fig. 9. Spectral power distributions of different types of phototherapy lamp (Diffey, 1990b).
l)rpe A: unfiltered medium-pressure mercury arc lamp; type B: optically filtered iron iodide
lamp; type C: fluorescent sunlamp (Philips TL12); type D: Wolff Helarium lamp; type E:
narrow-band UVB fluorescent lamp (Philips TLOl)
10 0 10 D r-------------r----.
....
TYPE A
; 10 I
0
Q.
"iii ral
....
0
Gl l
a. I ()
C/1
Q)
~ Ia
1111
Q)
a: 10 -s
10 i
200 250
10
....
TYPE C
; 10 I
0
Q.
"iii 10 -z
...
-
(J
~ 10-
1
(/)
4l
~ 10 .,
1111
Q)
a: 10 -s
10 6
200 250
30()
350
Wavelength (nm)
300 3SD
Wavelength (nm)
JO D
~ 10 I
0
Q.
(ij 10 -z
....
0
~ I0 -
1
C/1
Gl
~ 10_,
1111
a;
a: 10 -s
TYPE E
400
400
TYPE B
Qj 10 I
~
0
c..
(ijiOZ
...
0
~ 10-
1
0
4l
.:: 10 _,
iii
Q)
a: 10 -s
10 ...
200 250 300 350
Wavelength (nm)
10
....
TYPED
~ 10-l
0
Q. .
(ij 10 ~
!::
(J
4l . 1
g. 10
Q)
~ 10 _,
1111
a;
a: 10 -s
10 -
6
200 250 100 3SD
Wavelength (nm)
10 - L---.....I...U.U....----------1
200 250 300 350
Wavelength (nm)
4!1a
400
EXPOSURE DATA 65
psoriasis is typically 100-200 MED (Diffey, 1990a), usually delivered over a course
consisting of 10-30 exposures over 3-10 weeks (van der Leun & van Weelden, 1986).
Annual doses received by 90% of patients given UVB phototherapy for psoriasis range
from about 60 to 670 MED, with a typical dose in a single course being between 200 and 300
MED (Slaper, 1987).
Psora/en pholochemotherapy (see also IARC, 1980, 1986a, 1987b ): This form of treat-
ment, known colloquially as PUVA, involves the combination of photoactive drugs, pso-
ralens (P), with long-wave UVR (UVA) to produce a beneficial effect. Psoralen photo-
chemotherapy has been used to treat many skin disease in the past decade, although its
principal success has been in the management of psoriasis (Parrish eta/., 1974), a disorder
characterized by an accelerated cell cycle and rate of DNA synthesis. Psoralens may be
applied to the skin either topically or systemically; the latter route is generally preferred, and
the psoralen most commonly administered is 8-methoxypsoralen. The patient is usually
exposed to UVA radiation from banks of fluorescent lamps with the spectral power
distribution shown in Figure Sa. Values for UVA irradiance in clinical treatment cubicles
have been found to range from 16 to 140 W/m
2
(Diffey eta/., 1980; Diffey, 1990b), although
an irradiance of 80 W 1m
2
is probably typical. The UVA dose per treatment session is usually
in the range 1-10 J/cm
2
(Diffey et al. , 1980).
Generally, approximately 25 treatments over a period of 6-12 weeks, with a cumulative
UVA dose of 100-250 J/cm
2
, are required to clear psoriatic lesions (Melski eta/., 1977;
Henseler eta/., 1981). PUVA therapy is not a cure for psoriasis, and maintenance therapy is
often needed at intervals of between once a week to once a month to prevent relapse (Gupta
& Anderson, 1987).
Neonatal phototherapy for hyperbilirubinaemia: Phototherapy is sometimes used in the
treatment of neonatal jaundice or hyperbilirubinaemia. The preferred method of treatment
is to irradiate the baby for several hours a day for up to one week with visible light,
particularly blue light (Sisson & Vogl, 1982). The lamps used for phototherapy, although
intended to emit only visible light, may also have a UV component: One commercial
neonatal phototherapy unit was found to emit not only visible light and UVA but also
radiation at wavelengths down to 265 nm (Diffey & Langley, 1986).
Fluorescence in cutaneous and oral diagnosis: Wood's light-a source of UVA obtained
by filtering optically a mercury arc lamp with 'blackglass' -is used by dermatologists as a
diagnostic aid in skin conditions that produce fluorescence (Caplan, 1967; Diffey, 1990a). As
irradiation of the oral cavity with a Wood's lamp can produce fluorescence under certain
conditions, this has been used in the diagnosis of various dental disorders, such as early
dental caries, the incorporation of tetracycline into bone and teeth, dental plaque and
calculus (Hefferren et a!., 1971 ).
Polymerization of dental resins: Pits and fissures in teeth have been treated using an
adhesive resin polymerized with UVA. The resin is applied with a fine brush to the surfaces to
be treated and is hardened by exposure to UVA radiation at a minimal irradiance of 100
W/m
2
for 30 s or so (Eriksen et al., 1987; Diffey, 1990a).
66 IARC MONOGRAPHS VOLUME 55
(iii) Occupational exposures
Artificial sources of UVR are used in many different ways in the working environment.
In some cases, the UV source is well contained within an enclosure and, under normal
circumstances, presents no risk of exposure to personnel. In other applications of UVR, it is
inevitable that workers are exposed to some radiation, normally by reflection or scattering
from adjacent surfaces. Occupational exposure to UVR is also a consequence of exposure to
general lighting in the workplace.
lndustn"al photoprocesses: Many industrial processes involve a photochemical com-
ponent. The large-scale nature of these processes often necessitates the use of high-power
(several kilowatts) lamps such as high-pressure metal halide lamps (Diffey, 1990a).
The principal industrial applications of photopolymerization include the curing of
protective coatings and inks and photoresists for printed circuit boards. The curing of
printing inks by exposure to UVR is now widespread; as the cure takes only a fraction of a
second, UV drying units can be installed between printing stations on a multicolour line, so
that each colour is dried before the next is applied. Another major use ofUV curing has been
for metal decorating in the packaging industry (Phillips, 1983). UVA is also used to inspect
printed circuit boards and integrated circuits in the electronics industry (Pauw & Meulemans,
1987).
Artificial sources of UVR are used to test the weathering capability of materials such as
polymers. Xenon-arc lamps are often the light source because their emission spectra is
similar to the spectrum of terrestrial sunlight, although some commercial weathering
chambers incorporate carbon-arc lamps, high-pressure metal halide lamps or fluorescent
sunlamps (Davis & Sims, 1983).
Sterilization and disinfection: Radiation with wavelengths in the range 260-265 nm is the
most effective for this use, since it corresponds to a maximum in the DNA absorption
spectrum. Low-pressure mercury discharge tubes are thus often used as the radiation source,
as more than 90% of the radiated energy lies in the 254 nm line. These lamps are often
referred to as 'germicidal lamps', 'bactericidal lamps' or simply 'UVC lamps' (Diffey, 1990a).
UVC radiation has been used to disinfect sewage effluents, drinking-water, water for the
cosmetics industry and swimming pools. Germicidal lamps are sometimes used inside
microbiological safety cabinets to inactivate airborne and surface microorganisms (Diffey,
1990a). The combination of UVR and ozone has a very powerful oxidizing action and can
reduce the organic content of water to extremely low levels (Phillips, 1983).
Welding (see also IARC, 1990): Welding equipment falls into two broad categories: gas
welding and electric arc welding. Only the latter process produces significant levels of UVR,
the quality and quantity of which depend primarily on the arc current, shielding gas and
metals being welded (Sliney & Wolbarsht, 1980).
Welders are almost certainly the largest occupational group with exposure to artificial
sources of UVR. It has been estimated (Emmett & Horstman, 1976) that there may be as
many as half a million welders in the USA alone. The levels ofUV irradiance around electric
arc welding equipment are high; effective irradiance (relative to the action spectrum of the
American Conference of Governmental Industrial Hygienists) at 1 m at an arc current of 400
A ranged from 1 to 50 W/m
2
(Thble 6), and the unweighted UVAirradiance ranged from 3 to
EXPOSURE DATA
67
70 W 1m
2
, depending on the type of welding and the metal being welded (Cox, 1987; Mariutti
& Matzeu, 1987). It is not surprising therefore that most welders at some time or another
experience 'arc eye' or 'welder's flash' (photokeratitis) and skin erythema. The effective
irradiance at 0.3 m from many types of electric welding arcs operating at 150 A is such that
the maximum permissible exposure time for an 8-h working period on unprotected eyes and
skin varies from a few tenths of a second to about 10 s, depending on the type of welding
process and the material used (Cox, 1987).
Table 6. Limits of exposure to ultraviolet radiation and
radiation effectiveness
Wavelength
Exposure limit
Relative spectral
(nm)
(J/m2)
effectiveness (Sx_)
4
180
2500
0.012
190
1600
0.019
200
1000
0.030
205
590
0.051
210
400
O.D75
215
320
0.095
220
250
0.120
225
200
0.150
230
160
0.190
235
130
0.240
240
100
0.300
245
83
0.360
250
70
0.430
254b
60
0.500
255
58
0.520
260
46
0.650
265
37
0.810
270
30
1.000
275
31
0.960
28()b
34
0.880
285
39
o.no
290
47
0.640
295
56
0.540
297b
65
0.460
300
100
0.300
303b
250
0.120
305
500
0.060
308
1200
0.026
310
2000
0.015
313b
5000
0.006
315
1.0 X 10
4
0.003
316
1.3 X 104
0.0024
317
1.5 X 10
4
0.0020
318
1.9 X 10
4
0.0016
319
25 X 104
0.0012
68 IARC MONOGRAPHS VOLUME 55
Table 6 (contd)
Wavelength Exposure limit Relative spectral
(nm) (J/m2) effectiveness (S>..)a
320 2.9 X 104 0.0010
322 4.5 X 104 0.00067
323 5.6 X 104 0.00054
325 6.o x 10
4
0.00050
328 6.8 X 104 O.IXXl44
330 7.3 X 104 0.00041
333 8.1 X 104 0.00037
335 8.8 X 104 0.00034
340 1.1 X lQS
0.00028
345 1.3 X lOS 0.00024
350 1.5 X 105 0.00020
355 1.9 X 105 0.00016
360 2.3 X 1QS 0.00013
365b
2.7 X lOS 0.00011
370 3.2 X lOS 0.000093
375 3.9 X 105 0.000077
380 4.7 X lOS 0.000064
385 5.7 X lOS 0.000053
390 6.8 X l()S 0.000044
395 8.3 X lQS 0.000036
400 1.5 X lo6 0.000030
From American Conference of Governmental Industrial Hygienists
(1991); . wavelengths chosen are representative, and other values
should be interpolated at intermediate wavelengths.
a'f'or explanation, see pp. 46-47
bEmission lines of a mercury discharge spectrum
In a survey of electric arc welders in Denmark, 65% of those questioned had experienced
erythema; however, as no indication of the frequency of skin reactions was reported, it is not
possible to estimate annual exposure (Eriksen, 1987). Monitoring of the exposure to UVR of
non-welders working in the vicinity of electric arc welding apparatuses showed that their
daily exposure dose exceeded the maximum permissible exposure limits by almost an order
of magnitude (Barth eta/., 1990).
Phototherapy: Although there is a trend to the use of enclosed treatment cubicles, some
of the lamps used to treat skin disease (see the section on medical and dental applications)
are unenclosed, emit high levels of UVR and can present a marked hazard to staff; at 1 m
from these lamps, the recommended 8-h occupational exposure limits can be exceeded in less
than 2 min (Diffey & Langley, 1986).
In a study of the exposure of staff in hospital phototherapy departments (Larko & Diffey,
1986), annual exposure to UVR could be estimated from the number of occasions per year
on which staff had experienced at least minimal erythema (Diffey, 1989b ). Estimated annual
EXPOSURE DATA 69
occupational exposures to UVR were 15, 92 and 200 MED, corresponding to a frequency of
erythema of once per year, once per month and once per week, respectively.
Operating theatres: VVC lamps have been used since the 1930s to decrease the levels of
airborne bacteria in operating theatres (Berg, 1987). The technique requires complete
protection of the eyes and skin of staff and patients; for this and other reasons, filtered air
units are often preferred.
Research laboratories: Sources of UVR are used by most experimental scientists engaged
in aspects of photobiology and photochemistry and in molecular biology. These applications,
in which the effect of UV irradiation on biological and chemical species is of primary interest
to the researcher, can be differentiated from UV fluorescence by absorption techniques
where the effect is of secondary importance (Diffey, 1990a).
UV photography: There are two distinct forms of UV photography: reflected or
transmitted UV photography and UV fluorescence photography. In both applications, the
effective radiation lies within the UVA waveband (Lunnon, 1984).
UV lasers: High-power lasers which emit in the UV region, used in nuclear and other
research laboratories, are far less common than those that emit in the visible or infrared
regions of the electromagnetic spectrum.
Nitrogen lasers emit at a wavelength of337 nm (Phillips, 1983), and instruments with a
peak power output of up to 2.3 MW per pulse are available. Nitrogen lasers can be used in
conjunction with fluorescent dyes to produce spectral emissions of360-900 nm, with a power
pulse of 200-480 kW. If frequency doubling crystals are used in conjunction with a nitrogen
laser, UV emissions down to 260 nm are possible.
An alternative laser source of UVR is the excimer laser. (The term 'excimer' denotes a
homonuclear molecule which is bound in an electronically excited state but is dissociative in
the ground state [Phillips, 1983 ]. ) The wavelength of the pulsed UVR from this type of laser
depends on the excimer molecules, such as ArF, F
2
, XeCl and KrF, which emit at 193, 157,
308 and 248 nm, respectively (Phillips, 1983; Bos & de Haas, 1987). On the basis of worst-
case assumptions, the estimated annual risk for skin cancer for workers exposed to UV lasers
in medical applications is equivalent to about one additional day of sunbathing, and that for
workers exposed to UV lasers in laboratories is comparable to the risk for outdoor workers
(Sterenborg et al., 1991).
Quality assurance in the food industry: Many contaminants of food products can be
detected by UV fluorescence techniques. For example, the bacterium Pseudomonas
aeruginosa, which causes rot in eggs, meat and fish, can be detected by its yellow-green fluo-
rescence under UVA irradiation. One of the longest established uses ofUVA fluorescence in
public health is to demonstrate contamination with rodent urine, which is highly fluorescent
(Ultra-Violet Products, Inc., 1977).
Insect traps: Many flying insects are attracted by UVA radiation, particularly in the
region around 350 nm. This phenomenon is the principle of electronic insect traps, in which a
UVA fluorescent lamp is mounted in a unit containing a high-voltage grid. The insect,
attracted by the UVA lamp, flies into the unit and is electrocuted in the air gap between the
high-voltage grid and a grounded metal screen. Such units are commonly found in areas
where food is prepared and sold to the public (Diffey, 1990a).
70 IARC MONOGRAPHS VOLUME 55
Sunbed salons and shops: The continuing popularity of UVA sunbeds and suncanopies
for cosmetic tanning has resulted in the establishment of a large number of salons and shops
selling sunbeds for use at home. Some shops may have 20 or more UVA tanning appliances,
all switched on, thus exposing members of the public and staff to high levels ( > 20 W /m
2
) of
UVA radiation (Diffey, 1990a).
Discotheques: UVA 'blacklight' lamps are sometimes used in discotheques to induce
fluorescence in the skin and clothing of dancers. The levels of UVA emitted are usually low
( < 10 W/m2) (Diffey, 1990a).
Offices: Signatures can be verified by exposing a signature obtained with colourless ink
to UVA radiation, under which it fluoresces. UVA exposure of office staff is normally to
hands, and irradiance is low ( < 10 W/m
2
) (Diffey, 1990a).
(iv) Genera/lighting
Fluorescent lamps used for general lighting in offices and factories emit small quantities
of both UVA and UVB. A UVA irradiance of 30 mW/m
2
(Diffey, 1990a) and a UVB irra-
diance of3 m W 1m
2
(McKinley & Whillock, 1987) were found for bare fluorescent lamps with
a typical illuminance of 500 lux. These UV levels give rise to an annual exposure of indoor
workers to no more than 5 MED, and this dose can be reduced appreciably by the use of
plastic diffusers (McKinlay & WhiiJock, 1987). A study of the personal doses of UVR
received by workers in the car manufacturing industry who were engaged in inspecting
paintwork of new cars under bright fluorescent lamps indicated a similar annual exposure
(Diffey et al., 1986). Most plastic diffusers reduce erythemally effective irradiance to 0.2% or
less of that of the bare lamp. An exception is clear acrylic diffusers, which absorb only about
20% of the erythemally effective radiation. The absorption of UVA radiation by diffusers is
less effective, transmission ranging from 1% for opal polycarbonate to 74% for clear acrylic
(McKinlay & Whillock, 1987). Spectroradiometric measurements of the UV levels from
indoor fluorescent lamps carried out in the USA, however, indicated much higher annual
doses for people exposed occupationally for 2000 h per year: The annual estimated exposure
dose ranged from 8 to 30 MED for an illuminance level of 500 lux from bare lamps (Cole et
al., 1985).
Desk-top lights which incorporate tungsten- halogen (quartz) lamps may result in
exposure to UVR of the hands and arms, if the lamps are used in excess of recommended
occupational exposure levels (McKinlay eta/., 1989). Experimental studies have shown that
erythema can be induced in susceptible individuals after a 15-min exposure at 10 em from a
100-W tungsten-halogen source, principally by the UVB component of the emission
(Cesarini & Muel, 1989). Tungsten- halogen lamps are also used for general lighting (e.g.,
spotlights, indirect lighting, floor lamps) in some countries.
(c) Regulations and guidelines
(i) Cosmetic use
The most comprehensive guidelines for the use of sunlamps and sunbeds in cosmetic
tanning are those published by the International Electrotechnical Commission (1987, 1989).
The guidelines classify tanning appliances into one of four types according to the effective
irradiance at short (A. < 320 nm) and long (320 < A.< 400 nm) UV wavelengths (Thble 7).
EXPOSURE DATA
Table 7. Classification of tanning appliances
Type Effective irradiance{Wfm2)
1
2
3
4
X ~ 320 nm
< 0.0005
0.0005-0.15
< 0.15
~ 0.1
320 nm < X. ~ 400 nm
~ 0.15
~ 0.15
< 0.15
< 0.15
From International Electrotechnical Commission
(1989)
Effective radiance is defined as:
250
71
where Ex. is the spectral irradiance (W/m
2
x nm) at wavelength A. (nm) at the shortest
recommended exposure distance; ~ x is the wavelength interval used in the summation; and
Sx. is the relative erythemal effectiveness recently adopted by the Commission lnternationale
de l'Eclairage (McKinlay & Diffey, 1987), specified as shown in Table 8. The guidelines
recommend that the exposure time for the first session on untanned skin should correspond
to an effective dose not exceeding 100 J/m
2
; this is approximately equivalent to 1 MED for
subjects with sun-reactive skin type I. The annual exposure should not exceed an effective
dose of 25 kJ/m
2
(International Electrotechnical Commission, 1989).
Table 8. Specifications of relative erythemal effectiveness
Wavelength (X.; nm)
X. < 298
298 < X. < 328
328 < X. S. 400
Relative erythemal effectiveness (Sx.)
(weighting factor)
1
100.094(298- X.)
1Q0.015(139- A)
From McKinlay & Diffey (1987); International Electrotechnical
Commission (1989)
Although these guidelines form the basis of several national standards on sunlamp and
sunbed use, it should be noted that variations exist; for example, in the Netherlands, Norway
and Sweden, certain UV appliances are not permitted. Regulations concerning the use of
tanning appliances are in force in only a few countries, but many others have published
advice on sunbed use, including information on adverse effects, as well as guidelines on
manufacturing standards. ,
(ii) Occupational exposure
Guidance on the maximal limits of exposure to UVR as a consequence of occupation is
given by the International Non-ionizing Radiation Committee of the International Radiation
72 IARC MONOGRAPHS VOLUME 55
Protection Association. These exposure limits, which apply only to incoherent (i.e., non-
laser) sources, represent conditions under which it is expected that nearly all individuals may
be repeatedly exposed without adverse effects and are below levels which would be used for
medical or cosmetic exposure to UVR. The limits for occupational exposure to UVR
incident upon the skin or eye were considered separately for the UVA spectral region
(315-400 nm) and the actinic UVspectral region(UVC and UVB, 180-315 nm). In 1984, the
limit provided an equal spectral weighting between 315 and 400 nm, a maximal 1000-s
radiant exposure of 10 KJ/m
2
and a maximal irradiance of 10 W /m
2
for longer periods (Inter-
national Non-ionizing Radiation Committee of the International Radiation Protection Asso-
ciation, 1985). Studies of skin and ocular injury resulting from exposure to UVA led the
Committee to issue revised exposure limits in 1988: For the UVA spectral region (315-400
nm), the total radiant exposure incident upon the unprotected eye should not exceed 1.0
J/cm
2
(10 kJ/m
2
) within an 8-h period, and the total 8-h radiant exposure incident upon the
unprotected skin should not exceed the values given in Table 6. Values for the relative
spectral effectiveness S ,._are given up to 400 nm to expand the action spectrum into the UVA
region for determining the exposure limit for skin exposure. For the actinic UV spectral
region (UVC and UVB, 180-315 nm), the radiant exposure incident upon the unprotected
skin or eye within an 8-h period should not exceed the values given in Table 6 (International
Non-ionizing Radiation Committee of the International Radiation Protection Association,
1989).
The effective irradiance (Eerr) in W 1m
2
of a broad-band source weighted against the
peak of the spectral effectiveness curve (270 nm) is determined according to the formula:
where E>.. is the spectral irradiance (W /m
2
x nm) from measurements, S>.. is the relative
spectral effectiveness (Table 6) and is the band-width (nm) of the calculation or
measurement interval (International Non-ionizing Radiation Committee of the Interna-
tional Radiation Protection Association, 1985).
The maximal permissible exposure time in seconds for exposure to UVR incident on the
unprotected skin or eye within an 8-h period is computed by dividing 30 J/m
2
by the value of
Eerr in W 1m
2
(American Conference of Governmental Industrial Hygienists, 1991 ). A worker
receiving the maximal permissible exposure of 30 J/m
2
per 8-h day will, in the course of a
working year, have a cumulative dose of 60-70 MED (Diffey, 1988), a value comparable with
the naturaJ exposure of non-occupationally indoor workers (Diffey, 1990a).
Occupational exposure limits to lasers were also defined by the International Non-
Ionizing Radiation Committee of the International Radiation Protection Association in
1989, at 3 mJ/cm
2
and 40 mJ/cm
2
over 8 h for argon- fluoride and xenon-chloride lasers,
respectively (Sliney, 1990).
2. Studies of Cancer in Humans
2.1 Solar radiation
2.1.1 Nonmelanocytic skin cancer
Nonmelanocytic skin cancer is classified into two major histological types: basal-cell
carcinoma and squamous-cell carcinoma. Basal-cell carcinoma is the commoner type in
white populations. No information was available to the Working Group on other types of
nonmelanocytic skin cancer.
(a) Case reports
In general, case reports were not considered, owing to the availability of more infor-
mative data.
(i) Studies of xeroderma pigmentosum patients
Xeroderma pigmentosum is a rare autosomal-recessive genetic disease in which there is
an excision repair defect, as observed in cultured skin fibroblasts damaged by UVR (Cleaver,
1968). Patients display cellular and clinical hypersensitivity to UVR (Kraemer, 1980). The
disease is present in about one in 250 000 people in the USA and Europe (Cleaver &
Kraemer, 1989), and as many as 1 in 100 000 (Take beet a/., 1987) or even 1 in 40 000 (Cleaver
& Kraemer, 1989) people may be affected in Japan.
In a survey of 830 cases located through published case reports (Kraemer eta!., 1987),
45% had malignant skin neoplasms. Most of the patients were young, and the median age of
development of the first skin cancer in the 186 patients for whom information was available
was eight years; this observation presumably represents a substantial excess over the ex-
pected number. Only 259 neoplasms were specifically categorized as basal- or squamous-
cell carcinoma in the published reports. Of these, 97% were on constantly exposed sites (face,
head and neck) by comparison with 80% of similar tumours in the US general population.
[The Working Group recognized that data collected from previously published case reports
is not uniform and may not be typical of a true incidence or prevalence series.]
(ii) Studies of transplant recipients
Australian renal transplant recipients were reported to have an increased risk for non-
melanocytic skin cancer (Hardie eta/. , 1980). Among 875 male and 669 female Australasian
recipients, aged 35-64, 47 squamous-cell carcinomas and 27 basal-cell carcinomas were
observed among males and 27 squamous-cell and 15 basal-cell carcinomas were observed
among females (Kinlen eta/., 1979). The rates/10
5
person-years for squamous-ce1l carcinoma
were 2680 in males and 1710 in females, or 3.0 and 5.9 times the rates observed among resi-
dents of the same age distribution surveyed in Geraldton. Western Australia (Kricker et al.,
1990). For basal-cell carcinoma. the rates for 1540 (males) and 940 (females) were 1.154 and
1.150 times the Geraldton rates, respectively.
-73-
74
IARC MONOGRAPHS VOLUME 55
By February 1980, a registry in Denver, Colorado (USA), had received data on 906
organ transplant recipients who had developed 959 types of cancer: 42% arose iri the skin, of
which 47% were squamous-cell carcinomas (Penn, 1980). While several studies from areas
with lower solar radiation are available (Boyle eta/., 1984), neither singly nor collectively do
they contain enough observations to permit a comparable calculation.
(b) Descriptive studies
Nonmelanocytic skin cancer is often not recorded in cancer registries (e.g., in the USA
and in most parts of Australia), and when it is registered case ascertainment is likely to be
incomplete since many patients are treated in consulting rooms, frequently without histo-
logical verification (Doll et al., 1970). Thus, descriptive studies of the incidence of non-
melanocytic skin cancer can be difficult to perform because of the absence of routinely
collected data or difficult to interpret because of incomplete registration. Studies in Australia
and the USA have relied upon special surveys, while in the United Kingdom and the Nordic
countries data from cancer registries have been used. Studies of mortality rates are also
difficult to interpret because nonmelanocytic skin cancer is rarely fatal, and many deaths are
incorrectly attributed to skin cancer (Muir et al., 1987).
A number of features of the occurrence of nonmelanocytic skin cancer as revealed by
descriptive studies have been taken as evidence that exposure to the sun is a major cause of
the disease. These include features presumed to be related to sun exposure such as sex,
anatomical site, latitude of residence (or annual dose of UVB radiation), migration from
places of low insolation to places of high insolation, occupation and features related to
sensitivity to the sun such as race (i.e., degree of skin pigmentation).
(i) Host factors
The occurrence of nonmelanocytic skin cancer according to host factors such as race
provides indirect evidence that sunlight is a cause. In most white populations, non-
melanocytic skin cancer occurs more commonly in men than in women (Muir et al., 1987).
The highest incidence rates have been recorded among Australians, who are largely of
British (Celtic) descent (Giles et al., 1988). Populations with greater skin pigmentation have
low rates of nonmelanocytic skin cancer, for instance, in South Africa (Oettle, 1963) and
Singapore (Shanmugaratnam et al., 1983).
Albinism is an inherited disorder of melanin metabolism, with a decrease or complete
absence of melanin. Large numbers of skin cancers (mostly squamous-cell carcinomas) have
been reported in albinos (Luande et al., 1985; Kromberg eta/., 1989).
(ii) Anatomical distribution
The majority of cases of skin cancer recorded in cancer registries (Haenszel, 1963
[USA]; Whitaker et al., 1979 [United Kingdom]; Swerdlow, 1985 [United Kingdom]; Levi et
al., 1988 [Switzerland]; 0sterlind et al., 1988a [Denmark]; Moan eta/. , 1989 [Norway]) and in
special surveys in the USA (Haenszel, 1963; Scotto eta/., 1983) occurred on the head and
neck. In contrast, in two studies in Australia-one of incidence (Giles eta/., 1988) and the
other of prevalence (Kricker eta/., 1990)-the proportions of cancers on the head and neck
were lower. [The Working Group noted that the contrasting results may be due to time
differences.] In the incidence survey, 43% of squamous-cell carcinomas and 66% of
STUDIES OF CANCER IN HUMANS 75
basal-cell carcinomas were on the head and neck. In the prevalence survey, about one-third
of all basal-cell carcinomas were on the head and neck, whereas the trunk accounted for
about half of these lesions. The density of tumours was five times greater in men and eight
times greater in women on usually exposed sites than on sites which were sometimes exposed.
Squamous-cell carcinomas occurred almost exclusively on exposed sites. The site distri-
butions of both types of nonmelanocytic skin type are generally similar in the two sexes
(0sterlind eta/., 1988a; Moan eta/. , 1989; Kricker eta/., 1990).
A distinctive feature of the site distribution of basal-cell carcinoma is a virtual absence
on the dorsa of the hands and infrequent occurrence on the forearms, compared with the
distribution of squamous-cell carcinoma (Haenszel, 1963; Silverstone & Gordon, 1966; Levi
eta/., 1988; Magnus, 1991). Basal-cell carcinoma also occurs frequently on parts of the face
that receive comparatively little sun exposure (Urbach eta/., 1966).
[The Working Group noted that cancers on the head and neck may be more likely to be
diagnosed than cancers at other sites.]
(iii) Geographical variation
Nonmelanocytic skin cancer incidence and mortality have long been known to increase
with increasing proximity to the equator. Gordon and Silverstone (1976) demonstrated a
negative correlation between incidence of nonmelanocytic skin cancer in various countries
and latitudes by tabulating the incidence according to latitudinal zones. Much of the early
evidence came from surveys conducted in the USA. In the first of these, Dorn (1944a,b,c)
reported the results of the US First National Cancer Survey conducted in 10 urban areas in
1937-38. [Nonmelanocytic] skin cancer incidence was greater among whites living in the
south than in the north of the country. Blum (1948) subsequently reanalysed these data,
substituting latitude for place of residence, and showed a strong inverse relationship between
incidence of mostly nonmelanocytic skin cancer and latitude. No other cancer, with the
exception of the buccal cavity (including the lip), showed a similar latitude gradient.
Auerbach (1961), using data from the US Second National Cancer Survey conducted in
1947-48 in the same areas as the previous survey, calculated that the age-adjusted rates for
skin cancer doubled for each 3 o 48 ' (approximately 265 miles) of latitude towards the
equator; similar gradients were seen for men and women and in all age groups. Haenszel
(1963) reanalysed data from this survey for four southern and four northern cities. The
inverse gradient with latitude was present for both basal-cell and squamous-cell carcinoma.
In addition, there was some evidence that the gradient was strongest for head, neck and
upper limbs (sites which are usually exposed).
A similar latitude gradient was seen in the US Third National Cancer Survey (Scotto
eta/., 1974). Inverse latitude gradients have also been reported in Australia (Silverstone &
Gordon, 1966; Giles et al., 1988) and in the Nordic countries (Teppo eta/., 1980; Moan eta/.,
1989; Magnus, 1991).
Several authors have correlated nonmelanocytic skin cancer incidence (or mortality)
with estimates of UVR. Green eta/. ( 197 6) reported a positive correlation be tween estimates
of annual UV dose and of incidence rates in the USA, the United Kingdom, Canada and
Australia. Estimates of UV dose were derived from models relating latitudinal and seasonal
ozone distributions, adjusted for cloud cover. [The Working Group noted that no allowance
76 IARC MONOGRAPHS VOLUME 55
was made in the analysis for different methods of case ascertainment. It is not clear how well
the predicted values were correlated with actual levels of UVR.]
A positive correlation, stated to be stronger than that for latitude, was seen between
UVR, as measured by Robertson-Berger meters, and the incidence of nonmelanocytic skin
cancer in four cities in the US Third National Cancer Survey (Scotto et al., 1982). Scotto et al.
(1983) examined incidence data collected in eight cities in 1977-78 and again showed an
inverse relationship with latitude and a positive correlation with measurements of UVR. The
gradient was steeper for squamous-cell than for basal-cell carcinoma.
Moan eta/. (1989) examined nonmelanocytic skin cancer incidence in six regions of
Norway from 1976 to 1985, excluding the area around Oslo to reduce bias due to possible
differences in reporting and diagnosis. Two measures of UVR, one weighted according to the
action spectrum for erythema and the other according to the action spectrum for mutagenesis
in cells in the basal layer of the skin, were derived from atmospheric models. Similar, positive
relationships between UVR and nonmelanocytic skin cancer incidence were obtained with
each method.
Elwood eta/. (1974) conducted a study of mortality from nonmelanocytic skin cancer in
the contiguous states of the USA and in all of the provinces of Canada in 1950-67. The
correlation between latitude and mortality was as strong as that between mortality and an
index of UVR derived from a model relating erythemal dose according to latitude with
adjustments for cloud cover.
(iv) Migration
Studies of migrants to Australia (and other countries with high exposure to the sun) offer
the opportunity to examine, indirectly, the effect of exposure to the sun. Most migrants to
Australia come from higher latitudes which have lower levels of exposure to the sun than
Australia. The effect of exposure to the sun is most readily examined in migrants from the
British Isles to Australia, from whom most Australians are descended.
Armstrong eta/. (1983) found that the age-adjusted mortality rate among men born in
England or Wales was 0.55 (95% confidence interval (CI), 0.43-0.71) times that in
Australian-born men. There was little evidence that rates in migrants increased with duration
of residence in Australia, although the numbers of deaths were small and the rates unstable.
Giles et al. (1988) found age-adjusted incidence rates of 402 per 100 000 person-years
among immigrants from the British Isles and 936 in the Australian-born population.
(v) Occupation
Death certificates for 1911-44 in England and Wales were used in an analysis of cancer
of the skin, excluding melanomas, in male agricultural workers, miners and quarriers and
professionals (Atkin eta/., 1949). During part of the period (1911-16), cancers ofthe penis,
scrotum and skin were classified together, and the numbers of cancers of the skin alone were
estimated from the proportions occurring in the later period. The standardized mortality
ratios (SMRs) were greater for those engaged in agriculture (142.4 [137.4-147.6]) than for
those in mining (94.4 (88.8-100.3]), and lowest of all for professionals (47.5 (42.6-52.9]).
Whitaker eta/. (1979) examined occupations among cases of squamous-cell carcinoma
reported to the Manchester Regional Cancer Registry, United Kingdom, in 1967-69. The
occupations of 23% of cases were not ascertained. In men, standardized registration ratios
STUDIES OF CANCER IN HUMANS 77
(SRRs) were elevated for textile workers (238;p < 0.001) and farmers (243;p < 0.001). The
SRR was also high for female farmers (690; p < 0.001). Male fishermen, chemical workers
and paper/printing workers had high SRRs for squamous-cell carcinoma of the arm, and
building workers for squamous-cell carcinoma of the ear.
The association between occupation and nonmelanocytic skin cancer was examined in
England and Wales in 1970-75 in a 10% sample of all male incident cases for which occu-
pation was recorded (Beral & Robinson, 1981 ). Individuals were assigned, on the basis of
stated occupation, to one of three groups: outdoor workers, indoor office workers and other
indoor workers, according to the classification of occupations of the Office of Population
Censuses and Surveys. The SRRs for men aged 15-64 were 110 [95% CI, 109-116) for
outdoor work, 97 [92-103] for office work and 92 (86-89] for other indoor work. Since place
of work may be confounded with social class, the analyses were repeated for men aged 15-64
years in social class III; the SRRs were 112 (102-122) for outdoor work, 111 [100-123) for
office work and 85 [78-92] for other indoor work.
Vagero eta/. (1986) linked cancer incidence data in Sweden from 1961 to 1979 with
census data from 1960 to determine the occupations of cases of nonmelanocytic skin cancer.
Occupations were classified into three main groups: office workers, other indoor workers
and outdoor workers. SRRs standardized for age, county of residence and social class, were
slightly higher for outdoor workers (106; 95% CI, 101-112) than for office workers (103;
96-110) and other indoor workers (95; 91- 100). The authors noted that registration may
have been more complete among high socioeconomic groups.
(c) Cross-sectional studies
Design features of cross-sectional studies of exposure to the sun are summarized in
Table 9, and the results are shown in Table 10.
A population-based survey of the prevalence of nonmelanocytic skin cancer [types not
separated] was conducted in County Galway, Ireland (O'Beirn eta/., 1970). Exposed areas of
skin were examined for the presence of cancers. In the 26 cases found, there was no signi-
ficant association with frequent severe sunburn for basal-cell or squamous-cell skin cancer;
among males, there was a positive relationship between cumulative hours of exposure to
sunlight and the prevalence of nonmelanocytic skin cancer.
Silverstone and Gordon (1966) and Silverstone and SearJe ( 1970) reported the results of
three surveys in Queensland, Australia. Exposed areas of the skin were examined, and
subjects were asked to report previously treated nonmelanocytic skin cancer [types not
separated]. Women performing home duties were classified as indoor workers. Outdoor
occupation showed a weakly positive association with past and present incidence in men and
a negative association in women.
Holman eta/. (1984a) conducted a population-based survey of 1216 subjects in western
Australia. After controlling for age, cutaneous sun damage (as assessed by microtopography)
was strongly related to a past history of nonmelanocytic skin cancer.
Engel et al. (1988) analysed data on basal-cell epithelioma (carcinoma) from the First
National Health and Nutrition Examination Survey in the USA (1971-74). Dermatologists
diagnosed skin cancers and assessed actinic skin (solar) damage, but histological con-
firmation of the diagnosis was not obtained routinely. Strong associations between the
78 IARC MONOGRAPHS VOLUME 55
prevalence of basal-cell epithelioma and solar skin damage were seen in both men and
women.
Green eta/. (1988a) conducted a survey of the prevalence of nonmelanocytic skin cancer
(types not separated for calculation of RR] in Queensland, Australia. Information about
exposure to the sun was obtained from questionnaires; dermatologists diagnosed skin
cancers and assessed signs of actinic damage (solar lentigines, telangiectasia of the face, solar
elastosis of the neck and solar keratoses). After adjustment for age, sex, skin colour and
ability to tan, outdoor occupation and number of sunburns were both weakly associated with
increased prevalence. Stronger associations were seen for cutaneous indicators of sun
exposure, particularly for solar lentigines on the hands and telangiectasia on the face.
Recreational exposure was not associated independently with nonmelanocytic skin cancer.
In a later report (Green, 1991), the occurrence of nonmelanocytic skin cancer was posi-
tively correlated with grade of cutaneous microtopography.
In a subsequent study (Green & Battistutta, 1990), subjects were asked to report
nonmelanocytic skin cancer treated between 1 December 1985 and 30 November 1987,
around the survey in 1986. Medical records were searched to confirm the diagnoses. Subjects
who had had a skin cancer diagnosed at the prevalence survey were excluded. Outdoor occu-
pation, outdoor leisure activities and number of sunburns showed little association with
basal-cell carcinoma in an analysis including past history of skin cancer. All three variables
were related to incidence of squamous-cell carcinoma. [The Working Group noted that the
exclusion of subjects found to have skin cancer during the prevalence survey makes inter-
pretation of these results difficult. The inclusion of past history of skin cancer in the analysis
would have weakened any association with exposure to the sun. ]
Vitasa et al. (1990) conducted a survey of the occurrence of nonmelanocytic skin cancer
among men engaged in traditional fishing practices ('watermen') in Maryland, USA Subjects
were examined by dermatologists and interviewed about their history of exposure to the sun.
Estimates of individual annual and lifetime doses of UVB radiation were made by weighting
the ambient UVR by a history of occupation and outdoor activities and by taking into
account relative doses recorded by film dosimeters on the face. Patients with squamous-cell
carcinoma aged 15-60 had had an 11% higher annual dose ofUVB radiation and those with
basal-cell carcinoma had had an 8% lower annual dose than that of age-matched watermen
without cancers. The effect of cumulative UVB radiation was examined after adjustment for
age, eye colour, childhood freckling and skin reaction to sunlight, all of which were positively
associated with occurrence of both types of nonmelanocytic skin cancer. Cumulative UVB
radiation dose was not associated with basal-cell carcinoma but was positively associated
with squamous-cell carcinoma. The latter association was significant in a comparison of the
top quarter of cumulative UVB versus the bottom three-quarters but not in a comparison of
exposures above and below the median. (The Working Group noted that the results for the
two types of cancer are not necessarily incompatible, both because of the small number of
cases and the fact that the diagnosis was confirmed histopathologically in only 62%.]
Table 9. Design features of cross-sectional studies of sun exposure and nonmelanocytic skin cancer
Reference Place Period of Population Sample Response Cases Histological
diagnosis
size rate
confirmation
(/)
O'Beim et al. (1970) County 1960s Population-based 1338 Approx. 13 BCC; 13 sec on Incomplete; 57%
Galway,
81% exposed sites only had biopsies
t:J Ireland
.....
tTJ
Silverstone & Gordon Queensland, 1961- 63 Population-based About 2200 87% 221 BCC or SCC on Incomplete
(/)
(1966); Silverstone & Australia
exposed surfaces 0
Searle (1970) "r1
(')
Holman eta/. (1984a) Busselton, 1981 Population-based 1216 102, type not stated No
Western
z
(')
Australia
tTJ
El)gel et al. (1988) USA 1971-74 Population -based 20 637 74% BCC, number not Incomplete (small
- stated proportion]
z
Green el al. (1988a) Nambour, 1986 Population-based 2095 70-78% 42 sec or sec (90% Yes :I:
Australia
of subjects examined
c
a:
on head/neck/ hands/
)>
forearms only]
z
Green & Nambour, 1985-87 Population-based 1770 84% 66 BCC; 21 SCC self- Incomplete
(/)
Battistutta (1990) Australia
reported (confirmed
from medical records)
Vitasa et at. (1990) Maryland, 1985-86 Male fishermen 838 70% 33 Bee; 35 sec Incomplete
USA > 30 years old
BCC, basal-cell carcinoma; SCC, squamous-cell carcinoma
Table 10. Summary of results of cross-sectional studies of nonmelanocytic skin cancer
00
0
Reference Index of exposure Categories Odds ratio (95% CI) Comments
O'Beirn et a!., (1970) Sunlight hours (lifetime) < 30000h 1.00 Mean aged > 60 years;
> 50000h [8.10 (1.2-348.2)] calculated from raw data
(p = 0.02]
Silverstone & Searle Occupation Indoors 1.0 Men, chi-square = 1.4
(1970) Outdoors (1.29] (p > 0.1]; calculated from raw
data, no adjustment
Occupation Indoors 1.0 Women, chi-square = 0.3
- Outdoors [0.6} (p > 0.1J; calculated from raw
>
data, no adjustment
~
Holman et al. (1984a) Cutaneous microtopography Grades 1-3 1.0 p = 0.004, trend adjusted for age
~
Grade 4 3.9
0
Grade 5 3.6 z
Grade 6 9.2
0
0
Engel et al. (1988) Solar skin damage None 1.0 BCC, men, age-adjusted pre-
~
Any [8.0) valence ratio, p < 0.01
"'
None 1.0 BCC, women, age-adjusted pre-
::I:
Any [6.0) valence ratio, p < 0.01
Vl
<
Green et al. (1988a) Occupational exposure Indoors 1.00 Adjusted for age, sex, skin colour
0
Indoors and outdoors 1.01 (0.44:..2.31) and propensity to sunburn
t:
Outdoors 1.76 (0.77-4.05)
~
Painful sunburns None 1.00 Adjusted for age, sex, skin colour 1:!1
1 0.77 (0.22-2.61) and propensity to sunburn
Vl
Vl
2- 5 1.09 (0.41-2.95)
~ 1.66 (0.59-4.64)
Solar lentigines on hands None 1.00 Adjusted for age, sex and other
1-10 1.61 (0.78-3.35) signs of actinic damage
11-20 1.43 (0.43-4.77)
~ 21 3.78 (1.06-13.41)
Telangiectasia on face None 1.00 Adjusted for age, sex and other
Mild 1.63 (0.58-4.57) signs of actinic damage
Moderate 2.74 (0.89-8.40)
Severe 3.67 (0.79-17.11)
Table 10 (contd)
Reference
Index of exposure
Categories
Odds ratio (95% CI) Comments
Green et a/. (1988a)
Actinic elastosis on neck
None
1.00
Adjusted for age, sex and other
(contd)
Mild to moderate
1.42 (0.53-3.80) signs of actinic damage
Severe
1.75 (0.56-5.45)
Solar keratoses on face
None
1.00
Adjusted for age, sex and other
1-5
1.55 (0.67-3.59)
signs of actinic damage
C/)
6-20
1.86 (0.69-5.04)
d
21-50
3.00 (0.54-16.69)
0
-
51
2.72 (0.73-10.15)
m
V> Green & Battist utta BCC
0
(1990)
Occupational exposure
Mainly indoors
1.0
Adjusted for age, sex, skin colour
"'1
Indoors and outdoors 1.5 (0.8-2.9)
and past history of skin cancer (')
Mainly outdoors
1.3 (0.6-2.8)
>
z Leisure exposure
Mainly indoors
1.0
Adjusted for age, sex, skin colour ("')
Indoors and outdoors 1.0 (0.4-2.2)
and past history of skin cancer m
:;r;:l
Mainly outdoors
0.6 (0.3-1.3)
......
No. of painful sunburns
None
1.0
Adjusted for age, sex, skin colour
z
::r::
1
0.5 (0.2-1.4)
and past history of skin cancer
c: 2- 5
0.6 (0.3- 1.5)
s::
6 1.0 (0.4-2.5)
:>
sec
z
C/)
Occupational exposure
Mainly indoors
1.0
Adjusted for age, sex, skin colour
Indoors and outdoors 4.4 (0.9- 20.9)
and past history of skin cancer
Mainly outdoors
5.5 {1.1-28.2)
Leisure exposure
Mainly indoors 1.0
Adjusted for age, sex, skin colour
Indoors and outdoors
2.0 (0.2- 19.9)
and past history of skin cancer
Mainly outdoors
3.9 (0.5-30.9)
No. of painful sunburns (}-1
1.0
Adjusted for age, sex, skin colour
2-5
3.3 (0.9-12.3)
and past history of skin cancer
6 3.0 (0.7-12.2)
00
-
Table 10 (contd)
Reference Index of exposure Categories Odds ratio (95% CI) Comments
Vitasa et aJ. (1990) sec
Cumulative UVB dose to face Below median 1.0 Proportionate odds ratios; ad
Above median 2.05 (0.84-5.01) justed for age, eye colour. freck-
Below 75 percentile 1.0 ling and sunburn reaction
Above 75 percentile 2.53 (1.18-5.40)
BCC
Cumulative UVB dose to face Below median 1.0 Proportionate odds ratios; ad-
Above median 0.69 (0.31- 1.53) justed for age, eye colour, freck-
Below 75 percentile 1.0 ling and sunburn reaction
Above 75 percentile 1.11 (0.50-2.44)
BCC, basal-cell carcinoma; SCC, squamous-cell carcinoma; unless otherwise specified, all analyses are for the two types together
:;
f5
0
z
0
0
"tl
til
6
E
rn
Vl
Vl
STUDIES OF CANCER IN HUMANS 83
(d) Case-control studies
Design features of the case-control studies of exposure to the sun and the occurrence of
nonmelanocytic skin cancer are summarized in Table 11. Most of the studies employed
hospital- or clinic-based controls, which introduces potential for selection bias. The results
are summarized in Thble 12. The methods of analysis and of measurements of exposure to the
sun, particularly in the earlier studies, were crude. Neither sensitivity to the sun, usually
measured as the ability to tan or propensity to burn, nor pigmentary characteristics (such as
skin colour and hair colour), which are likely to be confounding variables, were taken into
account in most of the analyses.
The hospital-based study of Lancaster and Nelson (1957) in Sydney, Australia, was
primarily a case-control study of melanoma (described in detail on p. 100). It can also be
considered to be a case-control study of nonmelanocytic skin cancer, however, because it
included two control groups-one of patients with basal-cell carcinoma, squamous-cell
carcinoma or solar keratosis and the second of patients with leukaemia or cancer at a site
other than the skin. All groups were matched by age and sex. Among males, long duration of
occupational exposure to the sun was associated with an increased risk for nonmelanocytic
skin cancer or solar keratosis. A summary of total exposure to the sun was devised by
assigning scores to a number of factors considered to be related to exposure to the sun. Risk
was highest among subjects judged to have excessive exposure to the sun. [The Working
Group noted that the proportion of cases who had a solar keratosis is not stated, that no
account was taken of matching in the analyses, and that the effect of exposure to the sun was
not adjusted for sensitivity to the sun.]
Gellin et al. (1965) conducted a study in a single hospital in New York, USA, on 861
patients with basal-cell carcinoma and 1938 non-cancer dermatological patients attending
the same clinic. Since 95% of cases and 43% of controls were 40 years old and over, the study
was limited to these patients, resulting in 771 cases and 783 controls. The skin cancer patients
spent more time outdoors per day than did control patients and were significantly more likely
than controls to have light hair, fair complexion, blue eyes and an inability to tan. [The
Working Group noted that the analyses were not adjusted for age, sex or sensitivity to the sun,
and that confounding by age is likely because controls were younger than cases.]
Urbach et a/. (1974) conducted a hospital-based study in Philadelphia, USA, and
compared exposure to the sun of 392 patients with histologically confirmed basal-cell carci-
noma, 59 patients with histologically confirmed squamous-cell carcinoma and 281 out-
patients receiving treatment for a skin disease other than cancer. Controls were matched to
cases by age and sex. Among male patients, those with basal-cell or squamous-cell carcinoma
had more cumulative hours of exposure than did controls. Skin cancer patients also reported
more sunburns. [The Working Group noted that the analyses were not adjusted for ability to
tan, age or sex (apart from the sex-specific analysis).]
Vitaliano (1978) subsequently reanalysed the data of Urbach et al. (1974) and showed
that, after adjustment for complexion (dark versus pale), ability to tan and age ( < 60, > 60),
the cumulative time spent outdoors was related to both types of nonmelanocytic skin cancer.
For basal-cell carcinoma, the odds ratio for> 30 000 h of exposure relative to < 10 000 h was
3.19; for squamous-cell carcinoma it was 22.8. [The Working Group noted that confi-
84 IARC MONOGRAPHS VOLUME 55
dence intervals were not given. Part of the apparently stronger effect for squamous-cell
carcinoma could be due to confounding by age: the controls were matched by age to the
basal-cell carcinoma cases, who were younger than the squamous-cell carcinoma cases.]
A hospital-based case-control study was conducted in Montreal, Canada (Aubry &
MacGibbon, 1985), in which patients with histologically confirmed squamous-cell carci-
noma were identified in hospitals in 1977-78. Two patients with other conditions were
matched as controls to each case by age, sex and hospital. Information on exposure to the sun
was obtained from a postal questionnaire. Among 306 eligible cases, 94 (31%) replied, as did
186 (30%) of the eligible controls; 92 cases and 174 controls completed the questionnaire.
Most of the controls who replied had been seen for seborrheic keratoses (61 %) or intra-
dermal naevi (16%). Scores for nonoccupational and occupational exposures were esti-
mated, and the two scores were divided into thirds for analysis, which was based on logistic
regression. The odds ratios, adjusted for each other and for host factors, were 1.08 and 1.64
for the middle and upper thirds of occupational exposure and 1.23 and 1.58 for the same
levels of nonoccupational exposure, respectively. [The Working Group noted the low
response rate and that the complexity of the recreational exposure to sun indices and the
nature of the control group make the results difficult to interpret.]
O'Loughlin et al. (1985) conducted a case-control study in a hospi.tal in Dublin, Ireland.
Patients with histologically confirmed nonmelanocytic skin cancer [types not separated) were
compared with age- and sex-matched patients who had cancers of other organs. There was no
statistically significant difference between cases and controls in eight measures of exposure
to the sun summarized in a single index of exposure and either type of nonmelanocytic skin
cancer. [The Working Group noted that the measures of exposure to the sun were crude and
likely to be subject to considerable misclassification. No adjustment was made for sensitivity
to the sun.]
Herity et al. (1989) conducted a case- control study in the same hospital in Dublin of 396
histologically confirmed nonmelano<..ytic skin cancers in 1984-85. An equal number of age-
and sex-matched patients with other cancers, attending the same hospital, were used as
controls. More cases than controls lived in rural areas (p = 0.007), and cases reported more
frequently spending more than 30 h outdoors per week, but the difference was not significant.
For other indices of exposure to the sun, there was little difference between cases and
controls. (The Working Group noted that results were not adjusted for reaction to sunlight.]
In a case-control study (reported as an abstract) conducted in 1983-84 in Alberta,
Canada (Fincham & Hill. 1989), 225 men with basal-cell carcinoma and 181 men with
squamous-cell carcinoma were compared with 406 age-matched male controls. Sunburn in
adult life gave an odds ratio of 2.33 (p < 0.05) for all nonmelanocytic skin cancer; for basal-
cell carcinoma, childhoood sunburn gave an odds ratio of 2.48 (p < 0.05) and peeling an
odds ratio of 1.85 (p < 0.05).
A population-based case- control study was conducted in Saskatchewan, Canada
(Hogan eta/., 1989), which included all patients diagnosed with basal-cell carcinoma in the
Province in 1983. Two controls, matched by year of birth, sex and municipality of residence,
were selected for each case from a universal Provincial health insurance plan. Replies to
mailed questionnaires were received from 55.5% of the cases and 43.7% of the controls. A
number of measures of exposure to the sun were associated with incidence of basal-cell
L_ _ ___________ ___ _ _ _ -- - -
STUDIES OF CANCER IN HUMANS 85
carcinoma. In a stepwise logistic regression analysis, occupation as a farmer, history of severe
sunburn and working outdoors for more than 3 h per day in winter were independently
associated with basal-cell carcinoma, after adjustment for freckles in childhood, family
history of skin cancer, 'Celtic' mother, skin colour and hair colour. [The Working Group
noted that the measures of exposure were crude and that the estimates do not appear to have
been adjusted for the matching variables. The low response rate makes interpretation of the
results difficult.]
On the basis of a population-based survey in Western Australia in 1987 of skin cancer
among residents aged 40-64 years of age (Kricker et a/., 1990), Kricker eta/. (1991a)
conducted a case-control study of 226 confirmed cases of basal-cell carcinoma and 45 of
squamous-cell carcinoma; two sets of 1015 controls with no lesions, who had completed an
interview, were available for each type of cancer. The response rate among those eligible to
participate was identical for cases and controls: 89%. Separate analyses were undertaken for
basal-cell carcinoma and squamous-cell carcinoma using unconditional logistic regression
analysis. Risks for both cancers were higher in native-born Australians than in migrants, and
the risk for b s l ~ c e l l carcinoma decreased with increasing age at arrival in Australia. Only
four of the subjects with squamous-cell carcinoma had been born outside Australia-an
insufficient number to examine the effects of age at arrival. Indicators of sun damage to the
skin (facial telangiectasia, solar elastosis of the neck, facial solar lentigines and number of
solar keratoses), assessed by dermatologists during the prevalence survey, were examined in
models adjusted for age, sex, ethnicity and migrant status and including all other sun damage
indicators except solar keratoses, which were considered to be preneoplastic lesions and thus
inappropriate for inclusion in models concerned with etiology. Cutaneous microtopography,
an objective measure of actinic skin damage, graded without knowledge of the person's skin
cancer status, and solar elastosis of the neck had significant residual effects for basal-cell
carcinoma, while solar elastosis and facial telangiectasia had significant residual effects for
squamous-cell carcinoma. The independently significant indicators of sun damage were
analysed in models which included adjustment for age, sex, ethnicity and migrant status as
well as measures of sun sensitivity. Solar elastosis of the neck remained an independent
predictor of risk of basal-cell carcinoma (odds ratios, > 1.50; p = 0.003) and squamous-cell
carcinoma (odds ratios, > 2.00; p = 0.04).
A subsequent analysis of individual sun exposure was published as an abstract (Kricker
et al., 1991b). A positive association was found between nonmelanocytic skin cancer and
life-time potential for exposure to the sun, but no evidence of increasing risk for either
basal-cell carcinoma or squamous-cell carcinoma with increasing total hours of actual
exposure to the sun as recalled by subjects. Risk for basal-cell carcinoma on the trunk was
increased substantially in association with maximal exposure of the trunk to the sun, but
there was no consistent pattern of association of site-specific basal-cell or squamous-cell
carcinoma with exposure of the head and neck or limbs. Neither basal-cell nor squamous-cell
carcinoma showed evidence of an association with sun exposure on working days; however,
there was persuasive evidence of increased risk for both types of skin cancer with
. intermediate and high levels of accumulated exposure to the sun on non-working days.
Moreover, there was evidence of an association, stronger for basal-cell carcinoma than for
squamous-cell carcinoma, with a measure of intermittent exposure to the sun.
86
IARC MONOGRAPHS VOLUME 55
Gafa eta/. (1991) conducted a case-control study of nonmelanocytic skin cancer in
Sicily, Italy, in which 133 cases identified from a populationbased registry (response rate,
94%) were compared with 266 sex and age matched controls. For each case, one control was
selected randomly from among patients with non-neoplastic diseases at the same hospital as
the case, and a second control was selected randomly from among friends or relatives of the
case. After adjustment for family history of skin cancer, 'cancerrelated cutaneous disease',
skin colour and skin reaction to sunlight, sun exposure for at least 6 h per day and residence
for at least 10 years at more than 400 m above sea level were significantly related to risk for
nonmelanocytic skin cancer. In crude analyses in which the two types of cancer were
separated, sun exposure for at least 6 h per day without a hat was strongly associated with risk
for squamous-cell carcinoma [site unspecified) (odds ratio, 6.4; 95% CI, 1.9-21.1) but not for
basal-cell carcinoma (1.4, 0.7-2.6). [The Working Group noted that the nature of the control
group, the assessment of exposure and the failure to account for age in the analysis make the
results difficult to interpret. The crude analysis of the type-specific results, the lack of data on
the site of the tumours and the small numbers may explain the different results for the two
types.]
(e) Cohort studies (Thbles 13 and 14)
In a study in Chicago, IL (USA), Robinson (1987) investigated the incidence of second
nonmelanocytic skin cancer among a group of 1000 patients who had had basal-cell carci-
noma. Among 978 who were followed for five years after the initial diagnosis, 22% deve-
loped a second basal-cell carcinoma at the end of the first year and 36% within five years.
There was no significant correlation between developing a second cancer and frequent expo-
sure through sunbathing or outdoor leisure activities, work or currently living in an area with
heavy exposure to the sun, or according to estimated number of hours of daily exposure to the
sun. Among those with skin types I and II (always burn easily and never or minimally tan) who
reported frequent sun exposure, there was an increased risk of second cancer (p < 0.03).
[The Working Group noted that the methods of assessing exposure and the methods of
analysis were not described, and that no numbers were reported. Risk factors for second
cancers might not be the same as for the first.]
Marks et at. (1989) conducted a longitudinal series of examinations of the head, neck,
forearms and hands of a population in Maryborough, north-central Victoria, Australia, for
one week annually between 1982 and 1986. The incidence rates of squamous-cell and
basal-cell carcinoma were higher in outdoor workers than in indoor workers. In an analysis of
the two types combined, occupation was not significantly associated after adjustment for age,
sex and reaction to sunlight (p = 0.09). [The Working Group noted that no account was taken
of lesions that might have been removed between surveys.]
Hunter et a/. (1990) conducted a study of basal-cell carcinoma in a cohort of female
nurses in the USA. A total of 771 cases were identified from responses to follow-up ques-
tionnaires sent to the women two and four years after the initial exposure questionnaire was
given. In a sample of 29 women, the diagnosis was confirmed for 28; confirmation of the
diagnosis was not obtained routinely. Residents of California and Florida had the highest
incidence rates. There was a trend of increasing incidence with increasing number of sun-
burns. With respect to time spent outdoors during the summer, nurses who spent more than
Table 11. Design features of case-control studies of sun exposure and nonmelanocytic skin cancer
Reference Place Period of Cases Controls
diagnosis
No. Source No. Source
Cll
Lancaster & Sydney, Australia Unknown 173 BCC, SCC or Major hospitals 173 Other cancers, same
~
Nelson (1957) solar keratosis hospitals
C)
Gellin et a/. (1965) New York, USA 1955-59 771 BCC One skin hospital 783 Other diagnoses, same
......
~ 40 years old ~ 4 skin clinic
~
Urbach et al. Philadelphia, USA 1967- 69 392 BCC One skin and 281 Other diagnoses, same
0
"'1
(1974) 59 sec cancer clinic clinic
(')
Aubry& Montreal, Canada 1977-78 92SCC 12 hospitals 174 Skin conditions, same
~
MacGibbon (1985) hospitals
(')
O'Loughlin et a/. Dublin, Ireland Unknown 63 sec One hospital 121 Other cancers, same
tTl
:x;l
(1985) 58 BCC hospital
-
Herity er a/. (1989) Dublin, Ireland 1984-85 396 BCC and One hospital 396 Other cancers, same
z
sec hospital
::r=
c
Hogan et al. (1989) Saskatchewan, 1983 538 BCC Population 738 Population
~ Canada
Kricker et al. Geraldton, 1987 226 BCC Population 1015 Population
z
Cll
(1991a) Australia 45 sec 1015
Gafa eta/. (1991) Ragusa, Sicily, 1987-88 133 BCC and Cancer registry 133 Non-neoplastic diseases,
Italy sec 133 same hospital; friends
or relatives
BCC, basal-cell carcinoma; SCC, squamous-cell carcinoma
~
00
00
Table 12. Summary of results of case-control studies of nonmelanocytic skin cancer
Reference Exposure Categories Odds ratio Comments
(95% CI)
Lancaster & Nelson Years of occupational < 5 1.0 [p < 0.001, trend; p and odds ratio calcu-
(1957) exposure 5-10 [1.9] latec. from raw data)
>10 [4.2]
Thtal sun exposure Minimal 1.0 [p = 0.13; p and odds ratio calculated from
Moderate [1.8] raw data]
Excessive (2.4]
-
Gellin eta/. (1965) Hours per day outdoors 0-2 1.0 BCC [p < 0.001]
>
'='
3-5 (4.9 (3.8-6.3))
()
6 [7.7 (5.6-10.6)]
Urbach et al. (1974) Cumulative hours < 30 1.0 BCC
0
z
(X 1000) 30-50 [3.5 (2.0-6.6)]
0
> 50 [9.3 (3.2-37.4)] 0
< 30 1.0 sec
s:
30-50 [4.0 (1.7- 9.6)]
"'tj
> 50 (11.1 (2.8-53.6)]
::r:
C/)
Aubry & MacGibbon Non -occupational Low 1.0 sec [p .. 0.07] for continuous variable, ad-
<
(1985) exposure score Medium 1.23 justed for occupation and host factors
0
High 1.58
E
Occupational score Low 1.0 sec [p = 0.02] for continuous variable, ad-
Medium 1.08 justed for non-occupational score and host
m
High 1.64 factors
V\
Ul
Use of sunlamps Never 1.0 sec [p = 0.008), adjusted for sun exposure
Ever 13.4 (1.38-130.48) and host factors
O'Loughlin et al. (1985) Outdoor oCcupation No 1.0 Not significant (McNemar's test) (odds ratio
Yes [1.5) calculated from raw data ignoring matching)
Hours per week outdoors < 10 1.0 Not significant
10 [1.4]
Sunbathing > 4 h per day No 1.0 Not significant
on vacations Yes [1.0]
Herity et al. (1989) Living in rural area [1.4) p - 0.007
> 30 h outdoors/week [1.1] p = 0.7
TabJe 12 (contd)
Reference
Exposure
Categories Odds ratio Comments
(95% CI)
Hogan eta/. (1989) Fanner
No 1.0
BCC, adju'sted for each other, plus freckles,
Yes 1.29 [1.12-1.46]
family history of skin cancer, Celtic mother,
skin colour, hair colour
Severe sunburn No 1.0
Yes 1.19 [ 1.04-1.35] BCC
Working outdoors > 3 h per No 1.0
(,/)
....,
day in winter Yes 1.13 [1.01-1.27] BCC
c
Kricker er a/. (1991a) BCC tJ
.......
Age at migration (years)
Australian 1.0
p < 0.001, adjusted for other variables
[Tl
en
born 1.37 (0.55- 3.42)
below and for ethnicity, ability to tan, freck-
0
<10 0.32 (0.18-0.59)
ling as a child and number of moles on back 'Tl
> 10
(')
Solar elastosis of the neck None 1.00
p = 0.03, comments as above
>
z
Mild 1.85 (0.80-4.26)
n
Moderate 2.75 (1.16-6.50) rn
:;.:1
Severe 3.96 (1.58-9.93)
.....
Cutaneous microtopo- Grades 1-3 1.0
p = 0.10, comments as above z
graphy
Grade 4 2.01 (1.00-4.07)
:c:
Grade 5 2.42 (1.17-5.01) c::
a: Grade 6 2.15 (0.99-4.70)
> sec
z
Migrant to Australia No 1.0
p = 0.13, adjusted for variables below plus
(/')
Yes 0.46 (0.15-1.38)
ability to tan, skin colour, freckling as a
child
Pennanent colour No 1.0
p = 0.03, comments as above
difference between neck and Yes 2.58 (1.03-6.47)
adjacent skin
Telangiectasia of face None/mild 1.0
p = 0.10, comments as above
Moderate 2.22 (1.06-4.67)
Severe 1.88 (0.72-4.90)
Solar elastosis of the neck None/mild 1.00
p = 0.04, comments as above
Moderate 2.31 (1.00- 5.34)
Severe 3.33 (1.23-9.04)
00
\G)
Table 12 (contd)
Reference
Gafa et ai. (1981)
Exposure
Residence > 400 m above
sea level
Sun exposure 6 h/day
Categories
No
Yes
No
Yes
Odds ratio
(95% CI)
1.0
2.0 (1.2-3.2)
1.0
1.9 (1.2-3.1)
Comments
0
Adjusted for family history of skin cancer,
cutaneous-related conditions, skin colour,
skin reaction to sunlight and sun exposure
Adjusted for family history of skin cancer,
cutaneous-related conditions, skin colour,
skin reaction to sunlight and residence
> 400 m above sea level
BCC, basal-cell carcinoma; SCC, squamous-cell carcinoma; unless otherwise specified, analyses are for the two types together
8
;;
f5
0
z
0
0
'"0
:::c
(/)
6
::
m
\J\
\J\
STUDIES OF CANCER IN HUMANS 91
8 h per week outside and who used sunscreens had the highest incidence rates. The rates in
women who spent the least time outdoors were similar to those who spent more time
outdoors and did not use sunscreens. [The Working Group noted that the high incidence rate
in nurses using sunscreens, despite control for reaction to sunlight, might be due partly to
confounding.]
Table 13. Design features of cohort studies of sun exposure and nonmelanocytic skin cancer
Reference Place Period of Population Sample Response Cases Histological
diagnosis size rate confinnation
Robinson Chicago, IL, Not stated Patients 1000 98% BCC, Not stated
(1987) USA with approx. 350
previous
BCC
Mark Maryborough, 1982-86 Population- 1981 74% 35 SCC; 113 Yes
eta/. Australia based BCC on light-
(1989) exposed
surfaces only
Hunter USA 1980-84 Female 73 366 74% 771 BCC Not routinely
eta/. nurses (self-reported) (records of
(1990) 28 out of
sample of 29
confirmed]
BCC, no. of people with basal-cell carcinoma; SCC, no. of people with squamous-cell carcinoma
(j) Collation of results
The results discussed in this section come from cross-sectional studies by Holman eta/.
(1984a), Engel eta/. (1988), Green eta/. (1988a) and Vitasa et at. (1990), a case-control study
by Kricker eta/. (1991a) and cohort studies by Markset a/. (1989) and Hunter eta/. (1990), all
of which included information pertinent to the association between nonmelanocytic skin
cancer and different aspects of sun exposure. Other studies described individually were not
considered to provide useful information because of various methodological deficiencies.
No data were available on short periods of residence and intermittent exposure, issues which
are addressed for melanoma of the skin.
(i) Total sun exposure: potential exposure by place of residence
Consistent with descriptive data in a case- control study,' migrants to Australia had a
lower risk for squamous-cell carcinoma than did native-born Australians, after adjustment
for host factors related to risk for nonmelanocytic skin tumours. Late age at arrival in
Australia was associated with a lower risk for basal-cell carcinoma (Kricker et al., 1991a).
(ii) Biological responses to total sun exposure
Cross-sectional studies and a case-control study are consistent in showing a strong
relationship between cutaneous indicators of sun. damage and both types of nonmelanocytic
skin cancer. In most studies, the indicators of damage and diagnoses of skin cancer were
made by the same examiner, but cutaneous microtopography, graded without knowledge of
outcome, also showed strong associations.
tS
Table 14. Summary of results of cohort studies of nonmelanocytic skin cancer
Reference Exposure Categories RR Comments
(95% CI)
Marks eta!. Occupation BCC -
>
(1989) Indoors 1.0 Adjusted for age, p = 0.03
fS
Outdoors 1.6
sec
Indoors 1.0 Adjusted for age, p = 0.109
0
z
Outdoors 1.7 0
Hunter et a/. Severe sunburns on face BCC
0
(1990) or arms None 1.0 Adjusted for age; p (trend) = 0.001
1-2 1.40 (1.13- 1.75)
3-5 1.78 (1.42-2.25)
C/l
2! 6 2.91 (2.37-3.58)
a Severe sunburns on face None 1.0 Adjusted for age, time period, region, time
or arms 1-2 1.18 (0.94-1.48) spent outdoors, sunscreen habit, hair co-
3--5 1.34 (1.05--1.71) lour, childhood tendency to sunburn;
2!6 1.90 (1.50-2.40)
p (trend) < 0.001 m
Time spent outdoors during 2: 8 (sunscreen) 1.0 Adjusted for age
VI
VI
summer (h/week) 2: 8 (no sunscreen) 0.59 (0.50-0.69)
< 8
0.71 (0.58-0.88)
Time spent outdoors during .2: 8 (sunscreen) 1.0 Adjusted for age, time period, region,
summer (h/week) 2! 8 (no sunscreen) 0.70 (0.60-0.82) number of sunburns, hair colour, childhood
< 8
0.73 (0.59-0.90) tendency to sunburn
ascc, basal-cell carcinoma; sec, squamous-cell carcinoma
- - - --- - --------------------
STUDIES OF CANCER IN HUMANS 93
(iii) Total sun exposure assessed by questionnaire
No effect of time spent outdoors during summer was seen in a cohort study of basal-cell
carcinoma (Hunter eta/., 1990). In a cross-sectional study of fishermen, cumulative exposure
to UVB radiation was positively associated with the occurrence of squamous-cell carcinoma
but not of basal-cell carcinoma {Vitasa et al., 1990). The different results may be attributable
in part to small numbers and incomplete histopathological confirmation of diagnoses.
(iv) Occupational exposure
In two studies from Australia, outdoor occupation was not significantly associated with
the prevalence of the two types of carcinoma combined (Green et al., 1988a) or with the
incidence of squamous-cell carcinomas (Marks et a/., 1989).
{v) Sunburn
Acohortstudyofbasal-cell carcinoma in the USAshowed a trend of increasing risk with
increasing number of sunburns after adjustment for various factors, including tendency to
sunburn (Hunter eta/., 1990). Number of sunburns showed a nonsignificant positive asso-
ciation with risks for basal-cell and squamous-cell carcinoma of the skin after adjustment for
various constitutional variables, including propensity to burn (Green et al., 1988a).
2.1.2 Cancer of the lip
Assessment of the carcinogenicity of solar radiation for the lip is complicated by the fact
that carcinoma at this site is actually diagnosed as a mixture of cancers of the external lip and
cancers of the buccal membranes (oral cavity). Use of alcohol and tobacco are known causes
of the latter tumours {IARC, 1985, 1986b, 1988).
While there are wide variations in the apparent incidence of cancer of the lip with
latitude, evaluation of the association is difficult because of inconsistency in the definitions of
the boundaries of the lip. 'Cancer of the lip' is defined as cancer of the vermilion border and
adjacent mucous membranes and thus excludes cancers of the skin ofthe lip (WHO, 1977).
Most are squamous-cell carcinomas and are located on the lower lip (Keller, 1970; Lindqvist,
1979), which is more heavily exposed to sunlight than is the upper lip (Urbach et al., 1966).
In general, case reports were not considered, because of the availability of more infor-
mative data. One case report from Nigeria described the occurrence of two lip tumours in
albinos (Onuigbo, 1978).
(a) Descriptive studies
The incidence of lip cancer is 4-10 times higher in men than in women in most white
populations, and higher in whites than in populations of darker skin complexions living in the
same geographical areas (Muir et al., 1987).
{i) Geographical variation
The incidence of lip cancer is higher in rural than in urban areas, in particular among
men (Doll, 1991).
Mortality from and incidence of lip cancer are substantially lower in migrants to
Australia than in native-born Australians {Armstrong et al., 1983; McCredie & Coates,
94 !ARC MONOGRAPHS VOLUME .5.5
1989). Groups of migrants to Israel all show lower risks for lip cancer than the locally born
population (Steinitz et a/., 1989).
(ii) Occupation
As reviewed by Clemmesen (1965), several observations during the nineteenth century
pointed to an increased risk of lip cancer among people in outdoor occupations, in particular
farmers and farm labourers. In England and Wales, increased risks for lip cancer were
reported among agricultural labourers, fishermen, other dock workers and railwaymen
employed outdoors (Young & Russell, 1926). Atkin eta/. (1949) studied the occupations of
1537 men in England and Wales who died from lip cancer between 1911 and 1944. They
reported that mortality from cancer of the lip was 13 times higher among men employed in
agriculture than in men with professional jobs. Excess risks for lip cancer have also been
observed in farmers in western Canada (Gallagher et al., 1984) and in Denmark (Olsen &
Jensen, 1987: Lynge & Thygesen, 1990).
(b) Case-control studies
Keller (1970) compared 301 men with lip cancer admitted to veterans' hospitals in the
USA between 1958 and 1962 with two groups of white age-matched controls admitted to the
same hospitals, comprising 301 oral cancer controls and 265 general controls. Altogether,
59.9% of the lip cancer cases, 37.1% of the cancer controls and 40.6% of the general controls
had been born in the south of the USA. Farming was recorded as the occupation of 27% of
the lip cancer cases but of only 8% of cancer controls and 4% of the general controls [crude
odds ratios, 4.0 and 8.4, respectively]. Any type of outdoor work was recorded for 39% of
cases of lip cancer, for 20% of cancer controls and for 12% of the general controls [crude
odds ratios, 2.6 and 4.8, respectively]. Risk estimates were not adjusted for smoking, another
risk factor identified in the study.
Spitzer et a/. (1975) obtained information by personal interview on 339 men with
squamous-cell carcinoma of the lip registered with the Newfoundland (Canada) Cancer
Registry between 1961 and 1971 and 199 male controls chosen from the electoral register,
matched for age and geographical location in nine census divisions; the overall response rate
was 93%. An association was found between lip cancer and outdoor work (odds ratio, 1.52; p
< 0.05); an odds ratio of 1.50 (p < 0.05) was found for occupation as a fisherman for at least
eight full seasons, after adjustment for outdoor work, pipe smoking and age. No positive
association was found for specific fishing activities, such as use of mouth as a third hand or of
cast nets.
lindqvist (1979) obtained information by mailed questionnaires from 171 cases (149
men, 22 women; 74% response rate) of epidermoid carcinoma of the lip registered with the
Finnish Cancer Registry in 1972-73 and from a control group of 124 patients (56 men, 68
women; 77% response rate) registered with squamous-cell carcinoma of the skin of the head
and neck. Risk estimates were adjusted for age. Odds ratios for men working outdoors
ranged from 2.2 to 3.2 according to the calendar period during which the subjects had worked
outdoors. The odds ratio was significantly increased only for those who both worked
outdoors and smoked. [The Working Group noted that the choice of head and neck skin
cancer patients as controls would lead to an underestimate of the odds ratio for outdoor
work.] -
STUDIES OF CANCER IN HUMANS 95
Dardanoni et al. (1984) obtained information by personal interviews from 53 men with
lip cancer registered in the Ragusa Cancer Registry in Italy and from 106 male controls
matched for age and municipality of residence and admitted to the same hospitals for
non-neoplastic diseases. An association was found between lip cancer and working or
spending at least 6 h each day outdoors (odds ratio, 4.9;p < 0.001). After control for socio-
economic level, the odds ratio was 1.7 (p < 0.001). (The Working Group noted that the latter
p value is inconsistent with the number of subjects.]
2.1.3 Malignant melanoma of the skin
Melanoma of the skin is divided into three major histological types. The majority of
melanomas in white-skinned populations (of European origin) are superficial spreading and
nodular melanomas. Lentigo maligna melanoma-also known as Hutchinson's melanotic
freckle-occurs later in life than the other types, and more specifically on exposed sites;
however, the body site and evidence of sun damage in surrounding skin may influence its
pathological classification (McGovern et al., 1980). Acral lentiginous melanoma has not
been studied epidemiologically; it is rare in white-skinned populations, although it comprises
a substantial proportion of melanomas in Japan (Elwood, 1989a).
(a) Case reports
In general, case reports were not considered, owing to the availability of more
informative data.
In a survey of 830 cases of xeroderma pigmentosum located through published case
reports (Kraemer et al., 1987), melanomas were reported in 37 patients (5% ). As the median
age at last follow-up of these cases was only 19 years, this observation is likely to represent a
substantial excess over the number expected, although the exact nature of the study popu-
lation precludes an accurate comparison. Site was specified for 29 of the 37 cases; 65% of
these were on the face, head and neck (normally constantly UVR-exposed sites) as compared
with 19.4% on this site among affected members of the US general population. [The
Working Group recognized that data collected from previously published case reports are
not uniform and may be atypical of a true incidence or prevalence series. Furthermore, no
information is available on the relationship between solar exposure and the occurrence of
malignant cutaneous melanoma in these patients.]
(b) Descriptive studies
(i) Sex distribution
The sex distribution of melanoma, adjusted for age, varies widely between populations.
In many, it occurs as often as or more commonly in women than in men (Lee & Storer, 1980;
Lee, 1982), in contrast to other types of skin cancer which are uniformly commoner in men
(Muir et al., 1987).
(ii) Age distribution
Age distributions of melanoma in human populations vary with sex (Lee, 1982). They
cannot easily be interpreted because they represent a variable combination of the different
patterns of melanomas at different sites as well as a combination of time trends and trends in
the experience of birth cohorts.
96 IARC MONOGRAPHS VOLUME 55
(iii) Anatomical distribution
Melanoma is proportionately commonest on the back and face in men and on the legs in
women (Crombie, 1981); however, the incidence of melanoma per unit of body area is
similar on fully exposed sites, such as the face, and on partially exposed sites, such as the
lower limbs in women and the back in men. The frequency on body sites that are usually
covered, such as the buttocks, is much lower (Elwood & Gallagher, 1983).
(iv) Ethnic origin
Melanoma is predominantly a disease of white-skinned populations. Rates in dark-
skinned populations are much lower, the age-standardized incidence rate in India being 0.2
per 100 000 compared to around 30 in Queensland, Australia. In Los Angeles, USA, rates
were less than 1 per 100 000 in Japanese and Chinese subjects and 11- 12 in white subjects
(Muir eta/., 1987; Whelan et a/.. 1990). The site and histological distribution of melanoma
are different in non-white populations and have been little studied epidemiologically. The
remainder of this section deals only with melanoma in white populations.
The incidence of melanoma is substantially lower among Hispanics than among other
whites in the USA. For example, the incidence among Hispanics in New Mexico is less than 2
per 100 000 person years, but in other whites it is about 11 per 100 000 (Muir eta/., 1987). In
several case- control studies (described in detail below), subjects with a southern or eastern
European background had lower risks than those with northern European or British origins
(Elwood eta/. , 1984; Holman & Armstrong, 1984a).
In a Canadian study (Elwood eta/., 1984 ), people with an eastern or southern European
background had a crude odds ratio of 0.5 relative to those with an English background. This
effect was not changed appreciably after adjustment for constitutional factors of hair, eye and
skin colour and the skin's reaction to sun exposure. In contrast, the effect of ethnic origin
observed in Western Australia was substantially reduced after adjustment for pigmentation
characteristics (Holman & Armstrong, 1984a).
(v) Geographical variation
Armstrong (1984) showed that the relationship between melanoma incidence in
Caucasians and latitude of residence decreases from around 35 to a minimum around 55
and then rises with latitude due to high rates in Scandinavian and Scottish populations. This
pattern is likely to be due to both latitudinal and pigmentation factors. Within countries,
inverse relationships of incidence or mortality with latitude have been seen in England and
Wales (Swerdlow, 1979), Norway (Magnus, 1973), Sweden (Eklund & Malec, 1978) and
Finland (Teppo et al. , 1978).
In the first comprehensive analysis of the geography of melanoma in whites, Lancaster
(1956) noted that mortality from the disease was higher in Australia and South Africa than in
the parts of Europe from which their populations originated; that mortality in Australia, New
Zealand and the USA increased with proximity to the equator; but that within Europe it was
higher in Norway and Sweden in the north than in France and Italy in the south. These
patterns are also evident in more recent data (Armstrong, 1984).
Geographical variation in relationship to ambient UV irradiation levels: Several studies
have compared melanoma incidence and mortality rates in different areas of North America
to estimated or measured levels of ambient UVR, and Elwood (1989b) estimated the change
STUDIES OF CANCER IN HUMANS 97
in rate for a 10% change in UVR level (Thble 15). [The Working Group noted that these
studies did not assess any other component of the solar spectrum.]
Elwood eta/. (1974) showed, using mortality data for US states and Canadian provinces,
that the correlation coefficients with latitude were 0.79 for men and 0.72 for women. A
variation in latitude of 2 o, which is equivalent to 138 miles, was associated with a change in
death rates from melanoma of about 10%. Annual UV flux at erythema-producing wave-
lengths was calculated from information on latitude and meteorological data on cloud cover.
This calculated index of exposure was very strongly correlated with latitude (correlation
coefficient, 0.89), so melanoma mortality rates were strongly related to this index; a 10%
increase in received UVR dosage would be expected to give an increase of3.7-4.5% in the
death rate from melanoma at latitude 50 , and 6.8-10.3% at latitude 30 o {Thble 15). These
values were somewhat higher for men than for women; for example, 4.4% in men compared
with 3.0% in women at latitude 50 o using the exponential model.
Fears eta!. (1976) related melanoma incidence to latitude and to a calculated measure of
UVR. Their data cover a slightly narrower range of latitude, and they calculated that a 10%
increase in UVR would cause an increase in melanoma mortality of7- 12%, the higher figure
applying to more southerly latitudes, which already have higher rates. Incidence rates vary
more rapidly with latitude than do mortality rates, and therefore they predicted that a 10%
increase in UVR would be likely to give a 14-24% increase in the incidence of melanoma
(see Table 15).
Estimates using calculated UVR levels: Fears et a!. {1977) used measurements from
Robertson-Berger meters for four areas and a power model, in which the calculated
percentage changes are not dependent upon the initial latitude. These calculations showed
considerably stronger effects, with an estimated 25% increase in incidence for a 10%
increase in solar UVR (see Table 15).
Scotto and Fears (1987) used annual UVR counts from Robertson- Berger meters in
seven areas of the USA (Detroit, Seattle, Iowa, Utah, San Francisco, Atlanta and New
Mexico) and data on melanoma from incidence registries (the Surveillance Epidemiology
and End Results system). They fitted a power model and presented analyses by sex and by
body site of the melanoma divided into trunk and lower limb versus head, neck and upper
limb. They obtained data on covariates, including ethnic origin, pigmentation characteristics,
hours spent outdoors during weekdays and during weekends and use of suncreens, suntan
lotion and protective clothing, from telephone interviews with at least 500 households in
each area. Data on the melanoma patients were not available, however. The results predict
greater increases for females than for males, unlike the earlier work. The overall effects of a
10% increase in UVR are a 5.5% increase for trunk and lower limb tumours and a 9%
increase for head, neck and upper limb tumours, averaged over the two sexes. Adjustment for
the various covariates reduces the predicted increases to a 3.5% increase for trunk and lower
limb tumours, and 5.5% for head, neck and upper limb tumours (see Thble 15}.
Pitcher and Longstreth (1991) used data on melanoma mortality over a 30year period
and calculated UV flux on the basis of satellite data from the US National Aeronautics and
Space Administration, including measurements of ozone concentrations at high atmospheric
conditions. The models fitted are complex, as they are fitted for the two sexes, for three
different places covering a range of latitudes, and separately for changes in the annual UV
Table 15. Estimates by Elwood (1989b) of percentage increase in frequency of melanoma among whites with a 10%
increase in solar ultraviolet radiation, based on differences with latitude in Canada and the USA
Ultraviolet radiation level Model 50 latitude
derived from
0
Incidence Mortality
Calculation of erythema- Linear 4.5
weighted index Exponential 3.7
Calculation of erythema-
weighted index
Exponential 14.0 7.0
RB meter (1974) Power 25.0
RB meter (1978-81) Power
'Ihmk and lower limb
Crude 5.5
Adjusted 3.5
Head, neck and upper limb
Crude 9.0
Adjusted 5.5
1btal
Crude 6.7
Adjusted 4.2
Calculation of erythema- Power
weighted estimate from Annual 3.2
NASA including satellite Peak 7.0
ozone column measurements Exponential
Annual 2.1
Peak 5.8
Both sexes (simple average ofsex-specific results)
ORB, Robertson-Berger; NASA, National Aeronautics and Space Administration
bMortality data, USA and Canada 1950-67 by state/province; 58 areas
30 latitude References on which
estimates based
Incidence Mortality
6.8
10.3
Elwood et a/. (1974f
23.5 12.0 Fears et a/. (1976)c
25.0 Fears er a/. (1977)d
Scotto & Fears
(1987l
5.5
3.5
9.0
5.5
6.7
4.2
Pitcher &
3.2
7.0
Longstreth (1991/
4.5
8.2
CJncidence data. Third National Cancer Survey (1969-71) for nine areas; US mortality by state. Calculation based on latitude equivalent to
change in ultraviolet radiation
<lrncidence data, Third National Cancer Survey (1969-71) for four areas
"'ncidence data, Surveillance Epidemiology and End Results Program for seven areas. Crude results take account only of age; adjusted results
are controlled for ethnic origin, hair or skin colour, suntan lotion use and hours spent outdoors; total, for comparison, is based on 67% trunk
and lower limb and 33% head, neck and upper limb tumours
!Mortality data by US county 1950-79; estimates of changes in mean annual dose and in peak doses (clear day in June); estimates using DNA
action spectrum were also made and were 1-8% higher than those shown.
(")
0
z
0
0
::I:
Cll
6
r
c
tT1
VI
VI
STUDIES OF CANCER IN HUMANS 99
flux and changes in the peak levels in clear summer conditions. Larger effects were again
found for males than for females, and a larger effect when using the peak measurements than
when using the annual measurements. The overall estimates of the percentage increase in
melanoma mortality associated with a 5% decrease in ozone level, on the assumption that
this is roughly equivalent to a 10% increase in solar UVR, ranged from 2.1 to 7.0 at 50 oN and
from 3.2 to 8.2 at 30 ON (see Thble 15}.
(The Working Group noted that, despite the sophistication of some of the mathematical
models, these results are derived from population-based descriptive data and not from
individual measurements and are restricted to North America.)
(vi) Migration
The most informative data on risk in migrants come from Australia, New Zealand, Israel
and the USA Native residents of Australia (McCredie & Coates, 1989; Khlateta/. , 1992) and
New Zealand (Cooke & Fraser, 1985), mostly of British origin, experienced incidence and
mortality rates of melanoma roughly twice those of British immigrants. Native Israelis had a
risk at least twice that of immigrants to Israel from Europe for at least 30 years after
immigration (Steinitz eta/., 1989).
The higher incidence in white immigrants to Hawaii from the US mainland compared
with white natives has been attributed to a difference in skin colour (Hinds & Kolonel, 1980).
Non-Hispanic migrants to Los Angeles County (California, USA) from higher latitudes in
the USA are still substantially protected against melanoma of all histological types decades
after migration. Similar relative protection is enjoyed by native residents of more northerly
US communities in comparison with co-resident migrants from the south-western USA
(Mack & Floderus, 1991).
(vii) Socioeconomic status and occupation
Melanomas are much commoner in higher socioeconomic groups, as shown in data from
the United Kingdom since 1949-51. In the United Kingdom, the distribution of melanoma in
married women by social class (categorized by their husbands' social class) is similar to that
of men, indicating that this is a social rather than a specific occupational factor (Lee, 1982).
In the USA, the risk increases with income for men aged 30-69; at age 70 and above, the
trend is reversed, suggesting a role for long-term exposure to the sun (Kirkpatrick et a/.,
1990). In case- control studies, the effect of socioeconomic status is weakened after adjust-
ment for measures of exposure to the sun (Gallagher eta/., 1987; 0sterlind eta/. , 1988b).
Assessment of outdoor exposure on the basis of routine data on job descriptions showed
that melanoma is commoner in indoor than in outdoor workers, even within the same socio-
economic group (Lee & Strickland, 1980; Lee, 1982). Cutaneous melanoma incidence rates
during 1972-76 in New Zealand showed no pattern according to outdoor workplace (Cooke
eta/., 1984). An analysis of 3991 cases of cutaneous melanoma registered during 1971- 78 in
England and Wales and of 5003 cases registered during 1961-79 in Sweden suggested an
elevated incidence in professional occupations. The incidence among farmers was close to
that expected (Vagero et a/., 1990).
Garland et a/. (1990) reported 176 incident cases of melanoma among US Navy
personnel. The rate for indoor occupation was higher than that for outdoor workers.
100 IARC MONOGRAPHS VOLUME 55
(c) Case-control studies
Elements of each case-control study described below are given in Thble 16.
(i) Australia
Lancaster and Nelson (1957) carried out a case-control study on 173 patients aged over
14 years treated for malignant melanoma in hospitals in Adelaide, Melbourne and Brisbane,
and 173 hospital controls with cancers other than of the skin, matched for sex and age.
Information was obtained by interviews [response rate not given], and analysis was done by
single factor cross-tabulations only. Unmatched crude odds ratios were calculated by the
Working Group. Skin [odds ratio, 1.95 for fair versus olive and medium), hair colour [odds
ratio, 1.7 for fair and red versus black and brown), eye colour [odds ratio, 1.75 for blue and
green-grey versus brown and hazel] and skin reaction to sunlight [2.9; 95% Cl, 1.9-4.5 forred
versus brown reaction} were significantly associated with risk for malignant melanoma.
Among the other factors studied were birth outside Australia [0.8; 0.4-1.6], 10 years' or more
occupational exposure to sunlight in males [1.4; 0.7-2.7), sunbathing {1.5; 0.9-2.4] and
moderate (1.2; 0.5-3.1] and excessive (2.3; 0.8-6.3) total exposure to the sun compared to
minimal exposure. There were only eight cases and 11 controls in the latter category of sun
exposure.
Beardmore (1972) studied 468 cases of histologically confirmed malignant melanoma
and 468 sex- and age-matched hospital controls (including patients with skin cancer) at one
hospital in Brisbane. Information was obtained by interview [response rate and method of
evaluation of hair, skin and eye colour not given]. Hair, skin and eye colour and skin reaction
to sunlight were not associated with risk for malignant melanoma. Comparison of exposure
to sunlight from mainly outdoor occupations to that from mainly indoor occupations resulted
in a crude odds ratio of [1.42; 95% CI, 1.03- 1.97]; a similar comparison for recreational
activities gave a crude odds ratio of[l.03; 0.75-1.42]. Fewer cases than controls had a history
of treatment for keratosis and/or skin cancer or currently had keratosis and/or skin cancer
[crude odds ratios, 0.51, 0.38-0.69; and 0.16, 0.12-0.22, respectively).
In the Western Australia Melanoma study (Holman & Armstrong, 1984a,b), 511 cases
aged 10-79 years and 511 population controls matched for sex, age and area of residence
were interviewed at home using a questionnaire based on that of the Western Canada study,
which included objective measurements and naevi counts. The study also included a review
of pathology slides. Analyses were presented for superficial spreading, nodular and lentigo
maligna melanomas and for a fourth, unclassifiable group. Response rates were 76% for
cases and 62% for controls, and adjustment was made for chronic and acute skin reaction to
sunlight, hair colour, ethnic origin and age at arrival in Australia using a multiple logistic
regression model. Hair colour, acute and chronic reaction to sunlight, number of naevi and
family history of melanoma were significantly associated with risk; skin and eye colour were
significantly associated in a crude analysis only. Duration of residence in Australia was
strongly, positively associated with risk for all melanomas and for all sub-types except for
unclassifiable melanoma. After control for ethnic origin, the odds ratios for superficial
spreading melanoma were 1.2 (95% CI, 0.25-5.5) for people arriving in Australia at age 0-4,
1. 7 (0.34-8.0) for those arriving at age 5-9, 0. 74 (0.17-3.3) for those arriving at age 10-14,
0.25 (0.05-1.4) for those arriving at age 15-19 years or older ( < 30 years) and 0.38
STUDIES OF CANCER IN HUMANS 101
(0.19-0.78) for those arriving at age> 30 years (p for trend, < 0.0001) compared to those
born in Australia. A lifetime residential history was used to calculate the mean annual hours
of bright sunlight based on place of residence as a measure of potential exposure to the sun.
An analysis restricted to native-born Australians showed positive associations for all
melanomas and for each subtype except nodular melanoma. An analysis dichotomizing
exposure at an annual mean of > 2800 h sunlight at different ages showed that the highest
risk ratio for all melanomas and for the superficial spreading subtype were for high exposure
at ages 10-24. Cutaneous microtopography was used to measure skin damage; a positive
association was found with all melanomas, being strongest for lentigo maligna melanoma.
In a further analysis by individual habits of exposure to the sun (Holman eta/., 1986a), no
significant association was seen for total outdoor exposure. Analysis by recreational outdoor
exposure, expressed as a proportion of total exposure, at ages 10-24 years showed no
significant association. For superficial spreading melanoma, analysis by specific activity
showed positive associations with boating (p = 0.04) and fishing (p = 0.07) and weaker,
nonsignificant associations with swimming and sunbathing at ages 15-24 or 0-9 years before
diagnosis. For other types of melanoma, no clear positive association was found; regular
swimmers had a lower risk of lentigo maligna melanoma (trend test significant). Occupa-
tional exposure was analysed on the basis of whether the site of the melanoma was usually
covered by clothing and compared to that of a referent group for whom the site was usually
covered: subjects for whom the site was exposed showed a significant positive association. In
comparison with the same referent group, patients who had never worked outdoors had
significantly increased risks for all melanomas. The type of bathing suit usually worn by
females in summer was assessed, and a positive association was found for wearing bikinis or
for nude bathing, which was significant for all trunk melanomas and for superficial spreading
melanoma on the trunk. When previous sunburns were classified by severity, no significant
trend was observed for all melanomas; but there was a positive trend for lentigo maligna
melanoma (p = 0.06) and a significant negative association for nodular melanoma.
In the smaller Queensland Melanoma study (Green, 1984; Green eta/., 1985a), 183
patients with histologically confirmed melanoma, other than lentigo maligna melanoma or
acrallentiginous melanoma, and 183 population controls matched for sex, age and area of
residence were interviewed at home using a standardized questionnaire, which incJuded
objective measurements and naevi counts. The response rates were 97% and 92%, respec-
tively. Adjustment was made using a multiple logistic regression model. Hair colour, acute
sun reactions and naevi were significantly associated with risk. Skin colour, eye colour,
chronic sun reaction, freckling and family history of melanoma were significant in a crude
analysis only. Hours of occupational and recreational exposure to the sun from 10 years of
age across three categories gave risks of 1, 3.2 (95% CI, 0.9-12.4) and 5.3 (0.9-30.8) after
adjustment for naevi, hair colour and propensity to sunburn. Average levels of exposure to
UVB radiation were also allocated by residential history but showed no association with risk
for melanoma. People born in Queensland had moderately higher risks than those who
arrived there later in life or who had lived somewhere else at any time. Melanoma patients
had more kerotoses or skin cancers on their faces (odds ratio, 2.8; 1.1-7 .2). Sunburn (Green
eta/., 1985a) was defined as pain persisting longer than 48 h, with or without blistering, and
was recorded as the number of episodes in each decade. Risk increased with the number of
102 IARC MONOGRAPHS VOLUME 55
severe sunburns and was 1.9 and 5.0 in the two higher categories on matched analysis,
decreasing to 1.5 (0.7-3.2) and 2.4 (1.0-6.1), respectively, when adjusted for naevi and exact
age. An additional analysis of 49 cases of lentigo maligna melanoma and 49 controls showed
no association with sunburn (Green & O'Rourke, 1985; Green et al., 1986).
In a more detailed review of these data (Green eta/., 1986), no association was observed
with occupational exposure to the sun. Analyses of recreational hours spent on the beach in
the sun were made for lifetime exposures, exposures at 10-19 years of age and exposures in
the five years prior to diagnosis; no strong or consistent association was seen in either crude
or adjusted analyses. Associations with total accumulated hours of exposure to the sun
(calculated by adding occupational and total recreational exposures) showed a positive trend
for lifetime exposure and exposure at ages 10-19 (odds ratio, 4.4; 95% CI, 1.8- 184.5), but no
association was seen for exposure during the previous five years. Analysis of levels of UVR by
lifetime residential history showed no major association and no site-specific association.
(ii) Europe
In a case-control study of residents of Oslo, Norway (Klepp & Magnus, 1979), 78 mali-
gnant melanoma patients over 20 years of age were compared with 131 unmatched hospital
controls with other cancers. Both cases and controls with advanced disease were excluded.
Information was obtained by questionnaire [response rate not given]. Hair and eye colour
were recorded independent1y by the interviewer and subject but were not associated with risk
for the disease, whereas skin reaction to sunlight and freckling were. A nonsignificant odds
ratio of [ 1.5] was found for men working outdoors for more than 3-4 h/day; the odds ratio for
taking sunbathing holidays in southern Europe was 2.4 (p = 0.05). No significant association
was seen with degree of exposure of different body sites, classified from ' as often as possible'
to 'hardly ever'.
Adam et al. (1981) conducted a population-based case-control study in the United
Kingdom of 111 female cases of malignant melanoma aged 15-49 traced from registries and
342 female controls randomly selected from general practitioners' lists and matched for age
and marital status. Information was obtained by postal questionnaire; response rates were
66% for cases and 68% for controls. Hair colour and skin reaction to sunlight, but not skin
colour, were significantly associated with risk for malignant Slightly more cases
than controls reported deliberately tanning their legs or trunk, either at home or abroad. No
difference was reported in the amount of work, leisure or total time spent outdoors. {The
Working Group noted that the study concentrated on oral contraceptive use and that
information on exposure to the sun was very limited.)
MacKie and Aitchison (1982) conducted a case-control study in western Scotland of 113
malignant melanoma patients aged 18-76 years and 113 sex- and age-matched hospital
controls with conditions not related to the skin. Cases of lentigo maligna melanoma were
excluded. Information about exposure to the sun within the previous five years was obtained
by questionnaire [response rate not given) and included occupational and recreational
exposure(;;?::: 16 h versus < 16 h outdoor exposure per week) and history of severe sunburn,
defined as either 'blistering sunburn' or 'erythema persisting for a week or longer'. Other
factors included in the multivariate analysis were social class and skin type. A significant
negative association was observed for recreational exposure and for occupational exposure
STUDIES OF CANCER IN HUMANS 103
to the sun in males. A significant positive association was observed for severe sunburn. No
significant difference was observed for the number of continental holidays taken or total
number of days spent in sunnier climates.
Sorahan and Grimley (1985) studied 58 patients aged 20-70 years with cutaneous mali-
gnant melanoma (other than lentigo maligna melanoma) in two hospitals in the United
Kingdom and 182 hospital controls with diseases other than of the skin and 151 unmatched
controls from electoral rolls. The response rates were 64% for cases and 60% for each
control group. Information was obtained by postal questionnaire, and analyses were adjusted
using a multiple logistic regression model. A significant positive association was observed for
number of bouts of painful sunburn ever experienced, with an odds ratio reaching 7.0 for five
or more bouts compared to none. A significant positive association was also seen with the
number of holidays ever spent abroad in a hot climate, reaching 6.5 for 21 holidays or more,
compared to none. Both associations were weakened, and the latter became nonsignificant,
after adjustment for propensity to sunburn, number of moles and history of sunburn.
In another study in the United Kingdom (Elwood eta/., 1 9 8 6 ~ 83 histologically con-
firmed cases over 18 years of age and 83 hospital controls (in- and out-patients), matched for
sex, age and area of residence, were interviewed at home using a questionnaire which
included objective measurements and naevi counts. The responses were validated by replies
to a postal questionnaire. The response rates were 74% for cases and 92% for controls.
Adjustment was made using a multiple logistic regression model. Skin reaction to sunlight,
freckling and naevi were significantly associated with risk. A history of sunburn causing pain
for two days or more gave a significant odds ratioof3.2 (95% CI, 1.7-5.9). Past outdoor occu-
pational exposure showed a significantly reduced odds ratio of 0.2 (0.1-0.9) for the second
highest category but a nonsignificant odds ratio of 1.7 (0.3-8.6) for the highest category and
no overall trend.
In northern Italy, Cristofolini eta/. (1987) compared 103 patients aged 21-79 under
treatment for cutaneous malignant melanoma at one hospital with 205 hospital controls with
diseases other than skin tumours. Subjects were interviewed [response rate not given] and
assessed by a dermatologist. Adjustment was made using a multiple logistic regression
model. Hair and skin colour and family history were significantly associated with risk, but eye
colour, freckling and number of naevi were not. A history of frequent sunburn as an adult
gave an odds ratio of 1.2 (95% CI, 0. 7- 2.1) and that of severe sunburn in early life an odds
ratio of 0.7 (0.4-1.2). Heavy or frequent exposure to sunlight during the previous 20 years,
categorized as yes or no, gave a significantly reduced odds ratio of 0.6 (0.4-0.95}. Outdoor
compared to indoor occupation gave a nonsignificant odds ratio of 0.9 (0.5-1.7), and a
history of carcinoma of the skin gave a risk ratio of 0.4 (0.02-2.9), based on small numbers.
Melanoma at exposed sites showed positive associations with heavy sun exposure (1.44;
0.8-2.8) and outdoor occupation (1.8; 0.9-3. 7), while melanoma at normally unexposed sites
showed a significant negative association with heavy exposure to the sun (odds ratio, 0.25;
95% CI, 0.13- 0.47).
In a study of melanoma in eastern Denmark (0sterlind et al. , 1988b,c; 0sterlind, 1990),
474 cases of melanoma, excluding lentigo maligna melanoma patients, aged 20-79 were
compared with 926 population controls and matched for sex and age. Subjects were inter-
viewed at home using a questionnaire which included objective measurements and naevi
104 IARC MONOGRAPHS VOLUME 55
counts, and adjustment was made using a multiple logistic regression model. Response rates
were 92% for cases and 82% for controls. The number of sunburns (defined as those causing
pain for two days or longer) before age 15, from age 15 to 24 and over the previous 10 years
were all significantly associated with risk: crude odds ratios for the maximal categories, 3.7
(95% CI, 2.3- 6.1), 2.4 (1.6-3.6) and 3.0 (1.6-5.4), respectively. Adjustment for sex and host
factors, including naevi, freckles and hair colour. reduced the risk ratios, but they remained
significant. Adjustment for sunburns before age 15 rendered the associations with later sun-
burn weak and nonsignificant. Joint analysis of sunburns and naevi suggested independent,
additive risks. Significantly increased risks were seen with residence near the coast before
age 15 or for more than 30 years. Specific recreational activities were investigated and cate-
gorized by the number of years of regular participation, adjusted for sex and host factors,
including number of naevi, and for other activities. Significant positive associations were
observed with sunbathing, boating, winter skiing and swimming, the latter becoming non-
significant after adjustment. Regular participation in gardening, ball games, golf, horseback
riding or hiking was not associated with risk for melanoma. A positive trend was seen with
vacations spent in beach resorts in southern Europe (odds ratio, 1. 7; 95% CI, 1.2- 2.4), which
was weakened after adjustment for sunbathing and sunburn (1.4; 1.0-2.1). Socioeconomic
status showed a strongly positive association in men, which became nonsignificant when
adjusted for sunburn and recreational exposure to the sun. Occupational exposure outdoors
for at least six months was associated with a significantly reduced odds ratio of0.7 (0.5-0.9) in
men; the protective effect was most pronounced in men who started working outside at an
early age and continued for at least 10 years. No association was seen with skin grading
categories defined by microtopography.
In a study in northern Italy (Zanetti eta/. , 1988), 208 cases of histologically confirmed
malignant melanoma were identified from the regional tumour registry and were compared
with 416 controls chosen from the National Social Service Registry. Response rates were
87% for cases and 68% for controls. An increased risk was observed with light hair colour,
tendency to burn and a history of sunburn in childhood. No significant effect of region of
origin was observed. Exposure to the sun was assessed by activity: for outdoor work, a
nonsignificant increased risk was seen with the maximal duration of exposure(> 33 years) in
men, but the overall trend was nonsignificant. Outdoor sports, assessed by years of
participation, showed an increased risk at the maximal level in men and women (significant
for men). A significantly increased risk was found for men participating in sports categorized
as involving the greatest exposure to the sun. A nonsignificantly increasing trend in men was
observed for total number of weeks' holiday, but little effect was seen in women; a significant
positive trend was observed in men, but not for women, for the number of weeks spent at the
seaside in childhood. Similar exposure in adult years resulted in a nonsignificant positive
trend.
Garbe et al. (1989) studied 200 malignant melanoma patients at a dermatological
follow-up clinic in Berlin, Germany, in 1987 and 200 controls from the same clinic who had
any other skin disease (response rate, 90% ). Subjects of non-German origin were excluded,
as were those seeking consultation for pigmented naevi or who had been treated previously
by UVR (10% ). Occupational exposure to the sun, assessed as none, sometimes or nearly all
the time, showed a strongly increased risk up to an odds ratio of 5.5 (1.2-25.3 ). No significant
STUDIES OF CANCER IN HUMANS 105
relationship was found with duration of leisure-time exposure to the sun or number of sun-
burns. [The Working Group noted that little detail was given about exposure and that the
control group consisted of patients with other skin disease.]
Weiss eta/. (1990) studied 1079 cases of malignant melanoma reported to the German
Dermatological Society Registries in 1984-87 and 778 hospital controls from the same
clinics. Positive associations were seen with occupational exposure to the sun, which
increased with the number of years of exposure. No association was seen with exposure to the
sun during leisure time or with sunbathing. [The Working Group noted that this study
appears to overlap with that of Garbe eta/. (1989) and that the data were presented with
relative risks but with no test of significance.]
BeitneF eta/. (1990) studied 523 incident cases of malignant melanoma seen at a hospital
in Stockholm, Sweden (representing 64% of all cases registered in Stockholm County), and
505 controls selected from the population register for Stockholm County. Cases completed a
questionnaire while waiting at the clinic, and controls received the questionnaire by mail
(response rates, 99.6% and 96.2 %, respectively). A significant positive effect was seen for the
number of sunbathing sessions each summer, with a history of erythema after sunbathing and
with sunbathing vacations abroad. Residence in countries around the Mediterranean or in a
sub-tropical or tropical climates for more than one year during the previous 10 years gave a
significant odds ratio of 1.9 [95% CI, 1.0- 3.6]. There was no increase in risk with sunbathing
during winter vacations at high altitudes. Outdoor workers had a significantly reduced risk of
0.6 (0.4-1.0) after adjustment for age, sex and hair colour.
Elwood eta/. (1990) studied 195 cases of superficial spreading or nodular melanoma in
people aged 20-79 from five pathology laboratories in the United Kingdom and 195 controls
chosen from among all in- and out-patients in the region. Cases and controls underwent an
interview and a limited examination by an interviewer in their homes (participation
rate- cases and controls, 73%; voluntary response rate-cases, 91%; controls, 78%). Risk
was significantly increased with sunburn at age 8-12 (odds ratio, 3.6; 1.4-11.2}, but no
significant increase was observed with sunburn at age 18-22 or with sunburn received 18- 20
or five years prior to diagnosis. No other sun exposure variable was reported.
Grob eta/. (1990) compared 207 consecutive white patients, 18-81 years old, with histo-
logically confirmed invasive melanoma (at least level 2; lentigo melanoma and acral
lentiginous melanoma excluded) seen in one dermatology clinic in Marseilles, France, with
295 controls. Controls under 65 years of age were chosen from among subjects interviewed
after reportedly random selection and examined at a public health centre; those over 65 were
chosen from among out-patients with non-cancer and non-dermatological conditions.
Patients and controls were examined and interviewed by the same dermatologist. Multiple
logistic model analysis was used. The risk for melanoma was increased significantly in
association with annual outdoor leisure exposure during the previous two years (odds ratio,
8.4; 95% CI, 3.6-19.7), outdoor occupation (6.0; 2.1- 17.4) and total lifetime sun exposure
(odds ratio for maximum category, 3.4; 1.6-7.1). There was a nonsignificant association with
sunburns in recent years (1. 7; 0.63-4.6) after adjustment for number of naevi, maximal depth
of suntan, hair colour, social level, complexion and age. (The Working Group found the study
106 IARC MONOGRAPHS VOLUME 55
difficult to interpret because of the nature of the control group and the relative recency of
measurements of exposure to the sun.]
In a report designed to produce a risk prediction model, MacKie et al. (1989) studied 280
cases of invasive cutaneous malignant melanoma (level2 or deeper) from Scottish melanoma
registries. Controls were 280 hospital patients with non-dermatological diseases. Response
rates were 76% for cases and unknown for controls. An increased risk was observed for
history of severe sunburn (adjusted odds ratio, 7.6 (95% CI, 1.8-32.0) for men and 2.3 (0.9-
5.6) for women). A significant positive association for tropical residence was noted for men,
which became nonsignificant after adjustment. (The Working Group noted that, apart from
tropical residence, no data were presented on exposure to the sun.]
(iii) North America
Gellin et al. (1969) studied 79 patients, aged 30-79, with histologically confirmed mali-
gnant melanoma at one hospital in New York, USA. and compared them with 1037 hospital
controls with skin conditions other than cancer. Information was obtained by interview and
examination [response rate not given]. The odds ratios for duration of daily outdoor activity
were [2.8 (95% CI, 1.3-5.8)] for 6 hor more and [4.1 (2.5-6.8)} for3-5 h, compared to 0-2 h.
(The Working Group noted that the controls had skin diseases.)
Paffenbarger et al. (1978) reported on cases found by follow-up of subjects first exa-
mined when entering Harvard University in 1916-50 and the University of Pennsylvania in
1931-40. Out of a total of 50 000 male subjects and 1.71 million person-years of observation,
45 deaths from melanoma were observed and each compared to four controls born in the
same year, who were classmates and who had survived as long as the case subjects. Of the
many factors investigated, only outside remunerative work was associated with a significant
risk for melanoma (odds ratio, 3. 9; p = 0.01 ). Within the cohort, students from New England
had a 50% lower risk for melanoma than other students, presumably owing to more northerly
residence.
Lew eta/. (1983) carried out a study in Massachusetts on 111 cases of cutaneous mali-
gnant melanoma, aged 23-81, followed at one hospital and 107 controls who were friends of
cases, matched by age and sex. Information was obtained by interview at the clinic; response
rates were 99% for cases and 90% for controls, and analysis was made using a logistic
regression model. Cases showed poorer tanning ability, and a significant association was
observed with blistering sunburn during adolescence (odds ratio, 2.1; 95% Cl, 1.2-3.6) and
with 30 days or more vacation in sunny, warm places during childhood (2.5; 1.1-5.8). The
association with history of sunburn persisted after controlling for tanning ability. [The
Working Group noted that the nature of the controls and the simplicity of the analyses
presented make interpretation of the results difficult.]
Rigel et al. (1983) analysed data on 114 melanoma patients(out of a total of328)seen in
a referral centre in New York between 1978 and 1981, and on 228 controls who were staff and
patients at the centre. Significantly increased risks were seen with > 2 h per day sun exposure
11-20 years previously (odds ratio, 2.5;p = 0.005) and outdoor versus indoor recreation (2.4;
p = 0.01). [The Working Group noted that the selection of subjects and the nature of the
control group make these results difficult to interpret.]
STUDIES OF CANCER IN HUMANS 107
In the Western Canada Melanoma case-control study {Elwood et al., 1984, 1985a,b),
carried out in four Canadian provinces, 595 cases of malignant melanoma, aged 20-79, and
595 population controls, matched for sex, age and province of residence, were questioned by
trained interviewers at their homes (response rates: cases, 83%; controls, 48-59% ). Cases of
lentigo maligna melanoma and acral lentiginous melanoma were excluded. Analyses were
made using a multiple logistic regression model. Significant positive associations were found
after adjustment for host factors and ethnic origin for frequent recreational {odds ratio, 1.7;
95% CI, 1.1- 2. 7) and holiday exposure (1.5; 1.0-2.3) and with the number of sunny vacations
per decade (1.7; 1.2- 2.3). No overall trend was observed for occupational exposure, but a
significantly increased risk was associated with moderate occupational exposure, defined as
seasonal or short-term occupational exposure. Maximal occupational exposure was asso-
ciated with a significantly reduced odds ratio in men (0.5 [CI not given}) but not in women
{1.5 [ CI not given]). Analysis of total annual exposure to the sun from all sources showed no
overall trend (odds ratio, 1.0-1.6 in various categories above the minimal exposure referent
group). Severe or frequent sunburn in childhood resulted in a nonsignificant odds ratio of
1.3, after adjustment for host factors and sun sensitivity. From variables relating to sunburn
on vacation and the usual degree of suntan in winter and summer, positive associations were
observed for increasing sunburn and with decreasing usual tan. Cross-tabulation of sunburn
with tendency to sunburn (skin type) did not change the significant positive effect of tendency
to burn, but the odds ratio for sunburn fell from 1.8 in the maximal category to 1.4 (p > 0.2)
after adjustment for sun reaction. Similarly, cross-tabulation of usual degree of suntan
against skin type gave little difference in the positive association with reaction to the sun, but
a weakening of the association with usual degree of suntan was seen which became
nonsignificant. A multivariate analysis including history of sunburn, usual degree of suntan,
skin type and host factors showed significance for the two latter factors, nonsignificant
positive effects of holiday sunburn and a significant negative effect of usual degree of suntan.
These results are interpreted as showing a primary association with tendency to bum easily or
to tan poorly rather than with history of either sunburn or suntan. For men, a significant
negative association was seen with outdoor occupation, but this weakened and became
nonsignificant when adjusted for recorded exposure to the sun. Similarly, the crude odds
ratio for upper compared to lower socioeconomic groups was 3.8 (2.0-7.4) but was reduced
to 2.3 (1.0-5.1) after adjustment for host factors and for occupational, recreational and
holiday sun exposure (Gallagher et al. , 1987).
Elwood et a/. (1987) made an analysis separating superficial spreading melanoma,
nodular melanoma and lentigo maligna melanoma in the western Canada study, based on
415, 128 and 56 cases, respectively. Recreational exposure, holiday exposure and the number
of sunny vacations per decade were positively and significantly (trends) associated with
superficial spreading melanoma (odds ratios, 1.4, 2.0 and 2.2; 95% CI, 1.0-2.0, 1.4-2.9 and
1.5-3.3, respectively); recreational exposure was also positively associated with nodular
melanoma (2.4; 1.3-4.5), but neither holiday exposure nor the number of sunny vacations
showed an association. None of these measures of intermittent exposure was significantly
associated with lentigo maligna melanoma. Occupational exposure showed no significant
association with any of the three types. History of sunburn showed positive but nonsignificant
108 IARC MONOGRAPHS VOLUME 55
associations with superficial spreading and lentigo maligna melanomas but not with nodular
melanoma.
Brown eta/. (1984) identified 120 men who had been aged 18- 31 during the Second
World War from among 1067 patients seen at a melanoma clinic inN ew York City in 1972-80
and sent them questionnaires (response rate, 74% ). Controls were 65 age-matched subjects
attending the same dermatology department with skin diseases other than melanoma
[response rate unknown]. Within the total of 74 cases and 49 controls who had been in the
armed services, the odds ratio for service in the tropics as compared to service in the USA or
Europe was [7.7; 95% CI, 2.5-23.6).
In a-hospital-based study in Buffalo, NY, USA (Graham eta/., 1985}, 404 cases of cuta-
neous malignant melanoma referred to the Roswell Park Memorial Institute, aged from
under 30 to over 65, were compared with 521 controls with other neoplasms at the same
institute, using questionnaires completed on admission. There was a weak negative trend
with total number of hours of exposure to the sun, which was significant in men; a similar
trend was observed for average annual exposure to the sun. Occupational exposure to the sun
gave a nonsignificant reduction in risk in men in the highest exposure group after adjustment
for tendency to burn. Multivariate analysis showed a negative association with cumulative
exposure to the sun, which was significant in men when adjusted for tendency to burn,
freckling and light complexion. Results specific to recreational or holiday exposure to the sun
were not presented.
Dubin eta/. (1986) compared 1103 cases of melanoma seen at the New York University
Medical Center from 1972 to 1982 (mostly in 1977-79) to 585 controls interviewed in 1979-
82 at the skin clinic for conditions excluding cancer. Both cases and controls were inter-
viewed by physicians; response rates were 98% for cases and 78% for controls. In order to
complete the data on risk factors, a postal questionnaire was sent requesting information on
exposures to fluorescent lights and to the sun and on skin colour (response rates, 45% of
cases and 30% of controls). Mostly outdoor compared to mostly indoor work gave an odds
ratio of 2.5 (95% CI. 1.4- 4.4} and mostly outdoor compared with mostly indoor recreation
gave an odds ratio of 1.7 (1.2-2.3), although mixed indoor and outdoor recreation gave a
significantly reduced risk of 0.6 (0.5-0.8). Overall exposure to the sun (three categories)
showed no trend. A history of the presence of solar keratosis gave a significant risk ratio of
5.0 (2.3-10.5). Quantitative total sun exposure was assessed for 623 cases and all585 con-
trols: there was no significant trend with total hours of exposure to the sun per day 0- 5, 6-10
or 11- 20 years before diagnosis. [The Working Group noted that the cases and controls were
not interviewed over the same period.]
In a study based on a subset of the above (Dubin eta/., 1989), 289 cases and 527 controls
were interviewed using the same method (response rates, 100% of eligible cases; 70% of
controls [ 19% of potential controls were excluded because of diagnosis of a lesion known to
be caused by exposure to the sun]). Mostly outdoor occupation gave a nonsignificant ele-
vated risk. Mostly outdoor recreation was associated with a significantly elevated risk in light
tanners but a nonsignificant elevated risk in dark tanners (interaction nonsignificant).
Overall exposure to the sun was associated with significantly increased risks in all groups. A
history of sunburn was associated with a significantly increased risk in light tanners and in all
subjects but had a nonsignificant protective effect in dark tanners (interaction significant).
STUDIES OF CANCER IN HUMANS 109
When analysed by age group, a history of sunburn gave a positive association at age 20-39, a
weak association at 40-59 and a negative association at 60 or over (interaction significant).
Prior skin cancer or solar keratosis had a significant effect, which was stronger in men than in
women (interaction nonsignificant).
In a study in San Francisco, Holly et al. (1987) compared 121 patients with nodular or
superficial spreading melanoma at a university melanoma clinic with 139 controls from a
medical screening clinic or from an orthopaedic clinic at the same centre. Response rates
were 'over 95%'. Sunburn score, based on the number of blistering sunburns during school
and young adult years, showed a significant odds ratio of 3.8 (95% CI, 1.4-10.4) after
controlling for naevi, hair colour and previous skin cancers. A positive association was seen
with previous skin cancer (3.8; 1.2-12.4).
Weinstock et al. (1989) reported a case-control study within a cohort of US nurses (see
Hunter et al., 1990, p. 86). Data on 130 cases and 300 controls (response rates to post-
diagnosis questionnaire, 85% and 81%, respectively) were analysed using multivariate
models. Following adjustment for skin sensitivity, significant positive effects were seen for
sunburn at ages 15-20 (odds ratio, 2.2; 95% CI, 1.2-3.8), but not at age> 30 (1.3; 0.7-2.3),
and for residence at a southern latitude at age 15-20 (2.2; 1.1-4.2), but not at age> 30 (1.6;
0.9-2.8). No direct recording of exposure to the sun was reported.
A further analysis (Weinstock et a/., 1991a) assessed the use of swimsuits in these
subjects. There was a significant positive association of melanoma risk with the frequency of
use of swimsuits of any type in sun-sensitive women (odds ratio, 6.4; 95% CI, 1.7-23.8) but
not in sun-resistant women (0.3; 0.1-1.0). After controlling for type of swimsuit and sensi-
tivity factors, melanoma risk was increased with increasing hours per day of outdoor swimsuit
use (any type) after age 30, but no association was seen with intensity of exposure or with the
number of winter vacations in warm and sunny locations. The use at age 15-20 of a bikini
compared to high backline, one-piece swimsuits, gave an odds ratio for all melanomas of 1.9
(1.0-3.7) and for trunk melanoma specifically of 0.8 (0.3-2.6); the risks were 3.5 [CI not
given] among sun-sensitive women and 1.3 [CI not given] among less sun-sensitive women,
but the interaction was not significant.
In a case- control study of patients attending a pigmented lesion clinic in Boston, USA
(Weinstock et al., 199lb ), 186 had cutaneous melanoma; the 239 controls had other dermato-
logical diagnoses, the most frequent of which were common naevus and solar keratosis. Data
were obtained from medical records and from a self-administered questionnaire completed
before clinical examination and were analysed by a multivariate method. Significantly in-
creased risks for melanoma were associated with lack of tan after repeated exposures as a
teenager (odds ratio, 2.3; 95% CI, 1.0-4.9). A nonsignificant trend towards increased risk
was observed for residence in southerly areas. [The Working Group noted that the paper
dealt primarily with dysplastic naevi and the results on melanoma are not given in detail, and
that the controls also had dermatological conditions.]
.....
s
Table 16. Case-control studies of melanoma in which exposure to the sun and/or artificial ultraviolet radiation
was assessed
Place Period of No. of Source of cases Melanoma No. of l}tpe of control Reference
diagnosis cases type controls
Australia
East Australia NS 173 3 hospitals All types 173 Other cancers Lancaster & Nelson
(1957)
Queensland, 1963-69 468 1 hospital All types 468 Hospital patients, Beardmore (1972)
Australia including skin
cancers
Western Australia 1980-81 511 Population All types 511 Population Holman &
0
Armstrong (1984a,b)
z
Queensland, 1979-80 183 Population NoLMM 183 Population Green (1984); Green 0
Australia et al. (1985a)
C'l
Europe
:I:
Oslo, Norway 1974-75 78 1 hospital All types 131 Other cancers, same Klepp & Magnus
(/')
hospital (1979) <
0
United Kingdom 1971-76 111 Population All types 342 General practice lists Adam et al. (1981)
t;
Western Scotland 1978-80 113 Hospital NoLMM 113 Hospital, non-skin MacKie & Aitchison
a::
(1982)
tTl
Birmingham, UK 1980-82 58 2 hospitals NoLMM 333 Hospital and Sorahan & Grimley
Vl
Vl
population (1985)
Nottingham, UK 1981-84 83 Population All types 83 Matched hospital Elwood et al. (1986)
(2 hospitals)
'Itento, Italy 1983-85 103 1 hospital All types 205 Hospital Cristofolini et al.
(1987)
East Denmark 1982-85 474 Population NoLMM 926 Matched population 0sterlind et a/.
(1988a,b); 0sterlind
(1990)
Thrin, Italy 1984-86 208 Population All types 416 Population Zanetti et ai. (1988)
Berlin, Gennany 1987 200 1 hospital All types 200 Skin clinic patients Garbe et a/. (1989)
Table 16 (contd)
Place Period of No. of Source of cases Melanoma No. of 'JYpe of control Reference
diagnosis cases type controls
Scotland 1987 280 Population Invasive MM 280 Hospital, excluding MacKie et al. (1989)
at least type 2 skin
Germany 1984-87 1079 6 dermatology All types 778 Skin clinic patients Weiss et al. (1990)
clinics
Stockholm, 1978-83 523 I hospital All types 505 Matched population Beitner et a/. (1990)
Sweden
Midlands, UK 1984-86 195 Population SSM and NM 195 Hospital in-/out- Elwood et al. (1990)
patients tl
- Southeast France 1986-88 2fJ7 Hospital Invasive, all 295 Health centre Grob et al. (1990)
tTJ
r;n
types
0
'Tj
North America
()
New York, USA 1955-67 79 1 hospital All types 1037 Other skin diseases, Gellin et a/. (1969)
non-cancer
('j
tTJ
Boston, MA, USA NS 45 Cohort of All types 180 Classmates Paffenbarger et al. :;tl
Philadelphia, PA,
university alumni
(1978)
-z USA
::z::
Boston, MA, USA 1978-79
111 1 hospital All types 107 Friends of cases Lew et al. (1983)
c::
New York, USA 1978-81 114 1 hospital All types 228 Patients and staff Rigel et al. (1983)
New York, USA 1972-80 74 1 melanoma All types 49 Skin clinic patients Brown et at. (1984)
clinic
Western Canada 1979-81 595 Population SSM, NMor 595 Population Elwood et al. (1984,
UCM
1985a,b)
Buffalo, NY, USA 1974-80 404 Hospital patients All types 521 Cancer patients Graham et al. (1985)
New York, USA 1972-82 1103 3 hospitals All types 585 Skin clinic patients Dubin et a/. (1986)
Western Canada 1979-81 415 Population SSM 415 Population Elwood et al. (1987)
128 NM 128
56 LMM 56
San Francisco, CA, 1984-85 121 1 melanoma NMand SSM 139 Clinic patients HoiJy et a!. (1987)
USA
clinic
.....
.....
.....
Table 16 (contd)
Place Period of No. of
diagnosis cases
New York, USA 1979-82 289
USA 1976-84 130
Boston, MA, USA 1982-85 186
Source of cases
3 hospitals
Ntlrses cohort
1 hospital
Melanoma No. of 1Jpe of control
type controls
All types 527 Non-cancer skin
patients
AM excluded 300 Nurses cohort
All types 239 Skin clinic patients
Reference
Dubin et ai. (1989)
Weinstock et al.
(1989)
Weinstock et a/.
(1991b)
NS, not specified; SMM, superficial spreading melanoma; NM, nodular melanoma; UCM, unclassifiable melanoma; LMM, lentigo maligna
melanoma (or llutchinson's melanotic freckle); AM, acrallentiginous melanoma
....
;:::)
;;
0
6
0
d
B
rr1
V\
V\
STUDIES OF CANCER IN HUMANS 113
(cl) Collation of results
The studies summarized above show that a range of host characteristics are related to
melanoma risk, including ethnic origin, skin, hair and eye pigmentation, and, importantly, a
tendency to sunburn or suntan: often expressed clinically as skin type. These factors can be
assumed to reflect genetic sensitivity to cutaneous effects of sun exposure and, in addition to
the indirect evidence of a role of exposure to the sun in melanoma that they provide, should
be considered as confounders in a relationship between sun exposure and melanoma. The
numbers of acquired benign naevi and of dysplastic naevi have been shown to be very strong
risk factors for melanoma in several studies; the density of freckling on the skin has also been
shown to be a risk factor. Because there is evidence that these outcomes are themselves
related to sun exposure, and in the case of naevi may be intermediate steps in the genesis of
melanoma, they should not be considered confounding factors (Armstrong, 1988). Most of
the studies relied on a wide range of questions to assess different aspects of sun exposure.
Armstrong (1988) developed a useful classification of such questions, dividing them into
those that assess potential exposure, such as place of residence and time of migration, those
that record actual exposure and those that record response to exposure, such as questions on
sunburn and suntanning.
(i) Total sun exposure: potential exposure by place of residence (Table 17)
Consistent with the descriptive studies, Holman and Armstrong (1984b) showed that the
risk in migrants arriving in Australia before age 10 (odds ratio, 0.89; 95% CI, 0.44-1.80) is as
high as that of the Australian born (1.00), and the risk in those arriving at age 10 or above is
much less (0.34; 0.16-0.72 for age 10-29; 0.30; 0.08-1.13 for age> 30). These data are an
improvement on descriptive data as they allow control for ethnic background and pigmen-
tation. In the same study, an association was seen with annual hours of bright sunlight
averaged over all places of residence.
In the USA, two case-control studies (Graham et al. , 1985; Weinstock eta/., 1989)
showed increased risks for people who had lived at southerly latitudes.
Increased risks in people who have lived near the coast were seen in Denmark (0sterlind
eta/., 1988b) and in Queensland, Australia (Green & Siskind, 1983). It was assumed in the
Danish study that coastal residence would involve more exposure to the sun. In Queensland,
living near the coast is not related to annual ambient UVR, which varies with latitude, so that
peak summer UV irradiance is higher in the interior than on the coast (Green & Siskind,
1983). The observations are thus due either to different behavioural patterns with
geographical location or to differences in exposure to UVR.
(ii) Biological response to total sun exposure
It has been assumed that a history of nonmelanocytic skin cancer, solar keratoses, actinic
tumours or changes on cutaneous microtopography are all indicators of cumulative sun
damage. Positive associations are seen with these measures in studies in Australia and in the
USA, although 0sterlind et a/. (1988b) in Denmark saw no relationship with micro-
topographical change (Thble 17).
......
......
"""
Table 17. Results of case-control studies on melanoma: place of residence, biological markers
Place Direction of ORa 95% Cl p value Measurement of exposure Reference
association
Potential exposure by place of residence
Australia Up 5 Residence near coast; mortality Green & Siskind (1983)
rate/100 (XX) (incidence rate/
100 (XX), 37 )
Australia Down 0.3 (0.1-1.1) < 0.001 Age at arrival in Australia; OR Holman & Armstrong (1984b)
- given for age 30 years; p value ;l>
for trend
Australia Up 2.8 (l.S-4.8) < 0.001 Mean annual hours of bright Holman & Armstrong (1984b)
s:
sunlight at places of residence;
0
p for trend
z
USA Up 1.4 (0.9-2.0) > 0.05 Ever resided below 40 N latitude Graham era/. (1985)
0
0
a
Australia Down 0.3 (0.1-1.4) > 0.05 Length of residence in Australia; Green eta/. (1986)
risk associated with migration to
Australia
.,
::r:
Denmark Up 1.7 (1.1-2.7) 0.006 Residence near coast; crude OR 0sterlind eta/. (1988b)
en
USA Up 2.2 (1.1-4.2) 0.02 Residence in southerly latitude at Weinstock et al. (1989)
6
age 15-20, OR for 12.6
l'
Biological markers of cumulative sun exposure
c
s:
Australia Up 2.7 (1.4-5.0) 0.003 Cutaneous microtopography; p for Holman & Annstrong (1984b)
trl
VI
trend VI
Australia Up 3.7 (2.1-6.6) < 0.001 History of nonmelanocytic skin Holman & Armstrong (1984b)
cancer
Australia Up 3.6 (1.8-7.3) < 0.001 Actinic tumours on face Dubin eta/. (1986)
USA Up 5.0 (2.3-10.5) < 0.01 History of solar keratosis Green & O'Rourke (1985)
USA Up 3.8 (1.2-12.4) 0.03 History of nonmelanocytic skin Holly eta/. (1987)
cancer, adjusted
Denmark Flat 1.1 (0.7-1.8) > 0.05 Cutaneous microtopography; crude 0sterlind eta/. (1988b)
OR
4Qdds ratio for maximal category
bResults calculated by Annstrong (1988)
STUDIES OF CANCER IN HUMANS 115
(iii) Total sun exposure assessed by questionnaire
The results of studies in ~ h i h total sun exposure was assessed using questionnaires,
either over lifetime or at different periods of life, have been mixed (Thble 18). Positive
associations were seen by Green (1984) in Queensland, Australia; no consistent overall
association was seen in western Canada, and in Western Australia the association was
negative. The resultsofthe other studies are similarly mixed. This inconsistency, in contrast
to the results noted above by place of residence and by biological response, could be due
either to the difficulty of assessing total sun exposure by questionnaires (Armstrong, 1988) or
to different effects of differing patterns of exposure to the sun.
(iv) Short periods of residence implying high potential exposure
Several case-control studies have reported, usually as incidental findings, that subjects
who have had a short period of residence in tropical or sub-tropical environments have an
increased risk for melanoma (Thble 19).
(v) Occupational exposure
Regular outdoor occupational exposure is probably the most convenient measure of
relatively constant sun exposure and has been assessed with differing degrees of detail, from
simple questions on ever/never or a basic amount of outdoor exposure, to detailed
assessments involving assessments of clothing habits, geographical location of work and so
on. The results appear to be inconsistent (Table 20). The more detailed studies, however,
show more consistency, with a significant negative association, particularly in men, who
constitute most of the highly exposed subjects (Table 21).
An overall irregular pattern was seen in western Canada, probably because individuals
with relatively little occupational exposure are those who perform outdoor work seasonally
or for short periods, often in early life, so that this exposure may be an indication of inter-
mittent rather than constant exposure (Elwood eta/., 1985b). Such results are consistent with
the effects of a short period of residence in a sunny place, as reviewed earlier. Paffenbarger et
a/. ( 1978) also showed that students who recorded outdoor work before college [presumably
summer employment] had a significantlyincreased risk of melanoma in later life.
(vi) Intermittent exposure
To assess the effects of intermittent exposure, investigators have asked questions about
specific activities that would be likely to represent relatively severe intermittent exposure,
such as sunbathing, or asked particularly about holidays in sunny places, or used more
complex questionnaires to attempt to assess total intermittent exposure through recreational
or holiday activities. Most of these studies show positive associations, but few show large
effects (Thble 22).
In general, the more detailed studies show reasonably consistent positive results. For
example, in western Canada, significant positive associations were seen with recreational and
holiday sun exposures in activities involving reasonably intense sun exposure, such as beach
activities (Elwood et al., 1985b). In Denmark, rather similar relative risks of 1.5-1.9 were
seen with regular participation in activities such as sunbathing, boating, skiing, swimming
and vacations in sunny places (0sterlind eta/., 1988b). Significant positive associations with
sunbathing were seen in the Swedish study of Beitner et al. (1990). In the study of Zanetti eta/.
Table 18. Results of case-control studies on melanoma: total sun exposure assessed by questionnaire
Place Direction of ORa 95% CI p value Measurement of exposure Reference
association
USA Up 2.5 NA < 0.001 Sun exposure 2 h/day, 11-20 years Rigel et a/. (1983)
previously
Australia Up 5.3 0.9-30.8 NA Total sun exposure throughout life Green (1984)
> 50 000 h, adjusted
Canada Weakly up 1.2 0.7-2.0 > 0.1 Hours of sun exposure per year, p for Elwood et al. (1985b)
trend
USA Down 0.6 0.4-0.9 < 0.05 Total sun exposure throughout life Graham eta/. (1985t
USA Weakly up 1.1 0.6-2.1 > 0.05 Hours of sun exposure 0-5 years Dubin et a/. (1986)
previously, > 5 h/day
USA Down 0.85 0.5- 1.4 > 0.05 Hours of sun exposure 11- 20 years Dubin et al. (1986)
previously, > 5 h/day
USA Weakly up 1.1 0.8-1.6 > 0.05 Lifetime sun exposure Dubin et al. (1986)
Australia Down 0.7 0.4- 1.1 0.13 Mean total outdoor hours/week in Holman et al. (1986a)
summer, > 23 h/week; p for trend
Italy Down 0.7 0.4-1.1 > 0.05 Heary or frequent exposure in previous Cristofolini et al. (1987)
20 years
France Up 3.4 1.6-7.1 < 0.05 Total lifetime outdoor sun exposure, Grob et a/. {1990)
adjusted
0
0dds ratio for maximal category
bResults calculated by Armstrong (1988)
......
......
0'1
-)>
0
6
0
:I:
CI'J
6
G
m
u.
u.
Table 19. Evidence of melanoma risk with short periods of residence implying high potential exposure
Place Direction of Odds ratio 95% CI p value Measurement of exposure Reference
association
USA Up [7.7 2.5-23.6] 0.0002 US service: tropics versus USA/Europe Brown eta/. (1984)
UK Up 1.8 0.6-5.1 > 0.05 1 year living in tropics, subtropics Elwood (1986)
Scotland Up 2.6 (males) 1.3- 5.4 < 0.05 > 5 years living in tropics, subtropics; crude MacKie et a/. (1989)
1.8 (females) 0.8-4.0 > 0.05 OR
Sweden Up 1.9 l.G-3.6 < 0.05 Living in Mediterranean, tropics, subtropics Beitner et aJ. (1990)
> 1 year in last 10 years
0
ffi
0
'TJ
(')
(')
z
::t:
c::
t3
.....
Table 20. Results of case-control studies on melanoma: occupational exposure
Place Direction of OR
0
95%CI p value Measurement of exposure
association
USA Up 3.9 NR O.Ql Outdoor work recorded at college
medical examination; prospective
Norway Up 1.4 0.6-3.5 0.37 At least 3-4 h of outdoor work a day
Scotland Down 0.5 0.2-1.2 > 0.05 Hours of outdoor occupation a week
USA Up 1.2 NR > 0.05 Outdoor occupation versus indoor
Canada Irregular 0.9 0.6-1.5 < 0.01 Hours of outdoor occupation a week in
summer
USA Down 0.7 0.3-1.3 > 0.05 Lifetime hours of outdoor occupation
USA Up 2.5 1.4-4.4 < 0.05 Mostly outdoors; multiple logistic OR
= 2.4, p < 0.05
UK Irregular 1.7 0.3-8.6 0.5 Lifetime hours of outdoor occupation
Australia Down 0.5 NR 0.04 Mean hours of outdoor occupation a
week in summer
Denmark Down 0.7 0.5-0.9 < 0.05 Outdoor occupation versus indoor
Italy Irregular 2.1 0.6-6.8 0.32 Outdoor occupation
Gennany Up 5.5 1.2-25.3 < 0.05 Outdoor occupation; adjusted OR =
11.6 (2.1-63.3)
Sweden Down 0.6 0.4-1.0 NR Outdoor occupation, yes/no
France Up 6.0 2.1-17.4 < 0.05 Outdoor occupation versus indoor
NR, not reported
0
0dds ratio for maximal category
bCalculated by Annstrong (1988)
Reference
Paffenbarger et al. (1978)
Klepp & Magnus (1979)1'
MacKie & Aitchison (1982f
Rigel eta/. (1983)
Elwood et al. (1985b)
Graham et al. (1985)
Dubin et a/. (1986)
Elwood et al. (1986)
Holman eta/. (1986a)
0sterlind eta/. (1988b)
Zanetti et al. (1988)
Garbe et a/. (1989)
Beitner eta/. (1990)
Grob et a/. (1990)
......
......
OQ
-
>
fS
3::
0
z
0
0
5;:
'"'CI
::r:
Vl
6
G
3:
tT1
v.
v.
Table 21. Results of case-eontrol studies on different types of melanoma and occupational exposure en
2
Place 'JYpe of Odds 95%CI p value Measurement of exposure Reference
- melanoma ratio trJ
en
Canada Excluding LMM 0.5 [0.3-1.0] NR > 32 h outdoor occupation a Elwood eta/. (1985b)
0
'Tj
andALM week in summer (men)
(")
>
Queensland, Excluding LMM No association Outdoor occupation Green et a/. (1986) z
Australia andALM
(")
trJ
Western SSM 0.5 NR 0.04 for Top quaniJe, hours of outdoor Holman et a/. (1986a)
Australia trend occupation a week in summer
.......
z
Denmark Excluding LMM 0.7 0.5-0.9 < 0.05 Outdoor occupation (men) 0 st erlind eta/. (1988b)
'"T'
-
andALM
c:::
LMM, lentigo maligna melanoma; ALM, acrallentiginous melanoma; SSM, superficial spreading melanoma; NR, not reponed
>
z
en
.....
\0
Table 22. Results of case-control studies on melanoma: intermittent exposure
g
Place Direction of ORa 95% CI p value Measurement of exposure
Reference
association
Norway Up 2.4 l.Q-5.8 0.06
Sunbathing holidays in southern Europe in
Klepp & Magnus
previous 5 years
(1979)h
UK Up 1.5 0.9-2.5 0.16
Spent some time deliberately tanning their legs
Adam et al. (1981f
Up 1.6 l.Q-2.5 0.05
Spent some time deliberately tanning their trunk
Scotland Down 0.4 0.2-0.9 < 0.05 Hours a week in outdoor recreation
Mackie & Aitchison
(1982)b
-
USA Up 2.5 1.1-5.8 < 0.05
Days of vacation in a sunny warm place in
Lew et a/. (1983)
>
childhood
USA Up 2.4 NR 0.01
Outdoor versus indoor recreation
Rigel eta/. (1983)
Canada Up 1.7 1.1-2.7 < 0.01
Hours of high exposure in recreational activities
Elwood et al. (1985b)
0
z
per week in summer
0
Up 1.5 l.Q-2.3 < 0.01 Hours of high and moderate exposure in
0
recreational activities per day in summer vacations
5::
Up 1.7 1.2-2.3 < O.{Xll Number of sunny vacations per decade
'"0
:I:
UK Up 5 NR > 0.05
Number of holidays abroad in hot climate;
Sorahan & Grimley
Cl'l
adjusted
(1985) <
USA Irregular 1.7 1.2-2.2 < 0.01
Recreation type; multiple logistic OR, 1.0
Dubin et a/. (1986)
0
r-'
Australia Irregular 1.9 0.5-7.4 0.62 Recreational hours spent in sun on beach over
Green et at. (1986)
c
whole life; crude RR til
Australia Up 1.3 0.9-1.9 0.25
Proportion of recreational outdoor exposure in
Holman eta/. (1986a)
Vl
Vl
summer at lQ-24 years of age; p for trend
Up 2.4 1.1-5.4 0.04 Boating in summer; p for trend
Up 2.7 1.2-6.4 0.07 Fishing in summer; p for trend
Irregular 1.1 0.7-1.8 0.66
Swimming in summer; p for trend
Up 1.3 0.8-2.2 0.26
Sunbathing in summer at 15-24 years of age; p for
trend
Denmark Up 1.9 1.3-2.9 0.004 Sunbathing; crude RR; p for trend
0sterlind et al. (1988b)
Up 1.7 1.1-2.8 0.012 Boating; crude RR; p for trend
Up 1.5 0.9-2.4 0.006
Skiing; crude RR; p for trend
Up 1.5 1.2-2.0 0.004
Swimming (outdoors); crude RR;p for ,trend
Up 1.7 1.2-2.4 < 0.01
Vacations in sunny resorts; crude RR; p for trend
Table 22 (contd)
Place Direction of OR 95% Cl p value Measurement of exposure Reference
association
Italy Irregular 2.6 1.()....6.9 0.003 Years of outdoor sport (men); p for trend Zanetti et a/. (1988)
Up 3.8 1.1-13.0 . NR High-exposure sports (men)
(/)
C!
Irregular 1.9 0.6-5.8 0.27 Total weeks' vacation (men); p for trend
0
Up 3.7 1.4-9.7 0.001 Weeks' vacation near sea; early life (men); p for
-
trend
rn
Up 1.6 0.7-3.6 0.77 Weeks' vacation near sea; adult life (men); p for
0
trend
'Tl
Irregular 2.1 0.6-7.9 0.37 Years of outdoor sport (women); p for trend
(")
Up 2.3 0.6-9.1 NR High-exposure sports (women)
Irregular 1.1 O.S- 2.4 0.56 Total weeks' vacation (women); p for trend
(")
m
Up 1.2 0.6-2.5 0.56 Weeks' vacation near sea; early life (women); p for :;.::1
trend
-z
Up 1.5 0.9-2.7 0.16 Weeks' vacation near sea; adult life (women); p for
:I:
trend
c
Germany No association NR NR NR Free-time sun exposure Garbe et al. (1989)
Sweden Up 1.8 1.2-2.6 < 0.05 Number of sunbaths per summer Beitner et al. (1990)
Up 2.4 1.5-3.8 < 0.05 Sunbathing vacations abroad
(/)
France Up 8.4 3.6-19.7 < 0.05 Outdoor leisure exposure Grob et a/. (1990)
NR, not reported
4
0dds ratio for maximal category
bCalculated by Annstrong (1988)
......
122 IARC MONOGRAPHS VOLUME 55
(1988) in Turin, Italy, positive associations were seen with doing an outdoor sport for many
years and with number of weeks of holidays spent near the sea. These consistently positive
associations contrast with the less consistent pattern seen in Australia. In Western Australia,
stronger associations are seen with boating and fishing than with swimming and sunbathing,
which would be expected to involve more intense exposure to the sun, and only a weak
association was seen with the proportion of outdoor time spent on recreational activities in
teenage and early adult years (Holman eta/., 1986a). In Queensland, Green eta/. (1986)
found only irregular associations with recreational hours spent at the beach or in other
activities with intense exposure to the sun. This finding might be consistent with the concept
that, in a sunny environment, recreational activities may involve sufficient frequency or
intensity of sun exposure to result in a constant rather than an intermittent dose pattern.
(vii) Sunburn
Most of the studies show positive associations between risk for melanoma and a history
of sunburn (Table 23 ). The questionnaires usually defined very severe sunburn as a burn that
causes pain lasting for at least two days or blistering. The greater consistency of this
relationship compared to that with intermittent exposure may indicate a specific association
with sunburn per se or that sunburn is simply a more easily remembered measure of
intermittent and/or intense exposure to the sun.
A history of sunburn indicates both unusually intense exposure and skin sensitivity, and
therefore studies which assess sunburn while controlling for sensitivity through a separate
question on tendency to burn are important. Both the western Canada and Western Australia
studies when analysed in this way show that the association is primarily with tendency to burn
rather than with a history of sunburn (Elwood eta/., 1985a; Holman eta/., 1986a). The studies
in Queensland, Denmark and Scotland, however, show strong associations with sunburn
history even after controlling for tendency to burn and other measures of skin sensitivity.
Because sensitivity to the sun and sunburn are likely to be highly correlated and both are
likely to be measured with a degree of error, it is difficult to distinguish their effects.
Similarly, sunburn is likely to be confounded with intermittent exposure of a less intense
nature, from which it cannot readily be distinguished because of measurement error
(Armstrong, 1988).
The study in England by Elwood et a/. (1990) assessed sunburn at different ages and
showed the strongest association with sunburn at ages 8-12; a stronger association with
sunburns at young age was also seen by Weinstocket a/. (1989) and by 0sterlindeta/. (1988b).
2.1.4 Malignant melanoma of the eye
(a) Case reports
In general, case reports were not considered, owing to the availability of more infor-
mative data.
Kraemer et al. (1987) reported on 830 cases of xeroderma pigmentosum, with a median
age of 12 years at last observation, located through a survey of published case reports. Ocular
abnormalities were found in 328 of 337 patients on whom information was available. Of
these, 88 were reported to have some form of ocular neoplasm, mostly in the limbus, cornea
and conjunctiva. Five of these patients were reported as having ocular melanoma; only one
Table 23. Results of case-control studies on melanoma: history of sunburn
Place Direction of ORa 95%Cl p value Measurement of exposure Reference
association
Scotland Up 2.8 1.1-7.4 < 0.05 Blistering sunburn or erythema persisting > 1 MacKie & Aitchison
week (1982)
USA Up 2.1 1.2-3.6 < 0.05 Blistering sunburn during adolescence (yes/no) Lew et al. (1983)
-Canada Up 1.8 1.1-3.0 < 0.01 Vacation sunburn score Elwood eta/. (1985a/'
Australia Up 2.4 1.0-6.1 < 0.05 Number of severe sunburns throughout life Green et al. (1985a)
en
UK Up 4.2 NR < 0.01 Bouts of painful sunburn; adjusted Sorahan & Grimley
d
(1985)
0
Canada Up 3.2 1.7-5.9 < 0.001 Sunburn causing pain for ? 2 days Elwood et a/. (1986Y
51
Australia Irregular 0.9 0.5-1.5 0.43 Sunburn causing pain for ;:: 2 days, during last Holman et a/. (1986a/'
en
0
10 years
'T1
Up 1.2 0.6-2.3 0.1 Sunburn causing pain for ;:: 2 days, < 10 years of
(")
age
Up 1.7 1.0-2.9 0.003 Blistering sunburn
(")
trl
Italy Down 0.7 0.4-1.2 > 0.05 Severe sunburn in adolescence or early adult life Cristofolini eta/. (1987)
(yes/no)
z
Up 1.2 0.7- 2.1 > 0.05 Sunburn as an adult (yes/no)
:I:
USA Up 3.8 1.4-10.4 NA Number of blistering sunburns up to adult age, Holly et al. (1987) c
adjusted
Denmark Up 3.7 2.3-6.1 < 0.001 Sunburn causing pain for 2: 2 days, < 15 years of 0sterlind et a/. (1988)
age
Up 3.0 1.6-5.4 < 0.001 Sunburn causing pain for ;:: 2 days, during previous
10 years
Italy Up (men) 4.1 1.8-9.2 < 0.05 Sunburn in childhood (yes/no) Zanetti et al. (1988)
Up (women) 2.7 1.3-5.6 < 0.05
Germany No association NR NR N.R Number of sunburns Garbe et al. (1989)
Scotland Up (men) 7.6 1.8-3.2 NR Number of episodes of severe sunburn, any age, MacKie et a/. (1989)
adjusted
Up (women) 2.3 0.9-5.6 NR Number of episodes of severe sunburn, any age,
adjusted
E
Table 23 (contd)
Place Direction of OR
4
association
USA Up 2.2
Sweden Up 1.7
UK Up 3.6
No association 1.0
Up 1.8
Up 1.2
NR, not reported
aodds ratio for maximal category
boata calculated by Armstrong (1988)
95% CI
1.2-3.8
1.0-2.9
1.4-11.2
0.6-2.0
0.9-3.7
0.6-2.3
'Exposure to fluorescent and other lighting sources
p value Measurement of exposure
0.01 Number of blistering sunburns at ages 15-20
NR EI)'thema after sunbathing
< 0.05 Moderate sunburn at ages 8-12 (yes/no)
> 0.05 Moderate/maximum sunburn at ages 18--20 (yes/no)
> 0.05 Moderate/maximum sunburn 18-20 yrs before
diagnosis (yes/no)
> 0.05 Moderate/maximum sunburn 5 years before
diagnosis (yes/no)
Reference
Weinstock et al. (1989)
Beitner et al. (1990)
Elwood et al. (1990)
.......
>
f5
3'.:
0
z
0
0
s;
'"0
::r:
C/'J
6
t;
3'.:
t'I1
v.
v.
STUDIES OF CANCER IN HUMANS 125
was specified as being of uveal origin. [The Working Group recognized that data collected
from previously published case reports is not uniform and may not be typical of a true
incidence or prevalence series. Furthermore, no information is available on the relationship
between solar exposure and the occurrence of ocular melanoma in these patients.]
(b) Descriptive studies
As there is no separate lCD code for intra-ocular melanoma, descriptive data for cancer
of the eye (ICD-9 190) as a whole have been used as a surrogate. Intra-ocular melanoma
comprises some 80% of tumours of the orbit of the eye (0sterlind, 1987), and cancer of the
eye has been used as a surrogate for adult ocular melanoma in previous studies (Swerdlow,
1983a,b).
(i) Ethnic origin
Examination of incidence figures from many parts of the world reveals higher rates of
ocular tumours in whites than in blacks or Asians residing at the same latitude and under
similar conditions (Waterhouse et al., 1976; Muir eta/., 1987).
(ii) Place of birth and residence
When rates for whites are evaluated separately, no variation in incidence rates for ocular
tumours is seen with decreasing latitude in the northern hemisphere (Table 24). Similarly, no
incidence grading was seen among whites in the USA (Table 25). The more northerly states of
Australia do not show higher incidence rates for ocular tumours than the southern states
(Table 25).
Table 24. Trends in cancer of the eye for whites by latitude and by time period (rates per
100 000 age standardized to UICC 'world population')
Latitude
56 -{)t. N
47 -ss N
46 N
38 N
35 "N
32-38s
Area
Denmark
Finland
Sweden
Canada
British Columbia
Alberta
Saskatchewan
Manitoba
Geneva,
Switzerland
San Francisco, CA,
USA
New Mexico, USA
Australia
New South Wales
South Australia
-1968-72a
Men Women
1.4 1.2
0.9 1.0
1.3 1.2
1.0 0.8
0.8 0.6
1.3 0.8
1.7 0.9
0.4 0.2
0.9 0.9
1.0 0.7
NR NR
NR NR
- 1912-nb
...-.J 1977-82C
Men Women Men Women
0.8 0.7 1.0 0.7
0.9 0.7 1.0 0.7
0.9 0.8 0.9 0.6
0.9 0.6 0.7 0.4
0.8 0.9 0.7 0.7
1.1 1.0 1.0 0.7
1.2 1.0 0.8 0.8
0.8 1.1 0.6 1.1
0.9 0.5 0.9 0.8
1.3 0.7 0.9 0.9
0.8 0.8 0.9 0.5
0.9 1.0 0.7 0.6
126 IARC MONOGRAPHS VOLUME 55
Table 24 (contd)
Latitude Area 1968-72a ....._ l977-82C
22 s
3 s
Hawaii, USA
Cali, Colombia
NR, not reported
oJFrom Waterhouse et al. (1976)
bFrom Waterhouse et al. (1982)
Cfrom Muir et ai. (1987)
Men
0.4
0.6
Women
0.2
0.2
Men
1.2
0.4
Women
0.2
0.5
Men
1.0
0.5
Table 25. Incidence of cancer of the eye (ICD-9 190) in US and
Australian whites 1978-82 in various locations by latitude
Latitude Location Male rate/ Female rate/
100 ()()() 100000
USA
47 N
Seattle 0.9 0.8
42 N
Detroit 0.7 0.6
42 N Iowa 1.0 0.7
41 .N
Connecticut 0.6 0.3
41 .N
New York City 0.5 0.4
41 N
Utah 1.4 1.1
38 N
San Francisco Bay Area 0.9 0.8
35 "N New Mexico 0.9 0.9
34 N
Los Angeles 0.7 0.6
33"N Atlanta 0.7 0.8
22 "N Hawaii 1.0 0.0
Australia
43 s Thsmania 1.2 0.8
38 s Victoria a 1.1 0.4
34 s South Australia 0.7 0.6
33 s New South Wales 0.9 0.5
32 s Western Australia 1.6 0.5
28 s Queenslanda 0.6 0.7
From Muir et al. (1987); rates standardized to UICC 'world population
aoata available only for 1982
Women
0.0
0.5
Schwartz and Weiss {1988) compared the state of birth of 763 white (not of Spanish
origin) US patients with uveal melanoma diagnosed between 1973 and 1984 and identified in
nine cancer registries with those of the whites covered by the registries as recorded in the
1980 census. Patients with unknown or foreign birthplace or non-uve.al ocular melanomas
were excluded. Risk estimates were adjusted for age. sex and residence. The odds ratio for
subjects born in the southern USA(south of 40 ON) was 1.1 (95% CI, 0.8-1.5). When states
STUDIES OF CANCER IN HUMANS 127
were classified according to average daily global solar radiation, a nonsignificant gradient
was observed, only among women (odds ratio for > 15 500 kJ/m
2
versus :s: 12 300 kJ/m
2
, 1.6;
95% CI, 0.7-3.6).
Mack and Floderus (1991) examined birthplace and residence of patients diagnosed
with intra-ocular melanoma among non-latino whites in 1972-82 in Los Angeles County.
The proportional incidence ratio was not higher for cases born in California and Arizona
than for those born in more northerly areas.
Doll (1991) observed a small rural excess in the incidence of cancer of the eye compared
with urban residence, in a number of countries.
(iii) Occupation
Four studies of occupational mortality and one of incidence gave inconsistent results
with regard to ocular cancer. Two investigations using proportional mortality ratios demons-
trated more deaths from ocular cancer than expected among male farmers (Saftlas eta/.,
1987; Gallagher, 1988), a group likely to have substantial exposure to solar UVR. These
findings were not confirmed, however, in two other studies using similar methods (Milham,
1983; Office of Population Censuses and Surveys, 1986).
An investigation of ocular melanoma carried out on data from the cancer registry of
England and Wales did not show an elevated incidence in farmers, but an increased risk was
seen for professionals (relative risk, 124; 95% CI, 99-153), which was significant for teachers
(177; 120-248) (Vagero eta/., 1990).
(iv) History of skin cancer
Cancer registry-based studies (0sterlind et al. , 1985; Thcker eta/., 1985a; Holly et a/.,
1991) found no or a nonsignificant (Iischko eta/., 1989) association between the occurrence
of cancer of the eye and cutaneous melanoma or nonmelanocytic skin cancer. A single inves-
tigation of 400 sequential cases of uveal melanoma (Thrner et a/., 1989) suggested that
intra-ocular melanoma patients have an elevated frequency of prior cutaneous melanoma.
Thus, although one study indicated a possible association, the overall evidence does not
support an association between ocular melanoma and either melanoma or nonmelanocytic
skin cancer.
(c) Case-control studies
Four case-control studies were evaluated. The first study (Gallagher et al., 1985)
evaluated all ocular melanomas, while the other three (Thcker eta/., 1985b; Holly et al., 1990;
Seddon eta/., 1990) studied uveal melanomas (exduding conjunctival melanomas).
Gallagher et al. (1985) conducted a study of ocular melanoma in patients diagnosed in
the four western provinces in Canada between 1 April1979 and 31 March 1981. Of the 90
ascertained cases, 87 were eligible by age for interview (20-79 years); of these, 65 cases
(75%) were actually interviewed. For each case, a single control was randomly selected from
the general population, matched by age( 2 years), sex and province of residence. Response
rates for controls were 59% for Alberta, Saskatchewan and Manitoba and 48% for British
Columbia. Personal interviews were conducted in subjects' homes, and conditional logistic
regression was used to control for matching variables and eye, hair and skin colour. No signi-
ficant association was seen between ocular melanoma and either intermittent (occupational,
128 IARC MONOGRAPHS VOLUME 55
recreational and holiday) or cumulative exposure to solar UVR. A strong association was
detected between ocular melanoma and blue or grey iris colour (crude odds ratio, 3.0; p =
0.04) and blond or red hair colour (crude odds ratio, 7.7; p = 0.03). (In a multivariate
analysis, these odds ratios became nonsignificant.) A nonsignificantly elevated risk (crude
odds ratio, 2.8; p = 0.08) for ocular melanoma was also seen for subjects with light skin
colour by comparison with subjects with darker skin.
A case-control study conducted by Thcker eta/. (1985b) evaluated risk factors in 444
white patients with intra-ocular (uveal) melanoma treated at the Wills Eye Hospital in
Philadelphia, USA, and 424 controls with detached retinas seen at the same centre. (The
Working Group noted that use of a single disease category for the controls could introduce
spurious associations with risk factors for that condition.) Response rates were 89% for cases
and 85% for controls. Interviews were conducted by telephone; interviews were with next-of-
kin for 17% of the cases and 14% of the controls. Logistic regression models were fitted
which included sun-exposure variables, age, sex, eye colour and presence of cataracts, which
was included to reduce bias in view of the association between cataracts and detached retina.
Sunbathing appeared to increase the risk of intra-ocular melanoma, although no gradient of
risk was noted with frequency of exposure (frequent versus never, odds ratio, 1.5; 95% CI,
0.9- 2.3). A significantly elevated risk was detected for those who engaged in gardening (1.6;
1.0-2.4), but similar associations were not seen for other recreational outdoor activities, such
as fishing, camping and hunting. Cases of intra-ocular melanoma also reported increased
exposure to the sun during vacations in comparison with controls, with an odds ratio of 1.5
(95% CI, 0.97-2.3) for subjects 'frequently' experiencing increased exposure versus subjects
never exposed (test for linear trend over four strata,p = 0.01). Cases reported less frequent
use of eye protection (sunglasses, headgear, visors) when outdoors as compared with
controls, but there was no dose-response relationship with frequency of use of these pro-
tective devices. A gradient of risk was seen with use of any eye shading when iris melanomas
were examined separately, suggesting that eye shading may have been specifically important .
for lesions at the front of the eye (never versus occasional use of eye protection, odds ratio,
4.9; 95% CI, 1.4- 13.7). [Numbers of iris melanomas were not given.] Subjects who were
born in the southern USA (lower than 40 ON latitude) were found to have a significantly
elevated risk of intra-ocular melanoma {2.7; 1.3-5.9) after adjustment for number of years
spent in the south and for the presence of cataracts; with adjustment for all other sun-related
variables, the odds ratio was 3.2 (95% CI, 1.8- 5.7). The association persisted after excluding
subjects not living close to Philadelphia. There was no relation between the number of years
spent in the south and the risk of intraocular malignant melanoma, after adjustment for
having been born in the south. Blue-eyed subjects had the highest risk of intra-ocular
melanoma, with grey-green and hazel-eyed subjects at intermediate risk, and brown-eyed
subjects at lowest risk (unadjusted odds ratio for brown- versus blue-eyed subjects, 0.6; 95%
CI, 0.4-0.8). Cases were more likely than controls to have fair skin and blond or brown hair,
although no odds ratios are given and the differences disappeared when eye colour was taken
into account. Cases were also more likely to have 25 or more freckles (used as an indirect
measure of sun exposure and sensitivity) than controls (odds ratio, 1.4; 95% CI, 1.0- 2.0).
A case-control study by Holly eta/. (1990) involved 407 white cases of uveal melanoma
and 870 controls. The cases were diagnosed between January 1978 and February 1987 at the
STUDIES OF CANCER IN HUMANS 129
Ocular Oncology Unit of the University of California, San Francisco, USA, were aged 20-74
at diagnosis and lived in 11 western states. Controls were selected by random digit dialling
and were matched to cases on age and area of residence. Telephone interviews were con-
ducted by interviewers unaware of the study hypotheses, most cases being interviewed within
four years of their diagnosis. The response rate was 93% of cases and 77% of eligible
controls. No clear association was seen between uveal melanoma and vacation time spent in
sunny climates or high proportion of leisure time spent outdoors. Individuals who spent 50%
of their leisure time indoors and 50% outdoors had a reduced risk for uveal melanoma (odds
ratio, 0.6; 95% CI, 0.4-0.9) when compared to subjects who stayed mainly indoors. Signifi-
cantly elevated risks were seen in subjects with grey, green, hazel or blue eyes, compared to
those with brown eyes, with increasing frequency of large naevi (> 7 mm) (p = 0.04 for trend)
and with a propensity to burn rather than tan in the sun.
Seddon eta/. (1990) compared 197 white patients with uveal melanoma diagnosed in
1984- 87, who were resident in the six New England states close to the Massachusetts Eye and
Ear Infirmary, with 385 controls obtained through random digit dialling and matched to
cases by age ( 8 years), sex and area of residence. All subjects were interviewed by
telephone using a standard questionnaire. The response rate was 92% among cases, and 85%
of the eligible controls contacted agreed to participate in the study. Matched logistic
regression techniques were employed to evaluate potential associations between exposure to
UVR and risk of uveal melanoma, adjusting for age, sex. constitutional factors and socio-
economic variables. An inverse association with southern birthplace (south of 40 N
latitude) was detected (odds ratio, 0.2; 95% CI, 0.0-0.7) after adjustment for constitutional
and other factors. When cumulative lifetime residence in the south was examined, subjects
who had lived for more than five years south of 40 oN had an odds ratio of 2.8 (95% Cl,
1.1- 6.9) after adjustment for birthplace. Several indices of sun exposure were computed for
each subject. The first combined duration of residence in the north or south with self-
reported severity of sun exposure (low, medium, high). Subjects in the highest exposure
group appeared to have a higher risk of uveal melanoma by comparison with those in the
lowest exposure category (1.7; 0.9- 3.0) although no dose-response relationship was seen
over the three categories of exposure. A further index was obtained by taking average values
of solar radiation for each state in which the subject has resided and multiplying this value by
the duration of residence within the state and the reported amount of time spent in the sun.
No association was seen between this index and risk of uveal melanoma. Individuals who
reported having spent a great deal of time working outdoors 15 years prior to diagnosis
showed a somewhat lower risk of uveal melanoma than those who worked minimally
outdoors or were retired (odds ratio, 0.6; 95% CI, 0.3-1.4) after control for age, skin, eye
colour and southern residence. No association was seen with sunbathing, use of sunglasses or
visors, or outdoor hobbies all conducted 15 years prior to diagnosis. Use of eye glasses was
not related to uveal melanoma risk. Cases reported more cutaneous naevi and lighter skin
colour than controls and were more likely to be of northern European or British ancestry
than controls. An expanded analysis comparing 387 cases of uveal melanoma with 800 sibling
controls was also conducted. There was a gradient of risk with cumulative years of intense sun
exposure; the odds ratio for the highest exposure was 2.1 (1.4- 3.2).
130 IARC MONOGRAPHS VOLUME 55
2.1.5 Other cancers
No adequate data were available to the Working Group.
2.2 Artificial sources of ultraviolet radiation
Epidemiological investigations that have attempted to assess exposure to artificial
sources ofUVR have neither measured actual UVR nor considered the emission spectra. It is
presumed that in the studies described below, subjects were exposed to sources that varied in
intensity and emission spectra.
2.2.1 Nonmelanocytic skin cancer
Three case-control studies, described in detail on p. 84, addressed this issue. In the study
in Montreal, Canada, of Aubry and MacGibbon (1985), any use of a sunlamp gave an odds
ratio of 13.4 [95% CI, 1.4-130.5) after adjustment for sun exposure and constitutional
factors. O'Loughlin eta/. (1985) in Ireland found that fewer cases than controls reported
frequent exposure to 'artificial sunlight' (nonsignificant). In the study ofHerity et al. (1989) in
Ireland, a smaller proportion of cases than of controls reported ever having used sunlamps or
sunbeds (p = 0.2).
2.2.2 Malignant melanoma of the skin
1
The results of case-control studies of exposure to fluorescent light and melanoma are
summarized in Table 26.
Beral eta/. (1982) conducted a case- control study in Sydney, Australia, of 274 female
cases aged 18-54 identified at a melanoma clinic between 1978 and 1980 and 549 hospital
and pop.ulation controls matched by age and, for population controls, residence. The res-
ponse rate for cases was 71% [response rates for controls not given]. Each job lasting 12
months or longer was recorded, together with information about whether the work had been
carried out predominantly indoors or outdoors, whether fluorescent lighting was present,
and whether the fluorescent lights were switched on most of the time or less frequently.
Among women who always worked indoors, the odds ratio increased with duration of
working with fluorescent lights most of the time to a maximum of2.6 (95% CI, 1.2- 5.9) for 20
or more years' exposure. The effect was greater for office workers (odds ratio, 4.3) than for
other indoor workers (2.0). Stratification by amount of time spent outdoors, main outdoor
activity and amount of clothing worn, history of sunburn, place of birth, hair colour and skin
colour did not diminish the association. Among cases exposed to fluorescent lights, there was
a relative excess of melanomas on the trunk (a site likely to be covered at work); 24% in
exposed cases versus 4% in unexposed cases. [The Working Group noted that crude estimates
of sun exposure were used.]
Rigel et al. (1983) conducted a case-control study in New York, USA. described on
p. 106. Cases had had shorter average daily exposure to fluorescent lights ( 4.9 h) than had
1
After the meeting, the Secretariat became aware of a study by Walker et al. (1992) on the risk of cutaneous
malignant melanoma associated with exposure to fluorescent light.
STUDIES OF CANCER IN HUMANS 131
controls (5.4 h). Among office workers, average daily exposures were similar for cases and
controls. The crude odds ratio for any exposure was 0.7 among all subjects and 0.6 among
office workers.
English eta/. (1985) conducted a study in 1980-81 of the exposure to fluorescent light of
337 cases and 349 age-matched controls who had already participated in a population-based
case-control study in Western Australia (see Holman and Armstrong (1984a), p. 100). The
response rate was 68% for cases and 91% for controls. Detailed information was obtained
from telephone interviews about lifetime hours of residential and occupational exposure, the
distance to the nearest light fixture and the presence of diffusers. Neither the duration of
occupational exposure, the rate of total exposure (hours/year) nor cumulative total exposure
was associated with risk for melanoma. Analyses by body site showed no consistent
association with exposure to lights without diffusers. Adjustment for measures of total and
intermittent exposure to the sun did not alter the results. Subjects were also asked about
exposure to plan printers, laboratory equipment emitting UVR, insect tubes, black lights and
photocopiers. No association was seen with any of these sources, although the number of
exposed subjects was small. The odds ratio for any use of sunlamps was 1.1 (95% CI, 0.6-1.8),
although few subjects had used sunlamps (Holman et al., 1986b).
Sorahan and Grimley (1985) examined fluorescent light exposure in 1980-82 in a case-
control study in the United Kingdom, described in detail on p. 103. Information on exposure
was confined to whether lights were 'mainly on' or 'sometimes on' at work. After adjustment
for age and sex, no consistent association was seen for duration of exposure when cases were
compared with electoral register controls.
Dubin eta/. (1986) examined fluorescent light exposure in a subset of subjects in a case-
control study in New York, USA, described on p. 108. Subjects were interviewed and/or sent
postal questionnaires. In data obtained from interview, but not in data obtained from postal
questionnaires, the odds ratios increased with average daily exposure in the five years before
interview, after adjustment for age and sex (p value for linear trend, < 0.05). A similar
pattern was seen for exposure 6-11 years and 11-20 years previously.
Elwood et al. (1986) examined fluorescent light exposure in their case- control study in
the United Kingdom in 1981-84, described in detail on p. 103. Subjects were interviewed and
later sent postal questionnaires to validate the responses. From the interview data, exposure
to undiffused lights at work was associated with an odds ratio of 4.0 (95% CI, 0.8-19.2) for
those maximally exposed (p value for trend = 0.2). Control for constitutional factors did not
change the results. From the questionnaire data, the odds ratio for maximal exposure
(undiffused lights) was 1.9 (95% CI, 0.4-8.4). No association was seen with exposure at
home, and no association was seen for use of sunlamps. Subjects were also asked about
exposure to particular or unusual light sources, such as vacuum or discharge lamps, insecti-
cidal or germicidal lamps or welding equipment. The odds ratio for exposure to any such
source was 2.2 (95% CI, 1.0-4.9). (The Working Group noted that the use of open-ended
questions about lighting sources may have introduced recalJ bias.]
In the Western Canada case-control study in 1979-81 (see Elwood et al., 1984, 1985a,b,
p. 107), no association was seen with use of sunlamps (x2 = 6.1, 5 df) (Gallagher eta/., 1986).
132
IARC MONOGRAPHS VOLUME 55
0sterlind et al. (1988b) examined exposure to fluorescent lighting at work and use of
sunlamps and sunbeds in their case-control study in Denmark in 1982-85, described on
pp. 103-104. The same proportions of cases and controls reported having been exposed to
fluorescent lights at work, and no association was seen with age at first exposure, duration of
exposure or type of work place. Past use of sunlamps was also not associated with melanoma,
and a smaller proportion of cases than controls had ever used sunbeds (odds ratio, 0.7; 95%
CI, 0.5-1.0).
In a case-control study in Scotland (Swerdlow eta/., 1988), 180 cases aged 15-84 from
three clinics during 1979-84 were compared with 197 age- and hospital-matched patients
with various non-malignant diseases. Subjects were interviewed about exposure to fluo-
rescent lights and UV lamps, use of sunbeds, sun exposure and constitutional factors.
Controls with skin conditions were excluded from the analysis of UV lamps and sun beds. No
consistent association was seen with exposure to fluorescent lights at home or at work, with
or without adjustment for constitutional factors and sun exposure. Significant, positive
associations were seen for duration of use of UV lamps and sunbeds (p value for trend,
< 0.05). The odds ratio for use for more than one year was 3.4 (95% CI, 0.6-20.3) after
adjustment for constitutional factors and sun exposure. Amount of use within five years (1.9;
0.6-5.6) of the interview and more than five years (9.1; 2.0-40.6) before the interview were
both positively associated with the risk for melanoma.
MacKie eta/. (1989) examined use of sunbeds and sunlamps in their case- control study
in Scotland described on p. 106. Use was associated with melanoma in men (odds ratio, 2.6;
95% CI, 0.9-7.3) but showed little association in women (1.5; 0.8-2.9). The effect on men
largely disappeared after adjustment for sun exposure and constitutional factors.
In the study of Zanetti eta/. (1988) from Thrin, Italy, described in detail on p. 104, an
odds ratio of 0.9 (0.4- 2.0) was found for use of UVA lamps, although few subjects reported
exposure.
A large population-based case-control study on occupational exposures was conducted
during 1979-85 in Montreal, Canada (Siemiatycki, 1991). Overall, there were 3730 male
cases of cancer aged 35-70, including 124 cutaneous melanoma cases; the participation rate
was 82%. Each cancer site was compared with the other cancer sites. Exposure to 293 agents,
including arc welding fumes and UVR, was assessed by a team of chemists and industrial
hygienists on the basis of each individual's occupational history. Neither arc welding fumes
nor exposures to UVR was associated with the risk for cutaneous melanoma (odds ratios, 0.5;
90% CI, 0.3-1.1 and 0.3; 0.1-1.5, respectively).
In a population-based study in southern Ontario, Canada (Walter eta/., 1990), 583 cases
identified from pathology laboratories and from the cancer registry between 1984 and 1986
were compared with 608 controls randomly sampled from property tax rolls. Participation
rates were 90% for cases and 80% for controls. Odds ratios for any use of sunbeds or
sunlamps were 1.9 (95% CI, 1.2-3.0) in men and 1.5 (0.99-2. 1) in women. Adjustment for
constitutional factors did not affect the results. The odds ratios increased with duration of
use; for more than 12 months' use, the odds ratios were 2.1 (0.9-5.3) in men and 3.0(1.1-9.6)
in women.
Table 26. Case-control studies of melanoma of the skin and exposure to fluorescent lights
Country Cases/controls Odds ratio 95% Cl Definition of exposure
Reference
Australia 274/549 2.6a,b
1.2-5.9
Indoor workers, 20 years' occupational exposure
Beral eta/. (1982)
4.3o.b NR
Office workers, 20 years' occupational exposure
USA 114/228 0.7 NS Any exposure
Rigel eta/. (1983)
0.6 NS
Any exposure, office workers
Australia 337/349 1.20,0
O.S-1.9 35 000 h exposure
English et a/.
1.2a,b
0.7-1.9 1600 h per year
(1985)
1.3a,b
O.S-1.9
:? 22 500 h undiffused lights
en
1.2a,o
O.S-1.9
1300 h per year undiffused lights
1.2a,b
0.6-2.6
.:? 22 500 h head, neck, upper limbs, undiffused lights
t:1
United 58/333 0.6 NR
:? 20 years, occupational exposure (mainly on)
Sorahan &
-tT1
Kingdom
0.5 NR
20 years, indoor workers only (mainly on)
Grimley (1985)
en
USA 1103/585 2.3 1.0-5.8
.:? 9 h per day, 0-5 years previously (interview)
Dubin eta/.
0
'Tl 508/222 0.6 0.3-1.3
.:? 9 h per day, 0-5 years previously (postal
(1986)
(")
questionnaire)
> United 83/83 1.4a.b
0.4-5.1
50 000 h occupational exposure (total fluorescent
Elwood et al. z
(") Kingdom
light, interview)
(1986)
tT1 4.oa,b
O.S-19.2
50 000 h occupational exposure (undiffused lights,
interview)
-z 67166 l.za.b
0.3-5.7
50 000 h occupational exposure (total fluorescent
::z::
1.9a,b
light, postal questionnaire)
c::
0.4-8.4
:? 50 000 h occupational exposure (undiffused lights,
postal questionnaire)
Denmark 474/926 No association
Duration of exposure, age at first exposure, type of
0sterlind eta/.
Cll
workplace
(1988b)
Scotland, 180/197 1.2b
0.7- 1.9
Any occupational exposure < 5 years previously
Swerdlow et a/.
United O.Bb
0.4-1.4
Any exposure at home < 5 years previously
(1988)
Kingdom 1.6b
0.9-2.6
5 h per day < 5 years previously at work and at
1.4b
0.9-2.3 home
0.8b
0.4- 1.4
Any occupational exposure > 5 years previously
Any residential exposure > 5 years previously
NR, not reported; NS, not significant
0
0dds ratio for category with highest level of exposure
b Adjusted for sun exposure
w
134 IARC MONOGRAPHS VOLUME 55
2.2.3 Malignant melanoma of the eye
In the case- control study carried out in Philapelphia. USA. which is described in detail
on p. 128, cases of uveal melanoma were more likely to report use of sunlamps than controls.
After adjustment for age. eye colour and a history of cataracts, there was a trend to increasing
risk with frequencyofuse(odds ratio for frequent versus never, 2.1; 95% CI, 0.3-17.9; test for
linear trend over four levels: p = 0.10). The odds ratios for those who had ever worked as
welders was 10.9 (2.1-56.5) (Tucker et al., 1985b).
In the case- control study from San Francisco, USA. described on pp. 128-129, exposure
to artificial UV light or 'black light' [details not given] conferred over three-fold risks for
intra-ocular melanoma after adjustment for other significant factors (odds ratio, 3. 7; 95% CI,
1.6-8. 7). The odds ratios were 2.9 for 1-5 years of exposure and 3.8 for 6 or more years (Holly
et al., 1990).
In the case- control study from Boston, USA (Seddon et al. , 1990), described on p. 129,
exposure to fluorescent lighting was associated with an elevated risk of uveal melanoma
(odds ratio, 1.7; 95% CI, 1.1-2.5 for 40 h or more per week as compared to no exposure) in
the larger data set, based on case- sibling comparison. In the population-based comparison,
the corresponding odds ratio was 1.2 (95% CI, 0.6-2.1). A history of working with welding
arcs was reported with similar frequency among cases and controls in both comparisons.
Cases reported more frequent use of sunlamps in comparison with both sets of controls.
After adjustment for constitutional factors and exposure to the sun, the odds ratios for
frequent/occasional use versus never were 3.4 (1.1-10.3) in the population comparison and
2.3 (1.2-4.3) in the sibling comparison.
In the large Canadian study on occupational exposure, described on p. 132, 23 cases of
ocular melanoma were included. Analysis only of French Canadians revealed four cases of
eye melanoma with exposure to arc welding fumes (odds ratio, 8.3; 90% Cl, 2.5-27.10)
(Siemiatycki, 1991). No increase was found for substantial exposure; no increase in risk was
reported for exposure to UVR.
2.3 Premalignant conditions
2.3.1 Basal-cell naevus syndrome
Basal-cell naevus syndrome is a hereditary condition (Gorlin, 1987) in which affected
family members may show, among other major manifestations, an apparent excess of basal-
cell carcinomas. These seem to occur more commonly in sun-exposed parts of the body or in
unusual patterns. There is no other evidence that solar radiation plays a role in their
development.
2.3.2 Dysplastic naevus syndrome
Dysplastic naevus syndrome is a hereditary condition in which affected family members
have multiple dysplastic naevi and a greatly increased risk of malignant melanoma (Green et
al., 1985b). The distribution of tumours conforms to the usual distribution, and there is
anecdotal evidence that solar radiation plays a role in their development (Kraemer &
Greene, 1985).
.
STUDIES OF CANCER IN HUMANS 135
2.4 Molecular genetics of human skin cancers
Analysis of mutations in DNA isolated from tumours and believed to be relevant to
carcinogenesis can potentially help in making a causal link with exposures to carcinogens.
Two important qualifications must, however, be borne in mind. Firstly, the changes detected
may have arisen late in tumour development (whether or not the tumour is the result of
exposure to UVR) and may not be involved in initiation or other early steps. Secondly, the
spectrum of mutations that is seen may be constrained to those changes that can lead to a
functional gene product. This qualification applies, for example, to mutations that activate
ras genes but to only a lesser extent to tumour suppressor gene mutations in which
inactivation of gene function is involved.
Experimental studies indicate that UV-induced mutations have a distinctive pattern of
base-substitution mutations (see section 4.5):
- Virtually all mutations occur at dipyrimidine sites, especially 5'TC and 5'CC
sequences.
- The majority of the base substitution mutations involve cytosine with the C-+T
transition predominating.
- Tandem 5'CC-+5'TT mutations occur.
2.4.1 ras Gene mutations
Primary melanomas, metastases and cell lines derived from melanomas which
developed at body sites characterized as exposed rarely', intermittently' or continuously' to
the sun were analysed for the presence of N-ras mutations. Of 37 cutaneous melanomas,
seven had N-ras mutations; all were from ' continuously' exposed sites. All mutations in the
N-ras gene were at TT or CC sites, which are potential locations for mutagenic UV photo-
products, suggesting a role of sun exposure in N-ras mutation (van't Veer et al., 1989).
In several investigations, base-substitution mutations were found in Ha-, Ki- and N-ras
genes in human skin melanomas (Thble 27) and in squamous-cell and basal-cell carcinomas
(Table 28) from xeroderma pigmentosum and normal patients. In single studies, Ha- and
N-ras gene amplification was found in squamous-cell carcinomas of the skin (Ananthaswamy
& Pierceall, 1990), and loss of the Ha-ras allele was seen in basal-cell and squamous-cell
carcinomas (Ananthaswamy et a/., 1988). Whether exposure to the sun was involved in
tumour induction in these studies is, however, less clear.
2.4.2 p53 Gene mutations
Brasher a/. (1991) found p53 mutations at various codons in 14 out of24 (58%) invasive
squamous-cell carcinomas from sun-exposed skin (Table 29). The mutations found were
predominantly C-+T (5 of 14 total mutants, 36%) and CC-+TT (3 of 14, 21 %) transitions,
exclusively at tandem pyrimidine stretches. This finding is consistent with the hypothesis that
these mutations are induced by UV irradiation. CC-+ TT double-base changes in the p53
gene have not yet been found in tumours in any internal organ. These results strongly suggest
that solar radiation plays a role in the induction of p53 gene mutations.
Pierceall eta/. (1991) found p53 mutations in exon 7 in 2 out of 10 squamqus-cell
carcinomas from sun-exposed body sites; one was a C-+ T transition and the other a C-+A
transversion .
......
w
Table 27. ras Gene mutations detected in human naevi and primary and secondary melanomas that developed at
a..
sites subject to sun exposure
Oncogene Base change Base-substitution Site of original tumour Reference
codon mutation
N-ras-61 GGA CAAGAA
AAA C to A Neck van't Veer et al. (1989)
AAA C to A Lower leg van't Veer et al. (1989)
AAA CtoA Nose van't Veer et al. (1989)
AAA CtoA Cheek van't Veer et al. (1989)
-
CGA [Tto C] Lower leg van' t Veer et al. (1989)
CAT [T to A!GJ Xeroderma pigmentosum patient" Keijzer eta/. (1989)
n
CAT (T to A] Site unspecified, probably metastasis Sekiya et a!. (1984)
N-ras-13 GGT GGTGTT
0
GAT (C toT] Finger van't Veer eta/. (1989) z
GTT [C to A] Finger van't Veer eta/. (1989) 0
GTT [C to A] Lower leg van't Veer et al. {1989)
0
N-ras-12 GAT [C toT) Leg van't Veer eta/. (1989)
N-ras-61 CATIC [T to A/G) Back Shukla et a/. (1989)
'"0
:I:
Ki-ras-61 GGA CAAGAA
(/)
AAA CtoA Lower leg Shukla et al. (1989)
d
Ki-ras-12 GCT GGTGGC
TGT (C to A] Abdomen Shukla et a/. {1989)
TGT [C to A] Knee Shukla et al. (1989)
TGT [C to A] Site unspecified, probably metastasis Shukla et al. (1989)
CTl
Vl
TGT [C to A] Site unspecified, probably metastasis Shukla et al. (1989) Vl
TGT [C to A) Site unspecified, probably metastasis Shukla et al. (1989)
TGT [C to A] Site unspecified, probably metastasis Shukla et al. (1989)
[C toT] Buttock Shukla et al. (1989)
[C toT] Site unspecified, probably metastasis Shukla er at. (1989)
[C toT] Forearm (naevus) Shukla et al. (1989)
[C toT) Abdomen (naevus) Shukla er al. (1989)
Ha-ras-12 GCC GGCGGr
TGC [C to A] Abdomen Shukla et a/. (1989)
Italics indicate potential pyrimidine dimer site including neighbouring codon; ( ], base changes occurring in anti-sense strand
"Malignant melanoma probably resulting from metastasis of a primary skin tumour
Table 28. ras Gene mutations detected in human keratoacanthomas (KA), basal-cell carcinomas (BCC) and
squamous-cell carcinomas (SCC) that developed at sites subject to sun exposure
Oncogene Base change Base-substitution Thmour Site Reference
codon mutation
Ki-ras 12 GerGGTGGC
TGT {C to A] sec Lip van der Schroeff eta/. (1990)
BCC Shoulder van der Schroeff et a/. (1990)
BCC Neck van der Schroeff et a/. (1990)
GAT [CtoT] BCC Face van der Schroeff et a/. (1990)
Ha-ras 61 GGCCAGGAG
erG (T to A) sec Not specified Cororninas et at. (1989)
erG (T to A] KA Not specified Corominas eta/. (1989)
CAT [C to A] BCC Face van der Schroeff et at. (1990)
AAG CtoA KA Not specified Corominas et al. (1989)
Ha-ras 12 GCC GGCGGT
AGC [C toT] sec Not specified Corominas et al. (1989)
AGC [C toT] KA Not specified Corominas et al. (1989)
AGC [C toT] KA Not specified Corominas et a/. (1989)
TGC (C to A] sec Not specified Corominas et al. (1989)
TGC [C to A] sec Not specified Corominas et al. (1989)
Italics indicate potential pyrimidine dimer site including neighbouring codon; [ ), base changes occurring in anti-sense strand
(/')
....,
c:::
'='
-
rn
0
"Tl
(")
>
z
(")
m
::0
-z
:I:
>
z
(/')
.....
I.>)
-..l
138
IARC MONOGRAPHS VOLUME 55
Table 29. p53 Thmour suppressor gene mutations in human squamous-cell carcinomas
that developed at sites subject to sun exposure
Codon Nucleotide Base-substitution Incidencea Site of tumour Reference
sequence mutation origin
7 TCf TGT; C-+G 1114/24 Preauricular Brash et al. (1991)
56 T TCA TAA; C--+A l/14/24 Chest Brash eta/. (1991)
1041105 CG ccr deletion of a C 2/14/24 Preauricular/temple Brash eta/. (1991)
151 ccccc CAC; C--+A 1/14/24 Scalp Brash et at. (1991)
152 CC CCC CAC; C--+T 1114/24 Hand Brash et al. (1991)
179 A CCA CAA; C--+A 1114/24 Scalp Brash eta/. (1991)
244 CCGG TCG; C--+T 1/2/10 Face Pierceall eta/. (1991)
245 G CCG CAG; C--+A 1114/24 Cheek Brash et al. (1991)
245 G CCG T T; CC-+TT 1/14/24 Chest Brash eta/. (1991)
247/248 AC CG T T; CC--+TT 1/14/24 Nose Brash et al. (1991)
248 GCC GAC; C-+A l/2/10 Face Pierceall eta/. (1991)
258 T TCC TTC; c-T 1114/24 Face Brash eta/. (1991)
278 TCCT TCT; C--+T 1114/24 Cheek Brash eta/. (1991)
285/286 TC CT T T; CC--+TT 1114/24 Face Brash et al. (1991)
286 TCCT CTT; C--+T 1114/24 Forehead Brash et aL (1991)
317 CC CCA TCA; C--+T 1114/24 Postauricular Brash et al. (1991)
Italics indicate potential pyrimidine dimer site
UNo. of specific mutations/no. of total mutations foundfl'otal number of samples tested only from sites
continuously exposed to the sun
3. Studies of Cancer in Animals
3.1 Experimental conventions
3.1.1 Species studied
The experimental induction of skin cancers in mice following exposure to a mercury-arc
lamp was first reported by Findlay (1928). Initially, haired albino mice were used, but hairless
and nude mice are now preferred.
An important development was the use of the hairless mouse as a model (Winkelmann
et al., 1960, 1963). In haired animals, the fur provides effective protection of the skin against
UVR. This limits investigations to sparsely haired skin regions, mainly the ears, as, in long-
term experiments with frequent exposures, the mechanical trauma caused by shaving might
influence the process of tumorigenesis. The skin of hairless mice differs, however, from
human skin in many respects. It is, for instance, much thinner and has abnormal hair follicles.
The hairless mouse does, however, have a thymus and a functioning immune system, in
contrast to the nude mouse (Eaton eta/., 1978; Hoover et al., 1987). Many recent studies on
carcinogenesis induced by UVR used the hairless mouse model (Forbes et al., 1981; de Gruijl
eta/., 1983; Gallagher et al., 1984b}. The changing designations of 'Skh' mice are listed in
Table 30. Skin tumorigenicity has been evaluated experimentally in only a relatively small
number of species other than the mouse.
Table 30. Alternative designations used for 'Skh' outbred stocks of hairless mice
Phenotype 1970--86 After 1986
Albinob Skh: hairless-1 Skh:hr I
Pigmentedc Skh: hairless-2 Skh:hr II
(any colour)
llf'rom Forbes et al. (1990)
bforbes er a/. (1981); de Gruijl et al. (1983)
'Davies & Forbes (1988)
3.1.2 Wavelength ranges
Synonyms used
in the literature
Sk-1; Skh-1; Skh/Hr-1;
Skh:HR; HRA/Skh-1;
Skh-hrl
Sk-2; Skh-2; Skh/Hr-2
Inbred strains derived
from Skh:hr stocka
HRA/Skh (Temple Uni-
versity, Philadelphia, PA.
USA)
HRA/Skh-1 (University
of Sydney, Sydney,
Australia)
As noted in section 1.1, for the purposes of this monograph, the UV wavelength range is
subdivided according to the convention of the Commission Internationale de l'Eclairage
(1987) into: UVA (315-400 nm), UVB (280-315 nm) and UVC (100-280 nm). The UVB
-139-
140 IARC MONOGRAPHS VOLUME 55
range is generally found to be most effective in inducing skin cancer, i.e., tumorigenesis may
be achieved with smaller doses of radiant exposure than with UVA and UVC. A complete
discussion of wavelength ranges is given in section 1.1.
3.1.3 Measured doses
Many investigators of the carcinogenicity of UVR have reported the type of lamps they
used, which are frequently broad-spectrum lamps, sometimes in combination with filters.
When estimates of the doses of UVR administered are given, the measuring instrument is
usually mentioned and the result is given in terms of irradiance or dose, with no further detail.
Such information is of some value, especially for comparing the results of experiments in
which the same type of lamps were used.
The action spectrum (see section 1) given in Figure 10 shows that the carcinogenic
effectiveness of UVR in hairless mice changes steeply, even by orders of magnitude, over a
wavelength range of 10 or 20 nm. This pattern indicates that irradiance must be spectralJy
specified in order to be meaningful, and not integrated into one value over a broad spectrum.
One approach is to give irradiance weighted according to the action spectrum for UV
carcinogenesis, but this is available only in provisional form (see Fig. 10 and discussion on
pp. 46-47). Another approach is to provide data on erythemally weighted irradiance, since
the action spectrum for erythema corresponds approximately to that for carcinogenesis
(Forbes et al., 1978). A simple, direct way of calculating this is to relate the doses admi-
nistered to the minimal erythema dose or to the minimal oedemic dose for the animal being
investigated. When investigators supplied such measures of effect, they are mentioned in the
summaries below.
In experimental situations, there is never a perfectly sharp cut-off of wavelengths. The
expression 'mainly UV .A: is of questionable value, because even if UVB represents only 0.1%
of the emission spectrum, it may still dominate the effect (see pp. 144-147, 151 and Fig. 10).
Terms such as 'mainly UVB' are used below only when there are good reasons to assume that
the effects considered are due mainly to UVB radiation.
3 .1. 4 Protocols
Experimental investigations on the carcinogenicity of UVR, conducted mostly on mice,
have been reviewed (Blum, 1959; Urbach eta/., 1974; K.ripke & Sass, 1978; WHO, 1979; van
der Leun, 1984; Epstein, 1985).
Hundreds of studies have been reported. Most were not designed to test whether or not
the radiation used was carcinogenic per se but to investigate the process of UV carcino-
genesis. The methods used in these studies differ in many respects from those in standard
lifetime studies to evaluate the carcinogenicity of chemicals. For example, many studies do
not give complete details of the UVR emission spectrum used or exposure dose, do not
enumerate all tumours, do not provide data on survival or do not provide histological details
of tumours. Control groups are not always included; however, spontaneous skin tumours are
rare in mice and rats. In many of the studies presented in detail below, appropriate statistical
analyses have been done demonstrating clear dose-related trends in numbers of tumour-
bearing animals, number of tumours per animal and/or median time to first tumour.
STUDIES OF CANCER IN ANIMALS 141
Fig. 10. Sterenborg-Slaper action spectrum for ultraviolet-induced skin carcinogenesis
(1.0-mm tumours) in albino hairless mice. Effectiveness is defined as the reciprocal of the
daily dose at each wavelength that leads to tumours of 1-mm diameter in SO% of animals in
265 days, relative to the corresponding value at the wavelength of maximal effectiveness. The
effectiveness between 340 and 400 nm represents an average value for that wavelength range.
VI
VI
Q)
c
Q)
>
-0
Q)
-
....
Q)
Q)
>
-
10"
3
0
Q)
a:::
10"
10. L.__ ___ __._ ____ _._ ___ ___,
250
From van der Leun (1987a)
3.2 Broad-spectrum radiation
3.2.1 Sunlight
300 350
400
Wavelength (nm)
In one study by Roffo (1934), 600 rats [sex and strain unspecified) were exposed to solar
radiation (sunlight) at a latitude of 35 S in Buenos Aires, Argentina. The average exposure
was for 5 h per day, with avoidance of the hours around solar noon in the summer. In the first
days, 365 rats died from sunstroke. Of the 235 remaining animals, 165 (70%) developed
tumours. There were 140 tumours of the ear (58% squamous-cell carcinomas; 36% spindle-
cell sarcomas; 6% carcinosarcomas); 58 eye tumours (tumours of the conjunctiva, 100%
spindle-cell sarcomas; tumours of the eyelid, 50% squamous-cell carcinomas and 50%
spindle-cell sarcomas); and 15 other tumours, mainly squamous-cell carcinomas, at sites
including the nose, tail, paw and neck. In complementary experiments reported in the same
paper, groups of animals were exposed either to sunlight filtered through various colours of
glass, to radiation from various types of lamp (quartz mercury, glass mercury, neon gas and
142 IARC MONOGRAPHS VOLUME 55
filament lamps) or to short Hertzian wavelengths. Tumours [types and sites unspecified] were
observed in all 150 animals exposed to quartz mercury lamps; no tumour was induced in any
other experimental group. On the basis of this evidence, the author concluded that the
carcinogenicity of sunlight could be attributed to UVR.
In another report by Roffo (1939), 2000 white rats and mice [exact numbers unspecified)
were exposed to sunlight for an average of 5 h per day. After three to six months, benign
neoplasms and, after seven to nine months, malignant neoplasms of the skin of the ear (88%
of all malignant tumours), the forepaw (7.25%), the tail (2%) and nose (one tumour) deve-
loped in 600 animals; 25% of the tumours were seen on the eyes. The ear tumours were
diagnosed as squamous-cell carcinomas (58%), spindle-cell sarcomas (36%) and carcinosar-
comas (6%) by detailed histological examination. Similarly, the paw tumours were diagnosed
as squamous-cell carcinomas ( 42%) and spindle-cell sarcomas (58%); the tumours of the tail
were all squamous-cell carcinomas. The distribution of tumours of the eye was similar to that
in the study of Roffo (1934). (The Working Group considered that these are exceptional
studies which fully document the carcinogenicity of solar radiation in rats and mice, even
though quantitative detail is lacking. The resulting neoplasms are described and photo-
graphically illustrated in exact detail. The Working Group accepted the weight of evidence
contained in these studies as to the carcinogenicity of solar radiation to rats and mice.)
Domestic and other animals of many species (cows, goats, sheep (reviewed by Emmett,
1973), cats (Dorn eta/. , 1971) and dogs (Madewell eta/., 1981; Nikula eta/., 1992)) develop
skin tumours, and there are good indications that sunlight is involved. The tumours described
generally developed in sparsely haired, light-coloured skin. Cancers of the eye occur in many
species, including dogs, horses, cats, sheep and swine, but are particularly frequent in cattle
(Russell eta/., 1956).
3.2.2 Solar-simulated radiation
In several investigations on carcinogenesis by UVR, 'solar-simulated radiation' was used
(Forbes et al., 1982; Staberg eta/. , 1983a; Young eta/., 1990; Menzies eta/., 1991). In one
large, particularly informative experiment (Forbes et al., 1982), more than 1000 hairless
albino Skh-hrl mice were exposed to solar-simulated radiation from a xenon arc lamp, with
various filters to make the spectral distribution in the UV region similar to that of sunlight
under various thicknesses of the ozone layer. The exposures lasted for up to 80 weeks. More
than 90% of the mice developed skin tumours, predominantly squamQus-cell carcinomas.
The time to development of 50% of first tumours was shorter after exposure to the spectra
that included higher irradiance in the wavelength range 290-300 nm. The other experiments
mentioned were more limited and dealt with more specialized aspects ofUV carcinogenesis.
3.2.3 Sources emitting UVC, UVB and UVA radiation
Sources emitting radiation in the entire UV wavelength range were used in experiments
on UV carcinogenesis mainly between 1930 and 1960.
(a) Mouse
Gradyet al. (1943) exposed 605 strain A mice to broad-spectrum UVR at a wide range of
doses and irradiances (weekly doses, 3.6-43 x 10
7
ergs/cm2 [40-430 kJ/m
2
]; Blum &
'
STUDIES OF CANCER IN ANIMALS 143
Lippincott, 1942). The investigation dealt primarily with skin tumours (mainly spindle-cell
sarcomas). About 5% of the mice developed tumours of the eye. Histological examination by
Lippincott and Blum (1943) showed that the eye tumours arose mostly in the cornea and were
spindle-cell sarcomas or fibrosarcomas; haemangioendotheliomas were also found.
A particularly large, informative series of investigations was carried out with unfiltered
medium-pressure mercury arc lamps which emitted UVC, UVB and UVA (Blum, 1959).
More than 600 strain A mice were irradiated (daily dose, 0.32-8.6 x 10
7
ergs/cm
2
[3-86
kJ/m
2
)) in a series of investigations dealing with various aspects of UV carcinogenesis; the
dose-effect relationship was addressed particularly. In most of the experiments, more than
90% of mice developed skin tumours, mainly of the ears, the only site for which quantitative
data were given.
(b) Rat
Findlay (1930) exposed six epilatedalbino rats to broad-spectrum UVR from a mercury-
vapour lamp at a distance of 18 in (46 em] for 1 min three times a week. Rapidly growing
papillomas were reported in one rat. The time required was, however, much Jonger than in
mice exposed similarly, namely, 21 months as compared to eight months for mice.
Putschar and Holtz (1930) exposed 35 rats [strain unspecified) with very low sponta-
neous tumour incidence to almost continuous irradiation with broad-spectrum UVR from a
quartz mercury lamp for 11 months. They reported regular occurrence of skin tumours,
including papillomas, squamous-cell carcinomas and, occasionally, basal-cell carcinomas.
The tumours were first seen after 27 weeks of exposure.
Huldschinsky(1933) exposed seven white rats to UVR from a solar lamp for2 h per day,
six days per week for one year or more. Another group of five rats was exposed to a quartz
lamp emitting a predominantly UVC waveband ( < 270 nm). The doses given per session
were about 10 times higher than those used in phototherapy. Spindle-cell sarcomas of the eye
were found in 217 and 5/5 rats in each group, respectively.
Hueper (1942) reported squamous-cell carcinomas and, rarely, spindle-cell carcinomas
and sarcomas, round-cell carcinomas and basal-cell carcinomas of the skin in 20 rats [strain
unspecified] exposed for up to 10 months to broad-spectrum UVR from a mercury vapour
burner (a Hanovia Super S Alpine lamp) at a distance of 75 em.
In a study by Freeman and Knox (1964), a group of 78 rats (66 pigmented and 12 un-
pigmented) was exposed to broad-spectrum UVR from mercury lamps at 50 em from the skin
on five days a week for one year; the doses per session corresponded to approximately
1 MED for rat skin. A total of 98 eye tumours developed, with more tumours in pigmented
rats. The tumours arose in the corneal stroma; two-thirds were diagnosed as fibrosarcomas
and one-third as haemangioendotheliomas.
(c) Hamster
Hamsters exposed to an irradiation regimen similar to that described above also
developed eye tumours (Freeman & Knox. 1964). In 19 animals (9 pigmented, 10 un-
pigmented) exposed for one year, haemangioendotheliomas and fibrosarcomas developed in
14 eyes.
144 TARC MONOGRAPHS VOLUME 55
(d) Guinea-pig
Guinea-pigs were exposed to the same regimen as described above. None of 17 animals
developed a tumour of the eye (Freeman & Knox, 1964 ).
3.3 Sources emitting mainly UVB radiation
Many experiments have been carried out with sources emitting mainly UVB radiation, in
which increases in the number of tumour-bearing animals and/or in the number of tumours
per animal were seen (Blum, 1959; Winkelmann et al., 1963; Freeman, 1975; Stenback,
1975a; Daynes et al., 1977; Kripke, 1977; Spikes eta/., 1977; Forbes et al., 1981; de Gruijl et
a/., 1983; Gallagher eta/., 1984b). The most informative studies are described below.
3.3.1 Mouse
Freeman (1975) studied carcinogenesis induced by chronic exposure to narrow-band
UVB produced by a high-intensity diffraction grating monochromator with a half-power
band-width of 5 nm. Exposure was three times per week to one ear of each haired albino
mouse. Four wavelengths were used, and the doses were determined as the MED. Of a group
of 30 mice exposed to 300 nm (weekly dose, 60 mJ/cmZ), 16 developed squamous-cell
carcinomas of the ear. Of a group of 30 mice exposed to 310 nm (weekly dose, 750 mJ/cm
2
),
16 survived to 450 days and eight developed five squamous-cell carcinomas, two fibro-
sarcomas and one angiosarcoma of the ear. No skin tumour was observed among 30 mice
irradiated with UVR at 290 nm (weekly dose, 42 mJ/cm
2
); of five mice irradiated with 320 nm
(weekly dose, 4950 mJ/cm
2
), two developed squamous-cell carcinomas of the ear.
Two fibrosarcomas and one unspecified tumour of the eye were reported in 24 C3H/
HeN mice bearing 25 skin tumours (mostly fibrosarcomas) after exposure to UVR (168 J/m
2
three times a week) from Westinghouse FS40T12 sunlamps (280-340 nm) (Kripke, 1977).
In the experiment of Forbes eta/. (1981), groups of 24 male and female hairless albino
Skh:HR mice (the changing designations of sources of 'Skh' mice are listed in Thble 30), six to
eight weeks old, were irradiated on five days per week with Westinghouse FS40T12 sunlamps
(see Fig. 9c, p. 64), emitting mainly UVB (with < 1% below 280 nm; two-thirds at 280-
320 nm and one-third at > 320 nm). All animals had developed tumours by the end of the
experiment (up to 45 weeks), and a dose-response effect was demonstrated, as assessed by
time to tumours in 50% of animals (Thble 31 ). Histological examination showed tumours of 4
mm or more in diameter to be squamous-cell carcinomas; those of about 1-4 mm formed a
continuum from carcinoma in situ to squamous-cell carcinoma, and those less than 1 mm
comprised epidermal hyperplasia and squamous metaplasia tending toward carcinoma in
situ. Less than 1% of tumours were fibrosarcomas.
Six groups of 22-44 male and female Skh-hr 1 hairless albino mice (total, 199), six to
eight weeks of age, were exposed to daily doses ranging from 57 to 1900 11m
2
of mainly UVB
radiation from Westinghouse FS401L12 sunlamps; this dose range encompassed a factor of
33. Most of the animals developed skin tumours, although even the highest daily dose was
sub-erythemic. A clear-cut relationship was shown between daily dose and time required for
50% of animals to develop skin tumours, which were predominantly squamous-cell
carcinomas (Fig. 11 ). Squamous-cell carcinomas developed in 71% of the mice in the lowest
STUDIES OF CANCER IN ANIMALS
Table 31. Dose-response to ultraviolet radiation
of hairless Skh:HR mice
Daily dose
Time to 50% tumour Terminated
(Jfm2)
incidence (weeks) at week
420
38.6 45
587
33.3 45
822 29.2 45
1152 20.0 36
1613 17.6 36
2259 12.9 25
From Forbes et al. (1981)
145
Fig.ll. Dose-effect relationship for the induction of< 1-mm skin tumours in hairless mice
by exposure to UVB radiation over a wide range of daily doses; tm, median induction time
IOOOr---------------------------,
800
500
300
t: 100
.....
80
50
'-----'---'-....._.'-'-..... j_ ___ ___,_ __ ~ _ _ _ ~ _ _ _ _
3 5 1 0 30 50 80 1 00
Dose (as % of maximal dose)
From de Gruijl et al. (1983)
dose group, and two skin tumours were reported in a total of 24 nonirradiated control mice
(de Gruijl eta/., 1983).
In albino hairless Skh:Hr-1 mice irradiated with UVB or UVB plus UVA radiation three
times a week for 16 weeks, with a 17-week recovery period, the spectrum for UV tumori-
genesis was sharp and had a maximum near 300 nm (Bissett et al. , 1989).
146 IARC MONOGRAPHS VOLUME 55
3.3.2 Rat
Skin tumour induction was studied in a group of 40 shaven female NMR rats, 8-10 weeks
old at the start of the experiment. The animals were irradiated chronically at a distance of
37.5 em for 60 weeks with Westinghouse FS40T12 sunlamps (Fig. 9c), emitting mainly UVB
(weekly dose, 5.4-10.8 x 10
4
J/m
2
). A total of 25 skin tumours, most of which were papil-
lomas of the ears, developed in 16/40 animals (Stenback, 1975a).
3.3.3 Hamster
Stenback (1975a) irradiated 40 shaven female Syrian golden hamsters, 8-10 weeks of
age, using the same protocol as described above. A total of 30 skin tumours developed in
14/40 animals; 22 were papillomas (14 animals), four were keratoacanthomas (three
animals), one was a squamous-cell carcinoma of the skin and three were papillomas of the
ear (one animal).
3.3.4 Guinea-pig
Stenback (1975a) exposed guinea-pigs using the same protocol as above and found skin
tumours in 2/25 animals (a fibroma and a trichofolliculoma).
3.3.5 Fish
1\vo hybrid fish strains susceptible to melanocytic neoplasms by UVR were developed by
Set! ow eta/. (1989) by crossing platyfish and swordtails. A group of 460 fish were exposed to
mainly UVB radiation from Westinghouse FS40 sunlamps, filtered with acetate sheets
transmitting > 290 nm or > 304 nm at various doses (150 and 300 J/m
2
per day for > 290
nm; 850 and 1700 J/m
2
per day for > 304 nm) for 1- 20 consecutive days. There were 103
controls. Depending on the wavelength, the level, the number of days of exposure and the
strain, 19- 40% of the irradiated fish developed melanocytic tumours; 13 and 2% of the
controls in the two strains, respectively, developed such tumours.
3.3.6 Opossum
Monodelphis domestica, a South American opossum, is unusual in showing the pheno-
menon of photoreactivation (see Glossary) of pyrimidine dimers and erythema (Ley, 1985); it
also developed actinic keratoses and skin tumours (mainly fibrosarcomas and squamous-cell
carcinomas) on exposure to UVR from an FS-40 sunlamp (280- 400 nm) (Ley et al., 1987).
Animals were shaved regularly and exposed to mainly UVB radiation from Westinghouse
FS40 sunlamps, with relative emissions of 0.04, 0.27, 0.69, 1.0 and 0.09 at a dose of250 J/m
2
(which is approximately half of an average MED; see Fig. 9c) at 280, 290, 300, 313 and 360
nm, respectively. Eight of 13 animals developed localized melanocytic hyperplasia; 100
weeks after the start of the experiment, melanomas were found in 5/13 surviving animals. M.
domestica do not develop spontaneous melanomas, as was apparent in a much larger colony
not exposed to UVR. Exposure of another group to photoreactivating light after UV
irradiation reduced the incidence of melanocytic hyperplasia (3/17); this was considered to
be a precursor lesion of the melanomas, although photoreactivation could not be
demonstrated in the melanoma (Ley et al., 1989).
STUDIES OF CANCER IN ANIMALS 147
[The Working Group noted that the melanocytic lesions induced in fish and the South
American opossum differ histologically from human melanoma: they grow to a larger size
and do not metastasize readily.)
Ley et al. ( 1991) exposed groups of M. domestica to UVR from fluorescent sunlamps
(Westinghouse FS40; 280- 400 nm with a peak at 313 nm) three times a week for 70weeks at a
dose of250 J 1m
2
Besides skin tumours, tumours of the anterior eye were observed beginning
30 weeks after the start of exposure. At 69 weeks, 50% of the animals had eye tumours, which
were classified as fibrosarcomas of the corneal stroma. In animals exposed to UVR followed
immediately by photoreactivating light, tumours appeared later and in reduced numbers.
'Cancer eye' in cattle, which includes squamous-cell carcinoma of the eye and the
circumocular skin, is thought to be caused by solar UVR. In an attempt to confirm this
relationship experimentally (Kopecky et al., 1979), four Hereford cattle (which lack pigment
around the eyes) were exposed to UVB radiation from Westinghouse FS40 lamps. Three
cows developed grossly observable tumours ofthe eye, one of which was histopathologically
confirmed as a preneoplastic growth.
3.4 Sources emitting mainly UVC radiation
3.4.1 Mouse
Carcinogenicity studies have been performed mainly in mice, but no study is available in
which animals were exposed solely to UVC radiation. Several studies have been reported in
which the source of UVC radiation was low-pressure mercury discharge germicidal lamps,
which emit 90- 95% of their radiation at wavelength 254 nm and weaker spectral lines in the
UVB, UVA and visible light regions (Rusch et al. , 1941; Blum & Lippincott, 1942; Forbes &
Urbach, 1975; Lill, 1983; Joshi et al., 1984; Sterenborg et al., 1988). In all of these investi-
gations, the exposures induced tumours. Two of the most informative studies are described in
more detail below.
A group of 40 female C3H/HeNCr1Br mice were irradiated with these lamps at a weekly
dose of 3 x 10
4
J/m
2
Three animals died without tumours after 9, 43 and 63 weeks of
irradiation; all of the other animals had tumours. By 52 weeks, 97% of the animals had
developed skin tumours, with a median time to appearance of 43 weeks. The mean number
of tumours per tumour-bearing mouse was 2.9. Tumour histology was carried out in 29/37
mice. Of a total of 83 suspected tumours, 66 were squamous-cell carcinomas, 10 were
proliferative squamous lesions and 6 were invasive fibrosarcomas; one had the appearance
of a cystic dilatation (Lill, 1983). [The Working Group that resulted in IARC Monographs
volume 40 (IARC, 1986a) noted that the 4% UVB content of the source, representing a
weekly dose of 1170 11m
2
, could not be excluded as contributing to the induction of skin
tumours.]
Sterenborg eta/. (1988) presented evidence that the tumours they induced in albino
hairless mice were indeed due to UVC radiation. Groups of 24 male and female hairless
albino mice (Skh-hr1), 6-10 weeks of age, were exposed to UVC radiation from Philips
germicidal TUV 40W low-pressure mercury discharge lamps (mainly 254 nm) on seven days
a week for 75 min per day at 230, 1460 or 7000 J/m
2
(30 times the MED); this dose was 60%
less during the first seven days of the experiment. A total of 65 squamous-cell carcinomas of
148 IARC MONOGRAPHS VOLUME 55
the skin were found [number of animals with tumours not specified). Both the percentage of
tumour-bearing animals and the number of tumours per mouse were strongly dose-related.
By comparing their results with those of experiments with UVB, the investigators concluded
that (i) the UVB emitted by the low-pressure mercury discharge lamps was insufficient to
account for the induction of tumours at the rate found. as at least 850 days of exposure to the
UVB radiation present would be required to induce skin tumours at the rate observed, as
compared to 161 days with the low-pressure mercury discharge lamp used; (ii) there is a
qualitative difference between the effects of low-pressure mercury discharge and UVB
lamps, in that the tumours induced by the mercury discharge lamps were scattered more
widely over the skin of the mice than in the experiments with UVB; and (iii) the dose-effect
relationship for tumorigenesis was less steep with the mercury discharge lamps than with
UVB sources. [The Working Group noted that the evidence given to exclude UVB as
contributing to the induction of skin tumours does not obviate the possibility that some
interaction between UVC and UVB radiation led to tumour induction.]
3.4.2 Rat
Nine groups of 6 or 12 male CD-1 rats, 28 days of age, were shaved and exposed to
varying doses of UVC from Westinghouse G36T6L sterilamps emitting predominantly 254
nm (dose range, 0.08-26.0 x 10
4
J/m
2
) . Survival ranged from 75 to 92% for the nine
experimental groups. Keratoacanthoma-like skin tumours developed at a yield that was
approximately proportional to dose throughout the dose range 0.65-26.0 x 10
4
J/m
2
,
although no tumour was observed at 0.32 x 10
4
J/m
2
or below (Strickland eta/., 1979).
3.5 Sources emitting mainly UVA radiation
The carcinogenic properties of UVA radiation received little attention before the
introduction of UVA equipment for tanning, which led to the development of powerful
sources of UVA. Many experiments have now been performed, using mainly hairless mice, to
examine the possible carcinogenicity of UVA radiation (Zigman et al., 1976; Forbes et al.,
1982; Berger & Kaase, 1983; Staberg et al., 1983a,b; Kaase eta/., 1984; Santamaria eta/.,
1985; Strickland, 1986; van Weeldeneta/., 1986; Slaper, 1987; Kligman, 1988 [abstract]; van
Weelden eta/., 1988; Kligman et al., 1990 [abstract]; Sterenborg & van der Leun, 1990; van
Weelden et al. , 1990a; Kelfkens et al., 1991a; Kligman eta/., 1992). Some have shown no
induction of tumours (Staberg eta/., 1983a,b; Kaase et al., 1984; Kligman, 1988 [abstract]).
[The Working Group noted that the doses may have been too small (daily doses in the range
of 160 kJ/m
2
) 1983b) or the exposure period too short (Berger & Kaase, 1983;
Kaase eta/., 1984; Kligman, 1988 [abstract]), as noted by the authors in a subsequent report
(Kligman et al., 1992).) In the other experiments, tumours were induced. (The Working
Group noted that in some of the latter experiments either it is unclear whether UVB
radiation was sufficiendy excluded from the spectrum (Zigman eta/., 1976; Berger & Kaase,
1983; Staberg et al., 1983a; Santamaria et al., 1985) or the exclusion of UVB radiation was not
fully convincing (Strickland, 1986).]
Studies in which the exclusion of UVB radiation was documented to be sufficient and
which led to the induction of tumours by UVA in hairless mice were reported by van Weelden
eta/. (1986, 1988, 1990a), Slaper (1987), Kligman et al. (1990 [abstract], 1992), Sterenborg
STUDIES OF CANCER IN ANIMALS
149
and van der Leun (1990) and Kelfkens et al. (1991a). A few of the most informative studies
are described below.
Groups of 24 male and female albino hairless Skh-hr 1 mice were exposed to UVA
radiation from a bank of Philips TL40W /09 fluorescent tubes, filtered through a 10-mm glass
plate selected for strong absorption ofUVB radiation, for 12 h a day on seven days a week for
about one year, at which time the experiment was terminated. The daily dose was 220 kJfm2.
Most animals developed scratching lesions before they contracted skin tumours, which
occurred in all animals; the median time to tumour appearance was 265 days. At the end of
the experiment, the larger lesions were examined histologically: 60% were classified as
squamous-cell carcinomas, 20% as benign tumours, including papillomas and keratoacan-
thoma-like lesions, and 20% as mild cellular and nuclear atypia. The histological findings
were similar to those observed in a parallel experiment with UVB, but the tumours in the
UVA-exposed group appeared over a longer time span. Residual UVB radiation was
excluded as the cause of tumours in UVA-exposed mice on quantitative considerations: the
authors concluded that more than 100 000 times the UVB present would have been required
in order to induce tumorigenesis at the rate observed (van Weelden eta/., 1986, 1988).
Groups of 48 male and female hairless albino Skh-hr 1 mice were exposed to 220 kJ/m
2
UVA radiation ( > 340 nm) from four high-pressure mercury metal-iodine lamps (Philips
HPA 400 W), passed through Jiquid filters, for 2 h per day on seven days per week for up to
400 days. The spectrum matched that of a lamp used for tanning (the UVASUN 5000); UVB
was effectively excluded by the filters. Skin tumours developed in most of the animals, and 31
developed tumours before any scratching was observed. The largest tumours were examined
histologically at the end of the experiment: 15/20 tumours examined were squamous-cell
carcinomas (Sterenborg & van der Leun, 1990).
The desire to tan safely has raised interest in the possible carcinogenicity of long-wave-
length UVA (340-400 nm). In some experiments, UVB was excluded so rigorously that there
was also very little UVA in the range 315-340 nm; exposure was therefore mainly to
wavelengths in the region of 340-400 nm (van Weelden et al., 1988; Sterenborg & van der
Leun, 1990; van Weelden et al., 1990a). These experiments yielded squamous-cell carci-
nomas in most animals. [The Working Group noted that if these were to be ascribed to the
small proportion of shorter-wavelength UVA present in the spectra, a sharp peak in the
action spectrum for UV carcinogenesis would have to occur between 330 and 340 nm, which
does not appear likely.] In experiments by Kligman eta/. (1990 [abstract], 1992), wave-
lengths shorter than 340 nm were filtered out rigorously. Female hairless albino Skh-hr 1
mice were exposed several times per week for 60 weeks to UVA at wavelengths of 340-400
nm at daily doses of 360 and 600 kJ 1m
2
, as used in artificial suntanning. Eighteen weeks later,
44 surviving mice had 19 skin tumours, mostly papillomas. At week 100, 22 surviving mice
had 40 tumours, many of which were considered clinically to be squamous-cell carcinomas.
The carcinogenicity of short-wavelength UVA (315-340 nm) was investigated in one
experiment. Groups of 24 male and female albino hairless Skh:hr 1 mice were exposed to
average daily doses of 20 or 56 kJ/m
2
radiation from specially developed fluorescent tubes
with peak emission near 330 nm (UVB radiation was filtered out efficiently using a glass
filter) on seven days a week for 650 days. All mice in the high-dose group developed multiple
tumours, first mainly papillomas and later predominantly squamous-cell carcinomas. In the
150 IARC MONOGRAPHS VOLUME 55
lower-dose group, three mice developed skin tumours, all of which were papillomas. The
lamps also emitted long-wavelength UVA (340-400 nm), but in a proportion considered by
the authors to be too small to account for the rate of tumorigenesis observed (Kelfkens eta/.,
1991a). The investigators estimated the carcinogenic effectiveness of short-wavelength UVA
(315-340 nm) to be approximately five times greater than that of long-wavelength UVA
(340-400 nm).
3.6 Interaction of wavelengths
In daily life, the skin is exposed frequently to several wavelength ranges (UVA, UVB,
UVC) simultaneously, or to different combinations at different times. The simplest explana-
tion of an effect of such combined exposures is 'photoaddition', i.e., each exposure contri-
butes to the effective dose in an additive way. The validity of this hypothesis is one of the
assumptions underlying widely used concepts such as 'erythemal effective energy' and the
derivation of the action spectrum shown in Figure 10 (p. 141). It implies that any additional
exposure to an effective dose, in any wavelength region, increases the carcinogenic effect.
Several studies provide indications, however, that the situation is more complicated.
Interactions are seen between the effects of different wavebands that result in deviations
from photoaddition (for reviews, see van der Leun, 1987b, 1992). The literature on this topic
is controversial and cannot be summarized in detail here. The following two sections form an
attempt to give an overview and interpretation.
3.6.1 Interaction of exposures given on the same day
Several types of interactions have been reported between different wavelength ranges
administered simultaneously or in close temporal proximity. These have led to concepts of
processes such as:
- photorecovery: the effect of UVB or UVC is reduced by simultaneous or immediately
subsequent exposure to UVAor visible light [The Working Group noted that photo-
reactivation is a special case of photo recovery but applies only to species that have the
'photoreactivating enzyme', photolyase (see Glossary).];
- photoprotection: the effect of UVB or UVC is reduced by prior administration of
UVA or visible light;
- photoaugmentation: the effect ofUVB or UVC is enhanced by prior, simultaneous or
subsequent administration of UVA or visible light.
Photoaugmentation of UVB carcinogenesis by UVA was suggested by several investi-
gators (Urbach eta/., 1974; Willis eta/., 1981, 1986; Kligman, 1988 [abstract]; Thlve eta/., ----------
1990) but could not be confirmed by others (Forbes eta/., 1978; van Weelden & van der Leun,
1986). The latter investigators found evidence of photorecovery: the effect of UVB plus UVA
was smaller than that of the same UVB exposure given alone. The reduction was small;
however, UVA reduced the carcinogenic effective dose of UVB by 16%.
Interactions of different wavelength ranges when given simultaneously, prior to or
immediately after each other appear to be either nonexistent or unproven, as in the case of
photoaugmentation, or small, as in the case of photorecovery. Such interactions currently
play a small role in the evaluation of risks (see, for example, Health Council of the
STUDIES OF CANCER IN ANIMAlS 151
Netherlands, 1986). Other uncertainties in the estimates, such as the dose received, are likely
to have a greater influence than interactions. Photoreactivation, is, however, a well-defined
process in those species which possess photolyase and may result in reduction of effects.
3.6.2 Long-term interactions
A different type of interaction occurs when exposures to one wavelength band are
separated temporally from exposures to another. For example, a prolonged course of UVB
exposures, by itself sufficient to induce tumours, is compared with an identical UVB course
that is preceded or followed by a course of UVA exposures, usually over several weeks.
Forbes et al. (1978) exposed hairless mice to tumorigenic UVB or to UVB followed by
UVA and visible light for 30 weeks. The longer-wavelength exposures reduced the tumori-
genic effect of the UVB. Staberg et al. (1983b) gave mice a tumorigenic combination ofUVB
and UVA and found that subsequent exposures to UVA increased the tumorigenic effect.
The UVA was derived from Philips TL40W/09lamps filtered through 2-mm plain glass to
remove the UVB. (The Working Group noted that since the glass transmitted some UVB the
increased carcinogenic effect may have been due to added UVB radiation.] Bech-Thomsen
eta/. (1988a) pretreated lightly pigmented hairless female hr/hr C3H/Tif mice with UVA for
four weeks before exposure to broad-spectrum UVR. The UVA reduced the carcinogenic
effect of the broad-spectrum UVR. This result was not corroborated in a subsequent, similar
experiment by the same investigators (Bech-Thomsen et a/., 1988b), in which mice were
pretreated with radiation from various UVA sources. The purest UVA radiation neither
increased nor decreased the carcinogenic effect of UVB.
Slaper (1987) exposed one group of mice daily to UVB and a second group daily to UVA
at doses matched for approximately equal carcinogenic effect. In a third group of mice that
received the two regimens alternately every week, the carcinogenic effect was less than that in
the UVA- or the UVB-exposed group. The effective dose in the alternating regimen was
estimated to be 80% that in the UVB regimen. The investigator concluded that both UVA
and UVB contributed to the carcinogenic effect of the alternating regimen.
(The Working Group noted that the effect of long-term interactions appears to be
similar to that of interactions of exposures given on the same day. Photoaddition gives a
reasonable prediction, but the combined effects tend to be slightly less than would be
predicted.]
3.7 Additional experimental observations
3.7.1 Tumour types
Skin tumours in UV-exposed animals are commonly epidermal, benign papillomas and
malignant squamous-cell carcinomas; adnexal neoplasms, mainly basal-cell carcinomas, are
less common. Attempts have been made to induce naevi and malignant melanomas. Many
tumours are found, since the animals are followed for long periods of time; however, tumours
coalesce and regress, and all tumours are not examined histologically.
Squamous-cell carcinoma is the commonest type of tumour found after exposure to
UVR. These tumours have been reported in mice eXposed to predominantly UVB radiation
(Winkelmannet a/., 1960, 1963; Epstein & Epstein, 1963; Freeman, 1975; Forbes eta/., 1981;
152 IARC MONOGRAPHS VOLUME 55
de Gruijl et al., 1983), to predominantly UVA radiation (van Weelden et al., 1988; Sterenborg
& van der Leun, 1990) and to predominantly UVC radiation (Lill, 1983; Sterenborg et al.,
1988). They have also been found in rats (Putschar & Holtz, 1930; Roffo, 1934, 1939;
Hueper, 1942}, hamsters (Stenback, 1975a) and opossums (Ley et a/., 1989) following
exposure to broad-spectrum UVR.
Papillomas were reported to be the commonest tumour after exposure of hairless mice to
UVR consisting of UVB and UVA (Gallagher et ai., 1984b). Papillomas were also reported
to precede or accompany squamous-cell carcinomas induced in hairless mice by UVA (van
Weelden eta/., 1988), UVB (Stenback, 1978) or UVC radiation (Sterenborg eta/., 1988).
Papillomas were also common in rats (Findlay, 1930; Putschar & Holtz, 1930; Stenback,
1975a) and hamsters (Stenback, 1975a) exposed to broad-spectrum UVR.
The main type of tumour diagnosed after exposure of haired mice to broad-spectrum
UVR was fibrosarcomas (Grady eta/., 1941, 1943). Squamous-cell carcinomas were less
common, but the ratio of carcinomas to sarcomas increased with the number of exposures
per week (Grady eta/., 1943). Spikes eta/. (1977) reported many squamous-cell carcinomas
in clipped C3Hf mice irradiated with UVB, especially at low doses; the high-dose group had a
much higher proportion of fibrosarcomas. The investigators suggested that the type of
tumour induced might be dose-dependent. Norbury and Kripke (1978) found that the type of
tumour might depend on immunological factors. They compared UVB tumorigenesis in
normal C3H/HeN (MTV-) mice, in T cell-depleted mice and in T cell-depleted mice recons-
tituted with thymus grafts. In the normal mice, fibrosarcomas predominated; in the T-cell
depleted, reconstituted mice, squamous-cell carcinomas predominated. Spindle-cell
sarcomas were reported in rats irradiated with sunlight (Roffo, 1934), and fibrosarcomas
were seen in opossums irradiated with UVB (Ley eta/., 1989).
The diagnosis of fibrosarcoma was questioned by Morison eta/. (1986). After C3H/
HeNCr (mammary tumour virus-free) haired pigmented mice were exposed to mainlyUVB
radiation, the tumours induced were almost all squamous-cell carcinomas. The investigators
noted that the same type of tumour had been diagnosed in many previous reports as
fibrosarcoma; they diagnosed squamous-cell carcinomas by studying specific markers for cell
differentiation in the tumours. In a study by Phelps et al. (1989) in which hairless albino
Skh/hr-1 mice were exposed to UVA and UVB at 0.3 J/cm
2
[30 kJ/m
2
], all mice developed
epidermal neoplasia and 25% of animals developed spindle-cell tumours that resembled
human atypical fibroxanthoma. [The Working Group noted that earlier studies did not use
presently available cellular markers.]
Keratoacanthomas and similar benign epidermal neoplasms have been reported in mice
exposed to UVB (Stenback, 1978), rats exposed to UVB and UVC (Strickland et al., 1979)
and hamsters exposed to UVB (Stenback, 1975a).
Actinic keratosis, or solar keratosis, a precursor lesion of squamous-cell carcinomas, has
been reported in hairless mice exposed to UVA and UVB (Kligman & Kligman, 1981) and in
haired mice exposed to UVB (Stenback, 1978).
Basal-cell carcinomas have not been reported in studies in mice. A few studies on UV
carcinogenesis in nude mice, which have a deficient immune system, have been reported
(Eaton eta/., 1978; Anderson & Rice, 1987; Hoover et al., 1987). The skin tumours induced
STUDIES OF CANCER IN ANIMALS 153
by mainly UVB radiation in these studies were mostly squamous-cell carcinomas, but in the
experiments reported by Anderson and Rice (1987) in nude mice of BALB/c background
there were several basal-celJ carcinomas. Basal-cell carcinomas were found occasionally in
rats exposed to broad-spectrum UVR (Putschar & Holtz, 1930; Hueper, 1942). [The
Working Group noted that the classification of these neoplasms and their relation to the
corresponding neoplasms in humans is not clear.]
There is no report in which cutaneous malignant melanoma was induced in mice by UVR
alone (Epstein, 1990; van Weelden et al., 1990b; Husain et al. , 1991), in spite of concerted
attempts to achieve this.
No study was found in which the primary objective was to examine the susceptibility of
the eye to UVR; rather, eye tumours were found incidentally in studies designed to
investigate skin carcinogenesis. All of the tumours of the eye identified in these reports
involved superficial parts of the eye (cornea and conjunctiva); no tumour of the interior eye
was reported.
Studies of the effect of UVR on tumour induction in other organs (lymphoma in mice)
are few and were not designed to determine this effect (Ebbesen, 1981; Joshi eta!., 1986).
[The Working Group considered that the data were inadequate for evaluation and that data
on survival among treated and control groups, sample selection and analysis of data were
limited.]
3.7.2 Dose and effect
Quantitative information is available mainly on the induction of squamous-cell carci-
noma in mice. In most of the experiments, exposure was regular, several times per week or
every day, until tumours developed. The daily doses ofUVR required for skin tumorigenesis
are usually well below those present outdoors in the environment, and most experiments
have been conducted with UVB doses lower than those required to elicit acute reactions in
mouse skin (erythema or oedema). In one experiment in hairless mice, with a UVB dose 33
times lower than that required for acute reactions, 71% of the skin tumours were squamous-
cell carcinomas (de Gruijl et al., 1983). The effectiveness of UVB radiation is increased at
lower dose rates (Kelfkens eta!. , 1991b).
The higher the dose given, the less time it takes for tumours to appear. In most
experiments, the time required for 50% of mice to develop tumours ranged between a few
months and one year. By maximizing the exposure regimen in hairless mice (escalating doses
of UVB radiation), the time could be reduced to 18 days (Willis et al., 1981). In a few
experiments, in both mice and rats, skin tumours resulted from a single exposure to UVB
radiation (Hsu et a!. , 1975; Strickland et al., 1979); in mice, this required a dose that first
caused skin ulceration: hairless mice, 60 kJ/m
2
(Hsu et al., 1975); Sencar mice, 29 kJ/m
2
(Strickland, 1982).
Quantitative dose-effect relationships have been derived for mice exposed regularly
(usually daily) to UVR. The median time to first tumour, tm, has been used as a measure of
the effect and is related to dose level. Dose- effect relationships of the form
lm =CD-r,
where c is a constant incorporating the susceptibility of the strain of mice as well as the
effectiveness of the radiation spectrum, D is the daily dose of radiation and r is a numerical
154 IARC MONOGRAPHS VOLUME 55
exponent giving the steepness of the relationship, have been proposed by several authors.
Estimates of r vary from 0.2 (Sterenborg et al., 1988) for small tumours of the skin induced by
UVC radiation in hairless mice, to 0.5 (Blum eta/., 1959) for large tumours on the ears of
haired mice induced by broad-spectrum UVR and to 0.6 {de Gruijl et al., 1983) for small
tumours induced by broad-band UVB in hairless mice. Figure 11 (p. 145) illustrates the
shape of this dose-response relationship for r = 0.6; other forms of the relationship have
been proposed (Forbes et al., 1982). All of them provide adequate descriptions of the
dose- response within the range of the available data, although extrapolations outside this
range differ substantially.
3. 7.3 Dose delivery
The tumorigenic effect of UVR depends not only on the dose but also on the temporal
pattern of exposure. In general, the effectiveness of treatment increases with the number of
fractions of the dose per week (Forbes et al., 1981), for both daily and accumulated doses. A
daily dose administered over 12 h is more effective than the same daily dose. administered in
1 h (Kelfkens eta!., 1991 b). The same weekly dose is more effective when given over three to
five days than if given in one day (Forbes et al., 1981).
3. 7.4 Action spectra
Ideally, the carcinogenic effectiveness of UVR can be expressed as a continuous func-
tion of wavelength. That function, called the action spectrum for UV carcinogenesis, is not
yet completely delineated. Freeman (1978) made an early attempt to determine this
spectrum and found that it was limited to a few narrow bands around the wavelengths 290,
300, 310 and 320 nm. Narrow-band monochromatic sources are difficult to achieve.
Since that time, various action spectra have been proposed to weight the spectral irra-
diance of a source. Forbes et a/. (1982) and Cole et a/. (1986) determined dose-effect
relationships similar to that shown in Figure 11 for many different UV spectra. By weighting
these lamp spectra with various existing action spectra for photobiological effects, effective
doses were computed for each experiment. In this way, the investigators tried to align the
results from the experiments with different UV spectra into one dose-effect relationship.
One of the action spectra (MEE48), originally determined for the induction of oedema in
mice 48 h after exposure to UVR and which is similar to the human erythema action
spectrum, fitted well. The authors concluded that the mouse oedema spectrum was also
appropriate for describing skin cancer induction (Cole et al., 1986).
Sterenborg and van der Leun (1987) attempted to determine an action spectrum directly
from observations on UV carcinogenesis. They exposed hairless albino mice to seven
different lamp spectra under otherwise identical circumstances. The lamp spectra over-
lapped to some extent, and the action spectrum was derived by mathematical fitting. The
analysis yielded an action spectrum for the wavelength range 250-360 nm. Slaper (1987)
added observations in the UVA region and extended the action spectrum throughout the
UVA range (see Fig. 10, p. 141).
The action spectrum shown in Figure 10 is for albino hairless Skh-hr 1 mice with an
end-point of 1.0-mm tumours. Although different end-points may yield different action
spectra, this curve shows good agreement in the UVB range with the MEE48 spectrum and
STUDIES OF CANCER IN ANIMALS 155
also with the observations of Freeman (1978) for wavelengths 300, 310 and 320 nm. [The
Working Group noted that the action spectrum for UV carcinogenesis in the wavelength
range 300-320 nm may be considered a good approximation.] The different shapes of Figure
10 and MEE48 in the UVC reflect a scarcity of data in this wavelength range. [The Working
Group noted that the action spectrum for carcinogenesis by UVC is still highly uncertain.]
The MEE48 left widely different options open for the action spectrum of long-wavelength
UVA: the effectiveness in the wavelength range 330-400 nm could be either zero or as high
as 0.0002 (Cole et al., 1986). More recent data on the carcinogenesis of UVA, used to
construct the curve in Figure 10, indicate a mean effectiveness of 0.00015 in this range
(Slaper, 1987). (The Working Group noted that this value for the carcinogenic effectiveness
for UVA may be regarded as an estimate of the order of magnitude.]
3. 7.5 Pigmentation
Pigment was reported to be protective against tumours arising from the conjunctiva in
cattle (Anderson, 1963).
Freeman and Knox (1964) also examined the influence of pigmentation in a group of 78
rats composed of 66 pigmented rats of various strains (black, black and white, grey-brown,
grey and white) and 12 albinos. Under the same irradiation regimen, the pigmented rats
developed tumours in 73% of eyes and the albinos in only 8%. The tumour yield was
consistently higher in the pigmented strains than in the albinos. In nine pigmented and 10
albino hamsters exposed for one year, 50% of pigmented animals and 25% of non-
pigmented animals developed eye tumours.
Davies and Forbes (1988) exposed closely related albino hairless Skh-hr 1 mice and
pigmented hairless Skh-hr 2 mice to broadband UVR from a filtered xenon arc lamp.
Especially at high doses, the latent period until 50% of animals had first tumours was longer
in Skh-hr 2 mice.
van Weelden et al. (1990a) derived mice of different degrees of pigmentation-'browns'
and 'blacks' -by selective breeding from Skh-hr 2 stock and exposed 24 albinos (Skh-hr 1)
(van Weelden et al., 1988), 16 ' browns' and eight 'blacks' to UVA radiation. The brown mice
were less susceptible to skin tumours than the albinos, but the more heavily pigmented blacks
were as susceptible as the albinos: the median times for tumour induction were 265 days for
albinos, 267 days for blacks and 375 days for browns (van Weelden eta/., 1990a).
3.8 Administration with known chemical carcinogens
Since UVR alone produces tumours, it is a 'complete' carcinogen and may thus be
involved in cocarcinogenicity. Several investigators have attempted to determine whether
UVR has tumour 'initiating' and/or tumour 'promoting' activity when tested in a traditional
two-stage protocol. For the purposes of this monograph, a 'tumour initiator' is defined as an
agent that, at a stated amount and upon administration once, is incapable of causing tumours
in the population of animals unless the skin is subsequently treated with a 'tumour promoter'.
A 'tumour promoter' is defined as an agent that, under stated conditions is incapable of
causing tumours unless the skin was previously treated with a 'tumour initiator'. The test
systems used embody a number of variables, not all of which were necessarily considered by
156 IARC MONOGRAPHS VOLUME 55
the authors. For example, UVR has also been shown to influence the immune system, and
polycyclic aromatic hydrocarbons are photochemically active.
3.8.1 Administration with polycyclic aromatic hydrocarbons
Most of the studies summarized below demonstrate that UVR has a cocarcinogenic
action with other carcinogens. Other reports provide additional information on cocarcino-
genesis, on photolysis of polycyclic aromatic hydrocarbons and on other interference with
chemical carcinogenesis (Clark, 1964; Ito, 1966; Santamaria eta/., 1966; Davies eta/., 1972
[abstract]; Shabad & Litvinova, 1972; Stenback & Shubik, 1973; Stenback, 1975b; Roberts &
Daynes, 1980; Gensler & Welch, 1992).
(a) 3,4-Benzo[ajpyrene
Groups of 18 female SPF (specific pathogen-free} BALB/c mice, six weeks of age,
received 30-min exposures on the shaved dorsal skin to UVB from a Westinghouse FS40
sunlamp (280-320 nm)five times a week for 13 weeks (total dose, 7.0 x 10
5
J/m
2
) or no UVB
exposure followed one week later by twice weekly applications of 0, 0.1 or 1.0 mg 3,4-benzo-
[a ]pyrene in acetone on the shaved ventral skin for 20 (acetone only), 20 or 10 weeks,
respectively. Pre-exposure to UVB enhanced tumour growth in the high-dose group: 29
tumours (of 20 examined histologically, 90% were squamous-cell carcinomas and 10%
undifferentiated sarcomas) in the UVB-pretreated group compared to two (squamous-cell
carcinomas) in the non-irradiated 3,4-benzo[a]pyrene-treated animals 18 weeks after the
first treatment with 3,4-benzo[a ]pyrene. No such effect was seen in the low-dose group
(Gensler & Bowden, 1987; Gensler, 1988a).
(b) 7,12-Dimethylbenz[a]anthracene
In an attempt to assess the promoting effects of UVR, groups of 15-31 male and 16-22
female Swiss albino mice, 11-18 weeks of age, received a single application of two drops(O.l
ml) of 0 or 0.5% 7,12-dimethylbenz[a]anthracene (DMBA) in acetone on the posterior half
of the dorsal skin, followed 14 days later by exposures to UVB (280- 320 nm; high-pressure
Hanovia hot quartz contact lamp) twice a week for 67 weeks (total dose, 13.33 x 10
7
ergs/cm
2
[133 kJ/m
2
]) or no exposure. At the end of the UVB treatment, 16/31 mice treated
with DMBA and UVB had developed 19 skin tumours, compared to 4/41 and 0/47,
respectively, among mice treated with DMBA alone and UVB alone. Exposure to UVB also
enhanced the multiplicity and degree of malignancy of DMBA-induced tumours {Epstein &
Epstein, 1962 ).
Groups of 26-42 male and female outbred hairless mice, 7- 12 weeks old, received a
single application of two drops (0.1 ml) of 0 or 0.5% DMBA in acetone, followed six weeks
later by exposures to UVB (280-320 nm; high-pressure Hanovia hot quartz contact lamp)
three times a week for 29 weeks (total dose, 15.34 x 10
7
ergs/cm2 [153 kJ/m
2
]) or no
exposure. All animals were observed for 63 weeks. UVB exposure produced skin tumours in
22/26 animals, and DMBA treatment alone in 3/41; acetone alone produce no skin tumour.
Exposure to UVB following DMBA treatment enhanced carcinogenicity with regard to
appearance time (first tumour observed at 14 weeks compared to 30 in the group treated with
DMBA alone and 20 in that given UVB alone), multiplicity at 58 weeks after DMBA
STIJDIES OF CANCER IN ANIMALS 157
treatment ( 40 in 24 animals compared to 22 in 26 animals treated with UVB alone and 3 in 41
animals treated with DMBAalone) and degree of malignancy. Tho 'melanomas' appeared in
the group receiving the combined treatment (Epstein, 1965).
Groups of 18-46 outbred hairless pigmented mice [sex unspecified], 8- 11 weeks old,
received a single application of 0.05 ml of 0.4% DMBA (0.2 mg) in acetone or no DMBA
After 13 months, mice treated with DMBA had developed pigmented lesions ('blue naevi') in
the treated areas. For the following seven months, mice received UVB (280-320 nm;
high-pressure Hanovia hot quartz contact lamp) three times a week or no UVB treatment.
Exposure to UVB following DMBA treatment enhanced the growth of naevi into
appearing pigmented tumours ('melanomas'): 5/18 versus 0/41 in the group treated with
DMBA alone and 0/39 in the group treated with UVB alone (Epstein et al., 1967). [The
Working Group noted the limited reporting on metastases.]
A group of 56 B6D2F
1
/J mice [sex unspecified], six weeks of age, was irradiated with
UVB (280-340 nm; Westinghouse FS40 sunlamp) dorsally for 30 min per day on five days per
week (Roberts & Daynes, 1980) for 11.5 weeks (total dose, 6.2 x 10
5
J/ml). A control group
of 41 mice received no irradiation. Both groups subsequently received a single application of
100 J.Lg DMBA in 0.1 ml acetone on the shaved ventral skin, followed four days later by
applications of 5 J.Lg 12-0-tetradecanoylphorbol 13-acetate (TPA) three times a week for 32
weeks. Tumour yield was significantly decreased at 32 weeks (2.2 versus 4.8 tumours/mouse)
in the pre-irradiated mice (Gensler, 1988b).
Groups of 20-24 female hairless Skh-hr 2 mice, six to eight weeks old, received a single
application of 0 or 0.5% DMBA in acetone on the dorsal skin. Two weeks later, the animals
were irradiated with UVB (290-320 nm; Westinghouse FS40-T12 sunlamp), UVA(320-400
nm; fluorescent black light tubes) or a combination of UVA plus UVB three
times a week for 30 weeks or were not irradiated, and were observed for 12 months. All mice
receiving DMBA treatment developed multiple 'blue naevi'; virtually none of the untreated
mice or mice that received UVR treatment only showed this effect. Irradiation of
DMBA-treated animals induced a higher incidence of papillomas (70-100% ),
carcinomas (30-80%), melanomas (25-33%) and lymphomas (21-50%), than exposure to
UVA alone (0-32% papillomas, 0-47% squamous-cell carcinomas, no melanoma and no
lymphoma) or to DMBA alone (90, 25, 0 and 5% of these tumours, respectively). The authors
also examined selected lesions induced by DMBA alone or by DMBA with UVR for the
presence of H- or N-ras mutations. Mutations at codon 61 in N-ras were present in three (two
induced by DMBA plus UVR, one by DMBA alone) out of eight of the early pigmented
lesions examined and in one out of three of the malignant melanomas examined (induced by
DMBA plus UVR); no H-ras mutation was observed (Husain et a!., 1991). [The Working
Group noted that lesions were not induced by UVR alone.]
3.8.2 Administration with other agents with promoting activity
These studies were designed to evaluate the action of UVR as a tumour initiator.
(a) Croton oil
Groups of 15- 53 male and 9- 30 female random-bred hairless mice, 9-12 weeks old.
received a single exposure to UVB (280-320 nm; high-pressure Hanovia hot quartz contact
158 IARC MONOGRAPHS VOLUME 55
lamp) for 30 s (1.3 x 10
7
ergs/cm3 (13 kJ/m
2
]) or no exposure, followed two weeks later by
applications to the dorsal skin ofO or 0.1 ml croton oil in acetone twice a week for 18 months.
Neither UVB exposure nor croton oil alone produced any skin tumour over the course of the
study. The group of 79 mice that received both UVB exposure and croton oil had eight
persistent skin tumours (one per mouse) (Epstein & Roth, 1968).
Groups of 30 female Swiss mice, eight weeks old, received UVB once (5.5 x 10
7
ergs/cm
2
[55 kJ/m
2
]) from Westinghouse FS40T12 lamps or croton oil (0.02 ml of a 2.5%
solution, twice a week for 30 weeks); a group of 60 mice received UVB followed after 10 days
by croton oil for life. UVB alone produced no tumour; croton oil alone produced regressing
tumours, and the combination produced 11 tumours (four papillomas, four fibromas and
three regressing tumours) in seven mice (Stenback, 1975c).
Groups of 40 male haired mice (random-bred 'Hall' strain), 18 weeks of age, were
clipped and exposed once to UVC (medium-pressure mercury discharge lamp). One group
received no further treatment; the other received one application of croton oil one day
before irradiation and, beginning two weeks later, received applications of 0.25 ml croton oil
(0.5% solution) once a week for 30 weeks. By 35 weeks, the groups had 20 and 23 survivors,
with 0 and 12 skin tumours, respectively (Pound, 1970).
(b) 12-0-Tetradecanoylphorbo/13-acetate
Six groups of 25 eight-week-old female C3H/HeNCr(MTV-) mice were irradiated with
UVB (Westinghouse FS40 sunlamps) on the shaved dorsum for 30 min, five times a week for
two weeks (total dose, 1.44 x 10
5
J/m
2
) , followed two weeks later by ' promotion' with appli-
cations ofO or 5J..lgTPA in acetone twice a week. Ventral irradiation for30 min, three times a
week for 12 weeks (total dose, 4.54 x 10
5
J/m
2
) (to produce a 'systemic' effect) was begun two
weeks after completion of dorsal initiation. At 70 weeks, UVB exposure of the dorsum alone
had produced no tumour, and dorsal applications ofTPA alone had produced a 5% incidence
of tumours. The combination of these treatments produced a 41% tumour incidence. Ventral
irradiation of animals that had received TPA only produced a 33% incidence, and ventral
irradiation of mice that had received both UVB and TPA produced a 100% incidence. The
authors suggested that these findings reflect a systemic effect-possibly suppression of
immune surveillance or a biochemical influence on the epidermal growth regulatory system
(Strickland et al., 1985).
(c) Benzoyl peroxide
Benzoyl peroxide is considered to be a prototype promoter of two-stage chemical
carcinogenesis in the skin (Siaga et al., 1981 ). The studies summarized below were motivated,
however, by concerns about the safety of using this compound for treating acne vulgaris.
Groups of Used (Hr) stock hairless albino mice (total, 148) [sex unspecified], three to
four months old, were exposed on the posterior half of the back to UVR (Hanovia hot quartz
contact lamp emitting primarily UVB; 270 mJ/cm
2
[2.7 kJ/m
2
]) three times a week for eight
weeks. Four weeks later, the mice were divided into four groups. The final skin tumour
incidences at the irradiated sites were: 38% in the group that received applications ofO.l ml
of a 0.1% solution of croton oil in acetone on the back skin five times a week for the duration
of the experiment (62 weeks); 5% in the group that received applications of acetone alone;
STUDIES OF CANCER IN ANJMAI.S 159
8% in mice that received applications of the benzoyl peroxide base; and 8% in those that
received applications of a 5% lotion of benzoyl peroxide in water five times a week for the
duration of the study (Epstein, 1988).
Five groups of Oslo hairless mice (16 males and 16 females) were irradiated under
PhiJips HP3114 sunlamps (mostly UVB) twice a week for 52 weeks (total dose, 26.5 J/cm
2
(265 kJ/m
2
]). The mice were treated before or after each exposure with 5% benzoyl peroxide
in gel, with the gel alone or with no chemical. Throughout the study, the groups were
indistinguishable in terms of the proportion with one of more tumours (median latent period,
approximately 40 weeks) and of the total number of tumours per survivor (approximately 1.5
at 40 weeks and approximately 4 at 48 weeks). Thus, benzoyl peroxide did not enhance
photocarcinogenesis. The study also included several groups of SENCAR mice treated
topically with DMBA once (51.2 11g) or with vehicle followed by benwyl peroxide twice a
week. Benzoyl peroxide reduced the number of DMBA-induced tumours (Iversen, 1988).
Two unresolved concerns were raised by the author: Firstly, the fact that benzoyl peroxide
reduced the tumorigenicity of DMBA was contrary to the author's previous experience
(Iversen, 1986) and to that of several others; secondly, the UVR dose used in this study was
lower (total dose, 265 kJ/m
2
) than that used in the 1986 study (total dose, 480 kJ/m
2
), but the
tumour response was significantly greater.
(d) Methyl ethyl ketone peroxide
A postulated mechanism for tumour promotion involves the generation of free radicals,
possibly with reactive oxygen species, leading to enhanced lipid peroxidation and DNA
damage and/or cell phenotype. A study was therefore designed to test whether methyl ethyl
ketone peroxide (MEKP), which is known to produce lipid-peroxidizing activity in vivo, acts
as a tumour promotor in skin 'initiated' by UVR. Furthermore, since glutathione has been
shown to be a major endogenous reducing agent which protects against lipid peroxidation,
the study also tested diethyl maleate (OEM), which is known to deplete the intracellular level
of glutathione in mouse skin.
Groups of 24 male and female hairless albino mice (14-16 weeks old) were irradiated
with UVB (280-320 nm; Westinghouse FS40 fluorescent sunlamps; 2054 J/m
2
daily) for 18
weeks. Three weeks later, topical application of MEKP (20 111 containing 0 or 10 11-g MEKP)
was begun and continued twice a week for 25 weeks. Other groups received DEM (0 or 1 J.tg
in dibutyl phthalate) 1 h before each MEKP application. Otherwise identical control groups
received either the chemical treatments or UVB alone. At 46 weeks, the groups that did not
receive UVB irradiation had at most two tumours on two mice (among 21 survivors in mice
exposed to MEKP plus DEM). Exposure to UVB produced five tumours in four mice
exposed to the solvent, out of 19 survivors; 11 tumours in eight mice exposed to MEKP, out of
21 survivors; and 18 tumours in nine mice exposed to MEKP plus DEM, out of 16 survivors.
Using tumour onset rate analysis (Peto et a/., 1980), the overall effect of MEKP was
statistically significant. Tumour enhancement by MEKP was greater in the presence ofDEM
(Logani et a/., 1984).
160 IARC MONOGRAPHS VOLUME 55
3.9 Interaction with immunosuppressive agents
Investigations have been reported on agents known to influence immunological
responses in humans and on agents chosen to test some aspect of immunological response in
mice. [The Working Group noted that in most cases the effect on the immune system of the
animals was not evaluated directly; these agents have effects other than immunosuppression.
which may explain their interaction with photocarcinogenesis.]
Three groups of 12 male Skh-Hr1 hairless mice. eight weeks of age, were irradiated with
280-320 nm UVB (Westinghouse FS40T12 sunlamps} on five days per week for 30 weeks at
daily doses of 470 J/m
2
. Two weeks after the first UVB exposure. one group received
subcutaneous injections of 0.1 ml anti-mouse lymphocytic serum twice a week for 20 weeks; a
second received intraperitoneal injections of 12 mg/kg bw6-mercaptopurine (Purinethol) five
times a week for 20 weeks; and a third received intraperitoneal injections of 0.1 ml isotonic
saline five times a week for 20 weeks. Treatment with anti-mouse lymphocytic serum resulted
in an earlier appearance and a greater numbers of tumours than did treatment with saline; in
contrast. 6-mercaptopurine appeared to delay the appearance of tumours (Nathanson et al .
1976).
Groups of 24-28 female albino HRA/Skh-1 hairless mice. 21-35 weeks of age. were
irradiated with UVR (UVB from an Oliphant FlAOSE tube and UVA from six Sylvania 40BL
tubes) to simulate the UVR portion of terrestrial sunlight on five days per week for 10 weeks
to achieve a MED. At the same time. the animals received intraperitoneal injections of 15
mg/kg bwazathioprine in 0.1 ml glycine buffer, 10.6 mg/kg bw cyclophosphamide in 0.1 ml '
glycine buffer or 0.1 ml vehicle alone. At day 200, mice receiving UV irradiation alone had a
tumour incidence of 77%; those also receiving azathioprine had an incidence of 96%
{marginally significant enhancement of tumour growth); and those receiving cyclo-
phosphamide had an incidence of 85% (nonsignificant increase) (Reeve eta/., 1985).
Groups of 15 female albino HRS/J hairless hr/hr mice, eight weeks old, were irradiated
with UVB (280- 320 nm; Westinghouse FS40 sunlamps) on five days a week for 24 weeks;
further groups also received injections of 4 or 8 mg/kg bwazathioprine or 10 or 25 mg/kg bw
cyclosporine three times a week. The mean latent period for tumour development was 16
weeks in the group receiving UV irradiation only and 12-13 weeks in the groups also
receiving azathioprine or cyclosporine, indicating enhancement of photocarcinogenesis by
both drugs (Nelson eta/., 1987).
Groups of female C3H/HeN(MTV-) mice [initial numbers unspecified), four to six
weeks of age, received grafts of fragments of an antigenic ('regressor') tumour (fibro-
sarcoma) previously induce-d in a host animal by UVB. Some animals received no further
treatment; other groups received UVB irradiation (Westinghouse FS40; 5 kJ/m
2
per day on
five days a week for four to six weeks), subcutaneous injections of 25 or 75 mglkg bw cyc/o-
sporine once a day on eight consecutive days, or injections of 20 mg/kg bw cyclophosphamide
1, 3, 6, 9 and 13 days after tumour challenge. Thmours grew progressively in the groups
treated with UVB or cyclosporine, but not in the groups receiving no further treatment or
cyclophosphamide (Servilla eta/., 1987).
Groups of six female albino HRNSkh-1 hairless mice, 10- 12 weeks of age, were irra-
diated with UV A plus UVB (one Oliphant FlAOSE tube and three Sylvania F4/350 BL tubes)
STUDIES OF CANCER IN ANIMALS 161
on five days a week until death (about 35 weeks). During that time, they were also injected
intraperitoneally with 15 mg/kg bw azathioprine, 20 mg/kg bw prednisolone or 15 mg/kg bw
cyclophosphamide in 0.1 ml saline or given 60 mg/kg bw cyclosporine in 0.1 ml peanut oil by
gavage or 0.1 ml vehicle alone. Azathioprine, cyclophosphamide and cyclosporine all signifi-
cantly enhanced photocarcinogenesis with regard to median latent periods and tumour
multiplicity. Prednisolone did not enhance this effect, nor did it interfere with the
enhancement by other drugs when given in combination with them (Kelly eta!., 1987).
Groups of 15- 32 female albino Skh-hr 1 hairless mice, 10-12 weeks of age, were irra-
diated with UVA plus UVB (250-700 nm; one Oliphant FIAOSE tube, three Sylvania
F40/350 BL tubes and two True-Lite [Duro-Test Corp) tubes) on five days per week for 12
weeks. Two weeks after the first irradiation, mice received intraperitoneal injections on five
days a week of 15 mg/kg bwazathioprine or 6-mercaptopurine in 0.1 ml saline orO.l ml vehicle
alone. Both compounds significantly enhanced skin photocarcinogenesis with regard to
median latent period, proportion of malignant:benign growths and tumour multiplicity
(Kelly eta/., 1989).
3.10 Molecular genetics of animal skin tumours induced by ultraviolet radiation
Three skin papillomas and three skin carcinomas produced in female SENCAR mice
after a single exposure to UVB (280-315 nm; Westinghouse FS20; 70 kJ/m
2
) were examined
for ras gene alterations. A five- to 10-fold increase in cHa-ras RNA gene expression asso-
ciated with the gene amplification was found in papillomas and carcinomas, while DNA from
carcinomas, but not from papillomas, induced foci in the NIH-31'3 cell transfection assay
(Husain eta!., 1990).
4. Other Relevant Data
4.1 Transmission and absorption in biological tissues
UVR may be transmitted, reflected, scattered or absorbed by chromophores in any layer
of tissue, such as the skin and eye. Absorption is strongly related to wavelength, as it depends
on the properties of the responsible chromophore(s). Accordingly, transmission is also
wavelength-dependent. Transmission and other optical properties are affected by changes in
the structure of the tissue and, especially in the case of the lens of the eye, by ageing.
Absorption of radiation by a tissue chromophore is a prerequisite for any photochemical
or photobiological effect; however, absorption does not necessarily have a biological con-
sequence.
4.1.1 Epidermis
Since UVR-induced skin cancer is an epidermal phenomenon, this section focuses on
epidermis and excludes the dermis.
The epidermis, a tissue with a high replication rate, can be divided functionally into two:
an inner, living part (60-160-)lm thick in humans) of cells at various stages of differentiation
and the outermost, non-living, terminally differentiated stratum corneum (8- 15-)lm thick in
humans). The dividing cell population is located in the innermost basal layer of the living
epidermis. Optical properties have usually been studied using isolated strateum corneum or
whole epidermis. Absorption and scattering of UVR by the stratum corneum afford some
protection to the living part of the epidermis from UVR exposure.
Human and mouse epidermis have important structural differences. The living part and
the stratum corneum of human epidermis have about 10 cell layers each. In mice, the living
part has two to three cell layers and the stratum cornea one to two cell layers. The interphase
of human epidermis and dermis is highly undulated (i.e., epidermal thickness varies),
whereas in the mouse it is flat.
Skin contains sebaceous glands which secrete lipid-containing sebum, which forms a
film on the stratum corneum.
(a) Humans
The optical properties of human skin have been reviewed (Anderson & Parrish, 1981,
1982).
Everett eta/. (1966) used a variety of methods to obtain whole epidermal and stratum
corneum preparations of human skin. Transmission characteristics (from 240 to 700 nm)
were measured using a recording spectrophotometer via an integrating sphere which permits
the measurement of forward scattered radiation. lfansmission values of whole epidermis in
-163-
164 IARC MONOGRAPHS VOLUME 55
white skin ranged from 1% at 250 nm to 44% at 320 nm, while transmission at 400 nm was
about 50%.
Kaidbey et al. (1979) compared the optical properties (250-400 nm) of whole epidermis
and stratum corneum from black and white skins. In general. the absorption spectra from the
stratum corneum were similar in shape and magnitude; however, the absorption spectra for
whole epidermis were clearly different: At about 300 nm, the absorbance (accounting for
scattering) of black epidermis was twice that of white epidermis.
Anderson and Parrish (1981, 1982) presented data which show that epidermal trans-
mission between 260 and 290 nm will be overestimated if no correction is made for tissue
fluorescence (330- 360 nm). This is most evident at about 280 nm and is consistent with
tryptophan or tyrosine fluorescence.
Bruls et a/. (1984a) measured transmission in whole human epidermis and stratum
corneum of UVR between 248 and 546 nm, using a solar blind detector which corrects for
fluorescence, and found results different from those of Everett, in particular, that UVC
transmission was one to two magnitudes lower. The transmission spectra of whole epidermis
and stratum corneum showed a similar general shape but with differences in minima and
magnitude. The minimum for epidermis was 265 nm and that for stratum corneum was 275
nm, presumably reflecting different chromophores in those tissues. At 254 nm, transmission
in stratum corneum was about two orders of magnitude greater than that in whole epidermis.
At about 300 nm, this difference was only one order of magnitude. The transmission in
stratum corneum from previously sun-exposed skin was about one order of magnitude less
than that in unexposed epidermis at 254 nm. The difference was less at wavelengths > 290
nm. The minimal transmission in stratum corneum from previously sun-exposed skin was
shifted from 275 to 265 nm. The authors also showed that the relationship between tissue
thickness and transmission of UVR and visible light (log scale) is linear.
Bruls eta/. (1984b) studied the relationship between the MED ofUVB (filtered mercury
arc) and UVC (germicidal lamp) and epidermal transmission. A clear linear (log-log)
relationship was demonstrated; the MED increased with decreased transmission. Repeated
exposure to UVB resulted in higher MEDs of UVB and UVC and decreased transmission of
UVB (only epidermis measured) and UVC (epidermis and stratum corneum measured).
Beadle and Burton (1981) extracted skin lipids from human scalps and measured their
transmission spectra in hexane. They estimated that lipid concentrations normally present on
the skin surface of the forehead would reduce transmission at 300 nm by about 10%.
(b) Experimental systems
No data are available on transmission in the stratum corneum of mice. Sterenborg and
van der Leun (1988) measured transmission of 246- 365 nm in Skh-hr 1 mouse epidermis
in vitro. Minimal transmission (about 2%) was observed at 254 nm and 270 nm; 10% was
transmitted at 290 nm, 50% at 313 nm and 70% at 365 nm. Agin et al. (1981a) studied
changes in optical properties of the epidermis of six to eight Skh-1 albino and Skh-2
pigmented (ears and tails) hairless mice irradiated dorsally with a single, 125-h exposure to a
UVA source (GE F8T5-BL) with and without a 3-mm glass filter. When unfiltered, 1.4% of
the radiation was < 320 nm and when filtered, 0.12% was < 320 nm. The mid-back (whole
epidermis) was examined by forward scattering absorption spectroscopy (250-400 nm) at
OTHER RELEVANT DATA 165
48 h, 96 h, nine days and 23 days. With the filtered source, there was an increase in
absorbance across the spectrum at 48 h, and the absorption spectrum was similar to that of
control skin. Transmission returned to the control baseline by 23 days. With the unfiltered
source, there was a smaller increase towards baseline absorbance at 48 h. With time, there
was a general decrease in absorbance, except at 250-280 nm at which there was an increase at
nine and 23 days. At 23 days, the spectrum had not returned to baseline level, despite a
normal histological appearance.
de Gruijl and van der Leun (1982a) studied the effect of repeated exposure to UVR on
epidermal transmission in Skh-hr 1 hairless albino mice. Groups of 11-40 mice were exposed
to daily doses of UVR ranging from 0.11 to 1.9 kJ/m
2
from Westinghouse FS-40 sunlamps.
Transmission measurements corrected for fluorescence of the epidermis were made at 313,
302 and 297 nm. After six weeks' exposure, the higher daily doses resulted in decreased
transmission at all wavelengths. The optical density (the negative logarithm of transmission)
ratios for the three wavelengths were fairly constant with each dose. There was a simple
linear relationship between duration of treatment, increased optical density at 297 nm and
epidermal thickness, measured microscopically from frozen sections, which indicates that
increased optical density is a result of UVR-induced epidermal hyperplasia. These data show
that UVR-induced changes in epidermal transmission may modify the UVR dose-response
relationship for skin cancer.
(c) Epidermal chromophores
The influence of chromophores on the optical properties of the epidermis has been
reviewed by Anderson and Parrish (1981). The main chromophores are urocanic acid (A.max
277 nm at pH 4.5), DNA (A.max 260 nm at pH 4.5), the aromatic amino acids tryptophan (A.max
280 nm at pH 7) and tyrosine (A.max 275 nm at pH 7), and melanins (Morrison, 1985).
Urocanic acid is the deamination product of histidine and is present in human and
guinea-pig epidermis (mainly stratum corneum) at about 35 f.J.g/cm
2
dry weight. It exists in
two isomers, trans (E) and cis (Z); the trans-isomer is converted to the cis-isomer upon UV
irradiation. The absorption spectra of the two isomers are virtually superimposable, but the
extinction coefficient of the cis isomer at A.max is 20% lower (Morrison, 1985). Norval eta/.
(1988) quantified urocanic acid isomers in mouse (C3HfBu/Kam) skin during development
and after exposure to UVB radiation. Fetal dorsal mouse skin had a low total urocanic acid
content, which increased in neonatal and older animals. Exposure to UVR increased the
proportion of the cis-isomer within 16 h from 4.7% in nonirradiated mice to 31%, and this
was maintained for days (16% after seven days). The photostationary state for in-vivo
isomerization in guinea-pig skin is 45% cis-155% trans-isomer (Baden & Pathak, 1967).
DNA is not present to any extent in the stratum corneum of guinea-pigs (Suzuki et al.,
1977). Bruls eta/. (1984a) attributed the differences in transmission minima between whole
epidermis (265 nm) and stratum corneum (275 nm) in humans to the lack of DNA
Absorption by protein occurs throughout the epidermis.
Melanins are stable protein polymers packaged in melanosomes, produced by mela-
nocytes and transferred to keratinocytes. Melanins absorb broadly over the UV and visible
spectrum although they are not neutral density filters of the skin. For example,
3,4-dihydroxyphenylalanine (dopa)-melanin shows a steady decline in optical density
166 IARC MONOGRAPHS VOLUME 55
between 210 and 340 nm (Anderson & Parrish, 1981). There is no significant racial difference
in the number of melanocytes/unit area of a given body site (Szabo et a/., 1972), so that
differences in the transmission properties of black and white skin are believed to be due to
differences in melanin content and in the packaging and distribution of melanosomes in the
epidermis (Kaidbey et a/., 1979).
(d) Enhancement of epidermal penetration of ultraviolet radiation
Prolonged exposure of skin to water increases sensitivity to UVB. This effect is thought
to be due to the removal of UVR-absorbing compounds, especially urocanic acid, from the
stratum corneum (Anderson & Parrish, 1981).
Spectral remittance at 300-400 nm has been measured in normal and psoriatic white
skin after the application of mineral oil. No effect was observed in normal skin, but
remittance in psoriatic skin was reduced within seconds after application of oil, implying
greater transmission (Anderson & Parrish, 1982}. A similar enhancement of transmission
was proposed to explain the observation that topically applied arachis oil enhances tumori-
genesis by solar-simulated radiation in hairless albino mouse skin (Gibbs eta/., 1985).
4.1.2 Eye
(a) Humans
Boettner and Wolter (1962) measured transmission of direct and forward scattering
UVR (220-400 nm) in the cornea, aqueous humour, lens and vitreous humour from nine
freshly enucleated normal eyes. There was no corneal transmission of < 300 nm, beyond
which the transmission spectrum showed a very steep increase to about 80% transmission at
380 nm (the curve was almost vertical between 300 and 320 nm). Aqueous humour
transmitted > 220 nm, with a steep rise to 90% transmission at 400 nm and no evidence of
scattering. In a young (4.5-year-old) lens, transmission started at 300 nm with a peak at 320
nm, declining sharply to no measurable transmission between 370 and 390 nm; thereafter, it
showed a steep increase. A similar but slower pattern was reported for two older lenses (53
and 75 years old), with greater light scattering. Transmission in the vitreous humour began at
300 nm with a steep increase to 80% transmission at 350 nm. Lerman (1988) showed that
transmission of UV at 300-400 nm in normal human lenses decreases with age between three
days and 82 years. A review by Sliney (1986) stated that 1% of incident radiant energy in the
300-315 nm range reaches the human retina early in life.
(b) Experimental systems
Kinsey (1948) measured transmission of direct UVR [no mention of instrumentation to
detect scattering] in the corneal epithelium, whole cornea, aqueous humour, lens and
vitreous humour of young adult albino rabbits. The cornea, aqueous and vitreous humor
absorbed virtually all radiation at < 300 nm; the lens absorbed > 90% radiation at wave-
lengths < 370 nm.
Bachem (1956) measured absorption of UVR at 293-435 nm by the lens and cornea
from rabbit eyes. Few technical details were given, but the author indicated that scattering
was taken into account. The cornea absorbed all radiation at 293 nm, and the lens absorbed
OTHER RELEVANT DATA 167
all radiation < 334 nm. Calculation of absorption by the lens in situ gave a maximum at
365 nm, with little or no absorption at > 400 and < 300 nm.
Ringvold (1980) studied the absorption of UVR at 200-330 nm by cornea from young
adult albino rabbits, rats, guinea-pigs and domestic cats. In contrast to the results of other
studies, the cornea did not completely absorb wavelengths < 300 nm; depending on the
species, absorption at 300 nm ranged from about 30 to 80%. [The Working Group noted that
this discrepancy cannot be explained by scattering, as presumed failure to take its effect into
account would overestimate absorption.]
4.2 Adverse effects (other than cancer)
This section deals generally with adverse effects of UVR; however, beneficial effects
also occur in humans. The vitamin 0
3
precursor, previtamin 0
3
, is formed in the epidermis
and dermis through the photochemical action of UVB (Holick eta/., 1980). The total daily
requirement of vitamin 0
3
(cholecalciferol) is supplied in most people by the combination of
synthesis in the skin and contribution from dietary sources of animal origin. Older people are
at particular risk for developing vitamin D
3
deficiency, partly because the capacity for its
formation decreases with age (MacLaughlin & Holick, 1985). The sunscreen para-amino-
benzoic acid efficiently blocks the photosynthesis of previtamin D
3
in the skin (Matsuoka et .
a/., 1987). It has been estimated that exposure of the cheeks for 10-15 min in the midday sun
in Boston, USA, would be sufficient to provide the daily requirement of vitamin D.
4.2.1 Epidermis
(a) Humans
The most prominent acute effects of UVR on human skin are erythema ('sunburn') and
pigmentation, with cellular and histological changes.
(i) Erythema and pigmentation (sunburn and suntanning)
Dose-response curves for erythema were constructed for four radiation wavelengths,
254,280, 300 and 313 nm, by Farrand Diffey (1985); the erythemal response on the back was
assessed quantitatively by a reflectance instrument. At 254 nm, erythema was maximal
approximately 12 h after irradiation at doses up to about five times the MED. At higher
doses, erythema was more persistent, with little change in intensity from about 12 h to at least
48 h after irradiation.
At 313 nm, with doses around the MED, the maximal response was seen 7 h after irra-
diation; with doses of two to three times the MED, the maximal response occurred at about
4 h. The MED at 254 and 280 nm was substantially lower than that at 300 and 313 nm;
however, the slopes of the dose-response curves for erythema with 254 nm and 280 nm
radiation were much flatter than those at 300 nm and 313 nm (Farr & Diffey, 1985).
The time-course of UVA erythema following irradiation with a high-intensity UVA
source (predominantly 360-400 nm) was found to be biphasic. Erythema, which may be due
to heat, was present immediately. It was minimal at about 4 h then increased between 6 and
24 h. The intensity of the early phase was dose-rate dependent, whereas the intensity in the
latter phase depended on dose only. The slope of the log dose-erythema response to UVA at
24 h did not differ from that to UVB (Diffey et a/., 1987).
I
I
I
I
I
I
I
I
I
168 IARC MONOGRAPHS VOLUME 55
A number of variables affect the observation of erythema, including anatomical site,
time of observation after irradiation, size of irradiated area, method of recording erythema
and season (Diffey, 1982).
The pharmacological changes that may be responsible for erythema have been studied.
Plummer et al. (1977) examined suction blisters raised on UVB-inflamed human abdominal
skin. Bioassayable prostaglandin activity was elevated 6 and 24 h after irradiation, and levels
of prostaglandin F
2
~ measured by radioimmunoassay, were elevated at 24 h; levels had
returned to normal at 48 h, but erythema persisted. Greaves et al. (1978) extended these
observations. Following UVC irradiation, arachidonic acid and prostaglandin Ez and F2
levels were elevated at 6 h, reached a maximum between 18 and 24 h, when erythema was
most intense, but returned to control levels by 48 h, at which time the erythema had subsided.
Indomethacin substantially reduced blood flow, with a good correlation between the
reduction in visible erythema and prostaglandin E
2
and F
2
activity in irradiated skin. The
results are compatible with the view that UVC-induced erythema is mediated by products of
arachidonic acid metabolism. Changes in UVB-induced erythema were similar to those with
UVC at 24 h, but by 48 h the levels of arachidonic acid and of metabolites had returned to
normal, although erythema persisted. Further, although indomethacin suppressed prosta-
glandin formation, it altered blood flow only slightly, indicating that other factors must play
an important role in inflammation following UVB irradiation. Elevated histamine levels
have also been observed, but antihistamines have little effect in diminishing erythema
(Gilchrest et al., 1981).
Increased pigmentation of the skin by UVR occurs in two distinct phases: immediate
pigmentation and delayed tanning (Hawk & Parrish, 1982; Gange, 1987). Immediate
pigmentation, thought to result from oxidation and redistribution of melanin in the skin,
begins during irradiation and is maximal immediately afterwards; it occurs following
exposure to UVA and visible light and may fade within minutes or, after greater doses to
people with darker skin, may last up to several days. Delayed tanning is induced maximally by
exposure to UVB and becomes visible about 72 h after irradiation. It is associated with an
increase in the number of melanocytes as well as with increased melanocytic activity,
elongated dendrites, increased tyrosinase activity and increased transfer of melanosomes to
keratinocytes. Small freckles may be formed, particularly in fair-skinned individuals.
Not all pigmentary changes induced by UVR are localized at the site of irradiation.
Experimental exposures to UVB three times a week for eight exposures at the MED
increased the number of melanocytes and produced larger, more dendritic melanocytes in
both exposed skin and, to a much lesser extent, areas of skin shielded from the radiation. The
increase in melanocyte number in both exposed and covered areas was greater in individuals
whose melanocyte density was lower prior to exposure than in individuals with a high initial
density (Stierner eta/. , 1989).
The erythemal and tanning responses of human skin are genetically determined. Res-
ponses to a first seasonal exposure of about 30 min to the midday sun have been used as part
of the basis for a skin type classification for white-skinned people ranging from Celtic to
Mediterranean (Morison, 1983a; Pathak et al., 1987):
Skin type I Always burn, never tan
Skin type II Usually burn, tan less thanaverage (with difficulty)
Skin type III
Skin type IV
OTHER RELEVANT DATA
Sometimes mild burn, tan about average
Rarely burn, tan more than average (with ease)
169
UVA radiation produces immediate changes in melanocytes in white-skinned people. In
individuals with type-11 skin, multiple pinocytotic vesicles, larger vacuoles, swelling and
partial-to-total dissolution of the inner membranes of mitochondria and numerous small
vesicles associated with an enlarged Golgi apparatus were seen with doses that did not
produce immediate pigment darkening (Beitner & Wennersten, 1983). In those with type-III
skin, similar changes occurred but only with doses that produced immediate pigment
darkening (Beitner, 1986).
Three Japanese skin types have been described on the basis of personal reactions to the
sun (Kawada, 1986). Experimental exposure to monochromatic UVR showed that the MED
correlated well with skin type. Immediate tanning occurred but was not related to skin type.
After irradiation with the minimal dose that would produce immediate tanning, the tan faded
within 3-15 min; after greater exposures, the tan remained longer but never for more than 60
min. The action spectrum for immediate tanning had a maximum at 320 nm and decreased
gradually towards 400 nm. New pigment formation (delayed tanning) after exposure to 290
nm and 305 nm radiation began about 65 h after irradiation and increased until it reached a
maximum at 124 h (with a dose four times the MED) or 151 h (with a dose eight times the
MED). Following a dose three times the MED, some delayed tanning was still evident after
two months. The minimal melanogenic dose (producing delayed tanning) was greater than
the MED for all Japanese skin types, in contrast to findings in white Caucasians.
Parrish et al. (1981) showed that repeated daily exposure to doses of broad-band UVB
and UVA lower than the MED lowered the threshold for both erythema and true melano-
genesis for several subsequent days; the threshold for melanogenesis was decreased to a
greater extent than that for erythema, a separation that was more pronounced for UVA than
for UVB radiation.
(ii) Pigmented naevi
Exposure to the sun appears to stimulate the occurrence and behaviour of acquired
pigmented naevi. Kopf et a/. (1985) showed, in 80 consecutive patients with dysplastic naevus
syndrome, that the concentration of naevi on areas of the thorax protected relatively well
from the sun was substantially lower than that on areas exposed to the sun. Augustsson eta/.
(1990) showed that, in melanoma cases as well as in controls, the concentration of common
naevi was higher on the sun-exposed skin of the back than on the protected skin of the
buttocks. An Australian study compared naevi excised in summer to those excised in winter in
Western Australia. Inflammation, regression, mitotic activity and lymphocytic infiltration
were significantly more prevalent in naevi excised in summer than in winter (Holman eta/.,
1983b; Armstrong eta!., 1984). [The Working Group noted that these observations may be
confounded by the site of the naevi .]
In an Australian cross-sectional study of 511 people, the presence of palpable naevi on
the forearm was associated with female sex, young age, not having southern European grand-
parents, being born in Australia and intermediate categories of variables indicating sun
exposure (Armstrong et a/., 1986).
170 IARC MONOGRAPHS VOLUME 55
Gallagher eta/. (1990a,b) studied risk factors for common naevi in school children in
Vancouver, British Columbia, Canada. The number of naevi increased with age (from six to
18 years). Naevi occurred most commonly on intermittently than on constantly exposed parts
of the body and less commonly in skin that was rarely exposed. Ught and freckled skin,
propensity to burn rather than tan upon exposure to the sun and a history of frequent or
severe sunburn were associated with a large number of naevi.
Green et ai. (1988b) compared the prevalence of melanocytic naevi (benign pigmented
moles) in children aged 8- 9 in Kiddermister, United Kingdom, and Brisbane, Australia.
Regardless of skin colour, the mean number of naevi was at least five times larger in the
Australian children than in the British children. In both populations, naevi were more
prevalent in children with fair skin.
(iii) Ultrastructural changes
Jones, S.K. eta!. (1987) and Roth eta/. (1989) each described a patient who developed
many freckle-like lesions on all exposed sites following repeated exposure to high-dose UVA
from a home sunbed for tanning the skin. Biopsy showed increased numbers of large
melanocytes in the basal layers.
Rosario et a/. (1979) examined the sequential histological changes produced by single
exposures to UVA, UVB and UVC radiation on untanned skin of the lower back. Exposures
were designed to cause approximately equal degrees of erythema. Following UVB and UVC,
dyskeratotic cells ('sunburn cells') were scattered throughout the malpighian layer of the
epidermis at 24 and 48 h. By 72 hand seven days, they formed a continuous band in the upper
malpighian layer or the stratum corneum. Epidermal hyperkeratosis, parakeratosis and
acanthosis appeared concurrently at 72 h. The granular layer was focally absent at 24 and 48 h
and had increased focally at 72 hand seven days. There was a minimal-to-moderate lympho-
cytic infiltrate in the dermis which was most pronounced after 48-72 h. Infrequent mitotic
figures were observed in keratinocytes. UVA caused fewer dyskeratotic cells at all time
intervals, and these never coalesced into a band. UVA, however, elicited the greatest degree
of inflammation at 24, 48 and 72 h in terms of both quantity and depth of cellular infiltrate.
Endothelial cell swelling, nuclear dust and extravasation of red blood cells were generally
observed together. These dermal findings were more pronounced at 72 h. Neither epidermal
hyperkeratosis, parakeratosis nor acanthosis was observed. Intracellular oedema of mode-
rate degree was noted with all wavebands at all time intervals. The authors considered that
the production of more prominent dermal changes by UVA than by UVB and UVC might be
related to greater penetration of longer wavelengths. The histological changes returned to
normal earliest after UVB and latest after UVA irradiation.
Pearse et al. (1987) examined the effects of repeated irradiation with UVB (0.5, 1 and
2 times the MED three times a week for six weeks) and UVA (6 J/cm
2
[60 kJ/m
2
] three times
a week for three weeks). UVB irradiation at twice the MED led to significant increases in
epidermal thickness, stratum corneum thickness and keratinocyte height, as did UVA irra-
diation. Both UVA and UVB significantly increased glucose-6-phosphate dehydrogenase
activity and decreased succinic dehydrogenase activity throughout the epidermis. The auto-
radiographic labelling index was significantly increased following the highest dose of UVB.
OTHER RELEVANT DATA 171
The benign skin changes attributed to sunlight and seen on physical examination include
wrinkles, atrophy, cutis rhomboidalis nuchae (thick, yellow, furrowed skin, particularly on
the back of the neck), yellow papules and plaques on the face, colloid milium (firm, small,
yellow, translucent papules on the face, forearms and hands), telangiectasia, diffuse
erythema, diffuse brown pigmentation, ecchymoses in sun-damaged areas, freckles, actinic
lentigo (large, irregular, brown areas), Favre-Racouchot syndrome (yellow, thick come-
dones and follicular cysts of the periorbital, malar and nasal areas) and reticulated pig-
mented poikiloderma (reddish-brown reticulated pigmentation with telangiectasia and
atrophy and prominent hair follicles on exposed chest and neck) (Goldberg & Altman, 1984 ).
Although most commonly seen in fair-skinned Caucasians, these changes may also be seen in
Chinese heavily exposed to the sun (Giam, 1987). A visual system using facial photographs
has been developed to enable grading of the degree of elastosis (Cameron eta/., 1988).
Holman eta/. (1984a,b) made silicone rubber moulds of the microtopography of the skin
of the hands of 1216 subjects and developed a grading system to describe alterations in skin
surface characteristics observed under a low-power microscope. Using multivariate analysis,
independent risk factors for topographic evidence of actinic skin damage were: male sex. age,
tendency to burn upon exposure to the sun and outdoor occupation. Similar results were
reported by Green (1991).
Everett et al. (1970) reported ultrastructural changes in the epidermis of six elderly,
fair-skinned, freckled, blue-eyed, Caucasian male farmers with a history of multiple actinic
keratoses and skin cancers. Light microscopy showed effacement of epidermal rete ridges
and an irregular decrease in epidermal thickness in areas of skin exposed to sunlight. Three
groups of changes were apparent upon transmission electron microscopic examination:
firstly, local areas of degeneration involving groups of adjacent cells, with degenerative
changes resembling dyskeratosis in both the basal and the spinous layers of the epidermis;
secondly, disturbed cellular cohesion, with variable numbers, distribution and degrees of
maturity; and thirdly, changes in epidermal pigment-with the melanin concentration
varying from none to excessive-and melanosome complexes that were often abnormally
large.
Kligman (1969) described the changes in elastic tissue (elastic hyperplasia or actinic
elastosis) seen in the dermis of sun-exposed Caucasian facial skin. Such changes were quite
advanced before the extent of the damage became visible clinically. Some elastic hyperplasia
was seen in elderly blacks over the age of 70, but the changes were markedly less extensive
than those seen in whites.
Bouissou et al. (1988) studied elastic fibres in protected skin and skin highly exposed to
the sun from normal Caucasians of different ages, using light and electron microscopy. In
skin exposed to the sun, there was elastotic degeneration in the reticular dermis and
progressive thickening and curling of the elastic fibres in the upper dermis. Altered fibres
progressively formed thick, irregular masses, with clumps of amorphous, granular, elastotic
material and large areas of uneven staining appearing frequently thereafter. Electron
microscopy revealed that normal collagen and elastotic material were often contiguous but
never continuous.
172 IARC MONOGRAPHS VOLUME 55
(iv) Keratosis
The occurrence of keratosis, a benign but probably premalignant squamous neoplasm
of the skin (Marks eta/., 1988), has been studied in relation to exposure to sunlight in several
cross-sectional studies.
Chronic solar damage (assessed by cutaneous microtopographs and paraocular photo-
graphs) was associated with keratosis, after adjustment for age, in a study of 1216 people in
Busselton, Australia (Holman et a/., 1984a). A similar association between cutaneous
microtopography and prevalence of keratosis was observed by Green (1991) in a study of
1539 people in Nambour, Australia.
Vitasa eta/. (1990) conducted a study of 808 white watermen in Maryland, USA. The
prevalence of keratosis was 25%. The risk factors for this condition were found in a
multivariate analysis to be age, individually estimated cumulative exposure to sunlight, blue
eyes, childhood freckling and a tendency to sunburn.
Marks et al. (1983) studied 2113 adults in Maryborough, Australia. The prevalence of
keratosis was 56.9%. Adjusted for age, the prevalence of keratosis was significantly
associated with being born in Australia, with a tendency to sunburn and not tan and with blue
eye colour. In another survey by these authors, of 2000 adult in-patients from a hospital in
Melbourne, Australia, the prevalence of keratosis on the light-exposed areas of the head and
neck, forearms and back of hands was 37.7%. Prevalence of keratosis was significantly
associated with age and with being born in Australia and, among men, with outdoor occu-
pation (Goodman et a/., 1984). The Melbourne and Maryborough populations were
compared further by Marks and Selwood (1985), who attributed the higher prevalence of
keratosis in Maryborough to the fact that this population had a 14.2% higher erythemal
UVR level.
Foley eta/. (1986) studied 766 consecutive patients with keratosis. Lesions on the hands
and forearms in men were seen more often on the right side than on the left, which the
authors attributed to the higher exposure of the right side while driving an automobile. In
women, more lesions of the head and neck were on the left side.
(v) Photosensitivity disorders
Abnormal reactions to solar radiation, termed photosensitivity disorders, occur in a
relatively small number of exposed individuals; these have been reviewed comprehensively
(Harber & Bickers, 1981; Bernhard eta/., 1987). Genetic and metabolic diseases that may be
associated with photosensitivity include xeroderma pigmentosum, phenylketonuria, Bloom's
syndrome, Cockayne 's syndrome, Rothmund-Thomson syndrome, certain porphyrias,
Hartnup syndrome and pseudoporphyria cutanea tarda. The excision repair disorders are
discussed on pp. 191-194. Defects in pigmentation due to an absence of melanocytes
(vitiligo) and defective functioning of melanocytes (albinism) also confer susceptibility to
UVR because of failure to develop photoprotection through tanning responses.
In idiopathic photodermatoses, the primary abnormality is an acquired alteration in
reaction to sunlight. The commonest form is polymorphous light eruption. in which indi-
viduals who previously tolerated sun exposure develop itchy papules, vesicles or erythe-
matous patches or plaques on exposed areas after moderate exposure to the sun (Bernhard
et al., 1987). Other photosensitivity conditions include solar urticaria (Armstrong, 1986),
OTIIER RELEVANT DATA 173
hydroa vacciniforme (hydroa aestivate) (Halasz eta/. , 1983) and actinic reticuloid (Bernhard
et a/., 1987).
Photoaggravated dermatoses are conditions that may occur in the absence of exposure
to sunlight but can be induced or exacerbated by such exposure. The commonest is
recurrences of herpes simplex viral eruptions, usuaHy on the upper lip: this viral infection has
been reproduced by exposure to artificial sources of UVR (Spruance, 1985).
Other skin diseases reported to be photoaggravated include lupus erythematosus,
Darier's disease, acne vulgaris, atopic dermatitis, bullous pemphigoid, disseminated super-
ficial actinic porokeratosis, erythema multiforme, lichen planus, pellagra, pemphigus,
pityriasis alba, pityriasis rubra pilaris, psoriasis, acne rosacea, seborrheic dermatitis and
transient acantholytic dermatitis (Grover's disease) (Bernhard et al., 1987).
(b) Experimental systems
Agin eta/. (1981b) found that single exposures to UVA plus UVB caused thickening of
the whole epidermis and stratum corneum in pigmented and albino hairless mice.
Sterenborg et al. (1986) found similar changes after repeated exposures to mainly UVB in
hairless albino mice.
C57Bl mice irradiated with UVB daily for 10 days had a four-fold increase in the number
of epidermal melanocytes, with increased pigmentation and local thickening of the epi-
dermis (Rosdahl, 1979). A gradual, delayed, three-fold increase in the number of mela-
nocytes also occurred in shielded contralateral ears, without increased pigmentation or epi-
dermal thickening.
Generally consistent observations have been reported on chronic changes (photo-
ageing) in hairless mice (Bissett et al., 1987, 1989; Kligman, 1989). Bissett eta/. (1987)
described the progression of chronic UV damage to the skin in albino hairless Skh:Hr-1 mice
irradiated with UVB or UVB plus.UVA three times a week for 16 weeks, with a 17-week
recovery period. UVB and a combination of UVA and UVB produced similar changes. An
early increase in transepidermal water loss was seen, with a doubling of skin thickness and
changes in the microtopography of the skin surface with visible skin wrinkling. Dose-
dependent histological changes were seen, with thickening and hyperplasia of the epidermis.
Dermal elastic fibres thickened and proliferated throughout the upper dermis, and there was
a proliferation of fi broblasts, sebaceous cysts and dermal cysts in the upper dermis. By week
16, the skin was clearly elastotic, with thick, tangled masses of elastic fibres in the dermis. Use
of a broad-spectrum sunscreen product with a claimed SPF (skin protector factor) of 15
retarded but did not completely prevent the effects of UVB and of UVB plus UV A radiation.
Animals exposed to UVB and then allowed to recover for 12 weeks exhibited a zone of
clearance of all abnormal elastin from the dermal-epidermal junction to mid-way down the
dermis.
Animals exposed to UVA alone for 33 weeks with a recovery period of 18 weeks (Bissett
et a/., 1987) exhibited a different pattern of changes. Epidermal thickening occurred at a
slower rate, there was no increase in water loss; and sagging rather than wrinkling of the skin
occurred. There was a very gradual increase in cellularity; focal areas of collagen damage and
absence of elastic fibres were seen; the size and number of dermal cysts increased; and there
was only slight evidence of recovery after 18 weeks. UVA appeared to accelerate several
174 IARC MONOGRAPHS VOLUME 55
changes similar to those that occur with chronological ageing in mice. Using a dual grating
monochromator, Bissett eta/. (1989) examined the action spectra for these changes. Most
were similar and occurred in the UVB waveband: wrinkling, glycosaminoglycan increase,
collagen damage, elastosis, epidermal thickening, dermal cellularity and dermal inflam-
matory cell increase. In contrast, the spectrum for skin sagging was very broad, with a
maximum near 340 nm. These results suggest that more than one chromophore is involved in
UV-induced chronic skin changes.
High doses of UVA (cumulative dose, 3000 J/cm
2
) were reported to produce severe
elastic fibre hyperplasia, but no large aggregates of elastosis or destruction of collagen, in
female Skh-hr 1 albino mice (Kligman eta/., 1985; Kligman, 1989). A dose of 13 000 J/cm
2
from a filtered (50% cutoff at about < 345 nm) UVA source, however, produced only
insignificant changes. Dose- response studies with another UVA source, filtered to remove
all radiation below340 nm, produced some elastin thickening at a total dose of8000 J/cm
2
as
well as increased epidermal proliferation and increased and enlarged dermal cysts (Kligman
et a/., 1987).
Kligman and Sayre (1991) found that the action spectrum for elastosis in albino hairless
mice was similar to that for erythema, except that longer UVA wavelengths ( > 330 nm) were
less effective for elastosis.
The chronic effect of repeated UV irradiation was also investigated in naked albino N g/-
mice using high total doses ( > 20 000 J/cm
2
) from a predominantly UVA source (but con-
taining some UVB) administered for 16 h daily for 8.5 months (Berger eta/., 1980a). Dermal
changes similar to those seen in human actinic elastosis were observed. There was endo-
thelial swelling of dilated small capillary vessels and slight perivascular infiltration. Particu-
larly in the upper dermis, collagen was replaced with an amorphous material that stained
faintly with haematoxylin-eosin. Mast cells and a relatively increased number of spindle-
shaped fibroblasts were found in the middle and lower dermis. Large aggregates of nume-
rous tangled, thickened fibres with the staining properties of elastic tissue were seen.
Electron microscopy showed that elastic fibres were increased in number and size and there
was splitting of collagen fibres. Most small blood vessels were dilated, with multiple basal
lamina. The elastic tissue changes showed no signs of regression 2.5 months after irradiation
had been discontinued, although the epithelial changes regressed over this period.
Similar changes in elastic tissue (Berger et al., 1980b) were found after exposure to a
filtered UVA source which contained no UVB, but no alteration of collagen was observed
and inflammatory changes were absent. Electron microscopy showed changes similar to
those observed in actinic elastosis.
In female, lightly pigmented, hairless Oslo/Born mice, UVB alone produced moderate
elastosis, UVB and UVA together produced a slightly reduced degree of elastosis, but UVB
followed by large doses of UVA produced severe elastosis; UVA alone was reported to have
no effect (Poulsen et al., 1984). In Skh:Hr 1 albino hairless mice, a combination ofUVA and
UVB had additive effects (Kligman eta/., 1985).
(c) Comparison of humans and animals
No direct comparison has been reported of the optical properties ofwhole human and
mouse epidermis; however, the available data suggest that the absorption/transmission
OTIIER RELEVANT DATA 175
spectra are of a similar general shape but have marked quantitative differences. For example,
a comparison of data on a graph of effects on human epidermis not previously exposed to
UVR (Bruls eta/., 1984a) with tabulated data on mouse epidermis not previously exposed
(Sterenborg & van der Leun, 1988), generated in the same laboratory, showed that trang.
mission in the mouse was two orders of magnitude greater in the UVC region and one order
of magnitude greater in the UVB and UVA regions than in humans. In human and mouse
epidermis, prior exposure to UVR resulted in marked decreases in UVR transmission. No
study has been reported on mouse stratum corneum.
4.2.2 Immune response
Exposure to solar radiation and UVR can alter immune function in experimental ani-
mals and humans. This area of research is known as photoimmunology and has recently been
reviewed (Daynes eta/., 1983; Parrish, 1983; Parrish eta/., 1983; Bergstresser, 1986; Roberts
eta/., 1986; Krutmann & Elmets, 1988; Morison, 1989).
(a) Humans
(i) Contact hypersensitivity (allergy)
Exposure of normal subjects to radiation in a tanning solarium which emitted mainly
UVA but also UVB radiation reduced allergic reactions to 2,4-dinitrochlorobenzene
(Hersey eta/., 1983a). Halprin eta/. (1981) and Nusbaum eta/. (1983) found that UVB
radiation partially suppressed the development of contact allergy to nitrogen mustard in
patients with mycosis fungoides and psoriasis. Exposure to UVB was begun prior to
treatment with mustard, and the field of exposure to the chemical was included in the area
exposed to radiation, so that both a local and systemic effect may have been measured. In
both studies, the proportion of patients sensitized to mustard gas was reduced by exposure to
UVB radiation, and sensitization, when it did occur, was delayed. [The Working Group noted
that the presence of diseases known to influence the immune system makes the findings
difficult to interpret.]
Response to 2,4-dinitrochlorobenzene was diminished in sun-damaged skin in subjects
previously sensitized to the allergen (Kocsard & Ofner, 1964; O'Dell eta/., 1980). UVB-
induced suppression of contact allergy to nickel and other allergens (e.g. , cobalt) has also
been reported (M0rk & Austad, 1982; Sjovall & Christensen, 1986).
Studies on the possible mechanism of suppression have focused mainly on the effects on
antigen presentation in the skin. At low doses of UVB ( < 15 mJ/cm
2
), Langerhans' cells are
the only epidermal cells to be altered morphologically (Aberer el a/., 1981 ). Depletion of
Langerhans' cells after a few exposures to UVB radiation is transient (Tjemlund & Juhlin,
1982; Scheibner eta/., 1986a); however, chronic exposure to sunlight appears to result in a
sustained reduction, since fewer Langerhans' cells are found in exposed than in unexposed
skin of older adults but not of young adults (Gilchrest eta!., 1982; Scheibner eta/., 1983;
Thiers et a/., 1984; Czernielewski et al., 1988). Pigmentation does not seem to protect
Langerhans' cells, since exposure to UVB plus UVA radiation (simulating natural UVR)
produced similar degrees of depletion of these cells in dark-skinned Australian aboriginals
and in fair-skinned people of Celtic descent (Hollis & Scheibner, 1988); Langerhans' cells
176 IARC MONOGRAPHS VOLUME 55
were equally affected in fair-skinned and dark-skinned people after multiple exposures to
sunlight (Scheibner et a/., 1986b ).
The antigen-presenting function ofLangerhans' cells is also diminished after irradiation
in vivo with UVB (Cooper et al., 1985; Rasanen eta/., 1989). The function returns to the
epidermis within 24 h, owing to the appearance of two cell populations that are distinct and
different from Langerhans' cells (Cooper eta/., 1986). Both populations have receptors for
the monoclonal OKM5 antibody; one also has receptors for the OKMl antibody and is
possibly a dendritic cell from blood, while the other is OKM 1- and is related to a subset of
blood monocytes. These cells can activate T cells in the absence of exogenous antigen and
lead to the generation ofT-suppressor cells which can inhibit various immune responses.
Baadsgaard et al. (1988) showed that epidermal cells from UVB-irradiated skin can stimu-
late suppressor/cytotoxic lymphocytes. This may occur via at least two pathways: activation of
T-suppressor/inducer cells or induction of interleukin-2 production. These observations
suggest that UV-induced immune suppression is more closely related to the appearance of
OKMS + cells in the epidermis than to the disappearance of Langerhans' cells.
Systemic suppression of contact allergy may also result from exposure to UVR.
Granstein and Sauder (1987) exposed subjects to a MED of mainly UVB radiation and
measured levels of serum interleukin-1 activity that peaked 1-4 h after exposure and
returned to baseline by 8 h. This activity may originate from the skin, in which increased
levels have been detected after UVB irradiation (Kupper eta/., 1987; Oxholm eta/., 1988;
Rasanen eta/. , 1989).
A recent study (Yoshikawa et al., 1990) showed that suppression of UVB-induced
contact allergy may be a risk factor for nonmelanocytic skin cancer. Approximately 60% of
normal subjects were sensitized by application of 2,4-dinitrochlorobenzene to UVB-irra-
diated skin compared to 8% of patients with a history of skin cancer. Many skin cancer
patients were also immunologically tolerant to this allergen; this was not observed in normal
subjects.
Pigmentation does not protect against UV-induced immunosuppression, since it occurs
in the same proportion of black and white people (Vermeer et al., 1991).
(ii) Lymphocytes
A single, whole-body exposure to UVB radiation which produced painful erythema
produced a transient decrease in the proportion of circulating E rosette-forming cells and in
the response of lymphocytes to a mitogen (Morison et al., 1979a). McGrath eta/. (1986)
found a decrease in the proportion of circulating suppressor cells following exposure to half
the MED of UVB, although the total number ofT lymphocytes was not altered. Exposure of
normal subjects to sunlight daily for two weeks, however, produced different effects: The
total proportion ofT lymphocytes was diminished owing to a pronounced drop in the propor-
tion of helper/inducer cells associated with an increase in the proportion of suppressor cells
in the peripheral blood (Hersey et al., 1983b). Similar changes occurred after exposure of
normal subjects to UVA pi us UVB radiation (Hersey et al., 1983a). When UVB radiation was
removed by a Mylar filter (Hersey et al., 1988) or a sunscreen (Hersey eta/., 1987), most of the
effect was removed. The numbers of circulating T cells and helper-T cells were significantly
reduced by exposure of normal subjects to solar lamps containing UVA(with minimal UVB)
OTiiER RELEVANT DATA 1n
and to fl uorescent tubes emitting mainly visible light, which contained small quantities of
UVB, but the number of T-suppressor cells was only slightly reduced. These effects were
considered to be due to the UVB radiation (Rivers et a/., 1989).
(iii) Infectious diseases
Recurrent infections due to herpes simplex virus types 1 and 2 can be induced by
exposure to UVB radiation (Wheeler, 1975; Spruance, 1985; Klein & Linnemann, 1986;
Perna et a/., 1987). Presumably, local alterations of immunity, associated with extensive
UV-induced tissue damage, are responsible for this reactivation.
(iv) Photosensitive disease
An interaction between solar radiation and the immune system was first postulated on
the basis of observations that the pathogenesis of several diseases is characterized by photo-
sensitivity. Solar urticaria, photoallergy and lupus erythematosus are the main examples (for
reviews, see Morison, 1983b,c; Morison & Kochevar, 1983).
(b) Experimental systems
(i) Contact hypersensitivity
The first report of UV-induced suppression of contact hypersensitivity was in guinea-pigs
that received applications of a sensitizing chemical through UV-irradiated skin (Haniszko &
Suskind, 1963). This effect has since been termed local suppression of contact hyper-
sensitivity. Later, in studies of UV-induced tumour susceptibility in mice, it was found that
UVR could also induce systemic suppression of contact hypersensitivity when the sensitizer is
applied through unexposed skin only (Kripke et al., 1977). This occurred during chronic
treatment of mice, was transient and appeared to be due to failure of an effector mechanism
(efferent block) of the immune response (Jessup et al., 1978). These two phenomena, local
and systemic suppression of contact hypersensitivity, are probably mediated by different
mechanisms.
Local suppression of contact hypersensitivity: Pretreatment of mice with low doses of
UVB radiation (100-700 11m
2
fluorescent sunlamp radiation daily for four days) suppressed
the development of contact hypersensitivity to sensitizing chemicals (e.g., 2,4-dinitrofluoro-
benzene) applied subsequently to irradiated skin (Toews eta/., 1980; Elmets eta/., 1983). This
effect was associated with generation of hapten-specific LyT-1 + T cells which suppress the
induction phase of the immune response (Elmets et a/., 1983). The most effective wave-
lengths are < 300 nm (Elmets et al., 1985). Local suppression of contact hypersensitivity by
UVB radiation also occurs in hamsters (Streilein & Bergstresser, 1981).
Several hypotheses have been explored to explain the mechanism of local suppression.
Multiple exposures to sunlight result in a striking reduction in the number of Langerhans'
cells in guinea-pigs, as detected by ultrastructural examination (Fan et al., 1959). UV-induced
alterations occur in Ia + Langerhans' cells (Streilein et a/. , 1980; Perry & Greene, 1982;
Gurish eta/., 1983; Stingl eta/., 1983), but alterations in other cells may be involved.
Thy-1 + dendritic epidermal cells (identified by antibodies to surface markers on lym-
phocytes), found in mouse but not reported in human skin, are bone marrow-derived
lymphocytes which down-regulate contact hypersensitivity. They are not affected by low-
178 IARC MONOGRAPHS VOLUME 55
dose UVR, and hapten-conjugated Thy-1 + dendritic epidermal cells can induce tolerance on
subcutaneous injection into the footpad or after intravenous injection (Welsh & Kripke,
1990). This finding is supported by the observations {Okamoto & Kripke, 1987) that (i) the
draining lymph nodes of mice treated with low doses of UVR contained these hapten-
conjugated cells after exposure to a contact sensitizer, (ii) injection of these cells into other
syngeneic mice resulted in the generation of suppressor cells, and (iii) removal of these cells
from the lymph node cells abolished the suppression.
I-J +, Thy-1-, I a- antigen-presenting cells, which are also resistant to low doses of UVB
radiation and preferentially generate a suppressor cell pathway, may also be involved in local
suppression (Granstein eta!., 1984; Granstein, 1985; Granstein eta/., 1987; Okamoto &
Kripke, 1987).
Keratinocytes may also be involved through the production of epidermal cell-derived
thymocyte-activating factor (ETAF), which is functionally and biochemically very similar to
interleukin-1, a nonspecific helper factor necessary for activation ofT cells by antigen.
Interleukin-1 can reduce expression of contact hypersensitivity in mice (Robertson et a/.,
1987). Studies by several workers have suggested that exposure to UVR inhibits the
production of ETAF (Sauder eta!., 1983) or decreases its activity (Stingl et al., 1983). When
antigen-presenting cells are exposed to UVR, their ability to activate T cells is markedly
inhibited (Tominaga et al., 1983). UV irradiation of mice induces the release of a specific
interleukin-1 inhibitor, keratinocyte-derived, EC-contra IL 1 (Schwarz et al., 1988). Other
workers (Ansel eta/., 1983; Gahring eta/., 1984) have found increased production ofETAF.
[The Working Group noted that differences in the radiation sources and model systems could
explain the discrepancies between the results of these studies.)
Systemic suppression of contact hypersensitivity: Systemic suppression of contact hyper-
sensitivity in mice requires a higher exposure dose (40-50 KJ/m
2
) than local suppression
(Kripke & Morison, 1986a). A dose of 8.2 kJ/m
2
at 320 nm produced nearly 50% systemic
suppression, and 100 kJ/m
2
produced 80% suppression (Noonan eta/., 1984). Like local
suppression, systemic suppression is associated with the generation of suppressor Lyt-1 + T
lymphocytes (Noonan eta/., 1981a; Ullrich & Kripke, 1984). The pathways leading to the
appearance of these lymphocytes are, however, probably different. Systemic suppression has
also been induced in guinea-pigs (Morison & Kripke, 1984) and in the South American
opossum, Monodelphis domestica (Applegate et a/., 1989). Artificial sources of UVB
radiation and sunlight, but not UVA, induce systemic suppression of contact allergy in mice
and guinea-pigs (Morison eta/., 1985).
Determination of an. action spectrum for systemic suppression of contact hyper-
sensitivity in mice revealed peak activity in the 260-270 nm region, which is consistent with a
superficial location of the chromophore in the epidermis (De Fabo & Noonan. 1983; Noonan
& De Fabo, 1985). Two candidate molecules, urocanic acid and DNA, have been suggested.
Several lines of evidence indicate that abnormalities in Langerhans' cells are not in-
volved in systemic suppression, in contrast to local suppression (Lynch et al., 1983; Morison et
a/., 1984; Noonan eta/., 1984), and that a defect of antigen presentation is not an initial step
(Kripke & McClendon, 1986). Soluble mediators are released from irradiated skin and may
generate suppressor cells in a distant organ. Serum collected from UV-exposed mice and
epidermal cells exposed to UVR in vitro contain factors that can induce systemic suppression
OTHER RELEVANT DATA 179
(Schwarz eta/., 1986). The situation is far from straightforward, however, since a recent study
indicated that multiple suppressive factors, with different immunosuppressive properties,
may be released by different wavelengths of UVR (Kim et al., 1990). Indomethacin blocks
the development of suppression (Chung eta/., 1986; Jun eta/., 1988), indicating that prosta-
glandins may also be involved in the pathway.
Several properties of the suppressor cells have been defined: (i) they suppress primary
proliferative responses but not a secondary response in vitro (this is consistent with the idea
that they suppress induction of sensitization but not with the proposal that they elicit a
response in a previously sensitized animal) (Ullrich, 1985); (ii) their action is limited to
T-dependent antigens (Ullrich, 1987); and (iii) they can modulate other immunological
pathways, such as formation of anti-hapten antibodies and cytotoxic-T lymphocytes (Ullrich
eta/., 1986a).
(ii) Delayed hypersensitivity to injected antigens
Systemic suppression of delayed hypersensitivity was induced by UVB irradiation of
mice following injection of2,4-dinitrochlorobenzene into the footpad (Jessup eta/., 1978), of
hapten-coupled spleen cells into the footpad (Greene et al., 1979) or the ear (Noonan et al.,
1981b) or of erythrocytes and soluble protein antigens into the footpad (Ullrich eta/., 1986b)
and is associated with the generation of antigen-specific T lymphocytes. This suppression
differs from the suppression of contact hypersensitivity to topically applied allergens because
delayed hypersensitivity can be restored in UV-irradiated mice by injection of hapten-
coupled spleen cells from normal mice (Noonan et al., 1981b; Kripke & Morison, 1985,
1986b). Furthermore, systemic injection of methylprednisolone before immunization
prevented suppression of delayed hypersensitivity but had no effect on the suppression of
contact hypersensitivity (Kripke & Morison, 1986b).
Systemic depression of splenic antigen-presenting cell function was demonstrated in
UVB-exposed mice (Letvin eta/., 1980a,b; Gurish eta/., 1982). Two explanations have been
advanced: a transient redistribution of antigen-presenting cells to peripheral lymphoid
tissues in response to UV-induced inflammation (Gurish eta/., 1982; Spangrude eta/., 1983)
or direct damage to blood monocytes or other precursors of splenic antigen-presenting cells
as they circulate through the skin (Spangrude eta/., 1983). The latter theory is supported by
the observation that immunization with hapten-conjugated splenic antigen-presenting cells
or epidermal cells exposed in vitro to UVR can induce hapten-specific T-suppressor cells (Fox
eta/., 1981; Sauder et al., 1981).
The role of one of the proposed chromophores, urocanic acid, has been explored. UV-
irradiated urocanic acid (containing 74% cis-urocanic acid after 4 h) suppresses delayed
hypersensitivity to HSV-1 when injected subcutaneously or applied to the skin of mice (Ross
eta/., 1986), and is thus similar to UVB radiation (Ross et al., 1987). In both instances,
phenotypically similar suppressor celJs were induced (Howie et al., 1986a; Ross et al., 1987).
In addition, intravenous administration of cis-urocanic acid impairs antigen-presenting cell
function in splenic dendritic cells. h e ~ e observations suggest that trans-urocanic acid is the
photoreceptor for UVB-induced systemic suppression of delayed hypersensitivity and that
cis-urocanic acid acts as an immunomodulator (Noonan et al., 1988).
180 IARC MONOGRAPHS VOLUME 55
(iii) Immunology of ultraviolet-induced skin cancer
Most UV-induced tumours in mice are highly antigenic and are rejected upon transplan-
tation into normal syngeneic recipients; however, they grow progressively in immuno-
suppressed recipients (Kripke, 1974). The specific immunological rejection of these trans-
planted tumours is mediated by cytolytic-T lymphocytes aided by natural killer and cytotoxic-
T cells (Fortner & Kripke, 1977; Fortner & Lill, 1985; Streeter & Fortner, 1988a,b ). Thmours
grow in UV-irradiated recipients or primary hosts because T-suppressor lymphocytes
induced by the exposure to UVR block the normal immunological surveillance system
(Fisher & Kripke, 1977; Spellman et al., 1977; Fisher & Kripke, 1978; Spellman & Daynes,
1978}. The function of these suppressor cells is specific in that, whereas they prevent
development of UVR-induced tumours, they do not alter the growth of chemically induced
tumours or skin allografts (Kripke & Fisher, 1976; Fisher & Kripke, 1978).
The phenotype of the suppressor cells is LyT1 + 2-, Ia- (antibodies to surface markers on
lymphocytes}, similar to that of other UV-induced suppressor cells (Ullrich & Kripke, 1984).
These suppressor cells are important in the development of primary neoplasms. de Gruijl
and van der Leun (1982b, 1983) found accelerated development ofUVR-induced tumours in
hairless mice that had been exposed previously to UVR at a separate site. Fisher and Kripke
(1982) observed that, if suppressor cells were present from the time of commencement of
exposure to UVR, the latent period for development of tumours was shortened and the
tumour yield was increased. Thus, photocarcinogenesis in mice appears to involve at least
two UVR-induced alterations: (i) an alteration in DNA leading to transformation of cells (see
pp. 188-189) and (ii) a specific systemic immunological alteration that permits expression of
the tumour (Fisher & Kripke, 1977).
Suppressor cells can be induced by doses of 40-50 k.J/m
2
of radiation from fluorescent
sunlamps (see Fig. 9c, p. 64) (Kripke & Morison, 1986a), and susceptibility to transplanted
tumours is evident long before the de-novo appearance of tumours (Fisher & Kripke, 1977).
Suppressor cells can be induced by exposure to UVC (from low-pressure mercury discharge
lamps) (Lill, 1983}, UVB (De Fabo & Kripke, 1980), large doses of UVA (Morison, 1986)
and sunlight (Morison & Kelley, 1985). Wiskemann et al. (1986) described an effect of
neutral white fluorescent bulbs. [The Working Group considered that this effect may have
been due to low levels of UVB from this source.]
(iv) Transplantation immunity
. The immune responses in graft rejection and graft-versus-host disease are complex and
directed against class I antigens of the major histocompatibility complex which are expressed
on all nucleated cells and class II Ia antigens which are expressed normally on lymphocytes
and macrophages. Lindahl-Kiessling and Safwenberg (1971) demonstrated that UV irradia-
tion of stimulator cells could abrogate the proliferation of responder cells in a mixed-
lymphocyte reaction. Subsequent studies (Alter et al., 1973; Bach eta/., 1977) indicated that
this effect was due to alteration of class II Ia antigens on the cells bearing them. These initial
observations have been extended to various systems_
Pre-transplant, donor-specific blood transfusions have been used to reduce the need for
post-transplant immunosuppression, with varying success. The basis for this effect is thought
to be generation of donor-specific T-suppressor lymphocytes in the host. Lau et al. (1983)
OTHER RELEVANT DATA 181
found that exposure of the blood to UVB radiation prior to transfusion greatly enhanced this
effect and permitted long-term survival of allografts of islets of Langerhans across a major
histocompatibility barrier in rats. The effect was shown to be due to inactivation of
lymphocytes by radiation, resulting in cancellation of a signal from Ia antigen-positive cells
and permitting the generation of donor-specific T-suppressor cells. A similar effect was
demonstrated with rat heart allografts (Balshi et al., 1985).
Deletion of I a antigens or inactivation of cells bearing them may explain prolonged graft
survival in other systems. Exposure of mouse tail skin to UVB radiation in vitro prolonged its
survival as a graft when !-region differences only were present, but UVB had no effect in the
case of complete H-2 differences (Claas et a/., 1985). Similarly, mouse corneal allograft
survival was prolonged by exposure to UVB radiation in vitro (Ray-Keil & Chandler, 1986).
Prolonged survival as grafts of rat islets of Langer hans exposed to UVB radiation in vitro was
apparently due to inactivation of dendritic cells bearing Ia antigens (Lau eta/., 1984).
The model of UVR-induced systemic suppression of delayed hypersensitivity has been
extended to transplantation studies, because of the considerable potential for manipulating
the immune system in transplantation. Sensitization of mice with allogeneic spleen cells after
a single exposure to UVB radiation suppressed the delayed hypersensitivity response to these
cells and proliferation of lymphocytes from the irradiated mice in a mixed-lymphocyte
these effects are due to generation of suppressor cells specific for donor antigens
(Ullrich, 1986). Interestingly, exposure of the mice to radiation need not precede exposure to
the antigen but can be delayed up to five days after first contact with the antigen, unlike other
forms of suppression of delayed hypersensitivity (Magee eta/., 1989a). Similar observations
have been made in rats, but suppressor cells were not demonstrated in the spleen (Magee et
a/., 1989b). Subcutaneous injection of epidermal cells that have been exposed to UVB
radiation in vitro can similarly cancel a delayed hypersensitivity response in mice; this effect is
associated with prolongation of skin allograft survival (Thmaki & Iijima, 1989).
Graft-versus-host disease can also be reversed by UVR. Two rat models have been
studied. Pretreatment of donor bone marrow with UVB radiation did not increase the failure
of grafts, but it prevented graft-versus-host disease in most instances (Pepino et a/., 1989).
Pre-irradiation of rat skin with UVB prevented subsequent development of cutaneous
graft-versus-host disease at the site of exposure (Glazier et al., 1984). In both of these studies,
an alteration of Ia-bearing cells was postulated as the mechanism.
(v) Infectious diseases
Classic delayed hypersensitivity to complex protein antigens (correlated with resistance
to a number of infections) can be suppressed by exposure to UVB radiation (Ullrich et ai.,
1986b).
Exposure of mice to low doses (1.3-3.4 kJ/m
2
) ofUVB (less than a human MED) at the
site of intradermal infection with herpes simplex type 2 virus increased the severity of the
disease. Unirradiated mice developed only a single vesicle at the site of inoculation, whereas
irradiated mice developed zosteriform lesions which healed slowly and, at the highest dose of
radiation, were lethal. At doses that increased the severity of the infections, systemic
suppression of delayed hypersensitivity to the virus due to generation of antigen-specific
T-suppressor lymphocytes was observed (Yasumoto et a/., 1987). In-vitro assays showed
182 IARC MONOGRAPHS VOLUME 55
UVB-induced impairment of antigen presentation, which may have been due to the presence
of suppressor factors in the supernatant (Hayashi & Aurelian, 1986). Similar results were
found in a model of herpes simplex virus type 1 infections in mice (Howie eta/., 1986a,b,c;
Otani & Mori, 1987). [The Working Group considered that these experiments have not
demonstrated clearly that the effect of radiation on the induction of immunity is local, since
the possibility of an indirect systemic effect has not been explored.]
Exposure to low doses of UVB radiation prevented the development of delayed hyper-
sensitivity to the protozoan, leishmania, and reduced the number and severity of skin lesions
when leishmania was inoculated at the site of exposure. Exposure to radiation did not,
however, alter the viability of the organisms or the degree of their dissemination to distant
sites-the spleen, lymph nodes and skin. Furthermore, the irradiated mice reacted to a
second, distant inoculation as if it were a primary infection, presumably because they lacked
the cell-mediated immunity that would be needed to control this second attack of the
organism (Giannini, 1986).
Exposure of mice to UVB radiation also caused systemic suppression of delayed
hypersensitivity to the yeast Candida albicans (Denkins et al., 1989), through two possible
mechanisms: one mediated by suppressor cells (detected in the spleen) triggered by exposure
to radiation prior to contact with the antigen and another which did not involve splenic
suppressor cells and was triggered by exposure to radiation following exposure to the
antigen.
(vi) Human lymphocytes in vitro
Lymphocytes are highly sensitive to low doses of UVR. UVC was approximately 10
times more effective than UVB and 105 times more effective than UVA on mononuclear
peripheral blood cells in vitro (Morison eta/., 1979b). Cripps et al. (1978) found that UVC
was preferentially toxic to T lymphocytes, but that T and B lymphocytes were similarly
susceptible to UVB. UVA did not appear to kill Tor B cells. Exposure of mononuclear peri-
pheral blood cells to UVB radiation inhibited both natural killer cell activity and the
response of these cells to stimulation by a mitogen (phytohaemagglutinin) (Schacter et al.,
1983), in the absence of any apparent change in viability. The effect on natural killer cell
activity occurred selectively at the post-binding stage of lysis (Elmets et al., 1987) and could
be virtually reversed by the addition of interleukin-2 and superoxide dismutase (Toda eta/.,
1986).
(c) Comparison of humans and animals
Firstly, most observations have been made in experimental systems and few studies have
involved humans, and it can be only assumed that results of studies in mice can be
extrapolated to humans. Furthermore, in no instance have parallel studies in an experimental
system and in humans been performed to test this assumption. Secondly, while most
investigations of photoimmunology have focused on the effects of 'UVB' radiation, in most
studies this term refers to the emission spectrum of a fluorescent sunlamp (see Fig. 9c, p. 64)
which contains both UVC and UVA, as well as UVB radiation, besides having little in
common with the spectrum of sunlight. Fortunately, in the few studies in which the effects of
fluorescent sunlamps and sunlight have been compared in experimental systems, similar
alterations in immunity have been observed. Finally, with few exceptions, the effect of
OTIIER RELEVANT DATA 183
exposure to UVR is to suppress immunity highly selectively, at least in experimental animals.
Thus, in mice, certain cell-mediated immune responses are suppressed by UVR, whereas
humoral immunity is largely unaffected. The selective nature of UVR-induced iinmuno
suppression has not been established in humans, but no evidence exists to suggest that it does
not apply. The importance of such selectivity is that it differs from the forms of immuno-
suppression seen most commonly in humans, namely viral and drug-induced suppression,
which affect most functions of the immune system. Exposure of humans to UVR is unlikely
to cause paralysis of immune function but probably selectively negates a few immune
responses.
4.2.3 Eye
(a) Humans
(i) Anterior eye (cornea, conjunctiva)
The cornea absorbs UVC and UVB radiation (Sliney & Wolbarsht, 1980). Sunlight has
been implicated as causing nodular band keratinopathies (spheroidal degeneration and
climatic droplet keratopathy), pinguecula, pterygium, photokeratitis and photokerato-
conjunctivitis (Wittenberg, 1986). Artificial sources of UVR, including welding arcs and
germicidal lamps, cause photokeratoconjunctivitis and photo keratitis (Sliney, 1986). A study
by Taylor et al. (1989) of the association between exposure to broad-band UVR and corneal
disease in 838 fishermen in Chesapeake Bay, Maryland, USA, reported a significant
association with pterygium and climatic droplet keratopathy but a weak association with
pinguecula.
(ii) Lens
The lens absorbs radiation between 305 and 400 nm (Wittenberg, 1986). UVR produces
substantial photodamage to both the structural proteins and key enzymes of the lens (for
review, see Andley, 1987).
Taylor eta/. (1988) studied the two major types of senile cataract (nuclear and cortical
cataracts) in 838 Maryland fishermen for each of whom mean annual and cumulative UVB
exposure had been assessed. High cumulative exposure to UVB and high annual exposure to
UVB were both associated with increased risk of cortical cataract, but no association was
seen with nuclear cataracts. The association between exposure to solar radiation and cataract
is also supported by studies of cataract in northern India and China and in aborigines in
Australia and by an analysis of data from the US National Health and Nutritional Exami-
nation Survey. These studies were reviewed by Wittenberg (1986).
It has been claimed that the presence of low levels of photosensitizing compounds in lens
tissue may contribute to cataractogenesis (Lerman, 1988).
(iii) Posterior eye
The posterior eye is composed of the vitreous humour and the retina (Lerman, 1980). In
the normal eye, solar radiation in the visible and near infrared regions (400-1400 nm)
reaches these structures. Refraction of this waveband by the cornea and lens greatly increases
the irradiance between the surface of the cornea and the retina (Sliney & Wolbarsht, 1980).
Permanent retinal damage was observed after direct viewing of the sun and viewing of
solar eclipses and in aircraft spotters during the Second World War, but no epidemiological
184 IARC MONOGRAPHS VOLUME 55
study has associated retinal pathology with routine environmental exposure to sunlight
(Wittenberg, 1986). The suggestion that senile macular degeneration is related to solar
exposure was not supported by a large study of fishermen in Maryland (West eta/., 1989).
(b) Experimental systems
(i) Anterior eye
Pitts eta/. (1977) and Cullen (1980) studied the effects of exposure to UVR at 295 nm on
the corneas of pigmented rabbit eyes. The threshold dose for corneal damage was 0.05 J/cm
2
.
Changes observed with a slit lamp biomicroscope included discharge, corneal debris,
haziness, granular change, epithelial exfoliation, stromal opacities and stromal haze.
Applegate and Ley (1991) showed that UVR-induced corneal opacification and neo-
vascularization of the cornea of the South American opossum M. domestica was due to ON A
damage, as these effects could be delayed by subsequent illumination with photoreactivation
light, which specifically monomerizes pyrimidine dimers.
(ii) Lens
Cataracts have been produced in pigmented rabbit eyes by exposure to UVB radiation
(Pitts eta/. , 1977). Cataracts were produced in young albino mice 60 weeks after irradiation
with a black light (predominantly UVA) (Zigman & Vaughan, 1974; Zigman eta/., 1974).
Albino mice developed anterior lens opacities after daily exposure for one to two months to a
UVB plus UVA source (290-400 nm), but not after the source was filtered to remove
radiation < 320 nm (Jose & Pitts, 1985).
(iii) Posterior eye
The effects of solar radiation on the posterior eye have been reviewed (Wittenberg,
1986; Andley, 1987). Irradiation of calf vitreous humour in vitro with visible radiation in the
presence of photosensitizers resulted in partial liquefaction, suggesting that photogenerated
active species of oxygen may damage the vitreous structure. In rabbits in vivo, however, little
liquefaction was seen, suggesting a protective mechanism in the intact organ (Pitts eta/.,
1977).
Damage to the retina by exposure to sunlight may also be due to thermal effects at high
irradiances or to photochemical effects at lower irradiances. In various animals, continuous
exposure to sunlight produces a photochemical lesion involving the entire retina and
affecting both rods and cones (Young, 1988). The photopigment, rhodopsin, is the chromo-
phore for damage to the rods, while the three cone pigments are the chromophores for cones.
In monkeys, blue-lighfdamage caused by exposure to the 400-500 nm waveband affected the
macular or paramacular region of the retinal pigment epithelium. The chromophore
involved has been postulated to be melanin; active species of oxygen appear to act as
mediators of the photochemistry (Lerman, 1980; Andley, 1987).
(c) Comparison of humans and animals
The limited data available indicate that the optical properties of the components of
human and animal eye are broadly similar.
4.3 Photoproduct formation
4.3.1 DNA photoproducts
OTHER RELEVANT DATA 185
A multitude of photoproducts are formed in cellular DNA by solar UVR, many of which
were first recognized after their induction by non-solar radiation at a wavelength of 254 nm.
The ratio of the different photoproducts changes markedly with wavelength. A brief
description of the photoproducts is given below, together with a note on the wavelength
dependence of formation and susceptibility to repair. Substantial information on biological
consequences is available only for cyclobutane-type pyrimidine dimers and pyrimidine-
pyrimidone (6-4) photoproducts.
(a) Cyclobutanetype pyrimidine dimers
Shortly after the observation that thymine compounds irradiated with UVC in the frozen
state rapidly lose their absorption (Beukers et al., 1958), a dimer of thymine was shown to be
responsible for this effect, the two molecules being linked by a cyclobutane ring involving the
5 and 6 carbon atoms (Beukers & Berends, 1960; Wulff & Fraenkel, 1961). Continued
irradiation leads to a wavelength-dependent equilibrium between dimer formation and
dimer splitting to reform the monomer. Dimer formation is favoured when the ratio of dimer
to monomer absorbance is relatively small (wavelengths > 260 nm), whereas monomeri-
zation is favoured at shorter wavelengths (around 240 nm), when the ratio is larger (Johns
et al. , 1962). Although several isomers of the cyclobutane-type thymidine dimer have been
isolated from irradiated thymine oligomers, only the cis-syn isomer appears to predominate
in biological systems (Ben-Hur & Ben-Ishai, 1968; Varghese & Patrick, 1969; Banerjee etal.,
1988).
Cytosine- thymine (cyt+-+thy), thyrnine+-+thyrnine (thy .... thy) and cytosine-cytosine
(cyt+-+cyt) cyclobutane-type dimersare also formed in irradiated Escherichia coli DNA but
deaminate to uracil+-+thymine (ura+-+thy) and uracil- uracil dimers after the acid hydrolysis
usually used in chromatographic analysis (Setlow & Carrier, 1966). Cytosine moieties in
dimers are also deaminated at a slower rate under physiological conditions that produce
uracil residues (Fix, 1986), and recent evidence obtained in bacteria suggests that the rate
may be more significant than was previously thought (Tessman & Kennedy, 1991). After
treatment at 254 nm, thy+-+thy, cyt+-+thy and cyt+-+cyt appear in irradiated DNA at a ratio of
2:1:1 (U nrau eta/., 1973), but this ratio changes quite markedly at longer wavelengths, e.g., to
5:4:1 at 265 nm (Setlow & Carrier, 1966). At 254 nm, the relative proportion of cyclobutane
dimers was: 5'-thy+-+thy, 0.68; 5'cyt+-+thy, 0.17; 5'-cyt+-+thy, 0.08; and 5'-cyt+-+cyt, 0.07
(Kraemer et al., 1988). Ellison and Childs (1981} showed in E. coli that the ratio of
cyt+-+thy:thy+-+thy increases from 0. 75 at 254 nm to 1.5 at 313 nm then decreases to 0.8 at 320
nm, the longest wavelength tested. At 365 nm, the longest wavelength at which dimers have
been detected, the ratio of thy+-+thy:ura+-+thy was 5-6:1 ('JYrrell, 1973). The proportion of
cyt+-+cyt:thy+-+thy increased up to 300 nm, but cyt+-+cyt was undetectable at longer wavelengths
(Ellison & Childs, 1981). On the basis of these data, the latter authors argued that the
predominant dimer species formed in E. coli by exposure to sunlight are likely to be mixed
dimers of cyt+-+thy rather than thy.-.thy (cyt+-+thy:thy+-+thy, 1.2:1). The ratio of formation of
thy+-+thy:ura+-+thy dimers in bacterial DNA at 254 and 365 nm is approximately 7 x lOS nm
.-- ..
---- ------
186 IARC MONOGRAPHS VOLUME 55
(Tyrrell, 1973). A similar ratio of total dimer product formation was found in cultured human
skin fibroblasts irradiated at 254-265 nm (Enninga et a/., 1986).
Fisher and Johns (1976) described the photochemistry and mechanism of formation of
cyclobutane-type pyrimidine dimers in considerable detail. The mechanism of dimer
formation in the UVB region almost certainly involves direct absorption, since the action
spectrum for induction closely resembles that for the appropriate monomer for wavelengths
as long as 313 nm (Ellison & Childs, 1981). The mechanism of formation by longer wave-
lengths (e.g., 365 nm) has not been clarified.
Cyclobutane-type dimers can be removed from the DNA of both prokaryotic and
eukaryotic cells by the powerful excision repair mechanism that is deficient in cells from most
sun-sensitive, skin cancer-prone patients with the hereditary disease, xeroderma pigmen-
tosum (see Friedburg, 1984; Cleaver & Kraemer, 1989). Photoreactivation is specific for
pyr+-+pyr (pyrimidine dimers) and monomerizes them in situ via a photolyase. Many micro-
organisms and higher eukaryotes contain a photolyase, but the proteins and light-activation
spectra differ from species to species. The specificity of this process has proved a powerful
tool in analysing the role of pyr+-+pyr in biological effects. For example, the potential
photoreactivation of pyr+-+pyr has been studied in a set of experiments to demonstrate that
the presence of UVC-induced pyr+-+pyr in fish can be a precarcinogenic lesion (Setlow, 1975).
More recently, the small opossum, M. domestica, has been used by Ley and coworkers as an
animal model in studies on the effects of UVR, predominantly UVB, mainly because celJs of
the skin of this animal, unlike that of the mouse, contain a photoreactivating enzyme(s). They
showed that several biological effects, including decreased hair growth, erythema and
tumour formation, were suppressed by exposure to longer wavelengths (photoreactivating
light} (Ley & Applegate, 1989; Ley eta/., 1991).
Considerable evidence, including the fact that photoreactivation prevents formation of
the majority of mutations induced in bacteria by UVC, shows that the argument that pyr+-+pyr
is a major premutagenic lesion is overwhelming (Doudney, 1976). Recognition that UV-
induced mutagenesis in bacteria is an inducible process (see Witkin, 1976), however, compli-
cates this argument, since, assuming that a structure involving pyr++pyr constitutes the
inducing event, its elimination by photoreactivation would preclude error-prone repair at the
site of any premutagenic lesion. When all inducible functions relevant to mutagenesis are
turned on, the photoreversibility of UVC mutagenesis at several pyr++pyr sites disappears
(Bridges & Brown, 1992); e.g., UV-induced mutagenesis to his+ in certain recA441/exA51
bacteria was not photoreversible, indicating that pyrimidine dimers are not target lesions
(Ruiz-Rubio et al., 1986). This suggests that non-photoreversible photoproducts (such as the
pyrimidine-pyrimidone 6-4 photoproduct) are the principal premutagenic lesions at dithy-
mine sequences and that cyclobutane-type thymine dimers are weakly mutagenic. This
conclusion is consistent with the results of other studies with single-stranded vector DNA
containing cyclobutane-type (6-4) thy-thy photoproducts at specific sites (Banerjee et al.,
1988, 1990; LeClerc eta/., 1991).
(b) Pyrimidine-pyrimidone (6-4) photoproducts
The most extensively studied non-dimer photoproduct is that formed from thymine and
cytosine. Indirect evidence (Varghese & Patrick, 1969) suggests that this structure is the
OTHER RELEVANT DATA 187
in-vivo precursor of the compound 6-4 '-[pyrimidin-2 '-one ]thymine (thy( 6-4 )pyo ), originally
found in acid hydrolysates of UV-irradiated DNA (Varghese & Wang, 1967; Wang &
Varghese, 1967). Some years later, a type of UV-induced photoproduct, the pyrimidine
nucleoside-cytidine lesion, was recognized in highly reiterated sequences of human DNA
(Uppke et al., 1981); this is also probably a precursor of the thy(6-4)pyo product (Brash &
Haseltine, 1982; Franklin eta/., 1982). Using DNA sequencing analysis, UV photoproducts
were more frequent at the 3' end of pyrimidine runs. Although the overall ratio of 6-4 photo-
products to dimers was 15% at certain 5'-thy+-+cyt sequences, 6-4 photoproducts occurred at
approximately the same frequency as that of the cyclobutane dimer (Kraemer et al., 1988).
Patrick (1977) originally reported that the action spectrum for (6-4) photoproduct
formation resembles that for cyclobutane dimer formation, although the quantum yields are
two and ten times lower than that of cyt+-+thy and thy+-+thy formation, respectively. Using
irradiation at wavelengths as long as 334 nm, Chan et a/. (1986) found that the action
spectrum for induction of hot alkali sites (presumably the thy(6-4)pyo hydrolysis product)
was also similar to that for pyr .... pyr formation. The action spectra for the induction of
thymine dimers and (6-4) photoproducts were similar from 180 to 300 nm, whereas the action
spectrum values for thymine dimer induction were about nine and 1.4 times higher or more
than the values for (6-4) photoproduct induction below 160 nm and above 313 nm,
respectively (Matsunaga eta/., 1991).
Most xeroderma pigmentosum patients are defective in the excision of (6-4) photo-
products (Mitchell eta/., 1985) and cyclobutane pyrimidine dimers (Cleaver & Kraemer,
1989). In addition, a group of patients with trichothiodystrophy (type 3) showed a marked
reduction in the repair of (6-4) photoproducts (Broughton eta/., 1990).
Glickman et al. (1986) demonstrated in E. coli that the cytosine- cytosine pyrimidine-
pyrimidone (6-4) photoproduct is highly mutagenic; however, in other studies (e.g.,
Hutchinson et al., 1988), cyclobutane dimers were shown to be responsible for the majority of
observed mutations. Assessment of the relative contributions to mutagenesis of all dipyri-
midine photoproducts will require comprehensive studies in different biological systems with
specifically designed sequences containing the appropriate photoproducts. Both pyrimidine
dimers and pyrimidine- pyrimidone (6-4) photoproducts appear to be important in inducing
cytotoxic and mutagenic lesions in human cells, although the relative contributions of each
type remain controversial (Mitchell, 1988).
(c) Thymine glycols
A group of monomeric ring-saturated lesions of the 5,6-dihydroxydihydrothymine type
(thymine glycols) have been detected by alkaline- acid degradation in the DNA of UV-
irradiated human cells (Hariharan & Cerutti, 1976, 1977). Alkaline-acid degradation (see
Cerutti, 1981) can be used to detect a dass of structurally related lesions rather than a single
lesion, with a yield that has been estimated to be approximately 20% of the total of ring-
saturated thymine products (tsat)
Two aspects of this class of UV photoproduct are of particular interest: firstly, they are
closely related to a class of ionizing radiation products and are believed to arise through a
similar mechanism, i.e., indirectly via the action of hydroxyl radicals; secondly, their yield
(relative to that of other UV-induced base damage) increases with exposures in the UVB
188 IARC MONOGRAPHS VOLUME 55
region. Measurements in HeLa cells showed that at 265 nm the ratio ofthy .... thytotsat was 21,
whereas at 313 nm the ratio decreased to 1.3 (Cerutti & Netrawali, 1979). The saturated
thymine damage induced by UVA and UVB radiation may thus be due to the effects of active
oxygen species generated via endogenous cell components. There is little evidence per-
taining to the lethal or other biological consequences of such lesions in mammalian cells,
although a glycosylase capable of repairing these lesions has been isolated from human cells
(Higgins et al., 1987).
(d) Cytosine damage
The photochemical induction of pyrimidine hydrates has been reviewed (Fisher &
Johns, 1976). Significant levels of hydrates are probably formed initially by UVR; however,
their instability hampers measurement of their induction and removal in cells, and it has not
been possible to establish a cause-and-effect relationship between photohydrate induction
and biological effects in vivo. Using sequencing techniques, Gallagher eta/. (1989) observed
incision by human endonucleases of unidentified cytosine photoproducts that were neither
cyclobutane-type nor (6-4) pyrimidine dimers. The frequency of these two photoproducts
was two orders of magnitude lower than that of pyrimidine dimers, and the optimal wave-
lengths for induction were between 270 and 295 nm.
(e) Purine damage
Purine damage has been studied less frequently than pyrimidine damage, since the
quantum yields are at least one order of magnitude lower; however, the development of
sequencing techniques has made their detection easier (Kumar et al., 1991). Incisions
(endonuclease V) are detected at unidentified purine or purine-pyrimidine moieties after
broad-spectrum UV irradiation (Gallagher & Duker, 1986). Such damage appears to be
induced maximalJy in the wavelength region of 260-300 nm (Gallagher & Duker, 1989).
Although the overall yield is much lower than that of pyr .... pyr, similar yields occur at certain
loci.
(f) DNA strand breaks
UVC radiation induces a lower proportion of single-strand breaks than of other photo-
products. In contrast, strand breaks are the commonest initial lesion induced by ionizing
radiation. Although strand breaks form only a minority of lesions after irradiation at wave-
lengths up to 365 nm, they become increasingly important at longer wavelengths in the solar
UV region (290-400 nm). At 313 nm, the ratio of DNA strand breakage to pyr .... pyr induc-
tion in intact E. coli was 1:44 (Miguel & Tyrrell, 1983), whereas at 365 nm one strand break
was formed for approximately every two pyrimidine dimers (TyrrelJ et al., 1974). An action
spectrum for break induction in Bacillus subtilis DNA in vivo is available (Peak & Peak,
1982). More recently, an action spectrum for single-strand breaks in human skin cells has
been determined which shows that irradiation in the presence of deuterium (which enhances
singlet oxygen lifetime) increases the number of strand breaks observed at 365 and 405 nm.
At wavelengths of 405 nm and longer, strand breaks and DNA-protein cross-links are the
only forms of photochemical damage that have been determined (Peak eta/., 1987). Between
10 and 20% of the breaks induced at 365 nm are not frank breaks but rather alkali-labile
OTHER RELEVANT DATA 189
bonds which presumably include apurinic and apyrimidinic sites (Ley et al., 1978; Peak &
Peak, 1982). The formation of breaks is strongly dependent upon oxygen at both 313 (Miguel
& Tyrrell, 1983) and 365 nm ('JYrrellet al., 1974; Peak & Peak, 1982). Their formation in vitro
at 365 nm is also quenched by free-radical scavengers. Strand breaks are repaired rapidly by a
variety of cellular mechanisms in both prokaryotes and eukaryotes. The role of these lesions
in the biological action of solar radiation is not well understood (1Yrrell eta/., 1974).
(g) . DNA-protein cross-links
The photochemical addition of nucleic acids to amino acids and proteins both in vitro
and in vivo has been the subject of several reviews (Smith, 1976; Shetlar, 1980). Of the 22
common amino acids, 11 undergo photochemical addition to labelled uracil, the most
reactive of which is cysteine, and several heterophotoproducts involving cysteine have been
isolated and characterized.
Several prokaryotic and eukaryotic proteins have been cross-linked photochemically to
DNA in vitro, including DNA polymerase, RNA polymerase, helix destabilizing protein and
mixtures of proteins (Shetlar, 1980).
There is evidence that DNA-protein cross-links are formed in mammalian cells in
significant yields by wavelengths longer than 345 nm {Bradley et al., 1979; Peak & Peak,
1991). Action spectra for the formation of DNA- protein cross-links in human cells have now
been obtained. Two peaks of induction are observed: one at 254-290 nm, corresponding to
the peak of DNA absorption, and a second at 405 nm, presumably resulting from a photo-
sensitization reaction (Peak et a/., 1985). [The Working Group noted that DNA- protein
cross-links are likely to have important consequences for cells, but no data are available to
allow evaluation of their effects in eukaryotic cells.]
4.3.2 Other chromophores and targets
In addition to DNA. many other cellular components absorb and/or are damaged by
solar UVR and may influence the biological outcome of exposure. Both informational and
transfer RNA molecules are susceptible to photomodification. Studies in insects indicate
that damage to messenger RNA may be relevant to embryonic development, but the rele-
vance of these results to mammalian systems is unclear (Kalthoff & Jackie, 1982). Detailed
results of bacterial studies on the photolability of certain components of transfer RNA
(Jagger, 1981) are almost certainly not relevant to mammalian cells. Damage to proteins
could lead to modification of the level of persistent primary damage in DNA, such that
cellular DNA repair and antioxidant pathways are compromised (Tyrrell, 1991 ). There is also
evidence that components of electron transport and oxidative phosphorylation, as well as
membranes and membrane transport systems, can be damaged by solar wavelengths (Jagger,
1985). Non-DNA chromophores and targets become particularly relevant at longer wave-
lengths.
(a) Chromophores
Both nucleic acids and proteins weakly absorb UVA, and, although direct photo-
chemical events may occur, it appears likely that the initial event in the biological effects of
UVA radiation is absorption by a non-DNA chromophore which results in generation of
190 IARC MONOGRAPHS VOLUME 55
active oxygen species or energy transfer to the critical target molecules. As a consequence, at
long UV wavelengths, the range of targets is extended to all critical molecules that are
susceptible to active intermediates generated by chromophores.
Most of the knowledge on relevant chromophores has been obtained from in-vitro
experiments or from studies in bacteria (Eisenstark, 1987). Indirect evidence indicates that
porphyrins play a role in the inactivation of Propionibacterium acnes by UVA (Kjeldstad &
Johnsson, 1986). It has also been shown that E. coli mutants defective in the synthesis of
8-aminolaevulinic acid are resistant to inactivation by UVA (Thveson & Sammartano, 1986),
which strongly suggests that porphyrin components of the respiratory chain act as endo-
genous photosensitizers. This conclusion is supported by the finding that strains that over-
produce cytochrome were sensitive to broad-band UVA radiation (Sammartano & Thveson,
1987). Porphyrins are also essential to human cellular metabolism, and overproduction of
iron-free porphyrins in erythropoietic or hepatic tissues is the underlying cause of the photo-
destruction of the skin seen in the group of diseases known as porphyrias. Although direct
evidence is lacking, free porphyrins and proteins containing haem (such as catalase,
peroxidases and cytochromes) are also potentially important chromophores in skin cells
from normal individuals. Many other cellular compounds which contain unsaturated bonds,
such as flavins, steroids and quinones, should also be considered potential chromophores.
Although normal levels of catalase (which contains haem) and alkyl hydroperoxide reductase
(which contains FAD) would be expected to exert a protective role in bacteria (see below),
overproduction of these enzymes is correlated with an increase in sensitivity to UVA
radiation in bacteria (Kramer & Ames. 1987).
Porphyrins are an important dass of photodynamic sensitizers which are believed to
~ x r t their biological action via the generation of singlet oxygen. Recent experiments have
shown that deuterium oxide (which prolongs the lifetime of singlet oxygen) sensitizes human
fibroblast cell populations to the lethal action ofUVA radiation, while sodium azide (which
destroys singlet oxygen) protects them (1}rrrell & Pidoux, 1989). AJthough this finding is
consistent with the involvement of porphyrins in the lethality of UVA, other cellular
compounds may also generate singlet oxygen . .It is also important to consider active oxygen
species that may be generated intracellularly. Not only can hydrogen peroxide be generated
by UVA irradiation of tryptophan (McCormick eta/., 1976), but both superoxide anion and
hydrogen peroxide can be generated by photo-oxidation of NADH and NADPH
(Czochralska et al., 1984; Cunningham eta/., 1985).
The presence of chromophores (such as psoralens) in the diet may also influence
susceptibility to damage, bt1t this reaction is clearly subject to enormous individual varia-
bility. Accidental and deliberate application of chemical agents (such as sunscreens and
drugs) to the skin may also introduce potentially damaging chromophores.
(b) Membranes
The lipid membrane is readily susceptible to attack by active oxygen intermediates.
Many reports (e.g., Desai eta/., 1964; Roshchupkin et al., 1975; Putvinsky et al., 1979; Azizova
eta/., 1980) have shown that UVR can induce peroxidation of membrane lipids. In-vitro
studies with lecithin microvesicles have shown UVR-induced changes in the microviscosityof
membrane bilayers (Dearden eta/., 1981) which are correlated with the degree of unsatu-
OTHER RELEVANT DATA 191
ration of fatty acid chains (Dearden et al., 1985}. UVC and UVA radiation and sunlight have
been shown to cause lipid peroxidation in the liposomal membrane (Mandai & Chatterjee,
1980). Haem proteins such as cytochrome c and catalase are known to catalyse lipid permo-
dation and peroxidative breakdown of membranes (e.g., Brown & Wuthrich, 1977; Go iii
eta/., 1985; Szebeni & Tollin, 1988). A dose-dependent, linear increase in lipid peroxidation
of liposomal membranes was induced by UVA radiation, which was inhibited to a large
extent by butylated hydroxytoluene, a nonspecific scavenger of lipid-free radicals. Since both
sodium azide and L-histidine (quenchers of singlet oxygen) led to 40-50% inhibition of
peroxidation, the authors suggested that singlet oxygen is involved in initiation of the
reaction (Bose et al., 1989).
UVA irradiation of liposomes leads to lipid peroxidation in the absence of photo-
sensitizer molecules, so that singlet oxygen may arise through direct stimulation of molecular
oxygen (Bose et al., 1989). Biological membranes are, however, rich in endogenous photo-
sensitizer molecules, such as those involved in electron transport, and these may contribute
to the peroxidation of lipids observed in biological systems (see Jagger, 1985). Membrane
damage has long been implicated in the lethality of UVA in bacteria (Hollaender, 1943) and
almost certainly contributes to the sensitivity of UVA-treated populations plated on minimal
medium-a phenomenon which is highly dependent on oxygen (Moss & Smith, 1981).
Sensitivity to UVA has been related to levels of unsaturated fat in membranes (Klamen &
Thveson, 1982; Chamberlain & Moss, 1987). Furthermore, the presence of deuterium oxide
enhances the levels of membrane datnage, sensitivity to UVA and lipid peroxidation
(Chamberlain & Moss, 1987), suggesting that singlet oxygen plays a role in all three pro-
cesses. Leakage experiments have also been used to assess UVA-induced membrane damage
in yeast: again, changes in permeability correlated well with lethality and were highly oxygen
dependent (Ito & Ito, 1983). UVA irradiation of cultured human and mouse fibroblasts led to
the release of arachidonate metabolites from the membrane in a dose-dependent fashion.
The release was also dependent on the presence of both oxygen and calcium ion and may be
related to the induction of cutaneous erythema, which is also oxygen dependent {Hanson &
DeLeo, 1989). Studies of the effects of UVR on membrane transport have been undertaken
in prokaryotes (Jagger, 1985), but no information was available on the effects of UVR on
eukaryotic membrane transport.
4.4 Human excision repair disorders
4.4.1 Xeroderma pigmentosum
The commonest, most characteristic photoproducts produced in DNA by UVB and
UVC radiation involve adjacent pyrimidines. Evidence summarized above argues strongly
that these products give rise to a wide variety of alterations in DNA sequence and gene
expression. like many other types of DNA damage, these photoproducts may be excised, and
the resulting gap in one strand can be resynthesized accurately using the undamaged strand
as a template. How this is accomplished is best understood in the bacterium E. coli, in which a
multiprotein complex including the products of the uvrA, Band C genes excises an oligo-
nucleotide 12 or 13 bases in length containing the photoproduct. The resulting gap is filled by
a DNA polymerase {usually ill}, and the final ligase link to the adjacent DNA is effected by
192 IARC MONOGRAPHS VOLUME 55
polynucleotide ligase (Bridgeset al., 1987; Bridges, 1988; Bridges & Bates, 1990). Other gene
products are involved in the process, and a more comprehensive discussion is given by Sa ncar
and Rupp (1983). Bacteria that have defects in the uvrA or B genes cannot excise UV
photoproducts and are 10-20 times more sensitive to killing and the induction of mutations
by UVC. They are also more sensitive to UVB and (under certain conditions) UVA (Webb,
1977). It can be concluded that the function of excision repair is to minimize the deleterious
consequences of DNA damage, such as the persistence of UV photoproducts.
A similar process takes place in humans. Although much less is known about the
mechanism, many genes have been shown to be involved, and these are being cloned and the
role of their products is being elucidated (Hoeijmakers & Bootsma, 1990; Bootsma &
Hoeijmakers, 1991). Like bacteria, humans can also be deficient in aspects of excision repair.
The prototypic example is the genetic disorder xeroderma pigmentosum, which is actually a
complex of disorders comprising at least 10 different forms of DNA repair defect (nine
excision defective complementation groups and one excision repair proficient variant group)
(Kraemer eta/., 1987; Cleaver & Kraemer, 1989). The sensitivity of fibroblasts and lympho-
cytes from excision-defective individuals with xeroderma pigmentosum to mutation and
lethality by UVC is up to 10 times greater than that of cells from normal individuals (Arlett
eta/., 1992) and for UVR from a solar simulator (Patton et a!., 1984). The pigmentary
abnormalities are confined to sun-exposed portions of the skin.
The incidences of tumours of the skin, anterior eye and tip of the tongue in these
individuals are much higher than those in unaffected populations (Kraemer et al., 1987), and
the median age of patients at onset of skin cancers appears to be much younger than that of
the general population. Multiple primary skin cancers are common, which arise predo-
minantly on sunlight-exposed areas of the body (Kraemer et al., 1987); there is anecdotal
information that they are largely prevented if protection against exposure to sunlight is
afforded early in life (Kraemer & Slor, 1984). Studies of patients with excision-defective
xeroderma pigmentosum provide the strongest evidence that sunlight-induced photo-
products can result (in the absence of repair) in the genesis of basal-cell carcinomas,
squamous-cell carcinomas and melanomas and strongly support the contention that they can
also do so in normal individuals in whom repair is more efficient (although probably never
complete). The photoproducts that fail to be excised in xeroderma patients are known to be
produced in human skin, not only by UVC (used in most laboratory experiments with cells)
but also by UVB, particularly by wavelengths around 300 nm (Bridges, 1990; Athas el al.,
1991). Action spectra show that the difference in the cytotoxic action of UVB on cultured
cells from normal and xeroderma pigmentosum patients is similar to that of UVC, whereas
the differences in the response to UVA are only slight (Keyse eta/., 1983). The studies on
xeroderma pigmentosum i1lustrate that DNA repair is a major defence of the human skin
against the carcinogenic action of sunlight.
4.4.2 Trichothiodystrophy
The conclusions derived from studies of xeroderma pigmentosum have become more
complex with the availability of information on two related excision disorders. 'frichothip-
dystrophy is a rare disease in which patients generally have skin judged to be sun-sensitive by
erythemal response but no indication of the pronounced freckling or elevated incidence of
OTHER RELEVANT DATA 193
early skin tumours associated with xeroderma pigmentosum (Bridges, 1990). In the majority
of cases studied, trichothiodystrophy is associated with a deficiency in the ability to repair
UV-induced damage in cellular DNA
Three categories of response to UVR have been identified. In type 1, the response is
completely normal, whereas type-2 cells are deficient in excision repair, with properties
indistinguishable from those of xeroderma pigmentosum complementation group D.lYPe-3
cells survive normally after UV irradiation, and the rates of removal of cyclobutane pyri-
midine dimer sites are also normal (Broughton eta/., 1990). In xeroderma pigmentosum
diploid fibroblast lines, catalase activity was decreased on average by a factor of five as
compared to controls, while heterozygotic lines exhibited intermediary responses. All tricho-
thiodystrophy lines tested were deficient in UV-induced lesion repair and exhibited a high
level of catalase activity; however, molecular analysis of catalase transcription showed no
difference between normal, xeroderma and trichothiodystrophy cell lines. UV irradiation
induces five times more hydrogen peroxide production in xeroderma lines than in trichothio-
dystrophy lines and three times more than in controls. These striking differences indicate that
UVR, directly or indirectly, together with defective oxidative metabolism may increase the
initiation and/or the progression steps in patients with xeroderma pigmentosum to a greater
degree than in people with trichothiodystrophy, which may partly explain the different
tumoral phenotypes in the two diseases (Vuillaume et a/., 1992).
Five patients with trichothiodystrophy type 2 appeared to be in one of the xeroderma
pigmentosum complementation groups: Fibroblasts from these individuals were indistin-
guishable from xeroderma fibroblasts in the same complementation group and were equally
sensitive to the lethal and mutagenic effects of UVC (Stefanini eta/., 1986; Lehmann eta/.,
1988). Two other trichothiodystrophy patients (type 3) had cells markedly defective in the
removal of (6-4) pyrimidine photoproducts but not cyclobutane-type dimers (Broughton
eta/., 1990).
4.4.3 Cockayne 's syndrome
A third sun-sensitive excision repair disorder is Cockayne's syndrome. Patients with this
condition have fibroblasts which undergo normal excision repair in the overall genome but
which are defective in the excision of dimers from DNA strands undergoing active
transcription (Mayne eta/., 1988). Cockayne 's syndrome cells are sensitive to both killing and
mutation induction by UVC (Arlett & Harcourt. 1983) and have reduced repair of cyclo-
butane dimers; they show, however, normal repair of non-dimer photoproducts in a UV-
treated shuttle vector plasmid. Like patients with trichothiodystrophy, those with Cockayne's
syndrome do not have pronounced freckling or enhanced early incidence of skin cancers
(Barrett eta/., 1991).
4.4.4 Role of immunosuppression
If it is assumed that UV-induced DNA damage sustained by patients with trichothio-
dystrophy type 2 results in the same photo-induced mutations in their skin cells (including
mutations associated with the initiation of cancer) as is seen in xeroderma pigmentosum
patients of the same complementation group (D) (Bridges, 1990; Broughton eta/., 1990),
something other than unrepaired DNA damage and an elevated frequency of mutations must
be needed to trigger initiated cells into clonal expansion and early tumours, as is seen in
194 IARC MONOGRAPHS VOLUME 55
xeroderma pigmentosum. The assumed latency of initiated cells in such trichothiodystrophy
patients may be related to the latency seen in epidemiological studies of skin cancer in the
normal population (see section 2).
The nature of the circumstances that allow initiated skin cells to develop into tumours in
xeroderma pigmentosum patients, and perhaps later in life in other individuals, is unclear.
Burnet (1971) first suggested that individuals with this disorder might be deficient in some
immunosurveillance step. Bridges (1990) proposed that they were also hypersensitive to both
the immunosuppressive and the mutagenic action of UVR, so that the elevated skin cancer
rate in individuals with xeroderma pigmentosum would not accurately reflect the actual
increase in mutation frequency in exposed skin but would exaggerate it greatly.
4.5 Genetic and related effects
Any cell that is UV-irradiated can be expected to sustain DNA damage. The nature of
this damage is wavelength-dependent, and the major photoproducts of short-wavelength UV
irradiation are various types of dipyrimidine photoproducts, while DNA strand breakage and
DNA-protein cross-linkage occur relatively more frequently after irradiation with long-
wavelength UVR. As the wavelength is increased above 290 nm, the efficiency of formation
of pyrimidine dimers and other DNA photoproducts decreases greatly. This wavelength-
dependency of response presents a fundamental problem for the quantitative interpretation
of the genetic activities of different regions of the UV spectrum. In most experimental studies
with UVA and UVB irradiation and, of course, simulated solar radiation, monochromatic
radiation was not used. Also, the characteristics of the radiation emitted from the source are
variable over time and from source to source. Because of these practical considerations,
comparisons of the effects seen in different studies in terms of dose are commonly invalid:
Photoproduct yield is dependent on the energy contributions from the different wavelengths
within the spectrum used, but incident doses (tluences) are measured only as energy fluxes
over the whole spectrum emitted from the source. The problem of dosimetry within
experimental systems is compounded by the fact that absorbed dose is determined by the
geometry of the system and the position of the target within it: absorption by one layer (e.g.,
the medium or a layer of cells) will affect the tluence incident upon the layer beneath. The
tluence absorbed may thus differ substantially from the incident fluence of the system. For
these reasons, it was considered inappropriate to compile quantitative genetic profiles as is
customary in these monographs.
Given the generally significant responses in many different tests for the genetic activity
of UVR in a wide range of organisms and cultured cells, the simple qualitative questions
appear to have been answered in abundance. The main issues of outstanding interest are:
identification of the types of damage induced by the various portions of the UV spectrum; the
mechanisms by which damage is translated into mutation or other genetic changes; and the
dose characteristics of these responses.
4.5.1 Humans
The portions of the body that receive most exposure to UVR are the skin, anterior eye
and lip. Because dermal capillaries approach ~ skin surface, it can be anticipated that blood
OTHER RELEVANT DATA 195
will be exposed to the portion of UVR (see Kraemer & Weinstein, 1977; Morison et al.,
1979a; Larcom eta/., 1991) that penetrates the dennis. The biological consequences of this
exposure are unknown.
DNA damage in skin cells has been studied using three methods that are sensitive
enough to detect DNA damage after exposure to doses of UVR too low to induce erythema:
(i) use of antibodies specific for UV-altered DNA, followed by immunofluorescence.
This method can be used with immunoperoxidase staining and a secondary anti-
body {Eggset et al., 1983, 1986) or without them (Th.n & Stoughton, 1969);
(ii) autoradiography after tritiated thymidine incorporation (Epstein eta/., 1969, 1970;
Honigsmann et al., 1987; Wolf et al., 1988); and
(iii) treatment of extracted DNA with Micrococcus luteus cyclobutyl pyrimidine dimer
site-specific endonuclease, followed by alkaline agarose gel electrophoresis of the
single-stranded DNA fragmented at the dimer sites (Sutherland et al., 1980;
D'Ambrosio et a/., 1981; Gange eta/., 1985; Freeman et al., 1986, 1987, 1989;
Alcalay eta/., 1990). This method suffers the disadvantage that damage cannot be
localized to particular layers of the skin, but dimeryield can be calculated. Methods
for the study of resolved genetic damage have not been pursued.
(a) Epidermis
{i) Broad-spectrum ultraviolet radiation, including solar simulation
Effects on DNA synthesis were demonstrated in human skin in vivo which had been
exposed to three times the MED of UVR ( < 320 nm; mercury arc lamp [Fig. 9a, p. 64]) and
then injected intradermally with tritiated thymidine (8-41 x 10
6
ergs/cm
2
[8-41 kJ/m
2
]) in
the irradiated area immediately and at 0.25, 3, 5 and 24 h subsequently. S Phase was
suppressed in cells of the basal layer at 3-h and 5-h sampling times, but not at 24 h. Sparsely
labelled cells (indicating DNA repair) occurred in greatly variable proportions from person
to person in the basal, malpighian and granular layers at 0, 0.25, 3 and 5 h, but not at 24 h,
indicating that repair was complete by 24 h (Epstein eta/. , 1969). DNA repair was also
reduced in the skin cells of three patients with xeroderma pigmentosum in comparison to
eight normal controls (Epstein et al., 1970).
Sutherland et al. {1980) demonstrated a dose-related response for the induction of pyri-
midine dimers after exposure to a Westinghouse sun lamp (Fig. 9c, p. 64), with 50% energy
< 320 nm, at 0, 970, 1940 and 3880 J/m
2
In one subject, 0.5 of the MED of sun-lamp
exposure resulted in about 6 0.6 dimers per lOS Da.
D'Ambrosio et al. (1981) reported that approximately 12.8 and 23.6 dimers per lOS Da
were induced in skin DNA in vivo following irradiation with a mercury arc lamp (200-450
nm) at 150 and 300 J/m
2
, respectively. Repair or removal of dimers was measured 0-24 h
following exposure. About 50% of the dimers were lost 58 min after irradiation, and less than
10% remained at24 h. In an experiment with patients with lupus erythematosus, D'Ambrosio
eta/. (1983) obtained results similar to those found in the skin of normal individuals.
Strickland et a/. {1988) measured the induction of cyclobutane dithyrnidine photo-
products in human skin samples after exposure to simulated solar radiation. Tissue samples
from three non-pigmented (white) individuals were exposed to 18 or 36 kJ/m
2
UVR (0.5-1
MED), and those from three constitutively pigmented (black) individuals were exposed to 72
1% IARC MONOGRAPHS VOLUME 55
and 144 k11m
2
Constitutively pigmented skin required doses of UVR two to four times
higher than non-pigmented skin to produce roughly equivalent levels of thymine dimers.
[The Working Group noted the small number of people studied.]
(ii) UVA radiation
Freeman et al. (1987) showed in two subjects that similar pyrimidine dimer yields were
produced in skin by a broad-band UVA source (UV ASUN 2000), by broadband UVA filtered
to remove all light of wavelengths < 340 nm and by narrow-band radiation centred at 365 nm
(xenon- mercury compact arc), indicating that UVA radiation and not stray shorter wave-
length radiation was responsible. Dimer production was observed following exposures to
5 x 10
5
11m
2
. Since exposure to a UVA-emitting tanning lamp results in a dose of about
5 x 10
5
11m
2
, UVA exposure for cosmetic purposes could result in measurable levels of DNA
damage.
(iii) UVB radiation
The efficiency of UVA- and UVB-induced tans in protecting against erythema and the
formation of dimers induced by UVB was studied in five subjects by Gange et al. (1985). The
radiation sources were a UVASUN 2000 lamp (UVA; Fig. 8d, p. 61) and an FS36 Elder
fluorescent sunlamp (UVB). UVB-induced tanning protected against erythema produced by
subsequent UVB exposure two to three times better than UVA-induced tanning; however,
tanning with either UVA or UVB was associated with a similar reduction in yield of
endonuclease-sensitive sites in epidermal DNA (about 50%).
Eggset eta/. (1983) observed DNA damage in both epidermis and dermis following
exposure to a Westinghouse FS-20 sunlamp (Fig. 9c, p. 64) at 0.5-2 MED (2 MED, 900 J /m
2
).
The outer layers were more heavily damaged after small doses than the basal layer, which
may be better protected by its deeper location and shielding by melanin. The authors claimed
that DNA repair was weJI under way after 4-5 hand was apparently nearly complete at 24 h,
as judged by immunofluorescence and immunoperoxidase staining. Repair was faster in the
presence of visible light than when irradiated skin was shielded with thick black plastic. [The
Working Group noted the absence of quantitative data.]
In a study of two volunteers (Eggset et al., 1986), tanning was shown to protect against
DNA damage in skin (induced in a UVB solarium), but the conclusions were based solely on
observations of immunofluorescence. [The Working Group noted the absence of quanti-
tative data.]
Freeman eta/. (1986) measured UVB-induced DNA damage in the skin of seven indivi-
duals with different sensitivities to UVB irradiation, as measured by the MED, with irra-
diation from an FS36 Elder fluorescent sunlamp (280- 320 nm). The production of dimers
was correlated inversely with the MED. The slopes of the dose-response curves for the most
UVB-sensitive individual (MED, 240 Jlm
2
) and for the least sensitive individual (MED, 1460
11m
2
) were 11.5 x 10-4 and 2.6 x 10-4 dimer sites per 1000 bases per mJ/cm
2
[10 J/m
2
],
respectively.
Honigsmann et al. (1987) studied unscheduled DNA synthesis in epidermal cells in the
skin of 25 male volunteers (four with skin type II and 21 with skin type III; see pp. 168- 169)
after exposure to doses of UVB of 0.06- 6 MED, from a 6-kW xenon arc lamp (292- 304 nm).
The MED values ranged from 140 to 550 J 1m
2
The dose- response curve showed a significant
OTIIER RELEVANT DATA 197
increase in unscheduled DNA synthesis between 0.06 and 1 MED but no difference between
1 and 6 MED, suggesting a saturation of excision repair in vivo.
Freeman (1988) studied interindividual variability in 17 healthy volunteers in the repair
of pyrimidine dimers induced following exposure to 0.25- 1.5 MED from a Westinghouse
FS-40 sunlamp (see Fig. 9c, p. 64). Removal of dimers was detected within 6 h of irradiation.
The average half-time for removal of dimers was 11.0 4.3 (SD) h (range, 5.5- 21.1 h). [The
Working Group noted that the spectra and doses used in this study were different from those
used by D'Ambrosio eta/. (1981). It is not clear if the interindividual variability is greater
than the experimental error.)
Interindividual variability in the repair of UVB-induced pyrimidine dimers was also
studied by Alcalay et a/. (1990) in 22 patients aged 31-84 with at least one basal-cell
carcinoma. The control group consisted of 19 cancer-free volunteers aged 25- 61. Both
groups were given one MED of radiation from a 150-W xenon arc solar UV-simulated lamp
equipped with a 50-cm liquid light guide and a filter eliminating wavelengths below 295 nm.
Dimers were measured immediately and after 6 h. The two groups were similar at time 0, but
after 6 h, 22 4% (range about 8-64) of the dimers were removed in the cancer group
compared to 33 4% {range about 4-64) in the control group. Of the cancer patients, 23%
had repaired more than 30% of the DNA damage, compared to 53% of the control group.
[The Working Group noted that it is not clear if the interindividual variability is greater than
the experimental error.]
Wolf eta/. (1988) observed measurable amounts of unscheduled DNA synthesis in the
skin of 23 volunteers exposed to 0.5 MED UVB irradiation from a high-pressure mercury
lamp [spectral emission not given]. Administration of carotenoids (to reduce light sensitivity
in patients with erythropoietic protoporphyria) at a dose of 150 mg per day for 30 days did not
significantly alter the amount of unscheduled DNA synthesis (6 1.2 grains/cell before and
8 2 grains/cell after carotenoid treatment; seven subjects). The same investigation showed
no significant protection by carotenoids against UVA-, UVB- or PUVA-induced erythema,
on the basis of pre- and post-carotenoid MED or minimal phototoxic dose.
In 30 volunteers, it was demonstrated that the action spectrum for the frequency of
pyrimidine dimer formation in human skin DNA for a given fluence (incident dose) has its
maximum near 300 nm and decreases sharply on either side of this wavelength {Fig. 12). The
decrease at < 300 nm is probably due to absorption in the upper layers of skin. These data
were used to estimate that, at a solar angle of 40 , a reduction in the thickness of the
stratospheric ozone layer from 0.32 em down to 0.16 em would be expected to result in a
2.5-fold ~ n c r e s e in dimer formation {Freeman et al., 1989).
A dose-response for the formation of thymine dimers in epidermal cells isolated from
human skin irradiated with UVB in vitro was determined by Roza et a/. (1988) using a
monoclonal antibody.
(iv) UVC radiation
Exposure of human skin, from which the stratum corneum had been removed, to either a
germicidal (UVC) or a . Hanovia hot quartz lamp in vivo resulted in DNA damage
demonstrable by immunofluorescence ('Thn & Stoughton, 1969). When the stratum corneum
was intact, DNA damage was detected only after exposure to the germicidal lamp. [The
198 IARC MONOGRAPHS VOLUME 55
Fig.12. Action spectrum for pyrimidine dimer formation in human skin ( ) and solar spectra
at the surface of the Earth for stratospheric ozone levels of0.32 em (dotted line) and 0.16 em
(solid line). Each point in the action spectrum represents the slope of the dose-response line
(dimer yields at three exposures) for one volunteer at one wavelength, obtained from tri-
plicate independent determinations. Thirty points occur at 302 nm, although some points
overlie other values; five points occur at each other wavelength: points at 290 and 334 nm are
circled to indicate that identical dimer yields were recorded for two volunteers. ph, photon;
ESS, endonuclease-sensitive site
Action spectrum (ESS/kb/ph/cm
2
x 10 19)
..
..
0
< ... :-
< r --------
m g --------------
<
::I
-...
::r
S'i
@
-
Solar flux (ph/cm
2
/s/nm x 10-
13
)
From Freeman er al. (1989)
Working Group noted that more sensitive analytical techniques for DNA damage are now
available.]
(b) Lymphocytes
(i) Broad-spectrum ultraviolet radiation
In addition to ceHs of the skin, white blood celJs are also subject to exposure to UVB and
UV A, partly because some are temporarily resident in the skin and partly because it has been
estimated that the equivalent of the total blood volume circulates through the dennal
capiHaries approximately every 11 min (Kraemer & Weinstein, 1977). Detecting effects, e.g.,
on lymphocytes, is likely to be extremely difficult owing to the fact that they are continually
moving between the blood and other tissues; indeed, 90% of the lymphocyte population at
any given time is resident outside the blood. Thus, the concentration in the blood of any
OTHER RELEVANT DATA 199
lymphocytes irradiated while passing through the skin may fall substantially over time after
irradiation ends as they are diluted in the whole body lymphocyte pool. Extravascular
lymphocytes resident in the skin may also receive higher doses ofUVR. Nevertheless, studies
have been reported of genetic or related effects on lymphocytes sampled from peripheral
blood.
Larcom eta/. (1991) examined the capacity for DNA synthesis oflymphocytes from eight
subjects exposed in two commercial tanning salons. Blood was taken immediately before
tanning and again 24 h after tanning. System I used a sunlamp with a UVB: UVR ratio of
0.02% for 280-300 nm and 1.4% for 300-315 nm; the output of system II (Solana Voltarc
lamp) was not indicated. There was a 24-84% (average, 53%) decrease in phytohaemag-
glutinin-induced DNA synthesis with system I and a 8- 58% (average, 30%) decrease with
system II.
(ii) UVA radiation
Seven of 13 psoriasis patients receiving oral 8-methoxypsoralen and high-intensity,
long-wave UVA radiation had reduced leukocyte DNA synthesis; this did not occur in any of
10 controls (Kraemer & Weinstein, 1977}. These results indicate that UVA reduces the
incorporation of tritiated thymidine in lymphocytes circulating through the skin.
(iii} UVB radiation
In normal, fair-skinned subjects given whole-body exposure to 1.5-3 x MED doses of
UVB from a sunlamp (280- 380 nm), a dose-dependent decrease was seen in the incorpo-
ration of tritiated thymidine into DNA following stimulation by photohaemagglutinin; the
proportion of circulating lymphocytes was decreased and the proportion of null cells was
increased (Morison eta/., 1979a}.
These studies indicate that leukocytes should be included in any inventory of human cells
potentially exposed to solar radiation or artificial UVR.
4.5.2 Experimental systems [see Tables 32-35, in which exposures are separated according
to type of UVR]
(a) DNA damage
Inhibition of DNA synthesis has been induced in hairless albino mouse epidermis at
wavelengths of 260-320 nm, with a maximal effect at 290 nm. Inhibition was not detected at
335 nm (Kaidbey, 1988). The action spectrum was similar to that for formation of cycle-
butane-type pyrimidine dimers (Cooke & Johnson, 1978; Ley eta/. , 1983) and pyrimidine-
pyrimidone (6-4) photoproducts in mouse skin (Olsen et al., 1989). Pyrimidine dimers
(measured as endonuclease-sensitive sites} have been measured in the corneal DNA of the
marsupial, M. domestica, following exposure to a sunlamp (280-400 nm} (Ley et al., 1988}.
While DNA is the main photochromophore for UVC, there is evidence that active
oxygen intermediates are involved in the production of DNA damage by UVA (Tyrrell, 1991).
The production of several types of photolesions is oxygen dependent ('J:Yrrell, 1984, 1991). In
addition, the irradiation lethality of both cultured bacterial (Webb, 1977) and mammalian
(Danpure & 'JYrrell, 1976} cells is dependent on the presence of oxygen; this observation was
later linked with the production of singlet oxygen (Tyrrell & Pidoux, 1989). It has also been
200 IARC MONOGRAPHS VOLUME 55
observed that irradiation of cultured human skin cells with UVB (302 nm, 313 nm), UVA
(334 nm, 365 nm) and visible ( 405 nm) radiation is strongly enhanced in glutathione-depleted
cells (1Yrrell & Pidoux, 1986, 1988). This apparent protection by glutathione appears to be
due to its radical scavanging properties at the stated wavelength but may be due to induction
of a more specific pathway (such as its essential role as a hydrogen donor for glutathione
peroxidase) at longer wavelengths. Francis and Giannelli (1991) found that the abnormally
high yield of single-stranded DNA breaks produced by UVA in six UVA-sensitive human
fibroblasts (three from actinic reticuloid patients, two from sisters with familial actinic
keratoses and internal malignancies and one from a patient with an abnormally high
incidence of basal-cell carcinomas) could be reduced if sensitive cells were co-cultivated with
normal fibroblasts or with radical scavengers. They suggested that the UV A-sensitive cells
had deficits of small-molecular-weight scavengers of active oxygen species and that inter-
cellular cooperation allows the transfer of these substances from resistant to sensitive cells.
The presence of non-DNA chromophores that generate active oxygen species can also occur
with UVC. Melanin, normally regarded as a solar screen, has also been associated with the
formation of oxidative DNA damage, such as thymine glycols in mouse cells that vary in
melanin content (Huselton & Hill, 1990). A slight increase in pyrimidine dimer yield was
seen in human melanocytes as compared to keratinocytes following exposure to UVR at 254, .
297, 302 and 312 nm but was significant only at 297 nm (Schothorst et al., 1991).
(b) Mutagenicity
Numerous reports show that sunlight or solar-simulated radiation induces mutations in
bacteria, plants, Chinese hamster ovary (CHO) and lung (V79) cells, mouse lymphoma cells
and human skin fibroblasts.
Studies in bacteria exposed to radiation throughout the solar UV spectrum (reviewed by
Webb, 1977) demonstrate mutagenic activity unambiguously. The effects of sunlight on
mammalian cells have been reviewed (Kantor, 1985). UVA (320- 400 nm) is mutagenic to
yeast and cultured mammalian cells, UVB (290-320 nm) to bacteria and cultured mam-
malian cells and UVC (200- 290 nm) to bacteria, fungi, plants, cultured mammalian cells,
including CHO and V79 cells, and human lymphoblasts, lymphocytes and fibroblasts. Since
wavelengths in the UVC range do not reach the surface of the Earth, they are of no signi-
ficance as a source of damage in natural sunlight.
A characteristic of all of these studies is that UVA appears to be relatively inefficient as a
mutagen in comparison with UVB and UVC when activity is expressed per unit of energy
fluence, but not necessarily so when expressed per DNA photoproduct {see Tyrrell, 1984).
Webb (1977) compiled action spectra for the introduction of mutations in bacteria, as did
Coohill et al. (1987) for mutagenesis in human epithelial cells. In both Salmonella and human
cells, wavelengths > 320 nm were at least 103 times less effective than those between 270 and
290 nm.
A comparison of the mutagenicity of various UV-containing light sources towards a set
of S. typhimurium strains was reported by De Flora eta/. (1990). The approach did not involve
measurement of cytotoxicity, and mutagenicity was compared at roughly equitoxic doses
rather than as a function of fluence. Halogen lamps were as mutagenic as 254-nm UVC and
more mutagenic than fluorescent sunlamps or.sunlight. The mutagenicity of halogen lamps
OTHER RELEVANf DATA 201
was attributed to their UVC component, in contrast to sunlight which produced mutagenic
effects over a wide UV spectrum. The mutagenicity of halogen lamps, fluorescent lamps and
sunlight was partially inhibited by catalase, suggesting that peroxides may be involved in this
in-vitro system. It is also relevant that pretreatment of E. coli with hydrogen peroxide results
in an increase in both UVA resistance and hydrogen peroxide scavenging ability {Moss, S.H.,
quoted by Tyrrell, 1985; Sammartano & Thveson, 1985; Tyrrell, 1985).
Further evidence for the complexity of responses to the UVR region comes from
Schothorst et aJ. ( 1987b ), who examined the mutational response of human skin fibroblasts to
12 lamps differing widely in their emission characteristics. Surprisingly, they found that,
whatever the light source, mutation induction per MED was similar with UVC, UVB and
solar radiation; with UVA (only one data point), mutation induction perMED was much
greater. The authors emphasized that these conclusions hold only if it is valid to calculate the
mutagenicity of a light source by adding the effects of the contributing wavelengths; however,
the data of Coohill et al. (1987) argue against this assumption.
The inevitable consequence of the absorption spectrum maximum of DNA is that there
is a considerable body of data on mutagenicity toward microorganisms of UVC, which is
usually delivered by radiation from germicidal lamps with more than 90% of their output at
254 nm. The types of mutations that are induced by UVC and the mechanisms of their
induction have been reviewed (Witkin, 1976; Hall & Mount, 1981; Walker, 1984; Hutchinson
& Wood, 1986; Bridges eta/., 1987; Hutchinson, 1987). Specific cellular proteins, including
the products of recA and umuC genes, together with a cleaved derivative of the umuD gene
product, must be present for mutations to result from most types of DNA damage. These
proteins are themselves part of an inducible response to DNA damage. and their intra-
cellular level increases dramatically when photoproducts or other lesions are detected in
DNA It is not yet clear to what extent inducible systems are involved in UV mutagenesis in
higher eukaryotes.
Current evidence suggests that all photoproducts are likely to be potentially mutagenic,
although with greatly different specificities and potencies. The major UV photoproducts,
cyclobutane-type thymine-thymine dimers, are, for example, relatively weakly mutagenic
(Banerjee eta/., 1988, 1990). owing in part to the propensity of polymerases to insert adenine
when the template instruction is unclear or missing (Sagher & Strauss. 1983; Schaaper et al.,
1983; Kunkel, 1984). The relatively minor (6-4) thymine-thymine photoproduct is, in
contrast, highly mutagenic, the dominant mutation being a 3' T .... c transition (LeClerc et al.,
1991). By far the most frequent UVC-induced change in human cells is the transition from
G:C to A:T (Bredberg eta/., 1986; Seetharam eta/., 1987; Hsia eta/., 1989; Dorado et al.,
1991). A number of investigators have noted the production of tandem transitions from
G:C,G:C to A:T,A:T. Although this is not the most frequent change, it seems to be particu-
larly characteristic for UVC mutagenesis in human cells. The frequency of mutation per
lethal event at the hprt locus (which detects a broad spectrum of mutations) is approximately
the same at 254 nm and 313 nm in human lymphoblastoid cells; however, the mutation
frequency per lethal event at the Na + /K + ATPase locus (which ~ e t e t s point mutations) is
considerably higher at 313 nm. This finding may indicate a difference in types of pre,.
mutagenic lesions and/or rates of mutation between the two wavelength regions (Tyrrell,
1984).
202 IARC MONOGRAPHS VOLUME 55
Two bacterial studies provide positive evidence for the mutagenic activity of fluorescent
lamps. De Flora et al. (1990) employed Sylvania 36 W cool white tubes with E. coli and
Salmonella strains. (The Working Group had difficulty in evaluating these data because they
are presented in a highly transformed format.] Hartman et al. (1991) used General Electric
F15T8CW lamps; a lowest effective dose of 5500 J /m
2
can be estimated from the results with
Salmonella tester strains. Filters that block wavelengths < 370 nm effectively eliminated
mutagenesis, while radical scavengers such as superoxide dismutase or catalase stimulated
mutagenesis.
Hsie eta/. (1977) irradiated the hprt CHO system with Westinghouse white light F40CW
lamps. The minimal effective dose was 3.96 x 106 J/m
2
. Putting lids on the petri dishes
reduced mutant frequency by 30%. [The Working Group noted that the results were based
on a single dose point in a single experiment.) Jacobson eta/. (1978) exposed mouse lym-
phoma l.5178Y tk+l- cells to Sylvania F18T8 cool white lamps. The estimated lowest
effective dose was 2 x 10
4
J 1m
2
. [The Working Group noted that the selective agent used,
BUdR, is regarded as inefficient and has been superseded by trichlorothymidine, so these
results require confirmation.]
(c) Chromosomal effects
Sunlamps have been shown to produce sister chromatid exchange in amphibian cells
(Chao & Rosenstein, 1985) and in human fibroblasts (Bielfeld et al., 1989; Roser eta/., 1989).
Fibroblasts from a panel of cu,taneous malignant melanoma patients (Roser et al., 1989) and
heterozygotes ofxeroderma pigmentosum (Bielfeld et al., 1989) were more susceptible to the
induction of both sister chromatid exchange and micronuclei than those from normal donors.
Micronuclei were also induced in mouse splenocytes by exposure to sunlamps in vitro
(Dreosti et al., 1990).
A study with CHO cells provided evidence for a dose-related increase in the induction of
sister chromatid exchange by UV A. but the increased induction of chromosomal aberrations
showed no dose-response relationship (Lundgren & Wulf, 1988).
UVB induced sister chromatid exchange in CHO cells (Rasmussen et al., 1989) and
chromosomal aberrations in frog ICR 2A cells (Rosenstein & Rosenstein, 1985). In the latter
study, photoreactivation reduced the number of chromosomal ab-errations more effectively
at 265, 289 and 302 than at 313 nm, suggesting that non-cyclobutane dimer photoproducts
are more important primary lesions at the higher wavelength.
For UVC, more extensive data are available. Sister chromatid exchange was induced in
Chinese hamster V79 (Nishi et al. , 1984) and CHO (Rasmussen et al., 1989) cells. Chromatid
exchange was also r.ecorded in cultured fetal fibroblasts from New Zealand black mice, which
proved to be more sensitive than BALB/c cells (Reddy eta/., 1978). The induction of chro-
mosomal aberrations in Chinese hamster cells has been reported on a number of occasions
(Chu, 1965a,b; lfosko & Brewen, 1967; Bender et al., 1973; Griggs & Bender, 1973;
Ikushima & Wolff, 1974).
Exposure of frog ICR 2A cells to 254 or 265 nm radiation induced both sister chromatid
exchange (Chao & Rosenstein, 1985) and chromosomal aberrations, while photoreactivating
light significantly reduced the frequency of chromosomal aberrations, which implies a role
for pyrimidine dimers in their genesis (Rosenstein & Rosenstein, 1985). Chromosomal
OTHER RELEVANT DATA 203
aberrations were also seen with Xenopus cell cultures (Griggs & Bender, 1973).
frequencies of sister chromatid exchange and chromosomal aberrations induced by UVC
were reduced by photoreactivating light in chicken embryo fibroblasts (Natarajan et al.,
1980), lending further support to the concept that the cyclobutane pyrimidine dimer
represents a primary lesion in these two endpoints.
Parshad et al. (1980a) reported the induction of chromosomal damage in human IMR-90
fibroblasts following treatment with 4.6 W /m
2
over 20 h (331 kJ /m
2
) from F15T8-CW tubes.
Shielding and radical scavengers reduced the level of damage.
Extensive data are available on the induction of sister chromatid exchange in fibroblasts
from patients with Bloom's syndrome (Krepinsky et al., 1980), xeroderma pigmentosum (De
Weerd-Kastelein eta/., 1977; Fujiwara et aJ., 1981) or Cockayne's syndrome (Marshall et aJ
1980; Fujiwara et aJ. , 1981), as well as from normal individuals. In comparison with normal
individuals, more sister chromatid exchanges were induced per lethal lesion in fibroblasts
from excision-competent Bloom's syndrome (Kurihara et a/., 1987) and Cockayne's syn-
drome (Marshall et ai., 1980) patients. No such increase in sister chromatid exchange was
seen in fibroblasts from excision-defective xeroderma pigmentosum patients or from an
individual defective in the ligation step of repair (Henderson et al., 1985).
The induction of sister chromatid exchange by UV irradiation has also been studied in
human lymphocytes, with conflicting results. In one study, they were reported to be less
responsive than either human fibroblasts or CHO cells (Perticone eta/., 1986), while another
report, in which chromosomal aberrations were also studied, suggested that lymphocytes
were more sensitive than fibroblasts in their response at both end-points (Murthy et al.,
1982). These results may have implications for the interpretation of the effect of UV on the
immune system.
Fibroblasts from xeroderma pigmentosum patients are more sensitive to the induction
of chromosomal aberrations than cells from normal donors (Parrington et al., 1971;
Parrington, 1972; Marshall & Scott, 1976). Seguin et al. (1988) showed that lymphoblastoid
cells from five Cockayne's syndrome patients were similarly hypersensitive to UVC-induced
chromosomal aberrations. The induction of micronuclei in two normal and three Bloom' s
syndrome-derived fibroblast cell cultures was reported by Krepinsky et al. (1980). One
culture from a Bloom's syndrome patient, GM1492, proved to be exceptionally sensitive to
the induction of micronuclei; the other two were indistinguishable from normal cells. This
result emphasizes the potential.importance of heterogeneity in response among patients with
rare genetic syndromes.
(d) Transformation
Morphological transformation of mammalian cells has been induced by solar radiation,
unshielded fluorescent tubes, solar simulators, UVA. UVB and, most extensively, UVC.
There is weak evidence (Baturay eta/., 1985) for the induction of transformation by predo-
minantly UVA radiation (20T12BLB bulbs) in BALB/c 3T3 cells. In the same report, UVA
was shown to have promoting activity following initiation with The most
effective wavelength for Syrian hamster embryo cells (Doniger et al., 1981) and human em-
bryonic fibroblasts (Sutherland eta/., 1981) appears to be in the UVC range at about 265 nm.
'fransformation of human cells can be enhanced by delivering the dose on a number of
204 lARC MONOGRAPHS VOLUME 55
separate occasions (Sutherland eta/:, 1988). It has also been reported that excision repair-
defective xeroderma pigmentosum cells can be transformed to the anchorage-independent
phenotype at lower doses than those required for cells from normal individuals (Maher eta/.,
1982). Fisher and Cifone (1981) showed enhanced metastatic potential of mouse fibro-
sarcoma cells. Plasmids containing the human N-ras gene which were irradiated with UVR
(254 nm) in vitro acquired the ability to transform cultured rat-2 cells after transfection;
photoreactivation of irradiated plasmids eliminated their transforming ability (van der
Lubbe eta/. , 1988). In another study, UVB irradiation activated the human Ha-ras gene on a
plasmid in a transformation assay with mouse NIH-3T3 cells (Pierceall & Ananthaswamy
(1991).
An investigation of chromosomal breaks and malignant transformation in embryonic
mouse cells (Sanford eta/., 1979; Parshad eta/., 1980b) revealed that exposure of cultured
cells to t1uorescent lamps induced malignant transformation, as measured by tumour
formation following implantation into syngeneic hosts. The potential importance of active
oxygen species was revealed by experiments in which the partial pressure of oxygen in
cultures was increased, resulting in increased malignant transformation and correlated chro-
mosomal breakage.
Kennedy et a/. (1980) reported induction of transformation in C3H 10'Ph mouse
embryonic cell cultures by light from General Electric F18T8 lamps. The lowest effective
dose was estimated at 2 x 10
5
J/m
2
, and use of petri dish lids was effective in reducing
transformation.
(e) Effects on cellular and viral gene expression
A number of cellular oncogenes and other genes involved in the regulation of growth are
implicated in the process of carcinogenesis, as they are subject to both gene mutation and
alteration in expression due to chromosomal rearrangement. Many of these genes also ~ w
transient alterations in expression following DNA damage, which has led to the suspicion
that such transient changes are involved, either directly or indirectly, in the carcinogenic
process.
UVC radiation was found to increase transiently the expression of various cellular
genes, including those that code for collagenase (Stein et a/. , 1989), the fos protein
(Hollander & Fornace, 1989; Steiner al., 1989), the jun protein (Ronai et al., 1990), metallo-
thioneins I and II (Fomace et a/., 1988) and human plasminogen activator (Miskin &
Ben-Ishai, 1981). UVA radiation enhanced expression of the genes that code for the fos
protein (Hollander & Fornace, 1989), and UVB radiation increased the level of ornithine
decarboxylase (Verma et a/., 1979). Different levels of cytotoxicity were seen in these
experiments. UVA radiation at doses that inactivate a small fraction of the fibroblast cell
population induced expression of the haem oxygenase gene (Keyse & 'JYrrell, 1989) by a
transient enhancement in transcription rate (Keyse et a/., 1990). cis-Acting enhancer
elements have been shown to be involved in activation of the collagenase and c-fos, as well as
human immunodeficiency promoter (Stein eta/., 1989). In both rat fibroblasts and human
keratinocyte cell lines, exposure to UVR increased the levels of c-fos RNA within 10 min and
of c-myc RNA after about 1 h. The levels peaked at 30 min and 7 hand returned to normal
within 1 hand 24 h, respectively. The order of effectiveness was UVC > UVB > UVA
OTHER RELEVANT DATA 205
(Ronai et al., 1990). Elevated levels of p53 protein were observed in mouse cells treated with
UVR; the increase was due to post-translation activation or stabilization (Maltzman &
Czyzyk, 1984). In human keratinocytes exposed to UVA. increased levels of human
epidermal growth factor receptor RNA (HER-1) were found (Yang et al., 1988).
The mechanisms that mediate these transient and immediate inducible responses are
largely unknown. Some of them, however, overlap with those seen in response to tumour
promoters, and it is significant that natural sunlight has been reported to enhance the
expression of protein kinase C in cultured human epithelial P3 cells (Peak et al., 1991a). For
reviews of this general area, see Ananthaswamy and Pierceall (1990) and Ronai et al. (1990).
Other transient responses to UVR have been noted at somewhat later times (12-48 h).
Methotrexate resistance due to gene amplification was reported in 3T6 mouse cells (Tisty et
a/., 1984). Another selective DNA amplification response is induction by UVR of viral DNA
synthesis, e.g., of polyoma virus in rat fibroblasts. UVC was more effective than UVB, and
UVA was ineffective (Ronai eta/., 1987). In Chinese hamster embryo cells, UVC irradiation
increased DNA binding to the early domain of the SV40 minimal origin, resulting in SV40
DNA amplification (Liicke-Huhle et al., 1989). The induction of asynchronous viral
replication is mediated by cellular proteins that bind to specific sequences in the DNA of
polyoma (Ronai & Weinstein, 1988) and SV40 viruses (Liicke-Huhle et al., 1989).
Exposure to UVR can activate viruses. This phenomenon has been known for herpes
simplex virus for a long time (for a recent report, see Rooney et al., 1991). It was reported
recently that UVC can activate the gene promoters of the human immunodeficiency virus
(HIV) (Valerie et a/., 1988) and Moloney murine sarcoma virus (Lin et al., 1990).
Furthermore, activation of complete HIV grown in cells pre-exposed to UVC radiation was
observed (Valerie et a/., 1988). HIV activation may contribute to faster development of
AIDS, which in turn may facilitate development of malignancies. Further studies showed that
the HIV promoter and HIV are activated by UVC and UVB, but not UVA radiation even at
yery high exposures (Stanley et al. , 1989; Beer eta/. , 1991 [abstract); Lightfoote et al., 1992).
There are indications that pyrimidine dimers (Stein et al., 1989) or chromatin damage
(Valerie & Rosenberg, 1990) play a role in the initiation of HIV activation by UVR. The
in-vitro observations have been verified for UVC, UVB and UVA in experiments with
transgenic mice carrying the HIV promoter/reporter gene constructs (Cavard et al., 1990;
Frucht eta/., 1991; Vogel eta/., 1992). For reviews on the activation HIV by UVR, see
Zmudzka and Beer (1990) and Beer and Zmudzka (1991).
Table 32. Genetic and related effects of solar, simulated solar and sunlamp (UVA and UVB) irradiation
Test system
BS?, Bacillus subti/is, mutation
SSB, Saccharomyces cerevisiae D1, DNA damage
PLM, Wheat mutation
DIA, DNA damage, ICR 2A frog cells in vitro
DIA, DNA damage, ICR 2A frog cells in vitro
DIA, DNA strand breaks, Chinese hamster V79 cells
DIA, DNA damage, Chinese hamster V79 cells in vitro
DIA, DNA damage, C3H lO'flh mouse cells in vitro
GCO, Gene mutation, Chinese hamster ovary cells in vitro
G9H, Gene mutation, Chinese hamster V79lung cells in vitro, 6-TGr
G5f, Gene mutation, mouse lymphoma L5178Y cells in vitro
G9H, Gene mutation, Chinese hamster V79 lung cells in vitro, 6-TGt
GCO, Gene mutation, Chinese hamster ovary cells in vitro
G9H, Gene mutation, Chinese hamster V79 lung cells in vitro, 6-Tor
SIA, Sister chromatid exchange, ICR 2A frog cells in vitro
MIA, Micronucleus test, mouse splenocytes in vitro
TBM, Cell transformation, BALB/c 3T3 mouse cells in vitro
TBM, Cell transformation, BALB/c mouse epidermal cells in vitro
TCM, Cell transformation, C3H lOT% mouse embryo cells in vitro
TCM, Cell transformation, C3H lOT% mouse cells in vitro
TCL, Cell transformation, mouse fibrosarcoma cells in vitro
TCL, Cell transformation, l()Tlh mouse skin fibroblasts in vitro
DIA, DNA damage, fish in vitro
DIH, DNA damage, human skin fibroblasts in vitro
DIH, DNA damage, human skin fibroblasts in vitro
DIH, DNA damage, human skin fibroblasts in vitro
DIH, DNA damage, human skin fibroblasts in vitro
DIH, DNA damage, human HeLa cells in vitro
GIH, Gene mutation, human xeroderma pigmentosum fibroblasts in vitro
SHF, Sister chromatid exchange, humanb fibroblasts in vitro
Result a
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Reference
Munakata (1989)
Hannan et a/. (1984)
Morgun eta/. (1988)
Chao & Rosenstein (1986)
Rosenstein eta/. 1 9 8 ~ )
Elkind & Han (1978)
Suzuki eta/. (1981)
Suzuki eta/. (1981)
Hsie eta/. (1977)
Zblzer eta/. (1988)
Jacobson et a/. (1978)
Bradley & Sharkey (1977)
Burki & Lam (1978)
Suzuki eta/. (1981)
Chao & Rosenstein (1985)
Dreosti et a/. (1990)
Withrow eta/. (1980)
Ananthaswamy & Kripke (1981)
Kennedy eta/. (1980)
Suzuki eta/. (1981)
Fisher & Cifone (1981)
Ananthaswamy (1984a)
Applegate & Ley (1988)
Rosenstein et a/. (1985)
Chao & Rosenstein (1986)
Rosenstein (1988)
Rosenstein & Mitchell (1991)
Elkind & Han (1978)
Patton et a/. (1984)
Knees-Matzen eta/. (1991)
~
~
=:
0
6
0
~
'"tl
::r:
Cl'l
a
~
=:
tTl
u..
VI
Table 32 (contd)
Test system
SIH, Sister chromatid exchange, human xeroderma pigmentosum fibroblasts
SIH, Sister chromatid exchange, human malignant melanoma cells
MIH, Micronucleus test, human xeroderma pigmentosum fibroblasts
MIH, Micronucleus test, human malignant melanoma cells
DVA, DNA damage, BALB/c mouse skin cells in vivo
DVA, DNA damage, marsupial corneal cells in vivo
DVA, DNA damage, marsupial corneal cells in vivo
1VI, Cell transformation, l()Tih mouse skin fibroblasts treated in vivo scored in vitro
DVH, DNA damage, human skin cells in vivo
DVH, DNA damage, human skin cells in vivo
a + , positive
bpifst-degree relatives of melanoma patients
Result a
+
+
+
+
+
+
+
+
+
+
Reference
0
Bielfeld et al. (1989)
;1
tT1
Roser et al. (1989) ::0
Bielfeld et al. (1989) ::0
l'T1
Roser et al. (1989) t"""
Ananthaswamy & Fisher (1981)
tT1
Freeman et al. (1988a)
Ley et al. (1988)
Ananthaswamy (1984b)
0
Eggset et a/. (1983)
Freeman eta/. (1988b)
;l>
9
Table 33. Genetic and related effects of predominantly UVA irradiation (near UV)
Thst system
SA9, Sa/TTI()nel/a typhimurium TA98, reverse mutation
ECW, Escherichia coli WP2 uvrA. reverse mutation
EC2, Escherichia coli WP2 her-, reverse mutation
ECR, Escherichia coli Blrll, trp, r:everse mutation
ECR, Escherichia coli WP2 recA, reverse mutation
ECR, Escherichia coli WP2 uvrA recA. reverse mutation
ECR, Escherichia coli B/r uvrA trp thy, reverse mutation
ECR, Escherichia coli wild type, reverse mutation
ECR, Escherichia coli, mutation
SSB, Saccharomyces cerevisiae wild type, DNA damage
SSB, Saccharomyces cerevisiae excision-deficient, DNA damage
SSB, Saccharomyces cerevisiae D1, DNA damage
DIA, DNA damage, Chinese hamster ovary cells in vitro
DIA. DNA strand breaks, Chinese hamster ovary cells in vitro
GCO, Gene mutation, Chinese hamster ovary cells in vitro
GCO, Gene mutation, Chinese hamster ovary cells in vitro
GCO, Gene mutation, Chinese hamster ovary cells in vitro
G9H, Gene mutation, Chinese hamster lung V79 cells, hprt locus
G90, Gene mutation, Chinese hamster lung V79 cells, 6-TGr
G5T, Gene mutation, mouse lymphoma L5178Y cells, tk locus
SIC, Sister chromatid exchange, Chinese hamster ovary ceUs in vitro
CIC, Chromosomal aberrations, Chinese hamster ovary cells in vitro
TCL, Cell transformation, Syrian hamster embryo cells in vitro (neoplastic transformation)
TCL, Cell transformation, Syrian hamster embryo cells in vitro (morphological transformation)
DIH, DNA strand breaks, human fibroblasts in vitro
DIH, DNA strand breaks, human teratoma cells in vitro
DIH, DNA double strand breaks, human teratocarcinoma cells in vitro
DIH, DNA strand breaks, human fibroblasts in vitro
DIH, DNA-protein cross-links, human teratocarcinoma cells in vitro
DIH, DNA strand breaks, human epithelial P3 cells in vitro
DIH, Pyrimidine dimer formation, human skin fibroblasts in vitro
Result a
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
(+)
+
+
+
+
+
+
+
+
00
Reference
Calkins et al. (1987)
Tyrrell (1982)
Kubitschek (1967)
Webb & Malina (1970)
Tyrrell (1982)
Tyrrell (1982)
'JYrrell (1982)
.......
>
'JYrreU (1982)
f5
Wood et al. (1984)
a:
Zolzer & Kiefer (1983)
0
Zolzer & Kiefer (1983)
z
Hannan eta/. (1984)
0
0
Zelle eta/. (1980)
5:
Churchill eta/. (1991)
"'
Zelle eta/. (1980)
::r:
Singh & Gupta (1982)
V'l
Lundgren & Wulf (1988)
6
Wells & Han (1984)
r
c:
Wells & Han (1984)
a:
Hitchins eta/. (1987)
['11
Lundgren & Wulf (1988)
Ul
Ul
Lundgren & Wulf (1988)
Barrett et a/. (1978)
Barrett et al. (1978)
Rosenstein & Ducore (1983)
Peak eta/. (1987)
Peak & Peak (1990)
Francis & Giannelli (1991)
Peak & Peak (1991)
Peak eta/. (199lb)
Enninga eta/. (1986)
Table 33 (contd)
Thst system
DIH. Pyrimidine dimer formation, human skin fibroblasts in vitro
GIH, Gene mutation, human lymphoblastoid cell line in vitro
GIH, Gene mutation, human skin fibroblasts in vitro
GIH, Gene mutation, human epithelial cells in vitro
DVH, Pyrimidine dimer formation, human skin in vivo
a+, positive; ( + ), weakly positive; -, negative
"Positive result with 365 nm but not with 334 nm at same fluence
Result a
+
+
+b
+
Reference
Rosenstein & Mitchell (1987)
Tyrrell (1984)
Enninga eta/. (1986)
Jones et al. (1987)
Freeman eta/. (1989)
tT1
0
:::>
Table 34. Genetic and related effects of predominantly UVB irradiation
Thst system
SA9, Salmonella typhimurium TA98, reverse mutation
EC2, Escherichia coli WP2, reverse mutation
TSC, 1Tadescantia, chromosomal aberrations
DIA. DNA damage, Chinese hamster ovary cells in vitro
DIA, DNA strand breaks, Chinese hamster V79 cells
DIA, DNA-protein cross-links, Chinese hamster V79 cells
GCO, Gene mutation, Chinese hamster ovary cells in vitro
GCO, Gene mutation, Chinese hamster ovary cells in vitro
G9H, Gene mutation, Chinese hamster V79 lung cells, hprt locus
G9H, Gene mutation, Chinese hamster V79 lung cells, hprt locus
G90, Gene mutation, Chinese hamster V79 lung cells, ouabainr
G9H, Gene mutation, Chinese hamster V79 lung cells in vitro, 6TGr
051, Gene mutation, mouse lymphoma L5178Y cells in vitro
SIC, Sister chromatid exchange, Chinese hamster ovary cells in vitro
CIA. Chromosomal aberrations, ICR 2A frog cells in vitro
TCS, Cell transformation, Syrian hamster embryo cells in vitro
DIH, DNA strand breaks, human skin fibroblasts in vitro
DIH, Pyrimidine dimer formation, human skin fibroblasts in vitro
DIH, Pyrimidine dimer formation, human skin fibroblasts in vitro
DIH, DNA strand breaks, human teratoma in vitro
DIH, DNA double strand breaks, human teratocarcinoma in vitro
DIH, DNA-protein cross-links, human teratocarcinoma in vitro
DIH, Pyrimidine dimer formation in human skin keratinocytes in vitro
DIH, Thymine dimer formation, human fibroblasts in vitro
GIH, Gene mutation, human lymphoblastoid cell line in vitro
GIH, Gene mutation, human skin fibroblasts in vitro
GIH, Gene mutation, human epithelial cells in vitro
TIH, Cell transformation, human fibroblasts in vitro
DVA. Cyclobutane dimers in SV40 plasmid DNA in human fibroblasts in vivo
OVA, Cytosine photohydrates in SV40 plasmid DNA in human fibroblasts in vivo
Result
4
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
N
......
0
Reference
Calkins eta/. (1987)
Peak et a/. (1984)
Kirby-Smith & Craig (1957)
Zelle eta/. (1980)
Matsumoto eta/. (1991)
Matsumoto et at. (1991)
-
Zelle et al. (1980)
Rasmussen eta/. (1989)
("')
Wells & Han (1984) 3:
Zolzer & Kiefer (1984)
0
z
Wells & Han (1984)
0
Colella er al. (1986)
0
Jacobson era!. (1981)
Rasmussen et a/. (1989)
'"t'l
:I:
Rosenstein & Rosenstein (1985)
C/)
Doniger eta/. (1981)
d
Rosenstein & Ducore (1983)
E
Enninga er at. (1986)
Rosenstein & Mitchell (1987)
m
Peak eta/. (1987) VI
VI
Peak & Peak (1990)
Peak & Peak (1991)
Schothorst eta/. (1991)
Roza et a/. (1988)
l)'rrell (1984)
Enninga eta/. (1986)
Jones, C.A. eta/. (1987)
Sutherland eta/. (1981)
Mitchell et al. (1991)
Mitchell et al. (1991)
Table 34 (contd)
Test system
DVA, Pyrimidine dimer induction, mouse skin in vivo
DVA, Pyrimidine dimer formation, mouse skin in vivo
DVA, (6-4) Photoproduct formation, mouse epidermis in vivo
DVH, Pyridime dimer formation, human skin in vivo
UVH, Unscheduled DNA synthesis, human cornea in vivob
a+' positive; -, negative
bFrom people who had been dead for 15 min
Result"
+
+
+
+
+
Reference
Cooke & Johnson (1978)
Ley et al. (1983)
Olsen et al. (1989)
Freeman et al. (1989)
Grabner & Brenner (1981)
tTl
'='
'='
0
>
N
....
....
Table 35. Genetic and related effects of UVC irradiation
N
....
N
Test system Result a Reference
ECB, Escherichia coli, thymine dimer formation +
Setlow et al. (1963)
ECB, Escherichia coli, photoproduct formation + Setlow (1968)
ECB, Escherichia coli, thymine photoadduct formation + Smith (1964)
ECB, Escherichia coli, pyrimidine dimers +
Brash & Haseltine (1982)
ECB, Escherichia coli, (6-4) photoproducts
+
Brash & Haseltine (1982)
ECF, Escherichia coli, miscellaneous strains, forward mutation + Miller (1985)
ECR, Escherichia coli, mutation + Witkin (1976)
ECR, Escherichia coli, mutation + Walker (1984)
>
ECR, Escherichia coli, mutation +
Franklin & Haseltine (1986)
:::0
()
ECR, Escherichia coli, mutation + Bridges et al. (1987)
ECR, Escherichia coli, mutation +
Schaaper et al. (1987) 0
SSB, Sacdwomyces cerevisiae, pyrimidine dimer formation +
Wheatcroft et al. (1975)
z
0
SSB, Saccharomyces cerevisiae, pyrimidine dimer formation +
Resnick et a/. (1987)
0
SCN, Saccharomyces cerevisiae, aneuploidy + Parry et a/. (1979)
SCF, Saccharomyces cerevisiae, forward mutation +
Lee et al. (1988) '"d
:I:
SCR, Saccharomyces cerevisiae, reverse mutation + Siede & Eckardt (1986) Cl"l
PLU, Plants, DNA damage + McLennan (1987)
6
PLU, Nicotiana tabacum, unscheduled DNA synthesis + Cieminis et a/. (1987)
E
PLU, Chlamydomonas reinhardtii, pyrimidine dimer formation + Vlcek et al. (1987)
PLM, Chlamydomonas reinhardtii, mutation + Vlcek eta/. (1987)
m
TSC, Tradescantia, chromosomal aberrations +
Kirby-Smith & Craig (1957) lJI
lJI
DM?, Drosophila melanogaster embryo cells in vitro, DNA damage + Koval (1987)
DIA, DNA damage, ICR 2A frog cells in vitro
+
Chao & Rosenstein (1986)
DIA, DNA strand breaks, Chinese hamster V79 cells + Elkind & Han (1978)
DIA, DNA damage, Chinese hamster ovary cells in vitro + Zelle et at. (1980)
GCO, Gene mutation, Chinese hamster ovary cells in vitro + Zelle et al. (1980)
GCO, Gene mutation, Chinese hamster ovary cells in vitro + Rasmussen eta/. (1989)
GCO, Gene mutation, Chinese hamster ovary cells in vitro + Drobetsky & Glickman (1990)
G9H, Gene mutation, Chinese hamster V79 lung cells in vitro + Colella et a/. (1986)
G9H, Gene mutation, Chinese hamster V79 lung cells, hpn locus
+ Suzuki et al. (1981)
G9H, Gene mutation, Chinese hamster V79 lung cells, hprt locus
+ Zolzer & Kiefer (1984)
G90, Gene mutation, Chinese hamster V79lung cells, ouabainr + Suzuki eta/. (1981)
Table 35 (contd)
Test system
G51, Gene mutation, mouse lymphoma L5178Y cells in vitro
SIC, Sister chromatid exchange, Chinese hamster V79 cells in vitro
SIC, Sister chromatid exchange, Chinese hamster ovary cells in vitro
SIA, Sister chromatid exchange, ICR 2A frog cells in vitro
SIA, Sister chromatid exchange, chick embryo fibroblasts in vitro
CIC, Chromosomal aberrations, Chinese hamster fibroblasts in vitro
CIC, Chromosomal abermtions, Chinese hamster fibroblasts in vitro
CIC, Chromosomal aberrations, Chinese hamster V79 cells in vitro
CIC, Chromosomal aberrations, Chinese hamster V79 cells in vitro
CIC, Chromosomal aberrations, Chinese hamster ovary cells in vitro
CIC, Chromosomal aberrations, Chinese hamster CHEF-125 cells in vitro
CIA, Chromosomal aberrations, chick embryo fibroblasts in vitro
CIA, Chromosomal aberrations, A8W243 Xenopus cells in vitro
CIA, Chromosomal aberrations, ICR 2A frog cells in vitro
CIA, Chromosomal aberrations, New Zealand black mouse fetal fibroblasts
TBM, Cell transformation, BALB/c 3T3 mouse cells
TCM, Cell transformation, C3H 1QT1h mouse cells
TCM, Cell transformation, C3H IQTI/z mouse cells
TCM, Cell transformation, C3H 1QTI/z mouse cells
TCM, Cell transformation, C3H 1QTI/z mouse cells
TCM, Cell transformation, C3H lQTlh mouse cells
TCS, Cell transformation, Syrian hamster embryo cells
TCS, Cell transformation, Syrian hamster embryo cells
TCS, Cell transformation, Syrian hamster embryo cells
TEV, Cell transformation, SV -40/BALB/c 3T3 mouse cells
DIH, DNA strand breaks, human skin fibroblasts in vitro
DIH, DNA damage, human skin fibroblasts in vitro
DIH, Pyrimidine dimer formation, human skin fibroblasts in vitro
DIH, Pyrimidine dimer formation, human skin fibroblasts in vitro
DIH, DNA strand breaks, human teratoma cells in vitro
DIH, Thymine dimer formation, human skin fibroblasts in vitro
DIH, DNA damage, human skin fibroblasts in vitro
Result a
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Reference
Jacobson et al. (1981)
Nishi et at. (1984)
Rasmussen et al. (1989)
Chao & Rosenstein (1985)
Natarajan et al. (1980)
Chu (1965a)
Chu {1965b)
Bender eta/. (1973)
Griggs & Bender (1973)
Ikushima & Wolff (1974)
Trosko & Brewen (1967)
Natarajan et at. (1980)
Griggs & Bender (1973)
Rosenstein & Rosenstein (1985)
Reddy eta/. (1978)
Withrow et a/. (1980)
Chan & Little (1976)
Monda! & Heidelberger (1976)
Chan & Little (1979)
Suzuki et al. (1981)
Borek eta/. {1989)
DiPaolo & Donovan (1976)
Doniger eta/. (1981)
Borek eta/. (1989)
Withrow eta/. (1980)
Rosenstein & Ducore (1983)
Rosenstein et at. (1985)
Enninga et a/. (1986)
Rosenstein & Mitchell (1987)
Peak et a/. (1987)
Roza et al. (1988)
Chao & Rosenstein (1986)
0
m
::0
::0
m
- t""
m
0
>
N
w
Table 35 (contd)
Thst system
DIH, DNA strand breaks, human fibroblasts in vitro
DIH, DNA-prQtein cross-links, human fibroblasts in vitro
DIH, DNA double strand breaks, human teratocarcinoma cells in vitro
DIH, DNA-protein cross-links, human teratocarcinoma cells in vitro
DIH, Pyrimidine dimer fonnation, human skin keratinocytes and melanocytes in vitro
GIH, Gene mutation, human fibroblasts in vitro
GIH, Gene mutation, human fibroblasts in vitro
GIH, Gene mutation, human iymphocytes in vitro
GIH, Gene mutation, human lymphoblastoid cell line in vitro
GIH, Gene mutation, human skin fibroblasts in vitro
GIH, Gene mutation, human epithelial cells in vitro
GIH, Gene mutation, human HeLa cells in vitro
GIH, Gene mutation, human lymphocytes in vitro
GIH, Gene mutation, human fibroblasts in vitro
GIH, Gene mutation, human fibroblasts in vitro
GIH, Gene mutation, human melanoma cells in vitro
SHF, Sister chromatid exchange, human fibroblasts in vitro
SHF, Sister chromatid exchange, human fibroblasts in vitro
SHL, Sister chromatid exchange, human lymphocytes in vitro
SHL, Sister chromatid exchange, human lymphocytes in vitro
SHF, Sister chromatid exchange, human skin fibroblasts
SHF, Sister chromatid exchange, human skin fibroblasts
SHF, Sister chromatid exchange, human skin fibroblasts
SHF, Sister chromatid exchange, human skin fibroblasts
MIH, Micronucleus test, human skin fibroblasts in vitro
CHF, Chromosomal aberrations, human fibroblasts in vitro
CHF, Chromosomal aberrations, human skin fibroblasts
CHF, Chromosomal aberrations, human skin fibroblasts
CHL, Chromosomal aberrations, human lymphocytes in vitro
CHL, Chromosome exchanges, human lymphocytes in vitro
TIH, Cell transfonnation, human fibroblasts in vitro
TIH, Cell transfonnation, human fibroblasts in vitro
Result a
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
N
......
""
Reference
Lai & Rosenstein (1990)
Lai & Rosenstein (1990)
Peak & Peak (1990}
Peak & Peak (1991)
Schothorst eta/. (1991)
Maher et a/. (1979)
Myhr et a/. (1979)
.....
Sanderson eta/. (1984)
>
Tyrrell (1984)
;:1::1
n
Enninga et a/. (1986)
a:
Jones, C.A. eta/. (1987) 0
Musket a/. (1989)
z
0
Norimura eta/. (1990) a
Dorado eta/. (1991)
McGregor eta/. (1991)
'"CJ
:r:
Musket a/. (1989) en
Fujiwara eta/. (1981) <
0
Kurihara eta/. (1987)
t""'
Murthy eta/. (1982)
e
s::
Perticone eta/. (1986)
tTl
De Weerd-Kastelein eta/. ( 1977)
u.
u.
Krepinsky eta/. (1980)
Marshall et a/. (1980)
Henderson eta/. (1985)
Krepinsky eta/. (1980)
Parrington (1972)
ParTington eta/. (1971)
Marshall & Scott (1976)
Murthy eta/. (1982)
Holmberg & Gumauskas (1990)
Sutherland et al. (1981)
Maher et al. (1982)
Table 35 (contd)
'lest system
TIH, Cell transformation, human fibroblasts in vitro
???, Cyclobutane dimers in SV40 plasmid DNA in human skin fibroblasts in vitro and in vivo
???, Cytosine photohydrates in SV40 plasmid DNA in human skin fibroblasts in vitro and
in vivo
DVA, Pyrimidine dimer formation, mouse skin in vivo
a+ , positive
Result
4
+
+
+
+
Reference
m
Sutherland et al. {1988)
tTl
Mitchell et al. (1991)
Mitchell et al. (1991)
Bowden et al. {1975)
Cl
tv
th
5. Summary of Data Reported and Evaluation
5.1 Exposure data
Terrestrial life is dependent on radiant energy from the sun. Approximately 5% of solar
terrestrial radiation is ultraviolet radiation (UVR), and solar radiation is the major source of
human exposure to UVR. Before the beginning of this century, the sun was essentially the
only source of UVR, but with the advent of artificial sources the opportunity for additional
exposure has increased.
UVR spans the wavelengths from 100 to 400 nm. The biological effects of UVR vary
enormously with wavelength; by convention, the ultraviolet spectrum has been further
subdivided into three regions: UVC (100-280 nm), UVB (280- 315 nm) and UVA(315-400
nm).
Solar UVR that reaches the Earth's surface comprises approximately 95% UVA and 5%
UVB: UVC is completely filtered out by the Earth's atmosphere. The amount of solar UVR
measured at the Earth's surface depends upon a number of factors, which include solar zenith
angle (time of day, season and geographical latitude), stratospheric ozone, atmospheric
pollutants, weather, ground reflectance and altitude.
Exposed skin surface is irradiated differently depending on cultural and social beha-
viour, clothing, the position of the sun in the sky and the relative position of the body.
Exposure to UVB of the most exposed skin surfaces, such as nose, tops of the ears and fore-
head, relative to that of the lesser exposed areas, such as underneath the chin, normally
ranges over an order of magnitude. Ground reflectance plays a major role in exposure to
UVB of the eye and shaded skin surfaces, particularly with highly reflective surfaces such as
snow.
In cutaneous photobiology, radiant exposure is frequently expressed as 'exposure dose'
in units of J/cm
2
(or J/m
2
). 'Biologically effective dose', derived from radiant exposure
weighted by an action spectrum, is expressed in units of J/cm
2
(effective) or as multiples of
'minimal erythema dose' (MED). In cellular photobiology, the term 'fluence' is often used
incorrectly as equivalent to radiant exposure.
The cumulative annual exposure dose of solar UVR varies widely among individuals in a
given population, depending to a large extent on occupation and extent of outdoor activities.
For example, it has been estimated that indoor workers in mid-latitudes (40-60 oN) receive
an annual exposure dose of solar UVR to the face of about 40-160 times the MED, depen-
ding upon propensity for outdoor activities, whereas the annual solar exposure dose for
outdoor workers is typically around 250 times the MED. Because few actual measurements
have been reported of personal exposures, these estimates should be considered to be very
approximate and subject to differences in cultural. and social behaviour, clothing, occupation
and outdoor activities.
-217-
218 lARC MONOGRAPHS VOLUME 55
Cumulative annual outdoor exposures may be augmented by exposures to articial
sources of UVR. For example, the use of cosmetic tanning appliances increased in popularity
in the 1980s. The majority of users are young women, and the median annual exposure dose is
probably 20-30 times the MED. Currently used appliances emit primarily UVA radiation;
prior to the 1980s, tanning lamps emitted higher proportions of UVB and UVC.
UVR has been used for several decades to treat skin diseases, notably psoriasis. A
variety of sources of UVR are employed, and nearly all emit a broad spectrum of radiation. A
typical dose in a single course of UVB phototherapy might lie between 200 and 300 times the
MED.
UVR is used in many different industries, yet there is a paucity of data concerning human
exposure from these applications, probably because in normal practice sources are well-
contained and exposure doses are expected to be low. Acute reactions to overexposure are
common among electric arc welders. Staff in hospitals who work with unenclosed photo-
therapy equipment are at potential risk of overexposure unless protective measures are
taken. Individuals exposed to lighting from fluorescent lamps may typically receive annual
exposure doses of UVR ranging from 0 to 30 times the MED, depending on illuminance
levels and whether or not the lamps are housed behind plastic diffusers. There is increasing
use of tungsten-halogen lamps, which also emit UVR, for general lighting.
5.2 Human carcinogenicity data
5.2.1 Solar radiation
Subjects with the inherited condition xeroderma pigmentosum appear to have fre-
quencies of nonmelanocytic skin cancer and melanoma that are much higher than expected.
Some evidence suggests that the greatest excess occurs on the head and neck.
(a) Nonmelanocytic skin cancer
The results of descriptive epidemiological studies suggest that exposure to sunlight
increases the risk of nonmelanocytic skin cancer. These tumours occur predominantly on the
skin of the face and neck, which is most commonly exposed to sunlight, although the
distribution of basal-cell carcinomas is not as closely related to the distribution of exposure
to the sun as is that of squamous-cell carcinomas. There is a strong inverse relationship
between latitude and incidence of or mortality from skin cancer and, conversely, a positive
relationship between incidence or mortality and measured or estimated ambient UVR.
Migrants to Australia from the British Isles have lower incidence of and mortality from non-
melanocytic skin cancer than the Australian-born population. People who work primarily
outdoors have higher mortality from these cancers, and there is some evidence that outdoor
workers have higher incidence.
In several cross-sectional studies, positive associations have been seen between mea-
sures of solar skin damage and the prevalence of basal- and squamous-cell carcinomas. Mea-
sures of actual exposure to the sun have been less strongly associated with these cancers,
possibly because of errors in measurement and inadequate control for potential confounding
variables. In a study of US fishermen, estimates of individual annual and cumulative
exposure to UVB were positively associated with the occurrence of squamous-cell carcinoma
but not with the occurrence of basal-cell carcinoma.
SUMMARY OF DATA REPORTED AND EVALUATION 219
Only two population-based case-control studies have been conducted. In one of these,
from Canada, the response rate was low and the measures of exposure were crude. In the
other study, from Australia, facial telangiectasia and solar elastosis of the neck were strongly
associated with the risk for squamous-cell carcinoma, and cutaneous microtopography and
solar elastosis of the neck were strongly associated with risk for basal-cell carcinoma.
Migrants to Australia had a lower risk of squamous-cell carcinoma than did native-born
Australians, and migrants who arrived after childhood had a lower risk for basal-cell
carcinoma.
The hospital-based case- control studies that have been conducted suffer from methodo-
logical deficiencies, including choice of controls, measurement of exposure and confounding
by reaction to sunlight, and are therefore difficult to interpret.
In a cohort study of nurses in the USA, those who spent more than 8 h per week outside
without sunscreens had a similar incidence rate of basal-cell carcinoma to those who spent
fewer than 8 h per week outdoors. In a cohort study from Victoria, Australia, the rates of both
types of skin cancer were increased in outdoor workers, but the effect was not significant
after adjustment for reaction to sunlight.
(b) Cancer of the lip
Cancer of the lip has been related to outdoor occupation in a number of descriptive
studies. Migrants to Australia and Israel have lower risks than native-born residents.
Three case- control studies provide useful information about the association between
outdoor work, taken as a proxy measure for exposure to UVR, and cancer of the lip. All of
them showed a significantly increased risk, although potential confounding by tobacco use
was not controlled adequately in any of the studies.
Assessment of the carcinogenicity of solar radiation for the lip is complicated by the fact
that carcinoma of the lip as actually diagnosed is a mixture of cancers of the external lip and
cancers of the buccal membranes. Use of alcohol and tobacco are known causes of the latter
tumours.
(c) Malignant melanoma of the skin
Descriptive studies in whites in North America, Australia and several other countries
show a positive association between incidence of and mortality from melanoma and resi-
dence at lower latitudes. Studies of migrants suggest that the risk of melanoma is related to
solar radiant exposure at the place of residence in early life. The body site distribution of
melanoma shows lower rates per unit area on sites usually unexposed to the sun than on
usually or regularly exposed sites.
A large number of case-control studies are pertinent to the relationship between
melanoma and exposure to the sun. These include large, carefully conducted population-
based studies carried out in Western Australia, Queensland, western Canada and Denmark.
Their results are generally consistent with positive associations with residence in sunny
environments throughout life, in early life and even for short periods in early adult life.
Positive associations are generally seen between measurements of cumulative sun damage
expressed biologically as microtopographical changes or history of keratoses or nonmelano-
cytic skin cancer.
220 IARC MONOGRAPHS VOLUME 55
In contrast, the associations with total exposure to the sun over a lifetime or in recent
years, as assessed by questionnaire, are inconsistent. This inconsistency may be due to diffe-
rences in the effects of chronic and intermittent exposure. Chronic exposure, as assessed
through occupational exposure, appeared to reduce melanoma risk in three of the large
studies, particularly in men; this observation is consistent with the descriptive epidemiology
of the condition, which shows lower risks in groups that work outdoors. Several other studies,
which were generally smaller or had less detailed methods of exposure assessment, show
either no effect or an increased risk associated with occupational exposures.
Assessment of intermittent exposure is complex; nonetheless, most studies show positive
associations with measure of intermittent exposure, such as particular sun-intensive acti-
vities, outdoor recreation or vacations.
Most studies show positive associations with a history of sunburn; however, this asso-
ciation cannot be easily interpreted, because while it might accurately reflect sunburn it
could just as well reflect either the tendency to sunburn, if exposed, or intermittent exposure
more generally.
(d) Melanoma of the eye
There is no latitude gradient among white populations of the incidence of ocular neo-
plasms, some 80% of which are likely to be ocular melanomas. No effect of southern US
birthplace was seen in the two descriptive studies in the USA that examined this aspect.
Four case- control studies, from western Canada and from Philadelphia, San Francisco
and Boston, USA, provided information on the association between exposure to solar radia-
tion and ocular melanoma. All of these studies demonstrate an increased risk of ocular mela-
noma in people with light skin, light eye colour or light hair colour. Two of the studies
compared effect of southern US birthplace with birth elsewhere in the USA; a significant
difference was seen in the Philadelphia study.
Past residence south of 40 N latitude was positively associated with ocular melanoma in
the Boston study but was not significant in the Philadelphia study after control for southern
birthplace. Although several outdoor activities, such as gardening and sunbathing, were
associated in the Philadelphia study with ocular melanoma, participation in outdoor acti-
vities did not increase risk significantly in Boston or San Francisco.
The lack of consistency of the results of these studies makes their interpretation difficult.
(e) Other cancers
No adequate study was available to evaluate the role of solar radiation in cancers at
other body sites.
5.2.2 Artificial sources of ultraviolet radiation
No adequate study was available on nonmelanocytic skin cancer in relation to exposure
to artificial sources of UVR.
Two case- control studies, one from Scotland and one from Ontario, with detailed infor-
mation on use of sunbeds and sunlamps showed positive relationships between duration of
use and risk of melanoma of the skin. Several other studies with limited information showed
no association.
SUMMARY OF DATA REPORTED AND EVALUATION 221
One case- control study from Sydney, Australia, showed a positive relationship between
melanoma of the skin and exposure to fluorescent lights at work among women, but the
measurement of exposure was crude and among exposed cases there was a relative excess of
melanoma on the trunk, a site likely to be covered at work. A more detailed study from
Australia showed no consistent association between cumulative exposure or rate of exposure
to fluorescent lights and melanoma. Two other studies had detailed information on exposure.
One, from Scotland, showed no such association, while the other, from England, had
inconsistent effects depending on the method of ascertainment of information. Another
study, from New York, with limited information also showed inconsistent effects depending
on the source of information.
1\vo case- control studies, from Boston and Philadelphia, USA, showed significant posi-
tive associations between use of sunlamps and melanoma of the eye. Another case-control
study, from San Francisco, showed an increased risk for exposure to 'UV or black light',
although the nature of the exposure was not specified.
Two studies, from Philadelphia and Montreal, showed significant positive associations
between welding and melanoma of the eye.
5.2.3 Molecular genetics of human skin cancers
Base substitutions in a tumour suppressor gene, p53, found in human squamous-cell skin
carcinomas that had developed at sites exposed to the sun were similar to those found in
experimental systems exposed to UVR, and especially to UVB.
5.3 Carcinogenicity in experimental animals
Solar radiation was tested for carcinogenicity in a series of exceptional studies in mice
and rats. Large numbers of animals were studied, and well-characterized benign and mali-
gnant skin tumours developed in most of the surviving animals. Although the reports are
deficient in quantitative details, the results provide convincing evidence that sunlight is
carcinogenic for the skin of animals.
Broad-spectrum UVR (solar-simulated radiation and ultraviolet lamps emitting mainly
UVB) was tested for carcinogenicity in many studies in mice, to a lesser extent in rats and in a
few experiments in hamsters, guinea-pigs, opossums and fish. Benign and malignant skin
tumours were induced in all of these species except guinea-pigs, and tumours of the cornea
and conjunctiva were induced in rats, mice and hamsters.
The predominant type of tumours induced by UVR in mice is squamous-cell carcinoma.
Basal-cell carcinomas have been observed occasionally in athymic nude mice and rats
exposed to UVR. Melanocytic neoplasms of the skin were shown to develop following expo-
sure of opossums and hybrid fish to broad-spectrum UVR.
Studies in hairless mice demonstrated the carcinogenicity of exposures to UVR in the
wavelength ranges 315- 400 nm (UVA), 280-315 nm (UVB) n d ~ 280 nm (UVC), UVB
radiation being the most effective, followed by UVC and UVA UVB radiation is three to
four orders of magnitude more effective than UVA Both short-wavelength UVA (315-340
nm) and long-wavelength UVA (340-400 nm) induced skin cancer in hairless mice. The
carcinogenic effectiveness of the latter waveband is known only as an average value over the
222 !ARC MONOGRAPHS VOLUME 55
entire range; the uncertainty of this average is about one order of magnitude. In none of the
experiments involving UVC was it possible to exclude completely a contribution ofUVB, but
the size of the effects observed indicate that they cannot be due to UVB alone.
No experimental data were available on the carcinogenicity to animals of radiation from
general lighting fixtures, including fluorescent and quartz halogen lamps.
UVR has been studied in protocols involving two-stage chemical carcinogenesis (substi-
tuting UVR for the chemical initiator or for the chemical promoter or giving it in addition to
both). UVR has been reported to exert many effects on the carcinogenic process, including
initiation, promotion, cocarcinogenicity and even tumour inhibition. Chemical immuno-
suppressive agents have been shown to enhance the probability of developing UVR-induced
tumours in mice.
5.4 Other relevant data
5.4. 1 Transmission and absorption
Studies of transmission in whole human and mouse epidermis and human stratum
corneum in vitro show that these tissues attenuate radiation in the solar UVR range. This
attenuation, which is more pronounced for the UVB than for the UVA wavebands, affords
some protection from solar UVR to dividing cells in the basal layer.
The different components of the human eye act as optical filters for the UVR range.
Consequently, little or no UVR reaches the retina in the normal eye.
5.4.2 Effects on the skin
UVR produces erythema, melanin pigmentation and acute and chronic cellular and
histological changes in humans. Generally consistent changes are seen in experimental
species, including the hairless mouse.
The action spectra for erythema and tanning in humans and for oedema in hairless mice
are similar. UVB is three to four times more effective than UVA in producing erythema. In
humans, pigmentation protects against erythema and histopathological changes. People with
a poor ability to tan, who burn easily and have light eye and hair colour are at a higher risk of
developing melanoma, basal-cell and squamous-cell carcinomas (see section 5.2).
In humans, acquired pigmented naevi and solar keratoses, indicators of melanomas and
squamous-cell carcinomas, respectively, are induced by exposure to the sun.
Xeroderma pigmentosum patients have a high frequency of pigmentary abnormalities
and skin cancers on sun-exposed skin. These patients also have defective DNA repair.
5.4.3 Effects on the immune response
Relatively few investigations have been reported of the effects of UVR on immunity in
humans, but changes do occur. There is evidence that contact allergy is suppressed by
exposure to UVB and possibly to UVA radiation. The number of Langerhans' cells in the
epidermis is decreased by exposure to UVR and sunlight, and the morphological Joss of these
cells is associated with changes in antigen-presenting cell function in the direction of
suppression; this change may be due not only to simple loss of function but also to active
SUMMARY OF DATA REPORTED AND EVALUATION 223
migration of other antigen-presenting cells into the skin. A reduction in natural killer cell
activity also occurs, which can be produced by UVA radiation. These changes are short-lived,
and their functional significance is unknown. Pigmentation of the skin may not protect
against some UVR-induced alterations of immune function.
Several immune responses are suppressed by UVR in mice and other rodents. Sup-
pression of contact hypersensitivity has received most attention, and this response may be
impaired locally, at the site of exposure to radiation, or systemically, at a distant, unexposed
site. The two forms of suppression have different dose dependencies-systemic suppression
requiring much higher doses-and their mechanisms appear to differ, but the efferent limb
of each involves generation of hapten-specific T-suppressor cells that block induction but not
elicitation of contact hypersensitivity. Systemic suppression of delayed hypersensitivity to
injected antigens can also be produced by exposure to UVB radiation, and several obser-
vations suggest that the mechanism of this suppression differs from that of systemic
suppression of contact hypersensitivity.
Alterations in immune function induced by exposure to UVR play a central role in
photocarcinogenesis in mice. UVR-induced T-suppressor cells block a normal immuno-
surveillance system that prevents the growth of highly antigenic UVR-induced tumours. It is
not known whether this mechanism operates in humans.
5.4.4 DNA photoproducts
Solar UVR induces a variety of photoproducts in DNA, including cyclobutane-type
pyrimidine dimers, pyrimidine-pyrimidone (6-4) photoproducts, thymine glycols, cytosine
damage, purine damage, DNA strand breaks and DNA- protein cross-links. Substantial
information on biological consequences is available only for the first two classes. Both are
potentially cytotoxic and can lead to mutations in cultured cells, and there is evidence that
cyclobutane-type pyrimidine dimers may be precarcinogenic lesions. The relative and
absolute levels of each type of lesion vary with wavelength. Substantial levels of thymidine
glycols, strand breaks and DNA-protein cross-links are induced by solar UVA and UVB
radiation, but not by UVC radiation. The ratio of strand breaks to cyclobutane-type dimer
lesions increases as a function of increasing wavelength. In narrow band-width studies, the
longest wavelength at which cyclobutane-type pyrimidine dimers have been observed is 365
nm, whereas the induction of strand breaks and DNA-protein cross-links has been observed
at wavelengths in the UVB, UVA and visible ranges. Non-DNA chromophores such as
porphyrins, which absorb solar UVR, appeared to be important in generating active
intermediates that can lead to damage. Solar UVR also induces membrane damage.
5.4.5 Genetic and related effects
Measurable DNA damage is induced in human skin cells in vivo after exposures to UVA,
UVB and UVC radiation, including doses in the range commonly experienced by humans.
Most of the DNA damage after a single exposure is repaired within 24 h. The importance of
these wavelength ranges depends on several factors. UVB is the most effective, UVC being
somewhat less effective and UVA being much less effective, when compared on a per photon
basis, probably owing to a combination of the biological effectiveness of the different
wavebands and of their absorption in the outer layers of the skin.
Summary tabJe of genetic and related effects of ultraviolet A radiation
Nonmammalian systems Mammalian systems
Prok8 Lower Plants Insects In vitro In
l)'Otes eukaryotes
D
+ + +1 + +1 +' + + +'
A. aneuploidy; C. chromooomal aberrations; D, DNA damage; DI., dominant lethal mutation; G, gene mutation; I, inhibition of intercellular communication; M. micronucl<:i; R, mitotic recombination
and gene S, sister chromatid exchange; T, cell transformation
In completing the tables, tl)e following zymbo/s indica/< the consensus of the Wolking Group wirh rtganf ro lhe ruu/IS for each endpoint:
+ considered to be positive for the specific endpoint and level of biological complexity
+
1
considered to be positive, but only one valid study was available to the Working Group; sperm abnormality, mouse
considered to be negative
considered to be negative, but only one valid study was available lo the Worlcing Group
considered to be equivocal or inconclusive (e.g., there were contradictory results from different laboratories; there were confounding exposures; the results "'ere equivocal)
A
>
s:::
0
z
0
0
6
G
tT1
VI
VI
Summary table of genetic and related effects of ultraviolet B radiation
Nonmammalian systems Mammalian systems
Plants Insects In vitm Jn vivo
D
+ +' + + +l + + + +' + +
A, aneuploidy; C. chromosomal aberrations; D, DNA damage: DL. dominant lethal mutation; G, gene mutation: I, inhibition of mterczllular communication; M, micronuclei: R, mitot ic rerombination
and acne s, SUtor chromatid exchange; T. cell transiormation
ifl completing 1M rablu, 1M follo>Nrg symboh indkau IN. COtJS<ruW of 1M Group with rogard to resulrs for each t ndpoint:
+ considered to be posi tive Cor the specific endpoint and level of biological complexity
+
1
oomidered to be positive, but only one vaUd study was available to the Working Group; spenn &bntmnality, mouse
ronsldered to be negati..:
-
1
considered to be negative, but only one valid study was available to the Working Group
considered to be equivocal or inconclusive (e.g., there were contradictory resull$ from different laboratories: there were confounding exposures; the resultS were equivocal)
A
Vl
c
0
"Tj
tj
>
:;d
m
"'t1
0
tj
m
G
0
z
Summary table of genetic and related effects of ultraviolet C radiation
Nonmammalian systems Mammalian systems
Ptoka Lower Plants Insect In vilro In vivo
ryotcs eukaryotes
D
+ + + + +' + +' +'
+J + +
+ + + + + +' + +
... .. .
A. aneuploidy; C, chromosomal aberrations; 0, DNA damage; DL, dominant lethal mutation; G, gene mutation; I, inhtbition of intcn:ellular mmmunicat10n; M, micronuclei; R, mitotic
and gene conversion; S, sister chromatid exchange; T. cell transformation
In complnirrt tM tables, IM [Dllowillg symboh indiciJ/t lht COI!StllNS o/tM WOJting Group with rqard to rht mulrs for ttJdr endpoint:
+ mnsidcrcd to be positi>e for tbe specific endpoint and level of biological complel<ity
+
1
considered to be posJtiYe, but only one Vlllid study was a>'llilable to the Worklng Group; sperm abnormality, mouse
conaidercd to be negative
-
1
considered 10 be negative, but only one valid srudy was available to the Working Group
? oonaidered to be equivocal or inconclusive (e.g., there contradictory results from differe nt laboratories; there were confounding expo6Ures; the results were equivocal)
A
0
a
a
d
G
tT1
1.11
VI
SUMMARY OF DATA REPORTED AND EVALUATION 227
Solar and 'solar-simulated' radiation and radiation from sunlamps (UVA and UVB) are
mutagenic to prokaryotes and plants, induce DNA damage in fish and in amphibian cells in
vitro, are mutagenic to and induce sister chromatid exchange in amphibian cells, induce
micronucleus formation and transformation in mammalian cells in vitro, are mutagenic to
and induce DNA damage and sister chromatid exchange in human cells in vitro and induce
DNA damage in mammalian skin cells irradiated in vivo.
UVA radiation is mutagenic to prokaryotes and induces DNA damage in fungi. It is
mutagenic to and induces DNA damage, chromosomal aberrations and sister chromatid
exchange in mammalian cells and induces DNA damage and mutation in human cells in vitro.
UVB radiation is mutagenic to prokaryotes and induces chromosomal aberrations in
plants. It is mutagenic to and induces DNA damage, sister chromatid exchange and transfor-
mation in mammalian cells, is mutagenic and induces DNA damage and transformation in
human cells in vitro and induces DNA damage in mammalian skin cells irradiated in vivo.
UVC radiation induces DNA damage in and is mutagenic to prokaryotes, fungi and
plants and induces DNA damage in insects and aneuploidy in yeast. It induces sister
chromatid exchange in amphibian and avian cells in vitro; it is mutagenic to and induces DNA
damage, chromosomal aberrations, sister chromatid exchange and transformation in
mammalian and human cells in vitro; and it induces DNA damage in mammalian skin cells
irradiated in vivo.
UVR in the three wavelength ranges can induce or enhance cellular and viral gene
expression.
5.5 Evaluationl
There is sufficient evidence in humans for the carcinogenicity of solar radiation. Solar
radiation causes cutaneous malignant melanoma and nonmelanocytic skin cancer.
There is limited evidence in humans for the carcinogenicity of exposure to ultraviolet
radiation from sunlamps and sunbeds.
There is inadequate evidence in humans for the carcinogenicity of exposure to fluo-
rescent lighting.
There is inadequate evidence in humans for the carcinogenicity of other sources of arti-
ficial ultraviolet radiation.
There is sufficient evidence for the carcinogenicity of solar radiation in experimental
animals.
There is sufficient evidence for the carcinogenicity of broad-spectrum ultraviolet radia-
tion in experimental animals.
There is sufficient evidence for the carcinogenicity of ultraviolet A radiation in experi-
mental animals.
There is sufficient evidence for the carcinogenicity of ultraviolet B radiation in experi-
mental animals.
1
For defmition of the italicized tenns, see Preamble, pp. 32-35.
228
IARC MONOGRAPHS VOLUME 55
There is sufficient evidence for the carcinogenicity of ultraviolet C radiation in experi-
mental animals.
Overall evaluation
Solar radiation is carcinogenic to humans (Group 1).
Ultraviolet A radiation is probably carcinogenic to humans (Group 2A).
Ultraviolet B radiation is probably carcinogenic to humans (Group 2A).
Ultraviolet C radiation is probably carcinogenic to humans (Group 2A).
Use of sunlamps and sunbeds entails exposures that are probably carcinogenic to humans
(Group 2A).
Exposure to fluorescent lighting is not classifiable as to its carcinogenicity to humans
(Group 3).
6. References
Aberer, W., Schuler, G., Sting!, G., Honigsmann, H. & Wolff, K. (1981) Ultraviolet light depeletes
surface markers of Langerhans cells. J. invest. Dermatol., 76, 202-210
Adam, S.A., Sheaves, J.K., Wright, N.H., Mosser, G., Harris, R.W. & Vessey, M.P. (1981) A case-
control study of the possible association between oral contraceptives and malignant melanoma.
Br. J. Cancer, 44, 45-50
A gin, P.P., Rose, A.P., III, Lane, C. C., Akin, F.J. & Sayre, R.M. (1981a) Changes in epidermal forward
scattering absorption after UVA or UVA-UVB irradiation. J. invest. Dermatol., 16, 174-177
Agin, P.P., Lane, C. C. & Sayre, R.M. (1981b) Ultraviolet irradiation induces optical and structural
changes in the skin of hairless mice. Photochem. Photobiophys., 3, 185-194
AJcalay, J., Freeman, S.E., Goldberg, L.H. & Wolf, J.E. (1990) Excision repair of pyrimidine dimers
induced by simulated solar radiation in the skin of patients with basal cell carcinoma. J. invest.
Dermato/., 95, 506-509
Alter, BJ., Schendel, D.J., Bach, M.L., Bach, F.H., Klein, J. & Stimpfling, J.H. (1973) Cell-mediated
lympholysis. Importance of serologically defined H-2 regions. J. exp. Med., 137, 1303-1309
Ambach, W. & Rehwald, W. (1983) Measurements of the annual variation of the erythema dose of
global radiation. Radial. environ. Biophys., 21, 295-303
American Conference of Governmental Industrial Hygienists (1991) 1991-1992 Threshold Limit
Values for Chemical Substances and Physical Agents and Biological Exposure Indices, Cincinnati,
OH, pp. 123-128
Ananthaswamy, H.N. (1984a) Lethality and transformation of 10T1/2 mouse embryo fibroblast cell
line by various wavelengths of ultraviolet radiation. Photodermatology, I, 265-176
Ananthaswamy, H.N. (1984b) Neoplastic transformation of neonatal mouse skin fibroblasts in
culture after a single exposure to ultraviolet radiation in vivo. Photodennatology, l, 106-113
Ananthaswamy, H.N. & Fisher, M.S. (1981) Photoreactivation of ultraviolet radiation-induced pyri-
midine dimers in neonatal BALB/c mouse skin. Cancer Res., 41, 1829-1833
Ananthaswamy, H.N. & Kripke, M.L. (1981) In vitro transformation of primary cultures of neonatal
BALB/c mouse epidermal cells with ultraviolet-B radiation. Cancer Res., 41, 2882-2890
Ananthaswamy, H.N. & Pierceall, W.E. (1990) Molecular mechanisms of ultraviolet radiation
carcinogenesis. Photochem. Photobiol., 52, 1119-1136
Ananthaswamy, H.N., Price, J .E., Goldberg, L.H. & Bales, E.S. (1988) Detection and identification of
activated oncogenes in human skin cancers occurring on sun-exposed body sites. Cancer Res., 48,
3341-3346
Anderson, D.E. (1963) Effect of pigment on bovine ocular squamous carcinoma. Ann. N.Y. Acad. Sci. ,
100, 436-446
Anderson, R.R & Parrish, J.A. (1981) The optics of human skin. J. invest. Dermatol., 77, 13-19
Anderson, R.R. & Parrish, J.A. {1982) Optical properties of human skin. In: Regan, J.D. & Parrish,
J .A., eds, The Science of Photo-medicine, New York, Plenum, pp. 147-194
-229-
230 IARC MONOGRAPHS VOLUME 55
Anderson. L.M. & Rice. J.M. (1987) Thmorigenesis in athymic nude mouse skin by chemical carcino--
genesis and ultraviolet light. J. natl Cancer Inst., 78. 125-134
Andley, U.P. (1987) Yearly review. Photodamage to the eye. Photochem. Photobiol., 46, 1057-1066
Anon. (1979) Sun-lamps, Solariums, Sunbeds and Health Lamps, London, Which? Consumer Asso-
ciation, pp. 268-272
Anon. (1987) The Truth About Tanning. London. Which? Consumer Association, pp. 214-216
Ansel, J.C., Luger, 'I:A. & Green, I. (1983) The effect of in vitro and in vivo UV irradiation on the
production of ETAF [epidermal cell derived thymocyte-activating factor] activity by human and
murine keratinocytes. J. invest. Dermatol . 81. 519-523
Applegate, LA & Ley, R.D. (1988) Ultraviolet radiation-induced lethality and repair of pyrimidine
dimers in fish embryos. Mutat. Res., 198, 85- 92
Applegate, L.A. & Ley, R.D. (1991) DNA damage is involved in the induction of opacification and
neovascularization of the cornea by ultraviolet radiation. Exp. Eye Res . 52, 493-497
Applegate, L.A., Ley, R.D., Alcalay. J. & Kripke, M.L. (1989) Identification of the molecular target for
the suppression of contact hypersensitivity by ultraviolet radiation. J. exp. Med., 170, 1117-1131
Arlett, C.F. & Harcourt, S.A. (1983) Variation in response to mutagens amongst normal and repair-
defective human cells. In: Lawrence. C.W. ed., Induced Mutagenesis: Molecular Mechanisms and
their Implications for Environmental Protection, New York, Plenum, pp. 249-267
Arlett, C.F, Harcourt, S.A., Cole, J., Green, M.H. & Anstey, A.V. (1992)Acomparisonofthe response
of unstimulated and stimulated T-lymphocytes and fibroblasts from normal. xeroderma pigmen-
tosum and trichothiodystrophy donors to the lethal action ofUV-C. Mutat. Res . 273. 127-135
Armstrong, B.K. (1984) Melanoma of the skin. Br. med. Bull . 40. 346-350
Armstrong, R.B. (1986) Solar urticaria. Dermato/. C/in., 4, 253- 259
Armstrong, B.K. (1988) Epidemiology of malignant melanoma: intermittent or total accumulated
exposure to the sun? J. Dennatol. surg. Onco/., 14, 835-849
Armstrong, B.K., Woodings, 'I:L.. Stenhouse, N.S. & McCall, M.G. (1983) Mortality from Cancer in
Migrants to Australia 1962 to 1971, Perth, University of Western Australia, pp. 21, 81-83
Armstrong, B.K.. Heenan, P.J., Caruso, V., Glancy. R.J. & Holman. C.D.J. (1984) Seasonal variation in
the junctional component of pigmented naevi (Letter to the Editor).Int. J. Cancer. 34.441-442
Armstrong, B.K., de Klerk, N.H. & Holman, C.D.J. (1986) Etiology of common acquired melanocytic
nevi: constitutional variables, sun exposure, and diet. J. nat/ Cancer Inst., 77, 329- 335
Athas, W.F, Hedayati, M.A., Matanoski. G.M., Farmer, E.R. & L. (1991) Development
and field-test validation of an assay for DNA repair in circulating human lymphocytes. Cancer
Res., 51, 5786-5793
Atkin, M., Fenning, J., Heady. J.A., Kennaway, E.L. & Kennaway, N.M. (1949) The mortality from
cancer of the skin and lip in certain occupations. Br. J. Cancer. 3, 1-15
Aubry, F. & MacGibbon, B. (1985) Risk factors of squamous cell carcinoma of the skin. A case-
control study in the Montreal region. Cancer, 55, 907-911
Auerbach, H. (1961) Geographic variation in incidence of skin cancer in the United States. Public
Health Rep . 76. 345-348
Augustsson, A., Stierner, U., Rosdahl, I. & Suurkiila, M. (1990-) Melanocytic naevi in sun-exposed and
protected skin in melanoma patients and controls. Acta denn. venereal., 71, 512-517
Azizova, A.O., Islomov, A.I., Roshchupkin, D.I., Predvoditelev, D.A:, Remizov, A.N. & Vladimirov,
Y.A. (1980) Free radicals formed on ultraviolet irradiation of the lipids of biological membranes.
Biophysics, 24, 407-414
REFERENCES 231
Baadsgaard, 0 ., Fox. D.A. & Cooper, K.D. (1988) Human epidermal cells from ultraviolet light-
exposed skin preferentially activate autoreactive CD4 + 2H4 + suppressor-inducer lymphocytes
and cos+ suppressor/cytotoxic lymphocytes. llmmuno/., l40, 1738-1744
Bach, F.H., Grillot-Courvalin, C., Kuperman, OJ., Sollinger, H. W., Hayes, C., Sonde!, P.M., Alter, B.J.
& Bach, M.L. (1977) Antigenic requirements for triggering of cytotoxic T lymphocytes. Jmmunol.
Rev., 35, 76-96
Bachem, A. (1956) Ophthalmic ultraviolet action spectra. Am. 1 OphthaJmol., 41, 969-975
Baden, H.P. & Pathak, M.A. (1967) The metabolism and function of urocanic acid in skin.l invest.
Dermatol., 48, 11- 17
Balshi, J.D., Francfort, J.W. & Perloff, L.J. (1985) The influence of ultraviolet irradiation on the blood
transfusion effect. Surgery, 98, 243-249
Banerjee, S.K., Christensen, R.B., Lawrence, C.W. & LeClerc, J.E. (1988) Frequency and spectrum of
mutations produced by a single cis- syn thymine- thymine cyclobutane dimer in a single-stranded
vector. Proc. nat/ Acad. Sci. USA, 85, 8141- 8145
Banerjee, S.K., Borden, A., Christensen, R.B., LeClerc, J.E. & Lawrence, C. W. (1990) SOS-Dependent
replication past a single trans-syn T-T cyclobutane dimer gives a different mutation spectrum
and increased error rate compared to replication past this lesion in uninduced cells.l Bacteriol.,
172, 2105-2112
Barrett, J.C., Tsutsui, T. & Ts'o, P.O.P. (1978) Neoplastic tranformation induced by a direct pertur-
bation of DNA. Nature, 274, 229-232
Barrett, S.F., Robbins, J.H., Throne, R.E. & Kraemer, K.H. (1991) Evidence for defective repair of
cyclobutane pyrimidine dimers with normal repair and other DNA photoproducts in a trans-
criptionally active gene transfected into Cockayne syndrome cells. Mutat. Res., 255, 281-291
Barth, C., Knuschke, P. & Barth, J. (1990) Examination of welders exposed to UV radiation (Ger.).
Z. ges. Hyg. , 36, 654-655
Baturay, N.Z., Targovnik. H.S., Reynolds, R.J. & Kennedy, A.R. (1985) Induction of in vitro
transformation by near-uv light and its interaction with Carcinogenesis, 6,
465-468
Beadle, P.C. & Burton, J.L. (1981) Absorption of ultraviolet radiation by skin surface lipid. Br. l
Dennatol., 104, 549- 551
Beardmore, G.L. (1972) The epidemiology of malignant melanoma in Australia. In: McCarthy, W.H.,
ed., Melanoma and Skin Cancer, Sydney, V.C.N. Blight (Goverment Printer), pp. 39-64
Bech-Thomsen, N., Wulf, H.C., Poulsen, t. & Lundgren, K. (1988a) Pretreatment with long-wave
ultraviolet light inhibits ultraviolet-induced skin tumor development in hairless mice. Arch.
Dermato/., 124, 1215-1218
Bech-Thomsen, N., Wulf, H.C. & Lundgren, K. (1988b) Pre-treatment with UVA influences broad-
spectrum UV photocarcinogenesis in hairless mice (Abstract). In: Rikles, E., ed., Proceedings of
the lOth International Congress on Photobiology, Jerusalem, Jerusalem, International Association
of Biology, p. 34
Beer, J.Z. & Zmudzka, B.Z. (1991) Activation of human immunodeficiency virus by radiation. In:
Seymour, C. B. & Mothersill, C., eds, New Developments in Fundamental and Applied Radiology,
London, Taylor & Francis, pp. 113-123
Beer, J .Z., Olvey, K.M., Miller, S.A. & Zmudzka, B.Z. (1991) Studies on the human immunodeficiency
virus promoter induction by UVA and UVB radiation (Abstract). Photochem. Photobiol., 53, 25S
232 IARC MONOGRAPHS VOLUME 55
Beitner, H. (1986) The effect of high dose long-wave ultraviolet radiation (UVA) on epidermal
melanocytes in human skin: a transmission electron microscopic study. Photodermatology, 3,
133-139
Beitner, H. & Wennersten, G. (1983) The immediate action of long-wave ultraviolet radiation (UVA)
on suprabasal melanocytes in human skin: a transmission electron microscopical study. Acta
dermatol. venereal., 63, 328-334
Beitner, H., Norell, S.E., Ringborg, U., Wennersten, G. & Mattson, B. (1990) Malignant melanoma:
aetiological importance of individual pigmentation and sun exposure. Br.l Dermatol., 122,43- 51
Bender, M.A., Griggs, H.G. & Walker, P.L. (1973) Mechanisms of chromosomal aberration produc-
tion. I. Aberration induction by ultraviolet light. Mutat. Res., 20, 387-402
Ben-Hur, E. & Ben-Ishai, R. (1968) Trans- syn thymine dimers in ultraviolet-irradiated denatured
DNA: identification and photoreactivability. Biochim. biophys. Acta, 16(), 9-15
Beral, V. & Robinson, N. (1981) The relationship of malignant melanoma, basal and squamous skin
cancers to indoor and outdoor work. Br. 1 Cancer, 44, 886-891
Beral, V., Evans, S., Shaw, H. & Milton, G. (1982) Malignant melanoma and exposure to fluorescent
lighting at work. Lancet, ii, 290-293
Berg, M. (1987) Ultraviolet radiation in operation rooms. In: Passchier, WF. & Bosnjakovic, B.F.M.,
eds, Human Exposure to Ultraviolet Radiation: Risks and Regulations, Amsterdam, Elsevier, pp.
359- 363
Berger, D.S. (1976) The sunburning ultraviolet meter: design and performance. Photochem. Photo-
bioi., 24, 587-593
Berger, H. & Kaase, H. (1983) Risk for carcinoma from sources of UVA radiation (Ger.). Z. Hautkr.,
58,63
Berger, D.S. & Urbach, F. (1982) A climatology of sunburning ultraviolet radiation. Photochem.
Photobiol., 35, 187-192
Berger, H., Tsambaos, D. & Mahrle, G. (1980a) Experimental elastosis induced by chronic ultraviolet
exposure. Light and electron-microscopic study. Arch. dermatol. Res., 269, 39-49
Berger, H., Tsambaos, D. & Kaase, H. (1980b) Experimental actinic elastosis by chronic exposure to
filtered UVA radiation (Ger.). Z. Hautkr., 55, 1510-1527
Bergstresser, P.R. (1986) Ultraviolet B radiation induces 'local immunosuppression'. Current Probl.
Dermatol., lS, 205-218
Bernhard, J.D., Pathak, M.A., Kochevar, I.E. & Parrish, J .A ( 1987) Abnormal reactions to ultraviolet
radiation. In: Fitzpatrick, TB., Eisen, A.Z., Wolff, K., Freedberg, I.M. & Austen, K.F., eds,
Dermatology in General Medicine, 3rd ed., New York, McGraw-Hill, rp. 1481-1507
Beukers, R. & Berends, W. (1960) Isolation and identification of the irradiation product of thymine.
Biochim. biophys. Acta, 41, 550- 551
Beukers, R., Ylstra, J. & Berends, W (1958) The effect of ultraviolet light on some components of the
nucleic acids. II. In rapidly frozen solutions. ReeL Trav. chim. Pays-Bas, 77, 729- 732
Bielfeld, V., Weichenthal, M., Roser, M., Breitbart, E., Berger, J., Seemanova, E. & Rudiger, H.W.
(1989) Ultraviolet-induced chromosomal instability in cultured fibroblasts . of heterozygote
carriers for xeroderma pigmentosum. Cancer Genet. Cytogenet., 43, 219-226
Bissett, D.L., Hannon, D.P. & Orr, T.V. (1987) An animal model of solar-aged skin: histological,
physical, and visible changes in UV-irradiated hairless mouse skin. Photochem. Photobiol., 46,
367-378
REFERENCES 233
Bissett. D.L., Hannon, D.P. & Orr, T.V. (1989) Wavelength dependence of histological, physical. and
visible changes in chronically UV-irradiated hairless mouse skin. Photochem. Photobiol., SO,
763-769
Blum, H.F. (1948) Sunlight as a causal factor in cancer of the skin of man. J. nat/ /nst. Cancer, 9,
247-258
Blum, H.F. (1959) Carcinogenesis by Ultraviolet Light, Princeton, NJ, Princeton University Press
Blum, H. F..& Lippincott, S. W ( 1942) Carcinogenic effectiveness of ultraviolet radiation of wavelength
2537 A. J. nat/ Cancer lnst., 3, 211-216
Blum, H.F., Butler, E.G., Dailey, T.H., Daube, J.R., Mawe, R.C. & Soffen, G.A. (1959) Irradiation of
mouse skin with single doses of ultraviolet light. J. nat/ Cancer Inst., 22, 979-993
Blumthaler, M., Canaval, H. & Ambach, W (1983) Measurement of erythemally active doses of solar
UVB radiation (Ger.). Z. Med.Meteorol., 2, 14-17
Blumthaler, M., Ambach, W & Daxecker, F. (1985a) Computation of radiation doses from different
solar UVB radiations producing photoelectric keratosis (Ger.). Klin. Mbl. Augenheilk., 186,
275-278
Blumthaler, M., Ambach, W & Canaval, H. (1985b) Seasonal variation of solar UV-radiation at a high
mountain station. Photochem. Photobiol., 42, 147-152
Boettner, E.A. & Wolter, J .R. (1962) Transmission of the ocular media.lnvest. Ophthalmol., l, 776-783
Bootsma, D. & Hoeijmakers, J .H.J. (1991) The genetic basis of xeroderma pigmentosum.An1L Genet. ,
34, 143-150
Borek, C., Ong, A. & Mason, H. (1989) Ozone and ultraviolet light act as additive cocarcinogens to
induce in vitro neoplastic transformation. Teratog. Carcinog. Mutag., 9, 71-74
Bos, A.JJ. & de Haas, M.P. (1987) On the safe use of a high power ultraviolet laser. In: Passchier, WF.
& Bosnjakovic, B.F.M., eds, Human Exposure to Ultraviolet Radiation: Risks and Regulations,
Amsterdam, Elsevier, pp. 377-382
Bose, B., Agarwal, S. & Chatterjee, S.N. (1989) UVA induced lipid peroxidation in liposomal
membrane. Radiat. environ. Biophys., 28, 59-65
Bouissou, H., Pieraggi, M.-T., Julian, M. & Savit, T. (1988) The elastic tissue of the skin. A comparison
of spontaneous and actinic (solar) aging. Int. J. Dermato/., 27, 327-335
Bowden, G.T., Trosko, J .E., Shapas, B.G. & Boutwell, R.K (1975) Excision of pyrimidine dimers from
epidermal DNA and nonsemiconservative epidermal DNA synthesis following ultraviolet irra
diation of mouse skin. Cancer Res., 35, 3599-3607
Bowker, K. W & Longford, A.R. (1987) Ultraviolet radiation hazards from the use of solaria. In:
Passchier, WF. & Bosnjakovic, B.F.M., eds, Human Exposure to Ultraviolet Radiation: Risks and
Regulations, Elsevier, pp. 365-369
Boyd, R. W (1983) Radiometry and the Detection of Optical Radiation, New York, John Wiley & Sons
Boyle, J., MacKie, R.M., Briggs, J .D., Junor, B.J.R. & Aitchison, T.C. (1984) Cancer, warts and sun-
shine in renal transplant patients. A case-control study. Lancet, i, 702-705
Bradley, MO. & Sharkey, N.A. (1977) Mutagenicity and toxicity of visible fluorescent light to cultured
mammalian cells. Nature, 266, 724-726
Bradley, M.O., Hsu, I. C. & Harris, C.C. (1979) Relationships between sister chromatid exchange and
mutagenicity, toxicity and DNA damage. Nature, 282, 318-320
Brash, D.E. & Haseltine, WA. (1982) UV-Induced mutation hotspots occur at DNA damage hot-
spots. Nature, 298, 189-192
234 IARC MONOGRAPHS VOLUME 55
Brash, D.E., Rudolph, J.A., Simon, J.A., Lin, A., McKenna, GJ., Baden, H.P., Halperin, AJ. &
Ponten, J. (1991) A role for sunlight in skin cancer: UV-induced p53 mutations in squamous cell
carcinoma. Proc. nat/ Acad. Sci. USA, 88, 10124-10128
Bred berg. A., Kraemer, KH. & Seidman, M.M. (1986) Restricted ultraviolet mutational spectrum in a
shuttle vector propagated in xeroderma pigmentosum cells. Proc. nat/ Acad. Sci. USA, 83,
8273-8277
Bridges, B.A. (1988) Mutagenic DNA repair in Escherichia coli. XVI. Mutagenesis by ultraviolet light
plus delayed photoreversaJ in recA strains. Mutat. Res., 198, 343-350
Bridges, B.A. (1990) Sunlight, DNA damage and skin cancer: a new perspective. Jpn. J. Cancer Res.,
81, 105-107
Bridges, B.A. & Bates, H. (1990) Mutagenic DNA repair in Escherichia coli. VIII. Involvement of
DNA polymerase III a:-subunit (DnaE protein) in mutagenesis after exposure to UV light.
Mutagenesis, 5, 35-38
Bridges, B.A. & Brown, G.M. (1992) Mutagenic repair in Escherichia coli. XXI. A stable SOS..
inducing signal persisting after excision repair of ultraviolet damage. Mutat. Res. (in press)
Bridges, B.A., Woodgate, R., Ruiz-Rubio, M., Sharif, F., Sedgwick, S.G. & Hiibscher, U. (1987)
Current understanding of UV-induced base pair substitution mutation in E. coli with particular
reference to the DNA polymerase III complex. Mutat. Res., 181, 219-226
Broughton, B.C., Lehmann, A.R., Harcourt, S.A., Arlett, C.F., Sarasin, A., Kleijer, WJ., Beemer, F.A.,
Nairn, R. & Mitchell, D.L. (1990) Relationship between pyrimidine dimers, 6-4 photoproducts,
repair synthesis and cell survival: studies using cells from patients with trichothiodystrophy.
Mutat. Res . 235, 33-40
Brown, L.R. & Wuthrich, K. (1977) A spin label study of lipid oxidation catalyzed by heme proteins.
Biochim. biophys. Acta, 464, 356-369
Brown, J., Kopf, A.W., Rigel, D.S. & Fridman, R.J. (1984) Malignant melanoma in World War II
veterans. Int. J. Dermatol. , 23, 661-663
Bruggers, J .H.A., de Jong, W.E., Bosnjakovic, B.F.M. & Passchier, W.F. (1987) Use of artificial tanning
equipment in the Netherlands. In: Passchier, W.F. & Bosnjakovic, B.F.M., eds, Human Exposure
to Ultraviolet Radiation: Risk and Regulations, Amsterdam, Elsevier, pp. 235-239
Bruls, W.A.G., Slaper, H., van der Leun, J .C. & Berrens, L. (1984a) Transmission of human epidermis
and stratum corneum as a function of thickness in the ultraviolet and visible wavelengths.
Photochem. Photobio/., 40, 485-494
Bruls, W.A.G., van Weelden, H. & van der Leun, J .C. (1984b) Transmission of UV-radiation through
human epidermal layers as a factor influencing the minimal erythema dose. Photochem.
Photobiol., 39, 63-67
Bruyneel-Rapp, F., Dorsey, S.B. & Guin, J.D. (1988) The tanning salon: an area survey of equipment,
procedures, and practices. J. Am A cad. DermatoL, 18, 1030-1038
Burki, H.J. & Lam, C.K (1978) Comparison of the lethal and mutagenic effects of gold and white fluo-
rescent lights on cultured mammalian cells. Mutat. Res., 54, 373-377
Burnet, F.M. (1971) Implications of immunological surveillance for cancer therapy. Isr. J. med. Sci., 1,
9-16
Calkins, J., Selby, C. & Enoch, H. G. (1987) Comparison of UV action spectra for lethality and muta-
tion in Salmonella typhimurium using a broad band source and monochromatic radiations.
Photoclwn. Photobio/., 45, 631-636
REFERENCES 235
Cameron, L.L., Vitasa, B.C., Lewis, P.G., Taylor, H.R. & Emmett, E.A. (1988) Visual assessment of
facial elastosis using photographs as a measure of cumulative ultraviolet exposure. Photo-
demwtology, 5, 277-282
Caplan, R.M. (1967) Medical uses of the Wood's lamp. J. Am. med. Assoc. , 202, 1035-1038
Cavard, C., Zider, A., Vernet, M., Bennoun, M., Saragosti, S., Grimber, B. & Briand, P. (1990) In vivo
activation by ultraviolet rays of the human immunodeficiency virus type 1long terminal repeat.
J. clin. Invest., 86, 1369-1374
Cerutti, P.A. (1981) Measurement of thymine damage induced by oxygen radical species. In:
Friedberg, E.C. & Hanawalt, P.C., eds, DNA Repair. A Laboratory Manual of Research
Procedures, Vol. 1, Part A, New York, Marcel Dekker, pp. 57--68
Cerutti, P.A. & Netrawali, M. (1979) Formation and repair of DNA damage induced by indirect action
of ultraviolet light in normal and xeroderma pigmentosum skin fibroblasts. Radial. Res., Suppl.,
423-432
Cesarini, J.-P. & Muel, B. (1989) Erythema induced by quartz-halogen sources. Photodennatology, 6,
222-227
Challoner, A.V.J., Corless, D., Davis, A., Deane, G.H.W., Diffey, B.L., Gupta, S.P. & Magnus, I.A
( 1976) Personnel monitoring of exposure to ultraviolet radiation. C/in. exp. Dermatol., l , 175-179
Challoner, A.V.J., Corbett. M.F., Davis, A., Diffey, B.L., Leach, J.F. & Magnus, I.A. (1978) Des-
cription and application of a personal ultraviolet dosimeter: a review of preliminary studies. Nat/
Cancer Inst. Monogr., 50, 97- 100
Chamberlain, J. & Moss, S.H. (1987) Lipid peroxidation and other membrane damage produced in
Escherichia coli K1060 by near-UV radiation and deuterium oxide. Photochem. Photobiol., 45,
625--630
Chan, G.L. & Little, J.B. (1976) Induction of oncogenic transformation in vitro by ultraviolet light.
Nature, 264, 442-444
Chan, G.L & Little, J.B. (1979) Correlation of in vitro transformation with in vivo tumorigenicity in
10'Ph mouse cells exposed to UV light. Br. J. Cancer, 39, 590-593
Chan, G.L, Peak, M.J., Peak, J.G. & Haseltine, W.A. (1986) Action spectrum for the formation of
endonuclease-sensitive sites and (6-4) photoproducts induC'ed in a DNA fragment by ultraviolet
radiation. Int. J. Radial. Bioi . 50, 641--648
Chao, C.C.-K. & Rosenstein, B.S. (1985) Induction of sister-chromatid exchanges in ICR 2A frog cells
exposed to 254 nm and solar UV wavelengths. Photochem. Photobiol., 41, 625-627
Chao, C.C.-K. & Rosenstein, B.S. (1986) Use of metabolic inhibitors to investigate the excision repair
of pyrimidine dimers and non-dimer DNA damages induced in human and ICR 2A frog cells by
solar ultraviolet radiation. Photochem. Photobio/., 43, 165-170
Chu, E.H. Y. (1965a) Effects of ultraviolet radiation on mammalian cells. I. Induction of chromosome
aberrations. Mutat. Res., 2, 75-94
Chu, E.H.Y. (1%5b) Effects of ultraviolet radiation on mammalian ceJls. II. Differential UV and x-ray
sensitivity of chromosomes to breakage in 5-aminouracil synchronized cell populations.
Genetics, 52, 1279-1294
Chung, H.-T., Burnham, O.K., Robertson, B., Roberts, L.K. & Daynes, R.A (1986) Involvement of
prostaglandins in the immune alterations caused by the exposure of mice to ultraviolet radiation.
J. Immuno/., 137, 2478-2484
Churchill, M.E., Peak, J.G. & Peak, M.J. (1991) Correlation between cell survival and DNA single-
strand break repair proficiency in the Chinese hamster ovary cell lines AA8 and EM9 irradiated
with 365-nm ultraviolet A radiation. Photochem. Photobiol., 53, 229-236
236 IARC MONOGRAPHS VOLUME 55
Cieminis, K.G.K., Raneeliene, V.M., Prijalgauskiene, A.J., Tiunaitiene, N.V., Rudzianskaite, A.M. &
Jancys, Z.J. (1987) Chromosome and DNA damage and their repair in higher plants irradiated
with short-wave ultraviolet light. Mutat. Res., 181, 9- 16
Claas, F.H.J., Rothert, M., Havinga, 1., Schothorst, A.A., Vermeer, B.-J. & van Rood, J.J. (1985)
Influence of ultraviolet radiation treatment on the survival of heterotopic skin grafts in the
mouse.l invest. Dermatol., 84, 31- 32
Clark, J .H. (1964) The effect oflong ultraviolet radiation in the development oftumors induced by 20-
methylcholanthrene. Cancer Res., 24, 207-211
Cleaver, J.E. (1968) Defective repair replication of DNA in xeroderma pigmentosum. Nature, 218,
652-656
Cleaver, J.E. & Kraemer, K.H. (1989) Xeroderma pigmentosum. In: Scriver, C.R., Beaudet, A.L., Sly,
WS. & Valle, D., eds, The Metabolic Basis of Inherited Disease, New York, McGraw-Hill,
pp. 2949-2971
Clemmesen, J. (1965) Statistical Studies in the Aetiology of Malignant Neoplaims. I. Review and Results,
Copenhagen, Munksgaard, p. 409
Cole, C.A., Forbes, P.D., Davies, R.E. & Urbach, F. (1985) Effect of indoor lighting on normal skin.
Ann. NY. Acad. Sci., 453, 305-316
Cole, C.A., Forbes, P.O. & Davies, R.E. (1986) An action spectrum for UV photocarcinogenesis.
Photochem. Photobiol., 43, 275-284
Colella, C.M., Bogani, P., Agati, G. & Fusi, F. (1986) Genetic effects of UVB: mutagenicity of 308 nm
light in Chinese hamster V79 cells. Photochem. Photobiol., 43, 437-442
Commission Internationale de I'Eclairage (International Commission on Illumination) (1987) Voca-
bulaire International de I' Eclairage [International Lighting Vocabulary] (CIE Publication No.
17.4), 4th ed., Geneva, Bureau Central de Ia Commission Electrotechnique Internationale, p. 3
Coohill, T.P., Peak, MJ. & Peak, J.G. (1987) The effects of the ultraviolet wavelengths of radiation
present in sunlight on human cells in vitro. Photochem. Photobiol., 46, 1043- 1050
Cooke, K.R. & Fraser, J. (1985) Migration and death from malignant melanoma. Int. 1. Cancer, 36,
175-178
Cooke, A. & Johnson, B.E. (1978) Dose response, wavelength dependence and rate of excision of
ultraviolet radiation induced pyrimidine dimers in mouse skin DNA. Biochim. biophys. Acta,
517, 24-30
Cooke, K.R., Skegg, D.C. G. & Fraser, J. ( 1984) Socio-economic status, indoor and outdoor work, and
malignant melanoma. Int. J. Cancer, 34, 57-62
Cooper, K.D., Fox, P., Neises, G. & Katz, S.I. (1985) Effects of ultraviolet radiation on human
epidermal cell alloantigen presentation: initial depression of Langerhans cell-dependent
function is followed by the appearance of T6-nr+ cells that enhance epidermal alloantigen
presentation.l Immuno/., 134, 129-137
Cooper, K.D., Neises, G.R. & Katz, S.I. (1986) Antigen-presenting OKM5 + melanophages appear in
human epidermis after ultraviolet radiation. 1 invest. Dennatol., 86, 363-370
Corominas, M., Kamino, H., Leon, J. & Pellicer, A. (1989) Oncogene activation in human benign
tumors of the skin (keratoacanthomas): Is H-ras involved in differentiation as well as proli-
feration? Proc. nat/ Acad. Sci. USA, 86, 6372-6376
Cox, C. WJ. (1987) Ultraviolet irradiance levels in welding processes. In: Passchier, WF. &
Bosnjakovic, B.F.M., eds, Human Exposure to Ultraviolet Radiation: Risks and Regulations,
Amsterdam, Elsevier, pp. 383-386
REFERENCES 237
Cripps, DJ., Horowitz, S. & Hong, R. (1978) Spectrum of ultraviolet radiation on human B and T
lymphocyte viability. Clin. e.xp. Dermatol., 3, 43-50
Cristofolini, M., Franceschi, S., Tasin, L., Zumiani. G., Piscioli, F., Talamini, R. & LaVecchia. C.
(1987) Risk factors for cutaneous malignant melanoma in a northern Italian population. Int. J.
Cancer, 39, 150-154
Crombie, I.K. (1981) Distribution of malignant melanoma on the body surface. Br. J. Cancer, 43,
842-849
Cullen, A.P. (1980) Additive effects of ultraviolet radiation. Am. J. Optometry physiol. Optics, 51,
808-814
Cunningham, M.L., Johnson, J.S., Giovanazzi, S.M. & Peak, M.J. (1985) Photosensitized production
of superoxide anion by monochromatic (290-405 nm) ultraviolet irradiation of NADH and
NADPH coenzymes. Photochem. Photobiol., 42, 125-128
Czernielewski, J.M., Masouye, I., Pisani, A., Ferracin, J., Auvotat, D. & Ortonne, J.-P.(1988)Effectof
chronic sun exposure on human Langerhans cell densities. Photodermatology, 5, 116-120
Czochratska, B., Kawczynski, W., Bartosz, G. & Shugar, D. (1984) Oxidation of excited-state NADH
and NAD dimer in aqueous medium-involvement of Oz- as a mediator in the presence of
oxygen. Biochim. biophys. Acta, 801, 403-409
D'Ambrosio, S.M., Slazinski, L., Whetstone, J.W & Lowney, E. (1981) Excision repair ofUV-induced
pyrimidine dimers in human skin in vivo. J. invest. Dermatol., 77, 311-313
D'Ambrosio, S.M., Bisaccia, E., Whetstone, J.W., Scarborough, D.A. & Lowney, E. (1983) DNA
repair in skin of lupus erythematosus following in vivo exposure to ultraviolet radiation. J. invest.
Dermatol., 81, 452-454
Dan pure, H.J. & Tyrrell, RM. (1976) Oxygen-dependence of near-UV (365 nm) lethality and the inter-
action of near-UV and x-rays in two mammalian cell lines. Photochem. Photobiol., 23, 171-177
Dardanoni, L., Gafa, L., Paterno, R. & Pavone, G. (1984) A case-control study on lip cancer risk
factors in Ragusa (Sicily). Int. J. Cancer, 34, 335-337
Davies, R.E. & Forbes, P.O. (1988) Retinoids and photocarcinogenesis: a review. J. Toxicol. cutaneous
ocul. Toxico/., 7, 241-253
Davies, R.E., Dodge, H.A. & DeShields, L.H. (1972) AJteration of the carcinogenic activity of
7,12-dimethylbenz(a)anthracene (DMBA) by light (Abstract no. 54). Proc. Am. Assoc. Cancer
Res., 13, 14
Davis, A. & Sims, D. (1983) Weathering of Polymers, London, Applied Science
Daynes, R.A., Spellman, C.W, Woodward, J.G. & Stewart, D.A. (1977) Studies into the transplanta-
tion biology of ultraviolet light-induced tumors. Transplantation, 23, 343- 348
Daynes, R.A., Spikes, J.D. & Krueger, G. (1983) Experimental and Clinical Photoimmuno/ogy, Vols I
and II, Boca Raton, FL, CRC Press
Dearden, S.J., Hunter, TF & Philp, J. (1981) Bilayer microviscosity changes due to Oz (
1
.t..g) peroxi-
dation in lipid vesicles. Chern. Phys. Lett., 81, 606-609
Dearden, S.J ., Hunter, TF. & Philp, J. (1985) Fatty acid analysis as a function of photo-oxidation in egg
yolk lecithin vesicles. Photochem Photobiol., 41, 213-215
De Fabo, E.C. & Kripke, M.L. (1980) Wavelength dependence and dose-rate independence of UV
radiation-induced immunologic unresponsiveness of mice to a UV-induced fibrosarcoma.
Photo<:hem Photobiol., 32, 183-188
De Fabo, E. C. & Noonan, F.P. (1983) Mechanism of immune suppression by ultraviolet irradiation
in vivo. I. Evidence for the existence of a unique photoreceptor in skin and its role in photo-
immunology. J. e.xp. Med., 157, 84-98
238 IARC MONOGRAPHS VOLUME 55
De Flora, S., Camoirano, A., Izzotti, A. & Bennicelli, C. (1990) Potent genotoxicity of halogen lamps,
compared to fluorescent light and sunlight. Carcinogenesis, 11, 2171-2177
Denkins, Y ., Fidler, IJ. & Kripke, M.L (1989) Exposure of mice to UVB radiation suppresses delayed
hypersensitivity to Candida albicans. Photochem. Photobio/., 49, 615-619
Desai, I.D., Sawant, P.L. & Tappet, A.L. (1964) Peroxidative and radiation damage to isolated Iyso-
somes. Biochim. biophys. Acta, 86, 277-2135
De Weerd-Kastelein, E.A., Keijzer, W., Rainaldi, G. & Bootsma, D. (1977) Induction of sister chro-
matid exchanges in xeroderma pigmentosum cells after exposure to ultraviolet light. Mutat. Res.,
45, 253-261
Diffey, B.L (1982) The consistency of studies of ultraviolet erythema in normal human skin. Phys.
med. Bioi., 21, 715-720
Diffey, B.L. (1986) Use of UVA sunbeds for cosmetic tanning. Br. I Dermato/., 115, 67-76
Diffey, B. (1987a) A comparison of dosimeters used for solar ultraviolet radiometry. Photochem.
Photobiol., 46, 55-60
Diffey, B.L. (1987b) Analysis of the risk of skin cancer from sunlight and solaria in subjects living in
northern Europe. Photodermatology, 4, 118-126
Diffey, B.L. (1987c) Cosmetic and medical applications of ultraviolet radiation: risk evaluation and
protection techniques. In: Passchier, W.F. & Bosnjakovic, B.F.M., eds, Human Exposwe to Ultra-
violet Radiation: Risks and Regulations, Amsterdam, Elsevier, pp. 305-315
Diffey, B.L. (1988) The risk of skin cancer from occupational exposure to ultraviolet radiation in
hospitals. Phys. med. BioL, 33, 1187-1193
Diffey, B.L. (1989a) Ultraviolet radiation and skin cancer. Are physiotherapists at risk? Physio-
therapy, 15, 615-616
Diffey, B.L. (1989b) Ultraviolet radiation dosimetry with polysulphone film. In: Diffey, B.L., ed.,
Radiation Measurement in Photobiology, London, Academic Press, pp. 135- 159
Diffey, B.L. (1990a) Human exposure to ultraviolet radiation. Semin. Dermatol., 9, 2- 10
Diffey, B.L. (1990b) Ultraviolet radiation lamps for the phototherapy and photochemotherapy of skin
disease. In: Champion, R.H. & Pye, R.J., eds, Recent Advances in Dermatology, Vol. 8,
Edinburgh, Churchill Livingstone, pp. 21-40
Diffey, B.L. (1991) Solar ultraviolet radiation effects on biological systems. Phys. med. Bioi., 36, 299-
328
Diffey, B.L. & Farr, P.M. (1987) An appraisal of ultraviolet lamps used for the phototherapy of
psoriasis. Br. 1 Dermatol., 117, 49-56
Diffey, B.L. & Farr, P.M. (1989) The normal range in diagnostic phototesting. Br. J. Dermatol., 120,
517-524
Diffey, B.L. & Farr, P.M. (1991a) Quantitative aspects of ultraviolet erythema. Clin. phys. physiol.
Meas., 12, 311-325
Diffey, B.L. & Farr, P.M. (1991b) Tanning with UVB or UVA: an appraisal of risks. / Photochem.
Photobiol. B. Bioi., 8, 219-223
Diffey, B.L. & Langley, F. C. (1986) Evaluation of Ultraviolet Radiation Hazards in Hospitals (Report
No. 49), London, Institute of Physical Sciences in Medicine
Diffey, B.L. & McKinlay, A.F. (1983) The UVB content of 'UVA fluorescent lamps' and its erythemal
effectiveness in human skin. Phys. med. Bioi., 28, 351-358
Diffey, B.L., Kerwin, M. & Davis, A. (1977) The anatomical distribution of sunlight. Br. I Dennatol.,
97,407-410
REFERENCES 239
Diffey, B.L., Tate, T.J. & Davis, A. (1979) Solar dosimetry of the face: the relationship of natural
ultraviolet radiation exposure to basal cell carcinoma localisation. Phys. med. Bioi., 24, 931-939
Diffey, B.L., Challoner, A.V.J. & Key, PJ. (1980) A survey of the ultraviolet radiation emissions of
photochemotherapy units. Br. l Dermatol., 102, 301- 306
Diffey, B.L., Larko, 0., Meding, B., Edeland, H.G. & Wester, U. (1986) Personal monitoring of
exposure to ultraviolet radiation in the car manufacturing industry.Ann. occup. Hyg. , 30, 163-170
Diffey, B.L., Farr, P.M. & Oakley, A.M. (1987) Quantitative studies on UVA-induced erythema in
human skin. Br. l Dermatol., 117, 57-66
DiPaolo, J.A. & Donovan, P.J. (1976) In vitro morphologic transformation of Syrian hamster cells by
UV-irradiation is enhanced by X-irradiation and unaffected by chemical carcinogens. Int. l
radiat. Bioi., 30, 41-53
Doda, D.D. & Green, A.E.S. (1980) Surface reflectance measurements in the UV from an airborne
platform. Part 1. Appl. Optics, 19, 2140-2145
Doll. R. (1991) Urban and rural factors in the aetiology of cancer. Int. J. Cancer, 41, 803-810
Doll, R., Muir, C. & Waterhouse, J., eds (1970) Cancer Incidence in Five Continents, Vol. IL Berlin,
Springer
Doniger, J., Jacobson, E.D., Krell, K. & DiPaolo, J.A. (1981) Ultraviolet light action spectra for
neoplastic transformation and lethality of Syrian hamster embryo cells correlate with spectrum
for pyrimidime dimer formation in cellular DNA. Proc. nat/ Acad. Sci. USA, 78, 2378-2382
Dorado, G., Steingrimsdottir, H., Arlett, C.F. & Lehmann, A.R. (1991) Molecular analysis of ultra-
violet-induced mutations in a xeroderma pigmentosum cell line. J. mol. Bioi., 217, 217- 222
Dorn, H.F. (1944a) Illness from cancer in the United States. Public Health Rep., 59, 33-48
Dorn, H. F. (1944b) Illness from cancer in the United States: IV. Illness from cancer of specific sites
classed in broad groups. Public Health Rep., 59, 65- 77
Dom, H.F. (1944c) Illness from cancer in the United States: VI. Regional differences in illness from
cancer. Public Health Rep., 59, 97-114
Dorn, C.R., Taylor, D.O.N. & Schneider, R. (1971)Sunlight exposure and risk of developing cutaneous
and oral squamous cell carcinomas in white cats. l nat/ Cancer Inst., 46, 1073-1078
Doudney, C.O. (1976) Mutation in ultraviolet light-damaged microorganisms. In: Wang, S.Y., ed.,
Photochemistry and Photobiology of Nucleic Acids, Vol. 2, New York, Academic Press, pp. 309-374
Dougherty, M.A., McDermott, RJ. & Hawkins, MJ. (1988) A profile of users of commercial tanning
salons. Health Values, 12, 21-28
Dreosti, I.E., Baghurst, P.A., Partick, EJ . & Turner, J. (1990) Induction of micronuclei in cultured
murine splenocytes exposed to elevated levels of ferrous ions, hydrogen peroxide and ultraviolet
irradiation. Mutat. Res., 244, 337-343
Drobetsky, E.A. & Glit;kman, B.W. (1990) The nature of ultraviolet light-induced mutations at the
heterozygous aprt locus in Chinese hamster ovary cells. Mutat. Res., 232, 281-289
Dubin, N . Moseson, M. & Pasternack, B.S. (1986) Epidemiology of malignant melanoma: pigmentary
traits, ultraviolet radiation, and the identification of high-risk populations. Recent Results Cancer
Res., 102, 56-75
Dubin, N., Moseson, M. & Pasternack, B.S. (1989) Sun exposure and malignant melanoma among
susceptible individuals. Environ. Health Perspectives, 81, 139-151
Eaton, GJ., Custer, R.P. & Crane, A.R. (1978) Effects of ultraviolet light on nude mice. Cutaneous
carcinogenesis and possible leukemogenesis. Cancer, 42, 182-188
Ebbesen, P. (1981) Enhanced lymphoma incidence in BALB/c mice after ultraviolet light treatment.
J. nat/ Cancer Inst., 67, 1077-1078
240 IARC MONOGRAPHS VOLUME 55
Eggset, G., Volden, G. & Krokan, H. (1983) UV-Induced DNA damage and its repair in human skin
in vivo studied by sensitive immunohistochemical methods. Carcinogenesis, 4, 745-750
Eggset, G., Krokan, H. & Volden, G. (1986) UV-Induced DNA damage and its repair in tanned and
untanned human skin in vivo. Photobiochem. Photobiophys., 10, 181-187
Eisenstark, A (1987) Mutagenic and lethal effects of near-ultraviolet radiation (290-400 nm) on
bacteria and phage. Environ. mol. Mutag., 10, 317-337
Eklund, G. & Malec, E. (1978) Sunlight and incidence of cutaneous malignant melanoma. Effect of
latitude and domicile in Sweden. Scand. J. plast. reconstr. Surg., 12, 231-241
Elkind, M.M. & Han, A (1978) DNA single-strand lesions due to 'sunlight' and UV light: a compa-
rison of their induction in Chinese hamster and human cells, and their fate in Chinese hamster
cells. Photochem. Photobio/., 21, 717-724
Ellison, M.J. & Childs, J.D. (1981) Pyrimidine dimers induced in Escherichia coli DNA by ultraviolet
radiation present in sunlight. Photochem. Photobio/., 34, 465-469
Elmets, C.A, Bergstresser, P.R., Tigelaar, R.E., Wood. P.J. & Streilein, J.W. (1983) Analysis of the
mechanism of unresponsiveness produced by haptens painted on skin exposed to low dose ultra-
violet radiation. ! exp. Med., 158, 781-794
Elmets, C.A, LeVine, MJ. & Bickers, D.R. (1985) Action spectrum studies for induction of immuno-
logic unresponsiveness to dinitrofluorobenzene following in vivo low dose ultraviolet radiation.
Photochem. Photobiol., 42, 391-397
Elmets, C.A, Larson, K., Urda, G.A. & Schacter, B. (1987) Inhibition of postbinding target cell lysis
and of lymphokine-induced enhancement of human natural killer cell activity by in vitro expo-
sure to ultraviolet B radiation. Cell. lmmunol. , 104, 47-58
Elwood, J.M. (1989a) Epidemiology and control of melanoma in white populations and in Japan.
1 invest. Derrntltol., 92, 214S- 221S
Elwood, J.M. (1989b) Epidemiology of melanoma: its relationship to ultraviolet radiation and ozone
depletion. In: Jones, R.R. & Wigley, T., eds, Ozone Depletion. Health and Environmental
Consequences, New York, John Wiley & Sons, pp. 169-189
Elwood, J.M. & Gallagher, R.P. (1983) Site distribution of malignant melanoma. Can. med. Assoc. J.,
128, 1400-1404
Elwood, J .M., Lee, J .A. H., Walter, S.D., Mo, T. & Green, A.E.S. (1974) Relationship of melanoma and
other skin cancer mortality to latitude and ultraviolet radiation in the United States and Canada.
Int. J. Epidemiol., 3, 325-332
Elwood, J.M., Gallagher, R.P., Hill, G.B., Spinelli, J.J., Pearson, J.C.G. & Threlfall, W. (1984)
Pigmentation and skin reaction to sun as risk factors for cutaneous melanoma: Western Canada
Melanoma Study. Br. med. J., 288, 99-102
Elwood, J.M., Gallagher, R.P., Davison. J. & Hill, G.B. (1985a) Sunburn, suntan and the risk of cuta-
neous malignant melanoma: the Western Canada Melanoma Study. Br.l Cancer, 51, 543-549
Elwood, J.M., Gallagher, R.P., Hill, G.B. & Pearson, J.C.G. (1985b) Cutaneous melanoma in relation
to intermittent and constant sun exposure: the Western Canada Melanoma Study. Int.l Cancer,
35, 427-433
Elwood, J.M., Williamson, C. & Stapleton, PJ. (1986) Malignant melanoma in relation to moles,
pigmentation, and exposure to fluorescent and other lighting sources. Br. 1 Cancer, 53, 65-74
Elwood, J.M., Gallagher, R.P., Worth, A.J., Wood, W.S. & Pearson, J.C.G. (1987) Etiological
differences between subtypes of cutaneous malignant melanoma: Western Canada Melanoma
Study. l nat/ Cancer Inst., 18, 37-44
REFERENCES 241
Elwood, J.M., Whitehead, S.M., Davison. J., Stewart, M. & Galt, M. (1990) Malignant melanoma in
England: risk associated with naevi, freckles, social class, hair colour, and sunburn. Int J.
Epidemiol., 19, 801-810
Emmett, E.A. (1973) Ultraviolet radiation as a cause of skin tumors. Crit. Rev. Toxicol., 2, 211-255
Emmett, E.A. & Horstman, S. W (1976) Factors influencing the output of ultraviolet radiation during
welding. J. occup. Med., 18, 41-44
Engel, A., Johnson, M.-L. & Haynes, S.G. (1988) Health effects of sunlight exposure in the United
States. Results from the first National Health and Nutrition Examination Survey, 1971-1974.
Arch. Dermatol., 124, 72- 79
English, D.R.. Rouse, I.L., Xu, Z., Watt, J.D., Holman, C.D.J., Heenan, P.J. & Armstrong, B.K. (198))
Cutaneous malignant melanoma and fluorescent lighting. J. nat/ Cancer Inst., 74, 1191-1197
Enninga, I.C., Groenendijk, R.T.L., Filon, A.R., van Zeeland, A.A. & Simons, J.WI.M. (1986) The
wavelength dependence of UV-induced pyrimidine dimer formation, cell killing and mutation
induction in human diploid skin fibroblasts. Carcinogenesis, 1, 1829-1836
Epstein, J .H. (1965) Comparison of the carcinogenic and cocarcinogenic effects of ult raviolet light on
hairless mice. J. nat/ Cancer Inst. , 34, 741- 745
Epstein, J.H. (1985) Animal models for studying photocarcinogenesis. In: Maibach, H. & Lowe, N.,
eds, Models in Dermatology, Vol.2, Basel, Karger, pp. 30>--312
Epstein, J .H. (1988) Photocarcinogenesis promotion studies with benzoyl peroxide (BPO) and croton
oil. J. invest. Dermatol. , 91, 114- 116
Epstein, J.H. (1990) Induction of melanomas in experimental animals. Photodermatol. Photo-
immunol. Photomed., 1, 95-97
Epstein, J.H. & Epstein, WL. (1962) Cocarcinogenic effect of ultraviolet light on DMBA tumor
initiation in albino mice. J. invest. Dermatol., 39, 455-460
Epstein, J.H. & Epstein, WL. (1963) A study of tumor types produced by ultraviolet light in hairless
mice and hairy mice. J. invest. Dermatol., 41, 463-473
Epstein, J.H. & Roth, H.L. (1968) Experimental ultraviolet light carcinogenesis. A study of croton oil
promoting effects. J. invest. Dermato/., SO, 387-389
Epstein, J.H., Epstein, W.L. & Nakai, T. (1967) Production of melanomas from DMBA-induced ' blue
nevi' in hairless mice with ultraviolet light. J. nat/ Cancer lnst., 38, 19-30
Epstein, WL., Fukuyama, K. & Epstein, J .H. (1969) Early effects of ultraviolet light on DNA synthesis
in human skin in vivo. Arch. Dermato/., 100, 84- 89
Epstein, J.H., Fukuyama, K., Reed, WB. & Epstein, WL. (1970) Defect in DNA synthesis in skin of
patients with xeroderma pigmentosum demonstrated in vivo. Science, 168, 1477- 1478
Eriksen, P. (1987) Occupational applications of ultraviolet radiation: risk evaluation and protection
techniques. In: Passchier, WE & Bosnjakovic, B.F.M., eds, Human Exposure to Ultraviolet
Radiation: Risks and Regulations, Amsterdam, Elsevier, pp. 317-331
Eriksen, P., Moscato, P.M., Franks, J.K. & Sliney, D.H. (1987) Optical hazard evaluation of dental
curing lights. Community Dent. oral Epidemiol., 15, 197-201
Everett, M.A., Yeargers, E., Sayre, R.M. & Olson, R.L. (1966) Penetration of epidermis by ultraviolet
rays. Photochem. Photobiol., 5, 53J--542
Everett, M.A., Nordquist, J. & Olson, R.L (1970) Ultrastructure of human epidermis following
chronic sun exposure. Br. J. Dermato/., 84, 248-257
Fan, J ., Schoenfeld, R.J. & Hunter, R. ( 1959) A study of the epidermal clear cells with special reference
to their relationship to the cells of Langerhans. J. invest. Dermatol., 32, 445-450
242 IARC MONOGRAPHS VOLUME 55
Farr, P.M. & Diffey, B.L. (1985) The erythemal response of human skin to ultraviolet radiation. Br. J.
Dermatol., 113, 65-76
Fears, T.R., Scotto, J. & Schneiderman, M.A. (1976) Skin cancer, melanoma, and sunlight. Am. I.
public Health, 66, 4 6 ~
Fears, 'I:R., Scotto, J. & Schneiderman, M.A. (1977) Mathematical models of age and ultraviolet
effects on the incidence of skin cancer among whites in the United States.Am. J. Epidemiol., 105,
420-427
Fincham, S. & Hill, G.B. (1989) Risk factors for non-melanocytic skin cancer in Alberta males
(Abstract). Am. J. Epidemiol., 130, 841
Findlay, G.M. (1928) Ultra-violet light and skin cancer. Lancet, ii, 1070-1073
Findlay, G.M. (1930) Cutaneous papillomata in the rat following exposure to ultra-violet light. Lancet,
i, 1229-1231
Fisher, M.S. & Cifone, M.A. (1981) Enhanced metastatic potential of murine fibrosarcomas treated in
vitro with ultraviolet radiation. Cancer Res., 41, 3018-3023
Fisher, G.J. & Johns, H.E. (1976) Pyrimidine photohydrates. In: Wang, S., ed., Photochemistry and
Photobiology of Nucleic Acids, Vol. 1, New York, Academic Press, pp. 169- 224
Fisher, M.S. & Kripke, M.L. (1977) Systemic alteration induced in mice by ultraviolet light irradiation
and its relationship to ultraviolet carcinogenesis. Proc. nat/ Acad. Sci. USA, 74, 1688-1692
Fisher, M.S. & Kripke, M.L. (1978) Further studies on the tumor-specific suppressor cells induced by
ultraviolet radiation. J. Immunol., 121, 1139-1144
Fisher, M.S. & Kripke, M.L. (1982) Suppressor T lymphocytes control the development of primary
skin cancers in ultraviolet-irradiated mice. Science, 216, 1133-1134
Fix, D.F. (1986) Thermal resistance of UV-mutagenesis to photoreactivation in E. coli B/r uvrA ung:
estimates of activation energy and further analysis. Mol. gen. Genet., 204, 452-456
Foley, P., Lanzer, D. & Marks, R. (1986) Are solar keratoses more common on the driver's side? Br.
med. J., 293, 18
Forbes, P.D. & Urbach, F. (1975) Experimental modification of photocarcinogenesis. I. Fluorescent
whitening agents and short-wave UVR. Food Cosmet. Toxicol., 13, 335-337
Forbes, P.D., Davies, R.E. & Urbach, F. (1978) Experimental ultraviolet photocarcinogenesis: wave-
length interactions and time-dose relationships. Nat/ Cancer Inst. Monogr., 50, 31-38
Forbes, P.D., Blum, H.F. & Davies, R.E. (1981) Photocarcinogenesis in hairless mice: dose-response
and the influence of dose-delivery. Photochem. Photobiol., 34, 361-365
Forbes, P.D., Davies, R.E., Urbach, F., Berger, D. & Cole, C. (1982) Simulated stratospheric ozone
depletion and increased ultraviolet radiation: effects on photocarcinogenesis in hairless mice.
Cancer Res., 42, 2796-2803
Forbes, P.D., Davies, R.E., Urbach, F. & Dunnick, J.K. {1990) Long-term toxicity of oral8-methoxy-
psoralen plus ultraviolet radiation in mice. J. Toxicol. cutaneous ocul. Toxicol., 9, 237-250
Fornace, A.J ., Jr, Schalch, H. & Alamo, I., 1 r (1988) Coordinate induction of metallothioneins I and II
in rodent cells by UV irradiation. Mol. cell. Bioi., 8, 4716-4720
Fortner, G.W & Kripke, M.L. (1977) In vitro reactivity of splenic lymphocytes from normal and UV-
irradiated mice against syngeneic UV-induced tumors. J. Immuno/., 118, 1483-1487
Fortner, G.W & Lill, P.H. (1985) Immune response to ultraviolet-induced tumors. I. Transplantation
immunity developing in syngeneic mice in response to progressor ultraviolet-induced tumors.
Transplantation, 39, 44-49
Foukal, P. (1990) Solar Astrophysics, New York, John Wiley & Sons, pp. 66-75
REFERENCES 243
Fox, IJ., Sy, M.-S . Benacerraf, B. & Greene, M.l. (1981) Impairment of antigen-presenting cell
function by ultraviolet radiation. II. Effect of in vitro ultraviolet irradiation on antigen-
presenting cells. Transplantation, 31, 262-265
Francis, AJ. & Giannelli, F. (1991) Cooperation between human cells sensitive to UVA radiations: a
clue to the mechanism of cellular hypersensitivity associated with different clinical conditions.
Exp. Cell Res., 195, 47-52
Franklin, W.A. & Haseltine, WA. (1986) The role of the (6-4) photoproduct in ultraviolet light-induced
transition mutations in E. coli. Mutat. Res., 165, 1-7
Franklin, S.A., Lo, K.M. & Haseltine, W.A. (1982) Alkaline lability of fluorescent photoproducts
produced in ultraviolet light-irradiated DNA.J. bioi. Chern., 257, 13535-13543
Frederick, J .E. (1990) Trends in atmospheric ozone and ultraviolet radiation: mechanisms and obser-
vations for the northern hemisphere. Photochem. Photobiol., SJ, 757-763
Freeman, R.G. (1975) Data on the action spectrum for ultraviolet carcinogenesis. J. nat/ Cancer lnst.,
ss, 1119-1122
Freeman, R.G. (1978) Action spectrum for ultraviolet carcinogenesis. Nat/ Cancer Inst. Monogr . SO,
27-29
Freeman, S.E. (1988) Variations in excision repair of UVB-induced pyrimidine dimers in DNA of
human skin in situ.J. invest. Dennato/., 90, 814-817
Freeman, R.G. & Knox, J.M. (1964) Ultraviolet-induced corneal tumors in different species and
strains of animals.J. invest. Dennatol., 43, 431-436
Freeman, S.E., Gange, R.W., Matzinger, E.A. & Sutherland, B.M. (1986) Higher pyrimidine dimer
yields in skin of normal humans with higher UVB sensitivity. J. invest. Dermatol., 86, 34-36
Freeman, S.E .. Gange, R. W., Sutherland, J .C., Matzinger, E.A. & Sutherland, B.M. (1987) Production
of pyrimidine dimers in DNA of human skin exposed in situ to UVA radiation. 1 invest.
Dermatol., 88, 430-433
Freeman, S.E., Applegate, L.A. & Ley, R.D. (1988a) Excision repair of UVR-induced pyrimidine
dimers in corneal DNA. Photochem. Photobiol., 41, 159-163
Freeman, S.E., Ley, R.D. & Ley, K.D. (1988b) Sunscreen protection against UV-induced pyrimidine
dimers in DNA of human skin in situ. Photodennatology, S, 243-247
Freeman, S.E., Hacham, H., Gange, R.W, Maytum, OJ., Sutherland, J.C. & Sutherland, B.M. (1989)
Wavelength dependence of pyrimidine dimer formation in DNA of human skin irradiated in situ
with ultraviolet light. Proc. nat/ Acad. Sci. USA, 86, 5605-5609
Friedburg, E. {1984) DNA Repair, New York, W.H. Freeman & Co.
Frucht. D.M., Lamperth, L., Vicenzi, E., Belcher, J.H. & Martin, M.A. (1991) Ultraviolet radiation
increases HIV-long terminal repeat-directed expression in transgenic mice. AIDS Res. hum.
Retroviruses, 1, 729-733
Fujiwara, Y., lchihashi, M., Kano, Y., Goto, K & Shimizu, K (1981) A new human photosensitive
subject with a defect in the recovery of DNA synthesis after ultraviolet-light irradiation.! invest.
Dennato/., 77, 256-263
Gafa, L., Filippazzo, M.G., Tumino, R., Dardanoni, G., Lanzarone, F. & Dardanoni, L. (1991) Risk
factors of nonmelanoma skin cancer in Ragusa, Sicily: a case-control study. Cancer Causes
Control, 2, 395-399
Gahring, L., Baltz, M., Pepys, M..B. & Daynes, R. (1984) Effect of ultraviolet radiation on production
of epidermal cell thymocyte-activating factor/interleukin 1 in vivo and in vitro. Immunology, 81,
1198-1202
244 IARC MONOGRAPHS VOLUME 55
Gallagher, R.P. (1988) Ocular melanoma in farmers (Letter to the Editor). Am. l ind. Med., 13,
523-525
Gallagher, P.E. & Duker, N.J. (1986) Detection of UV purine photoproducts in a defined sequence of
human DNA. Mol. cell. Bioi., 6, 707-709
Gallagher, P.E. & Duker, N.J. (1989) Formation of purine photoproducts in a defined human DNA
sequence. Photochem. Photobiol., 49, 599-605
Gallagher, C.H., Path, ER.C., Canfield, P.J., Greenoak, G.E. & Reeve, V.E. (1984a) Characterization
and histogenesis of tumors in the hairless mouse produced by low-dosage incremental ultraviolet
radiation. l invest. Dermatol., 83, 169- 174
Gallagher, C.H., Greenoak, G.E., Reeve, V.E., Canfield, PJ., Baker, R.S.U. & Bonin, A.M. (1984b)
Ultraviolet carcinogenesis in the hairless mouse skin. Influence of the sunscreen 2-ethylhexyl-p-
methoxycinnamate. Aust. l exp. Bioi. med. Sci., 62, 577-588
Gallagher, R.P., Threlfall, WJ., Jeffries, E., Band, P.R., Spinelli, J. & Coldman, A.J. (1984) Cancer and
aplastic anemia in British Columbia farmers.J nat/ Cancer Inst., 12, 1311- 1315
Gallagher, R.P., Elwood, J.M., Rootman, J., Spinelli, J.J., Hill, G.B., Threlfall, W.J. & Birdsell, J.M.
(1985) Risk factors for ocular melanoma: Western Canada Melanoma Study. J. nat/ Cancer Inst. ,
74, 775-778
Gallagher, R.P., Elwood, J.M. & Hill, G.B. (1986) Risk factors for cutaneous malignant melanoma: the
Western Canada Melanoma Study. Recent Results Cancer Res., 102, 38-55
Gallagher, R.P., Elwood, J.M., Threlfall, W.J., Spinelli, J.J., Fincham, S. & Hill, G.B. (1987) Socio-
economic status, sunlight exposure, and risk of malignant melanoma: the Western Canada Mela-
noma Study. J nat/ Cancer Inst., 79, 647-652
Gallagher, P.E., Weiss, R.B., Brent, T.P. & Duker, N.J. (1989) Wavelength dependence of DNA incision
by a human ultraviolet endonuclease. Photochem. Photobiol., 49, 363-367
Gallagher, R.P., McLean, D.I., Yang, C.P., Coldman, A.J., Silver, H.KB., Spinelli, J.J. & Beagrie, M.
(1990a) Anatomic distribution of acquired melanocytic nevi in white children. A comparison
with melanoma: the Vancouver mole study. Arch. Dermatol., 126, 466-471
Gallagher, R.P., McLean, D.I., Yang, C.P., Coldman, A.J., Silver, H.K.B., Spinelli, J.J. & Beagrie, M.
(1990b) Suntan, sunburn and pigmentation factors and the frequency of acquired melanocytic
nevi in children. Similarities to melanoma: the Vancouver mole study. Arch. Dermato/., 126,
770-776
Gange, R.W (1987) Acute effects of ultraviolet radiation in the skin. In: Fitzpatrick, T.B., Eisen, A.Z.,
Wolff, K., Freed berg, I.M. & Austen, K.F., eds, Dermatology in General Medicine, 3rd ed., New
York, McGraw-Hill, pp. 1451- 1457
Gange, R.W., Blackett, A.D., Matzinger, E.A., Sutherland, B.M. & Kochevar, I.E. (1985) Comparative
protection efficiency of UVA- and UVB-induced tans against erythema and formation of endo-
nuclease-sensitive sites in DNA by UVB in human skin. 1 invest. Dermatol., 85, 362-364
Garbe, C., Kruger, S., Stadler, R., Guggenmoos-Holzmann, I. & Orfanos, C.E. (1989) Markers and
relative risk in a German population for developing malignant melanoma. Int. J. Dermatol., 28,
517-523
Gardiner, B.G. & Kirsch, P.J. (1991) European Intercomparison of Ultraviolet Spectrometers, a n o ~
rama, Greece, 3-12 July 1991 (Report to the Commission of the European Communities [STEP
Project 76], Science and Technology for Environmental Protection), Luxembourg, Commission
of the European Communities
Garland, F. C., White, M.R., Garland, C. F., Shaw, E. & Gorham, E.D. (1990) Occupational sunlight
exposure and melanoma in the US Navy. Arch. environ. Health, 45, 261-267
REFERENCES 245
Garrison, L.M., Murray, L.E., Doda, D.O. & Green, A.E.S. (1978) Diffuse-direct ultraviolet ratios
with a compact double monochromator. Appl. Optics, 17, 827-836
Gellin, G.A., Kopf, A.W. & Garfinkel, L. (1965) Basal cell epithelioma. A controlled study of asso-
ciated factors. Arch. Dennatol., 91, 38-45
Gellin, G.A., Kopf, A W. & Garfinkel, L. (1969) Malignant melanoma. A controlled study of possibly
associated factors. Arch. Dermato/., 99, 43-48
Gensler, H.L. (1988a) Enhancement of chemical carcinogenesis in mice by systemic effects of ultra-
violet radiation. Cancer Res., 48, 620-623
Gensler, H.L. (1988b) Prevention of chemically induced two-stage skin carcinogenesis in mice by
systemic effects of ultraviolet irradiation. Carcinogenesis, 9, 767-769
Gensler, H.L. & Bowden, G.T. (1987) UVB-Induced modulation of mouse skin tumor induction by
benzo[a]pyrene (Abstract no. 546). Proc. Am. Assoc. Cancer Res., 28, 137
Gensler, H.L. & Welch, K. (1992) Prevalence of tumor prevention rather than tumor enhancement
when repetitive UV radiation treatments precede initiation and promotion. Carcinogenesis, 13,
9-13
Giam, Y.C. (1987) Cutaneous gerontology: solar degeneration of the skin. Ann. Acad. Med. Singapore,
16, 94-97
Giannini, M.S.H. (1986) Suppression of pathogenesis in cutaneous leishmaniasis by UV irradiation.
Infect. Immun., 51, 838-843
Gibbs, N.K., Young, A.R. & Magnus, LA (1985) Failure of UVR dose reciprocity for skin tumori-
genesis in hairless mice treated with 8-methoxypsoralen. Photochem. Photobio/., 42,
Gibson, P. & Diffey, B.L. (1989) Techniques for spectroradiometry and broadband radiometry. In:
Diffey, B.L., ed., Radiation Measurement in Photobiology, London, Academic Press, pp. 135-159
Gies, P., Roy, C. & Elliott, G. (1988) The anatomical distribution of solar UVR with emphasis on the
eye. In: Radiation Protection Practice, Vol. 1, Sydney, Pergamon Press, pp. 341-344
Gilchrest, B.A., Soter, NA., Stoff, J.S. & Mihm, M.C., Jr (1981) The human sunburn reaction: histo-
logic and biochemical studies. J. Am. Acad. Dermatol., 5,
Gilchrest, B.A., Murphy, G.F. & Soter, N.A. (1982) Effect of chronologie aging and ultraviolet irra-
diation on Langerhans cells in human epidermis. J. invest. Dermato/., 79, 85-88
Giles, G.G., Marks, R. & Foley, P. (1988) Incidence of non-melanocytic skin cancer treated in
Australia. Br. med. J., 296, 13-17
Glazier, A, Morison, W.L., Bucana, C., Hess, A.D. & Tutschka, P.J. (1984) Suppression of epidermal
graft-versus-host disease with ultraviolet radiation. Transplantation, 37, 211-213
Glickman, B. W., Schaaper, R.M., Haseltine, W.A., Dunn, R.L. & Brash, D.E. (1986) The C-C (6-4) UV
photoproduct is mutagenic in Escherichia coli. Proc. nat/ Acad. Sci. USA. 83, 6945-6949
Goldberg, L.H. & A,ltman, A (1984) Benign skin changes associated with chronic sunlight exposure.
Cutis, 34, 33-39
Goiii, F.M., Ondarroa, M., Azpiazu, I. & Macarulla, J.M. (1985) Phospholipid oxidation catalysed by
cytochrome c in liposomes. Biochim. biophys. Acta, 835, 549-556
Goodman, G.J., Marks, R., Selwood, T.S., Ponsford, M.W. & Pakes, W. {1984) Non-melanocytic skin
cancer and solar keratoses in Victoria-clinical studies II. Aust. I. Derm., 25, 103-106
Gordon, D. & Silverstone, H. (1976) Worldwide epidemiology of premalignant and malignant cuta-
neous lesions. In: Andrade, R., Gumport, S.L., Popkin, G.L. & Rees, R.D.,eds, CanceroftheSkin,
Vol. 1, London, W.B. Saunders, pp.
Gorlin, RJ. (1987) Nevoid basal-cell carcinoma syndrome. Medicine, 66, 98-113
246 IARC MONOGRAPHS VOLUME 55
Grabner, G. & Brenner, W. (1981) Unscheduled DNA repair in the human cornea following solar
simulating radiation. Acta ophthalmol., 59, 847-853
Grady, H.G., Blum, H.F. & Kirby-Smith, J.S. (1941) Pathology of tumors of the external ear in mice
induced by ultraviolet radiation. /. nat/ Cancer lnst., 2, 269-276
Grady, H.G., Blum, H.F. & Kirby-Smith, J.S. (1943) 1)rpes of tumor induced by ultraviolet radiation
and factors influencing their relative incidence. J. nat/ Cancer Inst., 3, 371- 378
Graham, S., Marshall, J ., Haughey, B., Stoll, H., Zielezny, M., Brasure, J . & West, D. (1985) An inquiry
into the epidemiology of melanoma. Am. J. Epidemio/., 122,
Granstein, R.D. (1985) Epidermal I-J-bearing cells are responsible for transferable suppressor cell
generation after immunization of mice with ultraviolet radiation-treated epidermal cells.
/. invest. Dermatol., 84, 206-209
Granstein, R.D. & Sauder, D.N. (1987) Whole-body exposure to ultraviolet radiation results in
increased serum interleukin-1 activity in humans. Lymphokine Res., 6, 187-193
Granstein, R.D., Lowy, A. & Greene, M.I. (1984) Epidermal antigen-presenting cells in activation of
suppression: identification of a new functional type of ultraviolet radiation-resistant epidermal
cell. /. Immunol., 132, 563-565
Granstein, R.D., Askari, M., Whitaker, D. & Murphy, G.F. (1987) Epidermal cells in activation of
suppressor lymphocytes: further characterization. J. Immunol., 138, 4055-4062
Greaves, M.W., Hensby, C.N., Black, A.K., Plummer, N.A., Fincham, N., Warin, AP. & Camp, R.
(1978) Inflammatory reactions induced by ultraviolet irradiation. BuJJ. Cancer, 65, 299-304
Green, A.C. (1984) Sun exposure and the risk of melanoma. Aust. J. Dermato/., 25, 99-102
Green, A.C. (1991) Premature ageing of the skin in a Queensland population. Med. J. Aust., 155,
473-478
Green, A.C. & Battistutta, D. (1990) Incidence and determinants of skin cancer in a high-risk
Australian population. Int. /. Cancer, 46, 356-361
Green, A. & O'Rourke, M.G.E. (1985) Cutaneous malignant melanoma in association with other skin
cancers. /. nat/ Cancer Inst., 14, 977-980
Green, A. & Siskind, V. (1983) Geographical distribution of cutaneous melanoma in Queensland.
Med. J. Aust., 1, 407-410
Green, A.E.S., Findley, G.B., Jr, Klenk, K.F., Wilson, W.M. & Mo, T. (1976) The ultraviolet dose
dependence of non-melanoma skin cancer incidence. Photochem. Photobiol., 24, 353-362
Green, A.C., Siskind, V., Bain, C. & Alexander, J. (1985a) Sunburn and malignant melanoma. Br. /.
Green, A. C., McLennan, R. & Siskind, V. (1985b) Common acquired naevi and the risk of malignant
melanoma. Int. /. Cancer, 35, 297-300
Green, A. C., Bain, C., McLennan, R. & Siskind, V. (1986) Risk factors for cutaneous melanoma in
Queensland. Recent Results Cancer Res. , 102, 76-97
Green, A.C., Beardmore, G., Hart, V., Leslie, D., Marks, R. & Staines, D. (1988a) Skin cancer in a
Queensland population. /. Am. Acad. Dermatol., 19, 1045-1052
Green, A.C., Sorahan, T., Pope, D., Siskind, V., Hansen, M., Hanson, L, Leech, P., P.M. &
Grimley, R.P. (1988b) Moles in Australian and British schoolchildren (Letter to the Editor).
Lancet, ii, 1497
Greene, M.I., Sy, M.S., Kripke, M. & Benacerraf, B. (1979) Impairment of antigen-presenting cell
function by ultravi9let radiation. Proc. nat/ Acad. Sci. USA, 76, 6591-6595
Griggs, H. G. & Bender, M.A. (1973) Photoreactivation of ultraviolet-induced chromosomal aberra-
tions.Scknce, 179,86-88
REFERENCES 247
Grob, J.J., Gouvernet, J., Aymar, D., Mostaque, A., Romano, M.H. , Collet, A.M., Noe, M.C.,
Diconstanzo, M.P. & Bonerandi, J.J. (1990) Count of benign melanocytic nevi as a major indi-
cator of risk for nonfamilial nodular and superficial spreading melanoma. Cancer, 66, 387-395
de Gruijl, F.R. & van der Leun, J .C. (1982a) Effect of chronic UV exposure on epidermal transmission
in mice. Photochem. Photobiol., 36, 433-438
de Gruijl, F.R. & van der Leun, J .C. (1982b) Systemic influence of pre-irradiation of a limited skin area
on UV-tumorigenesis. Photochem. Photobiol., 35. 379-383
de Gruijl, F.R. & van der Leun, J.C. (1983) Follow up on systemic influence of partial pre-irradiation
on UV-tumorigenesis. Photochem. Photobiol., 38, 381-383
de Gruijl, F.R., van der Meer, J.B. & van der Leun, J.C. (1983) Dose-time dependency of tumor
formation by chronic UV exposure. Photochem. Photobiol., 37, 53-62
Gupta, A.K & Anderson, l:F. (1987) Psoralen photochemotherapy. J. Am. Acad. Dermatol. , 17,703-
734
Gurish, M.F., Lynch, D.H. & Daynes, R.A. (1982) Changes in antigen-presenting cell function in the
spleen and lymph nodes of ultraviolet-irradiated mice. Transplantation, 33, 280-284
Gurish, M.F., Lynch, D.H., Yowell, R. & Daynes, R.A. (1983) Abrogation of epidermal antigen-
presenting cell function by ultraviolet radiation administered in vivo. Transplantation, 36, 304-
309
Haenszel, W (1%3) Variations in skin cancer incidence within the United States. Nat/ Cancer Inst.
Monogr., 10, 225-243
Halasz, C.L.G., Leach, E. E., Walther, R.R. & Poh-Fitzpatrick, M.B. (1983) Hydroa vacciniforme:
induction of lesions with ultraviolet A. J. Am. Acad. Dermatol., 8, 171-176
Hall, J .D. & Mount, D.W (1981) Mechanisms of DNA replication and mutagenesis in ultraviolet-
irradiated bacteria and mammalian cells. Prog. nucleic Acid Res. mol. Bioi., 25, 53-126
Halprin, KM., Comerford, M., Presser, S.E. & Taylor, J .R. (1981) Ultraviolet light treatment delays
contact sensitization to nitrogen mustard. Br. J. Dermatol., 105, 71-76
Haniszko, J. & Suskind, R.R. (1%3) The effect of ultraviolet radiation on experimental cutaneous
sensitization in guinea pigs. J. invest. Dermato/., 40, 183- 191
Hannan, M.A., Paul, M., Amer, M.H. & Al-Watban, F.H. (1984) Study of ultraviolet radiation and
genotoxic effects of natural sunlight in relation to skin can<;er in Saudi Arabia. Cancer Res., 44,
2192-2197
Hanson, D.L. & DeLeo, V.A. (1989) Long wave ultraviolet radiation stimulates arachidonic acid
release and cyclooxygenase activity in mammalian cells in culture. Photochem. Photobiol., 49,
423-430
Harber, L.C. & Bickers, D.R. (1981) Photosensitivity Diseases. Principles of Diagnosis and Treatment,
Philadelphia, PA. WB. Saunders
Hardie, I.R., Strong, R.W., Hartley, L.C.J., Woodruff, P.WH. & Clunie, GJ.A. (1980) Skin cancer in
Caucasian renal allograft recipients living in a subtropical climate. Surgery, 87, 177-183
Hariharan, P.V. & Cerutti, P.A. (1976) Excision of ultraviolet and gamma ray products of the
5,6-dihydroxy-dihydrothymine type by nuclear preparations of xeroderma pigmentosum cells.
Biochim. biophys. Acta, 447, 375- 378
Hariharan, P.V. & Cerutti, P.A. (1977) Formation of products of the 5,6-dihydroxydihydrothymine
type by ultraviolet light in HeLa cells. Biochemistry, 16, 2791-2795
Hartman, Z., Hartman, P.E. & McDermott, WL. (1991) Mutagenicity of coolwhite fluorescent light
for Salmonella. Mutat. Res., 260, 25-38
248
IARC MONOGRAPHS VOLUME 55
Hawk, J .L.M. & Parrish, J .A (1982) Responses of normal skin to ultraviolet radiation. In: Reegan, J.D.
& Parrish, J .A, eds, The Science of Photomedicine, New York, Plenum, pp. 219-260
Hayashi, Y. & Aurelian, L. (1986) Immunity to herpes simple virus type 2: viral antigen-presenting
capacity of epidermal cells and its impairment by ultraviolet irradiation. l lmmunol., 136,
1087-1092
Health Council of the Netherlands (1986) UV Radiation: Human Exposure to Ultraviolet Radiation
(Report 1986/93), The Hague
Hefferren, JJ., Cooley, R.O., Hall, J.B., Olsen, N.H. & Lyon, H.W. (1971) Use of ultraviolet illumi-
nation in oral diagnosis.! Am. dent. Assoc., 82, 1353-1360
Henderson, S.T. (1970) Daylight and Its Spectrum, New York, American Elsevier
Henderson, L.M., Arlett, C. F., Harcourt, SA., Lehmann, AR. & Broughton, B.C. (1985)Cells from an
immunodeficient patient (46BR) with a defect in DNA ligation are hypomutable but hyper-
sensitive to the induction of sister chromatid exchanges. Proc. nat/ Acad. Sci. USA, 82,2044-2048
Henseler, T., Wolff, K., Honigsmann, H. & Christophers, E. (1981) OralS- methoxypsoralen photo-
chemotherapy of psoriasis. The European PUVA study: a cooperative study among 18 European
centres. Lancet, i, 853-857
Herity, B., O'Loughlin, G., Moriarty, M.J. & Conroy, R. (1989) Risk factors for non-melanoma skin
cancer. Irish med. J., 82, 151-152
Hersey, P., Bradley, M., Hasic, E., Haran, G., Edwards, A & McCarthy, W.H. (1983a) Immunological
effects of solarium exposure. Lancet, i, 545-548
Hersey, P., Haran, G., Hasic, E. & Edwards, A (1983b) Alteration ofT cell subsets and induction of
suppressor T cell activity in normal subjects after exposure to sunlight.l Immunol., 31, 171-174
Hersey, P., MacDonald, M., Burns, C., Schibeci, S., Matthews, H. & Wilkinson, F.J. (1987) Analysis of
the effect of a sunscreen agent on the suppression of natural killer cell activity induced in human
subjects by radiation from solarium lamps. l invest. Dermatol., 88, 271-276
Hersey, P., MacDonald, M., Henderson, C., Schibeci, S., D'Alessandro, G., Pryor, M & Wilkinson,
F.J. (1988) Suppression of natural killer cell activity in humans by radiation from solarium lamps
depleted of UVB. 1 invest. Dermatol., 90, 305-310
Hietanen, M. (1990) Spectroradiometric and Photometric Studies on Ocular Exposure to Ultraviolet and
Vzsible Radiation from Light Sources, PhD Thesis, Helsinki, University of Helsinki, Department
of Phys ics
Higgins, S.A, Frenkel, K., Cummings, A & Teebor, G. W. (1987) Definitive characterisation of human
thymine glycol N-glycosylase activity. Biochemistry, 26, 1683-1688
Hinds, M.W & Kolonel, L.N. (1980) Malignant melanoma of the skin in Hawaii, 196G-1977. Cancer,
45,811-817
Hitchins, V.M., Beer, J.Z., Strickland, A.G. & Olvey, K.M. (1987) Lethal and mutagenic effects of
UVA radiation in six strains of L5178Y mouse lymphoma cells. In: Passchier, W.F. &
Bosnjakovic, B.EM., eds, Human Exposure to Ultraviolet Radiation: Risks and Regulations,
Amsterdam, Elsevier, pp. 65-69
Hoeijmakers, J.HJ. & Bootsma, D. (1990) Molecular genetics of eukaryotic DNA excision repair.
Cancer Cells, 2, 311-320
Hoffman, J.S. (1987) Ultraviolet Radiation and Melanoma (with a Special Focus on Assessing the Risks
of Stratospheric Ozone Depletion) (EPA 400/1-87-00ID), Washington DC, Office of Air and
Radiation, US Environmental Protection Agency -
Hogan, DJ., To, T., Gran, L., Wong, D. & Lane, P.R. (1989) Risk factors for basal cell carcinoma. lnt.l
Dermatol., 28, 591-594
REFERENCES 249
Holick. M.F., MacLaughlin, J .A., Clark. M.B., Holick. S.A., Potts, J :r., J r, Anderson, R.R., Blank. I.H.,
Parrish, J.A. & Elias, P. (1980) Photosynthesis of previtamin 0
3
in human skin and the physio-
logic consequences. Science, 210, 203-205
Hollaender, A. (1943) Effect of long ultraviolet and short visible radiation (3500 to 4900 A) on
Escherichia coli. J. Bacterial., 46, 531-541
Hollander, M.C. & Fomace, A.J .. Jr (1989) Induction of[os RNA by DNA-damaging agents. Cancer
Res., 49, 1687-1692
Hollis, D.E. & Scheibner, A. (1988) Ultrastructural changes in epidermal Langer hans cells and mela-
nocytes in response to ultraviolet irradiation, in Australians of aboriginal and Celtic descent. Br.
1 Dermatol., 119, 21-31
Holly, E.A., Kelly, J.W., ShpaH, S.N. & Chiu, S.-H. (1987) Number of melanocytic nevi as a major risk
factor for malignant melanoma. J. Am. Acad. Dermatol., 17, 459-468
Holly. E.A., Aston. D.A., Char, D.H., Kristiansen, J.J. & Ahn, O.K. (1990) Uveal melanoma in rela-
tion to ultraviolet light exposure and host factors. Cancer Res., SO, 5773-5777
Holly, E.A., Aston, D.A., Ahn, O.K., Kristiansen, J .J. & Char, D.H. (1991) No excess prior cancer in
patients with uveal melanoma. Ophthalmology, 98, 608-611
Holman, C.D.J. & Armstrong, B.K. (1984a) Pigmentary traits, ethnic origin, benign nevi, and family
history as risk factors for cutaneous malignant melanoma. J. nat/ Cancer Jnst., 12, 257-266
Holman, C.D.J. & Armstrong, B.K. (1984b) Cutaneous malignant melanoma and indicators oftotal
accumulated exposure to the sun: an analysis separating histogenetic types. J. nat/ Cancer Inst.,
73, 75-82
Holman, C.DJ., Gibson, I.M., Stephenson, M. & Armstrong, B.K. (1983a) Ultraviolet irradiation of
human body sites in relation to occupation and outdoor activity: field study using personal UVR
dosimeters. C/in. exp. Dermato/., 8, 269-277
Holman, C.DJ ., Heenan, P.J ., Caruso, V., Glancy, R.J. & Armstrong, B.K. (1983b) Seasonal variation
in the junctional component of pigmented naevi. Int. J. Cancer, 31, 213-215
Holman, C.D.J., Armstrong, B.K., Evans, P.R., Lumsden. G.J., Dallimore, K.J., Meehan, C.J., Beagley,
J. & Gibson, I.M. (1984a) Relationship of solar keratosis and history of skin cancer to objective
measures of actinic skin damage. Br. 1 Dermato/., 110, 129-138
Holman, C.D., Evans, P.R., Lumsden, G.J. & Armstrong, B.K. (1984b) The determinants of actinic
skin damage: problems of confounding among environmental and constitutional variables. Am.
J. Epidemio/., 120, 414-422
Holman, C.D.J., Armstrong, B.K. & Heenan, P.J. (1986a) Relationship of cutaneous malignant mela-
noma to individual sunlight-exposure habits. J. nat/ Cancer Inst., 16, 403-414
Holman, C.D.J., Armstrong, B.K., Heenan, P.J., Blackwell, J.B., Cumming, FJ., English, D.R.,
Holland, S., Kelsall, G.R.H., Matz, L.R., Rouse,I.L., Singh, A., Tho Seldam, R.EJ., Watt, J.D. &
Xu, Z. (1986b) The causes of malignant melanoma: results from the West Australian Lions Mela-
noma Research Project. Recent Results Cancer Res., 102, 18-37
Holmberg, M. & Gumauskas, E. (1990) Chromosome-type exchange aberrations are induced by inhi-
biting repair of UVC-induced DNA lesions in quiescent human lymphocytes. Mutat. Res., 232,
261-266
Honigsmann, H., Brenner, W., Tanew, A. & Ortel, B. (1987) UV-Induced unscheduled DNA synthesis
in human skin: dose response, correlation with erythema, time course and split dose exposure in
vivo. J. Photochem. Photobiol. B Bioi., 1, 33-43
Hoover, T.L., Morison, W.L. & K.ripke, M.L. (1987) Ultraviolet carcinogenesis in athymic nude mice.
Transplantation, 44, 693-695
250 IARC MONOGRAPHS VOLUME 55
Howie, S.E.M., Norval, N., Maingay, J. & Ross, J.A. (1986a) 1\vo phenotypically distant T cells
(Lyl +z- and L y t ~ + are involved in ultraviolet-B light-induced suppression of the efferent
DTH response to HSV-1 in vivo. Immunology, 58, 653-658
Howie, S.E.M., Norval, M. & Maingay, J.P. (1986b) Alterations in epidermal handling of HSV-1
antigens in vitro induced by in vivo exposure to UVB light. Immunology, 51, 225-230
Howie, S., Norval, M. & Maingay, J. {1986c) Exposure to low-dose ultraviolet radiation suppresses
delayed-type hypersensitivity to herpes simplex virus in mice. J. invest. Dennatol., 86, 1.25- 128
Hsia, H.C., Lebkowski, J.S., Leong, P.-M., Calos, M.P. & Miller, J.H. (1989) Comparison of ultraviolet
irradiation-induced mutagenesis of the lacl gene in Escherichia coli and in human 293 cells.
J. mol. Bioi. , 205, 103-113
Hsie, A.W, U, A.P. & Machanoff, R. (1977) A fluence response study of lethality and mutagenicity of
white, black, and blue fluorescent light, sunlamp, and sunlight irradiation in Chinese hamster
ovary cells. Mutat. Res., 45, 333-342
Hsu, J., Forbes, P.D., Harber, L.C. & Lakow, E. (1975) Induction of skin tumors in hairless mice by a
single exposure to UV radiation. Photochem. Photobiol., 21, 185-188
Hueper, WC. (1942) Morphological aspects of experimental actinic and arsenic carcinomas in the
skin of rats. Cancer Res., 2, 551-559
Huldschinsky, K. (1933) Eye sarcoma in rats caused by abnormally long UV (Ger.). Dtsch. med.
Wochenschr., 59, 530-531
Hunter, D.J., Colditz, G.A., Stampfer, M.J., Rosner, B., Willett, WC. & Speizer, F.E. (1990) Risk
factors for basal cell carcinoma in a prospective cohort of women. Ann. Epidemiol., 1, 13-23
Husain, Z., Yang, Q. & Biswas, D.K. (1990) cHa-ras Proto oncogene. Amplification and over-
expression in UVB-induced mouse skin papillomas and carcinomas. Arch. Dennatol., 126,324-
330
Husain, Z., Pathak, M.A., Flotte, '[ & Wick, M.M. (1991) Role of ultraviolet radiation in the induction
of melanocytic tumors in hairless mice following 7,U-dimethylbenz(a)anthracene application
and ultraviolet irradiation. Cancer Res., 51, 4964-4970
Huselton, C.A. & Hill, H.Z. (1990) Melanin photosensitizes ultraviolet light (UVC) DNA damage in
pigmented cells. Environ. mol. Mutag., 16, 37-43
Hutchinson, F. (1987) A review of some topics concerning mutagenesis by ultraviolet light. Photo-
chem. Photobiol., 45, 897- 903
Hutchinson, F. & Wood, R.D. (1986) Mechanisms of mutagenesis of E. coli by ultraviolet light. Basic
Life Sci., 38, 377- 383
Hutchinson, F., Yamamoto, K., Stein, J. & Wood, R.D. (1988) Effect of photoreactivation on muta-
genesis of lambda phage by ultraviolet light. J. mol. Bioi., 202, 593-601
IARC (1980) !ARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans,
Vol. 24, Some Pharmaceutical Drugs, Lyon, pp. 101-124
IARC (1985) !ARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans,
Vol. 37, Tobacco Habits Other than Smoking; Betel Quid and Areca-nut Chewing; and Some
Related Nitrosamines, Lyon, pp. 37- i36
IARC (1986a) !ARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans,
Vol. 40, Some Naturally Occurring and Synthetic Food Compounds, Furocoumarins and Ultra-
violet Radiation, Lyon, pp. 317- 371
IARC (1986b) !ARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans,
Vol. 38, Tobacco Smoking, Lyon
REFERENCES 251
IARC (1987a)JARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Suppl. 7, Overall
Evaluations of Carcinogenicity: An Updating of !ARC Monographs Volumes 1 to 42, Lyon,
pp. 175-176
!ARC (1987b) !ARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Sup pl. 7, Overall
Evaluations of Carcinogenicity: An Updating of IARC Monographs Volumes 1 to 42, Lyon, pp.
242-245
IARC (1988) !ARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Vol. 44, Alcohol
Drinking, Lyon
IARC (1990) !ARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Vol. 49,
Chromium, Nickel and Welding, Lyon, pp. 447-525
Ikushima, T. & Wolff, S. (1974) UV-Induced chromatid aberrations in cultured Chinese hamster cells
after one, two, or three rounds of DNA replication. Mutat. Res., 22, 193-201
International Electrotechnical Commission (1987) Safety of Household and Similar Electrical
Appliances, Part 2, Particular Requirements for Ultra-violet and Infra-red Radiation Skin Treatment
Appliances for Household Use (Publication 335-2-27: 1987), Geneva, Bureau Central de Ia Com-
mission Electrotechnique Internationale
International Electrotechnical Commission (1989)Amendment, Geneva, Bureau Central de Ia Com-
mission Electrotechnique Internationale
International Non-ionizing Radiation Committee of the International Radiation Protection Asso-
ciation (1985) Guidelines on limits of exposure to ultraviolet radiation of wavelengths between
180 nm and 400 nm (incoherent optical radiation). Health Phys., 49, 331-340
International Non-ionizing Radiation Committee of the International Radiation Protection Asso-
ciation (1989) Proposed change to the IRPA 1985 guidelines on limits of exposure to ultraviolet
radiation. H ea/th Phys., 56, 971-972
Iqbal, M. (1983) An Introduction to Solar Radiation, New York, Academic Press, pp. 335-373
Ito, M. (1966) The photodynamic effect of acridine orange and ultraviolet on the mouse skin carcino-
genesis by 20-methylcholanthrene. Nagoya med. J., 12, 247-259
Ito, A. & Ito, T. (1983) Possible involvement of membrane damage in the inactivation by broad-band
near-UV radiation in Saccharomyces cerevisiae cells. Photochem. Photobiol., 37, 395-401
lversen, O.H. (1986) Carcinogenesis studies with benzoyl peroxide (Panoxyl gel 5% ). J. invest.
Dermatol., 86, 442-448
Iversen, O.H. (1988) Skin tumorigenesis and carcinogenesis studies with 7,U-dimethylbenz{a]-
anthracene, ultraviolet light, benzoyl peroxide (Panoxyl gel5%) and ointment gel. Carcinogenesis,
9, 803-809
Jacobson, E.D., Krell, K, Dempsey, M.J., Lugo, M.H., Ellingson, 0. & Hench, C.W, II (l978)Thxicity
and mutagenicity of radiation from fluorescent lamps and a sunlamp in L5178Y mouse lym-
phoma cells. M_utat. Res., Sl, 61-75
Jacobson, E.D., Krell, K & Dempsey, M.J. (1981) The wavelength dependence of ultraviolet light-
induced cell killing and mutagenesis in L5178Y mouse lymphoma cells. Photochem. Photobiol.,
33,257-260
Jagger, J. (1981) Near-UV radiation effects on microorganisms. Photochem. Photobio/., 34, 761- 768
Jagger, J. (1985) Solar-UV Actions on Living Cells, New York. Praeger
Jessup, J.M., Hanna. N., Palaszynski, E. & Kripke, M.L. (1978) Mechanisms of depressed reactivity to
dinitrochlorobenzene and ultraviolet-induced tumors during ultraviolet carcinogenesis in
BALB/c mice. CeU. Immunol., 38, 105-115
252 IARC MONOGRAPHS VOLUME 55
Johns, H. E., Rapaport, S.A. & Delbruck, M. (1962) Photochemistry of thymine dimers. J. mol. Bioi., 4,
104-114
Jones, C.A., Huberman, E., Cunningham, M.L. & Peak, M.J. (1987) Mutagenesis and cytotoxicity in
human epithelial cells by far- and near-ultraviolet radiations: action spectra. Radial. Res., 110,
244-254
Jones, S.K, Moseley, H. & Mackie, R. (1987) UVA-Induced melanocytic lesions. Br. J. Dennatol., 117,
111-115
Jose, J .G. & Pitts, D.G. (1985) Wavelength dependency of cataracts in albino mice following chronic
exposure. Exp. Eye Res., 41, 545-563
Joshi, S.D., Shrikhande, S.S. & Ranade, S.S. (1984) Studies on UV-induced skin tumors in experi-
mental animals. Photobiochem. Photobiophys., 1, 235-243
Joshi, S.D., Shrikhande, S.S., Naik, S.N. & Ranade, S.S. (1986) Multiplicity of tumours induced in the
laboratory animals by ultraviolet (UVC) irradiation. Indian J. anim. Sci., 56, 736-743
Jun, B.-D., Roberts, L.K., Cho, B.-H., Robertson, B. & Daynes, R.A. (1988) Parallel recovery of epi-
dermal antigen-presenting cell activity and contact hypersensitivity responses in mice exposed to
ultraviolet irradiation: the role of a prostaglandin-dependent mechanism.J. invest. Dermatol., 90,
311-316
K.aase, H., Zidowitz, B. & Berger, H. (1984) Spectral radiation measurements of UV-irradiation appa-
ratus and experiments to estimate the risk of photocarcinogenesis (Ger.). Lichtforschung, l,
43-47
Kaidbey, KH. (1988) Wavelength dependence for DNA synthesis inhibition in hairless mouse epi-
dermis. Photodennatology, S, 65-70
Kaidbey, KH., Agin, P.P., Sayre, R.M. & Kligman, A.M. (1979) Photoprotection by melanin-a com-
parison of black and Caucasian skin. J. Am. Acad. Dennatol., l, 249-260
Kalthoff, K & Jii.ckle, H. (1982) Photoreactivation of pyrimidine dimers generated by a photo-
sensitized reaction in RNA of insect embryos (Smittia spec.). In: Helene, C., Charlier, M.,
Montenay-Garestier, T. & Laustriat, G., eds, Trends in Photobiology, New York, Plenum, pp. 173-
188
Kantor, G.J. (1985) Effects of sunlight on mammalian cells. PJwtochem. Photobiol .. 41,741-746
Kawada, A (1986) UVB-Induced erythema, delayed tanning, and UVA-induced immediate tanning
in Japanese skin. Photodermatology, 3, 327-333
Keijzer, W, Mulder, M.P., Langeveld, J.C.M., Smit, E.M.E., Bos, J.L., Bootsma, D. & Hoeijmakers,
J.HJ. (1989) Establishment and characterization of a melanoma cell line from a xeroderma
pigmentosum patient: activation of N-ras at a potential pyrimidine dimer site. Cancer Res., 49,
1229-1235
Kelfkens, G., de Gruijl, F.R. & van der Leun, J.C. (1991a) Tumorigenesis by short-wave ultraviolet A:
papillomas versus squamous cell carcinomas. Carcinogenesis, 12, 1377-1382
Kelfkens, G., van Weelden, H., de Gruijl, F.R. & van der Leun, J.C. (1991b) Influence of dose rate in
ultraviolet tumorigenesis. J. Photochem. Photobiol. B Bioi., 10, 41-50
Keller, A.Z. (1970) Cellular types, survival, race, nativity, occupations, habits and associated diseases
in the pathogenesis of lip cancers. Am. J. Epidemiol., 91,486-499
Kelly, G.E., Meikle, WD. & Sheil, A.G.R. (1987) Effects of immunosuppressive therapy on the
induction of skin tumors by ultraviolet irradiation in hairless mice. Transplantation, 44, 429-434
Kelly, G.E., Meikle, WD. & Moore, D.E. (1989) Enhancement of UV-induced skin carcinogenesis by
azathioprine: role of photochemical sensitisation. Photochem. Photobiol., 49, 59-65
REFERENCES 253
Kennedy, A.R., Ritter, M.A. & Little, J.B. (1980) Fluorescent light induces malignant transformation
in mouse embryo cell cultures. Science, 207, 1209-1211
Keyse, S.M. & 'JYrrell, R.M. (1989) Heme oxygenase is the major stress protein induced in
human skin fibroblasts by UVA radiation, hydrogen peroxide and sodium arsenite. Proc. TUJtl
Acad. Sci. USA, 86, 99-103
Keyse, S.M., Moss, S.H. & Davies, DJ.G. (1983) Action spectra for inactivation of normal and
derma pigmentosum human skin fibroblasts by ultraviolet radiations. Photochem. Photobiol.,
37, 307-3U
Keyse, S.M., Applegate, L.A., Tromvoukis, Y. & Tyrrell, R.M. (1990) Oxidant stress leads to
criptional activation of the human heme oxygenase gene in cultured skin fibroblasts. Mol. cell.
Bioi., 10, 4967-4969
Khlat, M., Vail, A., Parkin, M. & Green, A. (1992) Mortality from melanoma in migrants to Australia:
variation by age at arrival and duration of stay. Am. J. Epidemiol., 135, 1103-1113
Kim, Y., Kripke, M.L. & Ullrich, S.E. {1990) Immunosuppression by factors released from
irradiated epidermal cells: selective effects on the generation of contact and delayed
sensitivity after exposure to UVA or UVB radiation. J. invest. Dermatol., 94, 26-32
IGnlen, L.J., Sheil, A.G.R., Peto, J. & Doll, R. (1979) Collaborative United IGngdom- Australasian
study of cancer in patients treated with immunosuppressive drugs. Br. med. J., ii, 1461-1466
Kinsey, V.E. (1948) Spectral transmission of the eye to ultraviolet radiations. Arch. Opthalmol., 39,
508-513 .
J.S. & Craig, D.L. {1957) The induction of chromosome aberrations in Tradescantia by
ultraviolet radiation. Genetics, 42, 176-187
Kirkpatrick, C.S . Lee, J .A.H. & White, E. (1990) Melanoma risk by age and status.
Int. J. Cancer, 46, 1-4
Kjeldstad, B. & Johnsson, A. (1986) An action spectrum for blue and near ultraviolet inactivation of
Propionibacterium acnes; with emphasis on a possible porphyrin photosensitization. Photochem.
Photobiol., 43, 67-70
Klamen, D.L. & Tuveson, R.W (1982) The effect of membrane fatty acid composition on the near-UV
(300-400 nm) sensitivity of Escherichia coli K1060. Photochem. Photobiol., 35, 167-173
Klein, K.L. & Linnemann, C.C., Jr (1986) Induction of recurrent genital herpes simplex virus type 2
infection by ultraviolet light (Letter to the Editor). Lancet, i, 796-797
Klepp, 0. & Magnus, K. (1979) Some environmental and bodily characteristics of melanoma patients.
A case-control study. Int. J. Cancer, 23, 482-486
Kligman, A.M. (1969) Early destructive effect of sunlight on human skin. J. Am. med. Assoc., 210,
2377-2380
Kligman, L.H. (1988) UVA enhances low dose UVB tumorigenesis (Abstract). Photochem. Photobiol.,
47,85
Kligman, L.H. (1989) The hairless mouse: a model for pbotoaging. J. Am. Acad.
Dermatol., 21, 623-631
Kligman, L.H. & Kligman, A.M. (1981) Histogenesis and progression of ultraviolet
tumors in hairless mice. J. nat/ Cancer Inst., 61, 1289-1297
Kligman, L.H. & Sayre, R.M. (1991) An action spectrum for ultraviolet induced elastosis in hairless
mice: quantification of elastosis by image analysis. Photochem. Photobiol., 53, 237-242
Kligman, L.H., Akin, F .J. & Kligman, A.M. (1985) The contributions of UVA and UVB to connective
tissue damage in hairless mice. J. invest. Dennatol., 84, 272-276
254 IARC MONOGRAPHS VOLUME 55
Kligman, L.H., Kaidbey, K.H., Hitchins, V.M. & Miller, S.A. (1987) Long wavelength ( > 340 nm)
ultraviolet-A induced skin damage in hairless mice is dose dependent. In: Passchier, W:F. &
Bosnjakovic, B.F.M., eds, Human Exposure to Ultraviolet Radiation: Risks and Regulations,
Amsterdam, Elsevier, pp. 77- 81
Kligman, L.H., Crosby, M.J., Miller, S.A., Hitchins, V.M. & Beer, J .z. (1990) Skin cancer induction in
hairless mice by long-wavelength UVA radiation: a progress report (Abstract). Photochem.
Photobiol., 51, 18S-19S
Kligman, L.H., Crosby, M.J., Miller, S.A., Hitchins, V.M. & Beer, J.Z. (1992) Carcinogenesis by long
wavelength UVA and failure of reciprocity. In: Urbach, F., ed., Biological Responses to Ultraviolet
A Radiatwn, Overland Park, KS, Valdenmar, pp. 301- 308
Knees-Matzen, S., Roser, M., Reimers, U., Ehlert, U., Weichenthal, M., Breitbart, E.W & Rudiger,
H.W (1991) Increased UV-induced sister-chromatid exchange in cultured fibroblasts of first-
degree relatives of melanoma patients. Cancer Genet. Cytogenet., 53, 265-270
Kocsard, E. & Ofner, F. (1964) Contact eczematous sensitization and sensitivity of the solar elastotic
skin. Aust. 1 Dermato/., 1, 203-205
Kolari, P.J., Lauharanta, J. & Hoikkala, M. (1986) Midsummer solar UV-radiation in Finland
compared with the UV-radiation from phototherapeutic devices measured by different
techniques. Photodermatology, 3, 340-345
Kopecky, K.E., Pugh, G.W., Jr, Hughes, D.E., Booth, G.D. & ChevilJe, N.F. (1979) Biological effect of
ultraviolet radiation on cattle: bovine ocular squamous cell carcinoma. Am. J. vet. Res., 40, 1783-
1788
Kopf, A. W, Lindsay, A. C., Rogers, G.S., Friedman, R.J ., Rigel, D.S. & Levenstein, M. (1985) Relation-
ship of nevocytic nevi to sun exposure in dysplastic nevus syndrome.! Am. Acad. Dermatol., 12,
656-{)62
Kostkowski, H.J., Saunders, R., Ward, J., Popenoe, C. & Green, A. (1982) Measurement of Solar
Te"estrial Spectrall"adiance in the Ozone Cut-off Region, Self study Manual on Optical Radiation
Measurements, Part III, Applications(NBS Technical Note 910-5; PB 83-184382), Washington DC,
National Bureau of Standards
Koval, T.M. (1987) Photoreactivation of UV damage in cultured Drosophila cells. Experientia, 43,
445-446
Kraemer, K.H. (1980) Xeroderma pigmentosum. A prototype disease of environmental-genetic inter-
action. Arch. Dermatol., ll6, 541-542
Kraemer, K.H. & Greene, M.H. (1985) Dysplastic nevus syndrome. Familial and sporadic precursors
of cutaneous melanoma. Dennatol. Clin., 3, 225- 237
Kraemer, K.H. & Slor, H. (1984) Xeroderma pigrnentosum. C/in. Dermato/., 2, 33-69
Kraemer, K.H. & Weinstein, G.D. (1977) Decreased thymidine incorporation in circulating leuko-
cytes after treatment of psoriasis with psoralen and long-wave ultraviolet light. J. invest.
Dermato/., 69, 211-214
Kraemer, K.H., Lee, M.M. & Scotto, J. (1987) Xeroderma pigmentosum. Cutaneous, ocular. and
neurologic abnormalities in 830 published cases. Arch. Dermato/., 123, 241-250
Kraemer, K.H., Seetharam, S., Protic-Sabljic, M., Brash, D.E., Bredberg, A. & Seidman, M.M. (1988)
Defective DNA repair and mutagenesis by dimer and non-dimer photoproducts in xeroderma
pigmentosum measured with plasmid vectors. In: Friedberg. E.C. & Hanawalt, P.C., eds,
Mechanisms and Consequences of DNA Damage Processing, New York, Alan R. Liss, pp. 325- 335
Kramer, G.F. & Ames, B.N. {1987) Oxidative mechanisms of toxicity oflow-intensity near-UV light in
Salmonella typhimurium. l Bacteriol . 169, 2259-2266
REFERENCES 255
Krepinsky, A.B., Rainbow, AJ. & Heddle, J.A. (1980) Studies on the ultraviolet light sensitivity of
Bloom's syndrome fibroblasts. Mutat. Res., 69, 357-368
Kricker, A., English, D.R., Randell, P.L., Heenan, P.J., Clay, C.D., Delaney, T.A. & Armstrong, B.K.
(1990) Skin cancer in Gerald ton, Western Australia: a suiVey of incidence and prevalence. Med. J.
Aust., 152, 399-407
Kricker, A., Armstrong, B.K., English, D.R. & Heenan, PJ. (1991a) Pigmentary and cutaneous risk
factors for non-melanocytic skin cancer-a case-control study. Int. J. Cancer, 48, 650-662
Kricker, A., Armstrong, B.K., English, D., Heenan, PJ. & Randell, P.L (1991b) A case-control study
of non-melanocytic skin cancer and sun exposure in Western Australia (Abstract No. IlL P2).
Cancer Res. din. Oncol., 117 (Suppl. II), S75
Kripke, M.L (1974) Antigenicity of murine skin tumors induced by ultraviolet light. J. nat/ Cancer
I nst ., 53, 1333-1336
Kripke, M.L. (1977) Latency, histology, and antigenicity of tumors induced by ultraviolet light in three
inbred mouse strains. Cancer Res., 37, 1395- 1400
Kripke, M.L. & Fisher, M.S. (1976) Immunologic parameters of ultraviolet carcinogenesis. J. nat/
Cancer /nst., 57, 211-215
Kripke, M.L & McClendon, E. (1986) Studies on the role of antigen-presenting cells in the systemic
suppression of contact hypersensitivity by UVB radiation. J. lmmunol., 137, 443-447
Kripke, M.L. & Morison, W.L (1985) Modulation of immune function by UV radiation. J. invest.
Dermatol. , 85, 625-665
Kripke, M.L. & Morison, W.L. (1986a) Studies on the mechanism of systemic suppression of contact
hypersensitivity by ultraviolet B radiation. Photodermato/ogy, 3, 4-14
Kripke, M.L. & Morison, W.L. (1986b) Studies on the mechanism of systemic suppression of contact
hypersensitivity by UVB radiation. ll. Differences in the suppression of delayed and contact
hypersensitivity in mice. J. invest. Dermatol., 86, 543-549
Kripke, M.L. & Sass, E.R., eds (1978) International conference on ultraviolet carcinogenesis. Natl
Cancer lnst. Monogr., 50
Kripke, M.L., Lofgreen, J.S., Beard, J., Jessup, J .M. & Fisher, M.S. (1977) In vivo immune responses of
mice during carcinogenesis by ultraviolet irradiation. J. nad Cancer lnst., 59, 1227-1230
Kromberg, J.G.R., Castle, D., Zwane, E.M. & Jenkins, T. (1989) Albinism and skin cancer in southern
Africa. Clin. Genet., 36, 43-52
Krutmann, J. & Elmets, C.A. (1988) Recent studies on mechanisms in photoimmunology. Photochem.
Photobiol., 48, 787- 798
Kubitschek, H.E. (1967) Mutagenesis of near-visible light. Science, 155, 1545- 1546
Kumar, S., Joshi, P.C., Sharma, N.D., Bose, S.N., Davies, RJ.H., Thkeda, N. & McCloskey,J.A.(1991)
Adenine photodimerization in deoxyadenylate sequences: elucidation of the mechanism through
structural studies of a major d(ApA) photoproduct Nucleic Acids Res., 19, 2841- 2847
Kunkel, T.A. (1984) Mutational specificity of depurination. Proc. nat/ Acad. Sci. USA, 81, 1494-1498
Kupper, T.S., Chua, A.O., Flood, P., McGuire, J. & Gubler, U. (1987) Interleukin 1 gene expression in
cultured human keratinocytes is augmented by ultraviolet irradiation. J. clin. Invest., 80,430-436
Kurihara, T., Tatsumi, K., Takahashi, H. & Inoue, M. (1987) Sister-chromatid exchanges induced by
ultraviolet light in Bloom's syndrome fibroblasts. Mutat. Res., 183, 197-202
Lai, L.-W. & Rosenstein, B.S. (1990) Induction of DNA strand breaks and DNA-protein cross-links in
norma! human skin fibroblasts following exposure to 254 nm UV radiation. J. Photochem.
Photobiol. B Bioi., 6, 395-404
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
I
256 IARC MONOGRAPHS VOLUME 55
Lancaster, H.O. (1956) Some geographical aspects of the mortality from melanoma in Europeans.
Med. J Aust., 1, 1082-1087
Lancaster, H.O. & Nelson, J. (1957) Sunlight as a cause of melanoma: a clinical survey. Med. J Aust.,l,
452-456
Larcom, L.L., Morris, T.E. & Smith, M.E. (1991) Thnning salon exposure suppression of DNA repair
capacity and mitogen-induced DNA synthesis. Photochem. Photobiol., 53, 511-516
Larko, 0. & Diffey, B.L. (1983) Natural UV-B radiation received by people with outdoor, indoor and
mixed occupations and UV-B treatment of psoriasis. Clin. exp. Dennatol., 8, 279-285
Larko, 0. & Diffey, B.L. (1986) Occupational exposure to ultraviolet radiation in dermatology depart-
ments. Br. J Dennatol., 114, 479-484
Lau, H., Reemtsma, K. & Hardy, M.A. (1983) Pancreatic islet aUograft prolongation by donor-specific
blood transfusions treated with ultraviolet irradiation. Science, 221, 754-756
Lau, H., Reemtsma, K. & Hardy, M.A. (1984) Prolongation of rat islet allograft survival by direct
ultraviolet irradiation of the graft. Science, 223, 607-609
Leach, J.F., McLeod, V.E., Pingstone, A.R., Davis, A. & Deane, G.H.W. (1978) Measurement of the
ultraviolet doses received by office workers. Clin. exp. Dermatol., 3, 77-79
LeClerc, J.E., Borden, A. & Lawrence C.W. (1991) The thymine-thymine pyrimidine-pyrimidone
(6-4) ultraviolet light photoproduct is highly mutagenic and specifically induces 3'-thymine-to-
cytosine transitions in Escherichia coli. Proc. nat/ Acad. Sci. USA, 88, 9685-9689
Lee, J.A.H. (1982) Melanoma and exposure to sunlight. Epidemiol. Rev., 4, 110-1.36
Lee, J.A.H. & Storer, B.E. (1980) Excess of malignant melanomas in women in the British Isles.
Lancet, ii, 1337-1339
Lee, J.A.H. & Strickland, D. (1980) Malignant melanoma: social status and outdoor work. Br. J.
Cancer, 41, 757-763
Lee, G.S.-F., Savage, E.A., Ritzel, R.G. & von Borstel, R.C. (1988) The base-alteration spectrum of
spontaneous and ultraviolet radiation-induced forward mutations in the URA3 locus of
Saccharomyces cerevisiae. Mol. gen. Genet., 214, 396-404
Lehmann, A.R., Arlett, C.F., Broughton, B.C., Harcourt, S.A., Steingrimsdottir, H., Stefanini, M.,
Taylor, A.M.R., Natarajan, A.T., Green, S., King, M.D., MacKie, R.M., Stephenson, J.B.P. &
Tolmie. J .L. (1988) Trichothiodystrophy, a human DNA repair disorder with heterogeneity in the
cellular response to ultraviolet light. Cancer Res., 48, 609()...6()96
Lerman, S. (1980) Radiant Energy and the Eye, New York, MacMillan
Lerman, S. (1988) Ocular phototoxicity. New Engl. J Med., 319, 1475-1477
Letvin, N.L., Greene, M.I., Benacerraf, B. & Germain, R.N. (1980a) Immunologic effects of whole-
body ultraviolet irradiation: selective defect in splenic adherent cell function in vitro. Proc. nat/
Acad. Sci. USA, 77, 2881-2885
Letvin, N.L., Nepom, J.T., Greene, M.I., Benacerraf, B. & Germain, R.N. (1980b) Loss ofla-bearing
splenic adherent cells after whole body ultraviolet irradiation. J. Immunol., 125, 2550-2554
van der Leun, J.C. (1984) Yearly review: UV-carcinogenesis. Photochem. Photobiol., 39, 861-868
van der Leun, J.C. (1987a) Principles of risk reduction and protection. In: Passchier, W.F. &
Bosnjakovic. B.F.M., eds, Human Exposure to Ultraviolet Radiation: Risks and Regulations,
Amsterdam, Elsevier, pp. 293-303
van der Leun, J.C. (1987b) Interactions of different wavelengths in effects of UV radiation on skin.
Photodermatology, 4, 257-264
REFERENCES 257
van der Leun, J.C. (1992) Interactions of UVA and UVB in photodermatology: what was photo-
augmentation? In: Urbach, F., ed., The Biological Responses to Ultraviolet A RadiaJioTJ, Overland
Park, KS, Valdenmar, pp. 309-319
van der Leun, J.C. & van Weelden, H. (1986) UVB phototherapy: principles, radiation sources,
regimens. Cun: Probl. Dermato/., IS, 39-51
Levi, F., LaVecchia, C., Te, V.-C. & Mezzanotte, G. (1988) Descriptive epidemiology of skin cancer in
the Swiss canton of Vaud. Int. l Cancer, 42, 811-816
Lew, RA., Sober, A.J., Cook, N., Marvell, R & Fitzpatrick, T.B. (1983) Sun exposure habits in patients
with cutaneous melanoma: a case control study./ Dermatol. surg. Oncol., 9, 981-986
Ley, R.D. (1985) Photoreactivation of UV-Induced pyrimidine dimers and erythema in the marsupial
Monodelphis domestica. Proc. nat/ Acad. Sci. USA, 82, 2409-2411
Ley, RD. & Applegate, LA. (1989) Photodermatological studies with the marsupial Monode/phis
domestica. In: Maibach, H.l. & Lowe, N.J., eds. Models in Dermatology, Vol. 4, Basel, Karger, pp.
265-275
Ley, RD., Sedita. B.A. & Boye, E. (1978) DNA polymerase !-mediated repair of 365 om-induced
single-strand breaks in the DNA of Escherichia coli. Photochem. Photobiol., 21, 323-327
Ley, RD., Peak, M.J. & Lyon, L.L. (1983) Induction of pyrimidine dimers in epidermai DNA of hair-
less mice by UVB: an action spectrum. J. invest. Dermatol., 80, 188-191
Ley, RD., Applegate, L.A.. Stuart, T.D. & Fry, RJ.M. (1987) UV radiation-induced skin tumors in
Monodelphis domestica. Photodermatology, 4, 144-147
Ley, R.D., Applegate, L.A. & Freeman, S.E. (1988) Photorepair of ultraviolet radiation-induced
pyrimidine dimers in corneal DNA. Mutat. Res., 194, 49-55
Ley, RD., Applegate, L.A., Padilla, RS. & Stuart, T.D. (1989) Ultraviolet radiation-induced
malignant melanoma in Monodelphis domestica. Photochem. Photobiol., SO, 1-5
Ley, RD., Applegate, L.A., Fry, R.J.M. & Sanchez, A.B. (1991) Photoreactivation of ultraviolet
radiation-induced skin and eye tumors of Monodelphis domestica. Cancer Res., 51, 6539-6542
Lightfoote, M.M., Zmundzka, B.Z., Olvey, K.M., Miller, S.A & Beer, J.Z. (1992) Effects of UVB
radiation on human immunodeficiency virus. In: Houck, M. & Kligman, A., eds, Biological
Effects of Light (in press)
Lill, P.H. (1983) Latent period and antigenicity of murine tumors induced in C3H mice by short-
wavelength ultraviolet radiation. J. invest. Dermatol., 81, 342-346
Lin, C.S., Goldthwait, D.A. & Samols, D. (1990) Induction of transcription from the long terminal
repeat of Moloney murine sarcoma provirus by UV-irradiation, x-irradiation, and phorbol ester.
Proc. nat/ Acad. Sci. USA, 87, 36-40
Lindahl-Kiessling, K & Safwenberg, J. (1971) Inability of UV-irradiated lymphocytes to stimulate
allogenic cells in mixed lymphocyte cultures. Int. Arch. AJ/ergy, 41, 670-678
Lindqvist, C. (1979) Risk factors in lip cancer: a questionnaire survey. Am. J. Epidemio/.,109, 521-530
Lippincott, S.W. & Blum, H.F. (1943) Neoplasms and other lesions of the eye induced by ultraviolet
radiation in strain A mice. J. nat/ Cancer Inst., 3, 545-554
Lippke, J.A., Gordon, L.K., Brash, D.E. & Haseltine, W.A. (1981) Distribution of UV light-induced
damage in a defined sequence of human DNA: detection of alkaline-sensitive lesions at pyri-
midine nucleoside-cytidine sequences. Proc. nat/ Acad. Sci. USA, 78, 3388-3392
Lischko, AM., Seddon, J .M., Gragoudas, E.S., Egan, KM. & Glynn, R.J. (1989) Evaluation of prior
primary malignancy as a determinant of uveal melanoma. A case-control study. Ophthalmology,
96, 1716-1721
Livingston, W. (1983) Landscape as viewed in the 320-nm ultraviolet. J. opt. Soc. Am., 73, 1653-1657
258 IARC MONOGRAPHS VOLUME 55
Logani, M.K, Sambuco, C.P., Forbes, P.O. & Davies, R.E. (1984) Skin-tumour promoting activity of
methyl ethyl ketone peroxide-a potent lipid-peroxidizing agent. Food chem. Toxicol., 22, 879-
882
Luande, J., Henschke, C.l. & Mohammed, N. (1985) The Thnzanian human albino skin. Cancer, 55,
1823- 1828
van der Lubbe, J.L.M., Rosdorff, H.J.M., Bos, J.L. & van der Eb, AJ. (1988) Activation of N-ras
induced by ultraviolet irradiation in vitro. Oncogene Res., 3, 9- 20
Lucke-Ruhle, C., Mai, S. & Herrlich, P. (1989) UV-Induced early-domain binding factor as the
limiting component of simian virus 40 DNA amplification in rodent cells. Mol. cell. Bioi., 9,
4812-4818
Lundgren, K & Wulf, H.C. (1988) Cytotoxicity and genotoxicity of UVA irradiation in Chinese
hamster ovary cells measured by specific locus mutations, sister chromatid exchanges and
chromosome aberrations. Photochem. Photobio/., 41, 559-563
Lunnon, RJ. (1984) Ultraviolet photography. In: Williams, R., ed., Medical Photography Study Guide,
Lancaster, MTP Press, pp. 225-233
Lynch, D.H., Gurish, M.F. & Haynes, R.A. (1983) The effects of high-dose UV exposure on murine
Langerhans cell function at exposed and unexposed sites as assessed using in vivo and in vitro
assays. J. invest. Dermatol., 81, 336-341
Lynge, E. & Thygesen, L. (1990) Occupational cancer in Denmark. Cancer incidence in the 1970
census population. Scand. l Work Environ. Health, 16 (Suppl. 2), 1-35
Machta, L., Cotton, G., Hass, W. & Komhyr, W. (1975) ClAP Measurements of Solar Ultraviolet
Radiation (Final Report, Interagency Agreement DOT-AS-20082), Washington DC, US Depart-
ment of nansportation .
Mack, TM. & Floderus, B. (1991) Malignant melanoma risk by nativity, place of residence at
diagnosis, and age at migration. Cancer Causes Control, 2, 401-411
MacKie, R.M. & Aitchison, T. (1982) Severe sunburn and subsequent risk of primary cutaneous mali-
gnant melanoma in Scotland. Br. l Cancer, 40, 955-960
MacKie, R.M., Freudenberger, T. & Aitchison, T.C. (1989) Personal risk-factor chart for cutaneous
melanoma. Lancet, ii, 487-490
MacLaughlin, J. & Holick, M.F. (1985) Aging decreases the capacity of human skin to produce
vitamin 03. J. clin. Invest., 16, 1536-1538
Madewell, B.R., Conroy, J.D. & Hodgkins, E.M. (1981) Sunlight-skin cancer association in the dog: a
report of three cases. J. cutaneous Pathol., 8, 434-443
Magee, M.J., Kripke, M.L. & Ullrich, S.E. (1989a) Suppression of the elicitation of the immune
response to alloantigen by ultraviolet radiation. Transplantation, 41, 1008-1013
Magee, MJ ., Kripke, M.L. & Ullrich, S.E. (1989b) Inhibition of the immune response to alloantigen in
the rat by exposure to ultraviolet radiation. Photochem. Photobio/., 50, 193-199
Magnus, K (1973) Incidence of malignant melanoma of the skin in Norway, 1955-1970. Variations in
time and space and solar radiation. Cancer, 32, 1275-1286
Magnus, K. (1991) The Nordic profile of skin cancer incidence. A comparative epidemiological study
of the three main types of skin cancer. Int. l Cancer, 41, 12-19
Maher, V.M., Dorney, OJ., Mendrala, AL., Konze-Thomas, B. & McCormick, JJ. (1979) DNA
excision-repair processes in human cells can eliminate the cytotoxic and mutagenic conse-
quences of ultraviolet irradiation. Mutat. Res., 62, 311-323
REFERENCES 259
Maher, V.M., Rowan, L.A., Silinskas, K.C., Kateley. S.A. & McCormick, J.J. (1982) Frequency of UV-
induced neoplastic transformation of diploid human fibroblasts is higher in xeroderma pigmen-
tosum cells than in normal cells. Proc. nat/ Acad. Sci. USA, 79, 2613-2617
Maltzman, W. & Czyzyk, L. (1984) UV-Irradiation stimulates levels of p53 cellular tumor antigen in
nontransformed mouse cells. Mol. cell. Bioi., 4, 1689-1694
Mandai, T.K. & Chatterjee, S.N. (1980) Ultraviolet- and sunlight-induced lipid peroxidation in Iipo-
somal membrane. Radial. Res., 83, 290-302
Mariutti, G. & Matzeu, M. (1987) Measurement of ultraviolet radiation in welding processes and
hazard evaluation. In: Passchier, W.F. & Bosnjakovic, B.F.M., eds, Human Exposure to Ultraviolet
Radiation: Risks and Regulations, Amsterdam. Elsevier, pp. 387-390
Marks, R. & Selwood, T.S. (1985) Solar keratoses. The association with erythemal ultraviolet radiation
in Australia. Cancer, 56, 2332- 2336
Marks, R., Ponsford, M.W., Selwood, T.S., Goodman, G. & Mason, G. (1983) Non-melanocytic skin
cancer and solar keratoses in Victoria. Med. J. Aust., 2, 619-622
Marks, R., Rennie, G. & Selwood, T.S. (1988) Malignant transformation of solar keratoses to
squamous cell carcinoma. Lancet, i, 795-797
Marks, R., Jolley, D., Dorevitch, A.P. & Selwood, T.S. (1989) The incidence of non-melanocytic skin
cancers in an Australian population: results of a five-year prospective study. Med. J. Aust . ISO.
475-478
Marshall, R.R. & Scott, D. (1976) The relationship between chromosome damage and cell killing in
UV-irradiated normal and xeroderma pigmentosum cells. Mutat. Res., 36, 397-400
Marshall, R.R., Arlett, C.F., Harcourt, S.A. & Broughton, B.A. (1980) Increased sensitivity of cell
strains from Cockayne's syndrome to sister-chromatid exchange induction and cell killing by UV
light. Mutat. Res., 69, 107-112
Matsumoto, K., Sugiyama, M. & Ogura, R. (1991) Non-dimer DNA damage in Chinese hamster V-79
cells exposed to ultraviolet-Blight. Photochem. Photobiol., 54, 389- 392
Matsunaga, T., Hieda, K. & Nikaido, 0 . (1991) Wavelength dependent formation of thymine dimers
and (6-4)photoproducts in DNA by monochromatic ultraviolet light ranging from 150 to 365 nm.
Photochem. Photobiol., 54, 403-410
Matsuoka, L. Y ., Ide, L., Wortsman, J ., MacLaughlin, J .A. & Holick, M.F. ( 1987) Sunscreens suppress
cutaneous vitamin D3 synthesis. J. c/in. Endocrinol. Metab., 64, 1165-1168
Mayne, L.V., Mullenders, L.H.F. & van Zeeland, AA. (1988) Cockayne's syndrome: a UV sensitive
disorder with a defect in the repair of transcribing DNA but normal overall excision repair. In:
Friedberg, E.C. & Hanawalt, P.C., eds, Mechanisms and Consequences of DNA DatrUlge
Processing, New York, Alan R. Liss, pp. 349-353
McCormick, J.P.. Fisher, J .R., Pachlatko, J.P. & Eisenstark, A. (1976) Characterisation of a cell-lethal
product from the photooxidation of tryptophan: hydrogen peroxide. Science, 191, 468-669
McCredie, M. & Coates, M.S. (1989) Cancer Incidence in Migrants to New South Wales. 1972 to 1984,
New South Wales Central Cancer Registry, Woolloomooloo, NSW, New South Wales Cancer
Council, pp. 22-23, 62-63
McGovern, V.J., Shaw, H.M., Milton, G.W. & Farago, G.A. (1980) Is malignant melanoma arising in a
Hutchinson's melanotic freckle a separate disease entity? Histopathology, 4, 235- 242
McGrath, H., Wilson, W.A. & Scopelitis, E. {1986) Acute effects of low-fluence ultraviolet light on
human T-lymphocyte subsets. Photochem. Photobinl., 43, 627-631
260 IARC MONOGRAPHS VOLUME 55
McGregor, W.G., Chen, R.-H., Lukash, L., Maher, V.M. & McCormick, JJ. (1991) Cell cycle-
dependent strand bias for UV-induced mutations in the transcribed strand of excision repair-
proficient human fibroblasts but not in repair-deficient cells. Mol. ceU. Bioi., ll, 1927-1934
McKinlay, AE & Diffey, B.L (1987) A reference action spectrum for ultraviolet induced erythema in
human skin. CIE (Commission Intemationale de /'Eclairage) J., 6, 17-22
McKinlay, A.F. & Whitlock, M.J. (1987) Measurement of ultra-violet radiation from fluorescent
lamps used for general lighting and other purposes in the UK. In: Passchier, W.F. & Bosnjakovic,
B.F.M., eds, Human Exposure to Ultraviolet Radiation: Risks and Regulations, Amsterdam,
Elsevier, pp. 253-258
McKinlay, A.F., Whillock, MJ. & Meulemans, C.C.E. (1989) Ultraviolet Radiation aruJ Blue-light
Emissions from Spotlights Incorporating Tungsten Halogen Lamps (Report NRPB-R228), Didcot,
National Radiological Protection Board
McLennan, A.G. (1987) The repair of ultraviolet light-induced DNA damage in plant cells. Mutat.
Res., 181, 1-7
Mecherikunnel, AT. & Richmond, J .C. ( 1980) Spectral Distribution of Solar Radiation (NASA
Technical Memorandum 82021), Greenbelt, MD, Goddard Space Flight Center
Melski. J.W., Tanenbaum, L., Parrish, J.A, Fitzpatrick, T.B. & Bleich, H.L (1977) Ora) methoxsaJen
photochemotherapy for the treatment of psoriasis: a cooperative clinical trial. J. invest.
DermatoL, 68,328-335
Menzies, S.W, Greenoak, G.E., Reeve, V.E. & Gallagher, C.H. (1991) Ultraviolet radiation-induced
murine tumors produced in the absence of ultraviolet radiation-induced systemic tumor
immunosuppression. Cancer Res., 51, 2773-2779
Miguel, A. G. & 1Jrrell, R.M. (1983) Induction of oxygen-dependent lethal damage by monochromatic
UVB (313 nm) radiation: strand breakage, repair and cell death. Carcinogenesis, 4, 375-380
Milham, S., Jr (1983) Occupational Mortality in Washington State 1950-1979 (DHSS (NIOSH) Publ.
No. 83-116), Cincinnati, OH, National Institute for Occupational Safety and Health
Miller, J.H. (1985) Mutagenic specificity of ultraviolet light. J. mol. Bioi., 182, 45-68
Miskin, R. & Ben-lshai, R. (1981) Induction of plasminogen activator by UV light in normal and
xeroderma pigmentosum fibroblasts. Proc. nat/ Acad. Sci. USA, 78, 6236-6240
Mitchell, D.L. (1988) The relative cytotoxicity of (6-4)photoproducts and cyclobutane dimers in
mammalian cells. Photochem. Photobiol., 48, 51-57
Mitchell, D.L., Haipek, C.A. & Clarkson, J.M. (1985) (6-4)Photoproducts are removed from the DNA
of UV-irradiated mammalian cells more efficiently than cyclobutane pyrimidine dimers. Mutat.
Res., 143, 109-lU
Mitchell, D.L., Jen, J. & Cleaver, J.E. (1991) Relative induction of cycJobutane dimers and cytosine
photohydrates in DNA irradiated in vitro and in vivo with ultraviolet-C and ultraviolet-B light.
Photochem. Photobio/., 54, 741-746
Moan, J .. Dahlback, A., Henriksen, T. & Magnus, K. (1989) Biological amplification factor for
sunlight-induced nonmelanoma skin cancer at high latitudes. Cancer Res., 49, 5207-5212
Molina, M.J. & Rowland, F.S. (1974) Stratospheric sink for chlorofluoromethanes: chlorine atom
catalyzed destruction of <_>zone. Nature, 249, 810-812
Monda!, S. & Heidelberger, C. (1976) ilansformation of C3H/10Tlf2 CL8 mouse embryo fibroblasts
by ultraviolet irradiation and a phorbol skin. Nature, 260, 710-711
Morgun, V.V., Logvinenko, V.F., Dvernyakov, V.S. & Timoshenko, V.M. (1988) Mutagenic activity of
pulsed concentrated sunlight. Sov. Genet., 24, 189-193
Morison, W.L. (1983a) Phototherapy and Photochemotherapy of Skin Disease, New York, Praeger
REFERENCES 261
Morison, W.L. (1983b) Solar urticaria. In: Parrish, JA, Kripke, M.L. & Morison, W.L, eds, Photo-
immunology, New York. Plenum, pp. 215- 226
Morison, W.L. (1983c) Autoimmune disease. In: Parrish, J.A., Kripke, M.L & Morison, W.L., eds,
Photoimmunology, New York. Plenum, pp. 255-266
Morison, W.L. (1986) The effects of UVA radiation on immune function. In: Urbach, F. & Grange,
R.W., eds, The Biological Effects of UVA Radiation, New York, Praeger, pp. 202-209
Morison, W.L. (1989) Effects of ultraviolet radiation on the immune system in humans. Photochem.
Photobiol., SO, 515-524
Morison, WL. & Kelley, S.P. (1985) Sunlight suppressing rejection of 280 to 320 nm UV-radiation-
induced skin tumors in mice. l nat/ Cancer Inst., 74, 525-527
Morison, W.L. & Kochevar, I.E. (1983) Photoallergy. In: Parrish, J.A., Kripke, M.L. & Morison, W.L.,
eds, Photoimmunology, New York. Plenum, pp. 227- 253
Morison, W.L. & Kripke, M.L. (1984) Systemic suppression of contact hypersensitivity by ultraviolet B
radiation or methoxsalenlultraviolet A radiation in the guinea pig. Cell. Immunol., 85, 270-277
Morison, W.L., Parrish, J.A., Bloch, K.J. & Krugler, J.I. (1979a) In vivo effect of UVB on lymphocyte
function. Br. 1 Dermatol., 101, 513-519
Morison, WL., Parrish, J .A., Anderson, R.R. & Bloch, K.J. ( 1979b) Sensitivity of mononuclear cells to
UV radiation. Photochem. Photobiol., 29, 1045-1047
Morison, W.L., Bucana, C. & Kripke, M.L. (1984) Systemic suppression of contact hypersensitivity by
UVB radiation is unrelated to the UVB-induced alterations in the morphology and number of
Langerhans cells. Immunology, 52, 299-306
Morison, W.L., Pike, R.A. & Kripke, M.L. (1985) Effect of sunlight and its component wavebands on
contact hypersensitivity in mice and guinea pigs. Photodermatology, 2, 195-204
Morison, W.L., Jerdan, M.S., Hoover, T.L. & Farmer, E.R. (1986) UV radiation-induced tumors in
haired mice: identification as squamous cell carcinomas. ! nat/ Cancer Inst., 77, 1155-1162
M0rk, N.-J. & Austad. J. (1982) Short-wave ultraviolet light (UVB) treatment of allergic contact
dermatitis of the hands. Acta dermatovenereol. , 63, 87-89
Morrison, H. (1985) Photochemistry and photobiology of urocanic acid. Photodermato/ogy, 2, 158-165
Moseley, H. (1988) Non-ionising Radiation: Microwaves, Ultraviolet and Laser Radiation (Medical
Physics Handbooks 18), Bristol, Adam Hilger, pp. 110-154
Moss, S.H. & Smith, K.C. (1981) Membrane damage can be a significant factor in the inactivation of
Escherichia coli by near-ultraviolet radiation. Photochem. Photobiol., 33, 203-210
Muir, C., Waterhouse, J., Mack, T., Powell, J. & Whelan, S., eds (1987) Cancer Incidence in Five
Continents, l-01. V (IARC Scientific Publications No. 88), Lyon, !ARC
Munakata, N. (1989) Genotoxic action of sunlight upon Bacillus subtilis spores: monitoring studies at
Tokyo, Japan.l Radial. Res., 30, 338-351
Murthy, P.B., Rahiman, M.A. & Tulpule, P.G. (1982) UV-Induced chromosome aberrations, sister-
chromatid exchanges and cell survival in cultured lymphocytes from malnourished children.
Pediatr. Res., 16, 663-664
Musk, P., Campbell, R., Staples, J., Moss, D.J. & Parsons, P.G. (1989) Solar and UVC-induced
mutation in human cells and inhibition by deoxynucleosides. Mutat. Res., 227, 25-30
Mutzhas, M.F. (1986) UVA-Emitting light sources. In: Urbach, F. & Grange, R.W, eds, The Biological
Effects of UVA Radiation, New York, Praeger, pp. 10-23
Myhr, B.C., Thrnbull, D. & DiPaolo, J.A. (1979) Ultraviolet mutagenesis of normal and xeroderma
pigmentosum variant human fibroblasts. Mutat. Res., 62, 341-353
262 IARC MONOGRAPHS VOLUME 55
Natarajan, A.T., van Zeeland, A.A., Verdegaal-Immerzeel, E.A.M. & Filon, A.R. (1980) Studies on the
influence of photoreactivation on the frequencies of UV-induced chromosomal aberrations,
sister-chromatid exchanges and pyrimidine dimers in chicken embryonic fibroblasts. Mutat.
Res., 69, 307- 317
Nathanson, R.B., Forbes, P.D. & Urbach, F. (1976) Modification of photocarcinogenesis by two
immunosuppressive agents. Cancer Lett., l, 243- 247
Nelson, E.W., Eichwald, EJ. & Shelby, J. (1987) Increased ultraviolet radiation-induced skin cancers
in cyclosporine-treated mice. Transplant. Proc., 19, 52h--527
Nikula, K.J., Benjamin, S.A., Angleton, G.M., Saunders, W.J. & Lee, A. C. (1992) Ultraviolet radiation,
solar dermatosis, and cutaneous neoplasia in beagle dogs. Radial. Res., 129, 11-18
Nishi, Y., Hasegawa, M.M .. Taketomi, M., Ohkawa, Y. & Inui, N. (1984) Comparison of 6-thio-
guanine-resistant mutation and sister chromatid exchanges in Chinese hamster V79 cells with
forty chemical and physical agents. Cancer Res., 44, 3270-3279
Noonan, F.P. & De Fabo, E. C. (1985) Immune suppression by ultraviolet radiation and its role in ultra-
violet radiation induced carcinogenesis in mice. Aust. J. Dennatol., 26, 4- 8
Noonan, F.P., De Fabo, E. C. & Kripke, M.L. (1981a) Suppression of contact hypersensitivity by UV
radiation and its relationship to UV-induced suppression of tumor immunity. Photochem.
Photobiol., 34, 683-689
Noonan, F.P., Kripke, M.L., Pedersen, G.M. & Greene, M.l. (1981b) Suppression of contact hyper-
sensitivity in mice by ultraviolet irradiation is associated with defective antigen presentation.
Immunology, 43, 527-533
Noonan, F.P., Bucana, C., Sauder, D.N. & De Fabo, E.C. (1984) Mechanism of systemic immune
suppression by UV irradiation in vivo. II. The UV effects on number and morphology of epi-
dermal Langerhans cells and the UV-induced suppression of contact hypersensitivity have
different wavelength dependencies. J Immunol., 132, 2408-2416
Noonan, F.P., De Fabo, E. C. & Morrison, H. (1988) cis-Urocanic acid, a product formed by ultraviolet
B irradiation of the skin, initiates an antigen presentation defect in splenic dendritic cells in vivo.
J invest. Dermatol., 90, 92-99
Norbury, K.C. & Kripke, M.L. (1978) Ultraviolet carcinogenesis in T-cell-depleted mice. J. nat/ Cancer
Inst., 61, 917-921
Norimura, T, Maher, V.M. & McCormick, J.J. (1990) Cytotoxic and mutagenic effect of UV,
ethylnitrosourea and in
diploid human T lymphocytes in culture: comparison with fibroblasts. Mutagenesis, 5, 447-451
Norval, M., Mcintyre, C.R., Simpson, T.J., Howie, S.E.M. & Bardshiri, E. (1988) Quantification of
urocanic acid isomers in murine skin during development and after irradiation with UVB light.
Photodennatology, 5, 179-186
Nusbaum, B.P., Edwards, E.K., Jr, Horwitz, S.N. & Frost, P. (1983) Psoriasis therapy. The effect of UV
radiation on sensitization to mechlorethamine. Arch. Dermatol., 119, 117-121
O'Beirn, S.F., Judge, P., Urbach, F., MacCon, C.F. & Martin, F. (1970) Skin cancer in County Galway,
Ireland. Proc. natl Cancer Conf, 6, 489-500
O'Dell, B.L., Jessen, R.T, Becker, L.E., Jackson, R.T. & Smith, E.B. (1980) Diminished immune
response in sun-damaged skin. Arch. Dermatol., 116, 559-561
Oettle, A.G. (1963) Skin cancer in Africa. Nat/ Cancer lnst. Monogr., 10, 197-214
Office of Population Censuses and Surveys (1986) Occupational Mortality: the Registrar General's
Decennial Supplement for Great Britain 1979-80, 1982-83 (Series DS No. 6), London, Her
Majesty's Stationery Office
REFERENCES 263
Okamoto, H. & Kripke, M.L. (1987) Effector and suppressor circuits of the immune response are
activated in vivo by different mechanisms. Proc. nat/ Acad. Sci. USA, 84, 3841-3845
O'Loughlin, C., Moriarty, M.J., Herity, B. & Daly, L. (1985) A re-appraisal of risk factors for skin
carcinoma in Ireland: a case control study. Irish l med. Sci., 154, 61-{55
Olsen, J.H. & Jensen, O.M. (1987) Occupation and risk of cancer in Denmark. An analysis of93 810
cancer cases, 1970-1979. Scand. l Work Environ. Health, 13 (Suppl. 1-91
Olsen, W.M., Huitfeldt, H.S. & Eggset, G. (1989) UVB-Induced (6-4) photoproducts in hairless mouse
epidermis studied by quantitative immunohistochemistry. Carcinogenesis, 10, 1669-1673
Onuigbo, W.I.B. (1978) Lip lesions in Nigerian lgbos. Int. J. ora/ Surg., 1, 73-75
0sterlind, A. (1987) Trends in incidence of ocular malignant melanoma in Denmark 1943- 1982. Int.l
Cancer, 40, 161- 164
0sterlind, A. (1990) Malignant melanoma in Denmark. Occurrence and risk factors. Acta oncol., 29,
1-22
0sterlind, A., Olsen, J.H., Lynge, E. & Ewertz, M. (1985) Second cancer following cutaneous mela-
noma and cancers of the brain, thyroid, connective tissue, bone, and eye in Denmark, 1943-80.
Natl Cancer lnst. Monogr., 68, 361-388
0sterlind, A., Hou-Jensen, K. & Jensen, O.M. (1988a) Incidence of cutaneous malignant melanoma in
Denmark 1978-1982. Anatomic site distribution, histologic types, and comparison with non-
melanoma skin cancer. Br. l Cancer, 58, 385-391
0sterlind, A., Tucker, M.A., Stone, B.J. & Jensen, O.M. (1988b) The Danish case-control study of
cutaneous malignant melanoma. II. Importance of UV-light exposure. Int.l Cancer, 42, 319-324
0sterlind, A., Tucker, M.A., Hou-Jensen, K., Stone, B.J., Engholm, G. & Jensen, O.M. (1988c) The
Danish case-control study of cutaneous malignant melanoma. I. Importance of host factors. Int.
l Cancer, 42, 200-206
Otani, T. & Mori, R. (1987) The effects of ultraviolet irradiation of the skin on herpes simplex virus
infection: alterations in immune function mediated by epidermal cells and in the course of
infection. Arch. Viral., 96, 1-15
Oxholm, A., Oxholm, P., Staberg, B. & Bendtzen, K. (1988) Immunohistological detection of inter-
leukin I-like molecules and tumour necrosis factor in human epidermis before and after UVB-
irradiation in vivo. Br. l Dennatol., 118, 369-376
Paffenbarger, R.S., Jr, Wing, A.L. & Hyde, R.T. (1978) Characteristics in youth predictive of adult-
onset malignant lymphomas, melanomas, and leukemias: brief communication. l nat/ Cancer
Jnst., 60, 89-92
Parrington, J.M. (1972) Ultraviolet-induced chromosome aberrations and mitotic delay in human
fibroblast cells. Cytogenetics, 11, 117-131
Parrington, J.M., Delhanty, J.D.A. & Baden, H.P. (1971) Unscheduled DNA synthesis, UV-induced
chromosome aberrations and SV40 transformation in cultured cells from xeroderma
tosum. Ann. hum. Genet., 35, 149-160
Parrish, J.A. (1983) The Effect of Ultraviolet Radiation on the Immune System, New Brunswick, NJ,
Johnson & Johnson
Parrish, J.A. & Jaenicke, K.F. (1981) Action spectrum for phototherapy of psoriasis. l invest.
Dennato/. , 76,359-362
Parrish, JA, Fitzpatrick, T.B., Tanenbaum, L. & Pathak, M.A. (1974) Photochemotherapy of
psoriasis with oral methoxsalen and longwave ultraviolet light. New EngJ.l Med. , 291, 1.207-1211
Parrish, J.A., Zaynoun, S. & Anderson, R.R. (1981) Cumulative effects of repeated subthreshold
doses of ultraviolet radiation.! invest. Dermatol., 16, 356-358
264 IARC MONOGRAPHS VOLUME 55
Parrish, J.A., Kripke, M.L. & Morison, WL., eds (1983) Photoimmunology, New York, Plenum
Parry, J.M., Sharp, D., Tippins, R.S. & Parry, E.M. (1979) Radiation-induced mitotic and meiotic
aneuploidy in the yeast Saccharomyces cerevisiae. Mutat. Res., 61, 37-55
Parshad, R., 'Thylor, WG., Sanford, K.K., Camalier, R.E, Gantt, R. & Tarone, R.E. (1980a) Fluo-
rescent light-induced chromosome damage in human IMR-90 fibroblasts. Role of hydrogen
peroxide and related free radicals. Mutat. Res., 13, 115-124
Parshad, R., Sanford, K.K., Jones, G.M., Tarone, R.E., Hoffman, HA. & Grier, A.H. (1980b)Suscep-
tibility to fluorescent light-induced chromatid breaks associated with DNA repair deficiency
and malignant transformation in culture. Cancer Res., 40, 4415-4419
Pathak, M.A., Fitzpatrick, TB., Greiter, F. & Kraus, E.W. (1987) Preventive treatment of sunburn,
dermatoheliosis, and skin cancer with sun-protective agents. In: Fitzpatrick, T.B., Eisen, A.Z.,
Wolff, K., Freedberg, I.M. & Austen, K.F., eds, Dermatology in General Medicine, 3rd ed., New
York, McGraw-Hill, pp. 1507-1522
Patrick, M.H. (1977) Studies on thymine-derived UV photoproducts in DNA-I. Formation and bio-
logical role of pyrimidine adducts in DNA. Photochem. Photobiol., 25, 357-372
Patton, J.D., Rowan, L.A., Mendrala, A.L., Howell, J .N., Maher, V.M. & McCormick, J J. (1984) Xero-
derma pigmentosum fibroblasts including cells from XP variants are abnormally sensitive to the
mutagenic and cytotoxic action of broad spectrum simulated sunlight. Photochem. Plwtobiol.,
39,37-42
Pauw, H. & Meulemans, C. C. E. (1987) Occupational exposure to artificial UV-A radiation within the
Philips factories in the Netherlands. In: Passchier, W.F. & Bosnjakovic, B.F.M., eds, HutrUln
Exposure to Ultraviolet Radiation: Risks and Regulations, Amsterdam, Elsevier, pp. 265-268
Peak, MJ. & Peak, J.G. (1982) Single-strand breaks induced in Bacillus subtilis DNA by ultraviolet
light: action spectrum and properties. Photochem. Photobiol . 35, 675-680
Peak, J.G. & Peak, M.J. (1990) Ultraviolet light induces double-strand breaks in DNA of cultured
human P3 cells as measured by neutral filter elution. Photochem. Photobiol., 52, 387-393
Peak, J.G. & Peak, MJ. (1991) Comparison of initial yields of DNA-to-protein crosslinks and single-
strand breaks induced in cultured human cells by far- and near-ultraviolet light, blue light, and
x-rays. Mutat. Res., 246, 187-191
Peak, M.J., Peak, J.G., Moehring, M.P. & Webb, R.B. (1984) Ultraviolet action spectra for DNA dimer
induction, lethality, and mutagenesis in Escherichia coli with emphasis on the UVB region.
Photochem. Photobiol., 40, 613-620
Peak, J.G., Peak, MJ., Sikorski, R.S. & Jones, C.A. (1985) Induction of DNA-protein crosslinks in
human cells by ultraviolet and visible radiations: action spectrum. Photochem. Photobiol., 41,
295- 302
Peak, MJ., Peak, J.G. & Carnes, B.A. (1987) Induction of direct and indirect single-strand breaks in
human cell DNA by far- and near-ultraviolet radiations: action spectrum and mechanisms.
Photochem. Photobiol., 45, 381-387
Peak, J.G., Woloschak, G.E. & Peak, MJ. (1991a) Enhanced expression of protein kinase C gene
caused by solar radiation. Photochem. Photobiol., 53, 395-397
Peak, J .G., Pilas, B., Dudek, EJ. & Peak, MJ. ( 1991b) DNA breaks caused by monochromatic 365 nm
ultraviolet-A radiation or hydrogen peroxide and their repair in human epithelioid and xero-
derma pigmentosum cells. Photochem. Photobiol., 54, 197-203
Pearse, A.D., Gaskell, S.A. & Marks, R. (1987) Epidermal changes in human skin following irra-
diation with either UVB or UVA. J. invest. Dermatol., 88, 83-87
Penn, I. (1980) Immunosuppression and skin cancer. Clin. plast. Surg., 7, 361-368
REFERENCES 265
Pepino, P., Hardy, M.A., Chabot, J.A., Berger, C., Marboe, C. & Wasfie, T. (1989) UVB irradiated allo-
geneic bone marrow transplantation in rats: prevention of graft versus host disease without
immunosuppression. Transpl. Proc., 21, 2995-2996
Perna, JJ., Mannix, M.L, Rooney, J.F., Notkins, A.L. & Straus, S.E. (1987) Reactivation of latent
herpes simplex virus infection by ultraviolet light: a human model. J. Am. Acad. Dermatol., 17,
473-478
Perry, LL. & Greene, M.I. (1982) Antigen presentation by epidermal Langerhans cells: loss of
function following ultraviolet (UV) irradiation in vivo. Clin. /mmunol. Immunopathol., 24,
204-219
Perticone, P., Hellgren, D. & Lambert, B. (1986) Effects of UV-irradiation on the SCE frequency in
human lymphocyte cultures. Mutat. Res., 175, 83-89
Peto, R., Pike, M.C., Day, N.E., Gray, R.G., Lee, P.N., Parish, S., Peto, J ., Richards, S. & Wahrendorf, J.
(1980) Guidelines for simple sensitive significance tests for carcinogenic effects in long-term
animal experiments. In: /ARC Monographs on the Evaluation of the Carcinogenic Risk of Chemi-
cals to Humans, Suppl. 2, Long-term and Shorl-term Screening Assays for Carcinogens: A Critical
Appraisal, Lyon, pp. 311-426
Phelps, R.G., Bernstein, L.E., Harpaz, N., Gordon, R.E., Cruickshank, F.A. & Schwartz, E. (1989)
Characterization of a dermal derived malignant mesenchymal tumor arising in ultraviolet irra-
diated mice. Am. 1 Patho/., 135, 149-159
Phillips, R. (1983) Sources and Applications of Ultraviolet Radiation, London, Academic Press
Pierceall, WE. & Ananthaswamy, H.N. (1991) Transformation of NIH 3T3 cells by transfection with
UV-irradiated human c-Ha-ras-1 proto-oncogene DNA. Oncogene, 6, 2085-2091
Pierceall, WE., Mukhopadhyay, T., Goldberg, L.H. & Ananthaswamy, H.N. (1991) Mutations in the
p53 tumor suppressor gene in human cutaneous squamous cell carcinomas. Mol. Carcinog., 4,
445-449
Pitcher, H.M. & Longstreth, J.D. (1991) Melanoma mortality and exposure to ultraviolet radiation: an
empirical relationship. Environ. int., 17, 7-21
Pitts, D.G., Cullen, A.P. & Hacker, P.O. (1977) Ocular effects of ultraviolet radiation from 295 to 365
nm. Invest. Ophthalmol. visual Sci., 16, 932-939
Plummer, N.A., Greaves, M.W., Hensby, C.N. & Black, A.K. (1977) Inflammation in human skin
induced by ultraviolet radiation. Postgrad. med. 1, 53, 6 ~ 7
Poulsen, J.T., Staberg, B., Wulf, H. C. & Brodthagen, H. (1984) Dermal elastosis in hairless mice after
UV-B and UV-A applied simultaneously, separately or sequentially. Br.1 Dermatol. , 110, 531-
538
Pound, A W (1970) Induced cell proliferation and the initiation of skin tumour formation in mice by
ultraviolet light. Pathology, 2, 269-275
Putschar, W. & Holtz, F. (1930) Production of skin tumours in rats by long duration UV irradiation
(Ger.). Z. Krebsforsch., 33, 219- 260
Putvinsky, A.V., Sokolov, AI., Roshchupkin, D.I. & Vladimirov, Y.A {1979) Electric breakdown of
bilayer phospholipid membranes under ultraviolet irradiation-induced lipid peroxidation.
FEBS Lett., 106, 53-55
Rasanen, L, Reunala, T., Lehto, M., Jansen, C., Rantala, I. & Leinikki, P. (1989) Immediate decrease in
antigen-presenting function and delayed enhancement of interleukin-1 production in human epi-
dermal cells after in vivo UVB irradiation. Br. l Dermatol., 120, 589-596
266 IARC MONOGRAPHS VOLUME 55
Rasmussen, R.E., HammerWilson, M. & Berns, M.W. {1989) Mutation and sister chromatid ex
change induction in Chinese hamster ovary (CHO) cells by pulsed excimer laser radiation at 193
nm and 308 nm and continuous UV radiation at 254 nm. Photochem. Photobiol., 49, 413-418
RayKeil, L. & Chandler, J. W. {1986) Reduction in the incidence of rejection of heterotopic murine
corneal transplants by pretreatment with ultraviolet radiation. Transplantation, 42, 403-406
Reddy, AL, Fialkow, P.J. & Salo, A. (1978) Ultraviolet radiationinduced chromosomal abnorma-
lities in fetal fibroblasts from New Zealand black mice. Science, 201, 920-922
Reeve, V.E., Greenoak, G.E., Gallagher, C.H., Canfield, PJ. & Wilkinson, FJ. (1985) Effect of immu-
nosuppressive agents and sunscreens on UV carcinogenesis in the hairless mouse. Aust. J. e.xp.
Bioi. med. Sci., 63, 655-665
Resnick, M.A., Westmoreland, J., Amaya, E. & Bloom, K. (1987) UV-Induced damage and repair in
centromere DNA of yeast. Mol. gen. Genet., 210, 16-22
Rigel, D.S., Friedman, RJ., Levenstein, M.J. & Greenwald, D.I. (1983) Relationship of fluorescent
lights to malignant melanoma: another view.1 Dermatol. surg. Oncol., 9, 836-838
Ringvold, A. (1980) Cornea and ultraviolet radiation. Acta ophthalmol., 58, 63-68
Rivers, J.K., Norris, P.G., Murphy, G.M., Chu, A.C., Midgley, G., Morris, J., Morris, R.W., Young,
A.R. & Hawk, J .L.M. ( 1989) UVA sun beds: tanning, photoprotection, acute adverse effects and
immunological changes. Br. 1 DermatoL, 120, 767-777
Roberts, L.K. & Daynes, R.A. (1980) Modification of the immunogenic properties of chemically
induced tumors arising in hosts treated concomitantly with ultraviolet light. J. Jmmunol., 125,
438-447
Roberts, L.K., Samlowski, W.E. & Daynes, R.A. (1986) Immunological consequences of ultraviolet
radiation exposure. Photodermatology, 3, 284-298
Robertson, D.F. (1972) Solar Ultraviolet Radiation in Relation to Human Sunburn and Skin Cancer,
PhD Thesis, University of Queensland, Australia
Robertson, B., Gahring, L., Newton, R. & Daynes, R. (1987) In vivo administration of interleukin 1 to
normal mice depresses their capacity to elicit contact hypersensitivity responses: prostaglandins
are involved in this modification of immune function. 1 invest. Dennatol., 88, 380-387
Robinson, J.K. (1987) Risk of developing another basal cell carcinoma. A 5-year prospective study.
118-120
Roffo, A.H. (1934) Cancer and the sun: carcinomas and sarcomas caused by the action of the sun in
toto {Fr.). Bull. ksoc. fr. Etude Cancer, 23, 590-616
Roffo, A. H. (1939) Physico-chemical etiology of cancer (with special emphasis on the association with
solar radiation) (Ger.). Strahlentherapie, 66, 328-350
Ronai, Z.A. & Weinstein, I.B. (1988) Identification of a UV-induced trans-acting protein that
stimulates polyomavirus DNA replication.1 Virol. , 1057-1060
Ronai, Z.A., Lambert, M.E., Johnson, M.D., Okin, E. & Weinstein, I.B. {1987) Induction of asynchro-
nous replication of polyoma DNA in rat cells by ultraviolet irradiation and the effects of various
inhibitors. Cancer Res., 47, 4565-4570
Ronai, Z.A., Lambert, M.E. & Weinstein, I.B. (1990) Inducible cellular responses to ultraviolet light
irradiation and other mediators of DNA damage in mammalian cells. Cell Bioi. Toxico/., 6,
105-126
Rooney, J.E, Bryson, Y., Mannix, M.L., Dillon, M., Wohlenberg, C.R., Banks, S., Wallington, CJ.,
Notkins, A.L. & Straus, S.E. (1991) Prevention of ultraviolet-lightinduced herpes labialis by
sunscreen. Lancet, 338, 1419-1422
REFERENCES 267
Rosario, R., Mark. GJ ., Parrish, J .A. & Mihm, M.C., J r (1979) Histological changes produced in skin
by equally erythemogenic doses of UVA, UVB, UVC with psoralens. Br. J. DennatoL, 101,
299-308
Rosdahl, I.K. (1979) Local and systemic effects on the epidermal melanocyte population in UV-
irradiated mouse skin. J. invest. Dennatol., 73, 306-309
Rosenstein, B.S. (1988) The induction of DNA strand breaks in normal human skin fibroblasts
exposed to solar ultraviolet radiation. Radial. Res., 116, 313-319
Rosenstein, B.S. & Ducore, J.M. (1983) Induction of DNA strand breaks in normal human fibroblasts
exposed to monochromatic ultraviolet and visible wavelengths in the 240-546 nm range.
Photochem. Photobiol., 38, 51-55
Rosenstein, B.S. & Mitchell, D.L. (1987) Action spectra for the induction of pyrimidine (6-4)pyri-
midone photoproducts and cyclobutane pyrimidine dimers in normal human skin fibroblasts.
Photochem. Photobiol., 45, 775-780
Rosenstein, B.S. & Mitchell, D.L. (1991) The repair of DNA damages induced in normal human skin
fibroblasts exposed to simulated sunlight. Radial. Res., 126, 338-342
Rosenstein, B.S. & Rosenstein, R.B. ( 1985) Induction of chromosome aberrations in ICR 2A frog cells
exposed to 265-313 nm monochromatic ultraviolet wavelengths and photoreactivating light
Photochem. Photobiol., 41, 57-61
Rosenstein, B.S., Murphy, J.T. & Ducore, J.M. (1985) Use of a highly sensitive assay to analyze the
excision repair of dimer and non-dimer DNA damages induced in human skin fibroblasts by 254
nm and solar ultraviolet radiation. Cancer Res., 45, 5526-5531
Rosenstein, B.S., Lai, L.-W., Ducore, J.M. & Rosenstein, R.B. (1989) DNA-protein crosslinking with
normal and solar UV-sensitive ICR 2A frog cell lines exposed to solar UV-radiation. Mutat. Res.,
217,219-226
Rosenthal, F.S., Phoon, C., Bakalian, A.E. & Taylor, H.R. (1988) The ocular dose of ultraviolet radia-
tion to outdoor workers. Invest. Ophthalmol. visual Sci., 29, 649-656
Rosenthal, F.S., Lew, R.A., Rouleau, LJ. & Thomson, M. (1990) Ultraviolet exposure to children from
sunlight: a study using personal dosimetry. Photodennatol. Photoimmunol. Photomed. , 7, 77-81
Rosenthal, F.S., West, S.K., Munoz, B., Emmett, E.A., Strickland, P.T. & Taylor, H.R. (1991) Ocular
and facial skin exposure to ultraviolet radiation in sunlight: a personal exposure model with
application to a worker population. Health Phys., 61, TI-86
Roser, M., Bohrn, A., Oldigs, M., Weichenthal, M., Reimers, U., Schmidt-Preuss, U., Breitbart, E.W.
& Rudiger, H.W. (1989) Ultraviolet-induced formation of micronuclei and sister chromatid
exchange in cultured fibroblasts of patients with cutaneous malignant melanoma. Cancer Genet.
Cytogenet., 41. 129-137
Roshchupkin, D.l., Pelenitsyn, A.B., Potapenko, A. Y., Talitsky, V.V. & Vladimirov, Y .A. (1975) Study
of the effects of ultraviolet light on biomembranes- IV. The effect of oxygen on UV-induced
hemolysis and lipid photoperoxidation in rat erythrocytes and liposomes. Photochem.
Photobiol., 21, 63-69
Ross, J.A., Howie, S.E.M., Norval, M., Maingay, J. & Simpson, T.J. (1986) Ultraviolet-irradiated
urocanic acid suppresses delayed-type hypersensitivity to herpes simplex virus in mice. J. invest.
Dennatol., 87, 630-633
Ross, J.A., Howie, S.E.M., Norval, M. & Maingay, J. (1987) Two phenotypically distinct T cells are
involved in ultraviolet-irradiated urocanic acid-induced suppression of the efferent delayed-type
hypersensitivity response to herpes simplex virus, type 1 in vivo. J. invest. Dermatol., 89, 230-233
268 IARC MONOGRAPHS VOLUME 55
Roth, D.E., Hodge, SJ. & Callen, J.P. (1989) Possible ultraviolet A-induced lentigines: a side effect of
chronic tanning salon usage. J. Am. Acad. DertnllloL, 20, 950-954
Roza, L., van der Wulp. KJ .M., MacFarlane, SJ ., Lohman, P.H.M. & Baan, R.A. (1988) Detection of
cyclobutane thymine dimers in DNA of human cells with monoclonal antibodies raised against a
thymine dimer-containing tetranucleotide. Photochem. Photobiol., 48, 627-633
Ruiz-Rubio, M., Woodgate, R., Bridges, B.A., Herrera, G. & Blanco, M. (1986) New role for photo-
reversible pyrimidine dimers in induction of prototrophic mutations in excision-deficient
Escherichia coli by ultraviolet light. J. Bacterial., 166. 1141-1143
Rusch, H.P., Kline, B.E. & Baumann, C.A. (1941) Carcinogenesis by ultraviolet rays with reference to
wavelength and energy. Arch. Patho/., 31, 135-146
Russell, W.O., Wynne, E.S., Loquvam, G.S. & Mehl, D.A. (1956) Studies on bovine ocular squamous
carcinoma ('cancer eye'). I. Pathological anatomy and historical review. Cancer, 9, 1-52
Saftlas, A.F, Blair, A., Cantor. K.P., Hanrahan, L. & Anderson, H.A. (1987) Cancer and other causes
of death among Wisconsin farmers. Am. J. ind. Med., l 1, 119-129
Sagher, D. & Strauss, B. (1983) Insertion of nucleotides opposite apurinic/apyrimidinic sites in
deoxyribonucleic acid during in vitro synthesis: uniqueness of adenine nucleoli des. Biochemistry,
22,4518-4526
Sammartano, L.J. & Tuveson, R.W. (1985) Hydrogen peroxide induced resistance to broad-spectrum
near-ultraviolet light (300-400 nm) inactivation in Escherichia coli. Photochem. Photobiol., 41,
367-370
Sammartano, L.J. & Tuveson, R.W. (1987) Escherichia coli strains carrying the cloned cytochrome d
terminal oxidase complex are sensitive to near-UV inactivation. J. Bacterial., 169, 5304-5307
Sancar, A. & Rupp, W.D. (1983) A novel repair enzyme: UVRABC excision nuclease of Escherichia
coli cuts a DNA strand on both sides of the damaged region. Ceil, 33, 249- 260
Sanderson, B.J.S., Dempsey, J.L. & Morley, A.A. (1984) Mutations in human lymphocytes: effects of
x- and UV-irradiation. Mutat. Res., 140, 2'23-227
Sanford, K.K., Parshad, R., Jones, G., Randleman, S .. Garrison, C. & Price, F.-(1979) Role of photo-
sensitization and oxygen in chromosome stability and 'spontaneous' malignant transformation
in culture. J. nat{ Cancer lnst., 63, 1245-1255
Santamaria, L., Giordano, G.G., Alfisi, M. & Cascione, F. (1966) Effects of light on 3,4-benzpyrene
carcinogenesis. Nature, 210, 824-825
Santamaria, L., Bianchi, A., Arnaboldi, A.. Daffara, P. & Andreoni, L. (1985) Photocarcinogenesis by
methoxypsoralen, neutral red, proflavine, and long UV radiation. Cancer Detect. Prev., 8, 447-454
Sauder, D.N., Tamaki, K., Moshell, A.N., Fujiwara, H. & Katz, S.I. (1981) Induction of tolerance to
topically applied TNCB using TNP-conjugated ultraviolet light-irradiated epidermal cells. J.
lmmunol., 127, 261-265
Sauder, D.N., Noonan, FP., DeFabo, E. C. & Katz, S.I. (1983) Ultraviolet radiation inhibits alloantigen
presentation by epidermal cells: partial reversal by the soluble epidermal cell product, epidermal
cell-derived thymocyte-activating factor {ETAF). 1 invest. Dermatol. , 80, 485-489
Sayre, R.M. & Kligman, L.H. (1992) Discrepancies in the measurement of spectral sources. Photo-
chem. Photobiol. , 55, 141-143
Schaaper, R.M., Kunkel, T.A. & Loeb, L.A. (1983) Infidelity of DNA synthesis associated with bypass
of apurinic sites. Proc. nat/ Acad. Sci. USA, 80, 487-491
Schaaper, R.M., Dunn, R.L. & Glickman, B.W. {1987) Mechanisms of ultraviolet-induced mutation.
Mutational spectra in the Escherichia coli laci gene for a wild-type and an excision-repair defi-
cient strain. J. mol. Bioi., 198, 187-202
-- - - - ---- - - --- --- --- - --
REFERENCES 269
Schacter, B., Lederman, M.M., LeVine, M.J. & Ellner, J.J. (1983) Ultraviolet radiation inhibits human
natural killer activity and lymphocyte proliferation. J Immunol., 130, 2484-2487
Scheibner, A., McCarthy, W.H., Milton, G.W. & Nordlund. J.J. (1983) Langerhans cell and melanocyte
distribution in 'normal' human epidermis. Aust. J DermatoL, 24, 9-16
Scheibner, A., Hollis, D.E., McCarthy, W.H. & Milton, G. W. (1986a) Effects of exposure to ultraviolet
light in a commercial solarium on Langer hans cells and melanocytes in human epidermis.Aust.J
Dermatol., 21, 35-41
Scheibner, A., Hollis, D.E., McCarthy, W.H. & Milton, G.W. (1986b) Effects of sunlight exposure on
Langerhans cells and melanocytes in human epidermis. Photodermatology, 3, 15-25
Schothorst, A.A., Slaper, H., Telgt, D., AJhadi, B. & Suurmond, D. (1987a) Amounts of ultraviolet B
(UVB) received from sunlight or artificial UV sources by various population groups in the
Netherlands. In: Passchier, W.F. & Bosnjakovic, B.F.M., eds, Human Exposure to Ultraviolet
Radiation: Risks and Regulations, Amsterdam, Elsevier, pp. 269-273
Schothorst, A.A., Enninga, E. C. & Simons, J. W.I.M. ( 1987b) Mutagenic effects per erythemal dose of
artificial and natural sources of ultraviolet light. In: Passchier, W.F. & Bosnjakovic, B.F.M., eds,
Human Exposure to Ultraviolet Radiation: Risks and Regulations, Amsterdam, Elsevier, pp. 103-
107
Schothorst, A.A., Evers, L.M., Noz, K.C., Filon, R. & van Zeeland, A.A. (1991) Pyrimidine dimer
induction and repair in cultured human skin keratinocytes or melanocytes after irradiation with
monochromatic ultraviolet radiation. J invest. Dermatol., 96, 916-920
van der Schroeff, J.G., Evers, L.M., Boot, A.J.M. & Bos, J .L. (1990) ras Oncogene mutations in basal
cell carcinomas and squamous cell carcinomas of human skin.J invest. Dermatol. , 94,423-425
Schulze, R. (1962) On the climate of the Earth (Ger.). Strah/entherapie, 119, 321-348
Schulze, R. (1970) Global radiation climate (Ger.). Wiss. Forschunpysber., 12, 1-220
Schulze, R. & Grafe, K. (1969) Consideration of sky ultraviolet radiation in the measurement of solar
ultraviolet radiation. In: Urbach, F., ed., The Biological Effects of Ultraviolet Radiation (Pro-
ceedings of the First International Conference), Oxford, Pergamon Press, pp. 359-373
Schwartz, S.M. & Weiss, N.S. (1988) Place of birth and incidence of ocular melanoma in the United
States. Int 1 Cancer, 41, 174-177
Schwarz, T., Urbanska, A., Gschnait, F. & Luger, T.A. {1986) Inhibition of the induction of contact
hypersensitivity by a UV-mediated epidermal cytokine. J. invest. Dermatol., 87, 289-291
Schwarz, T., Urbanski, A., Kirnbauer, R., Kock, A, Gschnait, F. & Luger, T.A (1988) Detection of a
specific inhibitor of interleukin 1 in sera of UVB-treated mice. J invest. Dermato/., 91, 536-540
Scotto, J. & Fears, T.R. (1987) The association of solar ultraviolet and skin melanoma incidence
among Caucasians in the United States. Cancer Invest., 5, 275-283
Scotto, J., Kopf, A.W. & Urbach, F. (1974) Non-melanoma skin cancer among Caucasians in four
areas of the United States. Cancer, 34, 1333-1338
Scotto, J., Fears, T. & Gori, G. (1976) Measurements of Ultraviolet Radiations in the United States and
Comparisons with Skin Cancer Data (NIH Publ. No. 76-1029), Washington DC, US Department
of Health, Education, and Welfare
Scotto, J., Fears, T.R. & Fraumeni, J.F., Jr (1982) Solar radiation. In: Schottenfeld, D. & Fraumeni,
J.F., Jr, eds, Cancer Epidemiology and Prevention, PhiJadelphia, W.B. Saunders, pp. 254-276
Scotto, J., Fears, T.R. & Fraumeni, J.F., Jr (1983) Incidence ofNonmelanoma Skin Cancer in the United
States (NIH PubJ. No. 83-2433), Bethesda, MD, National Cancer Institute
270 IARC MONOGRAPHS VOLUME 55
Seddon, J.M., Gragoudas, E.S., Glynn, R.J., Egan, K.M. , Albert, D.M. & Blitzer, P.H. {1990) Host
factors, UV radiation and risk of uveal melanoma. A case-control study. Arch. Ophthalmol., 108,
1274-1280
Seetharam, S., Protic-Sabljic, M., Seidman, M.M. & Kraemer, K.H. {1987) Abnormal ultraviolet
mutagenic spectrum in plasmid DNA replicated in cultured fibroblasts from a patient with the
skin cancer-prone disease, xeroderma pigmentosum. J. clin. Invest., 80, 1613-1617
Seguin, LR., Tarone, R.E., Liao, K & Robbins, J.H. (1988) Ultraviolet light-induced chromosomal
aberrations in cultured cells from Cockayne syndrome and complementation group C xero-
derma pigmentosum patients: lack of correlation with cancer susceptibility. Am. J. hum. Genet.,
42,468-475
Sekiya, T., Fushimi, M., Hori, H., Hirohashi, S., Nishimura, S. & Sugimura, T. (1984) Molecular
cloning and the total nucleotide sequence of the human c-Ha-ras-1 gene activated in a melanoma
from a Japanese patient. Proc. nat/ Acad. Sci. USA, 81, 4771-4775
Servilla, K.S., Burnham, D.K. & Daynes, R.A. (1987) Ability of cyclosporine to promote the growth of
transplanted ultraviolet radiation-induced tumors in mice. Transplantation, 44, 291-295
Setlow, R.B. (1968) Photoproducts in DNA irradiated in vivo. Photochem. Photobiol., 1, 64349
Setlow, R.B. (1975) The relevance of photobiological repair. An. Acad. Bras. Cienc., 45 (Suppl. 215),
215-220
Setlow, R.B. & Carrier, WL. (1966) Pyrimidine dimers in ultraviolet-irradiated DNXs. J. mol. Bioi.,
17, 237-254
Setlow, R.B., Swenson, P.A. & Carrier, WL. (1963) Thymine dimers and inhibition of DNA synthesis
by ultraviolet irradiation of cells. Science, 142, 1464-1466
Setlow, R.B., Woodhead, A.D. & Grist, E. (1989) Animal model for ultraviolet radiation-induced
melanoma: platyfish-swordtail hybrid. Proc. nat/ Acad. Sci. USA, 86, 8922-8926
Shabad, LM. & Litvinova, S.N. (1972) The combined effect of UV irradiation and 7,12-DMBA on the
skin of hairless mice (Russ.). Biu/1. eksp. Bioi. Med., 73, 84-85
Shanmugaratnam, K., Lee, H.P. & Day, N.E., eds (1983) Cancer Incidence in Singapore 1968-1977
(IARC Scientific Publications No. 47), Lyon, IARC, p. 73
Shetlar, M.D. (1980) Cross-linking of proteins to nucleic acids by ultraviolet light. Photochem.
Photobiol. Rev. , 5, 105-197
Shukla, V.K., Hughes, D.C., Hughes, L.E., McCormick, F. & Padua, R.A. (1989) ras Mutations in
human melanotic lesions: K-ras activation is a frequent and early event in melanoma deve-
lopment. Oncogene Res., 5, 121-127
Siede, W. & Eckardt, E (1986) Analysis of mutagenic DNA repair in a thermoconditional mutant of
Saccharomyces cerevisiae. III. Dose- response pattern of mutation induction in UV-irradiated
rev2ts cells. Mol. gen. Genet., 202, 68-74
Siemiatycki, J. (1991) Risk Factors for Cancer in the Workplace, Boca Raton, FL, CRC Press
Silverstone, H. & Gordon, D. (1966) Regional studies in skin cancer. Second report: wet tropical and
subtropical coasts of Queensland. Med. J. Aust., 2, 733-740
Silverstone, H. & Searle, J .H.A. (1970) The epidemiology of skin cancer in Queensland: the influence
of phenotype and environment. Br. J. Cancer, 24, 235-252
Singh, B. & Gupta, R.S. (1982) Mutagenic response to ultraviolet light and X-rays at five independent
genetic loci in Chinese hamster ovary cells. Environ. Mutag., 4, 543-551
Sisson, T.R.C. & o g ~ T.P. (1982) Phototherapy of hyperbilirubinemia. In: Regan, J.D. & Parrish, J.A.,
eds, The Science of Photomedicine, New York, Plenum, pp. 477-509
REFERENCES
271
Sjovall, P. & Christensen, O.B. (1986) Local and systemic effect of ultraviolet irradiation (UVB and
UVA) on human allergic contact dermatitis. Acta dermatol. venereol. , 66, 290-294
Slaga, TJ., Klein-Szanto, A.J.P., Triplett, L.L., Yotti, L.P. & Trosko, J.E. (1981) Skin tumor-promoting
activity of benzoyl peroxide, a widely used free radical-generating compound. Science, 213,
1023-1025
Slaper, H. (1987)Skin Cancer and UV Exposure: Investigations on the Estimation of Risks, PhD Thesis,
University of Utrecht
Sliney, D.H. (1986) Physical factors in cataractogenesis: ambient ultraviolet radiation and tempe-
rature. Invest. Ophtha/mol. visual Sci. , 27, 781- 790
Sliney, D.H. {1990) The IRPAJINIRC guidelines or limits of exposure to laser radiation. In: Grandolfo,
M., Rindi, S. & Sliney, D.H., eds, Light, Lasers, and Synchrotron Radiation. A Health Risk
Assessment, New York, Plenum, pp. 341-346
Sliney, D.H. & Wolbarsht, M. (1980) Safety with Lasers and Other Optical Sources: A Comprehensive
Handbook, New York, Plenum
Sliney, D., Wood, R.L., Jr, Moscato, P.M., Marshall, WJ. & Eriksen, P. (1990) Ultraviolet exposure in
the outdoor environment: measurement of ambient ultraviolet exposure levels at large zenith
angles. In: Grandolfo, M., Rindi, S. & Sliney, D.H., eds, Light, Lasers, and Synchrotron Radiation.
A Health Risk Assessment, New York, Plenum, pp. 169-180
Smith, K.C. (1964) The photochemistry of thymine and bromouracil in vivo. Photochem. Photobiol., 3,
1-10
Smith, K.C. (1976) The radiation-induced addition of proteins and other molecules to nucleic acids.
In: Wang, S.Y., ed., Photochemistry and Photobiology of Nucleic Acids, Vol. 2, New York,
Academic Press, pp. 187-218
Smith, K.C., ed. (1989) The Science of Photobiology, 2nd ed., New York. Plenum, pp. 47-53
Sorahan, T. & Grimley, R.P. (1985) The aetiological significance of sunlight and fluorescent lighting in
malignant melanoma: a case-control study. Br. 1 Cancer, 52, 765-769
Spangrude, G.J., Bernhard, E.J., Ajioka, R.S. & Daynes, R.A. {1983) Alterations in lymphocyte
homing patterns within mice exposed to ultraviolet radiation. J. lmmunol., 130, 2974-2981
Spellman, C. W & Daynes, R.A. (1978) Properties of ultraviolet light-induced suppressor lymphocytes
within a syngeneic tumor system. Cell. Immunol., 36, 383-387
Spellman, C.W, Woodward, J.G. & Daynes, R.A. (1977) Modification of immunological potential by
ultraviolet radiation. I. Immune status of short-term UV-irradiated mice. Transplantation, 24,
112-119
Spikes, J.D., Kripke, M.L., Connor, R.J. & Eichwald, E.J. (1977) Time of appearance and histology of
tumors induced in the dorsal skin of C3Hf mice by ultraviolet radiation from a mercury arc lamp.
1 nad Cancer Inst., 59, 1637-1643
Spitzer, WO., Hill, G.B., Chambers, L.W, Helliwell, B.E. & Murphy H.B. (1975) The occupation of
fishing as a risk factor in cancer of the lip. New Engl. 1 Med., 293, 419-424
Spruance, S.L. (1985) Pathogenesis of herpes simplex labialis: experimenta1 induction of lesions with
UV light. J. clin. Microbiol. , 22, 366-368
Staberg, B., Wulf, H.C., Poulsen, T., Klemp, P. & Brodthagen, H. (1983a) Carcinogenic effect of
sequential artificial sunlight and UVA irradiation in hairless mice. Consequences for solarium
' therapy'. Arch. Dennato/., 119, 641-643
Staberg, B., Wulf, H.C., Klemp, P., Poulsen, T. & Brodthagen, H. (1983b) The carcinogenic effect of
UVA radiation.1 invest. Dennatol., 81, 517-519
272 !ARC MONOGRAPHS VOLUME 55
Stanley, S.K., Folks, T.M. & Fauci, A.S. (1989) Induction of expression of human immunodeficiency
virus in a chronically infected promonocytic cell line by ultraviolet irradiation. AIDS Res. hum.
Retroviruses, 5, 375-384
Stefanini, M., Lagomarsini, P., Arlett, C.F., Marinoni, S., Borrone, C., Crovato, F., Trevlsan, G.,
Cordone, G. & Nuzzo, F. (1986) Xeroderma pigmentosum (complementation group D) mutation
is present in patients affected by trichothiodystrophy with photosensitivity. Hum. Genet., 74,
107-112
Stein, B., Rahmsdorf, H.J., Steffen, A., Litfin, M. & Herrlich, P. (1989) UV-Induced DNA damage is
an intermediate step in UV-induced expression of human immunodeficiency virus type 1, colla-
genase, c-fos, and metallothionein. Mol. cell. Bioi., 9, 5169-5181
Steinitz, R., Parkin, D.M . Young, J.L., Bieber, C.A. & Katz, L., eds (1989) Cancer Incidence in Jewish
Migrants to Israel, 1961-1981 (IARC Scientific Publications No. 98), Lyon, IARC, pp. 114-115,
134-135
Stenblick, F. (1975a) Species-specific neoplastic progression by ultraviolet light on the skin of rats,
guinea pigs, hamsters and mice. Oncology, 31, 209-225
Stenblick, F. (1975b) Studies on the modifying effect of ultraviolet radiation on chemical skin
carcinogenesis. J. invest. Dennatol., 64, 253-257
Stenback, F. (1975c) Ultraviolet light irradiation as initiating agent in skin tumor formation by the
two-stage method. Eur. J. Cancer, 11, 241-246
Stenback, F. (1978) Life history and histopathology of ultraviolet light-induced skin tumors. Nat/
Cancer Inst. Monogr., 50, 57-70
Stenblick, F. & Shubik, P. (1973) Carcinogen-induced skin tumorigenesis in mice: enhancement and
inhibition by ultraviolet light. Z. Krebsforsch., 79, 234-240
Sterenborg, H.J.C.M. & van der Leun, J.C. (1987) Action spectra for tumorigenesis by ultraviolet
radiation. In: Passchier, W.F. & Bosnjakovic, B.F.M., eds, Human Exposure to Ultraviolet
Radiation: Risks and Regulations, Amsterdam, Elsevier, pp. 173-191
Sterenborg, H.J.C.M. & van der Leun, J.C. (1988) Change in epidermal transmission due to UV-
induced hyperplasia in hairless mice: a first approximation of the action spectrum. Photo-
dermatology, S, 71-82
Sterenborg, HJ.C.M. & van der Leun, J.C. (1990) Tumorigenesis by a long wavelength UVA source.
Photochem. Photobio/., 51, 325-330
Sterenborg, HJ.C.M., de Gruijl, P.R. & van der Leun, J.C. (1986) UV-Induced epidennal hyperplasia
in hairless mice. Photodermatology, 3, 206-214
Sterenborg, H.J.C.M., van der Putte, S.C.J. & van der Leun, J.C. (1988) The dose-response relation-
ship of tumorigenesis by ultraviolet radiation of 254 nm. Photochem. Photobiol., 47, 245-253
Sterenborg, HJ.C.M., de Gruijl, P.R., Kelfkens, G. & van der Leun, J.C. (1991) Evaluation of skin
cancer risk resulting from long term occupational exposure to radiation from ultraviolet lasers in
the range from 190 to 400 nm. Photochem, Photobiol., 54, 775-780
Stierner, U., Rosdahl, 1., Augustsson, A. & Kagedal, B. (1989) UVB irradiation induces melanocyte
increase in both exposed and shielded human skin. J. invest. Dennatol., 92, 561-564
Stingl, L.A., Sauder, D.N., Iijima, M., Wolff, K., Pehamberger, H. & Sting}, G. (1983) Mechanism of
UVB induced impairment of the antigen-presenting capacity of murine epidermal cells. J.
Immunol., 130, 1586-1591
Streeter, P.R. & Fortner, G.W. (1988a) Immune response to ultraviolet-induced tumors. II. Effector
cells in tumor immunity. Transplantation, 46, 250-255
REFERENCES 273
Streeter, P.R. & Fortner, G.W. (1988b) Immune response to ultraviolet induced tumors. III. Analysis
of cloned lymphocyte populations exhibiting antitumor activity. Transplantation, 46, 256-260
Streilein, J.W. & Bergstresser, P.R. (1981) Langerhans cell function dictates induction of contact
hypersensitivity or unresponsiveness to DNFB in Syrian hamsters. 1 invest. Dermatol., 77,
272-277
Streilein, J.W., Toews, G.T., Gilliam, J.N. & Bergstresser, P.R. (1980) Tolerance or hypersensitivity to
the role of Langerhans cell density within epidermis. 1 invest.
Dermatol., 74, 319-322
Strickland, P.l: (1982) Tumor induction in Sencar mice in response to ultraviolet radiation. Carcino-
1487- 1489
Strickland, P.T. (1986) Photocarcinogenesis by near-ultraviolet (UVA) radiation in Sencar mice.
1 invest. Dermatol., 87, 272-275
Strickland, P.T., Burns, F J. & Albert, R.E. (1979) Induction of skin tumors in the rat by single exposure
to ultraviolet radiation. Photochem. Photobiol., 30, 683-688
Strickland, P.T., Creasia, D. & Kripke, M.L. ( 1985) Enhancement of two-stage skin carcinogenesis by
exposure of distant skin to UV radiation. J. nat/ Cancer Inst., 74, 1129-1134
Strickland, P.l:, Bruze, M. & Creasey, J. (1988) Cyclobuta-dithymidine induction by solar-simulating
UV radiation in human skin. I. Protection by constitutive pigmentation. Photodermatology, 5,
166-169
Sundararaman, N., StJohn, D.E. & Venkateswaran, S. V. (1975) Solar Ultraviolet Radiation Received at
the Earth's Surface Under Clear and Cloudless Conditions, Springfield, VA, National Technical
Information Service
Sutherland, B.M., Harber, L.C. & Kochevar, I.E. (1980) Pyrimidine dimer formation and repair in
human skin. Cancer Res., 40, 3181- 3185
Sutherland, B.M., Delihas, N.C., Oliver, R.P. & Sutherland, J .C. (1981) Action spectra for ultraviolet
light-induced transformation of human cells to anchorage-independent growth. Cancer Res., 41,
2211-2214
Sutherland, B.M., Freeman, A. G. & Bennett, P.V. (1988) Human cell transformation in the study of
sunlight-induced cancers in the skin of man. Mutat. Res., 199, 425-436
Suzuki, H., Fukuyama, K. & Epstein, W.L. (1977) Changes in nuclear DNA and RNA during
dermal keratinization. Cell Tissue Res., 184, 155-167
Suzuki, F., Han, A., Lankas, G .R., Utsumi, H. & Elkind, M.M. (1981) Spectral dependencies of killing,
mutation, and transformation in mammalian cells and their relevance to hazards caused by solar
ultraviolet radiation. Cancer Res., 41, 4916-4924
Swerdlow, A.J. (1979) Incidence of malignant melanoma of the skin in England and Wales and its
relationship to sunshine. Br. med. J., ii, 1324-1327
Swerdlow, A.J. (1983a) Epidemiology of melanoma of the eye in the Oxford region, 1952-78. Br. J.
Cancer, 47, 311-313
Swerdlow, A.J. (1983b) Epidemiology of eye cancer in adults in England and Wales, 1%2-77. Am.1
Epidemiol., 118, 294-300
Swerdlow, A.J. {1985) Seasonality of presentation of cutaneous melanoma, squamous cell cancer and
basal cell cancer in the Oxford region. Br. J. Cancer, 52, 893-900
Swerdlow, AJ., English, J.S.C., MacKie, R.M., O'Doherty, CJ., Hunter, J.A.A., Clark, J. & Hole, OJ.
(1988) Fluorescent lights, ultraviolet lamps, and risk of cutaneous melanoma. Br. med. J., 297,
.
274 IARC MONOGRAPHS VOLUME 55
Sylvania (undated) Germicidal and Short-wave Ultraviolet Radiation, Danvers, MA, GTE Products
Corporation
Szabo, G., Gerald, A.B., Pathak, M.A. & Fitzpatrick, T.B. (1972) The ultrastructure of racial color
differences in man. In: Riley, V., ed., Pigmentation. Its Genesis and Biologic Control, New York,
Appleton-Century-Crofts, pp. 23-41
Szebeni, J. & Tollin, G. (1988) Some relationships between ultraviolet light and heme-protein-induced
peroxidative lipid breakdown in liposomes, as reflected by fluorescence changes: the effect of
negative surface charge. Photochem. Photobiol., 47, 475-479
Takebe, H., Nishigori, C. & Satoh, Y. (1987) Genetics and skin cancer ofxeroderma pigmentosum in
Japan. Jpn. J. Cancer Res. (Gann), 18, 1135-1143
Talve, L., Stenback, F. & Jansen, C.T. (1990) UVA irradiation increases the incidence of epithelial
tumors in UVB-irradiated hairless mice. Photodei71Ultol. Photoimmunol. Photomed., 7,109-115
Tamaki, K & lijima, M. (1989) The effect of ultraviolet B irradiation on delayed-type hypersensitivity,
cytotoxic T lymphocyte activity, and skin graft rejection. Transplantation, 41, 372-376
Tan, E.M. & Stoughton, R.B. (1969) Ultraviolet light induced damage to deoxyribonucleic acid in
human skin. J. invest. Dermatol . 52, 537-542
Taylor, H.R., West, S.K., Rosenthal, F.S .. Munoz. B., Newland, H.S .. Abbey, H. & Emmett, E.A. (1988)
Effect of ultraviolet radiation on cataract formation. New Engl. J. Med. , 319, 1429-1433
Taylor, H.R., West, S.K, Rosenthal, F.S., Munoz. B., Newland, H.S. & Emmett, E.A. (1989) Corneal
changes associated with chronic UV irradiation. Arch. Ophthalmol., 107, 1481-1484
Teppo, L., Pakkanen, M. & Hakulinen, T (1978) Sunlight as a risk factor of malignant melanoma of the
skin. Cancer, 41, 2018-2027
Teppo, L., Pukkala, E., Hakama, M., Hakulinen, T. Herva, A. & Saxen, E. (1980) Way of life and
cancer incidence in Finland. A municipality-based ecological analysis. Scand. J. soc. Med.,
Suppl. 19, 5-84
Tessman, I. & Kennedy, M.A. {1991) The two-step model of UV mutagenesis reassessed: deamination
of cytosine in cyclobutane dimers as the likely source of the mutations associated with photo-
reactivation. Mol. gen. Genet . 227, 144-148
Thiers, B.H., Maize, J.C.. Spicer, S.S. & Cantor, A.B. (1984) The effect of aging and chronic sun
exposure on human Langerhans cell population. J invest. Dermatol., 82, 223-226
Tjemlund, U. & Juhlin, L. (1982) Effect of UV radiation on immunological and histochemical
markers of Langerhans cells in normal appearing skin of psoriatic patients. Acta dermatol., 272,
171-176
11sty, T.D., Brown, P.C. & Schimke, R.T. (1984) UV radiation facilitates methotrexate resistance and
amplification of the dihydrofolate reductase gene in cultured 3T6 mouse cells. Mol. cell. Bioi., 4,
1050-1056
Toda, K.-1., Miyachi, Y., Nesumi , N., Konishi, J. & Imamura, S. (1986) UVB/PUVA-induced sup-
pression of human natural killer activity is reduced by superoxide dismutase and/or interleukin 2
in vitro. J invest. Dermatol., 86, 519- 522
Toews, G.B., Bergstresser, P.R. & Streilein, J .W (1980) Epidermal Langerhans cell density determines
whether contact hypersensitivity or unresponsiveness follows skin painting with DNFB. J.
lmmunol., 124, 445-453
Tominaga, A., Lefort, S., Mizel, S.B., Dambrauskas, J.T., Granstein, R., Lowy, A., Benacerraf, B. &
Greene, M.I. (1983) Molecular signals in antigen presentation. I. Effects of interleukin 1 and 2 on
radiation-treated antigen-presenting cells in vivo and in vitro. Clin.Immunol. Immunopathol., 29,
282-293
REFERENCES 275
rrosko, J.E. & Brewen, J.G. (1967) Inhibition of ultraviolet-induced chromosome breaks by cys-
teamine in 5-bromouracil-substituted mammalian cells. Radial. Res., 32, 200-213
Thcker, M.A., Boice, J.D., Jr & Hoffman, D.A. (1985a) Second cancer following cutaneous melanoma
and cancers of the brain, thyroid, connective tissue, bone and eye in Connecticut, 1935-82. Nat/
Cancer Jnst. Monogr., 68, 161-189
Tucker, M.A., Shields, J.A., Hartge, P., Augsberger, J., Hoover, R.N. & Fraumeni, J.F., Jr (1985b)
Sunlight exposure as risk factor for intraocular malignant melanoma. New Engl. 1 Med., 313,
789-792
Turner, BJ., Siatkowski, R.M., Augsburger, J.J., Shields, J.A., Lustbader, E. & Mastrangelo, MJ.
(1989) Other cancers in uveal melanoma patients and their families. Am. 1 Ophtludmol., 107,
601-608
Tuveson, R.W. & Sammartano, LJ. (1986) Sensitivity of HemA mutant Escherichia coli cells to
inactivation by near-UV light depends on the level of supplementation with 8-aminolevuliriic
acid. Photochem. Photobiol., 43, 621-626
Tyrrell, R.M. (1973) Induction of pyrimidine dimers in bacterial DNA by 365 nm radiation.
Photochem. Photobio/., 17, 69-73
Tyrrell, R.M. (1982) Cell inactivation and mutagenesis by solar ultraviolet radiation. In: Helime, C.,
Charlier, M., Montenay-Garestier, T. & Laustriat, G., eds, Trends in Photobiology, New York,
Plenum, pp. 155-172
"JYrrell, R.M. (1984) Mutagenic action of monochromatic UV radiation in the solar range on human
cells. Mutat. Res., 129, 103-110
'JYrrell, R.M. (1985) A common pathway for protection of bacteria against damage by solar UVA (334
nm, 365 nm) and an oxidising agent (H202). Mutat. Res., 145, 129-136
1}rrrell, R.M. (1991) UVA (320-280 nm) radiation as an oxidative stress. In: Sir, H., ed., Oxidative
Stress: Oxidants and Antioxidants, London, Academic Press, pp. 57-83
'l}rrrell, R.M. & Pidoux, M. (1986) Endogenous glutathione protects human skin fibroblasts against
the cytotoxic action of UVB, UVA and near-visible radiations. Photochem. Photobiol., 44,
561-564
l:yrrell, R.M. & Pidoux, M. (1988) Correlation between endogenous glutathione content and
sensitivity of cultured human skin cells to radiation at defined wavelengths in the solar ultraviolet
range. Photochem. Photobiol., 41, 405-412
Tyrrell, R.M. & Pidoux, M. (1989) Singlet oxygen involvement in the inactivation of cultured human
fibroblasts by UVA (334 nm, 365 nm) and near visible (405 nm) radiations. Photochem.
Photobio/., 49, 407-412
Tyrrell, R.M., Ley, R.D. & Webb, R.B. (1974) Induction of single-strand breaks (alkali-labile bonds) in
bacterial and phage DNA by near UV (365 nm) radiation. Photochem. Photobiol., 20, 395-398
Ullrich, S.E. (1985) Suppression oflymphoproliferation by hapten-specific suppressor T lymphocytes
from mice exposed to ultraviolet radiation. Immunology, 54, 343-352
Ullrich, S.E. (1986) Suppression of the immune response to allogeneic histocompatibility antigens by
a single exposure to ultraviolet radiation. Transplantation, 42, 287-291
Ullrich, S.E. (1987) The effect of ultraviolet radiation-induced suppressor cells on T-cell activity.
Immunology, 60, 353-360
Ullrich, S.E. & K.ripke, M.L. (1984) Mechanisms in the suppression of tumor rejection produced in
mice by repeated UV radiation.! Immunol., 133, 2786-2790
276 IARC MONOGRAPHS VOLUME 55
Ullrich, S.E., Yee, G.K. & Kripke, M.L (1986a) Suppressor lymphocytes induced by epicutaneous
sensitization of UV-irradiated mice control multiple immunological pathways. Immunology, 58,
185-190
Ullrich, S.E., Azizi, E. & Kripke, M.L. (1986b) Suppression of the induction of delayed-type
hypersensitivity reactions in mice by a single exposure to ultraviolet radiation. Photochem.
Photobiol., 43, 633-638
Ultra-Violet Products, Inc. (1977) Laboratory Applications for Ultraviolet Equipment, San Gabriel, CA
United Kingdom Stratospheric Ozone Review Group (1991) Stratospheric Ozone 1991, London, Her
Majesty's Stationery Office
United Nations Environment Programme (1989) Environmental Effects Panel Report, Geneva
Unrau, P., Wheatcroft. R., Cox, B. & Olive, T. (1973) The formation of pyrimidine dimers in the DNA
of fungi and bacteria. Biochim. biophys. Acta, 312, 626-632
Urbach, F., Davies, R.E. & Forbes, P.D. (1966) Ultraviolet radiation and skin cancer in man. In:
Montagna, W. & Dobson, R.L, eds,Advances in Biology of Skin, Vol. VII, Carcinogenesis, Oxford,
Pergamon Press, pp. 195-214
Urbach, F., Epstein, J.H. & Forbes, P.D. (1974) Ultraviolet carcinogenesis: experimental, global and
genetic aspects. In: Pathak. M.A., Harber, LC., Seiji, M. & Kukita, A., eds, Sunlight and Man.
Normal and Abnormal Photobiologic Responses, Tokyo, University of Tokyo Press, pp. 259-283
Vagero, D., Ringback, G. & Kiviranta, H. (1986) Melanoma and other tumours of the skin among
office, other indoor and outdoor workers in Sweden 1961- 1979. Br. J. Cancer, 53, 507-512
Vagero, D., Swerdlow, AJ. & Beral, V. (1990) Occupation and malignant melanoma: a study based on
cancer registration data in England and Wales and in Sweden. Br. J. ind. Med., 47, 317-324
Valerie, K. & Rosenberg, M. (1990) Chromatin structure implicated in activation of IDV-1 gene
expression by ultraviolet light. New Bioi., 2, 712-718
Valerie, K., Deters, A., Bruck, C., Thiriart, C., Rosenberg, H., Debouck, C. & Rosenberg, M. (1988)
Activation of human immunodeficiency virus type 1 by DNA damage in human cells. Nature,
333, 78-81
Varghese, A.J. & Patrick, M.H. (1969) Cytosine derived heteroadduct formation in ultraviolet-
irradiated DNA Nature, 223, 299-300
Varghese, AJ. & Wang, S. Y. (1967) Ultraviolet irradiation of DNA in vitro and in vivo produces a third
thymine-derived product. Science, 156, 955-957
van't Veer, LJ., Burgering, B.M.T., Versteeg, R., Boot, AJ.M., Ruiter, DJ., Osanto, S., Schrier, P.I. &
Bos, J.L. (1989) N-ras Mutations in human cutaneous melanoma from sun-exposed body sites.
Mol. cell. Bioi., 9, 3114-3116
Verma, A.K., Lowe, N.J. & Boutwell, R.K (1979) Induction of mouse epidermal ornithine decarboxy-
lase activity and DNA synthesis by ultraviolet light. Cancer Res., 39, 1035-1040
Vermeer, M., Schmieder, GJ., Yoshikawa, T., van den Berg, J.-W., Metzman, M.S., Taylor, J.R. &
Streilein, J.W. (1991) Effects of ultraviolet Blight on cutaneous immune responses of humans
with deeply pigmented skin. J. invest. Dermato/. , 97, 729-734
Vitaliano, P.P. (1978) The use of logistic regression for modelling risk factors: with application to non-
melanoma skin cancer. Am. J. Epidemiol . 108, 402-414
Vitasa, B.C., Taylor, H.R., Strickland, P.T., Rosenthal, F.S . West, S., Abbey, H., Ng, S.K., Munoz, B. &
Emmett, E.A. (1990) Association of nonmelanoma skin cancer and actinic keratosis with
cumulative solar ultraviolet exposure in Maryland watermen. Cancer, 65, 2811-2817
REFERENCES 277
Vlcek, D., Podstavkova, S., Miadokova, E., Adams, G.M.W & Small, G.D. (1987) General charac-
teristics, molecular and genetic analysis of two new UV-sensitive mutants of Chlamydomonas
reinhardtii. Mutat. Res., 183, 169-175
Vogel, J., Cepeda, M., Tschachler, E., Napolitano, L.A. & Jay, G. (1992) UV activation of human
immunodeficiency virus gene expression in transgenic mice. J Viral., 66, 1-5
Vuillaume, M., Daya-Grosjean. L., Vincens, P., Pennetier, J.L., Tarroux, P., Baret. A., Calvayrac, R.,
Taieb, A. & Sarasin, A. (1992) Striking differences in cellular catalase activity between two DNA .
repair-deficient diseases: xeroderma pigmentosum and trichothiodystrophy. Carcinogenesis, 13,
321-328
Walker, G.C. (1984) Mutagenesis and inducible responses to deoxyribonucleic acid damage in
Escherichia coli. Microbiol. Rev., 48, 60-93
Walter, S.D., Marrett, L.D., From, L., Hertzman, C., Shannon, H.S. & Roy, P. (1990) The association of
cutaneous malignant melanoma with the use of sunbeds and sunlamps. Am. J. Epidemiol., 131,
232-243
Walter, S.D., Marrett, L.D., Shannon, H.S., From, L. & Hertzman, C. (1992) The association of cuta-
neous malignant melanoma and fluorescent light exposure. Am. J Epidemiol., 135, 749-762
Wang, S.-Y. & Varghese, A.J. (1967) Cytosine-thymine addition product from DNA irradiated with
ultraviolet light. Biochem. biophys. Res. Commun., 29, 543-549
Waterhouse, J., Muir, C., Correa, P. & Powell, J., eds (1976) Cancer Incidence in Five Continents, Vol.
III (IARC Scientific Publications No. 15), Lyon, IARC
Waterhouse, J., Muir, C., Shanmugaratnam, K. & Powell, J., eds (1982) Cancer Incidence in Five
Continents, Vol. IV (IARC Scientific Publications No. 42), Lyon, IARC
Weast, R.C., ed. (1989) CRC Handbook of Chemistry and Physics, 70th ed., Boca Raton, FL, CRC
Press, p. E-209
Webb, R.B. (1977) Lethal and mutagenic effects of near-ultraviolet radiation. Photochem. Photobiol.
Rev., 2, 169-261
Webb, R.B. & Malina, M.M. (1970) Mutagenic effects of near ultraviolet and visible radiant energy on
continuous cultures of Escherichia coli. Photochem. Photobiol., 12, 457-468
van Weelden, H. & van der Leun, J.C. (1986) Photorecovery by UVA. In: Urbach, F. & Gange, R.W,
eds, The Biological Effects of UVA Radiation, New York, Praeger, pp. 147-155
van Weelden, H., de Gruijl, F.R. & van der Leun, J.C. (1986) Carcinogenesis by UVA, with an attempt
to assess the carcinogenic risks of tanning with UVA and UVB. In: Urbach, F. & Gange, R.W,
eds, The Biological Effects of UVA Radiation, New York, Praeger, pp. 137-146
van Weelden, H., de Gruijl, F.R., van der Putte, S.C.J., Toonstra, J. & van der Leun, J.C. (1988) The
carcinogenic risks of modern tanning equipment: is UVA safer than UVB? Arch. dennatol. Res.,
280, 300-307
van Weelden, H., van der Putte, S.C.J., Toonstra, J. & van der Leun, J.C. (1990a) UVA-Induced
tumours in pigmented hairless mice and the carcinogenic risks of tanning with UVA. Arch.
dennatol. Res., 282, 289-294
van Weelden, H., van der Putte, S.C.J ., Thonstra, J. & van der Leun, J.C. (1990b) Ultraviolet B-induced
tumors in pigmented hairless mice, with an unsuccessful attempt to induce cutaneous mela-
noma. Photodennatol. Photoimmunol. Photomed., 1, 68-72
Weinstock, M.A., Colditz, G.A., Willett, W.C., Stampfer, MJ., Bronstein, B.R., Mihm, M.C., Jr &
Speizer, F.E. (1989) Nonfamilial cutaneous melanoma incidence in women associated with sun
exposure before 20 years of age. Pediatrics, 84, 199-204
278 !ARC MONOGRAPHS VOLUME 55
Weinstock. M.A., Colditz, G.A., Willett, W.C., Stampfer, MJ., Bronstein, B.R., Mihm, M.C., Jr &
Speizer, F.E. (1991a) Melanoma and the sun: the effect of swimsuits and a 'healthy' tan on the risk
of nonfamilial malignant melanoma in women. Am. J. Epidemio/., 134, 462-470
Weinstock. M.A, Stryker, W.S., Stampfer, MJ., Lew, R.A., Willett, WC. & Sober, AJ. (1991b)
Sunlight and dysplastic nevus risk. Results of a clinic-based case-control study. Cancer, 67,
1701-1706
Weiss, J., Garbe, C., Bertz, J., Biltz, H., Burg, G., Hennes, B., Jung, E.G., Kreysel, H.-W., Odanos,
C. E., Petzold, D., Schwermann, M., Stadler, R., Tilgen, W., Tronnier, H. & VOlkers, W (1990) Risk
factors for the development of malignant melanoma in Germany (Ger.). Hautartz, 41, 309-313
Wells, R.L. & Han, A (1984) Action spectra for killing and mutation of Chinese hamster cells exposed
to mid- and near-ultraviolet monochromatic light. Mutat. Res., 129, 251-258
Welsh, E.A. & Kripke, M.L. (1990) Murine Thy-1 + dendritic epidermal cells induce immunologic
tolerance in vivo. J. Jmmunol . 144, 883-891
West, S.K., Rosenthal, F.S., Bressler, N.M., Bressler, S.B., Munoz, B., Fine, S.L. & Taylor, H.R. (1989)
Exposure to sunlight and other risk factors for age-related macular degeneration. Arch.
ophthalmol., 107, 875- 879
Wheatcroft. R., Cox. B.S. & Haynes, R.H. (1975) Repair ofUV-induced damage and survival in yeast.
1. Dimer excision. Mutat. Res., 30, 209-218
Wheeler, C.E., Jr (1975) Pathogenesis of recurrent herpes simplex infections. J. invest. Dennatol., 65,
341-346
Whelan, S.L., Parkin, D.M. & Masuyer, E .. eds (1990) Patterns of Cancer in Five Continents (IARC
Scientific Publications No. 102), Lyon, IARC, p. 29
Whitaker, CJ., Lee, WR. & Downes, J.E. (1979) Squamous cell skin cancer in the north-west of
England, 1967-69, and its relation to occupation. Br. J. ind. Med., 36, 43-51
WHO (1977) Manual of the International Statistical Classification of Diseases, Jnjunes, and Causes of
Deatk International Classification of Diseases, 1975 rev., Vol. 1, Geneva, p. 102
WHO (1979) Ultraviolet Radiation (Environmental Health Criteria 14), Geneva
Willis, I., Menter, J.M. & Whyte, H.J. (1981) The rapid induction of cancers in the hairless mouse
utilizing the principle of photoaugmentation. J. invest. Dermatol., 16, 404-408
Willis, I., Menter, J.M .. de Fabo, E., Margolin, R. & Fisher, M. (1986) Photoaugmentation of UVB
effects by UVA. In: Urbach, F. & Gange, R.W., eds, The Biological Effects ofUVA Radiation, New
York. Praeger, pp. 187-201
Winkelmann, R.K., Baldes, E.J. & Zollman, P.E. (1960) Squamous cell tumors induced in hairless
mice with ultraviolet light. J. invest. Dermatol., 34, 131-138
Winkelmann, R.K., Zollman, P.E. & Baldes, EJ. (1963) Squamous cell carcinoma produced by
ultraviolet light in hairless mice. J. invest. Dermatol., 40, 217-224
Wiskemann, A, Sturm, E. & KJehr, N.W. (1986) Fluorescent lighting enhances chemically induced
papilloma formation and increases susceptibility to tumor challenge in mice. J. Cancer Res. din.
Oncol., 112, 141- 143
Withrow, T.J., Lugo, M.H. & Dempsey, M.J. (1980) Transformation of Balb 3T3 cells exposed to a
germicidal UV lamp and a sunlamp. Photochem Photobiol., 31, 135-141
Witkin, E.M. (1976) Ultraviolet mutagenesis and inducible DNA repair in Escherichia coli. Bacteriol.
Rev., 40, 869-907
Wittenberg, S. (1986) Solar radiation and the eye: a review of knowledge relevant to eye care. Am J.
Optom. physiol. Opt. , 63, 676-689
REFERENCES 279
Wolf, C., Steiner, A. & Honigsmann, H. (1988) Do oral carotenoids protect human skin against ultra-
violet erythema, psoralen phototoxicity, and ultraviolet-induced DNA damage? J. invest.
Dermatol., 90, 55-57
Wood, RD., Skopek, T.R. & Hutchinson, F. (1984) Changes in DNA base sequence induced by
targeted mutagenesis of lambda phage by ultraviolet light. J. mol. Bioi., 173, 273-291
Wulff, D.L. & Fraenkel, G. (1961) On the nature of thymine photoproduct. Biochim. biophys. Acta, Sl.
332-339
Yang, X.-Y., Ronai, Z.A., Santella, R.M. & Weinstein, I.B. (1988) Effect of 8-methoxypsoralen and
ultraviolet light A on EGF receptor (HER-1) expression. Biochem. biophys. Res. Commun., 157,
590-596
Yasumoto, S., Hayashi, Y. & Aurelian, L. (1987) Immunity to herpes simplex virus type 2. Suppression
of virus-induced immune responses in ultraviolet B-irradiated mice.J.lmmunol., 139,2788-2793
Yoshikawa, J., Rae, V., Bruins-Slot, W., Van den Berg, J.-W., Taylor, J.R. & StreiJein, J.W. (1990)
Susceptibility to effects of UVB radiation on induction of contact hypersensitivity as a risk factor
for skin cancer in humans. J. invest. Dermatol., 95, 530-536
Young, R.W. (1988) Solar radiation and age-related macular degeneration. Surv. Ophthalmo/., 32,252-
269
Young, M. & Russell, W.T. (1926)An Investigation into the Statistics of Cancer in Different Trades and
Professions (Medical Research Council Special Report No. 99), London, Her Majesty's
Stationery Office
Young, A.R., Walker, S.L., Kinley, J .S., Plastow, S.R.. Averbeck, D., Morliere, P. & Dubertret, L. (1990)
Phototumorigenesis studies of 5-methoxypsoralen in bergamot oil: evaluation and modification
of risk of human use in an albino mouse skin model. J. Photochem. PhotobioL B. Bioi., 7, 231-250
Zanetti, R., Rosso, S., Faggiano, F., Roffino, R., Colonna, S. & Martina, G. (1988) A case--<:Ontrol study
on cutaneous malignant melanoma in the province of Torino, Italy (Fr.). Rev. Epidemiol. Sante
pub/., 36, 309-317
Zelle, B., Reynolds, R.J .. Kottenhagen, M.J ., Schuite, A. & Lohman, P.H.M. (1980) The influence of the
wavelength of ultraviolet radiation on survival, mutation induction and DNA repair in irradiated
Chinese hamster cells. Mutat. Res., 12, 491-509
Zigman, S. & Vaughan, T. (1974) Near-ultraviolet light effects on the lenses and retinas of mice. Invest.
Ophthalmol . 13, 462-465
Zigman, S., Yulo, T. & Schultz. 1. (1974) Cataract induction in mice exposed to near UV light. Ophthai.
Res., 6, 259-270
Zigman, S., Fowler, E. & Kraus, A.L. (1976) Black light induction of skin tumors in mice. J. invest.
Dermatol., 67, 723-725
Zmudzka, B.Z. & Beer, J.Z. (1990) Activation of human immunodeficiency virus by ultraviolet radia-
tion. Photochem. Photobiol., 52, 1153-1162
ZOizer, F. & Kiefer, J. (1983) Wavelength dependence of inactivation and mutagenesis in haploid yeast
cells of different sensitivities. Photochem. Photobiol., 37, 39-48
ZOlzer, F. & Kiefer, J. (1984) Wavelength dependence of inactivation and mutation induction to
6-thioguanine-resistance in V79 Chinese hamster fibroblasts. Photochem. Photobiol., 40, 49-53
ZOlzer, F., Kiefer, J. & Rase, S. (1988) Inactivation and mutation induction to 6-thioguanine resistance
in V79 hamster fibroblasts by simulated sunlight. Photochem. Photobiol., 47, 399-404
SUMMARY OF FINAL EVALUATIONS
Agent
Solar radiation
Broad-spectrum ultraviolet radiation
Ultraviolet A radiation
Ultraviolet B radiation
Ultraviolet C radiation
Fluorescent lighting
Sunlamps and sunbeds, use of
Degree of evidence
of carcinogenicity
Human Animal
s s
s
s
s
s
I
L
Overall evaluation
of carcinogenicity
to humans
1
2A
2A
2A
3
2A
S, sufficient evidence; L, limited evidence; I, inadequate evidence; for definitions of degrees
of evidence and groupings of evaluations, see Preamble, pp. 32-35.
-281-
GLOSSARY OF TERMS
Actinic radiation: electromagnetic radiation capable of initiating photochemical reactions;
UVB and UVC radiation (180-315 nm)
Albedo: that fraction of the radiation incident on a surface which is reflected back in all
directions
Black light: primarily near-UV radiant energy in the 320-380 nm (or 400 nm) range
Effective irradiance: hypothetical irradiance of monochromatic radiation with a wavelength
at which the action spectrum of the relevant photobiological effect is equal to unity (see
also section 1.1)
Effective exposure dose: time integral of effective irradiance
Erythema: sunburn
Exposure dose: radiant exposure (J/m
2
unweighted) incident on biologically relevant surface
Fluence: radiant flux passing from all directions through a unit area in J/m
2
or J/cm
2
; includes
backscatter
Global irradiance: the irradiance of solar radiation at the Earth's surface
Global radiation: solar radiation at the Earth's surface comprising the sum of direct radiation
from the sun and diffuse radiation from the sky
Minimal erythema dose (MED): the lowest radiant exposure of UVR that produces a
threshold erythemal response 8-24 h after irradiation. There is no consensus on this
response; a just perceptible reddening of the skin and erythema with sharp margins are
both used as end-points.
Photoreactivation: the enzyme-mediated reversal of the biological effects of UVC or UVB
radiation mediated by radiation of longer wavelength and associated with the reversion
of cyclobutane-type pyrimidine dimers to monomeric pyrimidines
Radiant exposure: radiant energy delivered to a given area (J/m
2
)
Radiant flux: rate of flow of radiant energy (in W)
Solar simulated radiation: radiation from an artificial source (e.g., an optically filtered xenon
arc lamp) that approximates the terrestrial solar spectrum
Solar zenith angle: angle between the point in the sky directly overhead (the zenith) and the
sun
Spectral distribution: relative intensity of radiation of different wavelengths present in a
source emission spectrum
Spectral irradiance: surface density of the radiant flux that is incident on a unit surface area
per unit wavelength (see Thble 1)
UVA: electromagnetic radiation of wavelength 315-400 nm
-283-
284
IARC MONOGRAPHS VOLUME 55
UVB: electromagnetic radiation of wavelength 280-315 nm
UVC: electromagnetic radiation of wavelength 100-280 nm
UVR: electromagnetic radiation of wavelength 100-400 nm
Zenith angle: the angle between the point in the sky directly overhead (the zenith) and
another point or object
APPENDIX 1. TOPICAL SUNSCREENS
1. General
Sunscreens are physical and chemical topical preparations which attenuate the trans-
mission of solar radiation into the skin by absorption, reflection or scattering. Physical sun-
screens (sunblocks), for example zinc oxide or titanium dioxide, function by reflecting and
scattering and provide protection against a broad spectrum of UV and visible wavelengths.
They are normally nontoxic and have few known adverse effects. Chemical sunscreens
contain one or more colourless UV-absorbing ingredients which generally absorb UVB
radiation more strongly than UV A. The application of any sunscreen thus normally changes
the spectrum of radiation that reaches the target cells. General information is available on
sunscreens that have been or are in use (Liem & Hilderink, 1979; Boger eta/. , 1984; Murphy
& Hawk, 1986; Pathak, 1986, 1987; Ramsay, 1989; Lowe & Shaath, 1990; Thylor et al., 1990)
and on procedures for testing them (Azizi eta/. , 1987; Kaidbey & Gange, 1987; Urbach,
1989).
Although most sunscreens are designed to attenuate UVR, some contain additives such
as bergamot oil (containing 5-methoxypsoralen; see IARC, 1986, 1987) to enhance pigmen-
tation and photoprotection (Young et a/. , 1991). The role of such preparations remains
controversial.
The generally accepted parameter for evaluating the efficacy of sunscreen preparations
is the sun protection factor (SPF), which is defined as the ratio of the least amount of UVR
required to produce minimal erythema after application of a standard quantity of the sun-
screen product film to the skin to that required to produce the same erythema without sun-
screen application. The US Food and Drug Administration (1978) published recommen-
dations for the testing of proprietary sunscreens. Many factors influence SPF values; particu-
larly important are the spectral power distribution of the source used for SPF testing and a
clear definition of the end-point used for assessment (see Urbach, 1989). Variations in these
factors can lead to considerable differences in measured SPF values for the same product . .
SPF values generally reflect the degree of protection against solar UVB radiation, but
their protective capacity against UVA must also be defined. Several in-vivo and in-vitro
methods have been proposed for defining protection against UV A, but there is no consensus
on which is the most appropriate.
Correctly used, sunscreens are effective in preventing erythema. Little information is
available, however, on their protective value against harmful immunological changes, photo-
ageing or skin cancer or on their potential long-term adverse effects. The protective and
adverse effects of sunscreen use are summarized below.
-285-
286 IARC MONOGRAPHS VOLUME 55
2. Protective effects
2.1 Against DNA damage
UVR inhibits normal (semi-conservative) DNA synthesis. Knowledge about the preven-
tion of DNA damage is based on the results of studies of a small number of sunscreens. In a
limited in-vitro study, two commercially available sunscreens (Spectraban, SPF 15.0 and
Spectraban, SPF 5.6 [components unspecified]) were tested for their ability to protect
against the inhibition of semi-conservative DNA synthesis or the induction of unscheduled
DNA synthesis by UVB (300 nm) radiation (Arase & Jung, 1986). Protective factors were
found to correlate with the stated SPF values of the sunscreens.
The ability of sunscreens to protect against UV-induced inhibition of DNA synthesis has
also been tested in epidermal mouse skin. In a study of seven commercially available sun-
screens [components unspecified], the calculated protection factors corresponded fairly well
with the SPF values provided by the manufacturers (Walter, 1981). In a study of a single
sunscreen (7.5% octyl methoxycinnamate, 4.5% benzophenone-3; SPF, 15), the induction of
pyrimidine dimers in human skin in situ by a solar simulator (280- 400 nm) was measured as a
function of fluence (up to 10 times the MED), with or without application of the sunscreen.
Dimer induction was reduced by 40-fold in sunscreen-treated skin {Freeman eta/., 1988).
2.2 Against acute and chronic actinic damage
Protection against erythema is well substantiated by extensive human experience; how-
ever, other cellular and metabolic activities may not be afforded the same degree of pro-
tection (Pearse & Marks, 1983). In a histological assessment of mouse skin damage. Kligman
eta/. (1982) found that sunscreens provided protection against the effects of sunlamp
irradiation. Furthermore, the application of sunscreens (SPF 6 or 15) allowed previously
damaged dermis to be repaired despite continued irradiation (Kligman eta/., 1983). A UVB
sunscreen (2-ethylhexyl 4'-methoxycinnamate, SPF 8) was shown to protect against bio-
chemical changes induced in collagen by Westinghouse FS20 sunlamp irradiation of mouse
skin over 12 weeks (Plastow et a/., 1988).
2.3 Against immunological alterations
Various investigators have examined the efficacy of sunscreens to inhibit photoimmuno-
logica) reactions in the skin. Inhibition of the development of UV-induced suppression of
contact hypersensitivity has been reported (Morison, 1984 ), but in other studies sunscreens
have been ineffective in preventing immunosuppression (Gurish et al., 1981; Hersey et al.,
1987; Fisher eta/., 1989; van Praag eta/., 1991), or mixed results have been obtained depen-
ding on the sunscreen used (Reeve et al. , 1991). [The Working Group concluded that no
consistent relationship could be assumed between protection against photoimmunological
events and erythema other changes in the skin.]
2.4 Against tumour formation
Some sunscreens have been shown to protect mice against UV-induced skin tumour
formation (Knoxet a/., 1960; Kligman eta/., 1980; Wulf eta/., 1982; Gallagher et al., 1984;
Morison, 1984). Demonstration of effectiveness against skin tumour formation is, however,
APPENDIX 1 2137
not required by regulatory bodies in evaluations of sunscreens. Sunscreen use may encourage
people to have longer overall exposure to sunlight. because protection by the sunscreen
reduces the effective irradiance. Kelfkens eta/. (1991) observed that exposure of mice to a
daily dose of UVB over a longer period gives a higher tumour yield than the same dose given
over a shorter period. Accordingly, any assessment of the overall impact of sunscreens in
reducing human skin cancer should take into account both the efficacy of sunscreens in
reducing UV-induced damage to the skin and concomitant human behavioural changes with
respect to time spent in the sun. In some case-control studies (e.g., Holman eta/. , 1986;
Beitner et al., 1990), use of sunscreens has been associated with an increased risk for mela-
noma. This association is probably the result of confounding of sun exposure by skin type or
amount of exposure, because individuals who easily get sunburned or expose themselves
heavily (and who are at increased risk of skin cancer) may use sunscreens more frequently
than other people.
3. Adverse effects
3.1 Acute toxicity
Acute toxic side-effects of specific sunscreen agents include contact irritation, allergic
contact dermatitis, phototoxicity. photoallergy and staining of the skin (Schauder & Ippen,
1986; Pathak, 1987; Knobler et a/., 1989).
3.2 Chronic toxicity
Relatively little information is available on the mutagenic and carcinogenic potential of
sunscreen agents. This deficiency was reviewed in a report by the US National Cancer Insti-
tute (1989), which recommended the following six compounds for chronic testing in the US
National Toxicology Program rodent test programme: cinoxate, 2-ethylhexyl 2-cyano-3,3-
diphenyl-acrylate, 2-ethylhexyl para-methoxycinnamate, homosalate, methyl anthranilate
and oxybenzone. The bases for selecting these compounds, together with extensive refe-
rences. are given in the report. In short. neither epidemiological data nor long-term mamma-
lian carcinogenicity studies are available on these compounds. The results of in-vitro testing
were assessed as either negative or inconsistent among test systems or among batches of a
compound (because of impurities). 2-Ethylhexyl para-methoxycinnamate was implicated as a
potential tumour initiator in one study in which hairless mice were painted with the
compound over a nine-week period and subsequently treated with the tumour promoter,
croton oil (Gallagher ei al., 1984 ). Subsequent work by Reeve eta/. (1985), however, failed to
confirm these results, and Forbes eta/. (1989) found no evidence of tumour initiation by the
compound in an initiation-promotion experiment in mice.
trans-Urocanic acid (an additive in some commercial sunscreen products) increased the
yield of simulated solar UV-induced tumours in hairless mice (Reeve et al., 1989). The signi-
ficance of this finding for human exposure has not been evaluated.
3.3 Reduced vitamin D synthesis
Vitamin D production is almost completely blocked in subjects who use UVB sunscreens
(Matsuoka et a/., 1987). This finding may be significant for elderly individuals, who are
288 IARC MONOGRAPHS VOLUME 55
already at risk for vitamin D3 deficiency (MacLaughlin & Holick, 1985), but its significance
for clinical disease remains unknown (Fine, 1988).
4. References
Arase, S. & Jung, E.G. (1986) In vitro evaluation ofthe photoprotective efficacy of sunscreens against
DNA damage by UVB. Photodermatology, 3, 56-59
Azizi, E., Modan, M., Kushelevsky, A.P. & Schewach-Millet, M. (1987) A more reliable index of
sunscreen protection, based on life table analysis of individual sun protection factors. Br. J.
Dermatol., 116, 693-702
Beitner, H., Norell, S.E., Ringborg, U., Wennersten, G. & Mattson, B. (1990) Malignant melanoma:
aetiological importance of individual pigmentation and sun exposure. Br. J. Dermatol., 122,43-51
Boger, J., Araujo, O.E. & Flowers, F. (1984) Sunscreens: efficacy, use and misuse. South. med. J., 77,
1421-1427
Fine, R.M. (1988) Sunscreens and cutaneous vitamin D synthesis. Int. J. Dermato/., 21; 300-301
Fisher, M.S., Menter, J.M. & Willis, I. (1989) Ultraviolet radiation-induced suppression of contact
hypersensitivity in relation to Padimate 0 and oxybenzone. J. invest. Dermatol., 92, 337-341
Forbes, P.O., Davies, R.E., Sambuco, C.P. & Urbach, F. (1989) Inhibition of ultraviolet radiation-
induced skin tumors in hairless mice by topical application of the sunscreen 2-ethylhexyl-p-
methoxycinnamate. J. Toxicol. cutaneous ocul. Toxicol. , 8, 209-226
Freeman, S.E., Ley, RD. & Ley, K.D. (1988) Sunscreen protection against UV-induced pyrimidine
dimers in DNA of human skin in situ. Photodermatology, 5, 243- 247
Gallagher, C.H . Greenoak, G.E., Reeve, Y.E., Canfield, PJ., Baker, R.S.U. & Bonin, A.M. (1984)
Ultraviolet carcinogenesis in the hairless mouse skin-influence of the sunscreen 2-ethylhexyl-p-
methoxycinnamate. Aust. 1 e.xp. Bioi. med. Sci., 62, 577- 588
Gurish, M.F., Roberts, L.K., Krueger, G.G. & Daynes, R.A. (1981) The effect of various sunscreen
agents on skin damage and the induction of tumor susceptibility in mice subjected to ultraviolet
irradiation. J. invest. Dermatol., 16, 246-251
Hersey, P., MacDonald, M., Burns, C., Schibeci, S., Matthews, H. & Wilkinson. FJ. (1987) Analysis of
the effect of a sunscreen agent on the suppression of natural killer cell activity induced in human
subjects by radiation from solarium lamps. J. invest. Dermato/., 88, 271-276
Holman, C.D.J., Armstrong, B.K. & Heenan, P.J. (1986) Relationship of cutaneous malignant mela-
noma to individual sunlight-exposure habits.l nat/ Cancer Inst., 76, 403-414
IARC (1986) /ARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans,
. Vol. 40, Some Natura/Jy Occurring and Synthetic Food Components, Furocoumarins and Ultra-
violet Radiation, Lyon, pp. 327-347
IARC (1987) /ARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Suppl. 7, Overall
Evaluations of Carcinogenicity: An Updating of IARC Monographs Volumes 1 to 42, Lyon, pp.
243-245
Kaidbey, K. & Gange, R. W. (1987) Comparison of methods for assessing photoprotection against
ultraviolet A in vivo.l Am. Acad. Dermatol., 16, 346-353
Kelfkens, G., van Weelden, H., de Gruijl, F.R. & van der Leun, J .C. (1991) The influence of dose rate on
ultraviolet tumorigenesis. J. Photochem. Photobiol. B. Bioi., 10, 41-50
Kligman, L.H., Akin, FJ. & Kligman, A.M. (1980) Sunscreens prevent ultraviolet photocarcino-
genesis. J. Am. Acad. Dermatol., 3, 30-35
Kligman, L.H., Akin, F J . & Kligman, A.M. (1982) Prevention of ultraviolet damage to the dermis of
hairless mice by sunscreens. J. invest. Dermatol., 78, 181-189
APPENDIX 1 289
Kligman, L.H., Akin, F.J. & Kligman, A.M. (1983) Sunscreens promote repair of ultraviolet radiation-
induced dermal damage. J invest. Dermatol., 81, 98-102
Knobler, E., Almeida, L., Ruzkowski, A.M., Held, J., Harber, L. & DeLeo, V. (1989) Photoallergy to
benzophenone. Arch. Dermatol., 125, 801-804
Knox, J.M., Griffin, A.C. & Hakim, R.E. (1960) Protection from ultraviolet carcinogenesis. J invest.
Dermatol., 34, 51-58
Liem, D.H. & Hilderink, L.T.H. (1979) UV absorbers in sun cosmetics 1978. Int. J. cosmet. Sci., l,
341-361
Lowe, NJ. & Shaath, N.A., eds (1990) Sunscreens. Development, Evaluation and Regulatory Aspects,
New York, Marcel Dekker
MacLaughlin, J.A. & Holick, M.F. (1985) Aging decreases the capacity of human skin to produce
vitamin D3. J clin. Invest., 76, 5 3 ~ 5 3 8
Matsuoka, L.Y., Ide, L., Wortsman J., McLaughlin, J.A. & Holick, M.P. (1987) Sunscreens suppress
cutaneous vitamin D3 synthesis. J clin. Endocrinol. Metab., 64, 1165-1168
Morison, W.L. (1984) The effect of a sunscreen containing para-aminobenzoic acid on the systemic
immunologic alterations induced in mice by exposure to UVB radiation. J invest. Dennatol., 83,
405-408
Murphy, G.M. & Hawk, J.L.M. (1986) Sunscreens. JR. Soc. Med., 79, 254-256
Pathak, M.A. (1986) Sunscreens. Topical and systemic approaches for the prevention of acute and
chronic sun-induced skin reactions. Dermatol. Clin., 4, 321- 334
Pathak, M.A (1987) Sunscreens and their use in the preventive treatment of sunlight-induced skin
damage. J Dermatol. surg. Oncol., 13, 739-750
Pearse, A.D. & Marks, R. (1983) Response of human skin to ultraviolet radiation: dissociation of
erythema and metabolic changes following sunscreen protection. J. invest. Dermato/., 80, 191-194
Plastow, S.R., Harrison, J.A. & Young, A.R. (1988) Early changes in dermal collagen of mice exposed
to chronic UVB irradiation and the effects of a UVB sunscreen. J invest. Dermatol., 91, 590-592
van Praag, M.C.G., Out-Luyting, C., Claas, F.H.J., Vermeer, B.-J. & Mommaas, A.M. (1991) Effect of
topical sunscreens on the UV-radiation-induced suppression of the alloactivating capacity in
human skin in vivo. J invest. Dennatol., 91, 629-633
Ramsay, C.A. (1989) Ultraviolet A protective sunscreens. C/in. Dermato/., 1, 163-166
Reeve, V.E., Greenoak, G.E., Gallagher, C.H., Canfield, P.J. & Wilkinson, FJ. (1985) Effect of
immunosuppressive agents and sunscreens on UV carcinogenesis in the hairless mouse.Aust. J
exp. Bioi. med. Sci., 63, 655--&>5
Reeve, V.E., Greenoak, G.E., Canfield, PJ., Boehm-Wilcox, C. & Gallagher, C.H. (1989) Topical uro-
canic acid enhances UV-induced tumour yield and malignancy in the hairless mouse. Photo-
chem Photobiol., 49, 459-464
Reeve, V.E., Bosnic, M., Boehm-Wilcox, C. & Ley, R.D. (1991) Differential protection by two sun-
screens from UV radiation-induced immunosuppression. J invest. Dennatol., 97, 624-628
Schauder, S. & Ippen, H. (1986) Photoallergic and allergic contact dermatitis from dibenzoyl-
methanes. Photodennatology, 3, 140-147
Thylor, C.R., Stern, R.S., Leyden, JJ. & Gilchrest, B.A. (1990) Photoaging/photodamage and photo-
protection. I Am. Acad. Dermatol., 22, 1-15
Urbach, F. (1989) Testing the efficacy of sunscreens: effect of choice of source and spectral power
distribution of ultraviolet radiation, and choice of endpoint. Photodennato/ogy, 6, 1n-181
US Food and Drug Administration (1978) Sunscreen drug products for over-the-counter human use.
Establishment of a monograph; notice of proposed rulemaking. Fed. Regist., 43, 38206-38269
290
IARC MONOGRAPHS VOLUME 55
US National Cancer Institute (1989) Sunscreens (Class Study Report; Contract No. N01-CP-71082
(7/89)), Rockville. MD, ll"acor Technological Resources Inc.
Walter, J.F. (1981) Evaluation of seven sunscreens on hairless mouse skin. Arch. Dennatol., 117,
547-550
Wulf, H.C., Poulsen, T., Brodthagen, H. & Hou-Jensen, K. (1982) Sunscreens for delay of ultraviolet
induction of skin tumors. J. Am. Acad. Dermatol., 1, 194-202
Young, A.R., Potten, C.S., Chadwick, C.A., Murphy, G.M., Hawk, J .L.M. & Cohen, AJ. (1991) Photo-
protection and 5-MOP photochemoprotection from UVR-induced DNA damage in humans: the
role of skin type. J. invest. Dennatol., 91, 942-948
CUMULATIVE CROSS INDEX TO /ARC MONOGRAPHS ON
THE EVALUATION OF CARCINOGENIC RISKS TO HUMANS
The volume, page and year are given. References to corrigenda are given in parentheses.
A
AatC
Acetaldehyde
Acetaldehyde formylmethylhydrazone (see Gyromitrin)
Acetamide
Acetaminophen (see Paracetamol)
Acridine orange
Acriflavinium chloride
Acrolein
Acrylamide
Acrylic acid
Acrylic fibres
Acrylonitrile
Acrylonitrile-butadiene-styrene copolymers
Actinolite (see Asbestos)
Actinomycins
Adriamycin
AF-2
Aflatoxins
Aflatoxin B1 (see Aflatoxins)
Aflatoxin B2 (see Aflatoxins)
Aflatoxin Gt (see Aflatoxins)
Aflatoxin G2 (see Aflatoxins)
Aflatoxin M 1 (see Aflatoxins)
Agaritine
Alcohol drinking
Aldicarb
Aldrin
Allyl chloride
Allyl isothiocyanate
Allyl isovalerate
Aluminium production
Amaranth
5-Aminoacenaphthene
- 291-
40, 245 (1986); Suppl 7, 56 (1987)
36, 101 (1985) (con: 42, 263);
SuppL ~ 77(1987)
7, 197 (1974); Suppl. 7, 389 (1987)
16, 145 (1978); Suppl. 7, 56 (1987)
13, 31 (1977); Suppl. 7, 56 (1987)
19, 479 (1979); 36,133 (1985);
Suppl. 7, 78 (1987)
39, 41 (1986); Suppl. 7, 56 (1987)
19, 47 (1979); Suppl. 7, 56 (1987)
19, 86 (1979); Suppl. 7, 56 (1987)
19, 73 (1979); Suppl. 7, 79 (1987)
19, 91 (1979); Suppl. 7, 56 (1987)
10, 29 (1976) (con: 42, 255);
Suppl. 7, 80 (1987)
10, 43 1 9 7 6 ~ Suppl. 7, 82 (1987)
31, 47 (1983); Suppl. 7, 56 (1987)
1, 145 (1972) (con: 42, 251);
10, 51 (1976); Suppl. 7, 83 (1987)
31, 63 (1983); Suppl. 7, 56 (1987)
44 (1988)
53, 93 (1991)
5, 25 (1974); Supp/. 7, 88 (1987)
36, 39 (1985); Supp/. 7, 56 (1987)
36, 55 (1985); Supp/. 7, 56 (1987)
36, 69 (1985); Supp/. 7, 56 (1987)
34, 37 (1984); Suppl. 7, 89 (1987)
8, 41 (1975); Supp/. 7, 56 (1987)
16, 243 (1978); Supp/. 7, 56 (1987)
292
IARC MONOGRAPHS VOLUME 55
2-Aminoanthraquinone
para-Auninoazobenzene
ortho-Aminoazotoluene
para-Aminobenzoic acid
4-Aminobiphenyl
2-Amino-3,4-dimethylimidazo[4,5-Jlquinoline (see MeiQ)
2-Amino-3,8-dimethylimidazo[4,5-Jlquinoxaline (see MeiQx)
3-Amino-1,4-dimethyl-5H-pyrido[ 4,3-b] indole (see Trp-P-1)
2-Aminodipyrido( 1,2-a:3' ,2' -d]imidazo1e (see Glu-P-2)
1-Amino-2-methylanthraquinone
2-Amino-3-methylimidazo[ 4,5-Jlquinoline (see IQ)
2-Amino-6-methyldipyrido(1,2-a:3',2' -d]imidazole (see Glu-P-1)
2-Amino-3-methyl-9H-pyrido(2,3-b ]indole (see M e A - ~ - C
3-Amino-1-methyi-5H-pyrido(4,3-b ]indole (see Trp-P-2)
2-Amino-5-( 5-nitro-2-furyl)-1,3,4-thiadiazole
4-Amino-2-nitrophenol
2-Amino-5-nitrothiazole
2-Amino-9H-pyrido[2,3-b ]indole (see A - ~ - C
11-Aminoundecanoic acid
Amitrole
27, 191 (1982); Suppl. 7, 56 (1987)
8, 53 (1975); Suppl. 7, 390 (1987)
8. 61 (1975) (CO"- 42, 254);
Suppl. 7, 56 (1987)
16, 249 (1978); Suppl. 7, 56 (1987)
1, 74 (1972) (con: 42, 251);
Suppl. 7, 91 (1987)
27, 199 (1982); Suppl. 7, 57 (1987)
7, 143 (1974); Suppl. 7, 57 (1987)
16, 43 (1978); Suppl. 7, 57 (1987)
31, 71 (1983); Suppl. 7, 57 (1987)
39, 239 ( 1986); Suppl. 7, 57 (1987)
7, 31 (1974); 41, 293 (1986) (con:
52, 513; Suppl. 7, 92 (1987)
Ammonium potassium selenide (see Selenium and selenium compounds)
Amorphous silica (see also Silica) 42, 39 (1987); Suppl. 7, 341 (1987)
Amosite (see Asbestos)
Ampicillin
Anabolic steroids (see Androgenic (anabolic) steroids)
Anaesthetics, volatile
Analgesic mixtures containing phenacetin (see also Phenacetin)
Androgenic (anabolic) steroids
Angelicin and some synthetic derivatives (see also Angelicins)
Angelicin plus ultraviolet radiation (see also Angelicin and some
synthetic derivatives)
Angelicins
Aniline
ortho-Anisidine
para-Anisidine
Anthanthrene
Anthophyllite (see Asbestos)
Anthracene
Anthranilic acid
Antimony trioxide
Antimony trisu1fide
ANTU (see 1-Naphthylthiourea)
Apholate
Aramite
Areca nut (see Betel quid)
Arsanilic acid (see Arsenic and arsenic compounds)
Arsenic and arsenic compounds
50, 153 (1990)
11, 285 (1976); Suppl. 7, 93 (1987)
Suppl. 7, 310 (1987)
Suppl. 7, 96 (1987)
40, 291 (1986)
Suppl. 7, 57 (1987)
Suppl. 7, 57 (1987)
4, 27 (1974) (con: 42, 252);
27, 39 (1982): Suppl. 7, 99 (1987)
27, 63 (1982); Suppl. 7, 57 (1987)
27, 65 (1982); Suppl. 7, 57 (1987)
32, 95 (1983); Suppl. 7, 57 (1987)
32, 105 (1983); Suppl. 7, 57 (1987)
16, 265 (1978); Suppl. 7, 57 (1987)
47, 291 (1989)
47, 291 (1989)
9, 31 (1975); Suppl. 7, 57 (1987)
5, 39 (1974); Suppl. 7, 57 (1987)
1' 41 (1972); 2, 48 (1973);
23, 39 (1980); Suppl. 7, 100 (1987)
CUMULATIVE CROSS INDEX
293
Arsenic pentoxide (see Arsenic and arsenic compounds)
Arsenic sulfide (see Arsenic and arsenic compounds)
Arsenic trioxide (see Arsenic and arsenic compounds)
Arsine (see Arsenic and arsenic compounds)
Asbestos
Atrazine
Attapulgite
Auramine (technical-grade)
Auramine, manufacture of (see also Auramine, technical-grade)
Aurothioglucose
Azacitidine
5-Azacytidine (see Azacitidine)
Azaserine
Azathioprine
Aziridine
2-(1-Aziridinyl)ethanol
Aziridyl benzoquinone
Azobenzene
B
Barium chromate (see Chromium and chromium compounds)
Basic chromic sulfate (see Chromium and chromium compounds)
BCNU (see Bischloroethyl nitrosourea)
Benz[ a )acridine
Benz[c ]acridine
Benzal chloride (see also a:-Chlorinated toluenes)
Benz[ a ]anthracene
Benzene
Benzidine
Benzidine-based dyes
Benzo(b ]fluoranthene
Benzo[J ]fluoranthene
Benzo[k)fluoranthene
Benzo[ghi]fluoranthene
Benzo[a ]fluorene
Benzo[b ]fluorene
Benzo[c]fluorene
Benzo[ghi]perylene
Benzo[ c ]phenanthrene
2, 17 (1973) (CO"- 42, 252);
14 (1977) (con: 42, 256); Suppl. 7,
106 (1987) (con: 45, 283)
53, 441 (1991)
42, 159 (1987); Suppl. 7, 117 (1987)
1, 69 (1972) (co"- 42, 251); Suppl. 7,
118 (1987)
Suppl. 7, 118 (1987)
13, 39 (1977); Suppl. 7, 57 (1987)
26, 37 (1981); Suppl. 7, 57 (1987);
50, 47 (1990)
JO, 73 (1976) (CO"- 42, 255);
Suppl. 7, 57 (1987)
26, 47 (1981); Suppl. 7, 119 (1987)
9, 37 (1975); Suppl. 7, 58 (1987)
9, 47 (1975); Suppl. 7, 58 (1987)
9, 51 (1975); Suppl. 7, 58 (1987)
8, 75 (1975); Suppl. 7, 58 (1987)
32, 123 (1983); Suppl. 7, 58 (1987)
3, 241 (1973); 32, 129 (1983);
Suppl. 58(1987)
29, 65 (1982); Suppl. 7, 148 (1987)
3, 45 (1973); 32, 135 (1983);
Suppl. 7, 58 (1987)
7, 203 (1974) (CO"- 42, 254); 29, 93,
391 (1982); Suppl. 7, 120 (1987)
I, 80 (1972); 29, 149, 391 (1982);
Suppl. 7, 123 (1987)
Suppl. 7, 125 (1987)
3, 69 (1973); 32, 147 (1983);
Suppl. 7, 58 (1987)
3, 82 (1973); 32, 155 (1983); Suppl. 7,
58 (1987)
32, 163 (1983); Suppl. 7, 58 (1987)
32, 171 (1983); Suppl. 7, 58 (1987)
32, 177 (1983); Suppl. 7, 58 (1987)
32, 183 (1983); Suppl. 7, 58 (1987)
32, 189 (1983); Suppl. 7, 58 (1987)
32, 195 (1983); Suppl. 7, 58 (1987)
32, 205 (1983); Suppl. 7, 58 (1987)
294
IARC MONOGRAPHS VOLUME 55
Benzo[a ]pyrene
B cnzo[ e )pyrene
para-Benzoquinone dioxime
Benzotrichloride (see also a -Chlorinated toluenes)
Benzoyl chloride
Benzoyl peroxide
Benzyl acetate
Benzyl chloride (see also a-Chlorinated toluenes)
Benzyl violet 48
Bertrandite (see Beryllium and beryllium compounds)
Beryllium and beryllium compounds
Beryllium acetate (see Beryllium and beryllium compounds)
Beryllium acetate, basic (see Beryllium and beryllium compounds)
Beryllium-aluminium alloy (see Beryllium and beryllium compounds)
Beryllium carbonate (see Beryllium and beryllium compounds)
Beryllium chloride (see Beryllium and beryllium compounds)
Beryllium-copper alloy (see Beryllium and beryllium compounds)
Beryllium-copper-cobalt alloy (see Beryllium and beryllium compounds)
Beryllium fluoride (see Beryllium and beryllium compounds)
Beryllium hydroxide (see Beryllium and beryllium compounds)
Beryllium-nickel alloy (see Beryllium and beryllium compounds)
Beryllium oxide (see Beryllium and beryllium compounds)
Beryllium phosphate (see Beryllium and beryllium compounds)
Beryllium silicate (see Beryllium and beryllium compounds)
Beryllium sulfate (see Beryllium and beryllium compounds)
Beryl ore (see Beryllium and beryllium compounds)
Betel quid
Betel-quid chewing (see Betel quid)
BHA (see Butylated hydroxyanisole)
BHT (see Butylated hydroxytoluene)
Bis(1-aziridinyl)morpholinophosphine sulfide
Bis(2-chloroethyl)ether
N.N-Bis(2-chloroethyl}-2-naphthylamine
Bischloroethyl nitrosourea (see also Chloroethyl nitrosoureas)
1,2-Bis(chloromethoxy)ethane
1, 4-Bis( chloromethoxymethyl )benzene
Bis( chloromethyl)ether
Bis(2-chloro-l-methylethyl )ether
B is(2,3-epoxycyclopent}'l )ether
3, 91 (1973); 32, 211 (1983);
Suppl. 7, 58 (1987)
3, 137 (1973); 32, 225 (1983);
Suppl. 7, 58 (1987)
29, 185 (1982); Suppl. 7, 58 (1987)
29, 73 (1982); Suppl. 7, 148 (1987)
29, 83 (1982) (corr. 42, 261); Suppl. 7,
126 (1987)
36, 267 (1985); Suppl. 7, 58 (1987)
40, 109 (1986); Suppl. 7, 58 (1987)
11, 217 (1976) (corr. 42, 256); 29,
49 (1982); Suppl. 7, 148 (1987)
16, 153 ( 1978); Suppl. 7, 58 (1987)
1, l7 (1972); 23, 143 (1980) (corr. 42,
260); Supp/. 7, 127 (1987)
37, 141 (1985); Suppl. 7, 128 (1987)
9, 55 (1975); Suppl. 7, 58 (1987)
9, 117 (1975); Suppl. 7, 58 (1987)
4, 119 (1974) (corr. 42, 253);
Suppl. 7, 130 (1987)
26, 79 (1981); Suppl. 7, 150 (1987)
15, 31 (1977); Suppl. 7, 58 (1987)
15, 37 (1977); Suppl. 7, 58 (1987)
4, 231 (1974) (corr. 42, 253);
Suppl. 7, 131 (1987)
41, 149 (1986); Suppl. 7, 59 (1987)
47, 231 (1989)
Bisphenol A diglycidyl ether (see Glycidyl ethers)
Bisulfites (see Sulfur dioxide and some sulfites, bisulfites and metabisulfites)
Bitumens 35, 39 (1985); Suppl. 7, 133 (1987)
Bleomycins 26, 97 (1981); Suppl. 7, 134 (1987)
Blue VRS 16, 163 (1978); Suppl. 7, 59 (1987)
Boot and shoe manufacture and repair 25, 249 (1981); Suppl. 7, 232 (1987)
CUMULATIVE CROSS INDEX
Bracken fern
Brilliant Blue FCF, disodium salt
Bromochloroacetonitrile (see Halogenated acetonitriles)
Bromodichloromethane
Bromoethane
Bromoform
1,3-Butadiene
1,4-Butanediol dimethanesulfonate
n-Butyl acrylate
Butylated hydroxyanisole
Butylated hydroxytoluene
Butyl benzyl phthalate
13-Butyrolactone
y-Butyrolactone
c
Cabinet-making (see Furniture and cabinet-making)
Cadmium acetate (see Cadmium and cadmium compounds)
Cadmium and cadmium compounds
Cadmium chloride (see Cadmium and cadmium compounds)
Cadmium oxide (see Cadmium and cadmium compounds)
Cadmium sulfate (see Cadmium and cadmium compounds)
Cadmium sulfide (see Cadmium and cadmium compounds)
Caffeine
Calcium arsenate (see Arsenic and arsenic compounds)
Calcium chromate (see Chromium and chromium compounds)
Calcium cyclamate (see Cyclamates)
Calcium saccharin (see Saccharin)
Cantharidin
Caprolactam
Captafol
Captan
Carbaryl
Carbazole
3-Carbethoxypsoralen
Carbon blacks
Carbon tetrachloride
Carmoisine
Carpentry and joinery
Carrageenan
Catechol
CCNU (see 1-{2-Chloroethyl)-3-cyclohexyl-1-nitrosourea)
295
40, 47 (1986); Suppl. 7, 135 (1987)
16, 171 (1978) (con; 42, 257);
Suppl. 7, 59 (1987)
52, 179 (1991)
52, 299 (1991)
52, 213 (1991)
39, 155 (1986) (con: 42, 264);
Suppl. 7, 136 (1987); 54, 237 (1992)
4, 247 (1974); Suppl. 7, 137 (1987)
39, 67 (1986); Suppl. 7, 59 (1987)
40, 123 (1986); Suppl. 7, 59 (1987)
40, 161 (1986); Suppl. 7, 59 (1987)
29, 193 (1982) (con: 42, 261);
Supp/. 7, 59 (1987)
I I, 225 (1976); Suppl. 7, 59 (1987)
I 1, 231 (1976); Suppl. 7, 59 (1987)
2, 74 (1973); 11, 39 (1976) (con: 42,
255); Suppl. 7, 139 ( 1987)
51,291 (1991)
10, 79 (19',\:i); Suppl. 7, 59 (1987)
19, 115 (1979)(con: 42, 258);
39, 247 (1986) (con: 42, 264);
Suppl. 7, 390 (1987)
53, 353 (1991)
30, 295 (1983); Suppl. 7, 59 (1987)
I 2, 37 (1976); Suppl. 7, 59 (1987)
32, 239 (1983); Suppl. 7, 59 (1987)
40, 317 (1986); Suppl. 7, 59 (1987)
3, 22 (1973); 33, 35 (1984); Suppl. 7,
142 (1987)
1' 53 (1972); 20, 371 (1979);
Suppl. 7, 143 (1987)
8, 83 (1975); Suppl. 7, 59 (1987)
25, 139 (1981); Suppl. 7, 378 {1987)
10, 181 (1976) (con; 42, 255); 31,
79 (1983); Suppl. 7, 59 (1987)
15, 155 (1977); Suppl. 7, 59 (1987)
296 IARC MONOGRAPHS VOLUME 55
Ceramic fibres (see Man-made mineral fibres)
Chemotherapy, combined, including alkylating agents (see MOPP and
other combined chemotherapy including alkylating agents)
Chlorambucil
Chloramphenicol
Chlorendic acid
Chlordane (see also Chlordane/Heptachlor)
Chlordane/Heptachlor
Chlordecone
Chlordirneform
Chlorinated dibenzodioxins (other than TCDD)
Chlorinated drinking-water
Chlorinated paraffins
toluenes
Chlormadinone acetate (see also Progestins; Combined oral
contraceptives)
Chlomaphazine (see N,N-Bis(2-chloroethyl)-2-naphthylamine)
Chloroacetonitrile (see Halogenated acetonitriles)
Chlorobenzilate
Chlorodibromomethane
Chlorodifluoromethane
Chloroethane
1-(2-Chloroethyl)-3-cyclohexyl-1-nitrosourea (see also Chloroethyl
nitrosoureas)
1-(2-Chloroethyl)-3( 4-methylcyclohexyl)-1-nitrosourea (see also
Chloroethyl nitrosoureas)
Chloroethyl nitrosoureas
Chlorofluoromethane
Chloroform
Chloromethyl methyl ether (technical-grade) (see also
Bis(chloromethyl)ether)
(4-Chloro-2-methylphenoxy)acetic acid (see MCPA)
Chlorophenols
Chlorophenols (occupational exposures to)
Chlorophenoxy herbicides
Chlorophenoxy herbicides (occupational exposures to)
4-Chloro-onho-phenylenediamine
4-Chloro-meta-phenyleilediamine
Chloroprene
Chloropropham
Chloroquine
Chlorothalonil
para-Chloro-ortho-toluidine and its strong acid salts
(see also Chlordimeform)
Chlorotrianisene (see also Nonsteroidal oestrogens)
2-Chloro-1, 1, 1-trifluoroethane
Chlorozotocin
9, 125 (1975); 26, 115 (1981);
Suppl. 144(1987)
10, 85 (1976); Suppl. 7, 145 (1987);
50, 169 (1990)
48. 45 (1990)
20. 45 (1979) (corr. 42. 258)
Suppl. 7, 146 (1987); 53. 115 (1991)
20. 67 (1979); Suppl. 7, 59 (1987)
30, 61 (1983); Suppl. 7, 59 (1987)
15, 41 (1977); Suppl. 7, 59 (1987)
52. 45 (1991)
48, 55 (1990)
Supp/. 7, 148 (1987)
6, 149 (1974); 21' 365 (1979)
5, 75 (1974); 30, 73 (1983);
Suppl. 7, 60 (1987)
52, 243 (1991)
41, 237 (1986)(corr. 51,
Suppl. 7, 149 (1987)
52, 315 (1991)
26. 137 (1981) (corr. 42, 260);
Suppl. 7, 150 (1987)
SuppL 150(1987)
Suppl. 7, 150 (1987)
41, 229 (1986); Suppl. 7, 60 (1987)
1, 61 (1972); 20, 401 (1979);
Suppl. 7, 152 (1987)
4, 239 (1974); Suppl. 7, 131 (1987)
Suppl. 7, 154 (1987}
41' 319 (1986)
Suppl. 7. 156 (1987)
41, 357 (1986)
27, 81 (1982); Suppl. 7, 60 (1987)
27, 82 (1982); Suppl. 7, 60 (1987)
19. 131 (1979); Suppl. 7, 160 (1987)
12. 55 (1976); Suppl. 7. 60 (1987)
13, 47 (19n); Suppl. 7. 60 (1987)
30, 319 (1983); Suppl. 7. 60 (1987)
16, 2n (1978); 30, 65 (1983);
Suppl. 7. 60 (1987); 48, 123 (1990)
21, 139 (1979)
41, 253 (1986); Suppl. 7, 60 (1987)
50, 65 (1990)
CUMULATIVE CROSS INDEX 297
Cholesterol
Chromic acetate (see Chromium and chromium compounds)
Chromic chloride (see Chromium and chromium compounds)
Chromic oxide (see Chromium and chromium compounds)
Chromic phosphate (see Chromium and chromium compounds)
Chromite ore (see Chromium and chromium compounds)
Chromium and chromium compounds
Chromium carbonyl (see Chromium and chromium compounds)
Chromium potassium sulfate (see Chromium and chromium
compounds)
Chromium sulfate (see Chromium and chromium compounds)
Chromium trioxide (see Chromium and chromium compounds)
Chrysazin (see Dantron)
Chrysene
Chrysoidine
Chrysotile (see Asbestos)
Ciclosporin
CI Disperse Yellow 3
Cimetidine
Cinnamyl anthranilate
Cisplatin
Citrinin
Citrus Red No. 2
Clofibrate
Clomiphene citrate
Coal gasification
Coal-tar pitches (see also Coal-tars)
Coal-tars
Cobalt(IIl] acetate (see Cobalt and cobalt compounds)
Cobalt-aluminium- chromium spinel (see Cobalt and cobalt compounds)
10, 99 (1976); 31, 95 (1983);
Suppl. 7, 161 (1987)
2, 100 (1973); 23, 205 (1980);
Suppl. 7, 165 (1987); 49, 49 (1990)
(corr. 51, 483)
3, 159 (1973); 32, 241 (1983);
Suppl. 7, 60 (1987)
8, 91 (1975); Suppl. 7, 169 (1987)
50, 77 (1990)
8, 97 (1975); Suppl. 7, 60 (1987)
50, 235 (1990)
16, 281 (1978); 31, 133 (1983);
Suppl. 7, 60 (1987)
26, 151 (1981); Supp/. 7, no (1987)
40, 67 (1986); Suppl. 7, 60 (1987)
8, 101 (1975) (corr. 42, 254);
Suppl. 7, 60 (1987)
24, 39 (1980); Suppl. 7, 171 (1987)
21, 551 (1979); Suppl. 7, 172 (1987)
34, 65 (1984); Suppl. 7, 173 (1987)
35, 83 (1985); Suppl. 7, 174 (1987)
35, 83 (1985); Suppl. 7, 175 (1987)
Cobalt and cobalt compounds 52, 363 (1991)
Cobalt(II} chloride (see Cobalt and cobalt compounds)
Cobalt-chromium alloy (see Chromium and chromium
compounds)
Cobalt-chromium-molybdenum alloys (see Cobalt and cobalt compounds)
Cobalt metal powder (see Cobalt and cobalt compounds)
Cobalt naphthenate (see Cobalt and cobalt compounds)
Cobalt[II] oxide (see Cobalt and cobalt compounds)
Cobalt[II,III] oxide (see Cobalt and cobalt compounds)
Cobalt[II] sulfide (see Cobalt and cobalt compounds)
Coffee
Coke production
Combined oral contraceptives (see also Oestrogens, progestins
and combinations)
Conjugated oestrogens (see also Steroidal oestrogens)
51, 41 (1991) (corr. 52, 513)
34, 101 (1984); Suppl. 7, 176 (1987)
Supp/. 7, 297 (1987)
21' 147 (1979)
298
IARC MONOGRAPHS VOLUME 55
Contraceptives, oral (see Combined oral contraceptives;
Sequential oral contraceptives)
Copper 8-hydroxyquinoline
Coronene
Coumarin
Creosotes (see also Coal-tars)
meta-Cresidine
para-Cresidine
Crocidolite (see Asbestos)
Crude oil
Crystalline silica (see also Silica)
Cycasin
Cyclamates
Cyclamic acid (see Cyclamates)
Cyclochlorotine
Cyclohexanone
Cyclohexylamine (see Cyclamates)
Cyclopenta[cd]pyrene
Cyclopropane (see Anaesthetics, volatile)
Cyclophosphamide
D
2,4-D (see also Chlorophenoxy herbicides; Chlorophenoxy
herbicides, occupational exposures to)
Dacarbazine
Dantron
D& CRed No.9
Dapsone
Daunomycin
DDD (see DDT)
DDE (see DDT)
DDT
Decabromodiphenyl oxide
Deltamethrin
Diacetylaminoazotoluene
N.N' -Diacetylbenzidine
Dichlorvos
Diallate
2,4-Diaminoanisole
4,4' -Diaminodiphenyl ether
1,2-Diamino-4-nitrobenzene
1,4-Diamino-2-nitrobenzene
2,6-Diamino-3-(phenylazo )pyridine (see Phenazopyridine
hydrochloride)
2,4-Diaminotoluene (see also Toluene diisocyanates)
15, 103 (1977); Suppl. 7, 61 (1987)
32, 263 (1983); Suppl. 7, 61 (1987)
10, 113 (1976); Suppl. 7, 61 (1987)
35, 83 (1985); Suppl. 7, 177 (1987)
27, 91 (1982); Suppi. 7, 61 (1987)
27, 92 (1982); Suppi. 7, 61 (1987)
45, 119 (1989)
42, 39 (1987); Suppl. 7, 341 (1987)
1, 157 (1972) (carr. 42, 251); 10,
121 (1976); Suppl. 7, 61 (1987)
22, 55 (1980); Suppl. 7, 178 (1987)
10, 139 (1976); Suppl. 7, 61 (1987)
47, 157 (1989)
32, 269 (1983); Suppi. 7, 61 (1987)
9, 135 (1975); 26, 165 (1981);
Suppl. 7, 182 (1987)
15, 111 (1977)
26, 203 (1981); Suppl. 7, 184 (1987)
50, 265 (1990)
8, 107 (1975); Suppl. 7, 61 (1987)
24, 59 (1980); Suppl. 7, 185 (1987)
10, 145 (1976); Suppl. '7, 61 (1987)
5, 83 (1974) (carr. 42, 253);
Suppl. 7, 186 (1987); 53, 179 (1991)
48, 73 (1990) .
53, 251 (1991)
8, 113 (1975); Suppl. 7, 61 (1987)
16, 293 (1978); Suppl. 7, 61 (1987)
53, 267 (1991)
12, 69 (1976); 30, 235 (1983);
Suppl. 7, 61 (1987)
16, 51 (1978); 27, 103 (1982);
Suppl. 7, 61 (1987)
16, 301 (1978); 29, 203 (1982);
Suppl. 7, 61 (1987)
16, 63 (1978); Suppl. 7, 61 (1987)
16, 73 (1978); Suppl. 7, 61 (1987)
16, 83 (1978); Suppl. 7, 61 (1987)
CUMULATIVE CROSS INDEX
2,5-Diaminotoluene (see also Toluene diisocyanates)
onho-Dianisidine (see 3,3' -Dimethoxybenzidine)
Diazepam
Diazomethane
Dibenz( a,h )acridine
Dibenz[ a.J lacridine
Dibenz[ a,c ]anthracene
Dibenz( a,h ]anthracene
Dibenz[ a.Jlanthracene
7H-Dibenzo[c,g}carbazole
Dibenzodioxins, chlorinated (other than TCDD}
[see Chlorinated dibenzodioxins (other than TCDD)}
Dibenzo[ a,e )fluoranthene
Dibenzo[h,rst]pentaphene
Dibenzo[ a,e ]pyrene
Dibenzo[a,h )pyrene
Dibenzo[a,i]pyrene
Dibenzo[a,l)pyrene
Dibromoacetonitrile (see Halogenated acetonitriles)
1,2-Dibromo-3-chloropropane
Dichloroacetonitrile (see Halogenated acetonitriles)
Dichloroacetylene
onho-Dichlorobenzene
para-Dichlorobenzene
3,3' -Dichlorobenzidine
trans-1,4-Dichlorobutene
3,3' -Dichloro-4,4' -diaminodiphenyl ether
1,2-Dichloroethane
Dichloromethane
2,4-Dichlorophenol (see Chlorophenols; Chlorophenols,
occupational exposures to)
(2,4-Dichlorophenoxy)acetic acid (see 2,4-D)
2,6-Dichloro-para-phenylenediamine
1,2-Dichloropropane
1,3-Dichloropropene (technical-grade)
Dichlorvos
Dicofol
299
16, 97 (1978); Suppl. 7, 61 (1987)
13, 57 (1977); Suppl. 7, 189 (1987)
7, 223 (1974); Suppl. 7, 61 (1987)
3, 247 (1973); 32, 277 (1983);
Supp/. 7, 61 (1987}
3, 254 (1973}; 32, 283 (1983);
Suppl. 7, 61 (1987)
32. 289 (1983) (con: 42, 262);
Supp/. 7, 61 (1987}
3, 178 (1973) (con: 43, 261);
32, 299 (1983); Suppl. 7, 61 (1987)
32, 309 (1983); Suppl. 7, 61 (1987)
3, 260 (1973); 32, 315 (1983);
Supp/. 7, 61 (1987)
32, 321 (1983); Suppl. 7, 61 (1987}
3, 197 (1973); Suppl. 7, 62 (1987)
3, 201 {1973); 32, 327 {1983);
Suppl. 7, 62 (1987)
3, 207 {1973); 32, 331 (1983);
Suppl. 7, 62 (1987)
3, 215 (1973); 32, 337 (1983);
Suppl. 7, 62 (1987)
3, 224 {1973); 32, 343 (1983);
Suppl. 7, 62 {1987)
15, 139 (lm); 20, 83 {1979);
Suppl. 7, 191 (1987)
39, 369 (1986); Suppl. 7, 62 (1987)
7, 231 (1974); 29, 213 (1982);
Suppl. 7, 192 (1987)
7. 231 (1974); 29, 215 (1982);
Supp/. 7, 192 (1987)
4, 49 (1974); 29, 239 (1982);
Suppl. 7, 193 (1987)
15, 149 (1977); Suppl. 7, 62 (1987)
16, 309 (1978); Suppl. 7, 62 (1987)
20, 429 (1979); Suppl. 7, 62 (1987)
20, 449 (1979); 41' 43 (1986);
Suppl. 7, 194 (1987}
39, 325 (1986); Suppl. 7, 62 (1987}
41, 131 (1986); Suppl. 7, 62(1987)
41, 113 (1986); Suppl. 7, 195 (1987)
20, 97 (1979); Suppl. 7. 62 (1987);
53, 267 (1991)
30, 87 (1983); Suppl. 7, 62 (1987)
300
IARC MONOGRAPHS VOLUME 55
Dicyclohexylamine (see Cyclamates)
Dieldrin
Dienoestrol (see also Nonsteroidal oestrogens)
Diepoxybutane
Diesel and gasoline engine exhausts
Diesel fuels
Diethyl ether (see Anaesthetics, volatile)
Di(2-ethylhexyl)adipate
Di(2-ethylhexyl)phthalate
1,2-Diethylhydrazine
Diethylstilboestrol
Diethylstilboestrol dipropionate (see Diethylstilboestrol)
Diethyl sulfate
Diglycidyl resorcinol ether
Dihydrosafrole
1,8-Dihydroxyanthraquinone (see Dantron)
Dihydroxybenzenes (see Catechol; Hydroquinone; Resorcinol)
Dihydroxymcthylfuratrizine
Diisopropyl sulfate
Dimethisterone (see also Progestins; Sequential oral
contraceptives)
Dimethoxane
3,3' -Dimethoxybenzidine
3,3' -Dimethoxybenzidine-4,4' -diisocyanate
para-Dimethylaminoazobenzene
para-Dimethylaminoazobenzenediazo sodium sulfonate
trans-2-[ (Dimethylamino )methyl imino )-5-[2-( 5-nitro-2-furyl )-
vinyl]-1,3,4-oxadiazole
4,4' -Dimethylangelicin plus ultraviolet radiation (see also
Angelicin and some synthetic derivatives)
4,5' -Dimethylangelicin plus ultraviolet radiation (see also
Angelicin and some synthetic derivatives)
Dimethylarsinic acid (see Arsenic and arsenic compounds)
3,3'-Dimethylbenzidine
Dimethylcarbamoyl chloride
Dimethylformamide
1, 1-Dimethylhydrazine
1,2-Dimethylhydrazine
Dimethyl hydrogen phosphite
1,4-Dimethylphenanthrene
Dimethyl sulfate
3, 7-Dinitrofluoranthene
3,9-Dinitrofluoranthene
1,3 Dinitropyrene
1,6-Dinitropyrene
5, 125 (1974); Suppl. 7, 196 (1987)
21, 161 (1979)
11, 115 ( 1976) (con: 42, 255); Suppl. 7,
62 (1987)
46, 41 (1989)
45, 219 (1989) (con: 47, 505)
29, 257 (1982); Suppl. 7, 62 (1987)
29,269 (1982) (con: 42, 261); Suppl. 7,
62 (1987)
4, 153 (1974); Suppl. 7, 62 (1987)
6, 55 (1974); 21, 173 (1979)
(con: 42, 259); Suppl. 7, 273 (1987)
4, 277 (1974); Suppl. 7, 198 (1987);
54, 213 (1992)
II, 125 (1976); 36, 181 (1985);
Suppl. 7, 62 (1987)
], 170 (1972); 10, 233 (1976);
Suppl. 7, 62 (1987)
24, 77 (1980); Suppl. 7, 62 (1987)
54, 229 (1992)
6, 167 (1974); 21, 377 (1979)
15, 117 (1977); Suppl. 7, 62 (1987)
4, 41 (1974); Suppl. 7, 198 (1987)
39, 219 (1986); Suppl. 7, 62 (1987)
8, 125 (1975); Suppl. 7, 62 (1987)
8, 147 (1975); Suppl. 7, 62 (1987)
7, 147 (1974) (con: 42, 253); Suppl. 7,
62 (1987)
Suppl. 7, 57 (1987)
Suppl. 7, 57 (1987)
I, 87 (1972); Suppl. 7, 62 (1987)
12, 71 (1976); Suppl. 7, 199 (1987)
47, 171 (1989)
4, 137 (1974); Suppl. 7, 62 (1987)
4, 145 (1974) (con: 42, 253); Suppl. 7,
62 (1987)
48, 85 (1990)
32, 349 (1983); Suppl. 7, 62 (1987)
4, 271 (1974); Suppl. 7, 200 (1987)
46, 189 (1989)
46, 195 (1989)
46, 201 (1989)
46, 215 (1989)
1,8-Dinitropyrene
Dinitrosopentamethylenetetramine
1,4-Dioxane
2,4' -Diphenyldiamine
CUMULATIVE CROSS INDEX
Direct Black 38 (see also Benzidine-based dyes)
Direct Blue 6 (see also Benzidine-based dyes)
Direct Brown 95 (see also Benzidine-based dyes)
Disperse Blue 1
Disperse Yellow 3
Disulfiram
Dithranol
Divinyl ether (see Anaesthetics, volatile)
Dulcin
E
Endrin
Enflurane (see Anaesthetics, volatile)
Eosin
Epichlorohydrin
1,2-Epoxybutane
1-Epoxyethyl-3,4-epoxycyclohexane
3,4-Epoxy-6-methylcyclohexylmethyl-3,4-epoxy-6-methyl-
cyclohexane carboxylate
cis-9,10-Epoxystearic acid
Erionite
Ethinyloestradiol (see also Steroidal oestrogens)
Ethionamide
Ethyl acrylate
Ethylene
Ethylene dibromide
Ethylene oxide
Ethylene sulfide
Ethylene thiourea
Ethyl methanesulfonate
N-Ethyl-N-nitrosourea
Ethyl selenac (see also Selenium and selenium compounds)
Ethyl tellurac
Ethynodiol diacetate (see also Progestins; Combined oral
contraceptives)
Eugenol
Evans blue
F
Fast Green FCF
Fen valerate
301
33, 171 (1984); Suppl. 7, 63 (1987);
46, 231 (1989)
11, 241 (1976); Suppl. 7, 63 (1987)
11, 247 {1976); Suppl. 7, 201 (1987)
16, 313 (1978); Suppl. 7, 63 (1987)
29, 295 (1982) (corr. 42, 261)
29, 311 (1982)
29, 321 (1982)
48, 139 (1990)
48, 149 (1990)
12, 85 (1976); Suppl. 7, 63 (1987)
13, 75 (1977); Suppl. 7, 63 (1987)
12, 97 (1976); Suppl. 7, 63 (1987)
5, 157 (1974); Suppl. 7, 63 (1987)
15, 183 (1977); Suppl. 7, 63 (1987)
11, 131 (1976) (corr. 42, 256);
Suppl. 7, 202 (1987)
47, 217 (1989)
11, 141 (1976); Suppl. 7, 63 (1987)
11, 147 (1976); Suppl. 7, 63 (1987)
11, 153 (1976); Suppl. 7, 63 (1987)
42, 225 (1987); Suppl. 7, 203 (1987)
6, 77 (1974); 21, 233 (1979)
13, 83 (1977); Suppl. 7, 63 (1987)
19, 57 (1979); 39, 81 (1986);
Suppl. 7, 63 (1987)
19, 157 (1979); Suppl. 7, 63 (1987)
15, 195 (1977); Suppl. 7, 204 (1987)
11, 157 (1976); 36, 189 (1985)
(corr. 42, 263); Suppl. 7, 205 (1987)
11, 257 (1976); Suppl. 7, 63 (1987)
7, .45 (1974); Suppl. 7, 207 (1987)
7, 245 (1974); Suppl. 7, 63 (1987)
1, 135 (1972); 17, 191 (1978);
Suppl. 7, 63 (1987)
12, 107 (1976); Suppl. 7, 63 (1987)
12, 115 (1976); Suppl. 7, 63 (1987)
6, 173 (1974); 21, 387 (1979)
36, 15 (1985); Suppl. 7, 63 (1987)
8, 151 (1975); Suppl. 7, 63 (1987)
16, 187 (1978); Suppl. 7, 63 {1987)
53, 309 (1991)
302
IARC MONOGRAPHS VOLUME 55
Fe.rbam
Ferric oxide
Ferrochromium (see Chromium and chromium compounds)
Fluometuron
Fluoranthene
Fluorene
Fluorides (inorganic, used in drinking-water)
5-Fiuorouracil
Fluorspar (see Fluorides)
Fluosilicic acid (see Fluorides)
. Fluroxene (see Anaesthetics, volatile)
Fonnaldehyde
2-(2-Fonnylhydrazino )-4-( 5-nitro-2-fury! )thiazole
Frusemide (see Furosemide)
Fuel oils {heating oils)
Furazolidone
Furniture and cabinet-making
Furosemide
2-(2-Furyl)-3-( 5-nitro-2-f uryl )acrylamide (see AF-2)
Fusarenon-X
G
Gasoline
Gasoline engine exhaust (see Diesel and gasoline engine exhausts)
Glass fibres (see Man-made mineral fibres)
Glasswool (see Man-made mineral fibres)
Glass filaments (see Man-made mineral fibres)
Glu-P-1 .
Glu-P-2
L-Giutamic acid, 5-[2-(4-hydroxymethyl)phenylhydrazide)
(see Agaritine)
G lycidaldehyde
Glycidyl ethers
Glycidyl oleate
Glycidyl stearate
Griseofulvin
Guinea Green B
Gyromitrin
H
Haematite
Haematite and ferric oxide
Haematite mining, underground, with exposure to radon
Hair dyes, epidemiology of
Halogenated acetonitriles
Halothane (see Anaesthetics, volatile)
at-HCH (see Hexachlorocyclohexanes)
12, 121 (1976)(con: 42, 256);
Suppl. 7, 63 (1987)
1, 29 {1972); Suppl. 7, 216 (1987)
30, 245 (1983); Suppl. 7, 63 (1987)
32, 355 (1983); Suppl. 7, 63 (1987)
32, 365 (1983); Suppl 7, 63 (1987)
27, 237 (1982); Suppl. 7, 208 (1987)
26, 217 {1981); Suppl. 7, 210 (1987)
29, 345 (1982); Suppl. 7, 211 (1987)
7, 151 (1974) (con: 42, 253);
Suppl. 7, 63 {1987)
45, 239 {1989) (con: 47, 505)
31, 141 (1983); Suppl. 7, 63 (1987)
25, 99 (1981); Suppl. 7, 380 (1987)
50, 277 {1990)
11, 169 (1976); 31, 153 (1983);
Suppl. 7, 64 (1987)
45, 159 (1989) (con: 47, 505)
40, 223 (1986); Suppl. 7, 64 (1987)
40, 235 (1986); SuppL 7, 64 (1987)
11, 175 (1976); Suppl. 7, 64 (1987)
47, 237 (1989)
11, 183 (1976); Suppl. 7, 64 (1987)
11, 187 (1976); Suppl. 7, 64 (1987)
10, 153 (1976); Suppl. 7, 391 (1987)
16, 199 (1978); Suppl. 7, 64 (1987)
31, 163 (1983); Suppl. 7, 391 (1987)
1, 29 (1972); Suppi. 7, 216 (1987)
Suppi. 7, 216 (1987)
1, 29 (1972); Suppl. 7, 216 (1987)
16, 29 (1978); 27, 307 (1982)
52, 269 (1991)
CUMUlATIVE CROSS INDEX
(see Hexachlorocyclohexanes)
-y-HCH (see Hexachlorocyclohexanes)
Heating oils (see Fuel oils)
Heptachlor (see also Chlordane/Heptachlor)
Hexachlorobenzene
Hexachlorobutadiene
Hexachlorocyclohexanes
Hexachlorocyclohexane, technical-grade (see Hexachloro-
cyclohexanes)
Hexachloroethane
Hexachlorophene
Hexamethylphosphoramide
Hexoestrol (see Nonsteroidal oestrogcns)
Hycanthone mesylate
Hydralazine
Hydrazine
Hydrochloric acid
Hydrochlorothiazide
Hydrogen peroxide
Hydroquinone
4-Hydroxyazobenzene
caproate (see also Progestins)
&-Hydroxyquinoline
8-Hydroxysenkirkine
Hypochlorite salts
I
Indeno[ 1,2,3-cd]pyrene
Inorganic acids (see Sulfuric acid and other st rong inorganic acids,
occupational exposures to mists and vapours from)
Insecticides, occupational exposures in spraying and application of
IQ
Iron and steel founding
Iron-dextran complex
Iron-dextrin complex
Iron oxide (see Ferric oxide)
Iron oxide, saccharated (see Saccharated iron oxide)
Iron sorbitol-<:itric acid complex
lsatidine
Isoflurane (see Anaesthetics, volatile)
Isoniazid (see Isonicotinic acid hydrazide)
Isonicotinic acid hydrazide
Isophosphamide
Isopropyl alcohol
Isopropyl alcohol manufacture (strong-acid process)
(see also Isopropyl alcohol; Sulfuric acid and other strong inorganic
acids, occupational exposures to mists and vapours from)
Isopropyl oils
303
5, 173 (1974); 20, 129 (1979)
20, 155 (1979); Suppl. 7, 219 (1987)
20, 179 (1979); SuppL 7; 64 (1987)
5, 47 (1974); 20, 195 (1979) (con; 42,
258); Suppl. 7, 220 (1987)
20, 467 (1979); SuppL 7, 64 (1987)
20, 241 (1979); SuppL 7, 64 (1987)
15, 211 (1977); Suppl. 7, 64 (1987)
13, 91 (1977); Suppl. 7, 64 (1987)
24, 85 (1980); Suppl. 7, 222 (1987)
4, 127 (1974); Suppl. 7, 223 (1987)
54, 189 (1992)
50, 293 (1990)
36, 285 (1985); Suppl. 7, 64 (1987)
15, 155 (1977); Suppl. 7, 64 (1987)
8, 157 (1975); Suppl. 7, 64 (1987)
21, 399 (1979) (con: 42, 259)
13, 101 (1977); Suppl. 7, 64 (1987)
10, 265 (1976); Suppl. 7, 64 {1987)
52, 159 (1991)
3, 229 (1973); 32, 373 (1983);
Suppl. 7, 64 (1987)
53, 45 (1991)
40, 261 (1986); Suppl. 7, 64 (1987)
34, 133 (1984); Suppl. 7, 224 (1987)
2, 161 (1973); Suppl. 7, 226 (1987)
2, 161 (1973) (corr. 42, 252);
Suppl. 7, 64 (1987)
2, 161 (1973); Suppl. 7, 64 (1987)
10, 269 (1976); Suppl. 7, 65 (1987)
4, 159 (1974); Suppl. 7, 227 (1987)
26, 237 (1981); Suppl. 7, 65 (1987)
15, 223 (1977); Suppl. 7, 229 (1987)
Suppl. 7, 229 (1987)
15, 223 (1977); Suppl. 7, 229 {1987)
304
IARC MONOGRAPHS VOLUME 55
lsosafrole
J
Jacobine
Jet fuel
Joinery (see Carpentry and joinery)
K
Kaempferol .
Kepone (see Chlordecone)
L
Lasiocarpine
Lauroyl peroxide
Lead acetate (see Lead and lead compounds)
Lead and lead compounds
Lead arsenate (see Arsenic and arsenic compounds)
Lead carbonate (see Lead and lead compounds)
Lead chloride (see Lead and lead compounds)
Lead chromate (see Chromium and chromium compounds)
Lead chromate oxide (see Chromium and chromium compounds)
Lead naphthenate (see Lead and lead compounds)
Lead nitrate (see Lead and lead compounds)
Lead oxide (see Lead and lead compounds)
Lead phosphate (see Lead and lead compounds)
Lead subacetate (see Lead and lead compounds)
Lead tetroxide (see Lead and lead compounds)
Leather goods manufacture
Leather industries
Leather tanning and processing
Ledate (see also Lead and lead compounds)
Light Green SF
Lindane (see Hexachlorocyclohexanes)
The lumber and sawmill industries (including logging)
Luteoskyrin
Lynoestrenol (see also Progestins; Combined oral contraceptives)
M
Magenta
Magenta, manufacture of (see also Magenta)
Malathion
Maleic hydrazide
I, 169 (1972); 10, 232 (1976);
Suppl. 7, 65 (1987)
10, 275 (1976); Suppl. 7, 65 (1987)
45, 203 (1989)
31, 171 (1983); Suppl. 7, 65 (1987)
10, 281 (1976); Suppl. 7, 65 (1987)
36, 315 (1985); Suppl. 7, 65 (1987)
I , 40 (1972) (con: 42, 251); 2, 52,
150 (1973); 12, 131 (1976);
23, 40, 208, 209, 325 (1980);
Suppl. 7, 230 (1987)
25, 279 (1981); Suppl. 7, 235 (1987)
25, 199 (1981); Suppl. 7, 232 (1987)
25, 201 (1981); Suppl. 7, 236 (1987)
12, 131 (1976)
16, 209 (1978); Suppl. 7, 65 (1987)
25, 49 (1981); Suppl. 7, 383 (1987)
10, 163 (1976); Suppl. 7, 65 (1987)
21, 407 (1979)
4, 57 (1974) (con: 42, 252);
Suppl. 7, 238 (1987)
Suppl. 7, 238 (1987)
30, 103 (1983); Suppl. 7, 65 (1987)
4, 173 (1974) (con: 42, 253);
Suppl. 7, 65 (1987)
Malonaldehyde
Maneb
Man-made mineral fibres
Mannomustine
Mate
CUMULATIVE CROSS INDEX
MCPA (see also Chlorophenoxy herbicides; Chlorophenoxy
herbicides, occupational exposures to)
M e A ~ c
Medphalan
Medroxyprogesterone acetate
Megestrol acetate (see also Progestins; Combined oral
contraceptives)
MeiQ
MeiQx
Melamine
Melphalan
6-Mercaptopurine
Merphalan
Mestranol (see also Steroidal oestrogens)
Metabisulfites (see Sulfur dioxide and some sulfites, bisulfites
and metabisulfites)
Methanearsonic acid, disodium salt (see Arsenic and arsenic
compounds)
Methanearsonic acid, monosodium salt (see Arsenic and arsenic
compounds
Methotrexate
Methoxsalen (see 8-Methoxypsoralen)
Methoxychlor
Methoxyflurane (see Anaesthetics, volatile)
5-Methoxypsoralen
8-Methoxypsoralen (see also 8-Methoxypsoralen plus ultraviolet
radiation)
8-Methoxypsoralen plus ultraviolet radiation
Methyl acrylate
5-Methylangelicin plus ultraviolet radiation (see also Angelicin
and some synthetic derivatives)
2-Methylaziridine
Methylazoxymethanol acetate
Methyl bromide
Methyl carbamate
Methyl-CCNU [see 1-(2-Chloroethyl )-3-( 4-methylcyclohexyl)-
1-nitrosourea)
Methyl chloride
1-, 2-, 3-, 4-, 5- and 6-Methylchrysenes
N-Methyl-N,4-dinitrosoaniline
305
36, 163 (1985); Supp{. 7, 65 (1987)
12, 137 (1976); Supp{. 7, 65 (1987)
43, 39 (1988)
9, 157 (1975); Suppl. 7, 65 (1987)
51, 273 (1991)
30, 255 (1983)
40, 253 (1986); Suppl. 7, 65 (1987)
9, 168 (1975); Suppl. 7, 65 (1987)
6, 157 (1974); 2J, 417 (1979) (CO"- 42,
259); Suppl. 7, 289 (1987)
40, 275 (1986); Suppl. 7, 65 (1987)
40, 283 (1986); Supp{. 7, 65 (1987)
39, 333 (1986); Suppl. 7, 65 (1987)
9, 167 (1975); Suppl. 7, 239 (1987)
26, 249 (1981); Suppl. 7, 240 (1987)
9, 169 (1975); Suppl. 7, 65 (1987)
6, 87 (1974); 21, 257 (1979) (con: 42,
259)
26, 267 (1981); Suppl. 7, 241 (1987)
5, 193 (1974); 20, 259 (1979);
Suppl. 7, 66 (1987)
40, 327 (1986); Suppl. 7, 242 (1987)
24, 101 (1980)
Suppl. 7, 243 (1987)
19, 52 (1979); 39, 99 (1986);
Supp{. 7, 66 (1987)
Suppl. 7, 57 (1987)
9, 61 (1975); Suppl. 7, 66 (1987)
1, 164 (1972); 10, 131 (1976);
Suppl. 7, 66 (1987)
41, 187 (1986) (corr. 45, 283);
Suppl. 7, 245 (1987)
12, 151 (1976); Suppl. 7, 66 (1987)
41, 161 (1986); Suppl. 7, 246 (1987)
32, 379 (1983); Suppl. 7, 66 (1987)
1, 141 (1972); Suppl. 7, 66 (1987)
306
IARC MONOGRAPHS VOLUME 55
4,4' -Methylene bis(2-chloroaniline)
4.4' -Methylene bis(N.N-dimethyl)benzenarnine
4,4' -Methylene bis(2-methylaniline)
4.4' -Methylenedianiline
4,4' -Methylenediphenyl diisocyanate
2-Methylfluoranthene
3-Methylfluoranthene
Methylglyoxal
Methyl iodide
Methyl methacrylate
Methyl methanesulfonate
2-Methyl-1-nitroanthraquinone
N-Methyl-N' -nitro-N-nitrosoguanidine
3-Methylnitrosam inopropionaldehyde [see 3-(N-N itrosornethylam ino )-
propionaldehyde]
3-Methylnitrosaminopropionitrile (see 3-(N-Nitrosomethylamino)-
propionitrile]
4, 65 (1974) (con: 42, 252); Suppl. 7,
246 (1987)
27, 119 {1982); Suppl. 7, 66 (1987)
4, 73 (1974); Suppl. 7, 248 (1987)
4, 79 (1974) (con: 42. 252);
39, 347 {1986); Suppl. 7, 66 (1987)
19, 314 (1979); Suppl. 7, 66 (1987)
32, 399 (1983); Suppl. 7, 66 (1987)
32, 399 (1983); Suppl. 7, 66 (1987)
51, 443 (1991)
15, 245 (1977); 41, 213 (1986);
Suppl. 7, 66 (1987)
19, 187 (1979); Suppl. 7, 66 (1987)
7, 253 (1974); Suppl. 7, 66 (1987)
27, 205 (1982); SuppL 7, 66 (1987)
4, 183 (1974); Suppl. 7, 248 (1987)
4-(Methylnitrosarnino )-4-(3-pyridyl)-1-butanal (see 4-(N-Nitrosomethyl-
amino )-4-(3-pyridyl )-1-butanal]
4-(Methylnitrosamino )-1-(3-pyridyl)-1-butanone [see 4-(N-Nitrosomethyl-
amino )-1-(3-pyridyl)-1-butanone]
N-Methyl-N-nitrosourea
N-Methyl-N-nitrosourethane
Methyl parathion
1-Methylphenanthrene
7-Methylpyrido3,4-c ]psoralen
Methyl red
Methyl selenac (see also Selenium and selenium compounds)
Methylthiouracil
Metronidawle
Mineral oils
Mirex
Mitomycin C
MNNG [see N-Methyi-N' -nitro-N-nitrosoguanidine]
MOCA [see 4.4' -Methylene bis(2-chloroaniline)]
Modacrylic fibres
Monocrotaline
Monuron
MOPP and other combined chemotherapy including
alkylating agents
Morpholine
5-(Morpholinomethyl)-3-[ ( 5-nitrofurfurylidene )amino ]-2-
oxazolidinone
Mustard gas
1, 125 (1972); 17, 227 (1978);
Suppl. 7, 66 (1987)
4, 211 (1974); Suppl. 7, 66 (1987)
30, 131 (1983); Supp/. 7, 392 (1987)
32, 405 (1983); Suppl. 7, 66 (1987)
40, 349 (1986); Suppl. 7, 71 {1987)
8, 161 (1975); Suppl. 7, 66 (1987)
12, 161 (1976); Suppl. 7, 66 (1987)
7, 53 (1974); Suppl. 7, 66 (1987)
13, 113 (1977); Suppl. 7, 250 (1987)
3, 30 (1973); 33, 87 (1984) (con: 42,
262); Suppl. 7, 252 (1987)
5, 203 (1974); 20, 283 (1979) (con: 42,
258); Suppl. 7, 66 (1987)
10, 171 (1976); Suppl. 7, 67 (1987)
19, 86 (1979); Suppl. 7, 67 (1987)
10, 291 (1976); Suppl. 7, 67 (1987)
12, 167 (1976); Suppl. 7, 67 (1987);
53, 467 (1991)
Suppl. 7, 254 (1987)
47, 199 (1989)
7, 161 (1974); Suppl. 7, 67 (1987)
9, 181 (1975) (corr. 42, 254);
Suppl. 7, 259 (1987)
CUMULATIVE CROSS INDEX
Myleran (see 1,4-Butanediol dimethanesulfonate)
N
Nafenopin
1,5-Naphthalenediamine
1,5-Naphthalene diisocyanate
1-Naphthylamine
2-Naphthylamine
1-Naphthylthiourea
Nickel acetate (see Nickel and nickel compounds)
Nickel ammonium sulfate (see Nickel and nickel compounds)
Nickel and nickel compounds
Nickel carbonate (see Nickel and nickel compounds)
Nickel carbonyl (see Nickel and nickel compounds)
Nickel chloride (see Nickel and nickel compounds)
Nickel-gallium alloy (see Nickel and nickel compounds)
Nickel hydroxide (see Nickel and nickel compounds)
Nickelocene (see Nickel . and nickel compounds)
Nickel oxide (see Nickel and nickel compounds)
Nickel subsulfide (see Nickel and nickel compounds)
Nickel sulfate (see Nickel and nickel compounds)
Niridazole
Nithiazide
Nitrilotriacetic acid and its salts
5-Nitroacenaphthene
5-N itro-ortho-anisidine
9-Nitroanthracene
7-Nitrobenz[a ]anthracene
6-N i trobenzo[ a ]pyrene
4-Nitrobiphenyl
6-N itrochrysene
Nitrofen (technical-grade)
3-Nitrofluoranthene
2-Nitrofluorene
Nitrofural
5-Nitro-2-furaldehyde semicarbazone (see Nitrofural)
Nitrofurantoin
Nitrofurazone (see Nitrofural)
1-[ ( 5-N itrofurfurylidene )amino )-2-imidazolidinone
N-[ 4-( 5-Nitro-2-f uryl)-2-thiazolyl }acetamide
Nitrogen mustard
Nitrogen mustard N-oxide
1-Nitronaphthalene
2-Nitronaphthalene
307
24, 125 (1980); Suppl. 7, 67 (1987)
27, 127 (1982); Suppl. 7, 67 (1987)
19, 311 (1979); Suppl. 7, 67 (1987)
4, 87 (1974) (con: 42, 253);
Supp/. 7, 260 (1987)
4, 97 (1974); Suppl. 7, 261 (1987)
30, 347 (1983); Suppl. 7, 263 (1987)
2, 126 (1973) (con: 42, 252); 11, 15
(1976); Suppl. 7, 264 (1987)
(corr. 45, 283); 49, 257 (1990)
13, 123 (1977); Suppl. 7, 67 (1987)
31, 179 (1983); Suppl. 7, 67 (1987)
48, 181 (1990)
16, 319 (1978); Suppl. 7, 67 (1987)
27, 133 (1982); Suppl. 7, 67 (1987)
33, 179 (1984); Suppl. 7, 67 (1987)
46, 247 (1989)
33, 187 (1984); Suppl. 7, 67 (1987);
46, 255 (1989)
4, 113 (1974); Suppl. 7, 67 (1987)
33, 195 (1984); Suppl. 7, 67 (1987);
46, 267 (1989)
30, 271 (1983); Suppl. 7, 67 (1987)
33, 201 (1984); Suppl. 7, 67 (1987)
46, 277 (1989)
7, 171 (1974); Suppl. 7, 67 (1987);
50, 195 (1990)
50, 211 (1990)
7, 181 (1974); Suppl. 7, 67 (1987)
I, 181 (1972); 7, 185 (1974);
Suppl. 7, 67 (1987)
9, 193 (1975); Suppl. 7, 269 (1987)
9, 209 (1975); Suppl. 7, 67 (1987)
46, 291 (1989)
46, 303 (1989)
308
IARC MONOGRAPHS VOLUME 55
3-Nitroperylene
2-Nitropropane
1-Nitropyrene
2-Nitropyrene
4-Nitropyrene
N-Nitrosatable drugs
N-Nitrosatable pesticides
N' -Nitrosoanabasine
N' -Nitrosoanatabine
N-Nitrosodi-n-butylamine
N-Nitrosodiethanolamine
N-Nitrosodiethylamine
N-Nitrosodimethylamine
N-Nitrosodiphenylamine
para-Nitrosodiphenylamine
N-Nitrosodi-n-propylamine
N-Nitroso-N-ethylurea (see N-Ethyl-N-nitrosourea)
N-Nitrosofolic acid
N-Nitrosoguvacine
N-Nitrosoguvacoline
N-Nitrosohydroxyproline
3-(N-Nitrosomethylamino)propionaldehyde
3-(N-Nitrosomethylamino)propionitrile
4-(N-Nitrosomethylamino )-4-(3-pyridyl )-1-butanal
4-(N- Nitrosomethylamino )-1-(3-pyridyl )-1-butanone
N-Nitrosomethylethylamine
N-Nitroso-N-methylurea (see N-Methyl-N-nitrosourea)
N-Nitroso-N-methylurethane (see N-Methyi-N-methylurethane)
N-Nitrosomethylvinylamine
N-Nitrosomorpholine
N' -Nitrosonomicotine
N-Nitrosopiperidine
N-Nitrosoproline
N-Nitrosopyrrolidine
N- Nitrososarcosine
Nitrosoureas, chloroethyl (see Chloroethyl nitrosoureas)
5-Nitro-ortho-toluidine
Nitrous oxide (see Anaesthetics, volatile)
Nitrovin
NNA [see 4-(N-Nitrosomethylamino )-4-(3-pyridyl)-1-butanal]
NNK [see 4-(N-Nitrosomethylamino )-1-(3-pyridyl)-1-butanone]
Nonsteroidal oestrogens (see also Oestrogens, progestins and
combinations)
Norethisterone (see also Progestins; Combined oral
contraceptives)
46, 313 (1989)
29, 331 (1982); SuppL 7, 67 (1987)
33, 209 (1984); SuppL 7, 67 (1987);
46, 321 (1989)
46, 359 (1989)
46, 367 (1989)
24, 297 (1980) (con: 42, 260)
30, 359 (1983)
37, 225 (1985); Suppl. 7, 67 (1987)
37, 233 (1985); Suppl. 7, 67 (1987)
4, 197 (1974); 17, 51 (1978);
Suppl. 7, 67 (1987)
17, 77 (1978); Suppl. 7, 67 (1987)
1, 107 (1972)(corr. 42, 251);
17, 83 (1978) (corr. 42, 257);
Suppl. 7, 67 (1987)
1, 95 (1972); 17., 125 (1978)
(corr. 42, 257); Suppl. 7, 67 (1987)
27, 213 (1982); Suppl. 7, 67 (1987)
27, 227 (1982) (corr. 42, 261);
Suppl. 7, 68 (1987)
17, 177 (1978); Suppl. 7, 68 (1987)
17, 217 (1978); SuppL 7, 68 (1987)
37, 263 (1985); Suppl. 7, 68 (1987)
37, 263 (1985); Suppl. 7, 68 (1987)
17, 304 (1978); Suppl. 7, 68 (1987)
37, 263 (1985); Suppl. 7, 68 (1987)
37, 263 (1985); Suppl 7, 68 (1987)
37, 205 (1985); Suppl. 7, 68 (i987)
37, 209 (1985); Suppl. 7, 68 (1987)
17, 221 (1978); Suppl. 7, 68 (1987)
17, 257 (1978); Suppl. 7, 68 (1987)
17, 263 (1978); Suppl. 7, 68 (1981)
17, 281 (1978); 37, 241 (1985);
Suppl. 7, 68 (1987)
17, 281 (1978); Suppl. 7, 68 (1987)
17, 303 (1978); Suppl. 7, 68 (1987)
17, 313 (1978); Suppl. 7, 68 (1987)
17, 327 (1978); Suppl. 7, 68 (1987)
48, 169 (1990)
31, 185 (1983); Suppl. 7, 68 (1987)
Suppl. 7, 272 (1987)
6, 179 (1974); 21, 461 (1979)
CUMUlATIVE CROSS INDEX
309
Norethynodrel (see also Progestins; Combined oral
contraceptives
Norgestrel (see also Progestins, Combined oral contraceptives)
Nylon 6
0
Ochratoxin A
Oestradiol-1713 (see also Steroidal oestrogens)
Oestradiol3-benzoate (see Oestradiol-17M
Oestradiol dipropionate (see Oestradiol-1713)
Oestradiol mustard
Oestradiol-1713-valerate (see Oestradiol-1713)
Oestriol (see also Steroidal oestrogens)
Oestrogen-progestin combinations (see Oestrogens, progestins
and combinations)
Oestrogen-progestin replacement therapy (see also Oestrogens,
progestins and combinations)
Oestrogen replacement therapy (see also Oestrogens, progestins
and combinations)
Oestrogens (see Oestrogens, progestins and combinations)
Oestrogens, conjugated (see Conjugated oestrogens)
Oestrogens, nonsteroidal (see Nonsteroidal oestrogens)
Oestrogens, progestins and combinations
Oestrogens, steroidal (see Steroidal oestrogens)
Oestrone (see also Steroidal oestrogens)
Oestrone benzoate (see Oestrone)
Oil Orange SS
Oral contraceptives, combined (see Combined oral contraceptives)
Oral contraceptives, investigational (see Combined oral
contraceptives)
Oral contraceptives, sequential (see Sequential oral contraceptives)
Orange I
Orange G
Organolead compounds (see also Lead and lead compounds)
Oxazepam
Oxymetholone [see also Androgenic (anabolic) steroids]
Oxyphenbu tazone
p
Paint manufacture and painting (occupational exposures in)
Panfuran S (see also Dihydroxymethylfuratrizine)
Paper manufacture (see Pulp and paper manufacture)
Paracetamol
Parasorbic acid
Parathion
Patulin
6, 191 (1974); 21' 461 (1979)
(carr. 42, 259)
6, 201 (1974); 21' 479 (1979)
19, 120 (1979); Suppl.. 7, 68 (1987)
10, 191 (1976); 31' 191 (1983)
(carr. 42, 262); Suppl. 7, 271 (1987)
6, 99 (1974); 21, 279 (1979)
9, 217 (1975)
6, 117 (1974); 21, 327 (1979)
Suppl. 7, 308 (1987)
Suppl. 7, 280 (1987)
6 (1974); 21 (1979);
SuppL 7, 272 (1987)
6, 123 (1974); 21, 343 (1979)
(carr. 42, 259)
8, 165 (1975); Suppl. 7, 69 {1987)
8, 173 (1975); Suppl. 7, 69 (1987)
8, 181 (1975); Suppl. 7, 69 (1987)
Suppl. 7, 230 (1987).
13, 58 (1977); Suppl. 7, 69 (1987)
13, 131 (1977)
13, 185 (1977); Suppl. 7, 69 {1987)
47, 329 (1989)
24, 77 (1980); Suppl. 7, 69 (1987)
50, 307 (1990)
10, 199 (1976) (corr. 42, 255);
Suppl. 7, 69 (1987)
30, 153 (1983); Suppl. 7, 69 (1987)
10, 205 (1976); 40, 83 (1986);
Suppl. 7, 69 (1987)
310
IARC MONOGRAPHS VOLUME 55
Penicillic acid
Pentachloroethane
Pentachloronitrobenzene (see Quintozene)
Pentachlorophenol (see also Chlorophenols; Chlorophenols,
occupational exposures to)
Permethrin
Perylene
Petasitenine
Petasites japonicus (see Pyrrolizidine alkaloids)
Petroleum refming (occupational exposures in)
Some petroleum solvents
Phenacetin
Phenanthrene
Phenazopyridine hydrochloride
Phenelzine sulfate
Phenicarbazide
Phenobarbital
Phenol
Phenoxyacetic acid herbicides (see Chlorophenoxy herbicides)
Phenoxybenzamine hydrochloride
Phenylbutazone
meta-Phenylenediamine
para-Phenylenediamine
Phenyl glycidyl ether (see Glycidyl ethers)
N-Phenyl-2-naphthylamine
ortho-Phenylphenol
Phenytoin
Picloram
Piperazine oestrone sulfate (see Conjugated oestrogens)
Piperonyl butoxide
Pitches, coal-tar (see Coal-tar pitches)
Polyacrylic acid
Polybrominated biphenyls
Polychlorinated biphenyls
Polychlorinated camphenes (see Toxaphene)
Polychloroprene
Polyethylene
Polymethylene polyphenyl isocyanate
Polymethyl methacrylate
Polyoestradiol phosphate (see Oestradiol-1713)
Polypropylene
Polystyrene
Polytetrafluoroethylene
Polyurethane foams
Polyvinyl acetate
Polyvinyl alcohol
10, 211 (1976); Suppl. 7, 69 (1987)
41, 99 (1986); Suppl. 7, 69 (1987)
20, 303 (1979); 53, 371 (1991)
53, 329 (1991)
32, 411 (1983); Suppl. 7, 69 (1987)
31, 2fJ7 (1983); Suppl. 7, 69 (1987)
45, 39 (1989)
47, 43 (1989)
13, 141 (1977); 24, 135 (1980);
Suppl. 7, 310 (1987)
32, 419 (1983); Suppl. 7, 69 (1987)
8, 117 (1975); 24, 163 (1980) (con 42.
260); Suppl. 7, 312 (1987)
24, 175 (1980); Suppl. 7, 312 (1987)
12, 177 (1976); Suppl. 7, 70 (1987)
13, 157 (1977); Suppl. 7, 313 (1987)
47, 263 (1989) (con 50, 385)
9, 223 (1975); 24, 185 (1980);
Suppl. 7, 70 (1987)
13, 183 (1977); Supp/. 7, 316 (1987)
16, Ill (1978); Suppl. 7, 70 (1987)
16, 125 (1978); Suppl. 7, 70 (1987)
16, 325 (1978) (con 42, 257);
Suppl. 7, 318 (1987)
30, 329 (1983); Suppl. 7, 70 (1987)
13, 2fJ1 (1977); Suppl. 7, 319 (1987)
53, 481 (1991)
30, 183 (1983); Suppl. 7, 70 (1987)
19, 62 (1979); Suppl. 7, 70 (1987)
18. 107 (1978); 41, 261 (1986);
Suppl. 7, 321 (1987)
7, 261 (1974); 18, 43 (1978) (corr. 42,
258); Suppl. 7, 322 (1987)
19, 141 (1979); Suppl. 7, 70 (1987)
19, 164 (1979); Suppl. 7, 70 (1987)
19, 314 (1979); Suppl. 7, 70 (1987)
19, 195 (1979); Suppl. 7, 70 (1987)
19, 218 (1979); Suppl. 7, 70 (1987)
19, 245 (1979); Suppl. 7, 70 (1987)
19, 288 (1979); Suppl. 7, 70 (1987)
19, 320 (1979); Suppl. 7, 70 (1987)
19, 346 (1979); Suppl. 7, 70 (1987)
19, 351 (1979); SuppL 7, 70 (1987)
Polyvinyl chloride
Polyvinyl pyrrolidone
Ponceau MX
Ponceau 3R
Ponceau SX
CUMULATIVE CROSS INDEX
Potassium arsenate (see Arsenic and arsenic compounds)
Potassium arsenite (see Arsenic and arsenic compounds)
Potassium bis(2-hydroxyethyl)dithiocarbamate
Potassium bromate
Potassium chromate (see Chromium and chromium compounds)
Potassium dichromate (see Chromium and chromium compounds)
Prednimustine
Prednisone
Procarbazine hydrochloride
Proflavine salts
Progesterone (see also Progestins; Combined oral contraceptives)
Progestins (see also Oestrogens, progestins and combinations)
Pronetalol hydrochloride
1,3-Propane sultone
Propham
n-Propyl carbamate
Propylene
Propylene oxide
Propylthiouracil
Ptaquiloside (see also Bracken fern)
Pulp and paper manufacture
Pyrene
Pyrido(3,4-c ]psoralen
Pyrimethamine
Pyrrolizidine alkaloids (see Hydroxysenkirkine; Isatidine; Jacobine;
Lasiocarpine; Monocrotaline; Retrorsine; Riddelliine; Seneciphylline;
Senkirkine)
Q
Quercetin (see also Bracken fern)
para-Quinone
Quintozene
R
Radon
Reserpine
Resorcinol
311
7, 306 (1974); 19,402 (1979); Suppl. 7,
70 (1987)
19, 463 (1979); Suppl. 7, 70 (1987)
8, 189 (1975); Suppl. 7, 70 (1987)
8, 199 (1975); Suppl. 7, 70 (1987)
8, 207 (1975); Suppl. 7, 70 (1987)
12, 183 (1976); Suppl. 7, 70 (1987)
40, 207 (1986); Suppl. 7, 70 (1987)
50, 115 (1990)
26, 293 (1981); Suppl. 7, 326 (1987)
26, 311 {1981); Suppl. 7, 327 (1987)
24, 195 (1980); Suppl. 7, 70 (1987)
6, 135 (1974); 21, 491 (1979) (con: 42,
259)
Suppl. 7, 289 (1987)
13, 227 (1977) (corr. 42, 256); Suppl. 7,
70 (1987)
4, 253 (1974) (corr. 42, 253); Suppl. 7,
70 (1987)
12, 189 (1976); Supp/. 7, 70 (1987)
4, 259 (1974) (con: 42, 253); Suppl. 7,
70 (1987)
12, 201 (1976); Suppl. 7, 70 (1987)
19, 213 (1979); Suppl. 7, 71 (1987)
11, 191 (1976); 36, 227 (1985)
(corr. 42, 263); Suppl. 7, 328 (1987)
7, 67 (1974); Suppl. 7, 329 (1987)
40, 55 (1986); Suppl. 7, 71 (1987)
25, 157 (1981); Suppl. 7, 385 (1987)
32, 431 (1983); Suppl. 7, 71 (1987)
40, 349 (1986); Suppl. 7, 71 (1987)
13, 233 (1977); Suppl. 7, 71 (1987)
31, 213 (1983); Suppl. 7, 71 (1987)
15, 255 (1977); Suppi. 7, 71 (1987)
5, 211 (1974); Suppi. 7, 71 (1987)
43, 173 (1988) (con: 45, 283)
10, 217 (1976); 24, 211 (1980)
(con: 42, 260); Suppl. 7, 330 (1987)
15, 155 (lm); Suppl. 7, 71 (1987)
312 IARC MONOGRAPHS VOLUME 55
Retrorsine
Rhodamine B
Rhodamine 6G
Riddelliine
Rifampicin
Rockwool (see Man-made mineral fibres)
The rubber industry
Rugulosin
s
Saccharated iron oxide
Saccharin
Safrole
The sawmill industry (including logging) [see The lumber and
sawmill industry (including logging)]
Scarlet Red
Selenium and selenium compounds
Selenium dioxide (see Selenium and selenium compounds)
Selenium oxide (see Selenium and selenium compounds)
Semicarbazide hydrochloride
~ c i o jacobaea L (see Pyrrolizidine alkaloids)
Senecio longilobus (see Pyrrolizidine alkaloids)
Seneciphylline
Senkirkine
Sepiolite
Sequential oral contraceptives (see also Oestrogens, progestins
and combinations)
Shale-oils
Shikimic acid (see also Bracken fern)
Shoe manufacture and repair (see Boot and shoe manufacture
and repair)
Silica (see also Amorphous silica; Crystalline silica)
Simazine
Sl.agwool (see Man-made mineral fibres)
Sodium arsenate (see Arsenic and arsenic compounds)
Sodium arsenite (see Arsenic and arsenic compounds)
Sodium cacodylate (see Arsenic and arsenic compounds)
Sodium chlorite
Sodium chromate (see Chromium and chromium compounds)
Sodium cyclamate (see Cyclamates)
Sodium dichromate (see Chromium and chrolllium compounds)
Sodium diethyldithiocarbarnate
Sodium equilin sulfate (see Conjugated oestrogens)
Sodium fluoride (see Fluorides)
10, 303 (1976); Suppl. 7, 71 (1987)
16, 221 (1978); Suppl. 7, 71 (1987)
16, 233 (1978); Suppl. 7, 71 (1987)
10, 313 (1976); Suppl. 7, 71 (1987)
24, 243 (1980); Suppl. 7, 71 (1987)
28 (1982) (con: 42, 261); Suppl. 7,
332 (1987)
40, 99 (1986); Suppl. 7, 71 (1987)
2, 161 (1973); Suppl. 7, 71 (1987)
22, 111 (1980)(con: 42, 259);
Suppl. 7, 334 (1987)
1, 169 (1972); 10, 231 (1976);
SuppL 7, 71 (1987)
8, 217 (1975); SuppL 7, 71 (1987)
9, 245 (1975) (corr. 42, 255);
Suppl. 7, 71 (1987)
12, 209 (1976) (corr. 42, 256);
Suppl. 7, 71 (1987)
10, 319, 335 (1976); Suppl. 7, 71
(1987)
10, 327 (1976); 31' 231 (1983);
Suppl. 7, 71 (1987)
42, 175 (1987); Suppl. 7, 71 (1987)
Suppl. 7, 296 (1987)
35, 161 (1985); Suppl. 7, 339 (1987)
40, 55 (1986); Suppl. 7, 71 (1987)
42, 39 (1987)
53, 495 (1991)
52, 145 (1991)
12, 217 (1976); Suppl. 7, 71 (1987)
CUMULATIVE CROSS INDEX
313
Sodium monofluorophosphate (see Fluorides)
Sodium oestrone sulfate (see Conjugated oestrogens)
Sodium ortho-phenylphenate (see also ortho-Phenylphenol)
Sodium saccharin (see Saccharin)
Sodium selenate (see Selenium and selenium compounds)
Sodium selenite (see Selenium and selenium compounds)
Sodium silicofluoride (see Fluorides)
Solar radiation
Soots
Spironolactone
Stannous fluoride (see Fluorides)
Steel founding (see Iron and steel founding)
Sterigmatocystin
Steroidal oestrogens (see also Oestrogens, progestins and
combinations)
Streptozotodn
Strobane (see Terpene polychlorinates)
Strontium chromate (see Chromium and chromium compounds}
Styrene
Styrene-acrylonitrile copolymers
Styrene-butadiene copolymers
Styrene oxide
30, 329 (1983); Suppl. 7, 392 (1987)
55 (1992)
3, 22 (1973); 35, 219 (1985); Suppl. 7,
343 (1987)
24, 259 (1980); Suppl. 7, 344 (1987)
1, 175 ( 1972); 10, 245 (1976); Suppl. 7,
72 (1987)
Suppl. 7, 280 (1987)
4, 221 (1974); 17, 337 (1978);
Suppl. 7, 72 (1987)
19, 231 (1979} (con: 42, 258);
Suppl. 7, 345 (1987)
19, 97 (1979); Suppl. 7, 72 (1987)
19, 252 (1979); Suppl. 7, 72 (1987)
11 t 201 (1976); 19, 275 (1979); 36, 245
(1985); Suppl. 7, 72 (1987)
Succinic anhydride 15, 265 (lm); Suppl. 7, 72 (1987)
Sudan I 8, 225 (1975); Suppl. 7, 72 (1987)
Sudan II 8, 233 (1975); Suppl. 7, 72 (1987)
Sudan Ill 8, 241 (1975); Suppl. 7, 72 (1987)
Sudan Brown RR 8, 249 (1975); Suppl. 7, 72 (1987)
Sudan Red 7B 8, 253 (1975); Suppl. 7, 72 (1987)
Sulfafurazole 24, 215 (1980); Suppl. 7, 347 (1987)
Sulfallate 30, 283 (1983); Suppl. 7, 72 (1987)
Sulfamethoxazole 24, 285 (1980); Suppl. 7, 348 (1987)
Sulfites (see Sulfur dioxide and some sulfites, bisulfites and metabisulfites)
Sulfur dioxide and some sulfites, bisulfites and metabisulfites 54, 131 (1992)
Sulfur mustard (see Mustard gas)
Sulfuric acid and other strong inorganic acids, occupational exposures 54, 41 (1992)
to mists and vapours from
Sulfur trioxide
Sulphisoxazole (see Sulfafurazole)
Sunset Yellow FCF
Symphytine
T
2,4,5-T (see also Chtorophenoxy herbicides; Chlorophenoxy
hetbicides, occupational exposures to)
Thlc
54, 121 (1992)
8, 257 (1975); Suppl. 7, 72 (1987)
31, 239 (1983); Suppl. 7, 72"(1987)
15, 273 (1977)
42, 185 (1987); Suppl. 7, 349 (1987)
314
IARC MONOGRAPHS VOLUME 55
Thnnic acid
'Thnnins (see also 'Thnnic acid)
TCDD (see 2,3,7,8-Thtrachlorodibenzo-para-dioxin)
TDE (see DDT)
Tea
Thrpene polychlorinates
Testosterone (see also Androgenic (anabolic) steroids)
Testosterone oenanthate (see Testosterone)
Testosterone propionate (see Thstosterone)
2,2' ,5,5' -Tetrachlorobenzidine
2,3, 7,8-Thtrachlorodibenzo-para-dioxin
1, 1, 1,2-Thtrachloroethane
1,1,2,2-Thtrachloroethane
Tetrachloroethylene
2,3,4,6-Tetrachlorophenol (see Chlorophenols; Chlorophenols,
occupational exposures to)
Thtrachlorvinphos
Tetraethyllead (see Lead and lead compounds)
Thtrafluoroethylene
Thtrakis(hydroxymethyl) phosphonium salts
Tetramethyllead (see Lead and lead compounds)
Thxtile manufacturing industry, exposures in
Theobromine
Theophylline
Thioacetamide
4,4' -Thiodianiline
Thiotepa
Thiouracil
Thiourea
Thiram
Titanium dioxide
Thbacco habits other than smoking (see Tobacco products,
smokeless)
Tobacco products, smokeless
Thbacco smoke
Tobacco smoking (see Tobacco smoke)
ortho-Tolidine (see 3,3' -Dimethylbenzidine)
2,4-Thluene diisocyanate (see also Thluene diisocyanates)
2,6-Toluene diisocyanate (see also Toluene diisocyanates)
Toluene
Toluene diisocyanates
Thluenes, a-chlorinated (see (X-Chlorinated toluenes)
ortho-Toluenesulfonamide (see Saccharin)
ortho-Thluidine
10, 253 (1976) (coo: 42, 255); Suppl. 7,
72 (1987)
10, 254 (1976); Suppl. 7, 72 (1987)
51, 207 (1991)
5, 219 (1974); Suppl. 7, 72 (1987)
6, 209 (1974); 21, 519 (1979)
27, 141 (1982); Suppl. 7, 72 (1987)
15, 41 (1977); Suppl. 7, 350 (1987)
41, 87 (1986); Suppl. 7, 72 (1987)
20, 477 (1979); Suppl. 7, 354 (1987)
20, 491 (1979); Suppl. 7, 355 (1987)
30, 197 (1983); Suppl. 7, 72 (1987)
19, 285 (1979); Suppl. 7, 72 (1987)
48, 95 (1990)
48, 215 (1990) (con: 51, 483)
51, 421 (1991)
51' 391 (1991)
7, 77 (1974); Suppl. 7, 72 (1987)
16, 343 (1978); 27, 147 (1982);
Suppl. 7, 72 (1987)
9, 85 (1975); Suppl. 7, 368 (1987);
. 50, 123 (1990)
7, 85 (1974); Suppl. 7, 72 (1987)
7, 95 (1974); Suppl. 7, 72 (1987)
12, 225 (1976); Suppl. 7, 72 (1987);
53, 403 (1991)
47, 307 (1989)
37 (1985) (con: 42, 263; 52, 513);
Suppl. 7, 357 (1987)
38 (1986) (con: 42, 263); Suppl. 7,
357 (1987)
19, 303 (1979}; 39, 287 (1986)
19, 303 (1979); 39, 289 (1986)
47, 79 (1989)
39, 287 (1986) (corr. 42, 264);
Suppl. 7, 72 (1987)
16, 349 (1978); 27, 155 (1982);
Suppl. 7, 362 (1987)
CUMULATIVE CROSS INDEX
315
Toxaphene
Tremolite (see Asbestos)
'Iteosulfan
lliaziquone [see Tris(aziridinyl)para-benzoquinone]
Trichlorfon
Thchlormethine
Thchloroacetonitrile (see Halogenated acetonitriles)
1,1,1-Trichloroethane
1,1,2-Thchloroethane
Trichloroethylene
2,4,5-Trichlorophenol (see also Chlorophenols; Chlorophenols
occupational exposures to)
2,4,6-Trichlorophenol (see also Chlorophenols; Chlorophenols,
occupational exposures to)
(2,4,5-Trichlorophenoxy)acetic acid (see 2,4,5-T)
Trichlorotriethylamine hydrochloride (see Trichlormethine)
T 2Trichothecene
Triethylene glycol diglycidyl ether
Trifluralin
4,4' ,6:nimethylangelicin plus ultraviolet radiation (see also
Angelicin and some synthetic derivatives)
2,4,5-Trimethylaniline
2,4,6-liimethylaniline
4,5' ,8-liimethylpsoralen
Trimustine hydrochloride (see Trichlormethine)
Triphenylene
Tris(aziridinyl)-para-benzoquinone
Tris{l-azirid inyl)phosphin e oxide
Tris(1-aziridinyl)phosphine sulphide (see Thiotepa)
2,4,6-Tris(1-aziridinyl)-s-triazine
1tis(2-chloroethyl) phosphate
1,2,3-Tris( chloromethoxy )propane
Tris(2,3-dibromopropy I )phosphate
Tris(2-methyl-1-aziridinyl)phosphine oxide
Trp-P-1
'Itp-P-2
Trypan blue
Tussi/ago farfara L. (see Pyrrolizidine alkaloids)
u
Ultraviolet radiation
Underground haematite mining with exposure to radon
Uracil mustard
Urethane
v
Vat Yellow4
20, 327 (1979); Suppl. 7, 72 (1987)
26, 341 (1981); Suppl. 7, 363 (1987)
30, W1 (1983); Suppl. 7, 73 (1987)
9, 229 (1975); Suppl. 7, 73 (1987);
50, 143 (1990)
20, 515 (1979); Suppl. 7, 73 (1987)
20, 533 (1979); Suppl. 7, 73 (1987);
52, 337 (1991)
11, 263 (1976); 20, 545 (1979);
Suppi. 7, 364 (1987)
20, 349 (1979)
20, 349 (1979)
31, 265 (1983); Supp/. 7, 73 (1987)
11, 209 (1976); Supp/. 7, 73 (1987)
53, 515 (1991)
Suppl. 7, 57 (1987)
27, 177 (1982); Suppl. 7, 73 (1987)
27, 178 (1982); Suppl. 7, 73 (1987)
40, 357 (1986); Suppl. 7, 366 (1987)
32, 447 (1983); Supp/. 7, 73 (1987)
9, 67 (1975); Suppi. 7, 367 (1987)
9, 15 (1975); Suppl. 7, 73 (1987)
9, 95 (1975); Suppl. 7, 73 (1987)
48, 109 (1990)
15, 301 (19n); Supp/. 7, 73 (1987)
20, 575 (1979); Suppl. 7, 369 (1987)
9, 107 (1975); Suppl. 7, 73 (1987)
31, 247 (1983); Suppi. 7, 73 (1987)
31, 255 (1983); Suppl. 7, 73 (1987)
8, 267 (1975); Suppl. 7, 73 (1987)
40, 319 (1986); 55 (1992)
1, 29 {1972); Supp/. 7, 216 (1987)
9, 235 (1975); Suppl. 7, 370 (1987)
7, 111 (1974); Suppl. 7, 73 (1987)
48, 161 (1990)
316
IARC MONOGRAPHS VOLUME 55
Vmblastine sulfate
Vmcristine sulfate
Vinyl acetate
Vmyl bromide
Vmyl chloride
Vmyl chloride-vinyl acetate copolymers
4-Vinylcyclohexene
Vmyl fluoride
Vinylidene chloride
Yinylidene chloride-vinyl chloride copolymers
Yinylidene fluoride
N-Vmyl-2-pyrrolidone
w
Welding
Wollastonite
Wood industries
X
Xylene
2,4-Xylidine
2,5-XyHdine
y
Yellow AB
Yellow OB
z
Zearalenone
Zectran
Zinc becyllium silicate (see Becyllium and becyllium compounds)
Zinc chromate (see Chromium and chromium compounds)
Zinc chromate hydroxide (see Chromium and chromium
compounds)
Zinc potassium chromate (see Chromium and chromium
compounds)
Zinc yellow (see Chromium and chromium compounds)
Zineb
Ziram
26, 349 (1981) (corr. 42, 261);
Suppi. 7, 371 (1987)
26, 365 (1981); Suppl. 7, 372 (1987)
19, 341 (1979); 39, 113 (1986);
Suppl. 7, 73 (1987)
19, 367 (1979); 39, 133 (1986);
Suppl. 7, 73 (1987)
7, 291 (1974); 19, 3n (1979) (corr. 42,
258); Suppi. 7, 373 (1987)
7, 311 (1976); 19, 412 (1979) (corr.
42, 258); Supp/. 7, 73 (1987)
11, 2n (1976); 39, 181 (1986);
Suppl. 7, 73 (1987)
39, 147 (1986); Suppl. 7, 73 (1987)
19, 439 (1979); 39, 195 (1986);
Suppi. 7, 376 (1987)
19, 448 (1979) (corr. 42, 258);
Suppl. 7, 73 (1987)
39, 227 (1986); Suppl. 7, 73 (1987)
19, 461 (1979); Suppl. 7, 73 (1987)
49, 447 (1990) (corr. 52, 513)
42, 145 (1987); Suppl. 7, 3n (1987)
25 (1981); Suppl. 7, 378 (1987)
47, 125 (1989)
16, 367 (1978); Suppl. 7, 74 (1987)
16, 3TI (1978); Suppl. 7, 74 (1987)
8, 279 (1975); Suppi. 7, 74 (1987)
8, 287 (1975); Suppi. 7, 74 (1987)
31, 279 (1983); Suppl. 7, 74 (1987)
12, 237 (1976); Suppl. 7, 74 (1987)
12, 245 (1976); Suppl. 7, 74 (1987)
12, 259 (1976); Suppl. 7, 74 (1987);
53, 423 (1991)
PUBLICATIONS OF THE
INTERNATIONAL AGENCY FOR RESEARCH ON CANCER
Scientific Publications Series
(Available from Oxford University Press through local bookshops)
No. 1 Uver Cancer
1971; 176 pages (out of print)
No. 2 Oncogenesis and
Herpesviruses
Edited by P.M. Biggs, G. de-The and
LN. Payne
1972; 515 pages (out of print)
No. 3 NNitroso Compounds:
Analysis and Fonnation
Edited by P. Bogovski ,
R. Preussman and E.A Walker
1972; 140 pages (out of print)
No. 4 Transplacental Carcinogenesis
Edited by L Tomatis and U. Mohr
1973; 181 pages (out of print)
No. 516 Pathology or 1\lmours in
Laboratory Animals, Volume 1,
1\amours of tbe Rat
Edited by V.S. Thrusov
1973/1976; S33 pages (out of print)
No. 1 Host Environment
Interactions in tbe Etiology of
Cancer in Man
Edited by R. Doll and I. Vodopija
1973; 464 pages (out of print)
No. 8 Biological Effects of Asbestos
Edited by P. Bogovski, J.C. Gilson,
V. Timbrell and J.C. Wagner
1973; 346 pages (out of print)
No. 9 N-Nitroso Compounds in the
Environment
Edited by P. Bogovski and
E.A. Walker
1974; 243 pages (out of print)
No. 10 Chemical Carcinogenesis
Essays
Edited by R. Montesano and
L Tomatis
1974; 230 pages (out of print)
No. 11 Oncogenesis and
Herpesviruses II
Edited by G. de-The, M.A. Epstein
and H. zur Hausen
197S; Part 1: 511 pages
Part II: 403 pages (out of pn'nt)
No. 12 Screenin' Tests In Chemical
Carcinogenesis
Edited by R. Montesano,
H. Bartsch and L Tomatis
1976; 666 pages (out of print)
No. 13 Environmental Pollution and
Carcinogenic Risks
Edited by C. Rosenfeld and
W Davis
197S; 441 pages (out of print)
No. 14 Environmental NNitroso
Compounds. Analysis and Formation
Edited by E.A Walker, P. Bogovski
and L Griciute
1976; 512 pages (out of print)
No. 1S Cancer Incidence in Five
Continents, Volume Ill
Edited by J.A.H. Waterhouse,
C. Muir, P. Correa and J. Powell
1976; 584 pages (out of print)
No. 16 Air Pollution and Cancer in
Man
Edited by U. Mohr, D. Schmahl and
L Tomatis
1977; 328 pages (out of print)
No. 17 Directory of On-going
Research in Cancer Epidemiology
1977
Edited by C.S. Muir and G. Wagner
1977; S99 pages (out of print)
Prices, valid for November 1992, are subject to change without notice
No. 18 Environmeatal Carcinogens.
Selected Methods of Analysis.
Volume 1: Analysis of Volatile
Nitrosamines in Food
Editor-in-Chief: H. Egan
1978; 212 pages (out of print)
No. 19 Environmental Aspects of
NNitroso Compounds
Edited by E.A. Walker,
M. Castegnaro, L Griciute and R.E.
Lyle
1978; S61 pages (out of print)
No. 20 Nasopharyngeal Carcinoma:
Etiology and Control
Edited by G. de-Tile andY. Ito
1978; 606 pages (out of print)
No. 21 Cancer Registration and its
Techniques
Edited by R. MacLennan, C. Muir,
R. Steinitt and A. Winkler
1978; 23S pages (out of print)
No. 22 Environmental Carcinogens.
Selected Methods or Analysis.
Volume 2: Methods for the
Measurement of V"myl Chloride in
Poly(vinyl chloride), Air, Water and
Foodstuffs
Editor-in-Chief: H. Egan
1978; 142 pages (out of print)
No. 23 Pathology of 1\nnours in
Laboratory Animals. Volume II:
Thmours of the Mouse
V.S. Thrusov
1979; 669 pages (out of print)
No. 24 Oncogenesis and
Herpesviruses Ill
Edited by G. de:rhe, W. Henle and
F. Rapp
1978; Part 1: 580 pages, Part II: S12
pages (out of print)
No. 25 Carcinogenic Risk. Strategies
for Intervent.loa
Edited by W. Davis and
C. Rosenfeld
1979; 280 pages (out ofprinl)
No. 26 Directory of On-goi111
Research in Cancer Epidemiolocr
1978
Edited by C.S. Muir and G. Wagner
1978; 550 pages (out ofprinl)
No. 27 Molecular and Cellular
Aspects of Carcinogen Screening
Tests
Edited by R. Montesano,
H. Bartsch and L Tomatis
1980; 372 pages 29.00
No. 28 Directory of On-going
Research in Cancer Epidemiology
1979
Edited by C.S. Muir and G. Wolgner
1979; 672 pages (out of print)
No. 29 En-vironmental Carcinogens.
Selected Methods of Analysis.
Volume 3: Analysis of Polycyclic
Aromatic Hydrocarbons in
Environmental Samples
Editor-in-Chief: H. Egan
1979; 240 pages (out of print)
No. 30 Biological Effects of Mineral
Fibf'es
Editor-in-Chief: J.C. Wagner
1980; Volume 1: 494 pages Volume
2: 513 pages (out of print)
No. 31 N-Nitroso Compounds:
Analysis, Fonnation and Occurrence
Edited by E.A Walker, L Griciute,
M. Castegnaro and M. BOrzs6nyi
1980; 835 pages (out of print)
No. 32 Statistical Methods in
Cancer Research. Volume 1. The
Analysis of Case-control Studies
By N.E. Breslow and N.E. Day
1980; 338 pages 25.00
No. 33 Handli111 Chemical
Carcinogens in tbe Laboratory
Edited by R. Montesano el al.
1979; 32 pages (out of print)
List of IARC Publications
No. 34 Patholocr oi'I\Jmoun In
Laboratory Animals. Volume Ill.
1\Jmours ol the Hamster
Editor-in-Chief: V.S. Thrusov
1982; 461 pages (out of print)
No. 35 Directory ol On-going
Research in Cancel' Epidemiology
1980
Edited by C.S. Muir and G. Wagner
1980; 660 pages (out of print)
No. 36 Cancer Mortality by
Occupation and Social Class
1851-1971
Edited by W.P.D. Logan
1982; 253 pages (out of print)
No. 37 Laboratory Decontamination
and Destruction of Aflatoxins B
1
, B
21
G, G
2
in Laboratory Wastes
Edited by M. Castegnaro et al.
1980; 56 pages (out of print)
No. 38 Directory of On-going
Research in Cancer Epidemiology
1981
Edited by C.S: Muir and G. Wagner
1981; 696 pages (out of print)
No. 39 Host Factors in Human
Carcinogenesis
Edited by H. Bartsch and
B. Armstrong
1982; 583 pages (out of print)
No. 40 Environmental Carcinogens.
Selected Methods of Analysis.
Volume 4: Some Aromatic Amines
and Azo Dyes in the General and
Industrial Environment
Edited by L Fishbein,
M. Castegnaro, I.K. O'Neill and
H. Bartsch
1981; 347 pages(outofprint) .
No. 41 N-Nitroso Compounds:
Occurrence and Biological Effects
Edited by H. Bartsch, I.K. O' Neill,
M. Castegnaro and M. Okada
1982; 755 pages 50.00
No. 42 Cancer Incidence in Five
Continents, Volume IV
Edited by J. Waterhouse, C. Muir,
K. Shanmugaratnam and J. Powell
1982; 811 pages (oul of print)
No. 43 Laboratory Decoataminatioll
and Destructioa of Can:ioogens in
Laboratory Wastes: Some
N-Nitrosamines
Edited by M. Castegnaro tt al.
1982; 73 pages7.50
No. 44 Environmental Cardnogeas.
Selected Methods ol Analysis.
Volume 5: Some Mycotoxina
Edited by L Stoloff, M. Castegnaro,
P. Scott, I.K. O'Neill and H. Bartsch
1983; 455 pages 32.50
No. 45 Environmental Carcinogens.
Selected Methods ol Analysis.
Volume 6: N-Nitroso Compounds
Edited by R. Preussmann, l.K.
O'Neill, G. Eisenbrand, B.
Spiegelhalder and H. Bartsch
1983; 508 pages 32.50
No. 46 Directory of On-going
Research in Cancer Epidemiology
1982
Edited by C.S. Muir and G. W..gner
1982; 722 pages (out of print)
No. 47 Cancer Incidence in
Singapore 1968-1977
Edited by K. Shanmugaratnam,
H.P. Lee and N.E. Day
1983; 171 pages (out of print)
No. 48 Cancer Incidence in the
USSR (2nd Revised Edition)
Edited by N.P. Napalkov,
G.F. 1Serkovny, V.M. Merabishvili,
D.M. Parkin, M. Smans and
C.S. Muir
1983; 75 pages (out of print)
No. 49 Laboratory Decontamination
and Destruction of Carcinogens in
Laboratory Wastes: Some Polycyclic
Aromatic Hydrocarboos
Edited by M. Castegnaro et al.
1983; 87 pages (out of print)
No. SO Directory of On-going
Research in Cancer Epidemiology
1983
Edited by C.S. Muir and G. W..gner
1983; 731 pages (out of print)
No. 51 Modulators of Elo:perimental
Carcinogenesis
Edited by V. Thrusov and R.
Montesano
1983; 307 pages (out of print)
List of /ARC Publications
No. 52 Second Caocers ia Relation
to Radiation '&eatmeut for Cervical
Cancer: ~ t s of a Cancer Registry
Collaboration
Edited by N.E. Day and J.C. Boice,
Jr
1984; 207 pages (out of print)
No. 53 Nickel in the Human
Environment
Editor-in-Chief: F.W. Sunderman, Jr
1984; 529 pages (out of print)
No. 54 Laboratory Decontamination
and Destruction of Carcinogens in
Laboratory Wastes: Some
Hydrazines
Edited by M. Castegnaro et al.
1983; 87 pages (out of print)
No. 55 Laboratory Decontamination
and Destruction of Carcinogens in
Laboratory Wastes: Some
N-Nitrosamides
Edited by M. Castegnaro et al.
1984; 66 pages (out of print)
No. 56 Models, Mechanisms and
Etiology of Tumour Promotion
Edited by M. BOIZS6nyi, N.E. Day,
K. Lapis and H. Yamasaki
1984; 532 pages (out of print)
No. 57 N-Nitroso Compounds:
Occurrence, Biological Effects and
Relevance to Human Cancer
Edited by l.K. O'Neill, R.C. von
Borstel, C.T. Miller, J. Long and
H. Bartsch
1984; 1013 pages (out of print)
No. 58 Age-related Factors in
Carcinogenesis
Edited by A likhachev,
V. Anisimov and R. Montesano
1985; 288 pages (out of print)
No. 59 Monitoring Human
Exposure to Carcinogenic and
Mutagenic Agents
Edited by A Berlin, M. Draper,
K. Hemminki and H. Vainio
1984; 457 pages (out of print)
No. 60 Burkitt's Lymphoma: A
Human Cancer Model
Edited by G. Lenoir, G. O'Conor
and C.I...M. Olweny
1985; 484 pages (out of print)
No. 61 Laboratory Decontamination
and Destruction of Carcinogens in
Laboratory Wastes: Some
Haloethers
Edited by M. Castegnaro et al.
1985; 55 pages {out of print)
No. 62 Directory of On-going
Research in Cancer Epidemiology
1984
Edited by C.S. Muir and G. Wagner
1984; 717 pages (out of print)
No. 63 Virus-associated Cancers In
Africa
Edited by A.O. Williams,
G.T. O'Conor, G.B. de-The and C.A.
Johnson
1984; 773 pages (out of print)
No. 64 Laboratory Decontamination
and Destruction of Carcinogens in
Laboratory Wastes: Some Aromatic
Anlines and 4-Nitrobiphenyl
Edited by M. Castegnaro et al.
1985; 84 pages (out of print)
No. 65 Interpretation of Negative
Epidemiological Evidence for
Carcinogenicity
Edited by N.J. Wald and R. Doll
1985; 232 pages (out of print)
No. 66 The Role of the Registry in
Cancer Control
Edited by D.M. Parkin, G. Wagner
and C.S. Muir
1985; 152 pages 10.00
No. 67 'lransformation Assay of
Established Cell Unes: Mechanisms
and Application
Edited by T. Kakunaga and
H. Yamasaki
1985; 225 pages (out of print)
No. 68 Environmental Carclnor;ens.
Selected Metbods of Analysis.
Volume 7. Some Volatile
Halogenated Hydrocarbons
Edited by I.. Fishbein and
I.K. O'Neill
1985; 479 pages (out of print)
No. 69 Directory of On-&Qin&
Research in Cancer Epidemiology
1985
Edited by C.S. Muir and G. Wagner
1985; 7 45 pages (out of print)
No. 70 The Role of Cyclic Nucleic
Acid Adducts in Carcinogenesis and
Mutagenesis
Edited by B. Singer and H. Bartsch
1986; 467 pages (out of print)
No. 71 Environmental Carcinogens.
Selected Methods of Analysis.
Volume 8: Some Metals: As, Be, Cd,
Cr, Ni, Pb, Se Zn
Edited by I.K. O'Neill, P. Schuller
and I.. Fishbein
1986; 485 pages (out of print)
No. 72 Atlas of Cancer in Scodand,
1975-1980. Incidence 'and
Epidemiological Perspective
Edited by I. Kemp, P. Boyle,
M. Smans and C.S. Muir
1985; 285 pages (out of print)
No. 73 Laboratory Decontamination
and Destruction of Carcinogens in
Laboratory Wastes: Some
Antineoplastic Agents
Edited by M. Castegnaro et al.
1985; 163 pages 12.50
No. 74 Tobacco: A Major
International Healtb Hazard
Edited by D. Zaridze and R. Peto
1986; 324 pages 22.50
No. 75 Cancer Occurrence in
Developing Countries
Edited by D.M. Parkin
1986; 339 pages 22.50
No. 76 Screening for Cancer of the
Uterine Cervix
Edited by M. Hakama, A.B. Miller
and N.E. Day
1986; 315 pages 30.00
No. 77 Hexachlorobenzene:
Proceedings of an International
Symposium
Edited by C.R. Morris and
J.R.P. Cabral
1986; 668 pages (out of print)
No. 78 Can:inogeoicity of Alkylating
Cytostatic Drugs
Edited by D. Schmahl and
J.M. Kaldor
1986; 337 pages (out of print)
No. 79 Statistical Methods in
Cancer Research. Volume Ill: The
Design and Analysis or Long-term
Animal Experiments
By J.J. Gart, D. Krewski, P.N. Lee,
R.E. 'Throne and J. Wahrendorf
1986; 213 pages 22.00
No. 80 Directory of On-going
Research in Cancer Epidemiology
1986
Edited by C.S. Muir and G. Wagner
1986; 805 pages (out of print)
No. 81 Environmental Carcinogens:
Methods or Analysis and Exposure
Measurement. Volume 9: Passive
Smokinc
Edited by I.K. O'Neill,
K.D. Brunnemann, B. Dodet and D.
Hoffmann
1987; 383 pages 35.00
No. 82 Statistical Methods in
Cancer Resean:h. Volume II: The
Design and Analysis of Cohort
Studies
By N.E. Breslow and N.E. Day
1987; 404 pages 35.00
No. 83 Lone-term and Short-term
Assays for Carcinogens: A Critical
Appraisal
Edited by R. Montesano,
H. Bartsch, H. Vainio, J. Wilbourn
and H. Yamasaki
1986; 575 pages35.00
No. 84 Tbe Relevance oCN-Nitroso
Compounds to Humaa Cancer:
Exposure and Mechanisms
Edited by H. Bartsch, I.K. O'Neill
and R. Schulte- Hermann
1987; 671 pages (out ofprinl)
List of !ARC Publications
No. 85 Environmental Can:inogens:
Methods or Analysis and Exposure
Measurement. Volume 1 0: Benzene
and J k y l a ~ Benzenes
Edited by L. Fishbein and
I.K. O' Neill
1988; 327 pages 40.00
No. 86 Direetory or On-going
Research in Cancer Epidemiology
1987
Edited by D.M. Parkin and
J. Wahrendorf
1987; 6 76 pages (out of print)
No. 87 International Incidence or
Childhood Cancer
Edited by D.M. Parkin, C.A. Stiller,
C.A. Bieber, G.J. Draper,
B. Terracini and J.L Young
1988; 401 pages 35.00
No. 88 Cancer Incidence in Five
Continents Volume V
Edited by C. Muir, J. Waterhouse, T.
Mack, J. Powell and S. Whelan
1987; 1004 pages 55.00
No. 89 Method for Detecting DNA
Damaging Agents in Humans:
Applications in Cancer Epidemiology
and Prevention
Edited by H. Bartsch, K. Hemminki
and I.K. O'Neill
1988; 518 pages 50.00
No. 90 Non-occupational Exposure
to Mineral Fibres
Edited by J. Bignon, J. Peto and
R. Saracci
1989; 500 pages 50.00
No. 91 Trends in Cancer Incidence
in Singapore 1968-1981
Edited by H.P. Lee , N.E. Day and
K. Shanmugaratnam
1988; 160 pages (out of print)
No. 92 Cell Differentiatioa, Genes
and Cancer
Edited by 'I Kakunaga,
'I Sugimura, L. Tomatis and
H. Yamasaki
1988; 204 pages 27.50
No. 93 Directory or Oo-coinc
Resean:b in Cancer Epidemiology
1988
Edited by M. Coleman and
J. Wahrendorf
1988; 662 pages (out of print)
No. 94 Human Papillomavirus and
Cervical Cancer
Edited by N. Muiioz, F.X. Bosch and
O.M. Jensen
1989; 154 pages 22.50
No. 95 Cancer Registration:
Principles and Methods
Edited by O.M. Jensen,
D.M. Parkin, R. MacLennan,
C.S. Muir and R. Skeet
1991; 288 pages 28.00
No. 96 Perinatal and
Multigeneration Can:lnogenesis
Edited by N.P. Napalkov,
J.M. Rice, L. Thmatis and
H. Yamasaki
1989; 436 pages 50.00
No. 97 Occupational Exposure to
Silica and Cancer Risk
Edited by L Simonato,
A.C. Fletcher, R. Saracci and
'I Thomas
1990; 124 pages 22.50
No. 98 Cancer Incidence in Jewish
Migrants to Israel, 1961-1981
Edited by R. Steinitz, D.M. Parkin,
J.L. Young, C.A. Bieber and
L Katz
1989; 320 pages 35.00
No. 99 Pathology of'IUmours i
Laboratory Animals, Second
Edition, Volume 1, 'IUmours of the
Rat
Edited by V.S. Thrusov and
U. Mohr
740 pages 85.00
No. 100 Cancer: Causes,
OccuiTedce and Control
Editor-in-Chief L. Tomatis
1990; 352 pages 24.00
No. 101 Directory of On-goinc
Researdl in Cancer Epidemioloey
1989/90
Edited by M. Coleman and
J. w.threndorf
1989; 818 pages 36.00
List of IARC Publications
No. 102 Patterns or Cancer in Five
Continents
Edited by S.L Whelan and
D.M. Parkin
1990; 162 pages 25.00
No. 103 Evaluating Effectiveness of
Primary Prevention or Cancer
Edited by M. Hakama, V. Beral, J.W.
Cullen and D.M. Parkin
1990; 250 pages 32.00
No. 104 Complex MD:tures and
Cancer Risk
Edited by H. Vainio, M. Sorsa and
A.J. McMichael
1990; 442 pages 38.00
No. lOS Relevance to Human
Cancer or N-Nitroso Compounds,
Tobacco Smoke and Mycotoxins
Edited by I.K. O'Neill, J. Chen and
H. Bartsch
1991; 614 pages 70.00
No. 1 06 Atlas of Cancer Incidence
in the Fonner Gennan Democratic
Republic Edited by W.H. Mehnert,
M. Smans, C.S. Muir, M. Mohner &
D. Schon
1992; 384 pages 55.00
No. 107 Atlas of Cancer Mortality
in the European Economic
Community
Edited by M. Smans, C.S. Muir and
P. Boyle
Publ. due 1992; 280 pages 35.00
No. 108 Environmental
Carcinogens: Methods or Analysis
aod Exposure Measurement. Volume
11: Polychlorinated Dioxins and
Dibenzolurans
Edited by C. Rappe, H.R. Buser,
B. Dodet and I.K. O'Neill
1991; 426 pages 45.00
No. 109 Environmental
Can:lnogeu: Methods of Analysis
and Exposure Measurement. Volume
12: Indoor Air Contaminants
Edi'ted by B. Seifert, B. Dodet and
I.K. O'NeiU
Publ. due 1992; approx. 400 pages
No. 110 Directory or On-goiJll
Research in Cancer Epidemiology
1991
Edited by M. Coleman and
1. Wahrendorl
1991; 753 pages 38.00
No. 111 Pathology of Thmours in
Laboratory Animals, Second
Edition, Volume 2, Thmours of the
Mouse
Edited by V.S. Thrusov and
U. Mohr
Publ. due 1993; approx. 500 pages
No. 112 Autopsy in Epidemiology
and Medical Research
Edited by E. Riboli and M. Delendi
1991; 288 pages 25.00
No. 113 Laboratory
Decontamination and Destruction of
Carcinogens in Laboratory Wastes:
Some Mycotoxins
Edited by M. Castegnaro, 1. Barek,
1.- M. Fremy, M. Lafontaine,
M. Miraglia, E. B. Sansone and
G.M. Telling
1991; 64 pages 11.00
No. 114 Laboratory
Decontamination and Destruction of
Carcinogens in Laboratory Wastes:
Some Polycyclic Heterocyclic
Hydrocarbons
Edited by M. Castegnaro, J. Barek,
1. Jacob, U. Kirso, M. Lafontaine,
E.B. Sansone, G.M. Telling and
T. Vu Due
1991; 50 pages 8.00
No. 115 Mycotoxins, Endemic
Nephropathy and Urinary 1ract
'IUmours
Edited by M. Castegnaro, R.
Plestina, G. Dirheimer, I.N.
Chernozemsky and H Bartsch
1991; 340 pages 45.00
No. 116 Mechanisms ol
Can:inogenesls In Risk ldentir.cation
Edited by H. Vainio, P.N. Magee,
D.B. McGregor & A.J. McMichael
1992; 616 pages 65.00
No. 117 Directory of On-going
Research in Cancer Epidemiology
1991
Edited by M. Coleman,
J. Wahrendorl & E. Demaret
1992; 773 pages 42.00
No. 118 Cadmium in tbe Human
Environment: Toxicity aod
Carcinogenicity
Edited by G.F. Nordberg, R.F.M.
Herber & L Alessio
Publ. due 1992; approx. 450 pages
No. 119 The Epidemiology of
Cervical Cancer and Human
Papillomavirus
Edited by N. Munoz, F.X. Bosch,
K. V. Shah & A. Meheus
1992; 288 pages 28.00
No. 120 Cancer Incidence in Five
Continents, Volume VI
Edited by D.M. Parkin, C.S. Muir,
S.L Whelan, Y.T. Gao, J. Ferlay &
1.Powell
1992; 1050 pages 120.00
No. 122 International Classification
of Rodent 1\amoun. Part 1. The Rat
Editor-in-Chief: U. Mohr
1992/93, 10 fascicles, approx. 600
pages, .120.00
List of /ARC Publications
IARC MONOGRAPHS ON THE EVALUATION OF
CARCINOGENIC RISKS TO HUMANS
(Available from booksellers through the network of WHO Sales Agents)
Volume 1 Some Inorganic Volume 12 Some Carbamat.es, Volume 25 Wood, Leather and Some
Substances, Chlorinated Thiocarbamates and Carbaz.ides Associated Industries
Hydrocarbons, Aromatic: Amines, 1976; 282 pages Sw. fr. 34.- 1981; 412 pages Sw. fr. 60
N-Nitroso Compounds, and Natural
Volume 13 Some Miscellaneous Volume 26 Some Aotineoplastk and
Products
1972; 184 pages (out of print)
Pharmaceutical Substances lmmunosuppressi\'e Agents
1977; 255 pages Sw. fr. 30. 1981; 411 pages Sw. fr. 62.
Volume 2 Some Inorganic and
Volume 14 Asbestos Volume 27 Some Aromatic Amines,
Organometallic Compounds
1977; 106 pages (out of print) Aothraquinones and Nitroso
1973; 181 pages (out of print)
Compounds, and Inorganic
Volume 15 Some Fumigants, The
Fluorides Used in Drinking Water
Volume 3 Certain Polycyclic
Herbicides 2,4-D and
and Dental Preparations
Aromatic Hydrocarbons and
Chlorinated Dibenwdioxins and
Heterocyclic Compounds
Miscellaneous Industrial Chemicals
1982; 341 pages Sw. fr. 40.
1973; 271 pages (out of print)
1977; 354 pages Sw. fr. 50. Volume 28 The Rubber Industry
Volume 4 Some Aromatic Amines, Volume 16 Some Aromatic Amines
1982; 486 pages Sw. fr. 70.
Hydraz.ine and Related Substances, and Related Nitro Compounds - Volume 29 Some Industrial
N-Nitroso Compounds and Hair Dyes, Colouring Agents and
Chemicals and Dyestuffs
Miscellaneous Alkylating Agents Miscellaneous Industrial Chemicals 1982; 416 pages Sw. fr. 60.
1974; 286 pages Sw. fr. 18. 1978; 400 pages Sw. fr. 50.
Volume 30 Miscellaneous Pesticides
Volume 5 Some Organochlorine
Volume 17 Some N-Nitroso 1983; 424 pages Sw. fr. 60.
Pesticides
Compounds
Volume 31 Some Food Additives,
1974; 241 pages (out of print)
1978; 365 pages Sw. fr. 50.
Feed Additives and Naturally
Volume 6 Sex Honnones
Volume 18 Polychlorinated
Occurring Substances
1974; 243 pages (oul of print)
Biphenyls and Polybrominated
1983; 314 pages Sw. fr. 60
Biphenyls
Volume 7 Some Anti-Thyroid and
1978; 140 pages Sw. fr. 20.
Volume 32 Polynuclear Aromatk
Compounds, Part I: Chemical,
Related Substances, Nitrofurans and
Volume 19 Some Monomers,
En\'ironmental and Experimental
Industrial Chemicals
Plastics and Synthetic Elastomers,
Data
1974; 326 pages (out of print)
and Acrolein
1983; 477 pages Sw. fr. 60.
Volume 8 Some Aromatic Az.o
1979; 513 pages (out of print)
Volume 33 Polynuclear Aromatic
Compounds Volume 20 Some Halogenated
Compounds, Part 2: Carbon Blacks,
1975; 357 pages Sw. fr. 36. Hydrocarbons
Mineral Oils and Some Nitroarenes
Volume 9 Some Az.iridines, N-, S-
1979; 609 pages (out of print)
1984; 245 pages Sw. fr. 50.
and 0-Mustards and Selenium
Volume 21 Sex Hormones (II)
Volume 34 Polynuclear Aromatic
1975; 268 pages Sw.fr. 27.
1979; 583 pages Sw. fr. 60.
Compounds, Part 3: Industrial
Volume 10 Some Naturally
Volume 22 Some NonNutriti\'e
Exposures in Aluminium
Sweetening Agents
Production, Coal Coke
Occuning Substances
1980; 208 pages Sw. fr. 25.
Production, and Iron and Sceel
1976; 353 pages (out of print)
Founding
Volume 11 Cadmium, Nickel, Some
Volume 23 Some Metals and 1984; 219 pages Sw. fr. 48.
Metallic Compounds
Epoxides, Miscellaneous Industrial
1980; 438 pages (out of print)
Volume 35 Polynuclear Aromatic:
Chemicals and General Compounds, Part -4: Bitumens,
Considerations on Volatile Volume 24 Some Pharmaceutical Coal-tan and Deri"ed Products,
Anaesthetics Drup Shale-oils aad Soots
1976; 306 pages (oul of print) 1980; 337 pages Sw. fr. 40. 1985; 271 pages Sw. fr. 70.
I
I
I
I
I
I
I
Volume 36 Allyl Compounds,
Aldehydes, Epoxides and Peroxjdes
1985; 369 pages Sw. fr. 70.
Volume 37 Tobacco Habits Other
than Smoking: Betel-quid and
Areca-nut Chewing; and some
Related Nitrosamines
1985; 291 pages Sw. fr. 70.
Volume 38 Tobacco Smoking
1986; 421 pages Sw. fr. 75.
Volume 39 Some Chemicals Used In
Plastics and Elastomers
1986; 403 pages Sw. fr. 60.
Volume 40 Some Naturally
Occurring and Synthetic Food
Components, Furocoumarins and
Ultraviolet Radiation
1986; 444 pages Sw. fr. 65.
Volume 41 Some Halogenated
Hydrocarbons and Pesticide
Exposures
1986; 434 pages Sw. fr. 65.
Volume 42 Silica and Some Silicates
1987; 289 pages Sw. fr. 65.
Volume 43 Man-Made Mineral
Fibres and Radon
1988; 300 pages Sw. fr. 65.
Volume 44 Alcohol Drinking
1988; 416 pages Sw. fr. 65.
Volume 45 Occupational Exposures
in Petroleum Relining; Crude Oil
and Major Petroleum Fuels
1989; 322 pages Sw. fr. 65.
Volume 46 Diesel and Gasoline
Engine Exhausts and Some
Nitroarenes
1989; 458 pages Sw. fr. 65.
Volume 47 Some Organic Solvents,
Resin Monomers and Related
Compounds, Pigments and
Occupational Exposures in Paint
Manufacture and Painting
1989; 536 pages Sw. fr. 85.
Volume 48 Some Flame Retardants
and Textile Chemicals, and
Expos.ures in the Textile
Manufacturing Industry
1990; 345 pages Sw. fr. 65.
List of /ARC Publications
Volume 49 Chromium, Nickel and
Welding
1990; 677 pages Sw. fr. 95.-
Volume 50 Phannaceutit:al Drugs
1990; 415 pages Sw. fr. 65.-
Volume 51 Coffee, Tea, Mate,
Methylxanthines and
1991; 513 pages Sw. fr. 80.-
Volume 52 Chlorinated
Drinking-water; Chlorination
By-products; Some Other
Halogenated Compounds; Cobalt
and Cobalt Compounds
1991; 544 pages Sw. fr. 80.-
Volume 53 Occupational Exposures
in Insecticide Application and some
Pesticides
1991; 612 pages Sw. fr. 95.-
Volume 54 Occupational Exposures
to Mists and Vapours from Strong
Inorganic Acids; and Other
Industrial Chemicals
1992; 336 pages Sw. fr. 65.-
Volume 55 Solar and Ultraviolet
Radiation
1992; 316 pages Sw. fr. 65.-
Supplement No. 1
Chemicals and Industrial Processes
Associated with Cancer in Humans
(IARC Monographs, Volumes I to
20)
1979; 71 pages (out of prim)
Supplement No. 2
Long-term and Short-term Screening
Assays for Carcinogens: A Critical
Appraisal
1980; 426 pages Sw. fr. 40.-
Supplement No. 3
Cross Index or Synonyms and 'frade
Names in Volumes I to 26
1982; 199 pages (out of print)
Supplement No. 4
Chemicals, Industrial Processes and
Industries Associated with Cancer in
Humans (IARC Monographs,
Volumes 1 to 29)
1982; 292 pages (out of print)
Supplement No.5
Cross Index of Synonyms and 'frade
Names in Volumes l to 36
1985; 259 pages (out of print)
Supplement No. 6
Genetic and Related Effects: An
Updating of Selected IARC
Monographs from Volumes I to 42
1987; 729 pages Sw. fr. 80.-
Supplement No. 7
Overall Evaluations of
Carcinogenicity: An Updating of
IARC Monographs Volumes 1-42
1987; 440 pages Sw. fr. 65.-
Supplement No. 8
Cross Index of Synonyms and 1rade
Names in Volumes l w 46
1990; 346 pages Sw. fr. 60.-
IARC TECHNICAL
REPORTS*
No. 1 Cancer in Costa Rica
Edited by R. Sierra,
R. Barrantes, G. Munoz Leiva, D.M.
Parkin, C.A Bieber and
N. Muiioz Calero
1988; 124 pages Sw. fr. 30.-
No. 2 SEARCH: A Computer
Package to Assist the Statistical
Analysis of ~ o n t r o l Studies
Edited by G.J. Macfarlane,
P. Boyle and P. Maisonneuve
1991; 80 pages (out of print)
No. 3 Cancer Registration in the
European Economic Community
Edited by M.P. Coleman and
E. Demaret
1988; 188 pages Sw. fr. 30.-
No. 4 Diet, Hormones and Cancer:
Methodological Issues for
Prospective Studies
Edited by E. Riboli and
R. Saracci
1988; 156 pages Sw. fr. 30.-
No. 5 Cancer in the Philippines
Edited by AV. Laudico,
D. Esteban and D.M. Parkin
1989; 186 pages Sw. fr. 30.-
No. 6 La genese du Centre
International de Recherche sur le
Cancer
Par R. Sohier etA G.B. Sutherland
1990; 104 pages Sw. fr. 30.-
No. 7 Epidemiologie du cancer dans
les pays de langue latine
1990; 310 pages Sw. fr. 30.-
No. 8 Comparative Study or Anti-
smoking Legislation in Countries or
the European Economic Community
Edited by A. Sasco, P. Dalla Vorgia
and P. Van der Elst
1990; 82 pages Sw. fr. 30.-
No. 9 Epidemiologie du cancer dans
les pays de langue latine
1991; 346 pages Sw. fr. 30.-
List of !ARC Publications
No. 11 Nitroso Compounds:
Biological Mechanisms, Exposures
and Cancer Etiology
Edited by I.K. O'Neill & H. Bartsch
1992; 149 pages Sw. fr. 30.-
No. 12 Epidemiologie du cancer
dans les pays de langue latine
1992; 375 pages Sw. fr. 30.-
DIRECTORY OF AGENTS
BEING TESTED FOR
CARCINOGENICITY (Until
Vol. 13 Information Bulletin on
the Survey of Chemicals Being
Tested for Carcinogenicity)
No.8 Edited by M.-J. Ghess,
H. Bartsch and L Tomatis
1979; 604 pages Sw. fr. 40.-
No. 9 Edited by M.-J. Ghess,
J.D. Wilbourn, H. Bartsch and
L Tomatis
1981; 294 pagesSw. fr. 41.-
No. 10 Edited by M.-J. Ghess,
J.D. Wilbourn and H. Bartsch
1982; 362 pages Sw. fr. 42.-
No. ll Edited by M.-J. Ghess,
J.D. Wilbourn, H. Vainio and
H. Bartsch
1984; 362 pages Sw. fr. 50.-
No. 12 Edited by M.-J. Ghess,
J.D. Wilbourn, A. Tossavainen and
H. Vainio
1986; 385 pages Sw. fr. 50.-
No. 13 Edited by M.-J. Ghess,
J.D. Wilbourn and A. Aitio 1988;
404 pages Sw. fr. 43.-
No. 14 Edited by M.-J. Ghess,
J.D. Wilbourn and H. Vainio
1990; 370 pages Sw. fr. 45.-
No. IS Edited by M.-J. Ghess, J.D.
Wilbourn and H. Vainio
1992: 318 pages Sw. fr. 45.-
Available from booksellers through the network of WHO Sales agents.
t Available directly from IARC
NON-SERIAL
PUBLICATIONS t
AJcool et Cancer
By A Thyns (in French only)
1978: 42 pages Fr. fr. 35.-
Cancer Morbidity and Causes of
Death Among Danish Brewery
Workers
By O.M. Jensen
1980: 143 pages Fr. fr. 75.-
Directory or Computer Systems Used
in Cancer Registries
By H.R. Menck and D.M. Parkin
1986; 236 pages Fr. fr. 50.-
ILL Document Delivery
NI.t1 -- Y.ll PH661M (Get:); E-Journal. w/ILL access
US FEDERAL TRADE CONMISSlOl'i (FTC)
US FEDERAL TP..ADE COM14ISS!ON LIBRARY
600 PENNS'x'LVANIA. AVENUE NW
WASHINGTON. DC 20560
REG-14808602
DCUDJG
ATIN:
PHONE:
202-326-2732
E-MAIL: library@ftc.gov
SUBH!TI'ED:
PRINTED:
REQUEST NO, ;
SENT VIA:
2009-10-23 11:53;33
2009-10-23 15:25:36
REG-14808602
REG
TITI..E;
PUBLISHER/PUCE:
VOLu14E/ISSUE/PAGES:
DATE:
OF ARTICLE:
TITLE OF ARTICLE:
ISSN:
OTI-r:ER NUMEERS/LE i
SOURCE:
MAX COST:
COP'.t'RIGHT Cot1P . ;
CALL NUMBER:
NOTES:
REQUESTER INFO:
DELI'v"ER'x' ;
REPL't:
DOCLINE
OOCL INE NO, : K':iB-20004906
OPAC NO.:
Copy Journal
PHOTODERMATOLOGY. FHOTOIMML!NOLOG'i & PHOTOMEDlCINE
t<lunksg<:lard Copenhagen :
2007:23():59-60 59-60
2007
Hill (l'fr SA
CRITICISM Of FDA PILOT STUD'!
0905-4383
Unique ID.: 9013641
KYB-28004906
Loc:atorPlus
$14,00
Guidelines
Hl PH661M {Gen}: E-Journa.l. W/ILL access
T'1' 1-39800746
FTC
E-mail: lihra.ry@ftc.gov
Mail:
KEEP THIS RECEIPT TO RECONCILE WITH BILLING STATEMENT
For problems or questions. contact NLM at http://wwwcf_nlm_nih_
gov/ill/ill_web_form. cfm or phone 301-496-5511.
Include LIBID and request number_
NOTE:-TH!S HATERIAL f.1AY BE PROTECTED BY COPYRIGHT LAW (TITLE 17, U.S. CODE)
Ntl-1 Collection Access Section. Bethesda. MD
v
y
s
n
).
u
e
od
:s
.1.
I.
n.
.n
n
l'lmttlf>ii1JiUffiii'/1C)IOitmmmol P/mJuu,i 23! 5'}-00
11/Ndt'"'''" Mltllkrtflffl
.(: 1!10? Ttl\<
.a.' ZtXJ'I lJf(lfk'f'r!l
Pbotoriermatology
Photoimmunoiogy
& Photomedlcine
Letters to the editor
Criticism of FDA pilot study unfounded
(response toR. l\tl. Sayre and J. C. Dowdy)
Sharon A. Miller
1
, Sergio C. Coelho
2
, Barbara z. Zmudzka
1
, Janusz z. Bceri
1
US 1-'omlalllf Drug Atimir.i.rlmtimr, C.'t<ltler for Del'i<t unJ Rndlf!lctgicol Heolt/1. M JJ, USA. ami
Nutium:J of Hi!ult!l, Narimml Cum:cr .t'd D. iiS.-1
To the Ed1lcr,
We apprcchllc the opporLunity to to R. M.
Sayre's and .J. C. Dowdy's [Sayre and
Dowdy (1)} regarding our pilot sturly on indoor tanning
exposure sched1:les (2). Sayre and Dowdy analyLCd our
data antl indicated that our study is 'flawed' because we
relied on statements provided by Caswell and
(3, 4) that their study followed FDA guidelines for
tanning bed Sayre and now cblim
that the e"-posurc schedules used in Caswell's study
devi<1led from current FDA guidelines. To verify this
assertion, we oont<tcled Dr. Mich5iel Cm;well. According
to Dr. Cllswdl, their sunhed oulpul was .re-measurc:d
during the study a new maximum exposure time
was calculated. They delermim:d th<1t during weeks 4
and 5, the doses were JO% below the maxfml!m
aUo\vab!e dose. Therefore, Drs. Caswell and Sayre
opted to incn:ase the exposure time to 15 min for weeks
6-8. This rcsulled in a dose thai was 10% higher (noi.
25% llS Sayre and Dowdy chum) thun the theoretical
maximum chuing weeks 6--8. Caswell believes that this
ch;mge did not significantly affecl the biologicul
response and we agn!e. Using lhjs information, om
calcuiutions indicate th11l the cumulative dose ust>:d in
the Caswe!1 study was 2% higher thnn
thjlt recommended by lhe current FDA guidelines {5).
This small difference is highly unlikely Lo have any
imp?.{:t on 1he important finding,-; of our pilot i.e.
thnt we were able to produce similr:r tans to those
achieved following current guidelines by using cumula-
tive doses thar were a.t least a factor of three lowc:r.
Sayre and Dowdy also point om tha1 we did not
determine the degree or 'erythcmic uv acclimatizution'
maintained by once o.r twice a month exposures. This
is correct, and nowhere in our study do we claim
th'n 'crythemic acdim<ltization' ,viih our study
is r:quivn!ellt to that which may be obmined wiLh the
current FDA guidelines. Also. based on current
li!emtttre (6. 7} the degree of erythemlc acdimatiz;:Hion
conferred by a sunlamp-induced mn is sman, equivalent
lO n 'sun protection factor' of 1. 7-4.
Sayre and Dowdy aiso state that the 6 SED
mn.ximum exposure used 1n our study is approximately
30-61VV!l large.r than tlle current maximum dose
a11owcd by the FDA policy. Ba:;ed on our cukulatioas,
the maximum dose used in our pilot .study was
higber than the maximum dose ai!owed by the FDA
policy. This difference n:sults from the fact that we
used th.e intenmtionally-uccepted CJE erythemal action
spectrum, which varies from the CIELytlc actio!l
spectrum publisht.>d in the 1986 FDA Policy Letter.
1n designing our study, we chose a ma"'irnum dose of
600Jfm
2
-CIE (6 SED) as being. approximately equiva-
lent to the maximum dose in lhe FDA Polky .Lelter oi
624J/m
2
-FDA. As Sayre and Dowdy note. this dose is
highly dependent on lhe emission spectrum of the
sunlamp. Based on our earlier study (8j, the ratio of 6
SED to 4 MED--FDA as currently defined by the FDA
ranged from J. !0 to } .48 for six different lypes of
sunlamps which were evaluated. Again, this difference
in .maximum dose has no effect on the conclusions
presemcd in our paper,
The objection of Sayre and Dowdy that we only
studied the krwer area of our subjects, and that
the tanning response may be diiTerent 011 different
pans ot' the body, also has absolutely no bearing on
the conclusions of our study. We place in the same
category an cbjeciion to our using trained observers
<md color-measuring jnstrumcntation for evaluation
of skin color changes. Our approach optimi:?.es
by combining subjec.:tive evaluation by
ar. investigator with objective quantiltnive measure-
mem. Sayre and Dowdy assert that adequate
evaluation of whether a ian has reached the optimal
level can only be made by ihe indiviuuai who is
seeking the tun. n1is might 0::1 an interesting study of
customer satisfaction' nnhcr than a photobiologic
exploration of tanning process. The duta from our
59
Material may be protected by copyright law {TWa 17, U.S. Code)
-
LciU.'I'S rht' edinw
study compared with that of Caswell proves thai. dark
tans can be achieved using sigoiikantly reduced.
cumula!}ve doses as compared with those used in
current practices. Jf users desire a lighter cnlor, they
can cease tanning after fewer
Sayre and Dowdy assert that the succefisful rcsuli.S
of the cunent FDA sunlamp exposure guidance are
'frankly impressive.' However they base this assenioa
on the statistics of acute injuries. Indeed, in il.s early
stages, the tanning industry was p!ugucd with severe
bums, photokeratitis ancl even f<i1a1 outcomes when
dlcnts combined the use of tanning devices with
photosensitizing drugs. After IJ1c FDA Performance
Smnd;.ml for Sunlnmp ProducEs went imo effect, the
number of acme deleterious outcomes went down.
For this reason, Sayre Dowdy plead for retaining
the 1986 policies. However, there is no doubt lhat
of l 9!\6 require modernization bas::d on
scientific progress in the lust two decades. Aho, U1c
risk of delayed damage remains and is poorly under-
stood.
Skin cancer rates (including cutaneous malignant
mehmom<t) <lre rising at 1he rate of 5
1
Yo per year.
Here, t;mning devices are primary candidates for
scrminy. The reduction of the UV burden to a million
people a day who visit indoor tanning salons in the
US cottld 1ead lo a significant decrease in the
incidence of deleterious Jong-tem1 effects rrom th::se
exposur<lfi. We wmtld be remiss in not scorching for
means by which to reduce the cumulative UV dose
recdved by a signilk2nt segment of the Unjtcd St:lles
population.
60
In summary, while we ttppreciale Sayre
Dowdy's comments <m Oltr pHol study we find no
evidence that would supporr their n;:,lion that Otlr
study .is flawed_ The of the UV bmdra1 to
indoor tanners through new exposure scht:duleJ5 is O\.lr
goaL
References
L Sayr.: RM, Dowdy JC. lnd\)or tanning FDA pilot
study iinwc:d, Phorocier:m:tol Photmned 200'!:
23: 57 .SS,
2. Miller SA. Coelho SG. Ztm:dzka BZ, .Se.:r JZ. Reducti(lll vr
U V burden to ir.door through new exposure
a pilot study. J>!tutilderntalol !'huruimrmmo! Photomed 2006;
22:
3. M. The cf tho.' tanning r.::sponm: 10 trmning boo
Photmh:rrnlHC!I Photo.irnmunol .Pholomcd :moo; Hi:
HH4.
4. Sayn: 'R M, Dowdy JC, Cssweil M. M;linumanc(! of <I l:tn
induced hy " lannirl!l hetl. Photmimn Pholoimmur.<Jl .Phom-
med 7.GM; J'i; 92.
5_ US Food and Dn:g. Aclministrstiun. Pnlky ui'l mal!itm:m
timer in!erval !li!d exposure iiChedule rnr l\Unlamp;;. Rrn:hille,
MD: Dcpart:ncnr of Health and Human Services, Food and
Drug ;\dministrmion, Center lor Dcvi:cs ;.mu
Health. htlp:fiwww.frl:;.gevfcdrh/mclhlth/pdf;sunpalO!.
pdi.
6. lk<::h-Timmsen N, R:wnborg L. W\\lf HC. A study
of ;he mc-lnnugcnic effect of mult!ple Hlberytltem:ll dtt!reS of
ultraviolet n;dintion so1.m:cs. PhotodermrttoJ l,hotol.mmunol
Ph!ltom\!d 1994; SJ-56.
7. J)evgun MS, Johnsm1 !iF., CR. Tnn11ing. prolcclion
SIJtibl.!rn and n. British J Dcrmlltol 1982; 107:
275 284.
!!. Millet Si\, Hamilton SL Wester UG_ Cyr WH .. O.o of
U VA from and the poumtial importance for
Ph01ochem Pl\otol:lioi !.998: fill; 6.3 70.
Material may be protected by copyright law (Title 'l7, U.S. Code)
###
#
#
#
#
# #
# #
######
Job : 57
### ### ###### ### ### #####
# # # # ## # # #
# # # # # # # # #
##### ### # # # # #
# # # # # # # ####
# # # # # # # #
# # # # # ## # #
### ### ###### ### ## ### #
Date: l0/23/2009
Time: 7:24: 56 AM
### ###
# #
# # .
# #
#
#
#
###
#
###
#
#
#
#
#
#####
ILL Document Delivery
NLM -- Wl J06794 (Gen); E-Journal w/lLL access
US FEDERAL TRADE C0!-1t'IISSION' (FTC)
US FEDERP..L TRADE CD1<!MISSIDN LIBRARY
600 PENl'lSYLVANIA AVENUE NW
WASHINGTON. DC 40560
ATTN:
PHONE;
FAX:
20;;!-:326-2395
REG Copy
Sl.JBMil
PRINTED;
REQUEST NO. :
SElIT VIA.:
DOCLINE NO. :
Journal
2009-l0-22
REG-14807567
OOCti!'I'"E
KYB- 27 9 96'73 0
REG-14807567
DCUDJG
11:47:53
14:56:27
TITLE: JOURN,\L OF !l:TVESTIGATIVE DER!v!A.TOLOOY. SYMPOSIUtil
PROCEEDINGS / THE SOCIETY FOR INVESTIGATIVE
DERMATOLOGY. INC. EUROPEAN SOCIETY FOR
DERMATOLOGICAL
PUBLISHE!V'l?LACE:
VOLUME/ISSUE/PAGES:
DATE:
AUTHOR OF ARTICLE:
TITLE OF ARriCLE:
ISSN:
OTHER NUMBERS/LETTERS:
SOURCE:
l'IAX COST:
COPYRIGHT OJi-1? . :
CALL NUMBER:
NOTES:
REQUESTER .!HFO:
DELIVERY:
REP!.Y;
Nature Publishing Group
2009 Aug:l4{1):32-5
2009
New York. N'i :
32-5
Coelho S;Choi W:Brenner t<l;l-1iyamura Y:Yamaguchi
Y:Wolber R;Sm
SHORT- .AND LONG-TERH EFFECTS OF UV RADIA.TION ON
TH
1087-0024
Unique ID.: 5609059
K\'.!3-27996730
l%75550
PubMed
$1<:1 00
Guidelines
Wl J06794 (Gen); E-Journal w/ILL access
jkn
Linda Henry
E-mail: library@ftc.gov
Mail:
KEEP THIS l<ECEIPT TO RECONCILE ltJ!TH BILLING STATEMENT
For problsns or questions. contact NLM at
gov/ill/ill_web_form.cf.m or phone 301-496-5511.
Include LlE!D and request number,
NOTE;-THJ.S Ml>. TERlAL MAY BE PROTECTED B'i COP'iRlGH'f LAvl (TITLE l 7 U.S , CODE)
NLM Collection Access Section. Bethesda.
ILL Document Del ivery
REG-14607567
M.A.TERIAL MAY BE PROTECTED BY LJ.>.'IJ ( TITLE 1 ?. U.S, CODE)
: .
. ' . . . " '
>
32
. .
ORIGINAL ARTICLE, .. .
-' > {" - 0
Short- and long-Term Effects of UV Radiation on the
Pigmentation of Human Skin
Sergio G. Coelho\ Wonseon Choi
1
, Michaela Brenr.er\ Yoshinori Miyamurn.
1
, Yuji Yamaguchi\ Rainer
Wolber
2
, Christoph 5muda
2
, jan Ludger Kolbe
2
, Shosuke liol, Kazumasa Wakamatsu
3
, Barbara Z..
Zmudzka
4
, Janusz Z. Beer
4
1
Sharon A. Miller
4
and Vincent J. Hearing
1
The incidence of skin c:anc:er, including cutaneous melanoma, has risen substantially in recent years, and
epidemiological and laboratory studies show that UV radiation is a major causative factor of this increase. UV
damage afso underlies photoaging of the skin, and these deleterious effect's of UV can be, in part. prevented in
skin wi'th higher levels of constitutive pigmen1a1ion. We revie'>v the dini<:al studies we have made in recent years
regarding the rapid and the responses of the pigmentary system in human skin to UVexposure.
}oumal nf Derm:lio!ogy Symposium Proceedings 12009)14, :U-,15; doi:l O.HJ:l!lijid.symp.:.!!.l09.1 U
INTRODUCTION
The incidence of cnncer. esper.fally melanoma,
has increased subsrar.tlally in recent years, probably
as a result in part
1
oi increased exposure of fair-skinned
populations to uv radiation [NCI Seer Statistics, http:!!
seer.cancer.gov/}. Epidemiological and laboratory studies
provide convincing evidence that UV exposure is a major
causative factor in melanomagenesis {Gikhrest et aJ.f 1999;
Landi ct a/., 2003) and certainly is a critical facior in
pho!oaging (Yaar and Gilchrest
1
1998; Haldr and Am,
.2003)_
Constitutive plgmenlation of human skin provides excel-
lent proteclion against cellular and DNA damage due io UV
exposure (Taclokoro et a/., 2003; Miyamura et at., 2007;
Brenner and Hearing, 2008}, and this protection is doe to a
number of properties of the mlanins produced. Melanin has
a broad absorption s.pe<:trum because of ils strong
scattering component (Kolli<Js and Baqer, 1987; Chedekcl,
1995}. Melanin ls produced by mele:mocytes residing al the
basal layer of the epidermis bul then is rapidly transferred to
1ldjtlcent keratir.ocytes. Following the transfer, melanosomes
a;e distributed toward the surface of the skin, where they
shield nude<lr DNA in onrlerl>ing cells from UV {reducing
photodamage) and protect collag;=n and elastin irt th<! dermis
(reducing photoaging) {Pathak, 1995; Koba}'ashi et af., 1998j.
Constitutive pigmentation of the skin pl<'ys a critical role in
minimizing DNA damage from UV (Tadokoro et al., 2003:
2005; Yamaguchi et iii., 2006
1
200Bb) i!nd in reducing the
risk of (Gilchrest, J 993; GHch;est eta! ..
1999).
Our collaborative research groups have performed a series
of clinical studies examining tne effects of different wave
lengths, doses, and dos-e intervals of UV exposure on human
skin oi various racial!ethnic origins and phoi.Oiypes. These
studies have been reported in the literature in which
interested reuders can go for details (Tadokoro el Jl., 2003,
2005; Yamaguchi et aJ., 2006, 2007, 200Sa, b; Miyamura
el a!., 2007; Brenner and Hearing, 2008; Brenner eta/., 2009;
Coelho ef a f., 2009; Miller er aL, 2008; Wolber et al., 200f.l).
Considering the sum of these studies, we are able to drdw
conclusions about. the effects of UV on human skin and the
kinetics of the biological elicited.
UESULTS AND DISCUSS\ON
on the effects of UV on human skin
Subjects wlth a wide variety of skin photo:ypes, with different
racial/ethnic backgrounds, were recruited for our studies,
which the effects of individual or repetitive UV
irradiation on human skin, and at various times (up to several
after initial UV exposure. The som of these analyses
revealed that even within each radallethoic group there was
a greal range in the conslil.ulive levels of skin pigmentation,
that there was a great variation in the ranges of MED and
photosensitivity of the subjecls in each group, and that there
was also a wide range in the ability to increase skin
pigmentation ir. response to UV (termed facultative plgrnen-
latlon), as well as in rhe rate of increased pigmentation and its
persistence.
The different time points examined after UV exposure also
revealed four dear ;.Jnd distinct stage!; in pigmentation
_ ...... "--------------
'P!grmmt Cell P.io!olfl Sectif)(l, u{ Eiulogy, Nation'll CJm:t.Y lnst!lule, Nalinnal !r>slit:JIL'i of ."''t!.tllh, Mi!ryl.1nr/. USA;. ::R&D Skin
Reic-r'o/Jorf AC, Nifmburg, Ct:rmsoy;
ai Chemistry, Fujita He.;/th Uni'l':er>it.Y School nf 1-!P.a.lth .Scienct!S, Tayt.wkc:. Air.hi, }ilpiln imrl
c,'llll!l iot Devices and il;;rliofugica) Health US Fwd ;md Drug t\dmini';tralltm, Silvt!r Spring. M;1ryiimd, U!i.-'l
Dr VincP.nt }. 1-le;tring, l.i:!lxN>Jrory uf Cv!l 6iofogy, N.lt[dlloil C:mtl?f Nllllanaf of 1-!e<llth 8ulidi118 37, ileum 2132, MSC
4256, tJet!w.sda, M;;,ryl.i!ml 10892, IJSA E-mail: heJringvlil'nih.J:.>u"
RO!CPiveri 14 Nnvi!mhefl(JOlJ; ar:c!!p!ed tl J;muary 200!1
responses. 0) Immediate pigment darkening. which develops
in minutes and can remain for several hours (Honigsmann
et at., 1986; Routaboul et a!., 1999), is gray/black fn color
and is thought to be due to the direct effects of UV on exls!iog
melanin or melanin precursors, perhaps oxidizing them to
darker colors (Lim and Soter, 1993). {2) Persistent pigment
darkening, which occurs within hours and remains for days
(Moya! et al., 2000, 2.006}, is thought lo result from newly
synthesized meranin in the epidermis (Tadokoro et ul.l 2003,
2005). {3) Dela)ed pigmentation, which develops in d<1ys and
remains for we<!k.<i {Ortonne, 1990), results from prolonged
increases in melanin content (Brenner et al., 2009; Miller
ct al., 2008). (4} long-lasting pigmentation, which remains
>9 months after initial UV exposure, results from prolonged
activation of the pigmentary system {Brenner el al., 2009;
Coelho et af.
1
2009).
l<inetics oi pigmentary responses to UV in human skin
To the sequence of events that occurs in human skin
th;:lt would increase pigmentation after one or more UV
exposurf'..S, wa examined biopsies of human. skin of clifferenl
pho!otypes at various. times after a single or multiple UV
exposure(s). These biopsies were measured for melanin
content (using Fontana-Masson staining or chemical analysis)
and for various melanocyte-specific markers (fOf example,
MITf, TYR; and fvlt\RTl ). Skin color was measured by
reflectometry, and other parameters, such as melanosome
distribution melat'!ocyte density, were also evaluated.
The composite results of the studies are summarized in
Table 1.
The sequence of eventS
1
when considered with
development of color in skin of phototypes !I and Ill after
UV expasure, provides a very dear picture of what occurs in
the skin following UV exposure at the molecular leveL The
initial response noted (from the markers tested) is an increase
in MlTf !eve!s, MITF be!ng a transcription far.tor known as the
master regulator of melanocyte function. Significant increases
in M!TF levels occur within 1 oi UV exposure and no
SC Caeffw P.t al.
JfcC'Ji of UV on the Pigmenta!iun of Human Skin
other marker tested responds noticeably within that time
frame, other than the dramatic and quick increase in visible
skin color known as immediate pigment darkening (Figure 1 ).
As tyrosinase levels and melanin synthesis (determined
immunohistochemically and by chemical analysis) do not
increase wilhin the first few days, it is clear !hat the earlier
hypothesis that. immediate pigment darkening represents an
oxidation and/or polymerization of existing melanin (or
melanin interrnedi<nesl wns correct. M!Tr levels continue to
!ncre<Jse up to 1 week after UV exposure but !hen begin to
dedine and, by week 3 (even wtth repeated UV exposure),
MITF has returned to its baseline con:;titutlve leveL
By week 1, the expression of tyrosinase, f'mel17, and
MARTI (and other melanosomal proteins) has increased
significantly, whereas the melanin con1ent has increused only
slightly (-10%}. The major effect on pigmentation at this
time point is a large redistribution of the melanosomlls that
existed before UV from the basal layer of the epidermis to
layers higher up in the skin. In light of the very minor increase
in melanin content at 1 week aiter UV exposure, it is dear
that the visible increase in skin cD!or (termed persistent
pigrnenl darkening, shown in Figure 1} is due to the upward
movement of melanosomes tmvard the suriace of the skin,
where the visible color increases ond presumably, the
meianin i!\ more effective in preventing damage from further
UV exposures to underlying cells.
13y weeks 3-5, the melanocytic syslem becomes fulfy
ilCtivated, levels of melc:mogenic proteins are maxima!, leve!s
of melanin synthesis are increased, a!id even the density of
melanocytes in the skin ls increased {a!! at levels two to
threefold higher than belOre UV exposure). The sum of these
events leads to <1 pronounced increase in visible skin color
knowr. as delayed pigmentation {Figure l). How long delayed
pigmentation lasts from individual to individual and
not much is known about the faclo5 that determine it.
An interesting consideration is which wavelength n.>gion of
UV causes 1he increased skin pigmentalion, and in a separate
study {Wolber et al., 2008), we compared lhe effects of UVA
Table 1. Melanocyte markers sfudied (summary of results with skin phototypes 2.-3)
Marfler flay tl IJily T Weekl
,\11TF
1
+ -t.;. H.f.
TYR
1
+ + -t+
Pnrel1i
1
+ +
++
MAR'f1
1
+ + -t+
11-wlanln
1
+ + ++
+ + +
redis1ribulhm ...
+ .....r
+ + +
skln to lor .. +i
'tlliesso.:d as inteasity of staining
. . .;:o;uem as by hnnwn.;.!:listoc:hi!mlwy.of Sf ;tin.
:'Melanin contcn! as hy t:bemlcill
rP..>ults W4?11! ob:aine.:l wi:h for TYR, MA!l'f<, ami .'.UTF.
"Mca>urcd teJ1L'ttaoct-.
Weck2
+t +
++-t ++
+++ ++
+++ ++
H +I
+ ++
+
....
... .,
+++
Material may be protected by copyright law (Title 17, U.S. Code)
WeekS :<t9 moolh&
+ +
++
+
..
.... +
++ I-
++ +
+l +
+ +
++
.;.
T+f +
www.Jidonline.org 33
34
SG Coelho et al.
f:ffects of UV on th!? Pigment<ltion of Human Skln
a BeforeUV 1 weak anar uv b a ooys attsr uv
.. ,., ..
5 mlnules after UV 4+ weeks alter UV 1 c.Jay alter UV 1 .s years after UV
Figure 1. Exmnplei oi p!l.1w.s ni lncn:;r!Kd pi!lnl\!UiaHtm in human foHowi<'Jl UV {a) Subjl'Ct 13!1; tnp l'lf:: t;OIIIml unitrncliaied skin beit11e UV
hmtom lcit: immediate pigmenl darkening, 5 minute; ilite: UV l()p rigi,t; pe.sistetrt pigml!nt 1 week alrcr UV el!posure: houom
risht til!layecl pigmcntat!on, 4 + weeks afler UV uxposure. tb) S91; tup lelh t:Utllrol unirrlldiaivd si.rn: bottom l ai:r MED righl:
pe10istenl pigment darkening, ll duys after UV; bmiom ri]iht. fonr,fasrfng L'i )'l!li:S a iter U\/ exposure.
with UVB in eliciting increases in skin calor. UVB is rnore
effective at stimulating skin pigmen1ation th.ar. UVA, but both
wavelengths ciln e!icil campar.lble increases in skin pigmc.,on-
tation with <tppropriate doses, althoug!-! the mechanisms are
distinct UVA hus no effect on mdanin tonlent
1
activation of
melanocyte differentiation, or other parame1ers measured,
yet UVA expnSurf! stimulates visible skin pigmentation
significantly. Presumably, this is due to the Oleidation of
existing melanins nnd their precursors and/or due to the
effecls 001 the distribution of melanosomes in skin, perhaps
from thl:! known effects of UVA en cytoskeletal components
(jimbow and Fitzpatrick, 1975). Thus, UVA-induced in-
creases in skin pigmentation are comparable with prolonged
immediate pigment darkening. In conlrasl, UVB ,stjmulates
the melanogenic system, as discussed else'.vhere in !his
paper.
Recentiy, our follow-up studies the same
subjects from 9 months to 3 yenr!Y ilf1er UV exposure (these
individuals stated that they had no further significant UV
exposure after the original prottlcol), Interestingly, in a
sisnificanl portion of this populntion ( 30%), visible
increases in skin color remained in areas that were UV
exposed earlier. We have lermed this phenomenon long-
lasting pigmentation. and studies are underway to determine
why this occurs in some tndividvals and not in others, and to
dctermlne whet11er these factcrs might be involved in various
hypetpigmemary diseases, particularly in those that are UV
related.
In sum
1
our studies have determined th6L melanocyte
density is comparable in dorsal skin of subjects from
all raclaiJethnic skin types (ranging. from types I lo 6),
afthcugh the of melanins produced by these
melanocyws varies and results in the wide
variety of human skin colors. Melanocyte density can be
increased -2- to 3-fold within 3-4 weeks of repetitive UV
exposure. Visible skin pigmentation can be im:ruased
visibly 7- to 10-fold by repetitive UV exposure, although
melanin content varies only -2-fold, sugge.o;ting that the
type(s) of melanin produced and/or their distribution in
the skin is critical to the greater effect oi UV on skin
color. The long-term effects of UV on human skin can persisi
for ycurS1 even in the absence of further UV exposure.
As a complete turnover of the epidermis usually occurs
every 4-5 weeks, how the pigmentary system remains
activated ln some ct1ses even years later should be sludied
in more derail. The m(!Chanism{s) under!ying long-lasting
pigment<Jtinn are a r.ubject of great interesl for fulure study, as
they may provide important clues about the regulation of
melanocyte difieren!ia!ion and_ give further insights into
hyperpigmen!allon of hltman skin in UV-reiated
pigmentarr diseases.
MATERIAlS AND METHODS
Study suhjectst UV irradiation, and
These studie; invoived volunteer wbjects with skin l-6,
a.." reported \n tht! inili<JI studies ior each prutocol (Tadokoro el al.,
2003; Miller el al., :WOO; Wolber ei al., 200ll). The studies acnercd
to the Helstnki gHidelines :md were app!tlYecl by the Rcse:lrch
lnvolving Human Sr.;bjecls Committees d the US Food and Drug
,o..H r.ubjec..1s gave wrillen, ioiorrned consenl. Subjects
(labeled "T .. } from or.e of !he !itvdie;; (Miller ,)/., 2t10R) were UV
exposed one to three times per week for 4-5 subjects
(labeled "5"1 from a rJiiierenl study (Tadokoro ct al., 20031 rec<?ivad
a single UV t!xposurc. ancl subjects {lube-led "!.!")from }'e! another
study {Wolber cl af., 2008) wme UV exposed five times a week for
2 Wl!eks.
I
(
I-
f
..... """""'""""'._,,...,..,...... .. ........
Effects of UV on the Pigmentation oi Hunt<ln Skin I
Biopsies and immunohistochemical analysis
Skin biopsies were takert from control and UV-exposed sites al
various times after UV c.!tposure . .Each b!opsy wns plilced dermis side
dnwn on a Millipore fl!ter ;md Wils then fit;ed in 4% formaldehyde,
embedded in paraffin, sectionecl at l-j.lm thkkness, mounted on
5ili:me-coilfed glass slides, nnd thcr. stained using
chemistry, as described earlier (Tadokoro et a!., 2003, 2.005;
Yamaguchi er a/., 2004, 2006}. Sti!lning were :tnaly;,:ed
using a !..eicll DMRB/DMLO fluorescence microsc:opt-, and an
internal control was used eilc:h time to control for reprodudb!e
antibody stJlning. Neglltive controls omitting the pdmary ant!body
well:! performed each time.
Melilnocyte density and melanin content
Melanocytcs were following stilioing ior tyrosinase, MITt,
Pmel17. MARTl, and other markers ilS detailed in !he orlglnal
articles, and thelr density the epfdermaVdermal border was
determined ilS cells per mm. for
were nnrmaHzed ngainst 4'-
fr.dimnldino-2-phenylindole staining. for measurements of melanin
content, lipecimens were stalf!ed by the fontana-Masson method
and were also me:1sured by chemical aoal}'5is (Wolber el ill., 2008).
Tfansmitted light intensity was measured by the DMRB\OMLD
microscope and Sdonlmage softwate was used to analyze. melan!r.
qui!ntlty from integrated ciensity in the sk!n st'Clions, as desc;ibed
earlier (Yamaguchi et ttl., 2006, 20o&l}.
CONfliCT OF INTERFST
The no conii!CI of interest.
ACt;NOWlEDCMEN'fS
This wM suppot1X!d by tht! lf\!Mmural i'rogmm oi the
Cancer lnstitulc llt NIH, ar.d by Oftitli! cf Sc:icmc<!, Oiikc of
Women's Health and ttle Qnler fur Dt!l!ices and Hc.ahh, food
and D;ug {fDA}.
REFERENCfS
Bremnl!r M, r,of!lho SG, !lP.er JZ, Miller SA, Wo!ber R. SmudJ C eta!. (20C"ll
lof1&tetr.J roolcculilr changes in human skin repetitive in situ UV
J Dettl1atol12!l: 1001-11
M, Hearing VJ {2006) prolcctlvc role of melanin ogainst IJV
damage in ituman skin. Phmnchem Phmahinl !!4;539-4')
Chcr.k-ke! MR :19!t5} Photophysics and phntochemiSiry ol mc:anin. In:
MeiJnin: lf!i Role In HumJn {7.cisc L. Chedak:e! MR,
Fit.zpatrlck ill, ed$), Ovt?rland Park: Vafdcnmar f'ubl. 1T-22
Coolho SCi, 7.hou Y-C, Busf;ar HF, Miller SA, Zmuo';zka BZ, Hearing Vje! af.
G!OO'Jl long-lasting pigmcn!ation {LL?} of hum;ln skin, a nC!w type of
cuf;jfleoos respons11 to UV. Pigm1mr Co!l Mr:Mnoma Res .22:236-41
GiJcl,testl>'\ (l99.ll Stmsc-ccr$ public he-<h upportunit.y. N Eng/ J Mcd
Gll<:hresl IJ,\ MS. Geller AC, Yaar M (1999) The: polthogc:ncsis oi
melanomil iflcluced by ullravlo!e-r ratilalion. N Eng! J .'vll:!d 340: 1341-ll
Hairier RM, Ara q WYJ3} Skin C'ilnccr ;:mcl photoaging in ethnic
Dctm<::lal
Hunigsm1nn H, S:huler G, W, Romani N, Wolif K 1'1 986) Immediate
pigtncnl u.,rk.;r.lng phenomenon. A oJ h;
J In res: 0P.:nlalolli1:Ma.51
Jlmbow K, Te ( 19751 Changes l:J dlmibution p:merns of
cy;opfasm;c f!famcuts in trurr.iln during ultraviole;-
mldatcd pigtr.entation. 1 C!!ll Hiol65AR l-8
N, A, T, Y01mashlna Y, Shirai T,
M.W cl ilf. 0 9':!Ul Supt31'1u<:lr mcl;min cap$ R!dutc l.dlroviolcl
induc:ed DN\ photoproduc!S in epidermis. J 1nvest Dermillol
n o:fJOr!-1 o
KniHas N, B<1GE':f AH n9fli') Ab50rplion of hurm>n m::-luntn in the
visible, 40:1-no r.m. J /m-er D=ta/ 89:384-8
l;:mdi MT, A, Tarnne RE, Pearorl A. Tucker MA. Hedayati Met a/.
{20031 DNA n.'l'air, dysplimic I'ICYi, nnd sunlight sens!dvi:y in the
cie'lelopmenl ol melullOma. J N.t/1 Ciurcer lll!it
Lim HW, Soit..'l' NA fl993) Clinicill New York: Martel
Dekker, Inc.
Miller SA, Cooll'm SG, Zmwdzka !IZ, Hf, Yamnguchi 'I, Hearing VI
t.:t <tl, (l(!CJIJ} Dymnnic> of ind1.1c:tion by \.N
t'Xpc>!ll'CS: dose, dost! interval ami iJV spectnsm dcp<mdent:c. Sr )
Oermilto/159:921-JO
M!yam!Jra Y, Cooiho SG, Wolber R. Miilcr S.\, K, Zmudzka BZ
cl al. {l0071 Regulation of human skin pigment.:ltion ;:nd responses to
uhr,;wiolel tadiation. Pigment Cell 20:2-13
Moyal D, Ch;;rdon A, Koliias N (20001 Dl:!term!naliun oi UVA pral!o'Cliun
factor> using t!Je persi:telll pigment darkening {f'PDi us lhe end point.
(P.ld 11. cam:;rntron of ihe me:hoo. Pholaderm.ttol
f'lmir1med 1 !i:145-9
Moynl D, Wichrowski K. lricnuc C !:!t'OU} !n vivo pcrsist:mt
ml.!lhod: a dernor:slmtion of the reproducibility oi the UVA
pr01ect!on factors results Jt ll'!!iti"'g iJhor;;tmles. P{mtndermi!tn!
Phvtolmmunof PhoromE:d 22:1.<!4-ll
Orlonroe Jl' (1990! efli!c!S of exposure on
p!gmtmlillion. ) lnt Med 1 il:M:-l1C
Pathak MA (1995) FunclloM of melanin and protection by mi!l.:min. In:
MC!I;;min; Its Rolf! in Hum:m Piroroprotec:lion. tle1S<1 l, MR,
TB, eds). Over!;;ncl Park: Valdenmar Pub!, 125-34
Roulaooul C. Dtn\$ A. Vlrdu: I (19!J!J? lmmt<dia.te pigment darl!!.!ning;
rlescriplion, kinetic nnd bialogit:a I function. fur J Dermarol 9:95-13
Tndukciro T, Kobayashi N, Zmutizka BZ, hn 5, Waka:mHsu K', Yilmagut:hi V
1!1 a{. !:!003) UVindut.:t::d DNA damage ilmi )";''tianio in human
sl:ir. in r.lcillllethnic origin c.nd pilolosens!tivi:y. FA5B J
17:1177-!i
Tiidokom T, Y, Batzer j, Coelhu SG, BZ, Mille: al.
!2005) Mt;chnnisms of skin :ar.11ing r11 rlifferent :ildll!iethnic
groups in response lo j lr111esl Detma/(l/
124:H2t.-:J:Z
Wolber R, Sci1le11z K, Wakam.tl$U !<, Smuea C, Nakanishi Y; Hearing VJ el al.
i20.18) Plgmenlillion eff!!Ct5 of s<J!ar simulated tadialion as t:Omparl!d
wirh VVA and UVIJ radi<ltlon. Pi!)ml'ilt Cell Me.fanomn Res 21 :Hl7-91
Yaar M, Gilchrest 81\ {'1998) Aging photo;tginr,: rne<:han-
Jsms ar1d effectors. 1 !Jermaro! Symp Prvc );47-51
Yamaguchi Y, Btll/t Jl, HrmJir1g VJ (l006al Mel::min i.lpopiO$iS or
coli> hy uitr;wlole: radlalion: facfM lniJuencing the
inddeno: of skin um:er. Arch DmniJ/al Rm JUO{Suppl 1):543--50
Yi!magur.hi Y, Brenner M, VJ {2007) The regt:l.>fion of
pigmentation. J Bini Chem 162:27557-0t
Yam;Jguchi Y, Coc!ho SG. Zmudzka 9Z, Talwhasni !<,Beet J2, Hearing VIet <Jl.
!2CLlilb) CydDbutane dimet lind pS:! production in
hllman ikin after led UV Ommaio/17:ql:..,14
Yun1.1gUChi Y, ftami .S, Wi!ltlhc H, Yasu;nolo K, ZA, Kt:bo T et ill.
{2004} the ;kim lr.cre;sscd
expression of dk:k,opJl by p:Iimcp!ao:ar ilbrob!M13 Inhibits melimocyta
growth ;1nd dlifl;lf'entiarion, J Cali/Jia/165:275-85
Yamaguthl Y, Takahashi It 8%, Kami-1.1115er A, Miller SA,
Tadnkmo T cl al. !:Wli6l Human skin to liV radiation:
pigment in the epidermis against DNA daw.age in the
lowet epidermis and fadlital!!;!; FASEB J 20:1456-8
Material may be protected by copyright law (Title 17, U.S. Code)
www.jidnnlinc.org 35
i
;
'
l
!
.I
I
1
l
1
###
#
#
#
#
# #
# #
######
Job : 59
### ### ###### ### ### #####
# # # # ## # # #
# # # # # # # # #
##### ### # # # # #
. .
# # # # # # # ####
# # # # # # # #
# # # # # ## # #
### ### ###### ### ## ### #
Date: 10/23/2009
Time: 7:26:14 AM
### ###
# #
# #
# #
#
#
#
###
#
###
#
#
#
#
#
#####
ILL Document Delivary
NLM -- Wl EX502C (Gen); E-Journal w/IU. access
US FEDERAL TRADE COMMISSION !FTC)
US FEDERAL TRADE COMMISSION
600 PENNSYLVANIA AVENUE NW
WASHIN<:rroN. DC 20580
DCUD.TG
P.TTI-1:
PHONE:
FAX.:
202-326-2395
202-3-25-2732
library@f tc. gov
SUBt.HTTED:
PRINTED:
REQUEST NO. :
2009-lD-22 13:35:41
2009-10-22 15:10:40
REG-14807690
E-HAIL:
PEG
TITLE:
l?UEL r Sl-f"'.e.P./FLACE :
VC!.UME/I SSUE/PAGES:
DATE:
AUTHOR OF ARTICLE:
TITLE OF ARTICLE;
ISSN:
OTHER NUM.BERS/LETIERS;
SOURCE:
MAX COST:
COPYRIGHT COMP. :
CALL NUMBER:
NOTES:
REQUESTER lNFO;
.DELIVERY:
RB?L'i:
SENT VIA:
DOCLlNE NO.:
CPAC NO.:
copy Journal
EXPERIMENTAL DEffi{ATOLOGY
Munksgaard Copenhagen
DOCLn.lE
KYB-2?998071
AAACXNN
2C08;1?{11}:916-24 916-24
2008
N/A
N/A
0906-6?05
Unique !D.:
KYB-27998071
LocatorPlus
S14. oo
Guidelines
Wl EX502C {Gem): E-Journal W/ILL access
li.H
Linda Henry
E-mail: library@ftc.gov
Mail:
KEEP THIS RECEIPT TO RECONCILE \>HTH BILLING STATEMENT
For problems or quest ions. contact NLM at http:/ /WW!fn:f. nlrn. nih.
gov/ill/ill_web_form.cfm or phone 301-495-5511.
Include LI2ID and request number.
NOTE: -THIS MATERIAL MAY BE PROTECTED BY COPYRIGHT LA\'ol (TITLE 17. U.S. CODE}
MLM Collection Access Section. Bethesda, MD
Cyclobutane pyrimidine dimer formation and p53
production in human skin after repeated UV irradiation
Vuji Yamaguchl
1
"', Sergio G. Coelho
1
.z. Barbara z. Zmudzka
2
Kaoruko Takahashi\ Janusz l. Beerl',
Vincent J. Hearing
1
and Sharon A. Miller
1
f.abu:-atoty of Cell BiolU1J"f imtiaue, oflh"3lth, MP, I!SA;
for >ind US Fatld ilnd D:us At.!minislr.tlioil, SilYfr Spring, MO. USA
CarrcSJmndcnc; Dr Vinn:nt J, Heatit'ij PhD. of CcU Biology, N>1tional lmlihth:, N;lfinna! af Heal til. iluHding 37,
Ronm 21.:12, MSC <!256, BethcsC:, MD USA, 1 301 :!16 155-l, + 1 Jill 102 8187, e-mail: h.:aring"@nih.wv
J:'n:;cnl m:ldrt.ts: Dcparmtr.nt nf Gtrimrir EnYiflliWllllltttl Dmnnloi(IJ;;> Ciry School of Mnfita/ ,'idcntcs,
Aichi, Jnplln
f;r. p,;blit:otio11 l!i Fthnwry 20118
Abstract Suhst;mlial difference!i in DNA damage Cii\USl'd by a
irn:.dintiort iound irt nut prt!V!ous srurly on skin
difftt(llt levels of coll!ititutive pigL."lt'ntation. Tn thi5 swtly,
whether pigmenmr.!on iaduct!d by repciltcd tN
imdiatiun is Three nn the l1f 21 healthy
SUbjt:d$ \'lith t}'Pe !1-fH skin Wf!'ft: irradiated at lQ0-600 }/m.l
cvc:y 1-7 v.ver 4 to period. The received
different cumulillivc dos;.:s uflJV { 1900, 2900 or 4100 Jtrn
1
}
<1no were biJpsied l t,l:;aynfter the la'it irradiation, .Biomarkers
induJed pigmenlmntent assessed by Fnnl:llla-M:wou
>Stilling, fum:tion by of
DNA cydobutnn<: pyrimidine dimm (CPD}.
.nuclc.4r ;u:c:wnulation of pSl, cktt'f:rttned by TtJNll
and lcvd5 of p21 :md
in mdanoqi.c fundion and densi!]', :md lnlt:vels of apop!Ools
wctt similar among .S srndy irradiated '-'ith different
lJV ofOD while lhe number af
p53-positlve incrc:w:d as the cumuhtlve dose of l.IV
itKrrllsed. Tht".e suggest tk11 pi:;mrnt<ltion induced Jr. skin
by ftpented UV irradiOJtinn pmtetls LIV-
i.tJduceci DNA clnnmge bot not etTroht<ly constituti>e-
pigmtnliltion.
l'iJQH (itc r/li; ;mpr:r <m Cytlnl>nrilm' .PYJ'imidim: dimcr fotn'!llliol lnd p53 pmolur:it>n in t;ulll;ln $kin nflcr !.IV fmdi.'IIW-'1- &pcrimcnrl
20;Jll; li; 9l6-!l::!4.
Introduction
The risk of skin CA."lcer is inversely relotct! to constitutive
pigmmtatio.r. cf the skin due to its protective effects
agains; ultraviolet (UV) damage ( Accnrding to risk
f.ilctors for 2006 in the US, White/uucasi::m
(hereafter referred to as White} skin hM 11 70-fo!d higher
risk for and StjUnmous cell can:inomas compf!fed lO
.Black <::r (hereafter referred ro as Black)
lr.in, and fol' mclilf\oma are almost 20-fald higher in
White s\!bjects than in Blnck subjects (6-9). [ttl.!diatian hy
artificinl soul'ecs cf UV has mnil.arly dl!trimental conse
qur:nces in human >kin, and the use of tancing devices
has bi!l!n OlSSOdated 'o'.ith incrt'ilsed risk of skin cancer'
At:, unil; C.PD, cydobutane pyrimidine
MD, minima! erythema dnlll!; $Olnr simulatl!l:1
raciimior:; Tt.:Nr:I.. t=inal wwsferase-medin1td
dUTP-nic:k ead bbdling; t:V, ultnvjolet.
(6-S,lO,ll). Our group has published seve01! articles on
the imptntance of constitutive skin pigmentalion for the
reduction of ti"V damage resulting from :. single
to one minlmal ery!.hema.l dose (M'ED) ( 12-14}. !t is
time.s: :trgued that foculu.tive u:mning. i.e. skin pigmentc:tion
induced by UV i.-.mdiatlon. prort:c:ts against damage caused
by sub.sequ:!nt 'UV irradiation but no conclusive studies to
measure thac directly have been reported. h<Jve begun
io investigate the effects of repetitive l..:Y
including effects on skin pigmentJtion (15, 16), to
the ab!lil:"f of tacultative pigmenttttion to reduce DNA
d:tm;]ge from subsequt!nt 'LV' irradiation.
.Sew:tal studies have e:.\-amined whether pigment;;tlon
induced by repeated l<>wdusc UV imcliat1on is protective
in h:tmi'IJ1 :.kin, but the findings have been iru::ondus:ve.
One reported that pigme1.1talion by
multipk UV eg;Jinst UVlnduced DNA
damage 07). That stud; inr::re.:ml epidermal
pigmentation nnd thickness, and demo.nstr;;ted that
916
111o daim io or'glnar us
Jourr.2l C:lms;i'Ation el 28 Sl,l::Klii<!N Munk"!ii!ard. t:xpf'rimental 17. 91 !a-!n4
Material may be protected by copyright law {Title 17, U.S. Code)
) jl!i.>
f I
.;
f
,-
'
l
'
:;f
l;
:i!
/1
-<
t
I
'-:'
,,
;
\f
'
....
]
. f...
'
,.
1
.l
!
r
t
t
,,
:l
;:
'I
J
-
:;
F
p.
::
i
--
,
-3
"
J
g
1
.,
l
!,\
j
t
.
'
'<1
t
.,,
>
{
::I
,:-:
:;1
''1
. j :.-
,f\.
..
'1l
J
i)
..
..
"
j
1J
il
"
'I
.
(>
J
ii
r
'Snrr
*
.r
.:--.
..
:.;
,.
elcvati!d post-irradi:rtion levels of C"fdobutane pyrimidine
dimers (CPDs) and nudcar p53 return to background lev-
els within a re:l:Jijvdy short period oi time (3-'l day;;).
However, another study {18) reported that distinct DNA
damage persisted in skin. up to after a moder01tc
dose of s;olm simu1a!cd radi;ation (SSR). Anothe:: study
showed th;zt DNA accumulates with repetitive VV
irradiation and that compamblc levels of damage (per
physia1l occurred in t;'Pes U and IV skin (19).; the
authors proposed that the kinetics of DNA repair played
an impomml role in controlling DNA and con-
dndcd thm: increased skin pigmentution mny not be the
major fuctar .in nalurul photoprott'::tit.w'. Thus, although it
is weil-iicceptoo that ex:ce5sive UV irmdintion must
b(! .-;voided the::re is no consl!mms regarding
and hmv photoprotection can be induced by
moderate li"V irradiation.
In study, we CJCamlned hm" different doses and pro-
toco.ls of UV im.diation induce facultative pigmentation in
White (skin phototypc.s 2-3.5), wh<'lt
involved L11 nrdvation by t.JV and to whni
extent the: induced pigmentation .is protec.tivt:.' against sub-
SL'<}U::nt I.Jv irJdiat:ion. DNA repair in epidermis tepe1lt-
ed!y imdiati:d by UV is 11 very comp!e.11. process (19,22.,23}.
We compan-:d various biomarkers in humn.n skin inaclir.red
with hrcc. different l.:N irradiation prot.ocal$, in
cumulative UV doses of 1900, 2900 aud 4200 J/m:?. {Fig. I)
(16). The pmtcins examined included motr.ki:rs of melano-
cyte activation (e.g., tyrosinase, .MlTF and Pmdl7} ilnd
also w.arkers of cellular damage (e.g., CPDs. kvels of p53,
pll, npoptosis, etc), We previously reported thOlt incn::nscs
in CPD levels and the nuclear of p53 are sig
nificandy higher in skin thr.n in Black irradiated
witil ll single 1 MF.D exposure {14). The results now
..
FMI f!NI
ne:dM
A&a c:
+
"
figure 1. W irradiation pmtoro!s used ir 1his study, Hi>tograms show
:lldividual r.JV irratoii011 do><'S on d;ys on lha absossa.
::!! A, 2 a11d C are 5hown .l!i
r:nes using 1!':1! to rig11I .and l900,
29DO and ..t200 Jim'. resper:tive!y. Hops:es ir.l<.i!n 1 OilY ab:r the
iin<ll uv irradlafon nne<J. i.t'. on day 24 fo; protocols A and il, and or.
<i:-1 3 i for pi olea!! C .i!nd ;he unirr3;:ra!i!d t:M!toi.
MQ daim to Ofigina! US. govemmen:
Biomarkers of repeated UV krildiation of human l
reported indicate that UVlnduce<l. facultative pigmentation
in fair skin is iess effective in protec;ing suhsequer.i
1..i"V damage than is cmmitmive pigmentation in rhe
Materials and me-thods
Study subjects
Thls involved 2l vofunteer subjects with skin photo-
types l-3.5 who were recruited from W;rshi1.gton,
DC metropolitan o.m:;!, Sx, age, phototype and .M0 of
these subjects <Jre given in T<tbk l. This wns
nppmvcd hy ;he FDA Resc:uch !nvol'ling Humi!n Subje;;ts
Committee (#OI-026R}.
UV i.mtdintion and dosimetry
Throughout thi!i repori, UV dos<:.S are expressed in ery-
Jlm
2
, i.e. J/ml. weighted with the Cl refer-
ence <lr::tion spectrum for erythema {24). The UV
irrndiation protocols in this study have been prcvi-
ou5ly described ilnd discussed (16}. The MED rot each sub-
ject w.r; determir;.cd as previously dtscrib.:d {16) l.lslng un
array of !! Kodacel- tllteted (Eastman Chemica! Product!>.
King.'!Port, TN, USA) FS hunps {FSX24TI1/U'V.BIHO,
Naiional Bio!ogiCill Corp., 1'winsburg, OH, USA), Fm
.repeated. t..rv inadilttion, we a 12-lamp UV soum!
canopy (SunQuest l\liodel SQ :200DS; B'fS, Jndi:.mapoi.is.. L\!,
USA} equipped with 100 W lumps (Beach Sun; Light
Sources. Ornngc, Gfi USA) emitting 5% l.}VB, commonly
>. Stud-{ 5l.Ji:lj('CIS.
..
. .
Subjl!ttno. Age Se.!! !>hate'YpE!
wrn:;
.::. . . ...
;,""' . . ;;.
..
T7 f 2 :ails
ts AO f 2 2CS
T9 il3 M 2.5 HIS
TlO .28 f. 2.5
Tfl 23 f 2.5
Tl2 M 2.5 235
Tl3 50 f 3.5 355
Tl4 40 J J70
T16 45 M 2.5 335
....-."?
i 'l 38 f 2 . .5 331)
TlS 30 f 2.5 291.i
TI9 34 M 2 195
no JC 'F 9 185
ti!' 3S f 2.5 320
Tti 2'4 M 2,5 330
1"24 ;2 f 3 6]5
us 29 lv1 2.5 :ZCfJ
Tis 26
:-;
2.5 2;:,!.5
Ti7 11 F 3.5 :.?20
121!
.3.1 2.5 2io
..
T3u 27 r 2 ps
iuurr.el 'll 2001: lllad;wz:!l Drmrlillolot:jy, 17, 917 I
Material may be protected by copyright law (Trtle 17, U,S. Code)
I
I
.
I
I
1
I Yarnaguchl et al.
used in canning s:lions. The spectrum of this source w;;s
pre'l'iously shown in fig. L of Ref. (Hi}.
We app!id three different repeated UV irradiation :regi-
meo5 (ProrocoJs A, B a.nd C- Fig. l) on three 3 X 3-cm
areils on the back of each subject, as prcviou.sly dcsctibt!d
{ 16). Cumulative rltlscs were 1900 J/m
2
, :.?.900 and
4200 )/m: fur protocols A, n and C, respectively. The
put of borh UV sources used in this study was
using il double-grating spc:tttoradiomcte.r (Modd 754;
Oprronic l.aborawries. Or1and(l, FL, USI\), \"'hose calibra-
tion tnlceable t{) the National Institute of Standards :tnd
Technology. We used a low detector {SSD
lnternat.ioni\1 Light. Ne\vhuryport. lvi_J\, USA) before ea.::h
iT;)diatioll to determine rhe correct expnstm! time fot ca;.:h
of the three areas of skin.
Skin biopsies
Shave biopsies {4 mm diamercr} skin wcri! taken from
the 3 VV-inadintcd sites 1 day :;ft!!t the last IJV irradia-
tion, i.e., after eight imdiaJions (day 2.4) for protocols A
a.,d B, and after 10 irracl1arionll (day 31) for protocoi C,
and from a:1 adjllcent unirradiarcd area as ;; c:tlntrol (on
clay 31). Each biopsy W<lS pl;:.ct'd dermi> down on a
Millipme filrcr and was then fixed in 4%
embedded in pamffin, sectioned at 3 flrnthickncss nnd
mou..-1tcd on silane-coated glass slides.
Melanin content
Mel11nin r:tml.ent was amtlyzed in sections fixed and 3ec-
ticmed as noted above. Specimens were stained for melanin
using the method (25) and were quanli-
tllied l!ll p:;e'lious!y described {12,];}). Melanin content was
am!ly2ed U!.ing a Ldca DMRB/DMLD microscope (Lei.::a
Microsystems, Bannockburn, JL, USA}, a Dage-MTL 3CCD
3-thip co)OJ' video (Dagc..,MTJ:, Michigan City, lN,
USA) and SdonJrnage soft'o'\'are (Scion Corp, Frederick,
MD, USA) from the density in given of
!:he epidermis in each section, as described
( 12-l-l). '.llu! Fontana-Mo13son .stain correlates wc:ll with cu-
mdanin contem in lhe ski.n, but not with pheomelanin
content ( 12). Using rhls approach, m!!hmin content:; were
.me2Sutcd before and after rcpeot.ed IJV irradiation, and are
rc:purtcd in arbitrary units {AU}.
ll1ll!lunohistochcmical analysis
specimens we.rc mounted on sila.nc
.::oatd glass and were prm:essed as previously
( 14,26,27}. Briefly, !ipecimens wcr!! deparr.ffinized
twkc with :-.:yle.ne fur 5 min and were then dehydrated with
:1 gr-aduated of cthrmnl, followed by antigen retrieval
through belling ir. antigen unmasking soluliun (Vector
l.abuni!orie:;, [nc., Burlingame, CA, USA) for 12 min. They
were subsequendy incubated with IH% goat serum (Vector
Laboratories) for 30 min at 37C, ;md then with primary
nntibodies in 5% goat serum at 4"C ovemighL Secondary
antibodies were appropriate fur the primacy ;mtib(ldy,
Alc,;a Fluor 488/591 anti-mouse or anrirabbit JgG (H+L}
(at !:500 dilution. Mol.:!.:ular Lnc., Eugene, OR.
USA). Staining was :mil quantified ushlg a leica
D:v1RB/DMLD fluorescence microscope <Jnd Sdonlm11ge
lmr.ging software. The tluon:sce11ce intenoity was calculated
for .specific llreas in the and lO randomly selected
nreas were qunntif1ed for each point. An internal cun-
lrol was used time to control for reprodudble anti-
body staining. Fluorescence intcmiticl' for antibodies
detecting DNA drunage and melanocyre-spe<ific
\"en: normalized ngainM DAPI t.fainiog. The following were
measured:
Meltii!Oc;'IC density
Meklnacytes wue tmmted as c:ells positive for tht expres-
sion of tyrosinase, MART -I, Pme117 :md .MITF, and their
density along the:: ep.idermal:derrual border hi expresserl ru;
ccll>/mm. Primary antibodies used were <l!PEP7b {at 1:750
dilution) to detect tyrosinase (26), DS {al 1:20 dilution,
Inc, MA, USA) to detect M1TF,
HMB<I-5 {<'t 1:100 diiution; Dako Inc., CA.
USA) to detect GPIOO/Pmcll7, and Ab3 (;;t l;Jl)O diluli.on.
NeoMarkers, Fremont, CA. USA} to detect MART-I.
Scionlmage software was to semi-qunntify the grcc.it
and/or red Il:loresccncc intenl>ity of each primary antibody
from 10 random imagc:s photographed in cru:h S?:ction,
DNA clnrtJage
CPDs were detected by immunofluorescence u5ing a lhy-
min::! motJse monodonnl-2 (TDM.-1) antibody (:;t
1:40 000 dilution) (28). The TDM-2 umibody binds TT
and CT cydobutane dimcrs in 1! do:sc-dependem manner at
liV doses lis low as 0.5 J/mz (29).
p2J COnti!l!t
Primary antibodies used were anti-human p21 W.:\l't!CipJ
(#1\17.202, nt 1:25 dilulio.n, Dnko, Glvstrup, Denmark}.
p53 c011tem
Primary antibodies used p53 (#9282, at l:lfJO
dilntion, Cell Signaling Technology, B,;:vcrly, MA. USA),
and phospho-p53-Ser46 (#'2521, at I :100 dilution, Cell
Signnling) .
Apoptosis
An ApopTag in si:u detection kit {Se.mlogicals
Co.rp., Norcross, GA, USA), based on the terminal deoxy-
r.m.:leotid)'l transfcr.:tse-m1!dinted dl'TP-nick end labeling
(TUNEL) assay, wns used according to the manufacturer'&
protocol, detailed in ( 1.4).
1918
No claim to US VJOJi:s
<ti :woa Munksgaar::i, &pel;rnemai 17. 91 O-S24
rr
l
:.:
.
i
J
'.I
.
i
{
I
'
l
..
;
II
'
1
,I
<
,
Material may be protected by copyright law (1itie 17, U.S. Code)
.. -
:ry
ly,
L)
R .
ge
eel
ecl
tt
.cs
:rs
re
!So-
dr
as
m
n,
F.
r\,
ll,
L
Y"
at
T
at
),
JJ
Statistical
Vnlui'.'s ue repoMed as means SE:IvL All analyses, h:aclud
ing Studem's r and the estimation of ;;ortelatio.n
Fig1.1re 2. Melanin in the cpi::lemm; visualized by
Stilin!n9 alter ;epe;ued Repre.sent.al.ie cf
ftCrn subjKt TtR Dashed lin<!s in arl figlires reprto!Ent the
epirlermal:r!ermal bo:der; scllie bar = 50 Jm. lnset: ot
iacull;;tilli! skin pigmentat!on clk:itecl by three W l!radiatiol\ pratoco!s
compared w!m the control sile (SUbject no 23).
Biomarkers of repeated UV inadiatiM of human s'c'in
ccefiicients and P-values, were comh:cted with SPSS 10.0
software (SPSS fnc., Chicago, H., USA).
Results
Melanin content
The 5kin photettype, gender, .,.ge <md MF.D of !he 5uhjects
in this r;re reported itl Tnble J, The UV irradiation
. prolc.:(Jls llTt! shown ln .Fig. l, which give1< indivkli4al doses
and the cumulative doKe over the course of the
Note that the biopsies {Qr protocols A nnd B were taken Otl
day 24 while 1hc for protocol C anrl tho: unirrildi
aterl control were taken nn day 31 { 1 day after the :final
iuadiation}. Representative microgrnphs of melanin smim:d
jn the epidermis and the pigmeotation vjsihle in sludy
:m: 5hown in Fig. 2. Increased melanin content was
visible in :Jli subjet::ts nth::r all UV imdintion proto-
cols, and corrclaled 111ith cumulative UV dosts.
Md:mio cnnttnl wns quanti11ed fo:r 14- subjects and .-:nm
bined data show that after compl.etion of protocols B or C.
lhe epidermis contained ..... mcl;min than the
controL Even the average 60% increase :in melanin contellt
afrer protocol A was statistically sigailkanr (Table 2}. How-
fVer, there was no significc.mt in melanin cQnrent
between protoculs B nud C suggesting that the
system v..-as dose to maximal stimulation at doses.
D1llll1lre !l!ilorted il5 'ScM; NS"' "'P <: o.OS; .. p <:vAll; *'*P < 0.002 C0:'!1PJlrad ta ur.ir(lldi3ti:d ...
1
Data lor s.;;lljeru bl!lom .<nd 1 W.<=1i<' after a ;ir':{)!e: 1 MED UV irfildtatlo!l in Refs ( 12,13}.
fon4 subid (T12-Ti4;=-T17-""ra2, . . .. . . .. .. : .
r ..... 1 ...: .. ,. "') ...
.........
,:. ....... ..: _ .. l . - ! . ::."' .. :. :: ...
.,..s!e
.. n,., .. , J,,.,, ,-r4.::,
:; !mor"'"' il> F mi1!<1110CfU!5;'(nm.s..,n. .... ... , ":. .; . ..... ... : .. , ., ...
tor 9 subji?ct!i 'urbJtr;;:y ftimd<fod .. 1!'\"F. .. Pwel17 nnd
: . ::--... , : ... ,;"'::.': :.:;:;:;: :
. 'fof(o __ sl<ii ' .
:
,. ' -- t =
; .... ,., ". . ' .... ... ' ' ...
for 7 st&ji!C'.S 11 i.t :t rttl'!}
, 7., rn 2. t:!4-!;29} 53' p!Jokphoryiated st S:r4tm_m skin.
fo: 1.3 07-T!Q, T1J-;TI4, T17-T2:?. T?4-::T:2Bi},P.1l<ted (f!I!W.rn SKin.
fo: 7 sutjec.tsH12, ti3. Ti+:nsl re:P.Of. ": : ' =
. .. . - .... ,, ........ ,, .. , .. ' ....... ; ,:, .
:-t;, claim :o criginill J5 worl;.>
Journai l:;:lmpilatio!l tl 2.00S Fxpi!rimcn!ill Dermaltl/cgy. 17, S16921l
Material may be protected by copyright law (Title 17, U.S. Code)
919
l
I
I
I
r
j
I
l.
'
l
\'
I
i
l
I
:
l
l
I
J
l
J
I
l'
t
r
,.
I Yamaguchi eta!.
This with our ob:>ervations on the effects nf a
single 1 MED l!'V irmdiation [shown on the right side nf
Table 2, taken fmrn {13)1 whh:h showed no .significam
increase in mdunin content in White skin within 1
Melanocyte density an<! function
Mela:nocyre .io the skin of the 1hrec liV-.irmdiatcd
sites (assessed by counting t:dls in the b<lsal layer of the
c11idcrmis that \-rene J)(..l5itivc for MliF, Tyr, Prnell '7 and
M.A'ItT-1) aiso increased signlfir.antly (rv3-fold) compared
t>tilh the or mehH1ocytc.s in unirradiatcd
{Table 2}. There wen: no significant differences in melnno-
q;te density z.mong tbe three UV-irradintcd sittU; ir. tht 15
subjects ana.lyted. Again, rhls contrasts whh our previous
study whkn shown that there Wil.s uo increase in rnda
noC'}te density in White within I following :1
:;ingle J MED UV irradiaiion ['f<tble 1. Iuken from (13)1.
Bxamples of exprc:;:;ion of mel.anocyte-spedflc proteins
in skin subjected to the three UV irradiation protocols are
shown in Fig. 3. lncrttl.Scd of all four specific
melanocyte examined (iyrusinasc, MITF, Pmelt7
.-md MAltr" l) following ti'V imclia.tion WM dramatic
ana!ysl$ of exprer.sinn levels of tyrosinase is
shown in Table 2). Tyrosimm: apression in tJV-irr.tdiarcd
.A, B and C .increased 2- to 3-fold compared with
unirradiated skin but there were r.o
1n e:xpression of ty:msin:tac among the three UV-irradi;!ted
sites. Similar im:rcilsc.s were found for, Prnell7, wl.A.RT-1
and MITF, although the latter protein is !css abundant and
n fuctar .is primarily lor.:alizd in the nudci
Figure 3. Expression of proteins re!)G)red I..'V
im;.CiiJtil:ln stair.i!d fer IYR (gree:l, top
1
eft
p5ne:! in each grcup) .1ad for Mrrr {red, top right in each group}
from subJect "f?.1 at th!.! three site$ at lhC!
unirr cor.troi Site, Also c.re stoinerl
for ?me! 11 {J oottam :ef; l:1 e.Jdl !)roup) and ior MART-l {red,
bottom right in <.<<u::h group) irom wbJP.ct i2S. b01r "' 50 pm.
Our previous had shown 3 .slight, bet not stntistkaUy
significant, increase in expression of those fin.:r markers in
Whirc skin l week after a single l M.D UV irradiation
lTable 2, taken from (13)f.
M.arkcts of cellular function and damage
DNA lesimrs
To DNA damage .in skin lrmdiau:d by the three UV
irradiation protocols, Wf measured levels of CPDs in the
cpidennis. E.umples tlf sections LJSed fnr CPD a.nalysis are
shown in Fig, 4. Those same st:ct.ions siained 'Vlith DAP1
show that Ute damage was localized in oudci {as expected),
anci cost"ining fur Lyrosinns\! .showed that mehmocytes we.re
among the that rontni.ned CPDs. Campared io
cliated control CPD levels of the 18 subjects measured
we.re signifk:mtly higher ln skin from all three UV-irra-
di1tion sites as were the m..tmber of C.PD-positive cell.c;
(Trlble 2). There wrus no significant difference between CPP
in u"Virracii;;tion pxorm:ols A and B, but CPO levels
in UVirri!dia!ion praiocnJs A .and !:1 were liignificantly
higher than !11 protocol C {P $lUll). We also tbc
between melanin coment ;mci CPD ievelli i.n
the rhree UV-imdiarion sites, and found that UV-induccd
CPD damage correlated inverseiy :md signifi.::ardly with the
amount of melanin !R
2
::: 0.210, P < 0.02, 11 "" lS subjl:'crs),
p53 expr1!5sion
Representative .images of p53 c:l>.-prcssion and its nuclear
localization arc ghown for skin spt.:cirnen;; taken l day after
repeated UV irrndiation (Fig. 5). Combined data for seven
subjects 2) shows that the r.umber of p.53-positivt:
Figure 4. ol C i'Os 1n the epiaerrnis UV
irradtali::m. Rl!prcsentat;y.- images or !rained for CPO (t;r;;er.)
at the <iref! UV..frmcilled siles and at mntra! t:r:im1diared site
(laken from sun)Ki ii11. Staining fOt TYR (red) is tJS.:d 10 !oca.!i:e
m:!far.otyles; OAf'l shews nuclei; ro1!c hilr = 51! Jtl'll,
No c:'ia1m tO o:il)iroll US go,ernrm;m wetks
J::Jl.!ma: E!tperir.:eJ>/211 Dem:a!aiog.v, 11. 916-9211
Material may be protected by copyright law (Title 17, U.S. Code)
I
...
!
'
J
"!
fi,
:
l
.l
!'
:_
.
:{
.{
i l'
a. f
>
!
i:(
"
j
'{
'>
[
l!
.j
,:.
"
,.
J
,,
.t '
, .
"
,..
.,
,,
;;:
;,:
; :
..
:-
,,
..
)j
'
;L
lf :.'r.
1
}1
.,
'
11
"
<
f
i
.
<
.
, ....
' .
;
:!
..
;
"
''
ai
.t
g
5'
'
ii
l).
:iz
Figure 5. cl verlou) ar c<o-llu.ar clarr.agl! and
proliferation in th!? t'iJidtrmis afw :ep!!ated IN lrradlatlr:m.
specirner6 fa' p53 to::t :t; each
gro:Jp} at the three l.Nirndi;;.uon stes and 11:1irradiateci control
(t.1k!?n fr::;m subject 128). Nso $hown are (green, rop 1ighl pan:;l
ln IC.'l<:l) group), p53 S<!r46 (glf;>l!n, bottom ;:tM!ll in each qroup} and
pti (green. hoH.ilm right pun!?l in each gmt.pl; >C3Ie bar"" 5(} p"l.
cells w-JS signiiicomrly and dramatically highl!r in skin from
all three tJV irradintion protocols compared to
e.::l controls (which had almost uoclctectnble nwmbets of
p53-positive cells). Thete was no significant clii-
feren.:e het-.veen UV -irradiation A and ll in tht: num-
her of p53-positive c:c.lJs/Jnm skin. the number of
p.53-positive cells in l}V-irradiation siie C was signiliomdy
ami dramatically higher than in UV-irrndiation shes/-. a:nd
R {P < 0.01). The number of p53-positive cells correlated
positively with melanin content 0.305, P < 0.05.
11 "" 7) but ncgative.ly with the number of CPD-poshive
cells (R
2
= 0.912. P < 0.01. n = Hl).
Apoptolis
R\\llutt-; of n'll\;"EL staining revealed that levels of apoptosis
were! signific:mtly increased in to repeated UV
with unirraruated skin {Fig. 5,
2). However, the number of TUNEL-positive llpopto-
tic. cells was rclatjvely low und did not differ signifi<antly
among the three UV-irradiRtion 5iles. !n nn ;:arlier sludy,
we similur TUl\lf.L results for :t single 1 MED UV
irradiation {14).
Phosphorylntlon of p53 at Scr46 is an impurtnnl post-
lr:n"..smlional modificatiou tlu1t the f1.mction of p53
to induce apoptosis Jn response to stres!>. While no
Ser46P- cclls could be detected in unirradiated
control skin, significantly ittcrl!'.lsed nwnbers of those cells
Wl>re found b skin irrodinted b)' all three UV irradiation
protocols (Fig. 5, Table 2.) unlike in 1he samples from the
previous si.;gle I MED UV irradiation t U).
Nt'l :a orcgcnc!IJS uovemment wor'..:;;
Biomarkers of repei!!ted UV irradiatio11 of human skr;;l
p21 expression
Staining fur the cell c:yck rnarker p2 t revealed Lho:t the
number of p21-positivc Cti!!ls was t>YCri!mely low in
ated control skin but increased significantly following all
three protCJrois of rcpc!itivc l.iV 1rradia.tion (Fig. S, T<tble 1).
Discussion
.Previnmly, we reported the effects of a single UV irrad.in-
don at the level of I MED on human skin of different pho-
ttltypes [5,12-14}. However, ln real life, human 15
repe:1tedly !rradiared by UV emitted by 1hc sun, by thera-
peuik devices :mdlcr by indoor tanning equipment. Such
exposures can be carcinoge.!lic. The repetitive nature of the
contributes the complexi\y (If the moleculilr a:td
cel!ulur phenomena elicited. st,tdy explored the dfccts
of three protocols of repetitive UV irradiation:; that result
in !>.kin pigrneatation. We fotmd that some
cancer-related molecular and phenomen;l correlate
cliffcn!ntly with pigmentation inducf:d by repeated VV
irradiations { i,e. fr.cultative pigmentation) than with
constituti.\.:: skin pigmentatiosl.
We used three experimental UV pxotocols, A,
!l and C (fig. ) ), whkh resulted in cumulative do;;cs of
1900, 2901} and 4200 Jim:!., respectively. UV irrodiat!on
ncconling to eac:h o! those protucols stimulated skin pig
mentaticn vcz: effectively. Protocol B produced darker pig-
of the skin th:m did protocol A, however the
diffcrcm:e between pigmentation prcxluced by protocols B
and C at the end of thr. irradiations wu:s small as a.w:ssed
visually {inset of Fig. 2) and could only be derec.ted in.mu-
rnema.IJ.y {30). The resulrs of Fontana-Masson staining
{fig. 2) confirmed increases in pigmenl levels
following ruch of the three UV irrodh::.rion protocols.
Althoug., histologically there see..-ned to be a diffetcnt:e in
overall melanin content between protocols B und C, only
small in mdanin content were measured quanti-
tatively (Table I}. This cormhnrated what was se;:n by
visual e"l!alnntion fullo ... ing irrnrliarion ncc:.orrling to proto
cols Band C.
In our previous studies, a single dose of lJVB-rkh itradi-
ntion at lhe 1 M ED level hnd negligible effect on melano-
cyte dwsity in the skin within l week post-irradiation
taken from {12,13) arc included for compnriscn in
Table 2]. Tn the presem study, md:mocyte density was sig-
nificantly increased following .repeated UV irradiation givt<:n
over 3-4 weeks, and the three U'v' irradiation protocols
tested wel'e similarly effec.th:e (T;;hk 2). It is possible th:rt
melanoqtes in control skin may be p;cse..1l
but their specific matken at levels too low tn
be de!eclt:d. However, '"e do not believe this to be the
case smce we tne:lsured melanocyte density based ()$) the
Journ;;l compaaton :woa a;a:::!(wef: fxP<!rimenra' De:miJialugy, H. 915--924 921
Material may be protected by copyright law (Title 17, U.S. Code)
I
I
!
I
l
I
I
1
l
I
l,
!
t
I
I.
l
I
l
i
t
I Yamaguchi et a/.
el!.-pression uf a ;-ariel}' of melanoq.1e specific: markers, all
of \"hit::h gave cornpamhlc number!> at the time points
F1.1rther, in our previous study { 12), m used
identical and antibodies tQ show similar densi-
tiS nf mdanocytcs in unirradiated skin of the various
racial tlnd et.hnk groups examined and those densities did
not within the: first wee.'!.: uftct UV
The nmourtr of DNA d:J.magc mc:t.surcd as CPO in the
epiden:ois Wil$ dr.:tmnticnlly higher :tfter repeated tJV irradi-
ation ncccrding to all three protocols compared to unirra
tbated skin (Fig. 4, Table .2). lntt:.restingly, CPO levels were
significantly lnwcr after protocol C compar.::d wilh pmtG
cols A and B, both when as overall intensity per
am1 of or as the number of CPD-positive calls per
mm of skin which suggests a photopmtective benefit trom
the facultative pigmentation .induced by the repetitive UV
irradiatinr.s. A similar phenomenon wa..:; reported by
de Winter ct ul. ( li'}. In their study, 9 irradiations given
over 3 weeks resulted i:1 iower CJ:ID levels after a UV chal-
lenge tlum those obscrvi!d in unlrradintcd controls. A
recent study {31) reported that e..:prc.ss1on of DNA repair
enzymes in skin i.t1creases significantly foHowing various
types of J>trcs.s, .including UV irradiation. Hence, DN1\
repair kinetics may be altered by differenr
courses nf 'UV irradintion. However. neither de Winter and
co-workers nor our groul' a5e$;ed DNA damage during
the course of repetitive UV irradiations ro e.xrunine the
kinetics of CP.D genemtion and DNA rep;,ir. Sud1 are
needed to fully assess rl.iffenmces in .DNA damage caused
by diffcnmt UV irradiation regimens und for
tion of longtenn effects of these UV dcu;es. Additionally,
many biomarkers oilier thn.u CPO arc required tl
the photopmlectivc effect of UV-induc:ed pigmentation <!I
occasionally sun-c,.,"Posed
An intere!>ting. recent study (32) showed thut lhe type of
lJV used io irradiate human ilin li and TIIJ had
important consequences on effcxts in the epidennis
dermis. Tht study m;ed a repetitive t!V irradiation proto
cui that irradiated skin to 0.5 MED u'"V (96% tJVAf.;%
UV.B) 19 times over 5 weeks. That is a similar tJVA/UVB
ratio a.mi time course to OI!X study but contrasts with
respect io ibe dose protocols in our study. 1'hat
study alo;o used buttock skin, normally c-onsidered a
protected site, compaied w om whkh used dor!'o<!l
skin, c::onsidered nn occasionally sun-exposed site. Never-
theless, that study reported 5ignilicnnt in skin
color, p53 nudeac UCCU!Ut.dation, mdanin st:ahting
(detected by Fonlnnn-Masson), more dcm.lritic DOPA-
positivi! mclano(;)'tc:s and only a lilighr im:rcase in apoptutic
.::ells (sunburn cells). Those parameters are similar to what
we cbservd in this study whkh suggests that UV resporu;es
an; cumparable in different anatomical locations n:gardbs
of UV background. More Young et al.
(33) reponed "smcly on hllman skin (types r :md I!} using
repetitive UV irradiations. (ll irradiations of 0.5-{).6 :M.ED
pc.r cht}'), again on !.'Unprotccwd butted iki.o, They
reported the preventive effects of a on D-NA
damage ond p53 acs:.umul'lltion resulting from the repeliti,.e
lJV irradiations .:md also not.cd that virtually no apoptotk
cells (sunburn cells) were seen in clle UV.irmdi<:red
The low level of al'nptosis in bullY.ln skin following {e.pd
tivc UV irradiation may result from decreased expression
of the Fas ligand. In 1hat n:gard, ll recent study .reported
that while Fas ligand is relatively strongly i:Xpressed i.n the
basal of the epidermis and weakly expressed i.n the
upper la.ycr, it became totally negl'Jiv-i.!
UV irradiaiion {.:14). The sum of those results is consistcm
v;ith the and intcrpretutions in our
stmly.
The p53 tumor supprc_'l.!>or protein plays several .impor-
tant in the inhibition of photoc:m:inogt!ncsis_ 1t
cnh;;nccs the nuclear excision repair of DNA
damage, de\;;;'S cell proliferation to provide time for
repair, a.nd (foUuwing its phosphorylalion at stlrnu-
latt!s apoptu,;i!; (20,.35-37). p53 prori!in accumulates in !.he
nuclei of skin cells after UV irradiation (38) and expression
of p53 in the skin can serve as a risk marker for sldn
cer in humo.ns (39}. We previously reported t.l,at following
a single I Ivllill t.TV irradiation: (!) incrcnses in CPD kvelii
and the nuclear of p53 are significantly
higher in While skin !.han i.J1 .Black skin despite the fact
that the latter received up to 4-fuld more UV in physical
{13,14), but (2) the number of apoptoti1: ccl!s is sig-
nificantly lower in White skin than ir. BJnck skin (H). The
1csults repiJrted in this study (Fig.. S, Tiib!e 2) show !hat
p53 increased significantly w!tl1 increasing
cumulative tJV dos;;o.:;, i.e, it corrdaied well with increased
ikin pigmentation. Although this scerru; to conlmdh.:t om
p1evious report on p53 induction in skin, we think it sim
pl)' highlights the fuct that facultative skin pigmentation is
distinct from constitutive s!cin pi:gmi:ntalion. The increase
in $kin pigmentation eliciied by UV- irradiation protocol C
t<.ignifkantly higher level:; of pS3 nuclear accumula-
tinn thr.n seen after protocoh A or B (Fig. 5) and p5.3
wilh mdanin contenL HowcYer.
neithc.-r the rat.: of apaptosi {meilsured ilS TlTh.'EL-pos'itivc
cells) or the levcl of p55 pho5phorylation at Ser46 showed
a dosedcpend!!llce, illlhough levels of p53 and pll wt:re
dose-dependent. p2l in the skin after UV inadi-
<ltion can regulated by p5J-depcnJent and by p53
independent pmcc.s:.es; a recent study sho\,;ed the
p53-dependent trnnscriptioni.ll activation of the p21 pro-
moter whkh may be involved Jn tl1ill process \Iii). Again,
lack of data regarding c_."l-jar.ges in end. poinrs t>:Jrliet
stage;; of the e.x:p<!ri..'llent should be The eJ>.ttemely
low level of TUNEL-posltive cells is cons[ste.'lt v.ith ailt
No clal:n lu ori(linal US worb
klurnal cumpllatlcn@ 2ooa 51oci:well Mi.mksgaard. t7, 916-924
Material may be protected by copyright law (Title 17, U.S. Code)
earlier .single tJV dose !itudy (ll}. Very few TUNEL-posi-
cells arc ''isible in White skin nftt:r repetitive UV
irrJdi:trio.o, and litis is consistent with other recent reports
!.s.'laT found very low levels of a:popiotidsunburn cdls in
White skin after repetitive l.JV irradiation (31,33}. Signifi-
cantly iocreased numbers of TUNEL-positive cells were
found in darker skin ufter a single l MED UV irradiation
in our earlier study. The !:!fftcts of repetitive UV irradiation
on darker skin remain to be explored. These low levels of
apoptosis, which pote.r.tially couW redu.:e t.i.e risk of skin
ca;rscers from UV-mutated cells, would seem to be nlrnost
negligibk in White skin due to the low numbers seen, and
one could t.,;at they are too fu\v to be ph}>siologka!Jy
relevant.
While unalyzjng these fuldings, it is pilrncularly interest
ing to juxtapose the CPD and p53 dose-dependence data
for repeated \"S. ,acute UV ir;adiatkms. In both cru;es,
In nude<!r acOJmulation of pS3 correlates ""1th
increase;; of UV dose. This is comi&tcnt With the findings
of a study on subjects exposed to 6 weeks of natural sun
light (41). However, while higher ncute UV doses lead to
formation of more CPDs, the incr<!ll.Ses in
rcpedtivc UV doses result in lowering the CPD lcvcl {at
Je:JSI in the dose range explored in trus study}. 11 is tempt-
ing to speculate that the increMes in p53 llccumulation are
rnec.h;mistica!ly different in the twa cnses: \vithin l day
after a :;bgle uv irradiation it rugnifics <lfi initial, perhaps
primirive rCSpOllSi!, of d\e dcfcnsi!
tYhile after numerous irradiations - ancl
gi\'cn more time- it may refk'Ct development of a mature,
efficient defense This hut o11e
tion fur the decline t>f CPO levels at ilie higher cumulative
repented The of Stlt:h a put<ttive
nism for c;m:inogenet;is would depeiid on the fidelity of the
c:ellular defense system that during repi!<itad li'V
irrndintions. Further )nv!:Stigatlons of DNA damage,
chungcs .in ilic: p53 system (induding p53 mutations) sod
apoptosi:; i.ndaced by repented UV irradiation will be
to fully assess tht: c:arcinogenic d$k of such v'V
irradiations.
Acknowledgements and Disclaimer
This research was s.upported by the Office of Science and
Center for Devices and Radiological He.Uth, Food and
Drug Administration {FDA), by the lnttamur.tll Research
Prngrnm of tla: Nationlll Cancer at l\TfH, by a
grant-in-aid from the Ministry of EduoHion, Culrun:)
Sports, and Technology of Japan, and by the FDA Office of
Wo.men's Health. The opinkms and conclusions stnted in
this paper are of !he :mthors nnd do not :represent
the official position of the U.S. Department nf Health :.;nd
Humnn Ser..-ices. The mention of commerciai proclm:ts.
No dilim to US gcwemment wo:ics
Biomarkers of repeated UV irr.ocliatiol'1 of human skin
their sources, or their use in connection with
rcporied herein .is not to be construed as either ;;n actual
or endorsement of such products by the U.S.
Dcpartmo:;,t of Health a.nd .Human
References
'I K"idbl:\' l< H, Agin P P. Sayre il M. Kligm"r. AM. Photoproiection
hy - a oi black and skln. J Am Ar.ad
Cermatol i979: 1: 24!t-2c0.
2 Kollias N. Saym R M. L, Chi!de.k.ei M 11. by
melo'lin. J Phuta<:hPm i'hotabiot 1991: 9: 135-H.\0.
3 Slomlnsk.i A, Tobin 0 J. Shibaha1a S, Wortsman ), Mlli;min pigmen
1aticn in mammalf.ln skin <lnti its hcrmcral regulation. Phy9ol ll!ro
2004: M: 1!55-1223.
4 l<i:Jdelcaro l'o 1.. Wakamatsu K, Ito S, AbdelMaitk 2 A Cutuncous
photca;:rotec!ior; and beyond cr.el
anir; to the frontiers of DNA m;:ar. Front 200!1: 11:
2i57-2173.
S Y. Coeihc S G. Wolbl!r R er "' Rr<gt:l3ticn of
pigmentetion to ultrolviolet radiation. Piyrnent Cell
i!e:; 2001: 2-13,
5 Young A ft Tanning de11kes - fasl !filck to sldn c;mcer? Pigment
Cell R120.34: 17:
1 !.evlnC! J A. 5orac!! M. Spencer 1, 5legl'1 D M. The indoor VV Ianning
ildustr{ a revie-,rt of skin heallh benalil d,;ims, and
regulation. JAm Atati Dermatol 2005: 53:
8 Karaj<!5 M R, Stan1'..1td V A, Mo:t L A, Sli!!!I.!J'f M J, 5 K,
Weir.stod M A. Ust> rt! MMin!J d!!vitP.S llmi r1sit of haS3l and
squ;;mous <.t:!l cancer:; J Natl Cancer bsl 2002: 94: 224-126.
9 lea C s. SCOt\1l J A, !Mtlet I' A, Fine J. I! L, iletvJick M.
Arnb1;;nt uvs and melanoma ri;k ir. tM Uniterl Ste1es: a ccse-
cootrol illlatvsis. Ann Eprdemioi 2007: 17: 447-453.
10 !ltr..aille V, Winnett A. Sasicr.i i'. N!!\vl.Oil Bishop J fl. C J. Expo
!>till! to and and the of ml!lar.om3
in tn1 UK: <1 :;aSINonlrol siudy. ur J C::ar.c::t lOO<l: 40: 429---435.
11 Galfagher it P. Spinelli i ). T K. Tanning b<:-d>, sunlamps, and
oi cutiVl!!Oll ml!iilnoma. Cancer Ep'demiol iliomark
f'revent 2005: 14; S62-S66.
12 iadokoro T, Kobayashi N, .Lmudzk.:l e Z et aJ. W:ndu;:ed ONA
cii!mage and malanin content in humtlin differing b
orisin snd FASE!! J 2003; 17: 1177-1179.
U Taookaro ' Yatni!gur.hi Y, 6<1!1er 1 et aJ, Mec:hanisms of 5Jc.in
tanr.lng b diHerenl racin!Jalhni:: !lroops in r<!sponse lo
rariilltion. 1 lnlleSt D!!rmatai ;mos: 124: 13:26-1332.
14 Vi!milgt<chi V, Tak.o:h..'Shi K. 2mwdzka !I Z et al. Human $kin
to LIV radiaticf1: P7gm;nt in :re upper epidermis protects
against DNA damage in th!: epiderm:s ar..c! li:dtitel!1S l!pcplo
s:s. FA!>Ei! J ZOOC: :w: 1186-1488.
1S Coelho S G, Miller S A Zmuozka !i Z, ile-2r J z. Quantification of
erythema anti pigme-rtliltion using computer
:gitaltmage e;:aluatlon. Phctodtem J>hotobio! 200ti; 82; 651-656.
'lG Milli!r S A, Coeiho 5 G. Zr..udzt.:a tl 'Z, Seer J 1.. R!!d:Jction of the
UV to !illlfle:S through naw llXposur::- ;cl;addes:
pilot study, l'hotor.!errnatal i'hctulmm;moll'hoiomed 2005': 2A: 59-
65.
17 de \IVimer S, Viflk A A, Roza l. Pavet 5 skill
iion and its effect or; sub5eq:;ent Windured epidermal
dalllage. J lnve5r Dermatol 200l: 117: 678-682.
1B Hemminl:r K, Xu G, KaiJSI'! l, Koulu L M, Zhao c, larsen 1. OC!mOn
.stratioo of l.iV-dime1s rn human DNA in sit.\.l 3 weeks aftc:
Carcinogenesis 2002: 23: 605-609.
Jm.amal compiJ;;tian ;?OilS B!i.<::kwel! Munl!sgaud, E:>:pe!itrn!niiiii.Deml5ta!ogy, 17, 91 G-924 923
Material may be protected by copyright law (Title 17, U.S. Code)
l
l
!
1
f
I
J
I
I
I
t
...
Yamaguchi at al.
19 Sheehan J M, Cragg tJ, Chadw;d:. C A, ll'oa.m C s. Your!g A R.
ulltilii:Ol!.!l flxposure affords tt.e same pratedio:"! again;ot
CNA phctoc!amagl;! .or.d e:ythana in hJm.;n sk;n l'Jfl!.'.S t: <md N hut
is BSVc1i!ted wilh faster repair In type IV. 1 lr.v!?st uem'l&
:ol2002: 118: 315-329.
20 Ziegler A, Jcnason A s. D J ol. Sul\b\J.m ;;r:cl p53 in the
onset ci :sk1n carv.er. Nature 1994: 372: 773-776.
21 lJ A. Sunsctc-eM- a public heaith opporcunil)l. !l!.:;w Eng J
Med 1993: 3'29: 1193-ti!M.
La Hemmlr1ki i<, E. Hmv fast ar!l LN-ditnel$ rep;;lred :n
h<.:ml!n skir: DNA in situ? ! Invest Oe!!l'lQto! 2002: 699.
23 Voung A R, C S. Sheehan l M. Epidermal O!I!A rl!pail under
co;ulilians is complex. J Oer:n.alol .2002:
119; 7(!0-702.
24 Erythema Referen<e Action S.ooctrum af'ld Standard ODie.
Vienna, AU>tri<J; CIE, 1999: 171&6.
25 8anc1oit J D. Stevens A, and of Histolog'.t;tl.l
N;;w York; C::hun:hill
26 Vumuguchi '(, ltami S, Watahe H et iili
it1ler;;c1ons in th!! of dickl<opll by pai
mop!sn;a( rnetanocyte grO':.tth ar.d dillercntia
tlor . J Ceil S'ol 200<: 165: 215-iSS.
27 Pa5seron 1, C::Jdl;o G, Miy<:ft1Uii\ Y, K. Healing V J.
lmmunohisto<l'emisuy and tissue in situ hybrldi;mtion in >!.udy
of humM skin melanotytes. Exp Dermatol 2007: ,6: lGt-170.
28 l(t:Jbayllshi II.!, Na;:agawa A. 1\;hm;matsu T ei ;;r. Supr/lnuciear
nin caps reduce ultrilviolel induced ONA pho!cproduc'-s 1n
epidermis. 1 Invest Dermatoll998: 110; 80!HHO.
29 Mori T. t11.1kane M. Hattori T. MutSi.lllugil T, r.'lara M, Niklllt!o 0.
Simultaneous ast.abl!shm!!nl ol monoc:onal antibodies specific:. for
either cyclobut.ane pyrimidine d;m.::'r or (f:i4)ph0toproo'uct irom
same :mmun1ted w;til DNA. f'Miochem
Phr:lobiu! S4: 225-232.
30 Mii!er 5 A, Coelho S G, a Z et ai. Dynamu of Plfl:l'ler\ta-
ticn indualon by UV exposures: dosl!, inii:!Nal and
IJV spectarm C:i!pendunce. <lr j Ommatoi 20GB: ;ubmitted.
31 Markmnet C, !!emero F. Domas A er al. Mocit.llatlon of ge;r.e expres-
sion iMu\:ed in human epidermis by enlli!Pnmenti!l s!fess in vivo.
J lnvesr 2003: 121; 14fi-14SS.
32 Seite S. Medais!:o C, F et al. Siolc-;ie?l effl!CIS o; s1m:J
lateri !.iltra ... io1er ci;;yl!Qht IW'IV appro<Jch to daily
f'ho!odermatol Phorolmmu!loj Pllo!omed 20Cfi:
ll: 6.7-77.
33 Young h R. Ordli!Jrl G t, G I, Klock J L ihe d:?tnmental
effects of t:aiiV expo5ure or. hum:m sl(in 1n vivo can
be pre>Jented by a brooospectrum J :nvest
Oerrna:ol 20u7: 127: 975-978
:;;4 Crb I', .li J, Wetnll M, Kump E. Gla>er A. awthr.er SA. Role of apop-
tOSlS in basal cP.Ii aml S:Cll:lmou;; i.:E.>Jl catcinoma loonation. lmmuncl
let! 2005: 100; 6il-7:1..
35 Oren M. i:-cdsion makifig by p53: life. death .mci caf\Cf(. C!!!l 0!.9th
Oiff!!r 2003: 10: 4:$1-4.!.2,
36 !<, At;;kawa H. ianaka T eta/. pS3A<PI, a potl:'nlial med!.:tor
of apoplosis. 3M reguli'ltkln by Ser-46-phosphor-
ylaled p53. Cel! 2il00: 'EOl: 1!49-862.
37 iz;ke:.u::hl 5. Zhang W. Watwl'l)l;t.Si.l K et al. Melanin atts a po:ent
UVB to cause a newel of cdl desth in murine
5kin. i'1oc Na:l Al;ad 5d IJ SA 2004; 101: 15076-!SOSL
38 Hat! P A, f' H, H o, Dever R, Lane D P. High
of p53 in UVitradiateti norm<>! human
19!13: a: 203-207.
39 da GraM Y G. Rebel H, Elgha!blour! A er af. More epidermal p53
<'!d].:Jomt to skin <:c:rd;ornas in renal traosp<ar.t recip!erts
ther; m pali;mts; role cf authlopin;:o. !::cp
.2007: 17:
40 Mouret S, r,wie! A, llcilnl J C. l..cctia M 7. Oiilereotial p5lmedi
il!!!d 10 5elilr-simt<l3ted rm:Jiillion in human paplUomalliru;
type f.xp Dermaloi 2007: Hi; 476-484.
41 Wassberg C, Backva!l H, Ciffcy B. Poni.en F. aerne D. fnnaoci!d epi-
ckrmal ultruvio1et re.>pO't>es in cllror:ic?.liy sunI?Xpo<..l!ri are
dependent on preilioi.!S sun exposure. Ai:.lu Oerrn 2003:
83: 254-251.
9Z4
No c.:airn to vr:ginat IJ$ Wl:l!'ks
iouma! 2!iGEI Blccl<v.-eil O!!rm<:tok>gy, 17, !li!i-!)11
Material may be protected by copyright taw (Title 17, U.S. Code)
i
i I
.,
.J
:l
'
:.J.
; :
i
I
'
'
f.
1:t ,.
.
###
lf
#
#
#
# #
# #
######
Job : 60
### ### ###### ### ### #####
# # # # ## # # #
# # # # # # # # #
##### ### # # # # #
# # # # # # # ####
# # # # # # # #
# # # # # ## # #
### ### ###### ### ## ### #
Date: 10/23/2009
Time: 7: 27:17 AM
### ###
# #
# #
# #
#
#
#
###
#
###
#
#
#
#
#
#####
ILL Document Delivery
ro::G-H8075 6 a
DCUDJG
NLt.t -- W1 J0'/3 (Gem l; Film SllOOO; E-Journal w/ILL access
US FEDERAL TRADE (FTC)
US FEDERAL TRADE COMNISSION
600 PENNS'I.tVAHlA AVENUE NVJ
WASHINGTON. DC 2058D
A '!Til:
PHOHE: 202-326-2395
202-326-2732
E-MAIL: libraLy@ftc.gav
SUBMI'ITED:
P .RtNTED:
REQUEST NO. :
SENT VIA:
DOCLINE NO.:
OPAC NO.:
2009-10-22 11:50:56
2009-10-22 15:10:32
REG-1480756$
DeCLINE
K'x'B-2799678'6
AAXOXNH
Copy Journal
TITLE;
Ft.JBL ISHER/PLACE :
VOLUME/ISSUE/PAGES:
DATE:
AUTHOR OF ARTICLE:
TIT.tE OF ARTICLE:
ISSN:
OTHER NUMBERS/LETTERS:
SdURCE:
MAX COST:
COP'I.RIGHT COl1P , :
OLL NUMBER:
NOTES:
REQUESTER INFO:
DELIVERY:
.REPLY:
JOURNAL OF INVESTtGATIVE DERMATOLOGY
Publishing Group. N;;:w :
2009 Apr;l2S(4):1002-11. Epub 200S Oct 23
1002-11
2009
Brenner 1>1; Coelho S; Beer J; 1'-Iiller S: \IJolbar
R:Smuda C:Hearing
LONG-LASTING !>iJOLECULAR CHlu"iGES IN HUMAN SKIN
A.PTER
0022-202X
Unique !D.:
KYB-27996796
18946".195
PubHed
S14. 00
Guidelines
Wl J073 (Gen): Film SllOOO; E-Journal w/ILL
access
jkn
Linda Henry
E-mail: library@ftc.gov
Mail:
KEEP THIS RECEIPT TO RECONCILE WlTrl BILLING STATEMENT
For problems or questions. contact NLM at
gov/ill/lll_weh_form.cim or phone 301-496-5511.
Include LIEID and request number.
NOTE: -'l'H!S !1ATERIAL MAY BE PROTECTED BY COPYRIGHT LAW (TITLE 17. U.S. CODE)
NLM Collection Access Section. Bethesda. MD
ILL Docummn t: DsU.very
REG-14807568
N01'E: - TrliS MATERlAL MAY BE PROTECTED Bi' COPYRIGHT !.A'fl {TITLE 17. U.S . CODE)
..... ------------------lll!:::tl
long-Lasting Molecular Changes in Human Skin after
Repetitive In Situ UV Irradiation
Michaela Brenner
1
, Sergio G. Coelbo
2
, Janusz Z. Bee,-:;
1
Sharon A. Miller, Rainer Wolber
4
, Christoph Smuda
4
and Vincent J, Hearing:z
It is known that UV modulates the expression of paracrine factors that regulate melanocyte function in the skin.
We investigated the consequences of repeti1ive UV exposure of human skin in biopsies of '10 subjects with
phototypes 2-3.5 taken 1-4 years later. The expression of melanogenic factors (TYR, MART1, MlTF), growth
factors/receptors (SCF/KtT, bFGF/FGFR1, ET1/EDNRB, HGF, GM-CSF), adhesion molecules {!)catenin,
cell cycle proteins {PCNA, cyclins o1, E2) as well as Bcl-2, DKK1, and DKK3, were analyzed by
immunohistochemistry. Most of those markers showed no detectable changes al 1 year after the repetitive UV
irradiation. Although increased expression of DNRB protein was detected in 3 of 10 UV-irradiated subjects,
there was no detectable change in the expression of ET1 protein or in EDNRB mRNA levels. In summary, only
the expression of TYR, MART1, und!or EDNRB, and only in some subjects, was elevated at ;:;:.1 year after UV
irradiation. Thus the long-term effects of repetitive UV irradiation on human skin did not lead to significant
changes in skin morphology and there is considerable subjecHosubjcct variation in responses. The possibility
that changes in the expression and function of EDNRB triggers dovmstream activation of abnormal melanocyte
prol:feration and differentiation deserves further investigation.
tuurr:al Dcrm<'tclogy t20Wi U9, lOOl-1011; doi:l 0. t03llliid.1D06.325: publl$hoo M!i'le .!0011
INTRODUCTION
The incidence of metanoma has tripled over the past three
decades probably as a result
1
at lea:;t in part, from lifestyle
changes that have led to an increased exposure of the fair-
!'>kinned population to UV radiation {NC! Seer Stalislie,
http:i/seer.car.cer.gov/), Epidemiological ancl d<'lta
strong evidence that solar CJ.:posure is a major
causative factor in mel;:momageoesis {Gilchrest et ill., 1999).
Emerging evidence that there is il dear link b<.!lween
tanning devices and malignMt melanoma {International
Agency for Research on Cilncer. 2007; Ting et ill . 2007j
Clough-Gorr et al., 2008). Pathomech11nisms fm the devel-
opment of nonmelanocytic skin canct!rs have alread; beer.
revealed tStvry et <Jl., 1997; Jv\atsumuril and A11anthaswamy,
:mo2). hu\vever, the exact mechan!sm(s} of UV-Induced
'Dep;Jrllrtenl of Derm,<!ology, !.tdw(trI>.I.'!Ximi!i.ms-Ur:iversiiJ' f)( !Y:unic/1,
Munich, Germany; vf Cell BiologY> Narioniiil Cem:cr lmtilutc,
N.ariorrJ( of Be!hescJ.:;, Mary!;;nd, USA; 'Cenler for Dtwice5
and Health, food ai!d Drug Spring.
M.uyl;mrl, USA ifnC R&D, S!dn Research, lh:iemlorfAG, 1-1.1mhurg,
Germany
Dr Vincent/. 1-ieilrlng, of Ce!l Natfnnal
Cancer lr.i!i!ule, N.ltianai /n;tiMes u( He<:!t}t, 8ui/ding J7, Rt..'Dfll21.32, MSC
42Sb, 8;/hcsdJ, Mal)48nrf 20892, USA f-mnfl: he.1dngv@nil:.gQY
Abble'?i;U[ons: Bc!-2, 8-ce/1 lymphoma 1; bFGF. basic gwwth
(aclw; DKK, dit::klrop(; DNRB, receptor B: ET. endathr:lin; FCFR,
fibmb/ast gmw:h /ac;inr receplm; HCF. hepatCJc:yte growth factor; ,".ffARfl,
meii!n:Jmil ilnligcn recognized by r -ce/is; MED, minimal (tyifwtn,l
MliF, micrvphthalmJa mmscription fartur: fOJ/1, proiiff!riitlng c;e/1 nu::lcill'
ol!lf(!Jtm: SCF, cell {Jt:lor; 55. simul..ttor; 'TYR, t}rosinMe
21 Junf'! :miNI; revised 13 August 200/J; ilCr:cp!ed 20 August 200fJ;
published nnllne 2 3 October .2008
melanomagenesis in the skin in situ rem<1ins unknown. r'\S
tJV-flngerptlnt mutations are rare in melanomas, il has been
speculated that UV causes melanoma development by
indirect effects, for example, by clystegulatkm of growth
iactors in lhe skjn, as proposed in a skin graft model
for UV-induced melanomas {Berking ct <!I., 2004). We h;lVe
recently shown thilt UV modulates rhe production (by
keratinocyles and by fibroblasts in vilra) of growth factors
regulating rnelanocyte functlon (Brenner et Jl., 2005). UY is
presently the only known environmental carcinogen for
melanomas, however it is still controversial which wave-
lengths are critical. UVA has been shown to promote
melanoma in a hybrid fish melanoma model (Seliow et al ..
1993}, whereils UVB promotes melanoma in several trans
genic mouse models (Noonan el al.
1
2003).
There is nn urgent need 10 determine the specific
mechanisms thai are involved in photoc:arcinogenesis of
UV-irraciialed human skin in situ. Numerous sludies have
examined the effects of UV on skin cells in vitro, however
that experimen(al secting does not allow one to explore
interit'ldlvidual diiferences such as skin phctotype or minimal
erythema dose (MEO). The examinilliOn of UV-induced
changes in UVirradiated skin in situ, with respect to different
wavelengths and doses
1
provides a more r.uilabte approach to
characterize UV photocardnogenesis !n !he skin, particular!;
vith respect to early events in the casce1de.
Our gmup hns previously reporwd s!uciies on the
acute effects of UV radiation on human skin oi varying skin
pigmentation plumotypes. So far, we have shown !hat even a
slng!e, relativety low (1 MED) UV dose {oO(Vc> UVN40/Q UVBj
1002 Journal of IJermato!om IQ ;WU\J Tiw Sot;jcly for lflV(!:Sii!lllUve D11rmatology
Material may be protected by copyright law (Title 17, U.S. Code)
i
I
t
i
1
i
/
l
l
f)
<il
f
. .,
!
&
causes significant damage to DNA in epidermal cells and
stimulates the production of photoprotective melanin (Tado-
koro ct at., 2003). Most UV-induced DNA damage is
removed relatively quickly !with!n clays), however, some
UVwinduced molecular changes might persis! and r.ould
initiate malignant. transformation in the skin. Our earlier
studies exnmined only the short-tem1 effects of UV on human
skin in situ. To extend our understanding cf the !eng-lasting
and potentially photocarcinogenlc effects of UV, we exam-
ined biopsies from sites exposed to repetitive UV irradiation
sevewl years ago. In pnrticular, we the long-
lasting effects of UV on melanor:ytes and on keratinocyw .
We examined various potential morphologic and molecular
markers or malignant transformation in two different UV-
irradiated groups. One group of six subjects had been
repeatedly irradiated over several weeks at three different
cumulative doses with Sunlamps emitt!ng a UV spectrum
commonly u;ecl in tanning salons (;;,:95% UVB)
whereas in another group, four diiferent subjects had been
repeatedly irradiated over a period of 2 weeks with a solnr
simulator (SS, UVB). The molecular
markers examined can be divided lnto six and
were sel&tecl due to their involvement iJ' melano
cyte transiormation ar.dlor becatJse man}' previously pub-
lrs,hed studies have analyzed their responses in human skin
wit.hin 1 month oi UV exposure:
a. Melanin content ;md several melanocyte-speclfic pro-
teins: microphthalmia transcription factor (MITF). mela-
noma antigen recognized by T..celh; (MARTI), tyrosinase
(TYR};
b. growth factors and their receptors: stem cell factor (SCF}/
KIT, basic fibroblast growth factor/fibrobfast gro\vth
factor receptor 1 (bFGF/FGfR1), endothelin 1/endothelin
B receptor (ETl!EDNR6}, GM-CSF, and hepatocyte
growth factor (HGF);
c. cell cyde proteins; proliferating cell nuciBar antigen
(PCNA), tydins 01 and E2;
d. adhesion molecules: E- and N-cadherins,
e. the aotiapoptotic factor: 8-celllymphoma 2
f. Wnt-pathway regulator dickkopf 1 {DKK1) and its
homologue dickkopi 3 (DKK3) .
M Brenner et al.
Long-Term UV-Induced Molecular Changes in Human Skin
RESUlTS
Morphological changes in epidermal structure
Subjects (Hsted in Table i) irom two independent studies
{Miller el al., 2008; Wolber eta!., 2008j were invited 1o
return for reexamination more than l year a(ter their initial
UV exposur!:'s. Areas previously irradiated were identiiled
using photos taken at the time of initial exposure, considering
surface and in some cases, pigmentt:d areas that still
rernained.
.Skin specimens from atl subjects were stained with H&E
and were carefully examined by light microscopy for
morphological changes in the structure of the epidermis
and/or the dermis. No morphological changes were seen ln
any UV-irradialed skin spedmen5 or from the adjacent
unirradiated skin specimens (Figure 1}. There were no signs
that could be correlated to any clinical aspect oi a loc.1!ized
su1'bum reacl100
1
.such as a superficial inf!ammatory infiltrate
in the clermi'i or the presence of sunburn cells in the
epidermis. Special attention was paicl to detect possible
changes in the density, distribution and/or localization
of melanocytes (for exampfe, suprabasal localization of
melanoq'IP.s, formiltion of melanocyte cell ne!'>t5}. No
such changes were detected, although there was a signifkam
increase in melanocyte density in some svbjcct.s (see
below).
Visible pigmentation, mefanin cmlfenl, and e:ocpression of
melanogenic prGteins after UV irradia1ion
To evaluate changes in melanin content, the UV-
irradiated sldn areas and the- corresponding unirradiated
control tissues were examined visually and were biopsicd
after more than 1 year after exposure. Repetiiive UV
irradiation with the S1mlamp or with SS produced good e.:r!y
tanning reactions in all However, only one subject
(T50) !n the sunlamp-irradiated group showed lLP in the
exposed to the intermediate or high cumulative UV
doses (Miller eta!., 2008). Figure 2 shows such pigmentation
at 520 aiter irradiation. None of the subjects ln the 55-
irradiated group hod visibly pigmentalton in the
irradiated areas, at the time of biopsy (Table 1).
lhe melanin content io skin specimen
mined by quanlilative densitometry of the FontanaMasson
4
L Table 1. Visible long-lasting pigmentation fotlowing UV irradiation
.
..
.
Group 1: Sunlamp
Tl1
Tl6
T32
T35
TSO
Da)''S bel\veen iinnl
UV exposure otnd binpsy
1310
UlU
751
730
s:w
I
'i' Croup 1 liS dP.t<till!cltn Millt11 m .11., (:?OOa).
Group 2 as iu Wolber l.'l zf. !2003}.
1
Long.:lasting 11isible
pigmenlalion
No
No
No
No
No
.Yes
Grnup2:
ss
91
R2
B6
66
Days bctwei!ri finill'
UV exposure and biopsy
4U&
4()!
.JO:J.
ift,\6
Material may be protected by copyright law (Title 17, U.S. Code)
tiing-lastirig visible
pign1cnmtioo
No
No
No
No
www.jtdonline.org 1003
-- ..... - .. --------- .... --.
M Brenner el ar.
long-Term UV-fnduc;ed Molecular Changes in Human Skin
a
Unim!d\itfad Wi!hUV
b
1. OIO;Jlysis ur sk!n UV
(a} fKI mmpho!ogical ch::nscs were CcU!i:ltlblc in
Jhe UV-irradinU!d skin {left} or !right);
from ij& are shown ru; ;m lb) interinciividual differem:es
in skin content were seen !12 anti B6 .lr
shown as top l!nd hn!l<'lm, llr; =SO !!m.
fi&l.lrc 2. inc!MCd pigrnentllion in 2 suhlctts. Subject T47 ls
as <1il lll(i!rnple ro n.>s!dual pigmcnt<.o.tiun i5 ohst.!rlled {photo
taken al 427 llltcr
stained sectior.s (Figure 3). Only one subject \TSOl in the
Sunlamp-irradiated group and one subject iB6) in the 55-
irradiated group showed signlfic;mtly {P< 0.05) increased
total u( melanin (Table 2).
Th!:!re \Vere no significant differences in the numbers of
MI!F-posilive ceHs compared to the unitradialecl controls in
the UV-irradialed subiects. Although no difference could he
found between the UV-irradiated and the control specimens
in the number of MART1-positlve cells in the Sun!amp-
lrradiated group, two subjects (66 and 68) showed signifi-
cantly higher {P<D.05) numbers of cells in
the 55-irradiaied group. In the Sunlamp-irradiated group, 2
significant increase in the number of TYR-positive cells
compared to the unirradiated control was only found in
Uflirradlaled WilhUV
a
b
Figure J. Anulysls of in melanin conll':nl ar.d of
tlanogcmic pro mira aiter UV Signific;)r.t were noted
in mcl,;,nin o::ontenl in the skin of l of JO io:Jowinll UV irradli!llo.J.
wherens difierl?t\CI'S in lhn density of MARTIpo;itive cells were seen in 2 ci
l 0 In the density of TYRpositivP. in 4 of 1 () hut no
cliff!!tOOJ:c$ w.eMreen in lhe rir.nsil;t of MiTF-pnslflve cells iBn Is shown as an
example (ot all iour marker&}. Bars ,..50 J.lm.
subject T50, who was the on!y subject i.r. either study group
with visible pigmentation remilining in the previously UV-
irradiated <JrcilS. In the SS-irre1cliated group, three out of four
subjects (82, 86, ;:md 68) showed significant IP< .05)
increases in the density of TYR-positive cells (Table 2;
Figure 3), although r:o visibly increased pigmenlafion was
noted in those pr<!viously areas.
Expression patterns of markers in the skin after UV irradiation
.3 summarizes the molecular markers examined and
their longlerm responses to UV irradi1tion and examples of
the staining are shown in Figure 4.
Growth factors and their receptors. In the skif'l specimens
examined, SCF, bFGf, <Jnd ETl were expressed in the basal
epidermal layer. Bet\veen different Silmples, the staining
1004 journal uf hlVCSligufivc Dcrmah::liagy (2009}, Volume 129
Materia! may be protected by copyright law (Title 17, U.S. Code}
Tabfe 2. Cfmrncteristks of skin pigmentation
.. . ---- _ .. ____ ..
Differences in
Meli>r:ln content
rknsity
icontrol!UVl
Group J:
Sunliunp
irradiated
1/6
T11 (8.0ill.l)
116 (B.IJNA}
Gro-c:p 2: SS
irr.1dialcd
IH (6.]./7.1)
13:-! ('l.S/5.5} 1:!6 (1:;1,0/l $,;!)"
"" -- .. '. . .. - l3'1nHi.21HI9l . - . "'88"[6.YI7Af
of MITI'-posiliw
.:dis per :nm laverl!suJ
!comroi/UVl
Density of M:\RT1-pcsill\'e
cell$ pP.t mrrt (nvemge}
(corltrolill'v'l
Density oi
cells per mm lavcr.:ge)
tconm:of/UV!
T47 (5.415.1)
150 {6.1/9.5)
Cl!Cl
Tll Wi/50)
T1(i !3:11:10)
. _
TJ5 \:lli!J?)
T47 (19/22!
T50 (2312/ii
(Jl6
111 (45144)
Tl6 36f.l7l
T3:? i43/41l-
T47 (;!W1131
TSO (W2Z)
i/6
Tn tl9/4Zi
Tlu \J1/J4i
fj 1 !4H3:'11
ns {:1St.Ul
T47 f22/2Ul
T50 (Hi/.!5t
0/6
t:ll (171121
1'12 (1St'J2)
,
Fl6t4<1i32l
214
S1 (25ni)
Sl (27121!
--l\4 i r.u1 1 w
SflllSI<!J)
:114
IH (34/35)
at; rsi'ttm
oa {21/4.JJ
-
MARTl, !71el1l:'I0:713 11ntiger: r!!!:ogni2ed lry T-ce1!sJ MITI', m!crophthaln\!3
fiiclu'; TYR,
>f<OO::>.
intensity ranged irom weak !o moderate, but overall, no
marked differences in expression could be detected between
UV-irrarliated and control !;pecirnens from either prolocol.
KlT expfession was detected in all samples and showed a
strong regular pnttern of staining in the bnsal layers of the
epidermis, FGFR1 staining was weak and w:.s restricted to the
basal epidermal !ayer. Expression of HGF could not be
detected in the epidermis oi any skin sec! ions examined.
CSF e1epression in the skin showed irregular pattemst with
specimens !>howing basal expression and othl?r5
showing dispersed expression thmughout the whole
M Brenner et af,
l..ong-Term UY-Induced Molecular Changes in Human Skin
Table- 3, summary of staining patterns of various
markers after UV irradiation
Group 1:
Sunlilmp
LZ!iilnds; ;md recepfof!'
SCF -t
KIT
bFGF
FGFRl
Ei1
EDNRB
HGF
+
. " , ......... .
H i2./6j/+
CMC5f'' -
f\-t.ate,in +++
+H
N-Cm1hl'rin
Cell c::yda
'kNA.
Cydln Dl
Cydio E1
0/l!l;'r pmtFins
Ad-2
OKlO
OKlO ++
CaMtrol
....
-H-
...
+
++
++-io
++
.., . ... . , ....., ....... . , .................. ,.
-..
Gwup 2: ss Control
.;-
+
+o?-
+
.;.
...
+
++ ++
-++ {it-llf+
"""'""'"'
-++.)
+--. +-+-+
+-l+
t++
l:!d-1. EJ-cdl lympham.l :l; bFCF, b<!>ic growth fai':lor; DKK.
.. 6 ET1, hfCFRl;
growth faCior receptor 1; HGF, flt'!)il(OC}'II! ia(I<Jf;
PCNA. prnlliera:i:l!:l cell nuclr,ar antigen; SCF. mm ctoll factor.
r.;! li;;suc Slli:I!O:"JS wem hy !he invest:_g,llO!' IMHi. The Table
''" nV!'tl'i\11 plctum of II\!? slaioing pattr;m:. with 'laiiou$ aiter
UV irr3tliilHOn. St,linint: anrl CJ<Ienl w:u; ghlrled ,1;,: - !nu
-;. (\'>'f:!.?.k intensity ;md sm,;U area ++ imodr.r,,tr;
ar.d area s!nined) or +++ lhlsh ;,taining
ar.r! ilreil !'lilini!d}. cut-off tn d<!!isify staining as positivi': .
W\l.S 1%, i.e .. 1% of I he r!pidcrrni> positively cletet."tL'!l by
immunchistod-:zmislrv.
!Jm:gul.:u; $lain ill!! . . . -.. .. . . .... . . . , .. , ..... _ . .
epidermis (Figure 4). Two of the six subjects . in the
Sunlamp--irradiated group {T35 and T47) and one of the four
subject.s in the 55-irradiated group (86) showed marked
differences in the of EDNRB in the basill
epidermal fayers compared to the unirradii!ted controls. We
used a tissue array with 39 melanoma samples as a positive
control for EDNRB {Figure 5).
Tissue in situ fwbriditalion for EDNRB mRNA in the
or 55-irradiated skin showed cytopiasmic staining
rnc:tinly in the bas.al epidermal but no marked
difierencc in EDNRB mRN .. A expression between the UV-
irr.ldiated and conl;ol .skin (Figure 5).
Adhesion molecu/t!s. All skin specimens were ex11mcned for
expression oi various adhesion molecules (1}-catenin, E- and
N-cadherins). j)-Calenin showed a regular strong cytoplasmic
staining paflern throughout lhe whole epidermis with no
ww-.v.jidonline.ors lUOS
Material may be protected by copyright law (Title 17, U.S. Code}
M Brenner et a!.
Long Term UVInd;;cecl Molecular Changes in Human Skin
Unirradiated WithUV
Figure 4. I iUJ:\Iysis of diifl:!rnnce$ in e:<pr('.;sion of
growlh fatlor,; o:md !heir receptorS nfltt UV Stl:iining inlt!nsity
ranged from weak (o moderate, but ove:aH !hem 'h"l!re no mMked
in the e:<pressiar: of SCF, .KiT, bFCF, m, or G.'I.\-CSF between lN-
illildla1ed and control specimens (66 Is shown as .an fur
01!1 six ma1ke11). Bill$.., 50 !!m.
r.hanges in the expression between UV-irradiated and
unirraclialed skin. No nclear staining paHern could be
detected. ln all skin specimens, E-cadherin was expressed in
a regular slrong cytoplasmic pattern throughout the epidermis
1006 joumn\ oi Dermutology !2009}, Volume i.29
a
b
c
' ..
. ' .
fDNRB _;;;;,.
"'
EONRE! _::
"',.-....
.,
..-- ... ,
"--
EONRB -
-. - . .
..
. . ..
,. 0 : "'
. -
Wllh uv
'( i {"-- J
'
.. . .-.-.
: ... f:.:-:r ...
. ->
_:-.-
.-'
-
Wlthl./V
,.!' ....
0 ...
. .
. . .
.. '
_ -
figure S. Atlaiysls c-f tfiiferi!ntcs in EDNR.B :after UY irmtliation.
(al Cli!f!!tences ln f:DNR8 were mlu:d in 2 of o 5'-ibjl>clS (TJ5 am!
T47, top ilnd middic, in the Suniamp-irr.Jdialcd grQup 01nc.l in one
of iour (Bfi, bottom) in the SSRirradlated g:-oop; tbl Three different
sped mens Mille tissue a:m1y positi1o1e for i:OI'IRB el'pre!Osion;
rc:l Ti5sue in situ hybricli%ation for WNlW mRNi\ bi.l$-JI eJtprt:lision
b:ll m, differencer. between uninadlated control spec.imens
!subject T3S shown iln BM5"" SG pm.
and no marked differences between UV-irradiated and
control specimens were found. Ncadhetin expression could
not be detected (figure 6),.
CefJ cycle pmteins. Skin specimens were analyzed for
expression of the proliferative index of PCNA, cydins 01
<Jnd E2. Neither cyclio D1 nor cycffn E2 showed a positive
staining. PCNA expression showed no differences between
LJV-irratliated ;and controf specimens, e.lcept for one subject
(66) in the 55-irradiated group. A dearly higher nuclear
staining for PCNA was found in that specirnen, however,
double staining with TYR revealed th;u mainly keratinor.yles,
but not melanocyles, showed the increased cxpre!;sion of
PCNA (Figure 6).
DKK1, and Bcl-2. DKKl c:oufd no! be detected in any
skin specimen examined, UV irradiated or unirradii.lted.
DKK3 expression showed a regular and strong expression
pattern in the upper epidermal layers but did not exhibit any
significanl changes in response to UV irradiation. Bd-2
immunoreactivily was found in melanocyt.es in the basal eel!
layer of the skin ar. expected, but no marked differences in the
Material may be protected by copyright law {Title 17, U.S. Code}
WllhlN
.
'.
-
..
e--caanmin -
. . '
'. ii ;,.
PCNI\ -
...
) . ,.. . .. ..
PCNA -
;. :: :f .
... '
-
. . ' :; \ - .
;. .
- .
. .. . .
t.'
. .
' .
. .
ScJ ..2 .:..::._'- . - _....
-
Figurt! 6. lnnnunchiswchcmkal of in exprf'lsion oi
varlculJ afler UV iuacllation. Examples of staining panems in UV
spedmerts ltigh!l lilnd in t.lllirradiatecl t:Onlrals (!cftl. PCatt:tli,,
(suhject fl!;), -cildherin 861, PCNA (subjecl 31). PCNA lsl:bjed 86,
cioul:ll!l-Siair.ed iQr TYR in red on iar righ!J, lkl2 (subject Tm, and DKK3
(suhjecl !12}. Bars"" 50 JHT1.
expression of Bd-2 was noted betwet:n UV-irradiated and
unirradiated specimens (Figure 6).
DISCUSSION
In the past, many jn vitro and in viva experiments have been
conducted to characterize the carcinogenic eifects of UV
radiation on human skin cells. In vitro studies with human
melar.ocytes (Young el a/., 1998b; Sittner et al., 2000; Clark
et a/., 2000; Hipfe! et a!., 2000; Valery et a/,, 20011 and
in vivo studies on human skin have examined the effect!'> of
UV irradiation (Tronnier et aL 1997: Young eta/.,
1998a; Mass et at., .2003; Tatlokoro et al., 2003; Hac:hiy01
eta!., 20041 but so iar there have been no studies about the
long-lasting effects of UV. Sume in vivo studies hr:we
examined molecular ch<Jnges of atypical nevi (melanoma
precursor lesions; Wang et a/., 1996), but it has been
estimated lhil! melanomas mainly arise in the skin de nn'I(J
and in onfy 30% nf melanocytic nevi {Wolff eta!., 2005}.
In our study, we tried to identify long-lasting molecular
changes in human skin in situ many months Jfter the initial
M Brenner el al.
long-Term UV-lndw::ed Molecular Changes in Human Skin
repetitive IJV irradiation. The analysis was malnly based on
immunohistochemistry techniques and was comp:e1ed by
tissue- in situ hybridization for the analysis of EDNRS mRNA
1\llhough this <lpproach allowed the analysis of a consider-
able number of moiecular factors it does not permit
quantitative analysis of protein andior RNA expression. We
analyzed melanin content using Fonl.dna-Masson staining
and melanocyte density using antibodies to melanocyte-
specific markers, such as MITF, MART1, and T\'R. Earlier, we
reported the results of three din!caf studies measuring
melanocyte density after UV irradiation that showed sig-
nificant increases to levels about threefold higher than in
unirradiated skin at up to 5 weeks after irradiation and that
increase was consistent with the lncreilsed melanin content
(Tadokoro et al., 2003, 2005; YamrJguchi et al._ 2006). In this
study, a significant increase in MARTl-positive melanocytes
in 2 or 1 0 Sttbjects and a significant increase in
melanocyles in 4 of l D .subject!i was folmd, although only 1. of
those subjects still showed a visibly increased pigmentation
in the UV-irradiated area. Thls indicates that the acti\ation of
me!anocytes might persist much longer than the UV-induccr.!
pigmentation or the acute changes in
morphoiogy.
As toore are a wide variety of other possible genes of
interest and their corresponding encoded proteins, we
focused our analysis on representatives of five major groups
of proteins where changes in could be involved in
the transformation of melanocytes. The: growth factors {and
thei! cognate receptors) SCF/KIT, bFGF/FGFRl, ET1JEDNRB,
GMCSFiGM-CSFR, and HGF/MET, are part of the paracrine
nerwor!< between melanocytes and keratinoc.yte>'fibroblasts
(lmokawa, 2004; Yamaguchi et al., 2007; Brenner and
!-fearing, 2008}. SCF and ET1 ar{?! highly mllogenic fur human
melanocytes (lmokawa et al., 1996a; Grichnik eta!., 1995,
1998). The expression of KIT, the cognate receptot for SCF, is
dawn regulated with progression in melanoma cell lines and
tumors (Montone et. al., 1997). Recently. it was shown that
SCf and KIT are frequently expressed by melanomas and by
dysplastic nevi suggesting an <mlocrine growth factor
mechanism iGiehl el a!., 2007}. Also reported recently 3re
studies sf-lowing that bFGF, SCF, and m may be involved in
mefanomagenesis (Berking et af., 2004). FGFR1 is the
cognate receptor for bFGF and the coexpre5sion of FGFR1
and bFGF in melanoma cells was reported !o be
with increased microvessel density (Straume and Aksren,
2002).
In contrast to K!T expression, which is graduaily lost
during the !ransfommtion of me!anocytes to
melanoma, EDNRB expression is greatly enhanced and can
serve as a marker of mekmoma progression {Loftus et .-d.,
i99!:l; Bittner et aJ., 2000; Demunter et ai., 1001). Those
results and the finding that ET1 production by keratinocytes is
increased following UV irradiation (Ahn et af,, 1998) suggest
that EDNRB as well as its ligand, ET1, contribute to
melanomagenesis and progression (Demunter et iJI., 2001;
l.ahav, 2005}. Increased EDNRB expression, probably
cOi1pled w[th epidermal hypcn;ecretlon of ET1, could be a
fir-st step to generate local populations of melanocytes with
1007
Material may be protected by copyright law {Title 17, U.S. Code}
M Brenner e1 at
Lof'lg-Term UV-Indw.:ecl Molecular Changes in Human Skin
the potential to escape frorn the epidermis if further
occur {fa; example, loss of -cadhednj. EDNRa has been
recently reported to be upregulated in solar lentigos (Aoki
et al., 2007), which is consistent with the findings of our
study, and suggests that overexpression of that receptor may
result frcm chronic UV exposure and may be involved in the
increased pigmentation of human skin foHowlng UV. One
study in human 5kln in vivo showed an early increase in SCF
and KIT mRNA expression and a subsequent increas!:! in the
expression oi TYR, ET1, and EDNRB mRNA and protein7-10
days after 2 MED UVB irradiation {Hflchiya et al.
1
2004).
HGF is a multifunctional cytokine, among other
activities, acts as a growth filctor for melanocytes. It ha& been
shown that UVB irradiaticn leads to melanomas In neonatal
HGFtmnsgenk mice (Noonan et al., 200'1}. HGF
1
which is
e.'<pressed by fibroblasts and by melanoma cells, but not by
normal melanocvtes (lver et a!., 1990; Rosen er aJ., 1994; L i
et a!., 2001} not be detected h1 the epidermis of our
skin speclmens. GM-CSF has been shown to be secreted from
kcratinocytes after UVA Hmokawn ct a/., 1996b) or UVB
irradiation (Hi robe eta!., 2004) and might play an important
role in regulating the pmlifttrillion i!nd differentiation of
human melanocyles after UV irradiation.
ln our study, we could not detect any differences
between the UV-irradialeci skin and the unirracliated controls
in long-term follow-up specimens regarding the ex.prer.slon of
SCF, KIT, GMCSF, bFGF, FGFR1, or ETl in the epidermis.
However, irt J of 10 subjects, a clearly Increased expression
of EDNRB protein was detected in the irradiated skin;
however, that was not detected at the mRNA level. Whether
the increased expression of EDNRB in some of our subjects
might predict an increased risk for skin further in the
future deserves a longer term fo!low-up study.
fl-Catenin is a potent mediator of growth iur melanorna
cells and plays a dual role in cells, in cadherin-mediated cell
adhesion {Steinberg and McNutt, 1999) and in the Wnt
signaling pathway (Morin, 1999). E-cadherin, which is a
tumor invasion suppressor, ls downregula:ed in most
melanoma cells, and this renders them refractory to
keratinocyte-medlated control and enhances their cap<1bility
(or invasion (Hsu et al., 1000). Staining for E-cadherin and for
P..catenin resulted in strang staining pal!erns; however, no
differences in their expression in UV-irradiated skin and in
un!rradiated controls were detected. Afso, no expression of
N-cadherin could be detected, which might indicate that
changes in adhesion molecules occur in late stages of
melanomagenesis and are signs of the invasive behavior of
malignant skin cells.
Dysregulation of the cell cycle is " hallmark of tumor
progression and increased proliierative activity of tumor cells
is an important prognostic marker in m;rny human cancers.
Prolifer:ttion is by the formation, i.lctivation, ar.d
degrildation of a series of cycllnf>. Widely usi!d immunohis-
tochemical markers to cefl proliferation include PCNA
and Ki-67 (Unden eta(., 1992). In 1 of our 10 UV -irradiated
skin specimens, a strong increase in PCNA exprt'..'lision in
keratinocytes, but not in me!anocytes, was detected. We
could not detect any changes in the cxpress!oo of cyclin Dl
1006 Jtnorn;,! of lnvesilgatic Voh:me 129
or cyclin E2 in !he UV-irradiilted skin, which is po!;sibly duE'
to the fact that lJV-induced changes in cell cycle proteins are
early events that might already be removed at this late
timepoint (> 1 year}.
DKK1, a secreted protein pr!!ferentially expressed by
palmcplantar fibroblasts in the dermis, melanocyte
growth and differentiation through canonical Wnt signaling,
expression, and MITF function {Yamaguchi el a/.,
2004). In contrast, DKKJ, which is at higher levels
in fibroblasts in nonpa:moplantar dermis, has no effect on
melanocyte growth and function (Yamaguchi et al., 2005).
The potential roleis) of DKK proteins in melanoma i:r. totally
unknown. An anulysis of the expression profile of UVB
responses ir. normal human melanocytes detected a > lwo-
fold induction of DKK1 gene exprec.;sion after UVS irradia-
tion; however, ln many melanoma cell lines a loss of DKKi
expression has been reported (Yang et a!., 2006). A recent
study found a strong reduction of DKK3 expression in human
primilry melanomas and metas1ases compared to norma! skin
(K:.tphal ct al., 2006). In our study, DKK1 could not be
detected in the nonpalmop!antar skin thal was UV
(confinni;1g our earlier studies), whereas DKK3 expression
showed a regulur pilttern in the upper epidermal layers and
did not exhibit any significant changes in response to uv
exposure.
We the expre>sion of Bcl-2 as it represents
the prominent marker within the large Bcl2 famlly and
numerous studies have been published regarding the effects
of UV irradiation on humi.in skin with respect to Bci-2
expression_ !n our study, Bd-2 immunoreactivity was found
predominantly in the basal cell layer of the skin specimens.
One study that analyzed human skin in situ 6 hour after a
single SS irradiation found <l transient reduction of -40% in
the expression of Bcl-2 (lsoherranen el <JI.
1
1999). We could
not detect any significant different.es in the expressio!l oi
Bcl-2 between UV-irradiated and unirradiated skin. Regard-
ing the expression pattern of Bd-2 after UV exposure, the
literature is contradictory. One i11 vitro study described an
Induction of Scl-2 at the mRNA level, but not at the protein
level after UVB (8ivik el a!., 2005i. In vitw s!wclies on human
melanocytes revealed no changes in expression of Bcl2 a iter
UVA or UVB irradiation (Kim et ai., :woo; Zhang and
Rosd<1hl, 2003), whereas other groups reported that Sci-2
levels decrease after UV irradiation (lm el ill., 1998;
lsoherrarten et al., 1999; Kadekaro et at., 2003).
ln summary, among the 20 factors only
MART1, TYR, and EDNRB protein expressions, and only in
some subjects, were elevated at 1 year after UV irradiation.
These findings suggest that the effects of repetitive
UV irradiation on human skln in these studies do not lead to
significant changes in s.kin morphology and there is
considerable subject-to--wbject variation in effects on skin
pigmentation. The possibility that changes in the expression
of the DNR6 protein trigger downstream activation of
abnormal melanocyte proliferation and, considering the key
role- of the melanocottin system in regulating human skin
pigmentation, the lang-lasting UV-induced mo!ewlar
changes in the expression of factors such as prnopiomelano-
Material may be protected by copyright law (Title 17, U.S. Code)
cortin. peptides and mefano-
cortin 1 rP.r:eptor, also dcseNes further investigation.
MA TERIAtS AND METHODS
Study suhjeds, UV irradiation, and dosimctry
This involved volunteer suhjct:l.? with skin photolypcs 2-3.5. il!>
shown in Tnble 1, ilnd was approved by the Resei3rch Involving
Human Subjects Committees of the US food and Drug Ar:lminisira-
tian iilld Seiersdorf AG. Wril!en informed consent was obwined
from each donor ilnd the study w;;:s conducted according kl the
Each MED was tieterrnined prior 10 the
start of fhc experlmt!nt, ns in MiiiN et <Jl. (2006, 2006),
Wolber el a/. {2008), Yamaguchi et a!. {2008b). Subjects did not
significant UV exposvre between 1he of the initi<ll
irrildl<ttion and the longlerm biop5ies,
Group 1: Sunlamp. Six (T11, T15, T32, 135, T47, and
T5G), from the study detailed in Miller eta!. (2008), weH! studied
with long-term follow-up. For the tepetittve Sunlilmj)ltradiation
protocol,;:; 12-!amp tanning bi:!d canopy LNt\ UVBI
wa!; used ami monitored as previously iMil!er ct a/., :wocn.
rr.ree different repeaied UV exposure reg!mens were u.'lt!d 0\/er the
cauf5t:! of 3-4 O!l thn back of each subject. Cumu!atlv!o! doses
were 1,90DJm-
2
, 2,900J m-
2
, -.nd 4,2001 m-
1
for low, medium and
high oose exposure regimens,
Group 2: SS. Four subjects (81, Bl, B6, and 88, from Woiber et <1/.
(2001lj, wem s!IJdicd with long-term foliow-up. For the repetitive .SS
Irradiation protocol, an Oriel '!WOW SS WilS used ;lnd doses were
mcr.itoted previvusiy detcJiled 5rhlenz et aJ., 1UD5; Miyamurtl
vt .:1., 2007; Wolber aJ., :,woa;. lrr.tdialions were given a total of
10 times over .2 weE!b on 5 consecutive days with cumulative d05es
that rnnged between 333 and 1.030J m-
2
lm.tdiation doses varied
ir.:dividua.ls dept!nding on <!ildt subjecl's Mf.D to induce
comparable tilnr.log.
Biopsies and immunohistochemical analysis
Skin biopsies were tnktm from the centro; and UV-exposed at
various times after the last UV tCJCh biopsy piaced
dermis side dow11 on a MHHpore Jllter ;;nd was then fixed in 4%
rormalr.lehyde, embedded ln paraffin, !ectioned <I{ Jjlrn
mounted on silane-canted glass and tlllm stained using
immunohistochemistry, as prevkMiy clcscrlbt!d (Yamaguchi ct $1.,
2004, .2006). Briefly, were depariliiiniz:ed twice with
for 5 minv\e$ and were the:'l dehyrltaled wi\h a gtaduarcd
serles of erhanol, followed by an!igen retrieval via boiling ln antigen
unm<Jsking solulio11 {Vector laboratories Inc., Burlingame, CAl
for l2 minutes. For antigens axprt!ssed ln low abundance, 1 mM
EDT retrieval was Specimens were subsequently
wi1n 10% goat, 10% horse, or 10% donkey summ (Vector
for 30minutes <:t 37 "C, as appropriate, then with
prlm.lry <>ntlbodit in 5% goo! serum iS% horse or 5% donkey
5erum, resp!1ctivelyt at 4 "C VVIJHJight. Wetlll!
as appropr!ate for the primary an!ibody, t\lexa Fluor 41l8/594
anti-mouse, anri-rabbit, or anti-goilt lgG (H + l) 1:500 dilution;
Molecular Probes lr:c Eugene, OR). Staining was analyzed using a
Leica DMRB!DMl.D tluoresceoce microscope, >Jnd an internal
control each time to controi ror wprodudble antibody
M Brenr1er :et al.
Lang-Term UV-lnduccd Molecular Changes in Hum;m Skin
staining. Negntive tonirois omit11ng the primary ;u\!ibody were
performed each lime.
Prcleln expression using the iollowing antibodies was meilsured:
SCF antibody {at 1;1 D dilution; R&D Minnenpol1s, A1N),
SCF RIKIT antibody {at 'i :'1 00 R&D Sy.stems), bFGF antibody
(.1t 1:10 dirt; !ion; R&D Systems), FGFR 1 antibody !at 1:100 dilution;
Ahco;rn Inc., Camb:lr:lge, ET -1 antibody [at 1 :2.0{1 dilution;
Abeam lnc,J, WNRB antibody I<Jt 1:100 dilution: Abeam Inc.), GM-
CSF antibody (at 1:20 dilution; R&D Systems), HGF antibody (at 1:10
dilution; R&D PCNA antibody (I 1 :200 dilution; Dako
lnc., Carpinteria. CA), c:ydin D1 antibody {at 1:20 dilution; Zymecf
Laborntodes, South 5iln fmnci<ico, CA), cyd!n Ei. amibody (a! 1:20
dilution; Cell Sigr.i:!liog Technology, N'.-\), Ec.adhedn
antibody (at 1:100 dilution; Takara Bio Inc., Shiga, Japan}, N-
caciher!n antibody (at 1:l0 dilution; Oako lnc.l. f:lt::ilienin antibody
{at 1 :100 Cell Signaling Technology), Bcl-2 ;mtibr.x.ly
(al 1;20 dilution; Sanla Cruz Biotechnology lrlc., Santa Cru:t, CA),
DKK-1 antibody {ilt 1:50 dilution; R&D .Systems), and DKK-3
antibacly {a; l: 100 diltstion; R&D Sys;ems).
Tissue in sUu hybridization
'tissue in situ hybridlziltion was performed as previously detailed
(V<dencia cl a f., 1006; Passeron eta/., 2007a, b). Oiigonudwiicle
probes .specitlc for human tDNRB Wl!re designed, and target silcs
were selected bilsed on the analysis or sequence matches <!nd
mismalchcs BlAST (GenBankj. Probes showed no of cross-
reaclion with sequences oi oiher gf.'ne:> including other ETR family
genes. Opl!m;,;l results were obtained with the following probas:
sense primer 5' -CA TACGA TTTAGGTCACACT
gagat.gt-3
1
; ;mlisense primer S'-GCGCGTAATACGACTCACTATA
GGGgacanggac:caggcaanaga-3'. The probes were 3' !ailed with
digoxigcninl HIUTP with a DIG RNA kit 11aS\!l,
Swi!zcrland}, according to rccommem:iations of the manufacturer.
Briefly, <.tfler deparan1ni:zalion and rehydration. skin were
l mmersf.!d in antigen retrieval and heated in a micmwave for
12 minutes !hen ior 20 minutes. Slides were then washed in
glycine solution (2 mg tnl-
1
in buffered saline) for
l0mh11.ites, twice ln sa!inc, <lnd then
placed in .200m! acetylJiion buffer (0.1 M triethylamine, pH 8.0,
containing 0.25% acetic ilnhydride) ior 15 After further
washing in 4 X sse fur lOmin, 5itmples were inculm!ed in
ptehybridixatirll'l solution !2 :>:sse, 5D"h deionized for
t hour al47 Be. After overnight hybridization at 47 c, samples were
in hyhridizntion :;olution (Mutsugn cr a/,, ZOOII) r:onl<lining
Wpl purified OIG-Iilbeled an:isense riboprobe, Samples were then
incubated in 10mM Tris-HCI, O.h1 NaCI, 0.25 mM EDTA {TNfj
buffer, rreilled with for and returned to TNE
bairer for J minutes, all ;;t 37 "C After wa;hing in 0.1 X sse for
15 minutes at 47 c, sample!> were bincked for 30 minutes and
incuh;;tccl wilh conjugate ID.'lka) for 40minvte; ai
room The tyramidc signal 3mplification system
(GencPQinl kit; D<tkoj wi.\s used with VIP solution {Ver
laboratories} according !o the mar.ufucturers' instroctions. Samples
Wt?ro and pho1ographed in a OMRB microscope,
Melaooc.yle density ilnd melanin <ontenl
Mclanocytes were .:ounted foilowing sl<lining for
MART1, and MliF, and their denliily along \he epidermaltdermill
www,jidtmiint!.nrg 1009
Material may be protected by copyright law {Title 17. U.S. Code)
I
t .,
M Brenner ai.
long-Term UV-Induced Molecular Chr:nges ln Human Skin
border wi!s detf:!rmined as celfs per mrn. Primary anlihoclies used
were rtf'EP7 h (at 1:7$0 dilution) to dC"ict.'t (Yamaguchi
eta!., 2001J) nnci AbJ (all: 1 OD dilution; NeoMarkers, Fremonl, CA}
to clclcct MART1. Fluorcs1.ence intensities for antibodies detecting
melanocytespedfk markers were normdliZ:t;d against 4'-6-diamidi
no-2-phenylinctole staining.
For measuremeols of melanin spcdmcos were stained
by the method (Uilncrofl and Stever.s, 1982).
Transmitlcd light was measured by lhe Leit<:! DMRB\
microscope ;md Scionlrr.<lge 50rtw<Jre was used to ;;nalyze
melanin quantity from tiensity in the skin seciions, as
previously described {Yamaguchi et .1!., 1005, :HJUaa;. fjye
randomly salected areas of each specimen were photographed and
quantitated.
Statistical analyses
Stati5tical ao&lysi5 wus performed using Microsoft Office i:xcel
Analysis Toolpak. 5tilt1stical bet11ecn iuad!cttt.-d speci
mens and controls were determined by Student's t-Ies; with a twcr
tniled distribuiloo (two-sample unequill A P<IJ.05 is
defined signiiicam.
COt-:fUCT OF ZNTi:REST
The uuthor; no or
ACKNOWlEDGMENTS
ihi; res;;oMcll was supporter! l>y lntr"!murai I<I!Wclrch Prog:ao) of lite
Nalion<l! Cancer lr1stilute at NIH, ant! hy the Ofilc11 of Sdef!re, OiiJce ol
women's and the Center iot Ot!vlca and Rildioltl!:icul Hei!hll, Food
Drug Admlnist.-aliun ifD,\J. 1he au:hcr.> wi5h to lhank Dr Thierry
Pa!il\l!ran :md Or !t<Jro !iulukt ia; thclr advke and help on !he TI5H
REFERENCES
Ahn CY, Dull Kl, Jindo T, Yagucl'.i H, R, Dij11Wol H !1998!
of l.mdOti:n:!lin-1 .md it:> bind1ng si!es lu mbuse 5kin
alter uhr;,l/io!e\ B irr.sdialion or foc;;! !njc<:tion r.f tumor fattor
alphll. 1 Dcrmiilal25:7o-6;
Aoki N, Moro 0, Tagami H, l<ishiol(IIC J \2007) Ci(prcsslc<m profilin&
an.; lysis of mlar h:m!igo in relilliOn lb imm1.1rn>hislochetniC'ill charalter-
istic;. fir]
Rancro/i jD, Soevens A {19!12) Tbeory and i"nnc:tice af Histalusit;>[
T echfli'qllcs. Churchill Livingstone: N<.>W Ymk
fler't<ing C, R, Sal.ynmoonhy J.:, Shlrak;.wa T. Esk,;ndatpnllr M,
H;Jnsson J l!f ul. (2G04) lnd:.u::ti::m ui in
slcin by gmwtn iac1ors and ullfiiViolel 8. Cmc:er M;807-1 i
Blr.ne! M, .V.cltl:11r I', Chen Y, Jiang Y. !ief:or t, Hendrix M et ;;f. l:lOOIJ!
Mul!.-culilt tlJSsi!ie<llion oi cul:llneous mehmomil by gene
expression profiling. NatlJtrt! 406:5Jt)..40
t:li"ik G\ EIJ, Ro>rlahi IK !2005) 011
UVB-!Ildutct! 'lpoploii$ :n mdar.ocytes. II study of Bcl-2/ail:< expression
;tnd rescue e;lects. Me!;:momzt !lf:/!1 15:713
Brenner M, Degilz 1<, Besch R, lurking C !2005} Diif!!nmliuf of
tndanomaassocial!!cl growth facJors in kera;lrocyl(lS anl! fil::mhlas! by
A and ultraviolet B rJr!larion. Bt 1 Dli1fm3tnf 1 5);73J..J)
Brenne: M, 1-learing \II (2008} Modifying skin p:&mentotfion-approachcs
through Intrinsic and agents. Drug Disc:ov
Toe!Jy Dis ,\.fe:.:h 5 (In press)
EA. Golub rrt landL>r ES, fiyr:es RO t:mr.O} Genomic of
mc.>IM!a.>is r:ve.1!s an i!S$enli41 rote for RhoC. N.ill.lt!' On:Sl2 --5
Cloogh.Curr KM, Tit!.:s-Em;;toff I.; Perry AE, SK, MS i2006J
to iJnning b!lds, risk. Cilnc:l?r (.<JIJ/ieS
Con!f()/19:&59-69
1010 Jnutnal of Jnves1iga1im DermiliO!og; (2Htl'li, Voiumc urJ
DP.rnunler t\ De Wolf- C, Ot'Br<:r.! H, S:ili M, va.n den Oord JJ (:2001}
of th<! cndorhe!inP. receptor li1 pigment cell lesions oi the
skin. Evtdente fm it$ as rumor progress1un 1n.nket in m;,!ignant
melanoma. Vircflf1w Ach 431!:48.5-!H
Giehl KA. Nagele I.J, Volkenanrlt M, Berking C (20071 Protein Cl'!prcsslon oi
gmwlh f.1clor:. (bFGF, 5CF) .1ud !heir recepl(lrs (FGFP.i.
in ;md melarmm.1./ Culi11J Pathn! 34:7-14
Gi!chrcsl fiA, filer MS, Gdlcr AC, Y.1ar M {l!i!f'Jt The p.11hDgl!ncsis of
mP.lnnoma irnJuccd by ultr,wiolcl New Eng 1 ,4,ted 340: 1.34 i...,<l
Grit:hnik IM, aurch )A, Burchr.Ue J, Shea CR {lll'!B} ihe SCF/Kii p.1lnw"y
plays <! role in the control of normal human
homeost.lsis. ! lnvt.ost Oerml!tol t 11 :23 3-a
Grit::hnlk JM, Cr;)wford J, }1menez f, Ku;tzhP.rg J, 3uchun;m M,
S et ;d. {'1995) Human stcmceU factor i11duces
melanocy1 ic in susceptible patienis, } Am Acari Oe.-n1,1101
JJ:577...fl3
Hachiya A A. Y, Kttaharil T, Tuke:r.a Y, hnokm'>'a G
CW04) Uiphasic of two paratrlr:e mel;mogcnic: qr.okir.es.
factor .1nci t:r.cloihelin.:, in uhr.avio!et 3-inducoo
Am J f>ollhoi 1 &S:.:!0119-iO".J
Hipfel R, B, Y, C !200()) Spccilit:ally
in ;n;;ligf1ant mcJanom:t ti$WC.O OY SUb!t;ll;liYQ hyb:icli-
latiC!'I. Dr f Glr:c;;r IU: 1149-5 7
Hirobc 1, li. Haril t, Horii 1. Truo!!l!ag;:; M, lfuku 0 !:!rol}
t:Okltl'fSlirr.o1Mit1S {Gf\CSf)
the proliic,ation and n( mouse epidl'IT!"WII meli'ir.ocylc-5
from spot> induced by ultraviulct mrliation S. Pigmen: Cell
P.cs I 7;2.3Ckll
Hsu MY, Meier rt, Ncsh!t M, Hsu JY. Van Belle P. Eider DE eta!. (2.000) f:-
caciherin ic>llpres>ion in m11lanama cells kl'liv.inocym-mcrllaied
r,rowih nmtrol and clov,n-lcgulaJ;:os of inv.lsiOilrei<:!t.>d
adhesion fi!C<:p:ors. Am]
lm S, Moro M, Pcny, F. Medrano J::f.. Comcliu:; 1. B11hcor:k G cl a!. tl!Jt}il)
Activation oi the r.:ydk N.W by a-meliml.l' .mpin meolol.fts lhu
respoose o! hum1on mel;mocyles 10 ullravinlel 9 raclia!icn. Omcer Rt:s
5ll:47-!jtl
lm!:'kawn G [2004} Aulocrine and paracrine of me!anocylt"!' ln
skin a11d in Pigment Cell /?fti; 17:1J(,...; 10
JmokO!Wil G; Y<JdA Y, Kimura M ili:JC)tlai SiKmtiHn!J me<:h;misms of
and in human rneli\rtocyw.i.
iJiochtm!) 3l4:JOS<4 2
lmuk.:Jwa G. Yada Y, J<irnur-'1 M, ,\1nr:.o;aki N 09il6bi Granu!ocyie/
coh.my-s!!mulaling factor is an irurlnsic keradnoc:y!e-
grov.-.1-1 faciur for rp.t;lanocrws in llVA-indur.ed
melanosi;. Biochem J 313(i"t 2J:u25-31
Agency im on Ciltu:<!r 12007) The associlltion of of
with cut;Jncous tnilligna.l'lt mclanon\a n1her sllin can;;ers: <l
i111 J C,l/ICef l :W: 111
K, s,1urojal. !atistm C. P<..1nnunen KH9ll'lllN irrudiMion
of bd-2 in v1:ro .'!nrJ in v[HJ, .ArdJ DemratrA
Re1. 191:212-6
lyN A, Kmiecik TE, Park M, Di!ar 1
1
Blair D, Dunn 1<1 c! M. !<9901 Struclure,
;issvespcc:iiir: {!)(p:essicn, r.n\1 at:tivi:y of the mouse m111
pmtooncogene. Cr:lf Gro'Nth Diifer-1
i<adekaro J\t, K.wanagh R. WakatMISu K. Uo S, MA
2A {200.3) Cu!llneous pllotobia!op,y, The
the sun: who wUI win the linal rouod1 f'igmeflt Cell
I
r.im Yt;, Kim Hl, Kim DS, Kirn SD. W!i, Kim KH C'i' <:l. l:.!OOOi Up-
;mtl rf!<lisllibutlon of Sa:c in ullravio!o::t Ritrotllatecl mP.l3fiO
q1es. Cl!fl Res 1J:J52-1
K1.1phal S, lodemtr.;ycr S, !J.'Ita!Ut: f, Schulllrer M, liH, AK
(2C00} of Didknpf is ;trMgty recluccrl in m<Jii!lnant
mdanom.l. 25:Sul7-3b
talmv R (2005/ Endulltelin r<!cl:'ptor 5 is for the expansion of
melanorytc pre-cursors and malign.1nt met;:moma. lnt j Dav Bioi
49:173-80
Material may be protected by copyright law (lltle 17, U.S. Code)
m JiiJii;
li t.J. H, Sill)'<lotloorlhy K, Hanilkilwa Y. Hash!moto K, Herlyn M
tJOIH) nf Ec::adhcrin and Desrr,oglein I by
growth fac:or during rne!nnoma
1fi:lll2r;-35
Uncle:-. MD, Torr!!$ f)(, Kubus J, Zarbo I1
1
J\12) of
and lmmunocytuchemical ns!<!ssments of C<i!ll proliiilraiion.
Am J Cfin P'ntho/!li:S4-l3
Sit, Chen Y, Gooden G, Ryan JF, Sirznicks G, Hi!liatd M tlt .1!. (l !19!1)
selccllon of <1 ncuri!l cONA. set ior
mi(ro;may an.1lysi>. Proc Nati Acad Sci USA 9!:1:9177-ao
Mass P. Hoifm;:mn K, T, 1\llmeyr.r P, M;mnhet.: HG (:ZU03}
Prematurc l:cratinocyre delth and of mulmr prQteins of
in human skin afler UV!J Art:h Dt:rmil!ol
2S!!:71...V
Matsumur.t Y, tiN {2002) Short-term and loo!,lletm ed!ular
;;nd molt."'l.m.rr t'llnts following UV irradiation of skin: im
rnoler;ular rnedidne. Experl Rt!\' Mol Med 4:1-22
,V.Ilier S.\, Czy;Jiho SG, Zmud&a s:z. Beer JZ (2006) Reth:diuh o( the UV
burlkuto indoor tanners through new exposure r.chl!d1Jie5: n pilo; $lurly.
('hatoderrmtol PhotQimmuti(J/ Phoramed
Mlller S.o\, Coelho SG, :Z:mudzka U7., HF, Y3muguchi Y, VI
ei ,11. (2001ll Dynamic.s of plgmentatlon by repeated UV
dow, clos!! interv<!l and UV 5pet:trun d;;pcr.dencc. IJr j
Deummaf 159:921.-,10
Miy(lmura Y. Ctl<!l!m SC, Wo!i:mr R. Miller SA, K, Zmudz:.a BZ
t'l {].Q()7J Regulation uf humaa skin pigmenti\:lnn ;:md r!Sponscs to
ullravlolet radiation. Pigment Cell 883 20:2-13
!(T, van Ell', 1!, Eitk:r DE {19!17) f'roto-oncogene c-ki<
f:!Oiepros.(lon ill rnalig1anl melanoma: pm!ein luss wilh tv mar
Moo P<Hholl0:939-44
Murin PI 119991 h.Caumin signaling and r:<Jncer. Bloasa)l> :.!l:lil21,.,.JO
Mulsuga N, Shall.lr l, jG, Ml, Xiang CC. Bonnet RF et al.
(201J1) Selective gene tl!p;e.ssion in rl!i.\W'OCe!lular ncurnns in rat
sup.-aop1lc J Neurosci 24:7174-BS
l'h:-onMt fP, 01:clek j, Merlino G, De ri.lbo tc 1200:\l r\nirnal models of
melilnomu: an HGFlSF trnns;;enlc may ladlilate t!X(X)ri
menial il::cess to UV inilillllng l'igmcnt Cell Res lb:l,..,;!5
Nconan FP, Recio JA. TaJ.o.ayama Duray 1", Anver MR, Ru;;n WI. el ,1!.
!2031} Neonatni &unbum and melanoma in rnice, Ni!fllre 413:271-2
Pas;;f.!ron T, Coe!bo SG, Miyamura Y, Takaha;iri K, HeariOIJ \'j (2007\ll
!mmunohis1ad\t:>mistry ancl itr situ in study of
human ;kin melanocytes. Exp DermJtoJ 16: 162-70
Posseron T. Vnlenc1a JC, Bertolctio C, Hoasni'T, Takahashi K. Lt.d"ape 'E. e( a/.
(10ll7bl50X9 is a key player in liVD-Jnduc:ecf melanoeyte
and pigmentation. P.-or.:. Ac,uJ .'>ci VSA 1 04; l :1934-'J
f.\'1, Ni?,ilm .SK, Golc/bgrg ID (1994) Scattar folc:W ancl lhe c-mcl
a paradigm lor interuc:tion. 1 Cell 8io/
127:17!13-7
Schlcm: K, Smucla C, J, Sl(lb F, Wens;k H. Usac.m:r HP ct i:!l, !200.S)
Pig<nentalion i!ldur:t:d by differenl wavelengths nf \.lit light.
Pi8Jilent Rf!S HI:S:IJ
Setlow RB, Grisll', K, Wooo1:ead AD (1993) Wavele'lg!hs effeeti<.;c in
incbclion of trli.l!ignaMt Proc Nail ACld 5d US.>\ 9tl:&ti6&-70
S:ary A, Robett C, A (1997j Dcleleti(lf.l5 effects of ultravlolel A
radiat!on in human ciJil$. Mullll Res
Steinberg M5, McNutt PM (1999) (i)dherins and their
jur...:lions Mil"! bro.1cler fum:tions. Curr Opin Cell BJo/11 :554-f,()
Str.1Ume 0. Aks!en LA 12002) lmpormnce of vascular by basic
libmbla>t growth factor, ;md influence oi 1he ;;mgiogff.iC filciors
fibmhlast growth far:tor/ii!irobla5t growth illdot rt:tepM-1 (llld i!phti!1-
A I JEphA2 on roolanama Am) l'iJll;o! l 60: ll')if.}...19
Tndolcar-3 T, N, :Zm1Jc.l2k.1 az, lio S, Wakarnatsu K, Y
el ;;/. (20!)3j DNA clamilse ;md rm!lanin c:ontenlln hurnan
M 1JFenner el
Long-Term UV-Induced Molecular Jn Human Skin
:xkin diffc."ing in racinllcthflit: origin fAS!JJ I
17:'1177-!)
Ta.eokow T, Y<lrtlililVJ;hi Y, Billzcr J, Coolho SG. liZ, Milhzr SA
et ,1/. {2005) Mot:hani;rr;s of skin tanoing i11 rllficrcr.t r.JCiilllc\hnic
i11 rcspcnsc to racJi;;tioll. J Dr.rmatol 124!
1.'326-.U
Tlllg W, Sr;hultz. K, Cac NN, M, Wai:ing HW !2007} TanninG bed
i;.'XpmurC! inc;rtli!W the tl;k of malignJni mclanomil. In/ 1 D<!rm;uoi
'1&:1253-7
Tronr.ier M, ,<\lcl!andl!r M, Wol!f HH 11997} molecule expression in
Mrmal and lesion>. Role o! UV-irradiatic:n and
(lrchltt-ctur.11 c;h;;ractt'fisllcs in nevi. J Cutilll P.Jthol.l4:2lf!...a5
V."llendl JC, Walaoo K, Chi A, Rollznud F, Chen KG. Vieiro WD et ,11. [201lf\i
SQtting of l'melli' ro mcl:lfl!lt}'l.$1hrouyh lhe plasma rnembranc by .-.r1
and AP2: evidence ior the polarize(! na1ure Qf mclJnocyle;. J Cell Sci
( l !t: 1U80-!l1
V<tfcry C, Croh !J, V11rrondo P h:lentlf1tadon by eDNA mic:mariJY
technology of genes moclulau:d by anillc:i;:i ult"!vio!et in
humiln ml};;;nor;ytcs: ICiillion to me!ltnucarcinugvne!ii>. j itiYl?!it
Di!rmatalll7:14?1-ll2
Y, Rao u. R, TJ, AI, iirllnglon HO ct al. (1 9\16}
/v'.()!ecular of mcl.,.,orM Cell CfClwii} Oiffllt"
7:1733-10
Wolber R, 1\, WuknmaHu K. Sm<Jda C, Nakanish: Y, Hearing VIet .Jf.
(2000) Piy,meo!oll!loo <:fie<:!$ of $0l:tr
wi1h UVA llnd IJV!l C111i 21:487-91
Wolf! K, johnsOn Rt\, SuurmoMcl D (20U5l fitlp-.,lri<k's Cclnr Atlas ttn<l
r'lf Clinit.:ii! DltrmlltoiOf:Y. Mc:Graw-Hil!: New York
Yamab-ur.:hi Y, Bcwr JZ:. Hearing VJ (20011<!} Melilnin of
t'!)itlelmllf oomayoo by ul:til1iiotcr rutliallon: fac.:lOt$ ioCluc:ncinJl
the Df skin C;lnr:er. Arr:l Df!trfJi.llr1i Rer; 30iJ[Supp1 ll:
54HSO
Yamaguchi Y. !lnmncr M, Hi:'ilring VI (20.:}1) Th<! rcguliltion cf
pig:nenrotion.J f:/ial Chl:vn 282:27557-iil
V, Ccelho SG. Z:nLidz((a BZ, Takahashi K, Beer JZ, Hearing VI
t'f ;;J_ l2000bl Cyclobulanc p)'timidine t:lirner formation pSJ
production fn human skin aftt>r repeated UV irradiution. Exp Dcrmulol
17:!116-24
Yil<ni!f',VCh! V, Heating VJ, ltami S. Yoshikawa K, 1\atayamu I (20115)
Mt>SF:?nchymal-epitheiial inu::rac:tions in the skin: aiming fo: site-specific:
Um:e regeneration. J Dermato( Sci 4fr.l-'J
Yamaguchi Y, ll<!rni S, W.:stalle H. Yasumnto K Abck:I-M.:Jickli\, KubCI T ct a!.
!2004 i !ntcractlons In the tncrC<J!iecl
e<p1cssio:t of dickkopi1 b)" palmoplantar flbroblllSts inhibits melanocyte
g:mvth and clifferenti:.tion. I Cell 8io1 Hi5:275-B5
Yamaguchi Y, Taki!h;nhi l<. HZ, KornhaiJst:r A, Miller SA, Ttcklknro
T ct ill. Q.OOGl Humiln skin rc.sponSi.!S to UV PigrrK:nt in the
upper proli:!ctS ag.1in;;t DNA t!amasc io the lc,wcr epidermis
nr.d fadlil.illes llp-lplosis. MSEB) 2.0:1486-8
Yang G, Zhang G, Pit!clkow MR, Rnmonl M. Tsao ;; 12006) fxpri!Sskm
ptoiilinp, of UVB rcsporue in identffieJ> a ses of p53-tMgcl
genes. J lnV!!5! DMnatol 126:2A90-506
Young AI!, Chl!c!-r.ih::k CA, Hartirun Gl, 0. H,'!msdert J, Potten CS
(1998;} The similarity of action for thymine climt.:IS in h1Jr.'lllfl
cp:derml> ilnd ertlrema >uggcstS lh<>t DNA is the for
el)<1hema. J /1West O.."''mato/1! '
Ynung r\R, Pottcn CS, Nikaldo 0, PG, BCX!nder; J, Rmr:sclcn JM et i:!l.
(!991lbi Human and expi.)S!.!d !JJ UVB or UVA
in vi110 show compati!b;e oi thymine tlimes. J /nV!!$1 De.miltai
Zhar1g Rosdahl112003) Ul:rai.':Uie: J\ <!rnl B induce intracellular
prc;tcin expression ill human skin melanocyte> a spaeula!ion oi
separ;;!e pathways in initl<!tion uf u!!!lanoma. C,1rtinogc1!1!is 24:
www.jidonllne.mg 1011
Material may be protected by copyright law (Title 17, U.S. Code)
25-Hydroxyvitamin D and
Risk of J\1yocardial Infarction in
.A Prospe<:tive Study
Edward Gi.ovanJHuci, MD, SeD; Vim Li<t, MS; Hollis, !IJD, PhD; Erk R Rimm. SeD
Background: Vitamin D defldcncy may involved in
of <Urwrosdemsis <md coronary hearr
disease in hurnans.
Methods: We assessed prospectively whether plasma 25-
hydroxyvi!<mlln D (25{0H\D) are asso
cia ted rbk of coro:nary heart disease. A nested case-
control study was conducted in 18 225 me.n in Heal!b
Professionals follow-up Study; !h" men aged 40 to
75 years ;,;nd were free of diagr.wsed cardiovascular dis-
ease at blood cdkction. The blood sanmles were re-
turned between Aprill. 1993, and Novemher 30. 1999;
99% Wt;'te between Aprill, 1993, and
ber 30, 199'5. During lO years of fo!lovv-up, 454 men de-
veloped nonfatal myoc,;rdial 1nfar(tion or f,;tal coro-
nary hert disease-. Using risk st:t samphng, controls
(n =900) were selected in a 2: l ratio and tJunc.hed k)r age,
date of hlood c<1Hection, and smoking status.
for M1 compared wiih those to be suffkkni
in 2'5( OH.) D _j(} ng/mL) risk I RRj, 2 42: 95%
G.mfidencc. interval [ CJl, 1.33-3 84: P < .001 for :rend)
After addithmal adjustmetlt for f:.mily history of myo-
j;Jfarctlon, body mass index, alcohol consump-
tion, physical activity, his:ory d diabetes mellitus and
hypertension, region, tnmine !1}-3 intak<:\ low-
and high-densirr lipoprotein chokste:::ol kvds, and l.ri-
gl:yceride levels. this relationship signilkant (RR,
209; 95';1> Ci, 1.24-3.54; P= .02 for trendj Even men with
inlem::u:di.ale 25( OH!D levels were at elevated risk rda-
to those with sufficient 25(0H)D levels (22.6-29.9
ng!mL: RR. 1.60 [95<){> CI, LW-2.321; and. .l5.0-225ng!
mL RR, L4J [95% CI. 0 962.131. respeu.i.vely).
Results: After fr>t v;:rhbks,
deficient in 25(0H)D (::::s.T5 ng/mL [to convert to nann-
nwks per liter. nmh!ply by 2.496 J) we.te at increased risk
Conclusion: Low levds of25(0H)D are assoc':a1.ed with
higher risk of myocardial infarctirm in a graded man-
ner, even after con!rolling for factors known to be asso-
ciated wi.th coronarr artery disease.
An:h lman Med. 2008;168(11 H J i4-1l80
Author Affl!iat.ion<;;
of Nu!rtHon
(Dr;; Gionmnucci ami Rimm
1..iu) an,t
Gizw:mmK('i and Rimm),
Scho:.1l of
Ik;l1.th, lksto\1,
Channing Lahor.HDry,
or
Brigham and
and llanr"rd l\-kdical Sd1o0L
f>\}SlOn (Drs Gtov;mmK<:-i and
R\mm"); and Department of
Pediallks, Medical Univ,:rsiry
t>f Sotnh Chad.est.t>n
(l)rfklh:;;)
A
V,'.R1J:-, ")I' . _., ,_ .. r c t )... .. . . c .....
are not easily by
known cardi.ovasculm dis-
ease ( CVD) risk facturs. In
most populations stud-
ied, the rate of CVD-rdated death is d-
r.vated. at higher latitude;;, increases dur-
ing the winter months, and is lower at high
altitudes. As noted dsewhe:rc,
1
this p<H-
t<:-rn is consistt:m wHh m adverse- dien of
hypovi.f.aminosis D. whkh is more pnva-
lcm at higher latitudes, during win-
ter, and at altitudes. Ah.ermnive ex-
pl<mations for these observations are
possible, but a vmiety of pl<n.!5ihk biologi-
cal supp;m a rok for
min D. The vlwmin D axis <tfkcts
smooth nwsd<- cdJ
v-ascular cakification, th<"
renin-angiotensin syste-m (RAS ), and blood
all of which affect rbk of CVD
and myocardial infarction CtvU).
..................................................................................................................................... .....
ARCH INTEl"' MH)i\'OL HiR iNO l!}, JUNE i),
tiH
Dtspir.t :suggest.ive e('ol.ogk d.a:a
and plausible- mechanisms, directly
hnhng D lc-vds to risk of .MI ar.:-
sparse. A Danish exam.ined 25
hydw:-o.yvi:.amin D (15[0H!D) levels m.e:a
sured in 128 patients admitted to the hos-
pital with ischemic heart disease (75 with
angina pectoris and 53 with acute MJ) and
409 con:.rol subjects and found that
2.5( OH)D ltvds were signiJkantlylower in
those with angimt (23.5 ng/mL j lO c-<.:n-
vert w per liter, m.ultiply by
2..496!) or MI (2.4.0 ng!mL) than in con-
trols (28.8 ng/ml.). !n a New Zealand case-
control study; of 179 p<ttients with MI, caSe$
hl(d a lower 25(0H)l) levd (P= .02}.
which was nwn' in the winw;-
spring (P=.03) than in summ<-r-
(p,. .21 ), The rdalive !'is.k (RR) of
MI decrc.:l.,e-.d acmss quan1ks of
25(0H)D ( <IO ng/mL: RR, l [ refae-neej;
JO-.l3 ng/mL: RR, 0.56{95% confide;Jce in-
DowuJ.oaded lh>.m www.rchinh:rnrn.:tl.com at Federal Trade Commission, on June l7, 2009
1.00.8 .i.\mer.icau Medical A.<r.il)dliltiou. AU righrs t<'St'.rvcd.
0.32-LOJL 13J-l6.8ng!rnL RR, 0.33 !95%
C!, 0.17-0.M]; <md '> 16.8 ngimL RH, 0.30 [95% Cl, 0.15-
0.61 J). M.uhiv:niate <m<tlyst>$ of CVD factor-. di.d
no:. appreciably alter the re;;uhs. A small, nested. ease-
control of Ml based in Tromso lkmt Study
(northern wi.th only 30 cases and 60
controls found <1 slightly nonsignific:mr lowe.r 25(0H)D
level in cases (23.6 ng!mL) compared with controls
(25.4 ngtmU.
hypovitaminosis Dis prC'valemand cor-
e.stahhshing the rdationsh-tp between vitamin
D and. risk of Ml is important. Thus, we prospectively
examined. 25( OH)D concentrations relation to risk of Ml
in a large (Olton of lJS men, whkh is called lkahh
Professionals Fellow-up Study (HPFS}
Mf.TllODS
STUDY POPFLATlON
HPFS is ;l pwspenive cohort Ln;esJ.gation ln 'H '5.29 L 1S male
care prokssion;lhage.d 40 to 75 ye.ars;u.hasdine. in 1986.
This Cl)hort w;;s de&igned primar\!y to associations be
t.w?:?:n tlie; and .inddcnte-." \V<: iafnr-
maicm dJout beahh and <''I"Cly 2 vears bv using a sdf-
admi.nbtcn:d <Jut'stionndre and ;J.bour (Eel 4'yel1r:> by
:1 food freqm:m:y Be!w<:<:nJanu-
ary L 1993, ;md 3 L 1995, H hlood sample Wil:>
questcd. ri ()!t:i all cohon pa.rridpams: 18 225 pmvided
smnp!:.s lk5pondcnt<> wrr<: somewh11t young<'r hut were other
wise si.mJar m nonparticipants. Ha.Y'd on the- cohort tha; pro-
vided Silmples, and aft(t.l: the e.xr.:lusion of p;tn 1.r.:ip;:mts with a his
tory d CVD lldon: 199-t, w;;o identified +')4 witb
.lncidc:.H MJ or WJ(Jtu:.; (CHD} be-
tw;.>.;.>.nt.he da:e ofhb;)d coll:.ction 3L 2004 as-
sesse-d dise:.'t'ii.' sHHus thmugh.]aim:uy 3 1..2004. for 97.J% of the
m.en. ComroJ.s were randomly selected lrm.n p:lrtkipat1!S with ;,1
blovd :>ample whn were alive and wbo did not history d
CVD at w:t a 2J. rmio m1d
mmch;;;-.d for ;lgt:, momh ;md ye;,1r of blood wUectkn. and smok-
l.r:g (risk !>d Eight par1idpants wen' or';gi-
J.uHy C1HH.ro.l:> an:i had.:.m d.urin.g
folkw-up, lt:::P:ing 900 cGntmls fur No con-
trol was sdected twice during the random sekerion pmce;;.s. All
the partidp;mts g;tve w;itttn informed <:onscnt. and llar-
\';ml <.)f PdJlic Health committee revkw
ht}<:.rd app;.ov.:.d t.hc suldy protowl.
1\SSESSM.ENT OF NONFATAL Ml
AND FATAL CI-ID
$tuJ.y !lW mt.>.dkalte:c:1Hd1> ()[all the: par-
fx whom nonLud MI or CHD was repurt.-.d d:ar-
tng t(lll<lw-up. The revkwers masktd w panidp:nn.s' ex-
po:mre status Ll<:h mailed hie.nni;ll!y to EPFS
partkipams, cont<ir..s a qf:cstion ou whether the had
.. pmfcssionaJJy _ ..
in frrt.'.(:<:.ding 'l was con-
firrm:d jJ il woad Health whkh
inch;d.e plus citha diagnostic ekctroc;trdiogmphk
changes or kvel;; of <:-ardiH<: For appmxi-
7l)% of the men who sd.f-repotl.ed Ml. we wntrnned
th<:: diagnosis tlu..se t::w.lhods. lor
Ucm of MI. W('n: that e-irher no further informa:hm aV<1il-
. the. panidpam did not consent. or the
hospital did not send the hosph-al H' a
w>1s n:j(:cted b>1sed on r.he medical record inftnnation re-
crlw.d.: We t>x.dnd.ed from the Ci)n-
sdection process. (kalhs wc<e ide.nti.lkd from state vital
n:c<.)rds the National Death Index or were rc
poncd hy m:xf. of kin or hy t.he Fat;1l CHD w:1s
considered to have occurred if there. wc<s bt.al Mf n.>nfirmed
by h.ospJ.1al reei)rtls or amopsy ll.ndings or if CHD was hsH'<i as
rhc of d.eath o.n death Hit was ;he under-
lying a1:d most and if .:-vidence of CHD
was available. fn this analysis, Y52 paHidp.ams had
MI and 102 h<td fMa! C:HD as 1hr quahlying <'Vent.
ASSESSMENT OJ? MEDlCAL HlSTORY,
ANTHROPOMETRIC D1\TA. i\ND DlE'f
AND UFF.STYl.E FACTOR$
For this ana'lysis, amhmpom<:.lrk dat;I. 'tif.estyk fnctors, and dit:t
wn<: on lhe 1994 Body mass in(kx (HMD
was <:aku!atcd as wdght in kilograms divided by hdght in Ine-
ters squ;ued. Nutrient intake based on a vali
dated food qu<.'stivnnai.re, whkh ln-
quirt;s ahmlt average food intake during the past year using
!:ompo<>hion from the vs Department of
sourn.s, ;,, with tnha data. Physk<ll
expressed as cquivalen! lask,-ht)UTS hascd on sdf-
rqxrted. types and dunuimJs olactivilie$ <.w1a thepn'vil)f:!i year,
1
:
One metaholk cqui.v;th:nt ':quivakru. !O <:twrgy ex-
penditur;:. while sitting quietly for l hom. We de1in:.d rnedical
information. from quesLonnatrcs between
Jan\lary 1, .1986, ;\nd fktembe.r }1, 1994 Thnc prc-
vil)tl'>
on reproducibility of 1he col
data and
MEASUREMENT Of tHOCHEMlCAL VARI.i.\Bl.ES
were in three 10-mLhqutd EDTAb]c)od
tubes, pla,;,>d )fl icc packs, in bam contain
;md rttumt'd to 1b: HPFS blood storage and pro<:cssing fa-
cili.ty at the Ihmrard Scbod of Public l:kah.h via ovt:rnight cou-
rier. Mon: than 95% vf the arriv<:d within 24 hours of
Cl)lk<:rion. The blood sarnples Wc)e rhen cemrifuged and ali-
quoted for stotage !he Y<l-pnr pha::.e of liquid nitrog;:>n frecz
( .. DO''( <.)r colder). Fewer than 15% d' the w.:-re
slightly and few modcra;dv (<3'1!.;1.
[i,;.,mi' ( , . ti i or not c1+(1 1 r rria
1
')<";;} - .
,;V \ , '"' .(.v '"' (.,. ..1 V, 1, '"'\.1 . ,,)_.
:t'l(Oll)D kvt1s by means of ra-
dioitmmmXK\ssav iiS pre.viou,;lv dcs<:ribedn The. ..-.odfide.nt of.
for W;t> l 1.5%. In u subl:t)!wn t)( the 144
m.?:n who provided blood in. and
in 1997 (mean lSDl d [\1.461 y;;ars p<nt). tlw P;;ar-
son pmdut:t. corrdation codt:!eient for 25{0HJD v:m;
0. 70 (P< .oon '' Low-d.e.m:ity lipopn.)tdn cholest<:.n)l
mca:>tued using a direct fmm
Corp, C1l.t.<i.3lidg<:,
l!poprote-in ;:ho-
k'sterolle\'d$ using a <'nzyrm;tk colorinH:'trk assay. x,
1riglyceride i.t>\'ds enzym;<lkaUy with correnJ.on. for end(lge-
nous glyct.>.mF
1
The assays use.d ft)r lipoprotein and lipid ;uuly-
$iS approved by the US h1(td and Dwg Admini:>lraticm for
dinit.al me. an.tl. d variation were lt:.ss than 6%.
STAriSHCAL ANALYSES
wert:. into-+
on common d<:>.hnilions '"f "ddkien(' (:Sl5 ngimU, 'insuffi ..
tiott'' (15 l-29 .9 ngimL). ;:;nd Ksnffkkm" ( 2::30 nglmJ.)
25{0H}I)
We funht!r rlichntmni:::ed the insnff.kkm
..................................................................................................................................... ....
ARCH INTEl"' MH)i\'OL HiR iNO l !}, JUNE i),
t 115
Dowu.l.oaded lh>.m www.rchinh:rnrn.:u.ciJm at Federal Trade Commission, on June l7, 2009
1.00.8 .i.\mer.icau Medical A.<r.i<)dliltiou. AU righrs t<'St'.rvcd.
Abbrev ar:ons HDL 'l:gn-dens:ty lli:CPn:llem: <CJ.R, :nle<!l:"1'tile rii'(W
lDc. MtHl, metli.H:J ic equmlenl
Ml, imarc:-on; nT- 25(0H)C. 25-nvdroX'fvltanur: D.
Sl Wflu :sb--; fa;;tors. To CGnvort total. a::t! lDL to
mmi:rcJes pc Hler, muiiipy by 0.02&9: 25:0H)D to tW !:tc. mu::p!y
by amJ t1()tycendss tc mi:f ;clos ps :!te;, mu:tfp y :Jy u.O 113.
A(;e smckng stan:s a'd or b-co::! r.tl leer. on were matcnea
lf<lriab!es
as we i;lllir: !(jJograms divice:l b heigm :n souared.
range t\t i;.s :1:idpoint i:l:o l 5. l h> 22.) n&'mL .md 22..6 :o 29.()
llg/tnL hrr !ht :naln w tnve-sugau tht ta\':)n
2.:5(();!){) co:1ccnrr.ltions a;;d ot no:1t;l
tal Ml 1)\" nm us.:d
h)f lor lt'tnd, wt> :m)dded the tnt'l!ian
of tl.e 4 categones variahhs j,, the
1r.:cdd. h: lhP mu1tt'-:lflatl' nwckl, we furtha t(r fnn-
;ly ,,fMl bdorc tlw ag' or 61."' ye:m no), a1nhd
mtake (Jwndnni<ei, 0 1-+ 9, 5 0-14 9, t 5 O-l9 9, or -:::.>:30.0
g!d, t)t mi"<:->lng) BM! p:ty!;kal a::tidly
tihs), h,,tory >f di.1hdt:" me:litus. 1 ;--es or awl h;--perltn-
Sil)fl no), ( l)f
mid-Atlantic, ''T s,,uth), ()-3 iNakt \quin-
till's), <1nd antl high-deuscty 1i:3op,-nHtn ( lwksr;rol and
tr.gtyc(::alc levds (qu.ntile,) at hasdnw. Because of the drsign
,)f this the Puds rlh'() from :og:sril.
directly Cj'tirt\;ltes tlw i'1Cdence rat<: (hazatd) rail<' ar:d,
bre. 1he HR.!' ' We the g(o<iJ;,ss cf fit o( the mndds
lts:ag thl' r:ltrlwd de.",'l"ibtd ry Hosmer and
whkh did uot show ;my sig..nifkam lack of ft:.
r or t be :otra d f:ed \h' useti lll' cond il wna t c rt-
gres.j:i,,,, .ldjusted for variab:es \<50, 5()54, 55-
59, G0-64, <'r 2::65 ,.:.,:;,s lnev('f. .r ,\lr
lc1H!,a!td nh)ntb L)l {:') J Fm th{-!r,.ain
analysi!', uncot:di;i,'nal log::>\H: wuh adjl.\'itnH.'Ilt {,,,
variables yitJded &Jm]ar n'suks a-; c<mdt1wnall\1gistic'
H';;re5Sll>r. or irllt'r<Kiion 'i\Tre hasfd on IIH \\aid h>r
tlw mter;J.d;m; term :X l3l()ll)) l<vdl, \Vtlh the Yari-
abk ;>nd vll.ant'll D 111 the mGdd as M!
E' values arc l-t<uld; P< 05 w.>s 'it>Jtistically >:gn:l!-
l'Hll. A:l ;maiyse-s p<.:IJ(nmd :1s:ng SA.S
ware. wrs1;>r> 9.! htst'llHe :nc Nonb Car:!ina).
RESIJLTS
Sdecte:d at:d hi<) marker :ev!:'L'-> of cases and
arc given in Table 'I. As twd ''
highe-r HMC lcwtr IC'\d Gl physical acnvJty, and less
akoh,>l im;-.ke and wer<." m'>re !lkeh to have;;, famth hb-
tory or Mi before 1 he age of 60 yeHt:'- and a histi)l')' (;f dia-
betes mdliiU!'- and hypertension. In addition, ca ..... had
higher len+> ;)f towl <md hpopwtein dl(}--
lesterol and triglyt:cndes but lower levels of high
llpoprmcin Plasma 25(0H)D
we:t: siguilittllldy !nwer (2 3.0 ng/:nL) than m
(2-+5 ng/mU (P= 002)
We measured levels ')r percentages d ;,electe(l
factors ,wmss 25\,0H)D in comro:s
(Tobie 2). tvkr: with ](!wei' 25(0H)D le-ve:s more
likdy to be smokers, less physH::at:y act:Ye, and
heilvier and less l:kdy w be white and to h:we p<.nmtai
historv d ML Thc-v abo !tkdv w a mul-
;:iv:t,u;tin tlwy drcwk less and they
were mort: in n\mhc:rn with !own
25( OH)D a sngges1ive bw n<>t s1 ar,sn..:aEy slg-
nifi;;ant higher prevale::ce (}f dlabetec. mellitus <tnd hy--
pcr:e:J.swn ,md stgmfa.:<HHly higher levdf> of
i(\{:$ and lower 1evds of high-(knslty
dw!c-stt'rd.
Table 3 provides RR::> Gf Ml non{:ual Ml
plus faml CHD) dunng l 0 year;-; of ldkw-up <Kross 1he
vf 25(0H)D Altc>r ,Hlj.::.<;tm\.'Ht {o,-
matching factors. rnen with dcfident <lf 25\ om[)
h,tJ. asigmficanlly dev<ttcd risk of Ml (RR. 2 41; 95% C.
i P< .OOl ior !rend). In 1he nwdd
wilh<)ut plasma hpids. thr. RR was ::>omewhat a:tenuateci
buuem<>ined W.R, 2 01: 9'5% CI, 1.22-3. '0;
J> .Ol for trend). Arter iunher fm pla:o;m;, lip-
1ds. the RR was 2.09 (95% Cl. 1.24-3 54;P= .C21N \rt>nd"l.
The dJd not rh<mgc apprecw.hiy after exduding
tht: first l yc,ns of (RR, 1 .97, CL J. l.G-
3.51: P=.05 for trend kvds of 25IOH:D).
In al:emaltvc we cx,lmined ::.ea<>on-speLific
quimJle:- of in :d:mon w MI risk. For those in
the hcuom vs top quintiles. the mnl!hariate RR was
l 94 (';/5';;, Cl. 1.23-3 06). c,)mpand with men whh ad-
Dowuloaded 11-<m w,o,w,rchtnh:rnrn.:u.com at f"cdcral1rade on June l7, 2009
1.00.8 American Medical A.<r.io;,datiou. AU rights res.-.rvcd,
cquatt: 25( Ol OD l<.'veb, \'1 ith ins,lllicient vatues of
25(.0H)D werr 'With approximately" 50'\' in-
m risk In the !ull mndeL the ('OdTi-
cknt 1-nglml. ina""ment HJ 25(0H)Dwas -tJ.0214
\SF. 0.0099). ln.d:c<Hing that the r!sk d M'i (;kcrcased by
2 l'X' per 1-ng/mL in 25{0H)D We did nm have
to ;est
\n = 352) and fatal (n"" !02) cases, but the j3 coe-ffic,cnt for
Ml risk i;!l5(0WDsuggestedastron-
gt'r asscciarwn for fatal Ml ( 4. )<'i) m rL..;k; 1hw1 fer
nonfa1.1l Ml (1 S%decre;;;,;;e in risl() Fun hermon>, tht' mol-
uvariate Rg ior delkien.t vs suitkem 25( Oil )D vdues did
:1.01 change appredabl; wht'n Wf n::tdudcd C-reaeuvc p.m-
( R R, 2. 04: 95% CL l. 20-J. or eslima! ed
llir hltrat.on rate bL'it.TI on mca..;.;ured pLtsma t:reatinine level.
ag(', sex. and n1c<' (RR, 2 09; 9'5% Cl, l.B-3.54) in th<.> !ul:
mnlovali<ttf Jll\)dd.
\Ve :ested for intcr,l<.:Lior! acmss factors to f.'\-
<nnmc I he between 25(0H)D levd
and Ml risk varit'd \Vc did nm 5:atb!ical evJdenct>
d interac:ion by U'"" .85 {or mterac:t:on), high hlood
pre!>Sure (P=.84j. Hrv1l (P,.87). asp:::n use (P= 92},
physk:at a cavity (P"". 21}, alu,hol (P"". 53), low-
denstty ltpl)protein b e1 (P= ."33). M trtglyt>
t>ritie !evd (P= 73) Sugg(;:>tive evitie!:cc: wa:. obst.>rved for
<m intemcthm by bigh-densny lipopwtein
w:t h a smmger mverse ,\SSt)Clalion wi:h
25(0l!)D kvd in with a hlgher lipo
protein cholesterd level (P= .06). Excluding men i.ak-
ing ch()ksteroi-l<'Werlng drugs iiit basdinc. th<.> muh ivar-
mk RR for vs sulltciem 25(0H)D
VIS 2 30 (95<:-& Cl, 1.33-5 97:. Because tl:ns subet in-
du(led a lin:ated number of Wlth diabetes
:nd1ltus at Wt' evuM not c,1kulak effl'e: esri-
:nates in this subgroup; lwwever, d pm
i.ic-q::mnb did not sub5tantivdy alter rbe resulb. Stmi-
iarly. !he of with :1 p:trenwl hiswry
ol MI t!w of 60 years <md tttrrt'n l sawk'rs did
'HH afft.>cl :he results.
In thi." colwr: study. tnen with cin:t.:l;\:lng 2S(OH)D kv-
ol at kast 30 h<:J httlf the risk l)f
MI. inckpendemofotherCVD factors. Theassodati\)Twas
suggtstivdv stwngerl{lr fatal CHD. but tht: of cast:s
W<lS h)<' small t\.' make ckfimttn> conebsions. Alth<'ugh
traditklnal CVD r:sk factors (eg, lipids. hypertcnsk!n, dia
betr-;, mellitus, and smoking) remained ;,trong risk lac-
wrs :n this poputm:o:-:.. vitamin D delkiency 10 be
an risk factor. Oniy 2"3% d the mt:n m the-
HPFS had kvds of 2'5(0H)D ('{at least .30 ng/mL. This
is ty111e<tl of many populati()l1.". and th(;' prc\'a-
vi i" higher lt' suhpopuhuitms sudl
dark-skJnned and ekkrly [n JndJ-
nduals in s:.;,n-rich envmmmenL'i. v.hcre dothing or cul-
tt.:r:tl praetice-.s do not appr<-dahly limit vitamin D produc-
t ton, 2:')(01 CD d .34 to 90 ng/rnl. are at:aindY but
fnmt the pre::>ent :.tudy we cam1(H evaluate whether lev-
els th<m 35 ug/mL would be assomnd wuh '"'n
greatrr Ml nsk reduct;or..
ims. See 1iit;:e l
S! factor$: To . HDL. 'ltHI LDL dw:es!11ro! lc
mi:!imo!es per !iter ,,. ,,IIi ply by 0.0259: 25(0HiD 10 nanomoles per
mul!lpty :y 2.<'<96 1n: : iglycer:aes tc mi!:imoles per iile', 'h: t:ply by
0 0113
3
A:! var a!i:es cthertr.an age and 2:i{OHJD !eve! are <:ge standanl:zed.
3
at en as v:e ght >n kilogra:ns dtvid'd bv ;: n me:m
The design, ti'e high ft)H('Wup rail', and
the use of a nH1rker large>;- precluded n:wj,)l source:.
of bias, such as bias ,mJ. sdr-cnon Ina.>:>. \Vr- ex-
dnded men di:tgnos<:d as hav:ng CVD t.t baseline
furthermore. results were after e:Kcluding ftrst
2 years follow-up, arguing a,galnsl rever:-(:' causation
hias. which nnght '".:cur if mtn t() an MI
st.,.ved mdoN:. and. <herel)r, <lv('ided sun exposure We
for and slr<.l! ifkd hy major wHriates that
affect Ml r:sk and 25(0H)D indudmg
(whkh sun exposure), BML
race, muhi\itamiu u!'e, ,md marine tJ)- 3 int.ake. as fatty
Hsh is the significant natuml sour(;e (}{ dict;i(ry vi-
t<.min D. '"Wf. C\)OtWlled ror the lipid ri,;k !.-.ctors
ol MI. Jn <1tkli<itm, we C('Osidered tl;l' estimated glomer-
Dowuloaded t)<m W\>,W.rch\nh:rnrn.:tl.com at f"cdcral1rade on June l7, 2009
1.00.8 American Medical A.<r.io;,datiou. AU righrs res.-.rvcd.
Abbreviatiof's: Cl, confidence interval: M!, myocardia! fnfnrr.tion; rvw, mumvariate; tJA.oot applican!e: 25(0HJD. 25-hydroxyvitam:n 0: RR, relat:ve risk
S! factor: To convmt 25[0HiD to nanomolas per !iter. rm;!t!ply by 2.496.
matchinq variab:es /age, mor;th ami year of iJ!ocd ca!lect!m:. ami smoking stltus) ar:d tamliy histOJy ol M! betore the age of 60 years. hlstcry of niabet!ts
llistcry <::1 intake, !;t;{l\i mas:> phys;c<:! actil;lt>;, re!)inn, ;;luitlvitautirt U>!i. w3 intake, l>tatus.
b1-,1\f2: all the variables in MVi anc high- and fi;)v;J<otein cf:olesfe:ol and triglyceride levels.
ul<n fihr":ion rate because circulating 25(0H)D levd.s
could be lower in lndividuals with chr(lnic dis-
ease, which is a factor for Controlling fi)lthe
glomerular fHrration r;ue did not change the
:results. Given the sll:t'ngth of the association
between 25(0H)D kvd .ond Ml risk. and the f:.ct that
comrdling for thest racwr-. did not appreciably
the magniwde of t.he assodaHon, substantial. residua.!.
confounding by these fiKtors is not likdy but cannot
ruled out.
lkcliluse 25( OH)D kvds largdy by sun ex-
posure, plausihk that somt: other consequence ()f sun
exposure other trum vitamin D pmducr.ion i::> respon-
sible- for r.he ohservt:d association with ML
tess, uwch supports mechanisms vi-
wmin. D could CVD risk Of the potentially relevant
mechanisms, viwmin D affects vascular smooth musde
(dl infiammation. v;t>euhtr nnd
pressure through the RAS.l
rhe HAS hdps regulate blood pressure, lev-
els, and volumt hm:nC'osrasis, and exctssive RA.S mimu-
Jaticm is with hypertension. Animalstuchest.'
show that vit<unin Dis an imporwm regulator or the R-'\S
svstem ami. that.l ,25-dihvdroxrvit.amin D. the activated
of vitmnin D, ten in gene Di!:>
ruption of the vitat:nin D receptor gene leads tn elevated
renin pmducr.km. cardiac hypertrophy. amlde:v,;ted blood
prt:ssure in
In a mnd.omized controHed.
of either UV-B or UV-A administered rhrough
tm111i n g hoot hs, UV-1>, vihic b 2 5 (()fl) D levels
bv 162%, W<1S effective in 24-hour
blood ptessme (by mm Hg, P ';; .001), wht'reas tfV.;\
did not affect 25(0H)D levds or blood prcs..o.;ure. In an-
other RCT
3
(; of ittdivJ(bals with low vitamin D status ( <2.0
ng!mL; mean, 10 ngimL),
tion with 800 IU nf vit.am.in D resulted Jn an Jncre.ase in
serum. 25 (0 H )D of (J> < . G l), a decre<tst: in svsto I k
blood pressure of 9 3'};) (P= Cl\ and a d.e-
in diastolic pressure of 8.5% (P=. 10). In the
HPFS and the: Nmses' Health Study,
51
during 4 years of
and women who had 25(0H)D
kn'ls than 15 ng/mL 3 timC's aslikt"!y to have
.a new diagrwsb of hypertension in the next4 years com-
pard with those wi.fh 25{0H)D kvds gre<>J.er than :}0
:;g!mL f\.n association 25(0H)D levds
and blood pressure was al.so found using Third. National
m1d Nuttition Examinati>m Survey
Calcification is a common feature of
and nearly all angiographically signifkam lesions
Cakif',cation of coronary has assn-
dated with increased risk of MJH and poorer 5-ye.or sur-
vivaL'; Atherosderolic mkification is a proces& regulattd
in ways similar to ske:lNal A signlflcant
exists between and n.scuhlr ntl-
cilicatiou. suggesting that mechanisms
w bone. may .:He-ct cakifkndon in
the v':lscuhuure. Ltvc!s D have
shown to be. a:::;:::;odiiitcd with vascular cal-
dfkaliou,>r suggesting vi!.<tmin D may Hffen MI risk
through its effects on vascular caktf:c":ion.
Other mechanisms could. account for or contribute to
the association between 25(0!{)1) and Ml risk Vitamin
D ddkkn(y, possibly combined with low cakium in-
take. has been associated with impaired. fasting gl.ucose
and possibly risk of type 2 diabeks mdlitus,
37
'
1
') risk f,;c-
wrs for CVD. Vitamin D delkienqr has also bt"en asso-
date.d with a cytokinc profile th,;t lavors greater inflam-
mation (eg, higher C-re<Ktive prNein and. intcrkuktn 6
levels and lower imerleuki.n 10 levds),
4
Ht whi.eh could
predispos(: w heightened Ml risk. Finally, sea!:>onaltes ..
piratory tract. inJecti.cms, particuhrlyinllucnza. have been
proposed w acc()ttnt kr the winter in mort<1iity
d.ue to
and hypovitam.inosis D could contribute
to these
Tw case-<:<mtrd studies
2
3
and a 5maH prospective smdy
1
found that individuals with low 2.5(0H)D levels
higher f1)t ischemic ht:<ltt The strongest test
of the hypothesis that vitat:nin D lowers Ml risk would be
from RCT. Two RCTs re-pone-d on CVD .Itt a UK study
of 2686 men and women, the parli.cipallls were mndom.-
ized to receive 3.30 IU of vitamin D daily (administered as
100 OOG HT of oral vitamin D 3 every 4 months) or p1ac(;'bo
for 5 The in-studv 25( OH)D levels were 29 7 nglml.
in the vitamin D group .;;td 21.4 r:glmL in the pla(:ebo gr,yup.
There wao; a nons.':&rnillcant.decrease in CVD incidence (Rit
0.90; 95% CI, 0. 77-1 .06) and CVD Om, 0 84: 95<y.,
Cl, 0.651.10) i.n the int('rvention group. B<ts('d. on the
present swdr. a difference of 8. 3 ng/mL In 25( OH)D con-
centration woutd be <tssociated with an RR of G .92. which
is with previous results. A :rccem meta-
..................................................................................................................................... .....
ARCH INTEl"' MH)i\'OL HiR iNO l !}, JUNE i),
t
DowuJ.oaded lh>.m www.rchinh:rnrn.:tl.com at Federal Trade Commission, on June l7, 2009
1.00.8 .i.\mer.icau Medical A.<r.i<)dliltiou. AU righrs res.-.rvcd.
anal ys:l..s -;o of mort.tti.ty as a stcondary f:nd point of RCT s
wi:h varying levels of viwmh; D vs placebo contwb found
a slatiMi.caHy signi.fkam 8'/o reducl.ion in.Jisk of f.N<d tnor-
tahtv in ind.lviduals who had received vitamin D. Al-
t1w amhors could not mor-
tality, the rd.ativdy immediate efffct of a large enough
magnitude ro m'malily would suggesl a hen-
dhmlCVDr.i.sk
rhe largest RCT of vitamin D (and cakimn) st,ppk-
and CVD risk was from the H.ealth
lnitiahve,';
1
in which 36 282 postmenopausal women re-
ceived ei.ther cakium ( 1 000 mg/d) and vitamin D3 (cho-
lecalciferol) ( 400 TUcD or placebo. No was ob-
in MI- or CHD-rdaled (h;u.ard tatk), J .04:
95'X Cl, 0.92- L 18). The:sc results seem to he in co.ntrast
ro the present. findings. 2. possible cxphrna-
tions. first, despite our eff<.ms w exdude confounding.
!.t is possible that uncontrolled or residual
explained these results. Altemativdy, the mnge (lf vita-
min D was much wider in the HPFS. which al.-
1owed U$ to an assoch1tkm. ht:
tween the medians nr the top and bottom categ<Jrics, for
which we observed an RR d approximately 2, was 23.5
n.g!mL 05.5-12.0 ng/mL), and the cakul.attd
tlon in Ml r!.sk per increment of 1 nglmL of 25(0H)D
was 2!\, ln the Women's liealfh Initiative study, the dlect
of on 25(0H)D kvds was not reported,
but hm>ed on and compli;mc(:, L;:ppe ct al
mat.ed. it to be only 1 Hased on the p.resent data.
SU(h <m increme.nt would be to have. only a 4<;-1,
re-.dm:t.i.on in risk To inueasr 25(0II)D levds from 12
to 355 nglmL woutd require approximatelr 3000 IU of
viwmin D daf!y.
53
Although such imakes may seem high
bv current standards, bcreasing demonstn1tes
r:o toxic effel:ts at 10 000
current sources of vi.tamin D provide mudt less {eg. a
gbss d mllk has 100 llJ), those who
adrievt: high levds such 35 ng/mL nat.uraHy Jo so
largely through sun exposur.:.
Vitamin D ddkie:ncy has been related to an inueas-
i.ng numhcr or C(mdi.Orms'
5
and. to total. mortahtv_)'J These
re-snlts further support imp>rtant rok ior D
in Ml risk. lf this associ.;:ui'm is causal, which remains to
bt estab!ish<:d, the ameum of vitamin D required for op-
tima! benefit may he m.uch hi.ght'r than w:m!d he pro
v1dcd by current recomme.ndat\ons (200-600 lU!iO, es-
pecially in those with mininH<l sun exposure, rhus, the
present findi1;gs add further support th<ltt.he curre:Ht di.-
of vitmnin D need w he w
have an effect on circulating 25(0H)D levds substan-
ti-ally lor potc.ntial health benei1ts.
15
Accepted for Publication: December 18, 2007.
Corresponde.ncc: Ed.w<\rd Giovannucci. MD, SeD, De-
mntm.em of NutrilimJ. Harvard School of Pub he He.<1lth,
()65 Humln.gwn i\vt'. Boston, MA 02115 (egiovmm@hsph
harvard.nlu).
AlUhor Contrihmions: Dt had full
to ail of the data in the study and takes ft:5pG11Sibility for
the 1megrity of rhe dara and the accuracy of r.he :malr-
sis. Swdy urncept and de-sign: Giovannucci .Rirnm. Ac-
quisiiirm of data: Giovannucd. Uu, and Rimm.
au<t interprttaUtm dala: Gi.ovannucci. l.:iu, and lid lis.
Drajling of the nwn.uscri.pt: Giovammec.i and Hollis. Cri.ii-
ralrnision 1he nwtt!iS(ripl Ji>r imporWttt intd!eriuct! wr.-
ioli: Giovammcci, l.lu, HoUis, and Rimm. Stari.s!iwl anarr-
Giovannu<;d m1d Liu. Obtained ftmding: Glov.tmucci
and Rimm. Adminisn(ltivr, t.cdmi.w!, and matai.al. sup-
port: c; iov;tnnucd and BolUs. Swdy :>t1pervi:ilon:
GiovannuccL
Hrumdal Disdosure.: Dr HoHi" is a con::mltam for Diasmtn
Corp.
Funding/Support: This study W<1S supported by grant
P01CA055075 from the National Cancer Institute and
by grant ROl FlUH5464 from the Nat1nnal Heart, Lung,
and Blood lnstirme.
Role of the Sponsor; The sponsors had no role in the dt:-
sign and conducr. of the study; cdkdion,
analyses, and imerprer..nion of the data; or pr"pam!ion.
or approval of the. manuscript.
DisdHimer: The com em of the present smdy \s solely the
of the authors and should no:. be consti-
mte.d to the offidal of the. National Can-
cer institute or the Natio:nallnstitutes of H.eaJ.th,
1, zmermann A, ss. Kc&nsr R PtUiing cardiovascular disease nntl vi
tami11 [) im>ulfbiency io!o 8; J Nafr 20G5:g4(4) 4B34St.
2 lund !l. J.lund B. OH. V'lamin D and i$(;fleem!c i;eart
Hom; MB/!;i:J Res, i 978;1 Of:l
3. Scram1 R. J<dswn ft H:Jidcway IM. U:n T, R. MyGcardiai H;;rcli:;n
!s inversc!y wi!h p!asma 25-hydroxyvilemin 0:> tevEt!s: a ccmrrHmit';
bas<:d study. In! J fpir!emiai 19S1l;19(3) 55g-363.
4. \{k S, Try K, Thtlfle OS, Fun!e OH. Trcms;; H::;ut St:;dy: U
ami IJIY(car;!iat infarction. Br Mer! J. 19?9;2f6Hl3):176
5. Hoikk Mr. Wamin u dafidem:y. l.JE;;gt J M;;d. Lu07;357(3}26&-231.
6. Rirnm ES, G:oannuccf El., Wil!ctt WG, ct a:. Pwspectiw of a!colwl wn
and risk ol corQnary in mllrl. i.11ncei. !991 ;338!!>75};
464<168.
7. Rimm f.S, S.iovannucci EL MJ, G.4. Uti:1lB WC. P.ll
prcducib:!it'i and va!idit; of an selfMministerea 5emiquantitlt!ve tofru
::mono mi\lo ho<llth ptdessiom;!s. Am J p!aem!oi. 1992;
a. Rl, B; eshlw NL Retrcspectve studies and lai!me time mods!:;.
i$78;&5\i l 15:3153
9 Rose GA, H Sur!I1Y Meiflo:Js. Swiizmliln!i
Wmtd Orgfi:lilalian; 19a2. WHO Mo:log;aph Serias 5!!.
1 G, ut Composition of Foods: Raw. Processe!i
1
PmpJnJ!t.
i%N9iil. Agrieu/t::r<ti JirwlltJotJk, wasnir:oton, OG Gov<lmrmmt Printing Of
fice; 1992.
11. Ainsworth BE. WL Leon AS. r:t aL :/physical act;vmes:
c;:ts$ificat!ou of enHruy cosis of hurmu itclivi1ies. SD! Sports Exert,
l9!l3:25{1j71-80.
12, Rirr:m ES. Stampler MJ. CQI\iitz GA. C!H<W CG, Lit:nlS. Wll:!ffi WC. Vaiidi!y ol
sell-reported Wlfisi lfnd nip c!rtumfereoces in men wc.ne!l. Epidemioi(I{JJI.
990;1 (6):466413.
13, Giovannucci F.. Coloi!z G. Stampler MJ. ol alcohvl con-
sumphm by a simple questiMnaire. Am J Epidemiof. i991:
14, Cnasanlawr S. Rimm ES, MJ, ul al. ReproducillH:t'; and validity of a
physical activity Questionnai:< !Cir male heait!l pmfessiOn<l!S.
pi(fcmio!vyy. 1995; 7 p }:81 v8&.
15, A, Rimm i:G, Giovannucc! 1:1. e1 at A smdy of nutriliQna!
factors ar>l1 !JS rnm. Cirt:iiiation. Hl92;86(5):l475-1484.
16. Hu F8, leitzma.nu MF, Stampfer MJ, Culo:tr GA, W:Uett WG, Rmw ES Physics.!
activit/ anu lt!lttcning in mi<lt!on 10 for t'!ve 2 diabetes mellitus :a
mort Arch ft1tem Me!i 2C-()1; 15 i (i 2):1 542- t 5-18.
17. Ho!li> BW, Kameruc JW. Selva.ag SR. lcr<lnt. JO, Napoli ,JL ol
vitamin D S1?1us D\' mdiolmmuncassa>J using
tra<;er. Clin Cilsm 1993:
B$(3) 529-533 .
..................................................................................................................................... .....
ARCH INTEl"' MH)i\'OL HiR iNO 11}, JUNE i),
t 1?9
DowuJ.oaded lh>.m www,rchinh:rnrn.:tl,com at Federal Trade Commission., on June l7, 2009
1.00.8 .i.\mer.icau Medical A.<r.i<)dliltiou. AU righrs r<'s,..rvcd.
13, Pi at.:: EA. Leit<:msnn Mf. Ho:!is BW. Wil:e\t WC, L f'!asma 1
dih;>droxy- an(i 25-hyt:roxy'litarnir. D an(l subsequent risk ot i)rostale cancor. C.7;;-
cer Causes Centro!. 2m)4:15(3):255,..265.
19, Hifai N. :armott: , K, Law T. AnaMical aml cl!nir.al (letformante ct a
homogenous en1ymatk LDL-cholcsterol11ssay c-Jmparcd with ultmcant:i-
!u;;ativnd<:xtran nmlho(i Ctin Cilem, 1998;44(6. pt 1):1242
1250,
2C Sq;1iwchi H.Uii Y, H, et aL mor.surem<1nt cl high-density li;:cp:-o-
teir. ir >erum w:ti1 "?nzymes and sui
fateu ;:,-cyctoaEtxtrin. Ciit1 Cnsm.
2i. Stinsh:f;f K. Wsisshaar D. F. D, G:ube; W. Steier E. flelalioi1 ije-
of giycaro: in tn;man scm. Ci!n Ch!Ji1l,
1977:23\6):Hl2fH032.
22 Thomas MK. Uoyd.,JtH1es DM, ThadhMi R!, Et al Hypo;;itamirmss Din ma:!icttl
inpatie;,1s. N Engt J 19fi8;33S{12};??/ 733
23. Rothman KJ, Greenland S. Case-tcntroi studies. ln: KJ. Greenland S.
Modem Cpidiimia!ogy. 2n:J ::d I' A: Uppio:QttP.a;;en f>ubiis!J
0fS; 1 998:93114,
24. Hosmer S. Applied Logi.'ltfc i?Hgressfon. 2nd stl Ne\.: York, NY:
J<>NI W!!r:)l & Sons nc; :woo.
25, Hoi!is BW. 25-ny!iroxyviiamin D im!!r.at!w ot vitamin D sulli
cl1!ncy: tot 5stablishing a new offacHve recnmm::n-
j;;t!onfQrvitami;; 0. J Nlitr. 2005:135(2):317322.
2o. cnonenoi M, Scragq R. 25-liydmX';vitamin n, insu!ill nnd
"'
C.l.
20.
tion in the T!Jir:! Na!iOiiit! Heaith Ntltition E:<.an1inatlcn Kiliai!y inf.
2()01:"!1 \2}:131-139.
Li YC, Qiao G. lJskokovic M, Xiang W, Zhenu W. K(mg J. Vitamin D: negative
reguitttcf of the fenin-ao;;iotensi:: biood p:essc:re. J Ste-
roid Eioch!Jm Mol Bioi. 2004;89-90i15):3c7392.
)fang W. KCll9 J. Chen s. st aL Carfliac hypuimphy in vitamin D
uut rG!a Qf 'yste:m:c and renin-a:1yiotur;siu systfms, Am J Pflyiii[)i
Efidoc!I!Wi Mltti11J, 2C.U5;283!1 U:1 doi:1 0.11
Kr<:nsc A. BHhrin!} M, Hupf<nnml!cr W. il:)!ick MF, Shlwna AM. Uflm'lidel Band
h!ocd f)rest>ure. l.i!iiCi!! 1W8;352(g12S):709710,
3\l, Pfairer :.:. Eeguww 6, Minne HW. Nacntil)al! D, Hansen c. o! e short
ti!rm viti\mln Dt3} and calt:icm supp!omilntattnn Qn tlf:lcd p;tlSSc;ro and para-
nryroiC in -..rouum. J Cil:: fnc!ocrir:ci f.,f:tab, 2DC1: 86
(4):1\l331637
3i. Fo;man JP, Gi:l'lannucci E, Ho!mas MD. et:,L f'!asmil25-hyt!rm<yvitam'n n
el> risk Ql Hwetlcmsion. 2007;4S\5):;QS3-1059.
32. Scm@ R. M, 3e!l C. Serum D. el!miclty, atal
f)n:ssc;re in the Tll'r:i National a;1d NUtritiwn Examin;,Mn Swwy Am J
HyptJtiens. 200UCPi:713-719,
33. Honye J, Ma!Hm DJ. Jain A, et at Morphclfrgical effects of corcnar; an-
giuplasty io vivo by intravascu<:;r uill<tS:iun<l imai)ing. t:ir;:uiatfcm. 1992;
!)5(3} Hl121025,
:14. Baadenkoot WI:, D.1cud AS, love ElM. C.1idlca1inn fil the ccrcnary and
its r&k<liunsll\p lo :md :ntarctt<;u, Am J Roentg?no!
RMium T!1i!t Niil:i MNf. 1954;92:865871,
35 Ma:golis JR, ChH! JT, K:lng Y. Ps111r R!l. Bahar VS, K!sslo JA. The diagnos!ic
aud pro:vost\c slj;n\ficancr: of ccrwary artery ca:cilic<lt\on: a fflr:ort of 300 cases.
t?affiotoqy. 1 gso; 137!3):f09 6ic .
36, W3teon KE. Atmllal ML, LL. al. At:t!Vil vitamin 0 am in
v::rscly corrit!at::d with terr.O<lrt Cfu:iJiJ!ivii. 199?:96(6}: l '155
1761;,
':37, iG. t!an:s SS. Stark PC. Daws(mHugtes B. Tt:e effects of ca!ciurn aml
v:tamH1 Dsupp!ementafifrnon blood glccsea!ld markers of inflammation in !lcn-
\iiabet!c Jdults Care.
38. rittas AG, D:,wsm!il<;ghus S, U T. e1' a f. Vi;arn;o D r.od CllkiiHll intako i;' relation
to 1ypc 2 in wome;;, C.qm, 2(;1)6:29(3):650656,
f'ittas AG. latl J. Ht FB, Dawson-Hughes B. The role :;f vitam'!! 0 c;llciurn in
t'tP!l 2 oiabetus: a syslnmatic meta-anaiysis J C!in Eru:iocrinoi MetBil,
2001;92{6\:20112029.
40. fl:aahtloo!iZ. Hcssein-rJszhad A, Karim; F, Sh31aeiAR, ln:ijani B. Correlation be-
tw<mn vituwin 03 deficiency and in prr:gr.a11cy. Di<beres Mi!!iio
Res Rev. 2C{)S24(1):27-32.
41. littermann A. Dwnoinski J. Steh!n ?. Low vilam:n lJ sta!!Js is associated w!tll
!ow cnni tJkot! flwe<s of the c<;tvkino Hl. p,1di
:itr lmawrwl.
SS, A. G. Berth:;la liK Stehie P, t<oarler R.
Vitamir; D improve$ cytokina nmfiles til nat!ents with conges-
tive heart laibre: a randumlzev. placet;Qccntroi!r:d lri;;L Am J Cii11
!liiti. 20013;83( 4 ): 754-"{;}9.
<!;), Mai1Qrt 130, Gorden SA. Cruz J. F, Ca.ntornll MT. Cytok!ne Profile in pa
tient<. with mu!lip!e scler01>is 'tirdmin D . .I t!tfurofmmtli:al.
2Q03;134( 1-2}123132.
44. Timms PM, Mannan N, Hitn1a'1 GA. ct al Cku!atin(i 0 i\i1d
tiun in T!MP-1 respocM witt! VOR for inHammat<>rv
damage if; clunniC uisor:Jms? QJM, 2G02 ;95(12}:787 7%.
45, Van den G, Vao D. V3llhove f', Wouters PJ, Oe Pourcq L,
Soui:lof! fl. Bene turnover in crmcal Uness: eft:Jct r,f vitam if! D. J Cli!!
Endocrirmi ,\-fota!J. 200a:88(10):4823-4532.
46. Mathieu C, A<iorini L, Tile corping cl a;,; Q! 1,25 <JihyorvX'JVitllm'n 0(3)
as immnnQmcdc:latory agents. Trends MoJ Med 2002:!\(<1):174-179.
4/, Simonsen l, Sllarma A. Par\io SA. fedson DS. MmerMA. ln!HJEi!ll3
am! wintar increase in mmtalfty in the Llnitet! Statas, i 959-1909. Am J
Fpidemio!. 502
48, JJ, Vieth R. Umhnu JC, r.l ;;!. Epidemic infh;en<;; and iiilamin D. Epitie
mioi !!Jfect 2005;134(6} :129- 140.
4S. Jr-. UNg M. ;;pidr:mic infiu;;nza a::d v<tamin D Epi
d;;mfo! {;;f(;{rf. 2007:135(7)10%-10!36.
5\i. Autier P, Gand!ni S. V!lamin D tolai a mHla-analysis
o! randQmile:1 CQHircliod lri<1ls. Arch fnt!lm Med. :?.007;167(\6) 1730-1737.
51, Hsis J, G, r.en H, el aL CaltiumN!lamir: D supo!ementslicn and cenHo
vascular a'lant;;: Wum<n's Hallllh !nit'ative. Cin:a!,1tkm. 2007:t15(7):S46-85t.
52. Lappe JM, P, Davies KM, ER, Hegoey liP. Vitllmin D
a1l<i calcium :;l:ppiementatioii :&ctucss cance{ {rsk: resui!$ of a rafldornized triaL
Am .J G!in Nulr 2007;85(6):1
53. Heaney RP. 0.1vies KM, Chen rc, Hc!ick Mf. Barger -bx MJ. HHmm suum2S-
r<!S!)nnsr: to e;<t;mdr.d wilh cholm;;;t;;F;lwi. Am
J Ciin 2003;77{1):204210.
54. Hr.\llcock Jtt Shao A ViEth R. Hea'1e<f assessment fwr vi\amln D Am J
t:Hn fliiir 2007;85\1
..................................................................................................................................... ....
ARCH INTEl"' MH)i\'OL HiR iNO 11}, JUNE i),
DowuJ.oaded lh>.m www.rchinh:rnrn.:tl.com at Federal Trade Commission, on June l7, 2009
1.00.8 .i.\mer.icau Medical A.<r.io;,dati.ou. AU righrs t<'St'.rvcd.
I
Promotion of frequent tanning sessions by
indoor tanning facilities: 1\vo studies
Harry T. Kwon, MPH, CHES,aJont A. Mayer, PhD,
2
Kristina K MPH,a HeoryYu,
Elizabeth C. Lewis, MPH, and George E. Belch, PhDb San Diego, California
Background: Indoor tanning may increase the risk of melanoma and other healr.h problems. Frequem
users of indoor tanning facilities may be at partit:ularly high risk.
Objective: .1n study l our purpose wa'i to a!ise:-:; r.he prevalf'nce and nature of indoor tanning
advertisement:;; in study 2 we aimed t\) tanning fadli::y <:omplia.nce to te<:<rmmended exposure
schedule:;.
Methods: In study 1, tanning faci!iy over a 4-momh peiiod from 24 San Diego Counry
newspapers were monimred. [n study 2, we a&.<J::SSed compl!a.nce with exposure schedules
via a telephone interview of 60 San Diego C;Junty r-anning facihtie..o;,
Results: Approximately 75% of the indoor t<mning advertisements promoced unlimiK'<.l tanning. Only ')%
of fucHities were in compliant.--e with recommended lannlng schedules, and offered "unlimited''
tanning packages.
C<mclu#om: These findings suggest tha: the ill.door canning industry; through in<.:entives that
allow frequent sessions, may be promoting overexposure ID l.N R. legislation iS needed t) address
this i:ssue. (JAm Acad Dnmatol l 002;46:700-'5.)
W
ith an expected one million new cases per
year, skin cann:r is the most <:ommon of all
cancers and accounts for ncMly half of al.l
cancer cases.l Since the 1970s, the rate of
melanoma has increased significantly to about 4%
annually and will acco unt for more than. 9000 deaths
this year.l The link between exposure to solar ultra-
violet radiation (T.NR) and cancer is well accept-
ed by the sdentific cornmunity.i Although the
studies assessing the rel ario.nshi p between indoor
tanning (ie, exposure to l.NR) and
melanoma have yielded mixed resultS, t here now are
at !east 7 studies that show a elevated
risk},4 Most of the studie.:; documemed some furm
of a doseresponse relationship :l Modern tanning
From the Graduate School of Public Health" and the Department of
Marketin9,t> San Oiego State
Fundiog:None.
Conflict of interest: None.
Accepted for publication May 31, 2001.
Reprint Joni A. Mayer. PhD, Graduate SchQol of Poblk
Health-Hardy To-mr 119,San Diego State University. San otego,
CA 9218.2-4162. E-mail:
Copyri9ht 2002 by the .-..rnerican of Dermatoiogy, 1m:
-t 0 16/1/119560
doi:lO.l061/mjd. 2002.1 19500
700
bt:ds fluoreS(;ent light hulbs that emit mostly
lNA and ddiver up to 3 times rhe UVA dose
del ivered by natural s unlight.'>
1be demand for tanned skin yielded an expo-
nential growth of tanning f&dlitles in recent years. It
is estimated that there are 28 million users <.)f tanning
facilities and 50,000 tanning nationwide,
producing a billion dollar indu$try."' In San Diego
County alone, there are mr_; re than 100 tanning f<Kil-
iti<::s located within county lines. An estimated of
the US pupulation are regular users of tanning
Because of the growth of the tanning facility
industry, the Food and Drug Administration (FDA)
has established guidelines that limit amounL'> of UVR
to a person. Currently, expo:-ure
.schedule is "no more than 0.75 minimal erythemal
dose (MED) 3 :;imes the fir:;t week," gradually
inCD!asing the exposure thereafter.
7
'rhe Federal
1i:ade Commission dec.-eptive and false
.advcrtising of tanning dc-..ices, induding da!ms that
indoor tanning is safe.R Approximately one half <)f
the states have pa->scd tanning facility regulations.'-'
?(yr WH. CORH of UVemittiog sunlamp proclucts. In:
Proceedings of the for Contrci and
conference, San Diego, Call, feb 18,1999.
l AM AC.\[)
VOLUME 46. Nt!MlH.ll. s
California's Filante "1\mning Facility Act of 1988 states
that tanning must (1) give each customer a
written statement w.arning them about specitk risks
(eg, not using eye protection maycaw;e eye damage,
repeated exposure may cause skin cancer'); (2) post
warning sigM related m UVR; (3) nm claim that
using a device is safe; (4) have sufficiently
trained operators present; (S) provide each cus-
tomer with sanitized protective cyewtar and man-
date use of the e yewe-ar; (6) show e&ch customer
how to lJSC the device properly; (7) use accurate
timer during each (8) limi t each C:: \JS(Om<..'1" to
the manuf.1cturer's recommended maximum expo
sure rime; (9) obwin signed informed conse nt from
t!"dch ackn<.lwledgi ng understanding 1..>f the
warnings; ( 10) <:>htain signed parental consent for
cu..'itomcrs aged 14 to 18 years; and (11) require that
customers younger than 14 years be accompanied by
a p:uent or legal gu:1rdian.lu
!n a previous study recently pub!i::;hed In thil'
our g:oup found that 94A'X; of S4
indoor tanning f3dlities in San Diego County were
allowing a per day the first. week of tanning. a
During that study, the lnv(.'iltis;ttors informally c;:n<:o\.m-
tered promotional in<:entives that provideJ "unlimit
ed'' tanning for ll flat monthly rate. Subst:qucmly, we
the two studle$ reported in this artidc to
f<K'US spedfkally on the Issue of promoting frequent
wnnlng liessions. In study 1. we syst<::rnatk;dly moni
toned In San Diego County, California, to
r.'<-lte of "unlimited" tanning ads. To our
knowledge, this w.1s the tkst !HI.Idy w prumo-
tionalst!"".ate:gies for soliciting indoor mnning facility
msromer.s. to study 2, we conducted a replkn-
tion of our earlier fadliry {X>mpli.ant.:<:: tiLudy, II with
emphasis ( In the number of sessions alloweu by oper
ators during a customer's fir:lt week aml the rate ()f
"unlimited" Wl'lning fee packages.
METHODS
Study 1
Study 1 consihted of a (:valtmllon of
promotional tanning advertisement.-: in local ncw:->-
papers, The sample included 24 local new11pa.pers
representing a v-ariety of reado::rships in San Diego
County: The publications were selected from the var
ious gt..'ographic ref(ions of San Diego County and
consisted of <.laily city-wide, collegiate, community,
and entertainment newspapers.
The following operational definitions were used
to quantify the nf ''1lmoing
advertisement" was defined ;1s any or
reference located within a newspaper that included
the word "tanning" and referred to a service provid-
ed by the representeu in the
Kwon et al 701
mem. "Unlimited tanning advertisement" was
defined a.s any advertisement that fulfilled rhe defi-
nition above and included the following terms or
offers: unlimited tanning, no limir tanning, tanning
packages without a i>pecifled period of time to ren ..
der services, with .3 or more sessions with-
in one week, monthly UJnning or if time
rt.:riod l'endtr tanning services was not specified.
Additional chal'a.cteristics recorded for the tan
ning advertisement included date printed, source of
advertisement, type of printed media, luc.:ation of
advel'dsement (se!.:tion), dassifi<:<rtion of unlimited
t:ln.ning, and cosr of service . In addicio n, each adver-
ti:>cment Wa!i examined to see whether it was in
atx:o.rdanc:..--c with California's Filantc: Thnning Facility
Act of 1988, which prohibits the distribution of pro-
motional material claiming that of a tanning
device (tanning hed) wa .. safe or free from ri:;k.JO
'ttventy-four newspapef-s \Vere owr a 4
m{mth period during the winter/ear:ly
of 1999 2000, Ar.tai n ment pf ocwl!papers was acc:om-
plished in 3 Way:\: an:hival retrieval at l.ocal lihrnrles:
issue picked up at dropoff lind, If appli<.."a
ble, visiting to exami ne issues. When
tanning advertisements were found, they were pho
wcopied or labeled with l l rec:<>rd ldentifica
tion number. and cataloguttl <.>nto a cia record Jist.
D.ata were into the StatistkaJ for
the Social (SPSS); the issue of the newspa-
per wm; the unit of Dcl\c:..' rlptive dat::t
for all variables. Assessment.<: of the prey-.,..
h.:nce of tanning in nc:wspapern were
made by examining perct!ntage of the that
contained an advertisement. Of these advertise-
ments, the percentage promoting unlimited tanning
was computed. A r.est of betwct!n tanning
advertisement and type of
ed with a rest.
Study 2
Study 2 a cro:-.<>-ll(:!:tiona.l design consisting of
telt:phom: of tanning facility operators i n
San Diego County The $llmpk nmsisted of 60 tanning
facilities in San Diego County. A tMning .facility was
ddin(:d as any lotation, place, al\.-a, or busi
ness that pnwided persons access to any tanning
device (California Statute of 1988, Chapter 23, St.'t:tion
22702, P" .. m A)ltJ A list of tanning fltcilities in San Diegn
Collnty was created. by of a document
through P'.-1dfk Bdl Yellow and by the Int.e.rnet
through the search engines. of the Wnrld Wide Wch.
The search te.rm selened for both electronic and
paper \vas "tanning salon," and the regions
. were San Diego, San Diego County, and the
area (ode:-; of 619, B5H, and 760. Inclusion cfitcria
702 Kwon el al
Jl
35
e
30
i
25
20 " ,.
15
-
l'J
j
11)
5
:z
0
"'"-- .
. . .. ---------
,
/
<:)
Month
--+-General
Ta nning
AtJverJ$ement
, . Unllmiled
I
Tanning
Adverlisemenl
Fig 1. of tanning over 4
months.
included f:H.".lUty tha w.as in business and had at
l east one o}.leJ':.l ble tanning bed. Random selec[\on o;vas
used fnr !arming f}.).cilities that were part t}f a chain (>I
faci lity wirh the same busine.<os name) . One f:1d!ity
resenting each chai n w.1:; sdectt..U.
The principal outcome variables in study 2
wnnlng facility compUance with recommended
exposure schedule guidelines and prevalence of tan-
ning session pa(;kuges and pricing structures. Data
were coll ected in March 2000 by telephone by a 24-
year-o1d male confedcmce (H. T K) who po ' t!<.l as a
prospective customer. The confedel".ttt:! prefaced IUs
target questions by indicating he had fuir skin and
was tn vacation in Acapuh.:o in a wuple of
He then nsked the operator about (l) the
pen>onal recommendation fnr the mosr
number of times he should ran the fi rst week, (2) the
d uration per (3) the kind;; of packages
offered by the facili ty, and (4) whether the fitcilit}'
o ffered "unlimited" tanning. Fm:ili6cs wen: cnnsid
compliant if the operator':; responses were
within the FDA's recomm(."nded exposure guiddine5
on the frequency of $eS$lons.7 For the dmation of
each 5Cssion, the FDA's recommendation is stated in
terms of M.ED rather than minutes. Consequent!}', to
conduct the assessment of compliance with dura-
tion, we adopted the limit used in a recommenda
tion of the Council <.m Scienti fic Affuirs, American
,\1edic.al A.'5sod ;ltkm2; we coded ma:iCimum doratiom;
of 30 or less as compliant.
1h assess reliability, ail f:1cilities wert: interviewed a
second time by a di fferent intervit:wer, This inter
viewer was a 25-yea.r-o it.l male gmduate student. A
modified and a subset of the initial questions
were used. 1b a.sses5 further point-to-point rdiabili-
ty, the first name of the tanning P.1cility operator from
the primary and imcrvjew was recordet.l
and matched when applicable. Both studies were
J AM ACAf>
M.w J002
n:viewed by and received approval from the
Curnmittee on Protectiun of Human Subjects at San
Diego State University.
The SPSS was used for all statistical analyses.
Descriptive statisrics were computed for all variable:;.
Frequendes \Vcre catculaced for l"atcgorical va.riab!es,
Chi-square tests were used 10 test :he association
betwL>t:n compliance of tanning sessions recommend-
ctl ff:r the first Wt:!ek and gender (lf the open.ttor and
the type of facility (eg, $alon, gym). l-'er(;ent agree
and the Kstatistk:al were used to assess the
inrerrater rellahility b.:.."twet:n the two interviewers.
RESULTS
Stud)' 1
Sample cbatactcristics and pt:cvalcnce of
advertisements. A total of 584 newspaper i11sues
out of. 606 eligible issues was examined over a 4-
month period. 'lwenty-two issues were nOt
eithcr be('ause the was missing or it
was not The sample 14 com
munity pape.n; (Hl9 issues, 32'X> of all issues}, 4 col-
lto:giate (84 issues, 14%), 4 enter r.ainmeniJ'spedal
Interest (6fi 12<..), 2 major daily ncw . .,pa-
pers (243 issues, 42%).
Seventy-thn:t: ranninR found
recorded. on the O(XnHional de.finition of.
an unlimited tanning advertisement, 55 mnning
advertisements (75.3%) labeled as offering
unlimited tanning packages. I n addi.tion, 7 mnning
(9.6%) were found to promote safe
canning devices, which is a violati<1n of the Otlifornla
Filllnte limning Pllciilty Act <)f 1988 and Tr-.tde
Ct>mmh;:;lon
Price data. Promotional pr!ce:; loe;tt:::d !n rhe
advertisement wert: ret:ordeJ if the tanning advert ise-
had a monthly-unl imited package price or
a:nnomic incen!ive. For prmnwiunal pr ices in adver-
tisements wi th more than l month of tanning at a spe-
cific price, a monthly :I\'era).:le cost was The
average cnst of a.n unlimited monthly tanning p;u:kage
was (st;tn<l3rd deviation [SO]. $3.21). Forty-
\lOt:! tanning were linked to a
facility chain. Of those chaina, 31 advertisements rep-
resented a chain of 4 fJ.cilities and lO advertisements
represented a chain of 5 ' Jr facili ties, ;til within
the San Di(!!W metrnpolit ar. As shown in Fig l. a
:>eaSt>nal pattern of a numbcr of advertisements dis-
played w-..s found. More tanning advcrtbements (gen
era! and un!inured) were prevalent toward the end of
the +month
Associations between newspaper type and
advet'tisement prevalence. Table [ pre;st:nt:; the
propt !rtkms of by type, that contained a[
om: tanni ng advenhement and at kas1: one
l AM ACAD DEitMATOl.
46. NuMtltt:. 5
Ku>on et al 70;)
'Table I. A:s:sodation between tanning advertisements and t ype of newspaper
Major Entef'Wnment
Adven.ls.ernents No.(%} No.('!)
Had tanning ad o<-r 18 (26.5%)'
Had unlimited tanning ad ow 18
*'SignifK:<mtly different from other types, but not from ach other.
tSignificantly different from ccllegiate types.
Colleglak Cmrunu.nlty
No.(%) No.(%) Y/ (dj) Pvalue
16 ( 19.0%} 1 (0.5%)* 101.53 (3) <.()01
14 (16.7%) 1 (0.5%)* 98.26 (3) <.001
Table II. Percentage agreement between observers and x statistics
llelll
Sex
Frequency/week
Duration/session
Have unl imited tanning
uperaior (u"' l 5)
100.0
60.o
53.4.
too.ot
77.3
42.2*
58.5
l OO.Ot
.335
.131
The following <:ut offs for Interpreting reliabilit:t from the kappas wl!re 1.1sed;O to 0.4"" to 0,75 = good, 0.75to I = excellent.
*K could not he computed because rrr.Y valves did oot equal column values io a lable.
1.: could no1 be corn because I he number of nonempty rows and columns equaled 1.
wnning advertisement, as well as the
results of the analysis. As nored, type of
newspaper wa.s significantly associated with both the
presence nf any tanning ad and the presence of an
unJimlr.ed ad. Post hoc multiple indicat-
ed that majnr and community typc.s of nt:wspapers
had significantly smaller proportions of tanning
than rhc <>ther types of ncW:iP'dpers
(collegiale and entertainment), but wen: not different
from each Entertainment had sig-
nificantl y larger proportions of tanning at.lvt:rtis<:-
than collegiate newspapers. Multitude wmpar-
lsons for unlimited tanning yieltled (Y.trJ.Iid findings.
Study 2
Sample characteristics. A catal of 60 telephone
inte rviews was condw.:tcd. from an initial of
90 tanning facilities, 30 facilities did not meet the
inclusion criteria, including no longer having opera-
ble tanning beds or being out of The tan-
ning facility sampie consisted of 51 wnning salons
5 g}'fn/fttne:ss <:enters (8.3%), and 4- hair;heau-
ty salons (6.7'%.). Re$pOndents included 17 male and
<)3 female taO ning facility OJ:Jel"'dtors. Tile ;IYerage
pletion time of the interview was 3.23 min-
utel' (SD, 0.96; range, 26 minutes).
lnterobsener reliability. Percent agreement
between observers and lC srarjstic values for inter-
views wich the same or different oper.mor hy both
inten-icwers were rakulated. Fifteen llf the fadliry
operators (25%) were intervi!.::'.ved by both interview
Table 01. Summary of tanning f acility to
inte-rview questions
N'o, tanntog
llem n:$JK)nSt lacl.Utits %
Frequency dvring first week
Everyday 37 61.7
Every other <Jay 17 28.3
Three or less 4 6.7
Unable to determine" 2 3.3
Duration per session
3-S min 2 3.3
6 10 min 44 7B
1115 min 6 10
16-20 min 5 8.3
Unable to determine" 3 5
HaYe unlimited tanning
Yes 60 100
Came in as much as I want
Yes 43 71.7
Only once p'r day 17 183
Rf!$pondents t hat they needed to see the <:ustomer before
gMng an answe(.
ers, These are shc1wn in Table II. K Values for') of
variables <:buld not he computed. With the raw
percentage data, agreement ranged from
42.2% to 100%, with generally higher agreement
iound for observatir ms of ;he same opt:rator.
Compliance and other outcomes. Table 1li
presents rhe disnihutinn of responses to the con fed
704 Kwmt et al
erate's key questions. Only 4 of S8 respons-
es (6.8%) w the
mendation were classifled as compliant 3 times
per week). In contrast, of the S 7 opemtors who
spedfk number tJf minutes for the duration rec-
ommendation, :.11 respo.ndr:d with a duration of less
than 30 minute5 and were considered compliant.
Tests of association were performed to a.,<;sess rela-
tionships between compliance with n:commenda-
rions and !',render of opt:mtnr and facility type (r:g,
salon, gym). No statistically significant chi-square
ues were found between any of the compliance our-
and either operator gender or fadlity type.
All 60 f".tciHties (100%) reported offering unlimited
tanning packages. Fifty- four facili ties relt:a:;ed
monthly-unllmit.ed tanning package price!i over the
phone. The averag-e collt per month of an unlimited
tanning wa.'l $38.50 (SD, $8.10). The mngl!
of pdces was from $l5 IXl $55. Duri ng the
second (reliabili t y) inter:view, 59 o f 60
released tanning se::;:;inn
not assessed during the primary interview. Th(: aver
age cost of a single tanning was $6.48 (SD,
The prk:es 111f18t:cl from $4 w UO per
DISCUSSION
A key convergent finding from these two studies
was the frequent use by indo<)r t:tnnlng facilities of
"unli mited'' tanning packages as a promotional :mat
egy. Three fourths of the print ad'i used this s trategy,
and all of the f'.adlitks in nor sample oifen::d it as a
payment option. Compatible wlth pt"'a<.:tice, che
majority of facility operators indicated they would
allow a fairskinn.ed confederate to tan at high fre
(that exceed th FDA::; rt:..:omrnen<.led
guidelines). Although our daw on wnning duration
more encouragi ng, ;allowing .5udt frt:q\lent
neverthelesli rnay result in consumers' overex
posure 10 UVR.
Not surprisingly, because 2000 :sample of lot"All
()v(!rlapped with the s ample in our 1998
study,ll the patterns of compliance were cornpara
bk:, with low compliance with the frequenq ref...'\Jm
mendation and high cpmpliance with the
limit Other studie& havt: reported low c;;ompli
ance with the frequency guideHne:l.u.u
'Jb our knowkdge, ours are t.he <:mly :)tudieg to
date that have Sj':)tematimlly pricing strate
gies. The average package price quoted in ads
(study I) lower than the average price given by
facility in the study 2 imcrview""!i. This rnay
have to a greater ten<ien<.y of iower priced
facilities (relative to higher prked fadlitit::>) tO adver
tise and/or to the occurr:::ncc of onetimc-only pro-
motional quqted in the ads. Uhing the me-.m
I AM ACAO DtRMATOL
MAY 2002
monthly unlimited tanning package prkc based on
our intcrvk.'\v we e..'ltim:ue chat a consumer tan
ning daily over a 30-<.lay period would pay appwxi
m:Hdy $l.2R In contl'll5t, the single iiC.S
sion price was $6AH. (The monthly rates of these
strategies are BH. SO and $194.40, respectively.)
We do not have direct evidence that the package
prk:ing scr.ttc<gy rromote:1 greater session
(and (:umulative exposure) than ttl(: individual scs
:>ion strare;,:-y. Huwo:;:ver, it is likdy that rhc
Stl"<ltcgy attmcti! a lurg:er number of first-time users,
given that it prnvitlc:; an RO% discount. This lHscount
ho:: partiCularly :lttmctive to adnlescc:;:nts, who may
have le:;s tn<mt..-y, place a high value on bei ng
tanned,14 anct may be at w:t:ater ril\k ((;r skin cancer
than adults beomse of cumulative t NR expm;ure.l'>-17
)h ung age (16-24 yearn) predkretl use among
New York state residentslll and a survey of adoles-
cents in St. Paul showed rates ,)f indoor tanning,
parcir.;ulady gil'l!t. t!>
H<lth had methodologk Study
1 would have :>tt-engthened by samplinp, news-
papers 1.2n1<1.lith period <tnd by obtaining rcli
estimate:s. fn s tudy 2, resrom.l ents n:portc:d
their practices for a fu ture visi t; these data not
co11"e.late with t he practices durin!{ an 3xtual In
additi<m, the lntcrconft.'<.il;!f"J.te agreement estimates
were relatively low for ()[ the variables. The
la<.:k of toncordam:e may be explained, in part, by
imervk.wing di fferent operator:; at most of t he fadli
tic:;. [ t may also reflect a lack of in what
one opet".ator says to different dients. all
Indoor in Di ego County may
not listt:d in the Yt::llow .Pages or Internet
bl!auty salon:> and
indoor tanning as ttn an<.: illary
not bave l1<1d :1 listing under "tanning
Thul\ the .search may have omltted
some tanning businesses. ln future studies, sopp!e
rnental such .American Bu:;iness Di!'<.:
and Dun & Bmdslreet .Marketing Service, :>hould he
used to idt::ntify potential sites.
in nur earlier anidc,u to impwve con
safety we re<:nmmend mandatory operator
training and enfm"Ccment (lf existing reg-
Be(:ausc the session frequency uiterlon is
only a feder.tl, state, and lm:al pol
ky-makel'$ !ihould cml:>ider changing it to a regula-
tion. (The FDA currently is considering revisions to
sunlamp pcodm:t performance standards 20) Finally,
additional exploration is warranted of the "unlirnit
ed" tanning prom1)tiUn<t! strategies. Rt:searchers
need syst.emaric<llly evaluate the specific impal:ts
these strategies have on facility use, pa.nkularly
among adolescents. In (he meantime, given the
J AC:!\0 DER.v.ATOl
VmuME 46. NUMSER 5
widespread use of these strategies, health
should develop int<."'-vent:ions at
(and their parents), informing them alr.Jut exposure
guidelines At; one iotervemi on component, -;elect
communications could be placed in the .same media
that print indoor canning advertisement;;.
REF.RRENCF..S
1. American Cancer Canc.er filers and 2000.
Attanta: American Cancer Siety; 2000.
2. Countil on Affairs. Harmful etrecu ofultrnvioll!t ratJia
don. JM,.'IJ\ 1989;262-38{1-4.
3. Swerdlow fiJ, We!nsro<k MA. Do tanmng lam1>5
melanoma1 An epidemiologic assessment.) Am Acad (iecm(l1ol
1998;38:8998.
4. Westerdahf J, tngvar C. M<\sbatk. A. )On$.SOn N, Olsson H. Risk of
malignant melanoma in to u.se of s11nbeds:
funher for UV-A carcinogenicity. 8r J Cancer 2000;
52:1593-9.
5, Dilfey Bl. Use of IN-A sunbeds for cosmetic tlnnlng,. Br J
De.rmatol 1986;1 15:67-76.
6. Deleo VA. Tanrung salons. tn: Arnencan Academy of
De.rmatofogy, l!ditors. Proceedings of natiOnal conference on
environmentel ro t he skin, October 1992.Schaumburo
{IL): American Ac;ademy ofDermarology; l994.p. 37-41.
7. US Department of Health and tium.:m Servica Owlity control
guide for sunl11mp products. (\10): Public Health
SeNit:e; 1988..0HHS Publlcarion No. >OA 88-8234.
8 Federal Trade Commission. ff\door tanning (factsheet}; 1997
[onlme]. Available at; l'trtp;//www.ftc.gov/b<p/(oolme/
pubslhcaltn/indootan.tttm. Accessed January 15, zooo.
9. American Academy of Dermatology. Amerlti!n Acacremy of
Dermatology summary of unning parlor legislation;
Schaumbvrg American Academy or Dermatology; 1 995.
Kwon eJ al 705
10. California Department of Health Services, Department of
F"tlante Tanning Fac!l!ty Act of 1988.
and ProfessiansCodl!;ChiJPter .23-2.2700081998.
ll. Cultey CA,Mayer JA. l, Busic AJ, lF,Sallls JF,
et at. Compliance with redetal and state legislation by indoor
tanning f.tcilities in San D.iego.J Am Acad Of:rmatol 200 1 ;44:53
60.
12. Sruyneel-ftapp F, Dorsey SB.GtJin JO. The tanning salon: an are.t
survey of equipment, procedures, 3nd J Am Acad
Deunalnl 1 988;18:1 030-8.
13. f aifchi!d A, Gemsoo D. safety information provided to cus
to.'T!ers or New Yorlc City sontanmng salons. Am J Prev Med
19948;381-3.
14. Me.rmelsrein IU, Riesenberg LA. Changing knowledge and att
tudeSc aboot skin Goancer risk factors in adolescents. Health
Ps<;chol1992;11:371-6.
1.5. R. An overview of skin cancers: incidence and causation.
Cancer Suppi1995;7S:607-12.
16. Marks It cancer-childhood protection affords lifl!!time
protection. 'Aed J Aust 1997;147:475-6.
17. WemstOc:k MA. Coldrtt GJ., WC., Stampler MJ, Bronstein
811. Mihm N'C.et aJ.Nonfamilial cvtllneous melanoma lnc!dente
in women aswc!ated with run before 10 yeats of age.
Pedllltrtcs 1989:t!4: 199-204.
18. UI!Qulsl PP. Baptlsfe MS, Witzlgm;m MA. Nasca PC. A popula
tloobaS\!d survey of sun lamp and tanning parlor use in New
York State. 1990.J Am Ac:a.d O!rmatol 1994;31:510-2.
19. Oliphant JA. Forstf.'f JL. Mc.Bride CM. The use of commerdal ran
fling by suburban Minnesota adolc.-scents. -'m J Public
Health 1994;84:476-8.
20. Department of Health .Jnd Human Services, Food and Drug
Admu'liSirtlt iOn. Medical devices; sunilmp produ<: ts perform
standard; requests for comment' and In I ormation, pro
posed n1fe (21 CFR 1020).Fed Reg l999;64:628S--!IO.
190
Original Article
Indoor Tanning Use Among
Adolescents In the US, 1998 to 2004
Vilma Cokk:nides, PhD
1
, Martin Weinstock, HD, PhD
2
;;,
4
5
, DeAnn L.azov:ch. PhD
5
, El:zaoeth Ward PnDl.
and M<chae! Thur'l, tV: D, :V1S
1
Artificial (indoor) tanning can be a common source of ulttaviob radi<Hion (UVR). of" the
skin r.o UVR in tanning boodLS has several adverse health consequences. including skin and eye bmns,
alt..:rations of immune sysre.m function, photoaging, photo--induced m-edication and increased
risk d skin
1
Recently, a large oonduded th<lt firsr to sunbeds before 35
years of age wa.:s significantly associated with an increased risk of melanoma, b,tsed on 7 infornMrive smdie'i
(summary relative risk, 1.75; 95% conHdence interval [95% CI], 1.35-2.26)?
<:orrupond!ng a11thor; Y1:na !'hO, Clep<>rtrnettt of Epidemio:Q9y 3l>d F!es.earch. Am"r.can SoCJct'y. 250 Wi:hen;
Strt'et, NW, Atlanta, GA 3u30J lC>02: f ax: \404) 317-6<!50; vcol:!Cr.l@car.c;;;.Of9
of an;j Research, An'.erican Society, (*.nrgia: : fJerr't'atc!:pidem:ebgy Uni:. Pr.wider.c.<' Vr'!("
1\hvde Gf Drr..atolvgy, StvWn Pcv:vrm<:e. Rhode l;:otnd; ct
(<NF>hoorty ;<edt1. Bmwn llniff'iity, Providr.ce, Rhode l;ta,'l C3r:cer Skin !lcivm><y Car.c;:r S\n::ety
Georgi3;
6
Divis ()( and Communit")l H<>..a:m. ()( Minnesoto, Minneapclis, Mtnnesota
'This is a U S. won< and, ;.s is i'> the i>'Jblk. C<:r..ain in th$ United of
Mq 21, 2CU8, Relllsed: Aug<ru 2008; Acc:epted: Auyu>. 6, 2008
on!inlil; l O. 2CdlS, 2008 by Am<>Fican Cor-<:<?< Society"
001: 10.
Cancer Jan:...ary 1, 2009
Previous .smdks condncr(:d in adoli':St:enrs haw shown
that the of indoor mr.:min.g :.L-.e by sex.
(ranging fmm 2(1(; to 1 i (y(j in boys and from 12% to 37%
in girls}; rhis bdli:vior is more pre.--a.lenr. .in older ado!o-
girls, in wlm tan or have
positive coward <l r<l.n, <l.nd in those less likdy ro
ase Sorne hav-e found thar social
int1uences. such ;:tS ha:ving &knds or who usc
.tnd<>o.r tanning or having paremal permissiorr m use
indoor tanning, are corrd atx:d ;"<ith i ndoor tanning use hy
Because of r.he. known he.ahh risks associ-
;ucd wirh indocr tam;ing, rnany hc:alrh-rdatcd orga.aha-
rions re<:ommend Hmiring rni no;s' to indoor
tanning rhrough regulatiun.
!n the US, .seme f:. tates have passed to
.!imir minors' to indoor ranning. Stamrory require
ments vary by state. Nearly all stares permit minors' access
wirh p;;rema] consem ;mel/or <Kcomp2nimenr., and only .a
few t.)n rnimm agt.
9
"
11
Stud.ie.t-: sul!-
'
gesr rh;;t compliance with minors' restrictions >aries
by l
4
In l smdy in which compli.ance ..,..,.irb laws
to aged < J 5 yeats was
by tdephone, rhe of esmblishmenrs adhering
to the st;ate 's r<i:qt:iremenr ll <y;;, in Texas, 77% in Wis-
consin. and 80()/o in No prkw srudy has
wh::rhe-r indoor tanning use among differs in
states with youth access h:gislat lot1 versus S"<2tes with no
such ;;I ale laws.
Our objective to ;malyt); data fwm 2 llatioo:.tl
surveys and 20t).4, respectively)
thar collected informs.tion r::{!ardim! t he recent us-e of
.... , .;.;
indoor in l l tu 18 years. In the
cur.rem study, we assessed. change in p ast-year illie of
indoo! mnning among berween 1998 and
20G4; in addition, we e.-<amined whr:rht>r legisbtion
r::s!rktlng to indoor tanning is aswdat<:d
wirh youths' use of indoor cmni ng after comro!Hng for
signitkanr. corrdates and assessed shorr-rerm adYene
from rec:m.t use ofindoor ranning (eg, burns).
MATERIALS AND METHODS
ln 1998, and. again in 200':i, American Cmcer Soci-
(;'t'j conduct(;'d 2 nation2.l, cross-sec-
r.ion;d r.dtphone survey;:; of hdl;lviors reb red ro skin
CaJJ<:tr risk among yomhs ages l I w 18 r-ear$ :md their
Cancer
Indoor Tanning by US Adolescents/ Cokkin!des et al
primary careg,vers i n the lJS. 'J'h(: surveys
were conducr::d h om .August ro of re
spective years. The smveys consisted of a youth inter-
view (requi ri ng permission and conscm hom a parem
or caregiver} and a t1<:a.r!y identkal that
a*ed questions n-gwding sol<l.r <lnd :wnmlr {'Xp<.mm::
and sun protection beh:tvi<. 1rs, 'lh: 1998 survey had a
sample of 1 l96 youth-caregiver pairs; rhe 2004
quent survey had a sa.mpk of 1613 such pair8, Both sur-
vey-s used a similar telephone-based sampling
meiliod.ology (dual lisr-asiiisted. random digi: dialing
methodology}, Hdd opt>rarions <md monitmlng
t)f interviewers), and data Ct)lkcr.ion surv<.ys. :\c.cord;ng
to srandard fonnclas to estim.ate of
bsd survcy5, the rate )iB'i; iu
1998 .-.nd 44% in 2004. Despite lower r:ue.s,
there were no significant demographic notted
among sampltd addescem;:; hy r.ime periods. rn :t prior
published srudy of trer<d:; in $Un and mn pro-
tection
15
we (esred for any Jifter-
ences i.n rhe de::wgraphic pmflle of yomhs between The
2 survey.} and determineJ tht samples mmpa<
rable. The mrvcycd were mosdy whixc
(77%). with a meau age of 14 years and a sex ratio of
;.. : ,. l 15 t '\ ) 1' ..'>.,_ j t <; H'fl: )If>'
r1-ar.y . . H.lo, la . m.crn.atKn . 1 ..
methodology a.nd sratisti.cal comparahiliry d' .2 sam.
pies can be. d sewhert!.
15
Both surH:Ts Jsked iden-
rical reg:trding the use of indoor r;mning
bot)tUS :>r sunlamps, f1equency within the past
demographics, susceptibdity to tJV expo$ure,
and attitudes w ward tanning. 'l'he :W()4 sur>t'}' also
asked burns or skiu fn)m indoor
Iannin.g me,
Measures
Use of Indoor Tanning and Adverse
Reactions From l ndoor Tannfng
w::r:: a$ked in the p;lsr y:;;u
had used :m indoor tanning hoorh <.:r s1mh11:r.<p <Wd rht:
Ilumber of t irut s {fre-.ju\:ncy of use) during rhe past year,
Th:e 2004 survey asked hums
from indoor r.arming Cg<>r red <>r lmmed at any rime in
past when. you ranning booth or a wnlamp") 'lnd
another question concerning sk.in infecrion or rash ("ever
gor au infcaion or ll:om kt mrming booth").
191
Oricinal .Article
Demographics and Skin Type
Ead1 survey age, se.x, and race, and
4 que-stions rdating tG skir1 characterisrics (ie,
:-endt:.tt(.:y of tht skin w bam, ability to t-an, nauLral skin
color, <tnd hair color) . .From t hese, we derived a composite
efsun sensitivity based on ;1 validatd measure.
Attitudinal Correlates and Social Factors
Tanning attiwdes were using 2 items ("I ted
heahhy whtn I have a nice mn ,, ami "I look better l
have <t t;tn") an;;.hored on <t ) -point I...ikert formac from
mongly ro mongJy (Cronbach ':t af .69). In
the .2004 survt)', a attitmhna.l irem was added ("even
though it may 11ot good fin l sriH like to get a ran"'),
wirh a Liken f{mnar. 'rhi.s was combined with rhc
ocher 2 attiwdina! items ro a composite
mdinal factor (Cronhach .77) a;<d ;1sed in t he mub-
variate logistic to :assess of indoor
r.anning use. In addirior1, in the 2004 :mrve<;, we
par::nt:<-1! p::rmission hy asking yuuths abom their 1evel of
agn!ement with the following .statement: "My parents/
guardian woutd allow me m l.L<J:: indoor sunbmps or
bo(1tb." t'Yidence suggest$ rhat this panicuiar facr(lr
is a srrong ofyomh indoor tanning u,';(!_
7
x'
Sunscreen Use
The fttquency of ming in rhe mos; recem
sunnner <l;;sesstd by asking 'IH)W often was
applied when going omside during the and.
"how often was sunscree.rJ. w.i.d::. SPF (skin protection fac--
tot} 15+ used when at the heach or at the pool?''
m Ihese (jUcsiions were provided on a 5- poi n!:
S(ak nmging fwm always to ntv.::r.
Parental Factors
Similar from the parerdcaregiver $U<'-'e"f
were t{) cz)llec.r inform<ltion regardi ng their ,,f
lndoor tanning b1.1otb or sunlamp$ in d1e pasr well
as thtir status.
Legislation Restricting Minors' Access
to Indoor Tanning
We reviewed policy-based reg:udjng if and
when states had passed r;;gulatinns restricting minors'
a!xess w indoor ra.nning. tn, l?i This iJlfo.rmariou w.as linked
rhe stare uf and. to derive
192
Table 1, of With Le-9is!at!or-: on t<linors'
Access Restrictions to Indoor Tannin9
Policy Dates State, Date of Statute
Ca!ifotnia, 1997
Goorgia.
Louisiana, 1992
Maine. 1995
t ...
Mif1rl<!S(>Ia, 1995
Misr;is;,ipp!, 1flSfl
florida. 1998
Uiir!()i$, 2001
!n<:iiana, Hi99
North Caroiina. 2001
Ohio,
Oregon, 2000
H!1od?. ISiand, 1998
Sout11 Cam :ina, 2C'(} 1
T;e:-es, 2001
Wisconsh 1999
Pilii<-:y ra;:lC!'1S i.lSOd i: to stati! :.;gistatir.f1: McLa'JfJh!in et <.>Jl" and
l'l'anc'.s et
;1 srate-polk.r indicator w be f()t' carego-
rie; of rfus sm::e-pd.icy i.ndkat<:>r variahk were developed
using a coding of su te.level dnr took into accotwr
whe;:; legislation was impltmemcd and Iht possibili;y of
repeal by
Henct', 5tatt' were
illw 3 levds: 1) sr.a.!:es 1har pa.ssed !t::gisLnion bef(m: 1998
and. retai ned the policy through 2004 (8 stare$}; 2)
that passed l:!g!slacion betNtt:n J 998 and 2004 ( ll stares);
and 3) .srares rhat had no legislarion on r.h.is i.ssue duri.ng
the 1998 to 2QfJ4 pe.dod oflmetest. (See Table 1 h1r addi-
rional informaricm regarding hsting of sr<nes ili<H had laws
passed during tbe smdy period.)
Statistical Analysis
For bow surveys. sampling wdghrs wok inw aaoum
unequal of sdecr.ion bemuse ()f sa.m.p.ling
design, nmuespmu;e, and poststtadfkation. Data manage-
ment w:u cond ucred using Sz\S si:nistic:t! (ver-
$tOO 9,1 ; SAS fnsritut:: Jnc, Cary, NC). ;<; All descriptive
and. were conduced using SUDAAN
sofrwarc 9.(); R::search 'l'riangJ.e 1mti-
.,<'
C'J.re, Research P;uk, NC):' Th)s sd"tware
into acco um rhe compk'X survey sampling design ami
sampling weights to derive approprbte st.andard errors
used for sradsticrl and. derivation of 95% Cis for
the weighted a..lillysi$.
Cancer
Assessment of Change in indoor
Tanning Use
'wtight;,ed to desc ribe. the prevalence
estimates of indoor ranni ng artd of rimes ,,f
lndoor ranning wirhin rhe pasr year (b..::cause of rhe
skc.wd distdhutkHt of rh.: hure.r variable. the median
rarher rhan rhc mean was used). To c.xami.11.e
l ')98 and 2004. we the 1,.vnesponding
weighr.ed (of p::1sr-ye::1r u:se of indoor rcmnillg
and rn.tdim mm::ber of rime<s indoor tanning was
within the past yeat) and 95% Cls around hese
dilfcrcnces. By using g::.nt"ral Hnear comrasrs, we resEed
the smtbtic;ll of trends.
Predictors of Indoor Tanning Use
Among Adolescents
A d' predktor variable>, which i.,"lciuded age-, sex, skin
sun sensitivity, attitudes mward. having a t2tl. and parent2l
E:e<ors, was sdccu::d based. on previolli research-'H; rbc key
predkwr of st;He policy on minor'$ to
indoor t.:mning. By (unadjusr.ed)
analysis, \Ve examined. r.he unadjusred corrc:lation between
these ptedlct()tS ;Hld indoor tanning use within the past
ye.:;.r. Frmr.. rhese all factors 8ignificam a< P= .OS
were for the weightt>d multiv;;.dare bgLstk
regression rhar examined the ind.::pendenr. a;;soa:uion
wtti.e minors' a;;x;ess and youth indoor
ranning use . .Multivariate logistk regte11sion moddi ngwa.<;
used to rest hn di.Here.n,:es in the. l.ikdi..b.ood of adolescems'
lndm)!. onning in states \vith policies tdadve to states
widwttt such policies after cornrolling t.:.Jr imporrat<t rova-
riates (set described measme.s'i.
Predictors of Sums From Indoor Tanning
Using data fro.m tbe 2004 survey, we estirnated the pl<:Ya-
.lencc of burns <md skin msh from ind onr tanning in ::Jdo-
b.cent us.:rs of sunlamps or tanning bo(lths within the
p:m yt:;lr. Weighr.ed biv<lriaJe <Ul alysis were conducted rc
a;;scss .individual dHma.cteristio; (age, se;-s:, skin sun se.rurriv-
ity) with sdf-r.:poned adverse dfe;;ts from
.tnd<>o.r :uu:.ing. individual fa:.-tors \vere used as con-
trol in t:\e ind;;penclenr relation
becweer.J experier.Jce of hurns from i ndoor r::mn.ing aud
fn:quency of Wit Hmong youths reporting U$ of indoor
Cancer
Indoor Tanning by US Adolescents/ Cokkin!des et al
c-anning wichin rhe pasr. yt:ar. a small number 1)f
skin rashes were reported, W<." were w corHhJ..:t
of this cham,:tedstk.
RESULTS
Trends in Indoor Tanning
Nationally, the prevalence of indoor tanning use among
adolescents chang{d trom 1998 m 2004 (a l (!-iJ
increase; 95% CL --1.5'K-3.5'Yo} {'L1bk 2i. i\Jdwugh not
statistically signifkanc, in the of pasr.-
year use of imbor m;ming were observed ;lmong: gir.f.s
(from i 5.6% to 17.7%), youths 14m 1.5 (ftotn
7.1% m 1 d:wse wir.h .m.tdimn sun se.ns.irivi.y {from
J 0% tn l3.5'Ytl), and with po;;itiv:: attln:dinalptder<
ences for a tan (fro.m !8.8()/o w 250(;). i\ sig.nificam
increase was noted in dioSe who report<:>d applying
Sllil!iCteen often ot always while l)tltdoors on Sllnny days
{3.7% P , . 02}, ahhongh rhi8 group had a.1ower
pre.vaiena: of ind<.K.n tanning ln contrast, among
youth.s whose pa.rems used .indoor Lllming, rhere was a
slight d::cre-J.se in ofindo:>r t<uwing J.998 and
2004 (fmm 29.5% w 27.2%). W.;; f1mnd ''
declining rr.:nd in the prevalence of .tndom r.anning
over the time pef'icd (1 99R-2004) in with legisLuion
u:...ar resrriaed ac:ct"s..: : o indoor ra11r.ing hy .min<>rs com-
par-.ed with those without such legishrion.
Berween 1998 aa d .2004, 1he mtmber of
times i...'1dom: rau.ning was us;;:d d.uri.ng the past
stable 2). predictive tlfindoot tan-
rung use rimes wi rbin rhe pas1 year included older
adolesce.na; female sex, medium sun u:d
posirive arti mdes roward Ianning.
Predictors of Indoor Tanning
Mulrivariare a.ru1.lysis .\demii1ed 5 f.acmrs significandy
associared with indoor tanning;.;$;; (Tabk :>): ()id;;r (in
age<; 1 6-18 adjus1ed prevalence: odds r<trio
[iPOR] of 4.26 [95% CI, 1.91-9.47\), em:!.le st'X (<iPOR
of I 0.60; 95% CJ, 5.74-19.59}, <tttin;.des wwJtd
a t:m (al'OR of 8.65; 95% Cl, 3.49-2!. AOJ, having a par-
entiguardian who used indoor rann.ing w.irbb the
ous year (aPOR of 4.. 18; l))<>:f: CI, 1.20-7 .90), and
parental permission to use indoor tanning :;.s by
193
Oricinal .Article
Tabi!i' 2. C! !1d Ch<Jnge ir Past Year of indoor Tanr:ing ir Yout hs BetweeJ' 1998 and 2004 and Amor:g
Year Ur;ers: t-1cHan Chang in th<: Frequ.:ncy of Use of indoor Tannlng Between 1998 and 2004
indoor Tanning Use Within
the Past Year, Prevalence
19S8 2004 Change,
% {95% Cl)
No. % No. %
Frequency of Use
Among Users
1998 2004 Change,
(n= 123}, {n:::::: 204), % (95% Cl)
median median
! 19 !0.1 1589 11.1 i.O ( .. 1.5-3 5) 6.4 6.0 0.4 (40 3.3}
$0)(
Mala
Famale
Ag&, y
1113
14-15
Hl1S
Race
White
Nonwhite
Skin sun
Low
Medium
H;gn
Attitudes toward a tan
H;gn
Meolum
Low
Ll!;;ed sunscreen on stmny days
Always or often
Sometimes
Rarely or
Used sunscrefi'n with SPF 15+ at fili)ach/poot
Always or often
Sometimes
Rarely or never
Parent/guardian used indoor tanning in thi! past yi!ar
Yes
No
State has legislation restrictin9 youth iru:loor tanning
Policl!lst pres(m! 1 997
Policies after 1997 {up to 2004}
No throughout 1998 2004
002
594
506
289
400
-;o;s
!00
318
591
287
196
425
4M
3S1
45C
583
224
178
!03
247
.j
::
538
!)5% C! iodic<%>s !)$',, SPf svn p.-ctecti().-. fac:tcv..
4.8 808 4.a
15.6 ?81 i?.?
3.8 533 2.7
''
-t37 10.5
600 1B.7
-;-; _Q 1372 12.8
?.G 207 5.1
11.8 417 ii.O
1QQ 1'8 13.5
8.3 400 a a
213 25.0
;{)] 630 14.3
S.8 729 SA
.() 668 9.?
12.6 51$ 11.2
1J3 404 12.6
7.0 95i 8.4
-;-;_g
338 15.2
288 14.2
29.5 i88 27.2
8..S 1401 9.0
8.4 311 S.O
5?0 10.0
'1()8
12.9
o.o (--?.6-2.6} 3.7 4! 0.4 ( 3.?4. 1)
2.1 (-2.1-63) .9 8.5 1.6
I
11
'
- (-3.9- 1.'7} 2.6 4.1 1 .5
I
\
18-48)
3,4 (--OFi' .6} 7.1 4 0 <S.1 ( H),0-3.7}
0.3 .. 5.6} ?.a 8.0
.
i
I
..J.35.5}
1.8 (- '!.i -4.6} 7.9 6.1 1.8 (
.1:
-'L9 2.1 53 ( 6.4-12.7}
-O.S 6.1 1U 5.2 ' \
3.0-13,4)
3.5 {- 0.3 7.3) 9() 5.1 3.9
I
'
8.71 0)
-1.7 (--6.3-2.9) 3.3 4 0 0,7
\
3
6.2 (--2.4-i 4,6l fl.S 'JJ 1.2 '
5.5-7.9}
'
3.6 {- i.0-8. 1}
6 ,,
5.6 0.9 ( 6.5---4.-r:
-' .4 (--4.5-1.7} 43
.....
LO ( 4.2-2.2}
3.7 (0.2?.1)] 7.0 49 ;:,, 1 ( 5,7133)
S.O a- 3.7
I
24-98) . I
'
.o (--3.55. 7} 6.3 6.4 0. ( 7.4-7.f>)
(-- ,54.:?) 5.6 5,7 0.
'
S.3 {-J.Q .. "A &.0 0.2
I
'
6 6-63}
84 2.6 (
" 8--6 8}
-2,3 (--13,0-9.3} e.e 9 0 2.4 ( 6.6
'
0.5 (-2.0-3.0) .4 5.4 LO
I
'
46-22)
-0.4 {-5.1 .. t.3) 6 .8 3.0 3.8
I
\
8.91 A)
- 2,5 (--6,02.0) 5.4 8,7 .3.S
'
0,7--7,3)
S.S ?.a &.0 2.8
I
'
... ;
.51 8}
- se,!sit!vity index tassd on at:iilly l c i:<m, tu b!.:rii, ar.<C natural and color skin.
1F <.05 .
. t. Eight stiltes had !eg!st<ltkm restrictirg m!t:C$' m:= to larrir;-g 1997 a,-,.:;1 tt;rvugh 2004.
-Eleven had not passed iegis!<Jticr. after 1997 and ;?C.c.t.
st.?.tes '"ith r.o $t!Ch legislation p,assed ill both i99S a1'id
the adobcent (aPOR 15.42; CI,
Srat{: bgisbtiot1 access ro indoor tanning was
not f(1tl!1d to be signi tl c,lndy assnd atd with indoor
niug use in ehher or adjused analyses {aPOR
of0.77; 950tf> Cl, 0.49- l.ll).
194
Adverse Effects From Indoor Tanning Use
1\mong 204 adolescems wih) used indoor t;tnning homhs/
surrla.n1ps wirhi11. the paH y{"ar, rhe sdfn:pmted oo:;ur-
ten:::e ofburns from indoor tanning was 57.5(Yo Crable 4).
Tb.e occurrence of bums from indoor ra.r.ming w:L;; f.{mnd
Cancer
Indoor Tanning by US Adolescents/ Cokkin!des et al
Tabi!i' 3, Predictors cf Youth lr,door Tanning (Booths/StH'liarnps) Use iii the Past
Age, y
11-13
14-15
1618
Sex
Female
Male
Skin sun sensitivity indexj
Low (bottcm lertile scorei
Medium
H:gh (top tertile score)
Attitudes toward tanning
H:gh (top terlile score)
Medium (medium
Low (bmtcm te:iile scor;;.i
Unadjuste<:l
POR* (95% Cl)
HlO
3.f>9 (1.S7 -<t12)
S.C4 {4.02.-15.0Bj
4.74 (3.1S..7.07j
u:v
i .23 (U.B4-1.82}
0.55 (0.34-Q.9(Jj
10.72 (5.34-21.53}
37 {1 ,!)5... 7. 75}
LC.V
Stare has legislation restrictln{l minors' to indoor tanning:
Policies present before 1007!! (0.40 1.00)
Policies passoo 1997 (up to <HS (D.52-1J.l9)
No policies# during 1998 and 2004 1.00
Parental factors: parent/guardian used indoor tanning twoth ln the year
Yes 4.1>1 (3.04-5.97j
No U'(;
My parents/guardian would allow me io tan indoors using a sunlamp or a tanning booth
Agree 2D.3 (1S.2-S1.a..J)
Disagre;;.
Parent education
school
Some college
College graduate
PCR i:1dlcat.es odds ri.l!io: P.!i% Cl, 95% il\t$'-.-al.
POR a"d %% Gis <;r1cl<;se-d ir>
t AdjLts!ed FOR anrJ co1re.spondi:;g 95% Cis !lnrnosec in
1.53 (0.00-2.3S)
(0.99-.2.05}
1.nn
t Si<in sv: iildax on to tan, atiiity 10 !)<_.rn. and naif and o:;loi of t'le skin.
;'> A\t:tudes towan:j tarmi;;:J pref10r;:nce;; (based e-n 3 altitudinal it-di-ns; re;'?r to Spo<:::ifi.:;ation in lel'.t).
n Eight r13d access tc inXc1 ta"lnitlg befe 1997 a.'\d tr,rOt.;gh .2004,
t,ad not paosed leg!sfeticn alter :20C'4.
Rema:ning ;;t;:;t.;;s witt no such passed 1r. b<:Jt.'l 100S arrj ZC04.
DISCUSSION
Adjusted
POR (95"/lj C l)t
1 OG
2.00 (().35--t.50)
4.25 (1.91-9.50)
i()Jj(j (:>.73-19.60)
i_i)i)
100
1 55 (D.M-2. 71 i
0.71 (().:-!5-1.43)
8.84 (3.57-:?.1.86)
3.36 (l.2C>9.1 0)
1.{)0
0.77 (OA31.3ei
0 76 (OA6 1.29)
i.t-'0
4.2 i (?..23-?.SS)
1.00
Hi.55 (9.0226.80)
1.00
1. 01 (0.55-1.85)
1 20 (OJ2-2.0:.l)
i.C>O
m be significantly aswc!ated wi th the &equenr use ,,f
indonr t<wning C?:6 sessk)ns within the pa.-;r. yc-u: ndds ra-
rio jORI of3.23 [95/o CL IAH5.39]), bmwas found
robe reb red w sex, agt:, or sun scnsiriv.i.r:y.
Among 204 adoksccms Nho used iudoor ra.nnir1g
boo!hs/sunlamps, 7 reported ever getTing an infection or a
skin rsh (es!lm;m:d prev .. of 3%) from indoor
ning. 'These 7 were all aged ?.1 5 yeus, were moscly girls
(n = {)), iirtd had high h::vds of skin sun sensh:.ivity (n = 5)
(d.au not shown).
Tb.e principal findi ngs from (hesc 2 popularion-b:E;ed sur-
r)f adolesce.ots was mti(ma!ly the r)r
past-year use of indoor r;wni;,g did not change from 1998
to 2.004 (10% to 11%), despite an incr<::asing ll'..Unbcr of
swtes restricting wch usc by minors. The prevalence of
indoor tanni ng use nonsign.i.Gcandy among
youths who resided in th<;t Ja,:ked policies to l".ontrol
minors' acces-s to indoor unning ;l.nd decreased. nonsigni-
ficamly in thar enacted policies. States that h:l.d
Cancer
Oricinal .Article
Tabi!i' 4. and of Erythe-ma From li1do-:Jr Tannir,g Vse l.mong Who Use-d
indoor Tanning Booths/Sunlamps
Erythema
or Bums/'%
Tvta! 204 57.5
$ex
Female 161 6i.i
Male 44..
Age,y
H-15 H 50.8
16-18 137 51.0
Skin sun
Low 58 55.1
Medium 112 57.2
H;gn 34 64.0
No. of times tJsed indoor tanolng within the past ;;ear-
?6 1W
97 42.5
Univariate
OR (95% Clj
1.96 \0.9l-420i
1.0
l.O
1.50 (0.76-2.95)
1.0
1.10
1.45 (0.57 -3.69)
3.41 0. 78-6,54i 1 i
1.0
Multivariate
logistic Model for
Erythema/Burns,
AOR {95% Cl}
(Cl.894.33i!
i.O
'i.O
1.46 (!).73-
1.0
Ui (0.562.44)
AB (0.56-3.9:{/
3.2;) (i 'I
i.O
08 od<:ls ratio; E15% Cf. 95% cvdictence 1r!tffl'Val; AOF!.
- event assessed Have ycu gct31 red or at any Cr,'}E> 1.tE' past Nhen ynu ilS6d a. ta:rfl.,_\9 booth cr a sunlarnp't'
j .t\OH fer
ACR adjusted fer
AOR adjusted fur and age.
jjP<.00{)j,
] AOR ,,,ljuste..i fN age, s<;x. s1<.i11 sun soositivity.
rninors' rtstriction had lower 0<.-ids of
w.nning use among ado!escerm OR of
0.64; CL OAG-1.00) compared wir.h srarcs ilia
lacked such However, after ccrmolling for
strongly associated (r;:wrc p rmiimar.e) de1:erminarm of
indoor tanning use in yourhs, scate policies w:.:r:.: no.- sig-
nifkandy asstKhted with indoor t;J.nning (adjusred OR cf
0,77; 957i) Ci, 0..43-1 ,:)9).
Strengths of the srudy include the use of
methods and questions m assess rrends in
lndoor twer time, the ir.clusit)f'< of nationally
samples of adolescems, and th.:: ahili1:y ro
and C(mtrd h1r f-acwr;; .associated v.'ith
ind(}<X usc. Limitations of ch::! $tudy include reli-
ance on self n:ports ofhorh yom.hs and prim.'lly care givers
and a sample size that Jimired ror certain analyses.
Om m.::.dy's sa.mple W<1S limited w rel.iably es'itr..,.1re preva-
bKe of common events from indoor tanning use (ie,
rash or infe-ctions) and ;;.) sr.a re-to-state varia-
tions .in minors' induor access resrricrjons and indoor am-
niug u5.e.
Powe.r lim.itatiuns may bvt> co.ntributtd. t(l the bck
of a signifk:uu association between sr:;te minnrs'
law-s and prevalence of indoor mnning usc. Iris also likdy
that inadequate and
. ' h t'r . . , . ! l . . . 1.').1
amsms rccmce r e tEeG!Vtn.e:.ss OI. sue 1 eg1sJ.anon.
for example. Forster er a!
14
studied 2 states (Minnesota
wd Massadmsetr.s} with pol ides pa-
.rem ... 'll wTitren permission bd()rt' the. ()f indoor tan
niog d<CYices by an minor (aged < 16 years) and
found 81% of indoor mnning businesses sold a &cs-
slon to an underaged mlnor on at l (}f 2 attempts,
and hat the adolescems' <lge was nm ass.::ssed in 40'}-il of
art<:mpi:S.
In keeping with oth<:r rcpl)!'ts,
7
21
we: noted du:
re.po.rt of p.-.nnmi permission to use incloo.;: mn-
nl ng wJS strongiy corrda;ed with highet indoot tanning
used among ado!escems. Tlms, in rhar allow indoor
with parental ()f accompaniment,
grearer efforrs ro infi.mn par<:nrs a.hottt t.h<: h<lZ:uds (If
indoor tlllli1.i.ng llll.dfo.r more legisLrrion may
requitd to redut."l:! expo:mre to indoor
Cancer
r.anning.
22
He.ahh and. r.he medical ctJmmu-
nity could. play a gre<Her in !Y.lrenrs about
the shott-te:Wl and !ong-te:tm skin cancer risks
wirh rhe of indoor ranning and rhe role rhey can play
ln aSSilring that thdr children Jo not u.)e indoor tann!ng
] 'he <lpp.roach of ad.opting more re-
strictive (b.sed or1.m.inors' age) is ;,1.tppon:ed by
tbt \V<lrld Organizarion and rhe
Cnmmission on. Nor.:1-lonizing Radi.rri) l1 Protection.
Both org.mizadons rc(;ommend that use of these device$
''(')T I .... , ; !)"' . ,< Jwr !'
1
l()<e ' 10:'' c:! ... ' " "''"I l ,il
"-." .1t, <.. nt:: ... . .i/ .I ... 1 bt: "" -
Of particular with t" the preverrriou of
healrh to indo(lr tanning <.:posure, no
deer casts in indoor r.ann ing '>'it:r<.: am.ong the sub-
groups of' ;tdok-scents whe typbHy exhibit a higher
prt"v-aknce of indoor raani ng: use, such :JS old.er youths, girls,
those with medium skin sun s<:nsitivit"f, those with high le-ds
(}f positive tanning :mimdt.>s, r.hose "\."1-'ho are le;-s
u:;trs of -;ur:.su:een, ;;.nd whose parem also used indoor
tanalag. As t'X!X"ttr.d, many of th::!sc f.ac-
r)rs were amflm:::d as s1mng indepen.denr prediL"ffir of
lndoor tanning in ym\ths, a11d th::.-se ac-? mnsist-
c.m with :findings. r-.
7
'
2
' J 1 is concerning t:har older ad-
girls cominue co demonstrate higher use of indoor
ranning. In the US, nH)SC <ldnkscems ;u-e aware of the delcteri-
.. ,l .. ,.a;.. ..... s ,.,J: llVR t;; w " 'l 'll1" .-,,net 1= +s l-r--:.
E.,;" ,) t.,;,, \. . / . _t C:\ .1'.1! _1 \,. \ . .l .\"v l....,.,hl t's \o.
One pdndpai G1cto1 driving behavior is the &-x:iocul-
Elral bdief chat \'.':irh hcalrhincs;; and.
In addition .. the lack of impwv-111ems ln
ind.x)r t<>.nning among tt:tnage girb may be rdar.e-J ro envi-
ronmental. ftcwrs; there is to sugg-est d1at tanning
arc more cottctmt-ared in geographic with
. higher proponions :eenagets and fcrna.k:S ages t5 m 24
yeats:.> BeGwsc of the <mgoing gn:J\Vth and popularity of the
indoor mnning i.ndusuy,
1
1he:se iJ ndings underscore rhe need.
t()r signifkant :;duGHinn <H hoth the individual aad commu-
nity k"Vd m dt..1nge norms pe.rc;ining Ct) .ha'<ing a cttl
and to cor:nmuniry membtl'S reganling rl:te s.."'ious
ri:>b ofindom !anning.
12
Previous smdies have also reponed rhar indoor
ning caus(;'S bums (erythema) in to 55% of
29 wir.h rhc:;:;c: findings, we found rhar 57.)% of
aJokscenr of indo!lr mrming re-ported gctring re-d or
bumt:d from using dcvkc:;. Il1e strongest tacror
a;;sociate.d w.tth eryrhema from .indoor tanning af::er con-
twlling h:1r possible {sex, ag..-; and skin
Cancer
Indoor Tanning by US Adolescents/ Cokkin!des et al
sensit!viry) wa.s higher frequency (}f u.st: C:6 rim.cs). rhis
apparent relation between burns from d::vi..:cs and
higher-fteque!lC)' me may be the te:sdt of
m:.1ge of appmpria[e saf:e[y measur\C's {ie, ti.me-limired ses-
sions) to reduce dsks.
31
; Half of indonr tanners
in the US used. indoor tanning ?.6 rim.es dur:ing tht::
year. It is important to bear in mind that a burn fi:om UV
equipmem likd y rhe risk fi.w skjn c:H1C.trs as \s
ilie cast> for stmbums from
especially at young(;'r
Su::;h high of
associaJ:ed with. indoor r.anning .may nhim,ndy resulr in ;m
increasing btird<.>n of mdan.omi and ker;::.tir.wlyte card-
noma jn middle age. :<-<
Conclusions
1n conclusion, the of .i.ndoor r,wnhg in
youths did not ms.rbdly 1.998 and 2004,
despite incr:!;ls!ng nurnhers ,)f' states with kgisLuion
rescricring yomh access ;:o indoo.r tanning. 'I'his sugg:ess
the ned co develop mu1tiprong(;'d approa<.ll(;'S thar could
.::nh;.UJce change;; in this among underage
mimm.. Glven the known with thi$
practice, U.R strategies for reducing adoks..::cnt exposure to
indoor rarllliug include more stringent l.cg.isbri.ve mea-
sur:!S, such ;tS prohibiting the use of ind{)\)l' faciH-
by ag,d < 18 years, al<mg .vi1h
enforcement m;;chanisms. as weH 'l$ l':tt(:m to educte
adolescenlli and their parenrB regarding :he of
induor raruling, It is imponant to continue to monitor
the prevalence of indoor tanning u:>e among
31ld to ::valu.are snaregies t;)r reducing such exposure .
Conflict of Interest Disclosures
Th{' American Ca.at:{'r (L.w ii.):: both
st!rYry'"- Funding supporr for !Lwl Ct.\lb:ri!.'!l d mrvcy
'>\"aS provded bv rhe Amnicw C;u1<:.r.r Society Ncutmgena,
inc. OdJer rhan flnandal sappon, hm<'r !)rg,ml7.arkm had no
iovol vemr.m m th:= .udysis and. .i.rm:rprcfat.i.oll (:.f fhr dat;J., or Jn
the p!ep,<mricn, re-.'iew, or appwval of th<: anid<:.
References
L...o,tin;e So rac-e Ni. J. l)\L rhe indo<)r
IJV t,uU'Jng lndu.my; ;\ rtvitw 1)f skin tisk,
bend] t d::ims, and re:gctlat \nn. j Am Afr.1.d f),rmato!.
1(ll));53: 1035--1041,
197
Oricinal .Article
2. kn::mation<A! !\g;<:r1cy f(;r r.ln Cancer Working
GMtp on Ard\dd (UVi Light and Sklo Cao-
<:t:r. Tht: d. oF snnbe;is with cuf:;mf!Dns H12.-
tJgn;\m other $kin .::anc.:rs: 4 svsrem11dc
/ C:ma:r. 2007;!20: !1 1.& 1122.
.'3. [), h;mer j. lnd<.l!H hy
and. EUr J Cnru:D'. 200.S;41:
20-2::',
4. VE, W<?im1ock MA, O'Conm:H MC, Th11.11
MJ of indm7r tanning hy US youth, ;,:.ges
J \- ; 8 and by rhd r <>r C<'tegiv.:rs:
:md Pedi:tt.-:-i""!. 2002:109:112*-i 130.
). D('m)w CA, H<.Fawski EA, Dch:mnc SM, KD,
KC. Us<: ,,.;: indc.xJr. tanning Edl!des by white ado-
in rb: Unh(:d kld.
200.3: l57:8.54-B60
6. Geiler AC, Colditz G, Otivcria S, et Use of swJrn:ea,
su nbu.rnlag <l!lll bt>d a,-ncng .t.l<:!fi: than
lO 000 US antl Pdi:ltri<"!.
200:2; l O"J:! OO!:Il OH.
J.E, Lmwkh D, Fors1.er J L Emmom KNI, Scrt>lh<en
G, Demkrre ;\-!F. influ,U<:e$ )n
indoor t:.:nning. J ,16Jfzy;: Hrultl;. 2004:35!
')2S.e
::<, S\ndair C .. Artifldal ra;1ning risk and guidance.
World Org;mi:.mrion: 2!h1.-3. Av-.!Hable
April1.9, 1.008.
<J. EJ. Hdlig LF, R. Dr;\k,. SchHIJng
LM. RF. LHnpliziKi: whh yomh ac::ess reguh-
t.im:s ind.c:or UV A;.-d; D(Tjj:.rtul. 200'):14 1:
10, Md.:n;ghlin JA, Fr:md$ SO. Burkh:.m:lr DL, Ddbv-.11ie RP.
Indoor UV nmninf: you.ch <J(:c..;.ss uphte 20H7. Ard>
Dmfl!!to!. 2007.:1
11. Ddbv,Jile RP, Parka ER, ( ;.;rs<m$k) N, {".( a!. Yourh
in the d.;;.rk. at th.: Luwtng Arri1 Dt>rmllwi.
2003: !59:44:3.448
!2. CA, Mayer }A, Eckbanit L, et. al. with
f
: .. J .... ;! 'll.,; J .. rld., ..;,,., 1r (r. l' P'ne: faci!iries ;p
(,(, .. l ... ( ... b .... ,,, ,.,.. .;. , ' f t ..Avv ail .. ..., ' .0 ..
San [)!ego. j .An:: 2001
13. AB Jr. L.::e Wj, Adam> OP, MD. Ta.!'lning
fadiity comp1iancc with sr;;tc ;;nd feticn l reguhrions i..n
North <l pGor perbnmm::c . .f Am Ar:ad [Jc;;urrol.
1993;1.8{2 pr. n 2 L:->2 P .
14. Fcrs:cr JL, Lazovkb D. Hickle A, ScrcnS(>Jl G, Dcmierre
M.P. Complb.1\;;c wi.dl restr.i;:ti.,) .. on sale uf icdt>Or 1aruung
ses.>ions m yomh in M:!.>'s.a.:hmo;;rrs. JAm
Acaci.Detmawi. 2006;));%2-%7.
C<!kkinkks V, Wdnsto.::k rvt Glam. K. Albano]. Ward E.
193
Thw.l M. Tr::mh in ;;u.n protection p.ra<.."tices, .md
,u;iwd::s sun <':<pn5m:: protection :md ranninf_
anHJng tJS 1998-2004. Pcdiutrics . .2006;118;
H). Weimroc:k MA. A>se-sHnenr of by que>rion
nail'<:'; v..t!hiity <f unJ f(mrw!ati<)t\ >f :: ptdkdon
J C!irz ..'))2 ..
17, KD. ]:\, SI:< y)
SC, Clapp E. T!:t: in.Hm:nn. oE a ad pi:?t:::s oa
c<:m indo(>! tanning bduvl<r: t}ndings hom a mdd-dty
sa..tiiple. jAm [>en;-:<.rto!. 2007;57:'J{}fl ...:i07.
18. Franc!;; SO. Burkhardl DL RP. 2G05: A !nnr.<::
fUr US yuut:h tani.ing /hi:h
fM1'1'4Nf.. .J.(){)); (-i 1524-525.
l:J. SAS be. SAS/STAT U.5n'5 G;.ridt<., 9.L
C<lty, NC: SA5 1nsdnm ln:.:;
20. SUDAA.N User's M;;nu4l. r<:ka;;e
4
j.(i. Triangl<:
NC: rr\angk lrmimt<::; 2006.
21. Wvodruff .Sl, Pkkn LC, KD. .lL. Gihn<:r
T, Jviayer j i\ .. Meas11ri11g th' i.>f Jndt:>,;1
rannirtg n:",;;uiattcrts:
] Am :'le;;d Dmr.;;;q/, 20075<i:774-7HG.
22. &tlk AC. and. t:211I1:ng. ..
tricf. 2G{lH;l21: 1040-.l 04i.
:2;) .. Abdulla FR. .SR. Wil1if:l'd PM, Krow<1mk D,
Kaur M. T;mnlng ;md skJn G.\lll:t>J. Periitltr Demmtl)/.
200);21:50!-512
24. Jolll\St.)O KR. Hd.llg LL H:=strt EJ. SO, D(:akyn{:
$), Dc:Ha.,-aUe RP. lnd<ll)r n nn\ng; Jnd of
US .::omp;>r<-d with <>tht m<:;d.kul
Axch Dctmt:t:ui. 200{); 141:46) ...
2-). D, F{}ft{C< J, G, Ct al. ;\$SO
ciare""J wi th o r intention. to ind.onr t:mnir:g ::unong
ado!t$CCIH$. Arth Pd.i,:tr Ad<Jwsc t'v!<:d. ::WOt 158;9
:2t). P,;.te! .MR, j, Slymen DJ, W,.,>eksJR, rLndi\L
of t;UU' .ing within S;m Dleg1> Ct>umy, C\!l-
forni;e ..
27. &kl.anan C, H, H, Ni]ssoa B. Ulkn H.
Sud-I u.-;e in m <:Jyche1u:t, sum;.::re.::n
tl-6<: !lad skin /'-, su:Yey ;<!nong Swd-
.-.d.ule..'<:em:s. E J DtYmtit.ui. !9%; l }):712-71 6
28, .M, Dl:' G11ir.: L, ]. A
n:y on the ase of artiJ)c:ia i :anniag :n. the oF
0.n;ld.a. I Am ,1<'t!d Di!mUIJ>Ji. t 999;<:i0:572 5/(;,
:2y. Boldeman C, R, Dd H, aL 'T'ur1a:ng b.bits
aud ;;un!:>um in .t Sw<:d.ish. p<;pdadon ag.: L?-50 y(;;lr.s. Eur
J C.zJ1Ci't'. 20l1l ;.. F:244!-:24<i8.
30. Heilig LF, R.. AL. Ddlav;llt(: RP.
EJ. A !or hdoor UV r:mning f:tcil-
iry <per$wr's pr>Yt$kn of health inf(,rrn;Hkn iUnlttXI
Gmnr C.:-:ii>t>r Crmtm!. 100); I 6:557-560.
3l. DC, Whirtmar. CA. Gr<::<:n ;\C Childh>Gd stm
as a iiu:tnr i:or mdaaoma: ;, .. of
cpidemidogk swdks. C.mtH CmfSC.' Gmrro!. 2001; 12:69-1\2.
32. r.-1.R, Stan.n:ml VA, .Mott LA., Slatt:i:.'ry \-1},
SK. \);:dusrock MA. of wmlng devi<.Xs and of bll
sat !:<"lJ and S{1Ha tt lOti .. r..cH Clnt<:ri .. / lYrttl !rr.ft.
Cancer
MD Compliance with federal and state legislation by indoor tanning facilities in ... Pagel of 12
Use of this content !s subject to the Terms and Conditions
Compliance with federal and state legislation by indoor tanning facilities in San Diego
Journal of the American Academy of Dermatology - Volume 44, !ssue 1 (January 2001) - Copyright 2001
American Academy of Dermatology, Inc.
REPORTS
Compliance with federal and state legislation by indoor tanning facilities in San Diego
Carla A. Culley MPH"
Joni A. Mayer PhDa
Laura Eckhardt MPH;)
April J. Busic MPH a
Lawrence F. Eichenfield MD b
James F. Sallis PhOn
P. J. E. Quintana PhD a
Susan I. Woodruff PhD n
From the Graduate School ot Public Health" and the Department of Psychology,'-' San Diego State University,
and the Division of Pediatric Dermatology, University of California, San Diego School of Medicine and Children's
Hospital and Health Center, San Diego.
Accepted for publication July 13, 2000.
Reprint requests: Joni A. Mayer. PhD, Graduate School of Public Health, Hardy Tower #119, San Diego State
University, San Diego, CA 92182-4162.
JAm A cad Derma.tol 2001 ;44:53-60.
Copyright 2001 by the American Academy of Dermatology, Inc.
0190-9622/2001/$35.00 + 0 16/1/110063
San Diego, California
Background: The prevalence rates of both skin cancers and indoor tanning among the US population
are high and have increased substantially in recent years. Low compliance by indoor tanning
facilities with safety regulations may place consumers at greater risk of skin and ocular damage.
Objective: This study quantified the level of compliance by indoor tanning facilities with selected
federal and state regulations and recommendations.
Methods: Tanning facilities (N =54) in San Diego County, California, were visited by a confederate
posing as a prospective customer. Compliance with 13 regulations/recommendations were assessed
by either direct query or observation of the presence/absence of signs and warning labels. Operators'
responses to 5 risk-based questions also were noted.
Results: No facility complied with all13 regulations/recommendations. Compliance with 3 protective
eyewear regulations was high (89%"100o/o).ln contrast, compliance with maximum tanning frequency
recommendations (approximately 6/o) and parental consent regulations {approximately 43%) was
disturbingly low.
Conclusion: The investigators recommend instituting mandatory, comprehensive training for
http://www .mdconsult.com/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities in ... Page 2 of 12
operators, as well as systematic compliance monitoring with enforcement of penalties for
noncompliance. (J Am Acad Dermatol 2001 ;44:53-60.}
Ultraviolet radiation (UVR) from the sun is a known risk factor for both nonmelanoma skin cancers and
melanoma.lri f4! Although the evidence is sparser and less clear, UVR produced from indoor tanning beds
also has been linked to melanoma risk. [s; 16l Additionally, medical personnel have documented many cases
of skin burns and eye damage (including corneal burns) that resulted from indoor tanning devices. l7i tB! The
indoor tanning industry, which has grown substantially in recent years, !9l has argued that indoor tanning
is safe because tanning beds primarily emit "harmless" UVA radiation and that indoor tanning provides a
''base tan" that protects customers against future sunburns. P11 In contrast, several health organizations,
including the American Academy of Dermatology and the American Medical Association, have lobbied for a
complete ban on Indoor tanning facilities. These requests were spurred by the data linking both solar and
indoor UVR to malignant melanomaw! and the damaging acute effects of tanning beds. Additional data
have indicated that the majority of indoor tanners have skin types I througt1 Ill (Fitzpatrick classification),
f14! indicating a high to moderate propensity to burn after the first (summer} exposure to midday sun. r'sl
These data are particularly disturbing because skin type is considered a risk factor for both nonmelanoma
skin cancers and melanoma.l1! f4!
Currently, the Food and Drug Administration {FDA) regulates various aspects of indoor tanning equipment
(ie, sunlamp products) through the Code of Federal Regulations (CFR) 1040.20, rsunlamp products and
ultraviolet lamps intended for use in sunlamp products"). tHi.1 As of 1999, the FDA has been in the process of
considering revisions and updates to current sunlamp product pertormance standards. Revisions may
address developing a recommended exposure schedule on the basis of recent epidemiologic data and
simplifying/clarifying the messages on warning labels, as well as other issues. [l7J In general, the
operations of tanning facilities (eg, consent of parents for minors) are regulated at the state level. In
California, the Filante Tanning Facility Act of 1988 was created to protect and promote safety "concerning
tanning with artificial ultraviolet light." ;1aJ Compliance by tanning facilities with the regulations may help
reduce some of the health and safety risks associated with indoor tanning.
In Southern California, individuals have the potential to be exposed to relatively high levels of solar UVR. !19!
(20! Those who frequent indoor tanning facilities may be (eceiving unusually high overall doses of UVR,
particularly if tanning facilities are not in compliance with regulations that attempt to control exposure. The
objective of this study was to use direct observations to assess compliance with select federal and California
regulations by San Diego indoor tanning facilities.
Methods
The study sample consisted of 54 tanning facilities in the San Diego metropolitan area. A tanning facility was
defined as any location, place. area, structure. or business that provides persons access to any tanning
device. tHJ.1 A list of tanning facilities was obtained from the listings under "Tanning Salons" in the San Diego
Yellow Pages and a search of the Big Yellow directory at www.bigyellow.com t'Y of "Tanning Salons" in
the San Diego (Metro) area. From these lists, those who were found to be out of business or who no longer
offered tanning services were excluded. When there was more than one facility listed that had the same
owner (ie, a chain), one facility was selected at random for inclusion. The final list consisted of tanning
salons, fitness centers, hair and nail salons, and other beauty supply companies.
The primary dependent measure was tanning facility compliance with select federal and state regulations as
assessed by direct observation of facilities and conversations with facility operators. Data were collected by a
confederate (C. A. C.) who posed as a potential customer seeking information about the indoor tanning
process. An assessment tool was developed for this study, on the basis of variables addressed by the federal
Sunlamp Products Performance Standard Final Rule of 1985t1S! and California's Filante Tanning Facility Act
of 1988. r1ai The federal regulations that were assessed were the presence of a shut-off switch that would
terminate radiation emission, and the presence and legibility of danger signs and other labels on the tanning
machines themselves, The federal recommendations involved the frequency and duration allowed to tan. The
recommended exposure schedule is "no more than 0.75 MED (minimal erythema dose) 3 times the first
week, gradually increasing the exposure the following weeks until maximum tanning has occurred ... 1211 The
http://www .mdconsultcom/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities in ... Page 3 of 12
California regulations consisted of provision, sanitation, and requirement of protective eyewear, warning signs
posted and legible In the tanning area, and written parental consent required for 14- to 18- year-olds (several
of the safety issues, including protective eyewear, are addressed by both the federal and California
recommendations). Compliance was defined by means of criteria provided by the fede(al !H>! and state 18
regulations.
Additionally, the confederate asked the facility operator 5 open-ended questions regarding the safety of
tanning facility use. including: (i)"Are tanning beds safe?", (2)"Can I get sunburned from using tanning
beds?", (3)"1s tanning in beds safer than tanning outdoors?'', (4)"Does a base tan protect me from burn?'',
and (5)"Can I get skin cancer from tanning beds?" These questions were adapted from questions asked in
previous studies. [22: :241 Responses to these questions were manually recorded and later coded for analysis.
Other factors that were monitored included the number and types of beds. availability of written materials,
and demographic information about tanning machine operators.
Data were collected during April1998. One confederate, posing as a potential customer, visited all 54 tanning
facilities, and a second confederate visited 26 of the facilities 2 weeks later. One half of the facilities randomly
were selected to be revisited in an attempt to conserve resources, while still obtaining reliable estimates of
agreement Twenty of the 41 tanning salons and 6 of the 13 "other'' facilities were revisited. The second visit
measured a subset of the variables as a means to check reliability of results without provoking suspicion by
tanning facility operators. Each confederate was female, mid-to-late twenties, and non-Hispanic white.
without a noticeable tan. Each visit lasted approximately 1 0 to 15 minutes. The confederate introduced
herself as someone who had never used tanning beds before. She also explained that she wanted to get a
tan before going to Hawaii the next month and had some questions on the safety of tanning beds. To assess
compliance with parental consent requirements for minors, the confederate mentioned that she was
considering sharing a package of tanning sessions with her i 5-year-old sister, and inquired whether this
would be allowed. The confederate then asked a series of questions and made direct observations of the
facilities per a standardized protocol. The protocol consisted of the script, including specific questions (eg,
"Do you provide goggles?") and directions for observations (eg, look for danger warning signs on tanning
bed) that coincided directly with the federal or state codes.[;eJ [1SJ After exiting the facility, the confederate
recorded whether she observed specific practices (such as the presence of warning signs) and recorded the
verbal responses to the scripted questions (as close to verbatim as possible} on the assessment tool
checklist. All study procedures were approved by the Committee on the Protection of Human Subjects at San
Diego State University.
Using the Statistical Package for the Social Sciences (SPSS), descriptive statistics were calculated for all
variables. Frequencies were calculated for the categorical variables, and means were calculated for the
continuous variables. Chi-square and t tests were used to compare tanning salons and other facilities on
outcomes. lnterrater reliability was calculated by means of the kappa statistic.
Results
lnterobserver reliability
Table I presents interconfederate agreement data (and kappavalues) on select variables for the 26 facilities
that were visited by both confederates.
Table I. Agreement between observers (n = 26 sites revisited)
Same operator {n = 13) Different operator (n = 13) Overall
% % %
Agreement kappa Agreement kappa Agreement kappa
Gender of 100.0 1
operator
Age of 61.5 .492
operator
Tan ness 25.0 .000
Frequency 100.0 84.6 -.083 92.3 -.040
http://www .mdconsultcom/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities in ... Page 4 of 12
allowed to tan
Maximum
duration
allowed to tan
Goggles
provided
Goggles
required
Goggles
sanitized
Warning sign
Parental
consent
required
Written
materials
provided
Shut-off
switch
Danger labels
on bed
Exposure
labels on bed
01: Are
tanning beds
safe?
05: Can I get
skin cancer
from tanning
beds?
100.0
100.0
84.6
100.0
92.3
91.7
84.6
53.8
76.9
76.9
100.0
50.0
t
.755
.833
.435
.093
.316
.316
.000
100.0
100.0
76.9
100.0
92.3
53.8
76.9
61.5
100.0
100.0
100.0
66.6
i
t
1
.755
.093
-.114
.269
i
.333
100.0
100.0
80.8
100.0
92.3
72.0
80.8
57.7
88.5
88.5
100.0
58-3
.102
.755
.448
.198
.183
.661
.661
.167
*Pe(cent agreement based on answering in the positive (yes, indirect yes} or liegative {no, indirect no).
t kappa Statistic cannot be computed; the number of nonempty rows or columns in the contingency table
is one.
At half of these facilities, the two confederates encountered different operators, which may influence the
between-observer consistency estimates. Therefore data are segregated by whether the same versus
different operators were encountered, as well as presented for all facilities combined. In general, agreement
was high. Excluding the variables that assessed characteristics of the operator. across the 26 facilities that
were visited twice, 1 0 of the 13 variables showed interobserver agreement of .80 or better. In interpreting
kappa, wtlich controls for chance agreements, values greater than .75 indicate excellent reproducibility, with
other categories defined as good (AO-. 75), marginal (0-.40), and disagrees more than expected by chance (<
0}. [25! Reliability estimates for the majority of variables were comparable at facilities with the same operator
and facilities with different operators. It appeared that operators behaved consistently (across time) regarding
obtaining parental consent.
Characteristics of tanning facilities and operators
The tanning facility sample consisted of 41 tanning salons, 6 fitness centers, and 7 beauty salons located in
the San Diego metropolitan area. The number of tanning devices housed in each facility ranged from 1 to 15,
http://www .mdconsultcom/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities in ... Page 5 of 12
with an average of 6 beds/booths per facility. Tanning salons had an average of 7 bedsibooths, and other
facilities had an average of 3 beds/booths. A total of 325 bedsibooths was reported for all 54 facilities.
The type of tanning devices available to consumers varied. All of the facilities offered what they referred to as
"standard" or beds. These were advertised as the ''Wolff System'' or ''Solaria System" tanning units
that contain a variety ot tanning bulbs of various intensities that emit both UVA and UVB rays. In addition, 13
(24%) of the facilities offered the high-pressure ''Uitrabronz,'' "Super bed," or ''Orbit bed," which were
advertised as containing 100% UVA rays and no "harmful burning UVB rays.''
The tanning device operators included 35 (65%) females and i 9 (35%) males. The age distribution of
operators was estimated as 13 (24.1%) between the ages of 16 and 25 years, 19 (35.2%) between the ages
of 26 and 35 years, 14 (25.9%) between the ages of 36 and 45 years, and 8 (14.8%) older than 45 years.
Compliance with federal and slate regulations
Fig 1 summarizes compliance with the 13 regulations! recommendations.
.. 4 $ . :; a . . . to 11 u
. . . . .
. Number of reguraliooS/recommMdatiorts being complied With.by fadlitles
F!g. 1. Tanning facl!ity comp!iant:iif !o !3 nnd s1atn reguinHons!mcommiim(ialion;:;.
No facility was in compliance with all regulations. The mean number of regulations complied with was 8.33
(standard deviation [SO]"" 2.0).
Compliance with specific federal and state regulations, overall and by type of tanning facility, is summarized
in Table II.
Table II. Compliance of tanning facilities with federal and state regulations/recommendations, by facility type
Federal
regulations
Shut-off switch
present and
compliant
Percent complying
Tanning
All facilities salons (n =
{n =54) 41)
56.1%
Other
facilities (n
= 13}
61.5'%
chiz df Pvalue
.1i9 .729
http://www .mdconsultcom/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities in ... Page 6 of 12
Danger labels 85.2% 87.8% 76.9% .926 .336
present
Danger 74.1% 75.6% 69.2% .209 .647
statement legible,
accessible,
correct
Other 85.2% 87.8% 76.9% .926 .336
(exposure) labels
present
Other 74.1% 75.6% 69.2% .209 .647
(exposure) labels
legible,
accessible,
correct
Federal
recommendations
Frequency 5.6% 7.3/o 0.0% i.01 .316
allowed to tan
Duration 97.7'"/o 96.8% 100.0% .396 .529
allowed to tan
California state
regulations
Protective 100.0% 100.0% 100.0%
eyewear provided
Protective 100.0% iOO.OQ/o 100.0%
eyewear
sanitized
between use
Protective 88.9% 85.4% 100.0% 2.14 .143
eyewear required
for facility use
Warning sign 20.4% 19.5% 23.1% .077 .781
posted in tanning
area
Warning sign 14.8/o 14.6% 15.4% .004 .947
legible,
accessible,
correct
Parental 42.6% 46.3% 30.8/o .979 .322
consent for ages
1418 required
Note: Data are from the first visit.
Fitness centers and beauty salons were combined into an "other" category because of small sample sizes.
Compliance with individual federal regulationsirecommendations ranged from 5.6/o to 100%. As shown,
compliance with individual California regulations ranged from 14.8% to 1 00%.
Compliance was found to be relatively high for provision and sanitation of protective eyewear; maximum
duration allowed to tan; requirement or the use of protective eyewear to tan; presence of warning labels of
UVR danger and exposure labels; and the legibility, accessibility, and correctness oi these labels. lower
http://www .mdconsult.com/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities in ... Page 7 of 12
compliance was observed for frequency allowed to tan; presence of warning signs; legibility, accessibility,
and correctness of warning signs; parental permission for those between the ages of 14 and 18 years; and
presence and compliance of an appropriate shut-off switch. Confederates were unable to obtain a statement
of acknowledgment or written warning statement from any of the facilities visited.
When confederates asked how long they would be allowed to tan, tanning facility operators recommended
starting with 7 to 16 minutes with an average of 1 0.4 minutes (SD = 1.88). Twelve facilities limited tanning
sessions to 20 to 30 minutes, and 1 facility allowed double tanning sessions (2 consecutive 20 minute tanning
sessions). The FDA's recommended exposure schedule for first-time users varies according to skin type, but
it suggests that exposure be limited to 3 times the first week at a maximum of 30 minutes per session. l2ll The
response distribution for the frequency item was generally bimodal and consisted of giving the range of "3 to
5 days per week'' (coded as compliant) or daily (coded as non-compliant). Thus, because the compliant
category included some responses that implied that more than 3 days per week is recommended, our criteria
for this variable were somewhat lenient.
Chi-square tests of association between facility type (tanning salon vs other facilities) and compliance with
tanning facility regulations/recommendations were conducted. There were no significant associations found
between facility type and compliance. Chi-square values, degrees of freedom, and P values for each
regulation/recommendation are reported in Table IL No difference between salons and other facilities was
found for the length of time allowed to tan during initial visits (ie, early in the tanning process) (t [df"' 32]
= .438. p = .664).
Summary of claims made
Coded responses to the confederate's openended safety questions are summarized in Table IlL
Table Ill. Responses to dskisafety questions
1. Are tanning beds safe?
Yes
Indirect yes
Indirect no
Other t
2. Can I get sunburned
from using tanning beds?
Yes
Yes, qualified
No
3. Is tanning in beds safer
than tanning outdoors?
Yes
Indirect yes
Indirect no t
No 1
Other i
4. Does a base tan
protect me from burn?
Yes
Indirect yes
Tanning salons (n = 41) Other facilities (n = 13) Total (n =54)
22.0/o
63.4%
14.6%
0.0%
9.8/o
87.8%
2.4%
7.3%
53.7%
2.4%
31.7%
4.9%
92.7%
4.9%
38.5%
46.1%
7.7%
7.7%
38.5%
61.5%
0.0%
15.3%
38.50/.:,
O.OQ/o
38.5%
7.7%
92.3"/o
0.0%
25.9%
59.2%
13.0%
1.9/o
16.6/o
81.5%
1.9%
9.2%
50.0%
1.9%
33.3/o
5.6%
92.5%
3.7%
http://www .mdconsult.com/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities in ... Page 8 of 12
Indirect no
Other t
5. Can I get sl\in cancer
from tanning beds?
Indirect yes
Indirect noievaded
question t
No :t
Other t
2.4%
0.0%
26.8%
63.4%
4.9%
4.9%
0.0'%
7.7%
46.2'%
53.8"/o
0.0%
0.0%
1.9%
1.9%
31.5%
61.1%
3.7%
3.7%
*Responses to these questions were combined for statistical analysis (all were in the affirmative direction).
t This response was not included in the statistical analysis.
1 Responses to these questions were combined for statistical analysis (all were in the negative direction).
When asked "Are tanning beds safe?", approximately 85% of operators directly or indirectly replied in the
affirmative. Those responses coded as an indirect yes included: "Tanning beds are safer than outside," or
"It's OK if you use them in moderation." The remaining operators answered "no," an indirect no, or other. The
answer coded as an indirect no was, "I can't tell you they are safe or free from risk." Other responses for all
questions included, "I don't know," or "I can't say."
When asked "Can I get sunburned from usir1g tanning beds?'' all but one of the opefators directly replied
"yes" or gave a qualified yes. Examples of answers coded as a qualified yes included: ''Yes, but not like when
you burn outside," or "Yes, that's why we only let you start out for a sho(t amount of time at first."
When asked ''Is tanning in beds safer than tanning outdoors?", 59% replied "yes" or gave an indirect yes
response. Indirect yes answers included, "There are only UVA rays indoors, so it's better,'' "You have more
control over the type of rays indoors,'' and "You have more control over the amount of time exposed indoors."
The remaining operators replied with a direct no, indirect no, or other. The answer coded as an indirect no
was "It's a little more intense indoors."
When asked "Does a base tan protect me from burn?", approximately 96% of operators responded
affirmatively. The indirect yes answers Included "Tanning is the body's natural defense against burning." The
indirect no answer consisted of "You still need to be careful and wear an SPF of 15 when you are outside."
When asked "Can I get skin cancef from tanning beds?'', approximately 320f.., of answers were coded as an
indirect yes. These answers included "There is a risk,'' "It's the same risk as outside," or" You can get cancer
from everything.'' The majority (68.5/.,) of responses were coded as an indirect no/evaded question.
Examples of these responses included: "Skin cancer is genetic," "Burning causes skin cancer," or "There is
less risk indoors." The results of chi-square tests indicated no significant associations between the answefs
provided to the safety questions and tanning facility type.
Discussion
To our knowledge, this study was the first to evaluate the compliance of California tanning facilities with
federal and state regulations. To reduce possible self-reporting biases, data were collected by confederates
posing as customers. In addition to evaluating compliance with formal regulations and recommendations, we
also assessed information that operators provide to clients when queried about the risks of indoor tanning.
Key findings are discussed below.
Compliance with the individual regulationsHecommendations varied widely. Fo( example, all facilities were
complying with the regulations for providing and sanitizing protective eyewear, and the majority required them
http://www .mdconsultcom/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities in ... Page 9 of 12
for facility use. In alarming contrast, even using a liberal definition ot compliance, only 6% of the facilities
were recommending appropriate tanning frequencies. Facilities also showed a relatively low rate of
compliance with requiring parental consent for minors. In general, the responses to the confederate's
questions about risk tended to minimize concerns about the safety of indoor tanning and the risk of skin
cancer. However, the majority of operators did admit (or at least imply} that one can get sunburned using a
tanning bed.
Our findings regarding protective eyewear were reassuring, given the damaging effects UVR has on the eye.
f7l 1.2e; However, they should be interpreted cautiously, because they are based on the operator's
verbalization of what they would require in a future tanning session. An study, in which
confederates actually received tanning sessions, found that no facility required the use of eyewear.rzz;
Umits placed by facilities on duration and frequency of tanning sessions likely are significant in protecting
consumers from overexposure to UVR Although our data on the duration variable were encouraging, the
data on tanning frequency showed poor compliance. Even though the confederate stated she previously had
never used tanning beds, the majority of operators said they would allow daily tanning. Other investigators
also have reported low compliance with tanning frequency regulations. i22! Promotional incentives that
provide an number of tanning sessions for a flat monthly rate were encountered during the study,
although not systematically assessed. These types of promotions, coupled with the lax frequency practices
found at most of the facilities, are allowing and even encouraging high-risk tanning behaviors.
Perhaps the most disturbing finding of this sludy was that facilities were not complying with regulations
regarding parental consent for minors. Given that (1) adolescents have been found to place a high value on
having a tan 1.211 ; (2} UVR exposure during youth is a major contributor to the subsequent appearance of skin
cancert3J [2s; [29! ; and {3) facilities tend to allow "more than optimal" tanning session frequency, as noted
above, adolescents are a particularly vulnerable group that is interacting with a high-risk environment. A
survey of Minnesota adolescents found that respondents used commercial tanning facilities at high rates.
These indoor tanners frequently did not perform protective behaviors such as wearing goggles, reported high
levels of skin and eye problems, and stated they had not been warned by operators on the risks of tanning.
[30!
In 1991, 32 tanning facilities in North Carolina were inspected for compliance with 21 state and federal
requirements. L3ll Results of our study specific to complete compliance were comparable to the earlier study
and equally disappointing; no facility in our study and only 1 facility in the other study was in compliance with
all regulations. For the 4 regulations assessed in both studies, compliance in our study was consistently
higher: 85% (vs 780/.:,) for visible warning signs, 100% (vs 84%) for eyewear available, 100% (vs 84e/..,) for
eyewear sanitized, and 43% (vs 13%} for parental consent for minors. However, inferences regarding secular
trends toward improved compliance with these specific regulations must be made cautiously, given that the
two studies used different data collection strategies and were conducted in different geographic locations.
Several methodologic issues related to our study should be considered. First, because the confederate was
not able to view every room of each site, data on some variables (eg, presence of warning labels} may not
accurately reflect the absolute level of compliance with these regulations for individual facilities. Second, our
confederate posed as a prospective client, and operators reported what would be required (eg, eye gear) in
near future. Although we assume these responses mirror the operator's actual behavior with ''real" clients at
the time of their tanning session, the relationship between these two outcomes was not evaluated. Finally,
our sample was restricted to one geographic location. Consequently, the generalizability of our findings may
be limited.
Strengths of the study included (i) visiting a larger number of sites relative to previous studies and visiting all
sites (minus facilities in the same chain) in a large city; (2) reducing potential social demand biases by not
revealing the true pu(pose of the confederate's visit; (3) using rigorous procedures in developing, pilot testing,
and refining all observational and coding activities, including the training of the confederates {these
procedures likely enhanced the reliability of the data}; and (4) assessing responses (ie, claims) made by
operators when posed specific questions, in addition to assessing compliance with state and federal
regulations.
Our findings, in conjunction with the generally low level of safety regulation compliance found in previous
http://www .mdconsultcom/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities... Page 10 of 12
studies, f12i have important implications related to operator training and facility inspection. Tanning facility
operators are a first line of contact for the public regarding information about tanning bed use and safety, and
they are the "gatekeepers" for indoor UVR exposure. Consequently, comprehensive training of them should
be mandated. Currently, the majority of the states do not (equire such training, and a previous study repO(ted
low levels of operator knowledge regarding safety issues as well as low rates of previous training. 132! Training
should include strategies for complying with each federal and state regulation, and provide a scientifically
based orientation about the potential dangers and benefits of artificial UVR exposure. Participation by
dermatologists in the development and delivery of operator ttaining likely would help ensure the quality of the
content.
In addition to mandatory operator training, we recommend that county or state health officials systematically
monitor facility compliance. In California, a violation of any of the state regulations is punishable by a fine of
$250 to $1 000. :z1! However, anecdotal information suggested that routine Inspections of California facilities
(and subsequent enforcement of the law) are infrequent. On the basis of the current findings, inspectors
should pay particular attention to practices related to the frequency of sessions and parental consent.
In conclusion, in a county with high levels of UVR 20 and high melanoma rates, l33J f34l many indoor tanning
facilities were noncompliant with key federal and state regulations. Our results suggest that operators are not
informing consumers about the health hazards of excessive use of tanning beds. Improved inspection
policies and enforcement of existing regulations, along with mandatory, high-quality operator training, could
help reduce the risk to consumers.
References
1. Friedman RJ, Rigel DS, Berson DS, Rivers J. Skin cancer basal ce!i and squamous cell carcinoma. In Ho!!eb AI, Fink DJ. Murphy GP, edi:ors.
American Cancer Society textbook of clinical oncology. Atlanta: American Cancer Society: 1991. p. 290-30$.
2. Singletary SE, Balch CM. Malignant melanoma. In: Ho!!eb A!, Fink DJ, Murphy GP, edi!ors. American Cancer Socie!y textbook of clinical oncology.
Atlanta: American Cancer 199L p. 263-70
3. Mar1<S R. An ovetview of skin cancers: incidence and causation. Cancer Suppl 1995;75:607-12.
4. Elwood JM Recant developments in melaloma 1993 Melaflorna Res 1993;3:149-56. Abstract
5. Westerdahl J, Olsson H. Masback A, lngvar C, Jonsson N, Brandt L. Use of sunbeds or sunlamps and malignant melanoma in southern Sweden.
Am J Epidemic! 1994;140:691-9. Abstract
6. Walter SD, Marreu LD, From l, Hertzman C, Shannon HS, Roy P. The association ol cutaneous malignant melanoma with the use ot sunbeds and
sunlamps. Am J Epidemiol 1990; 131 :232-43 Abstract
7. Centers fer Disease Control and Prevention. Injuries assoc:ated with ultraviolet tanning devices-Wisconsin. MMWR Morb Mortal Wkly Rep
1989;38:333-5. Citation
8. Walters 8!, Kelley TM. Commercial tanning faci!ilies: a new source ol eye injury. Am J Emerg Med 1987;5:386 9. Abstract
9. DeLeo VA, Tanning salons. lr.; American Academy of Dermatology, editors. Proceedings of na!lona! conference on environmental hazards to !he
skin, October 1S92 (IL) American Academy of Dermatology; 1994, p. 37-41.
10. The $1,000,000,000 industry worth its weight in gold. Looking Fit 1992;7(5):46-70.
11. Cyr WH. CDRH evaluation of UV-emitting sunlamp products. In: Proceedings of National Conference of Radiation Control Officers. Mesa (All:
1998.
12. Spencer JM, Amonette RA. Indoor tanning: risKs, benefits, and tu!ure trends. JAm Acad Dermatol 1995;33:28898. Full Text
13. Diffey BL. Use of UVA sunbeds for cosmelic Ianning. Br J Dermatol1986:115:67 76. Abstract
http://www .mdconsult.com/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities... Page 11 of 12
14, Mawn VB, Fleischer AB. A survey ot attitudes, be!lefs, ar1d behavior regarding tanning bed use, sunbathing, ancl sunscreen use. JAm Acad
Dermatol 1993;29:959-62. Abstract
15. Fitzpatrick TB. The validity and practicality ol sun-reactive skin types 1 !hrough VI. Arch Dermatol1938;124:869-71. Citation
16. Department of Health and Human Services, Food and Drug Administration. Sunlamp products: performance standard; final rule {21 CFR 1040).
Fed Reg 1985:50:36546-52.
17, Department of Health and Human Services, Food and Drug Administration. Medica! oevices; Sunlamp products pertormance standard: request lor
comments and information, proposed rule (21 CFR s 1 020). Fed Reg 1999;64:6288-90.
18. California Department of Health Services. Department of Consumer Affairs. Filante Tanning Facility Act of 1988 Business & Professions Coda
23-22700081998.
19. National Weather Service: 1999 [Online]. Available at: http:/iv.ww.wrh.noaa.gov!sandiego C'!jf and http:f/www.nwsla.noaa.gov/climate
20. Environmental Protection Agency: 1998 [Online}. Available at htlpJ!nic.!b4.noaa.gov/productsfstratosphere!uv-index .
21. Department of Health and Human Services Quality control guide for sunlamp products. Rockville (MDi: Public Health Service; 1988; DHHS
Publication No, (FDA) 888234.
22. Bruyneei-Rapp F, Dorsey SB, Guin JD. The tanning salo11: an afea survey of equipment, p(ocedures, and pfactices. JAm Acad Dermatol
1S88;tS:103o-s. Abstract
23. Fairchild A. Gemson D. Safety information provided to customers of New York City suntanning salons. Am J Prev Med 1 992;8:381-3. Abstract
24. Beyth R. Hunnicutt M, Alguire PC. Tanning sa tons: an area survey of proprietos' knowledge ol risks and precautions. JAm Acad Oermatol
1991;24:277-82. Abstract
25. Rosner B. Fundamentals of biostatisHcs, 4th eel. Belmont (CA): Wadsworth Pubiishing: 1995.
26. Council on Scientific Ailairs. Harmful effects of ultraviolet ractiaHon, JAMA 1989:262:380-4. Abstract
27. Mermelstein RJ, Riesenberg LA. Changing knowledge and altitudes about skin cancer risi( factors !n adolescents. Health Psychol1992;11 :3716.
Abstract
28. Marks R. Sl<in cancer-childhood proJection a!fords lifetime protection. Med J Aust 1997;147:4756.
29. Weinstock MA. Colditz GA. Willett WC. Slampler MJ, Bronstein 8R, Mihm MC,et al Nonfamitial cutaneous melanoma incidence in women
associated with sun exposure before 20 years of age. Pediatrics 1989;84:199-204. Abstract
30. O!ipha11t JA, Forster JL, McBnde CM. The use ol commercial ta11ning facilities by subufban Minnesola adolescents. Am J Public Health
1994;84:476-a. Abstract
31. Fleischer AB, Lee WJ, Adams DP, Zanolli MO. Tanning ladli:y compliance with state and federal regulations in Norm Carolina: a poor
per!ormance. JAm Acad Dermatol !993;28: 2127. Abstract
32. Fleischer AB Jf, Fleischer AB. North CaroH11a tanning open:l!ors: hazard on the horizon? JAm Acad Oermalol 1992:27:199-203. Abstract
33. American Car.cer Society. Cancer facts and figures, California. Oakland (CA): American Cancer Society; 1998.
34. American Cancer Society. Cancer !acts and figures. Atlanla {GA): American Cancer Society; 1999.
http://www .mdconsult.com/das/article/body/162799091-2/jorg=joumal&source=&sp= 1 16... 9/29/2009
MD Compliance with federal and state legislation by indoor tanning facilities... Page J 2 of 12
Copyright 2009 Elsevier Inc. AI! rights reserved. vvww.mdconsult.com
Bookmark URL:
http://www .mdconsultcom/das/articlelbody/162799091-2/jorg=joumal&source=&sp=ll6... 9/29/2009
I
Tanning facility use: Are we exceeding Food and
Drug Administration limits?
Robin L. Hornung, MD, MPH," Kris tin H . . Magee, BS/' Willit" J Lee, 1\<lPH, MSPH,<'
t ori A. Hansen, BA. d and Yi-Ching Hsieh, MS"
Seattle, Wasbington; Cary. No-rth Carolina; Evanston,
and Portland, Ot-egon
Bm:kgrmmd: The US Food and Drug Administration (FDA) rccommends exposure limits for tanning bed
u;;e. Tanning patrons may n.ot following and may be- O\'erexposed to damaging
radiation (UV) .
Objectit:e: This study \;as conducted w assess ran.ning patron.">' adherence to FDA-re,:omme.nde.d exposure
limits and. w m0a:>ute the amounr of UV A and UVB radiation <.micte.d by tanning beds.
Methods: A community-based w--as administered during routine lnspec!ions of North Carolina
tanning fadities (n = ">0) . . At each f:<cility, patron records were randomly selected (n = 483) for a survey
of t'XP<)Sure nxords. :md UVA :md U\-13 outputs were mt:aSurcd for each tanning bed.
Results: The recommended limit:.:; were exct:eded by 95% of patrons, and 33(rr; of p:nrons began tanning
;H maximum recommt:.ndt:.d for maintenance tanning. Average t:a.nning bed output \.vas 192.1
tNA and 0 35 w.:m
2
eryi:hemally weighted UVB.
Cmu:lustmUt: for t -mning beJ ope-rators and p-Jtmn::- are needeJ 10 inne<.t!:'t:' cnmplhmce with
fe<.kra!Jy limits. U Am Acad lkrmato! 2003;49:655-<) J. .)
I
n re . .:;pon:>e to increasing :>kin cmcer ind-
dence.u public health t..ave brought
Mrention to dangers of tJltravio!et radi-
ation OiV). HoNever, much k'ss is known .about the
dangers of UV iiorn tanning bed use. St1.1dies have
sllown that. bed can incur severe
skin or corneal bums.:> tiV exposure also can in-
Hcute to medica-
tk)n;;,5( such as the reported psor-alen reaction re-
sulting in the dear.h of a tanning bed patron.
7
Chronic uv can photoaging of
From the Division of Derm<ltology, Department of Pediatrics;'
Vo!versity of Washington School of Medicine/' Radiation
Prote<:tion, Inc, Cary<; the Institute for Health Services P.eseatch
Policy Studies, Northwestern Univ('rsity, and
Bioinformatics and Biostatistics Core, Oregon Health and
Science University ...
Funding sources: Grants from the Dermat ology the
Julius C. Franklin Foundation, and the North Carolina chapter of
the American Cancr:r Society.
Conflict of interest: None identified.
Accepted for pubHC<ltion J<mu<.lry 27, 2003.
Reprint requests: Robin L Hornung, MD, MPH. Dermatology 4H-4,
Children's Hospital and Regional Medical Center, 4800 Sand
Point Way, NE, Seattle, WA 98105. E-mail: robin.homuog@
seattlechildrens.org.
Copyright 2003 by the Ameri<an of Dermatology. Inc.
019{)-962V2003/$30.00 + 0
doi: 10.1 067/SO 1909622(03}01586-X
Avbrevia.ttot;,s 11sed:
GEE:
FDA:
MED:
l1V;
generalized (;:.">tirnating
Food and Drug Adminbtra!ion
minuna! erYthemal dose
\lltwviolet radiation
and catardct formation H:.n More importantly,
sttJdies shown an assodmion sunb<:d
use and both mdanornar.t-t:; and nonrndanon1:1 skin
CMK.ersJt>,17 The potential <1:'i:>odation wn-
ning hed use and skin cancer is concerning gh'en
the popuklrity of indoor tanning.
The US tanning .industry serves an estimated 28
million persons. It is a $5 billkm pet
bus.iness that continues to grow.'K There are cur-
rently 30,000 t;mning f<lciliries in United
including prirn::try tanning salons and facilities such
as hair salon . .; and he;1llh cluhsY' l.\-!o<lem ranning
beds emit nY.:tinly UVA. of W<t\'dengths 320 to 400 nrn
and a srn;11l arnoum ( <Hro-9. 5%} of lJVB of
lengths 290 to 320 nm Js; 2" Tanning proponents
daim thnt tanning hed:> emitting predominamly LTVA
are a safe altemative to sun although
sttJdies have shown tbat UVA be particulnrly
effective at causing photoaging with its dc:.nnis-pen-
etr:.lting and f'kin cancers have bCd1
655
656 Jlomung et al
reported aJter thewpy with psora1en and ultraviolei.
A radiat.ion.
2
u
2
The promotion of indoor t<mning as
a healthful way to aehkve a p rotective tan is con-
tradicted by results of studies demonstraring thar
tans from l1V heds offer little protec-
tion from sunburn,
2
5 equi vale nr to rJ1ar of sun pro-
tection htcror 4
Federal. regulation of rhe tanning industJy is pri-
marily through the Cod e of Federal Hegulations
1040.20 published by the t iS Food and DrugAdmin-
lsrratlon (FDA\ The Code of Federal Reguhltio.os
details requi.re.ments for sunlamp manufacturers on
lamp posting of waming bbels, and
provision of suitable eye The FDA does
not regul;1te amounts of 'CVA and UVB
produced by sunlamps, although it does limit ac-
(Cpwbk amounts of UV or wavdt"ngths 200 to 26o
nm. Guidelines for recommended. tanning bed ex-
doses were issued by the }"DA in 1986. The
guidelines ca.Jkd for a maximum exposure of 0.75
minim::tl erythemul <k)st, (MED) 3 time:> during the
first week of follo\.ved by a gradual increa..o:;e
to maintenance doses of a :mnxim.u:m 4.0 MED de-
livered weekly or biweekly.
21
On the basis of these
guideline::;, mam.Jfacturers develop a rt".conuncn.ded
exposure schedule for each of r.a.nning unir. and
it is a requiremem r.hat the guidelines be posred with
each unit.25 These schedules represent
FDA-recommended maximum exposures for firsr
wt:eks of ranning by exposure time:;
in minutes speci.fic to the tanning unit and patron
skin rimes are recom-
mended for tanning beds with newly replaced
bulbs, nwchines have higher UV out-
put. Specifications for decreased e:x posure during
the ... arly lifespan of a bulb v;uy by m;muf;Kturer.
Adherence to exposure schedules is !e!1. to d1e dls-
cr<:>tion of individtJHl wnning fnciliry oper.1tors and
tanning patrons.
Exhriog reguh1tioo:> do not provide for
national enforcement of exposure adher-
ence by tanning parrons or for moniroring the
amounts of UVA and. UVB emiu.ed. by r..1nniog units.
'fhis was conducted to e.xarrune conuntlllily
of in an attempt to identify the
extent to which were follo\\-ing or exceeding
FDA-recommended. exposure limits and to identify
rhe and amount of radimion USt'rs we.re receiv-
ing.
METHODS
Study design
The study involved a community-based sur.:ey of
tanning facilities and their patrons in North Carolina.
Nol'th Carolina chosen as the n?.'>eflrch site be-
JAM ACAD
OCTCHlH:, 2003
cau'it: it has comprehensive tanning fa.clliry rt:guht-
rions thar .require maintenance of records of tanning
patrons visirs with and dormions of t<mning
exposures. 2" The regulat.ions also mandate training
and cerrificali.on of oper::ttors, di$play of warning
signs. eye protection and. equipment
and regisrration nnd biennial inspections of each
facility rhroughout rhe smw by Nonh Cwolina
Division of Radiation Pro!ect.ion. Penalties for viola-
tion of these regulations can indude monetary
or possible closure.
A conwnience sample of 62 tanning facilities
wt-re invi(ed. to parlidp<lie as 1Xllt of lhcir rego.lnrly
;;cheduled state inspections. The data "i.ve.re gathered
by 1 stare tanning inspector who rwd bt'en
trained 1n ihe study proiocoL Data colleciion
spanned a consecutive 8-month period including
the winrer and spring of 1999. Approxim<lkly 7 or 8
fa<.ilitie.s were invited to participate per month as the
inspector's schedule allowed i.ime for adm.inist.ration
of the survey during inspec:rion visits. The inspector
administered !he survey in aH region::; visired during
statewide inspection rounds to elimiru1te geogGlphic
,'>amphng bias.
Each [;ld.lity and irs fYJtrons w<;.>rf;:! evalumed by
meart'i of a survey instrument that consisted of 12
items assessing tanning facility chara('(erisrks <tnd B
items as..'>essing patron hd1avior. The survey items
pertaini ng to tanning facility characteristics covered
tile facility type (tanning only, hnir S<llOn :and tan-
ning, healrh fitnt:SS cemer, other), r.he number of
years in opemtkm, the number of f.anning units, the
number of operators, the percentage of opemtors
certified, the number of daily custon;er!i, and the
of t.t$ers among ws-
tomers. The inspector answt::red ihese items on the
survey by personally inrerviewing the facility oper-
ator and recording tJ1e answers.
Survey evaluation of patron behaviors was ac-
complished by ex<l minMion of 10 rrmdornly
patron record-; at each facility, although occasionally
fe-wer than 10 r<---cords were reviewt'd per f,Kility
because of ihe inspector's time limitations. Patrons'
records were used to evaluate rhc type of exposure
schedule followt.:..d (i f any), exposure f()j'
the first tanning visit, the history of indoor tanning in
the previous year, the t.ime period for tanning, and
the frequency and length of visits. A sample lisr. of 15
commonly used expusure was compiled
and provided w ans ... vering the S\.trvt:y sec-
tion on t.."Xposure Patrons were consid-
c>red ro L"l<: not following an exposure sch<:,dule if
record.:; ind1c-.1ted that durlng any week of tanning
the exposure times recommenued for
that week of tanning hy npproprhlre
1 AM Ao.n Df.RMATm
VOLI.IMI' 49, NUr-<1\ER 4
Table I. Tanning facility characteristics
No.
In operation> 2 y*
Have tanning units
Have :2:3 tanning operators
Have 2::50% of operators certified
> 30 patron visits per day*
<25% of weekly patrons are first-time users"'
Taoruog
mcility
All type$ onJy
50 8 (16%}
29{59%) 2(25%)
32(64%} 6{75%)
29(58%) s (62.5%}
50 (100%} 8 {100%}
26 (53%) 5 (62.5%)
48{98%) 8{100%}
Homung et al 657
Hair atld Heahb
tanning 1\tness
fa.:Hir;r <:enter Othet
29 (58%) 4(8%) 9(18%)
19 (67.9%j 3(75%) 5(55.6%)
18 (62.1%) 2(50%) 6(66.7%)
14 (48.3%) 3(75%) 7 (77.8%)
29 (100%} 4{100%) 9 (100%)
13 (46.4%) 3(75%) 5 (55.6%)
27 (96A%) 4 (100%) 9(100%)
For these data, n '' 49 for al l facility types (information not available at 1 slte}.
scheduk. The insped or answered the>e items on
the .survey by accessing the >v rillen patron records
<ind <lpprop rlate information.
In addition. UV A and UVB measurements were
t:1ken from e<JCh <1vaih1bk bed in facility. The UV
measurements were obtained \Vith a uv
bn)adb;md rnder (Solar Light, PA)
with UVA and UVB (abo described as a
Solar light sunburning or ultraviok:t intt>nsity
meter). This device allowed analysis of l.JVA and
UVl) outpur io wnning bed. l11e PMi\2100
detector mea,sures UVH output in .MED/h, defining
<In MED as 21QJ/ rn
2
of weighted FVB.
Instrument detectors were placed in the middle of
ea<.:h unit on the lower surf<tce so rhar the
distance from the radiatJ on was the same for
each unit.
Statistical analysis
Data were initially entered into 1 of 3 different
computer in Stara (Collegt:: Swwon, Tex):
(I) tanning data, (2) tanning bed data, and t3)
[XItro.o Jaw. The:->e 3 cont;limd an idemi-
cai facility number variab le between them, allowing
cbt;l Fitul!y, each of the databases was con-
verted to Microsoft Excel for further analysis. De-
scriptive st<ltisrics were pt:tfonnt-d in both the Staw
statistical package and Excel. The disCTete variables
were summarized wirJ1 freq tlencies and percent-
ages. Continuous variables were summarized with
mean. standard t-rror, range.
The Genrnod procedure with Bonferroni
tion of the Si\.S srarisricaJ software (C1ry, NG) wa:=;
used for analysis. Generalized estimating equations
(GEE) used in r.he becll!se rhis
method accounted for the necessary covariance
Wirh seleoion of different link fundions.
ali outcome measures could be analyzed \'Vith the
GEE method. Sites (tanning f<K'ilities) wert:: the
unit of anal.ysis. Clustering and repeated of
beds or p;mon:> wirhin htken into account
in the analysis. Compound symmetry within and
independence between s ites were assumed.
RESULTS
Of (he 62 tMming fadliries ;tsked to p<iJticip;lW,
81% consented to the study. Fifty tanning facilitie:->
wt-re surveyed, <H"'ld a tot<ll of 483 patron records
were re\riewed. The facilities were located through-
om the srare, incltJCHng the are;ts amnnd
A<>ht"ville, Charlotte, Winston-Salem, Greensboro,
Durham, Raleigh, Goldsboro, and Fihy-
cighr percent of the participating facilities were a.
combination of hair and tanning S;llon:->, 16/il
were tanning only' 8-i> were health and ih-
ness centers, <tnd 18% were other (eg,
grocery storts, sportswear anc! clothing For
comparison. the distriburlon of facility
tyT)es in N01th Carolina is <j.(iry,J hair and tanning
salons, 26% tanning-only S<llons. B% lle;llth fit-
ness centers, and 20%l other (personal communica-
(ion. Amy Sawyer, North <:arolinn Division <)f Radi-
ation Protection). Of the tot<il surveyed,
59'% had been in business for more than 2 years,
had 3 or more tanning units, and 58(hl or more
operaror:5 <Tahle Jl. of 50 facilities
indicated that more than 75%, of their tanning bed
oper<ltors were use found w
be more than 30 patrons per day at 53%1 of the
fndHrie:>, and of tht- th<lt less
than 25% of weekly customers were f1rst-time tan-
ners. A range of 1 to 3 differt:n.t
were avai.labie for use at t.h..:: facilities (mean, 13
schedule-'>; :5wnch1rd error. 0.08).
In evaluation of patron data (n = 48:1), it '-Yas
found th<lt 95% of patrons were the rec-
ommended times and therefore did not f()llow the
wnning bed exposure schedules ourlined by
FDA (Table H). Of the 483 patrons, 33% were start-
ing their fir:5t t;mn.ing session <lt or above exposurt'
times recommended k).r patrons in the mainttnance
phase of tanning (ccm-esponding to ;;;;:,] ,0 MED_).
658 Jlomung et al
Table ll. Tanning patron behaviors
No.
Following exposure schedul e
{n =483)
1\feao
JAM ACAD
OCTCHlH:, 2003
Standard <:t'ror Range
No 460 (95%} No. of min on first visit 483 14.25 0.27 3-30
Yes 23 (5%)
Starting at maximum exposure Tanning period (wk) 477 632 028 0.50-52
time (n = 483)
No 326 (67%)
Yes 157 {33%) No. of minlwk 483 43.00 U2 513S
Previous tanning (n = 231)
No 139 (60%) No. of visits/wk 482 2.37 0.06 0.25-7
Yes 92 (40%}
Tabl e m. UVA and UVB measurements
UVA(W/m
2
)
UVB (W/mz.}, erythemally
weighted
136 192.1
171 0.35
181.1 17.7-674.0
0.33 0.12-0.82
average length f(Jr tanning on the first. visit
14.2'5 (range, 3-30 minutes), The com-
pil.ation of 15 common exposure schedules li-;ted a
:>ugge:>r.ed r<1nge of 2- to 1 <:-rnimu:e sessions (<lver-
age, 5.76 minutes) for the week of tanning with
gr<Klual over ;J or longer p<:'riod lO
a r:mge of 8- to 30-minute m.aintenance scs.sions
(;lVerage, 20.'51 minure.s\ 'I11e average period of
tanning for each patron \vas 6.3 w eeks, and patrons
spent appmxim<ltdy 43 minutes in the wnning bed
each week (range, 5-135 minutes) during an average
of 2.4 sessions week (wngt-. 0. 25-7
Forty percent of had tanning histories ftom
tbe previous year and were repeat use!'$.
The GEE method was u:;ed to compare patron
behavior::; tanning faciliry type, ye.ars in op-
t:ration, numbers of tanning units, numbers of op-
erators. and nurnbt:r of d<1ily customers. The average
nmnber of minutes of tanning per week was found
to be .slgnific<H)tly (p < .005) between pri-
mary tanning facilities (34, 8 minutes) and facilities
categorized other (50.33 mim.ttes). In compa!i-
of prima1y tanning facilities with the combined
group (>fall orher E1eiliry types (hair salon . .:;, he- . llth
fitnes!:', and othe!;). there was still a dif-
ference: :)1.8 minutes compartd with 44.76 minure$
(P = .009} No other significant pairwise compari-
:><ms found.
As for UV output, the beds on average emitted a
mean UVA of 192.1 \V/ m
2
(rtmge, 17.7-674.0 W.!m
2
)
and UVB of 6.01 MED/h (range, 2.11-14.00 MED/h)
(L1ble III). UVB convened from
units of MED/11 to W /m
2
on the basis of rhe defini-
tion of 3 MED as measured with the PMA2100 de-
rector. The measun::d average tTVB outpur of 6.01
MED! h was equivak:nt to 0 35 W /m
2
of eryrhemally
weighted UVB (range. 0.12-0.8:2 The (J.EE
method was used f or ('Omparisons of UVA and UVB
measurements against t:mning facility type, years in
operation, number of units, number of op-
erators. and number of Jaily customers, but no sig-
nificant (P < .005) comparisons were
found.
DISCUSSION
It is alarmingly thal
posure schedults are not being followed in the com-
munity. In this swdy. 95% of p<liron..:; were
ing the times recommended by exposure schedules.
We found lhat the i.anning Llcilities did h;we expo-
-'>ure schedules on site (rnean, 1.:1 schedules), but the
fY.H.rons records indknt.ed thtlt rhe schedules
not being followed. We also observed that as marry
as one third of p;ltrons were ;-:;t;Jrting their first tan-
ning visit at or above the maximum exposure limit
for maintenance wnning. This rr;lC!.ice goes a.guinsr
the cunent recomr.nendatkms for a gmdual increase
in with limited do.st:'S in thE first
of tanning. These in thei.r initial week of
wnning more li.kely m h.tve untanned skin and
to be more susceptible to UV damage. These patrons
also receiving maximum doses reserved for
maintenance tanning.
Tanning expo.sure
by other methods. but none involving direct analysis
of patrons' records <1$ in (>W' study. In a 2000 sr.udy of
frequency and exposure in 60 San Diego t.<m-
ning facilities, as pownrial t:tl:>-
tomers asked operators about the allowable fre-
quency and duration of tanning. The
fmmd that only 6.8'Yt1 of tanning operators were
comp!ianr with FDA frequency
1 AM Ao.n Df.RMATm
VOLI.IMI' 49, NUr-<1\ER 4
and operators dalmed they would limit patrons
tanning to less than 30 minutes. 2M Our in(li-
cated trwt most parrons are exceeding recom-
mended tlme.s of exposure for inilla! and sub.sequent
wnning sessions. W<:., reporf a m<.Kh higher of
with FDA-recommended time5 than
that cited by Kwon et a1,2;; 'Nhich may reflect rhe
claims of h.1ture enforcemen:. by
operators versus true patron use patterns. The study
by Kwon et al also broadly deii.ned complianze with
<::xposur<:: a;:; being a duration of Jess than
30 minur.es. NoncomplimKe with recommended tan-
ning times also W<ls reported in n survey of 20 New
York tanning bed operators. The a:verage l.ength of
wnning r.he daimed they would was
43 ;md some opt':rators 'l.vould allow up to
an hour of exposurt.
2
9 A survey of high school
:>t.udems who used wnning beds showed Ul<lf 57%
claimed to have had tanning .session.s of 30 minutes
or lnadequatt' limits of length and fre-
quency of tanning were found in a survey of
tanning facility operators in :\.rkan..S<ls:\
1
and by an
undercover ltwe::;tigation of tanning facilities in
Given the findings of this study and
oThers and rht' of "unHmitt>d ranningr.
publicized hy tanning it dear that
large numbers of r.anning bed may bt ex-
ceeding limits.
These of frequent indoor tanning
pmtems without lim.i cs <ll'' of concern in
light of the popularity nf A survey in New
York showed rhat 21.5'% of 1720 persons had used
beds, the highest rate occun-ing among
young women.53 One st11dy showed that 34.-f.; of
I 008 Minnesow (t't>nagers lu1d ever us<:'<l tanning
and another study showed that lROA of 210
Tex,;s teens had used tanning beds within the last 6
m()mhs.3J High u::;e is of concern
because cumulative UV exposure occurs he-
fort?. 18 yt:ars of age5s in most states
parental permission is not required for Imming hed
U$t', Abo troubling is that mo::;t indoor ttnners have
skin types I through III, and patrons with skin types
.I and H may panicubrly at risk of poor tanning,
burning, <1nd skin C<l nc.t:r.-><> Finally, tanning ht-d
overexposure has been found to cause molecular
damage such as p'55 dimer fonnation in kerntino-
cytes r.aken from votunteer subjects to tan-
ning be1.b at. doses <md fre<iuencie;:; more intense
t!un that recommended by the
11)e trend
reported herein of a .sizable portjon of ta.nning pa-
trons exceeding the recornmended li.mirs is dearly
concerning.
Most of the salons in this study been in
for :;ewral yeMs and 1-<.lll sever-al ranning
Homung et al 659
beds more than 30 per &1.y.
.findings imply these use patr.erns may have indudeu
many patrons over <ln exlendt:d time
ciaHy hecause more than of patrons were n::peat
tanners \-..,i.th a history of tanning in r.he previou:.;
year. Notably, these. exposure patterns were docu-
mented from salons in \Vhich rno;:;r operators were
cerrified according to :>tate regubtions. of
pasl studies have indicated that tanning bed opera-
tors as a group are poorly inforrned about the risk<.
of indoor tanning. A survey of r:anning operators in
.M:ichigan showed rhat 6;:>%1 of Dperators did not
believe rhar t;mning beds C<ln An-
other study .showed that tanning patrons in New
York w<;>re told by 65'% of operators thm they could
not get a sunburn from tanning beds, and of
operators told parron ..'5 they could not. ger skin cancer
from tanning beds.
2
'' A srudy in North Carolina
showed that operators '\.Vere un:n.\'are ot common
photosensitizing drugs. and some even allowed chil-
dren younger than 10 years old to tan.'\" Because
operators play such an integral role in controlling
tanning b<.>d use, rheir collective lack of knowledge
and questionable- history of enforcing regulations
highlighr tanning af:i <t public
danger
UV output i.n standard ranning facility beds is very
high given that, for UVA output
in this study was 1')2 W / m.l when
sok1r noon output in W<Jshington. DC. was 18
TI1e avewge weighted UVB
output of 0.35 W/ nrl also is very high sum-
mer sobr noon ervthemallv weighred. tJVB in \"Vash-
ington, DC was ().1R 6ther measun:.mems
t)f .summt-r sohlr t'rytht'f'O<Illy '-Veighted l.NB fmm
various locations in the l Jnlted have a maxi-
mum of approximately 0.25 'X'!mz_:
1
Om measure-
ments of an average of 0.35 and a maximum
of O.Sl W/ m
2
erythernal!y weighted UVB indicate
that tanning bed patrons are receiving higher doses
of l :"VB than they would from summer sun expo-
Sl.lre. FUithermore, a dO$\:.' of 0 35 W /m
2
to a UV index of H . Our of
0.82 W / rn
2
erythemally weighted 1JVB corresponds
to a tN index of 33:''
0
These uv indexes are abnn-
ingly high and indicate that patrons with fair skin
can bum their skin VC'ry quiddy. Because. however,
the PMA2100 detector does not perform .spectral
analysis. we could not determine the percentage
these high amounrs of VVB irradinnce comribur<:' ro
total UV emitted from tanning beds. The 1JVA.Ievels
we measured were comparabk wiTh those in report:>
of UVA range'i of 5ri to 21t
and 50 to 190
W/ rn
2
:l
1
; however, our upper range of 674 \V/m
1
was
higher rhan h<1:> been reporwd. Our
660 Jlomung et al
higher range for UVA levds and the wide range..'> we
found in hoth the UVA and l!VB me-.L'Urements
could be due to differences in specific ranning bed
models Hnd varying ages of the bulbs.
Primary tanning facili ties were found ro have sig-
,.:;hortt::r patron wnning timet> rhan rht:. orher
bcility typ<':S in the pairwise comparison;:;. This find-
ing may indicate salon owner.s in htLsinesse:s dedi-
cated to tanning may be more conscientious of en-
forcing patron adherence to e .. '{posure limits, unlike
fHt'iliiies wlwn.' operators m<1y be with
otlwr of business. J[ is poss ible thm primary
tanning salons rnay prove to be rh0. bt."St type of
business arrangement for ensuring p:u.ron be-
havior. Howev-er, our sample size of tanning-only
facilities wm; small (n = 8), and the. proportion of
tanning-only facihties in rhi:; study was lower than
the in Norrh Caroliru1 06% v::;
269"<), which may limit of this finding.
A of study was that 1he facilities
were not randomly cho$e!l but were included as
time allowed on the state inspecro.r's rounds. This
method rnay .have;:' resulttxl in selection bias th::tt
could the dar.a. Our sample may h<lve
nwre hair and tanning combination facilities in place
of tanning-only faciliiies given the pre>'31ence statis-
tics for facility t:ypes in North Carolina, but
the disr.ribution pf the other fa(ility rypes studied
;:vas rdlective or rhe distribution. Geo-
gmphical bias in fadlity W<l='> unlikely be-
the fadlities were distributed throughoul the
statt:. Strengths of the study induded consistency in
data collection and objectivity of w1itten records for
determining patron behavior as opposed to infomu-
r.ion or by or operaton;.
lt may not w generalize i.hest results
to other North Carolina has thorough
regulations for tl-aining and certification,
and only 17 other st.ates have regulatory programs
for tanning salon oper<1rors r.lun differ widely in size
and srope.
12
We predkt that the results may be
:>imibr or evt:n wor:->e in m.ar.es wirh !itrk or no swte
regulations, certified North Carolina opera-
tor;; may more kn<i\vledgeable about tanning bed
rlsb and may be rnore llkdy to e nforce exposure
scheduk' adherence .. However, adherence to expo-
les i!:' nor puJi of tilt> North C.lro!ina sr.are
regubti(lDS. Evtn wirh ;1 r..horough state regulation
program, North Ctrolina operator compliance wii:h
tanning bed regulati ons is poor:e To obtain more
generalizable data, future studies conducted with
objective measures of exposure time could explore
expo!:;ure schedtJle comptiam:e in swtes with vary-
ing Jegrt::es of rt:gnlarion.
JAM ACAD
OCTCHlH:. 2003
In summ.ary, we report that tanning patrons are
uniformly nor. following the schedules for tanning
recommt!nded by the FDA These findings indicate a
need for future educ;ltional interventions to increase'
fhe knowiedge of both tanning patrons and facility
operotors for compli<mce with recommended e.xpo-
sure guidelines. is also a need to further es-
rablish enforcement of rht'se safery recommenda-
tions, as ''-'ith policy changes to exposure
schedule adhen::nce manr..huory in combination with.
jnspections of tanning L1cilities to ensure compli-
ance. The .FDA is considering updating indud-
ing exposure scheduk:s into the Code of Ft:deral
Regulations 1040.20 so thaf exposure schedule ad-
Jterence would be an enf(m:eabk regulation as op-
posed to a guidel!ne:H This change \Vould be wdl
advised given the poor rakfi
herein. ln the future, tracking patrons' cumulative
exf)Q<mres may be hdpful t<x ckkrmining total
amounts of ranning bed exposures that patrons are
receiving nationwick and in confikkring establish-
ment of cumularive exposure li.rnirs. A combinmion
of educational interventions with updated and man-
datory enforced reguhr.ions is hkdy best ap-
proach to ensuring hettt::r proteLilon of tanning bed
patrons from oven:'xposun:'.
Wt: 11Y.mk A:nr Sawyer, North C<lrolina Div!!\iOn of
Radiation Pro!ection; Anne Dean, Nonh Carolin;J.
Jn;;peuor, Division of Radiation and A!ptsh
Patel, Nor<.bwestern University i'vkdicai School for
thf:!ir hdp with daw and organization of the
study.
REFERENCES
1. Gloster HM Jr, Brodland DG. The epidemiology of s.kin cancer.
Dermatol Surg 1996;22:21726.
2. Rigel DS, Friedman RJ, Kopf AW. The itKidEC>nce of malignant
melanoma in the Unit ed States: issues as we approach the 21st
century. JAm Acad Dermatol1996;34:839-47.
3. Centers for Disease Contrc! and Prevention. Injuries associated
with ult raviolet tanning devices: Wisconsin. MMWR Morb Mor-
tal Wkly Rep 1989;38:3335.
4. Walters BL. Kelley TM Commercial tanning facilities: a new
source of eye injurf. Am J Em erg Med 1987;5:386-9.
S. Council on Scientific Affairs. Harmful effects of ultraviolet radia-
t ion. JAMA 1 989;262:380-4.
6. Epstein JH. Suman salons and rhe American skin. South Med J
1981;74:837-40.
7. Woman dies from bums. Winston-Salem Joumal1989 May 28.
8. lavker RM. Gerberick GF, Veres D, lr-Nin CJ, Kaidbey KH. Cumu-
lative effects from repeated exposures to suberythemal doses of
UVB and UVA in human skin. JAm Acad Dermato11995;32:53-
62.
9. Lov,re NJ, Meyers DP, Wieder JM, Luftman D, Borget T, Lehman
MD, et a!. Low doses of repetitive ultraviolet A induce morpho-
IQ9ic changes in huma11 skin. J lnve>t Dermatol 1995;105;739
43.
10, Ham \o\IT Jr, Ruffolo JJ Jr. MueHer HA, Guerry D 3rd. The nature of
retinal radiation damage: dependence on wavelength, power
level and exposure time. Vision Res 1980:20:11 0511.
1 AM Ao.n Df.RMATm
VOLI.IMI' 49, NUr-<1\ER 4
11. HoHows f, Moran D. Cataract: tne ultraviolet risk factor. lancet
1931;2:1249-50.
12. Autier P. DoreJF.Lejeune F, l<oefmel Kf, HiUeP,et at
malignant melanoma and exposure to sunlamps or
sunbeds: an EORTC multicenter case-control st udy in Belgium,
France and Germany. EORTC Melanoma Cooperative Group. 1m
J Cancer 1994;58:809--i 3.
13. Walter SD, Marrett lD, from t, Hertzman C, Shannon !-IS, Roy P.
The association of cutaneous malignant melanoma with the use
of sunbeds and sunlamps. Am J E.pidemiol 1990;131 :232-43.
14. Westerdahl J, Olsson H, Masback A, lngvat c_ Jonsson N, Brandt
L. et al. Use of sun beds or sunlamps and malignant melanoma in
southern Sweden. Am J Epid{.!miol 1994; 140:691-9.
15. Westerdahl J, !ngvar C, Masback A, Jonsson N, Olsson H. Risk of
malignant melanoma in relation to use of sunbeds:
further evidence for UV A carcinogenidty. Br J Cancer 2000;82:
1593-9.
16. Dinehart SM, DodgeR, Stanley WE, Franks HH, Pollact<SV. Basal
cell carcinoma treated with Mohs surgety: a comparison of 54
younger P<ltients with 1050 older J Derfl13tol Sorg On
col 1992;18:560-6.
17. Karagas MR. Stannard VA, Mott LA. Slattery MJ, Spencer SK,
Weinstock MA. Use of tanning devices and risk of basal cell and
squamous cell skin cancers. J Natl Cancer lnst 2001;94:22+6.
18. Looking Fit Tanning Fact Book 200212003. Phoenix: Virgo Pub-
fishing; 2002.
19. MiUer SA, Hamilton SL, Wester lJG, Cyr WH. An analysis of WA
emissions from suniam ps and the potential impcJrtance for mel-
anoma. ?hotochem Photobiol1998;68:63 70.
20. Spencer JM,Amonette R. Tanning bedsanct skin cancer: artfficial
sun+ Oid Sol= real risk. Cl in De rmatoi199S;16:487-501.
21. Stern Nichols KT, Vakeva LH. Malignant melanoma in pa-
tients treated for psoriasis with methoxsalen (psoralen; and ul-
traviolet A radiation (PUVA}: the PVVA Follow-\Jp Study. N Engl
J Med 1997;336:1041-5.
12. Stern RS, Liebman E.J. Vakeva L Oral psoraien and
light (PUVA) of psoriasis and persistent risk of non-
melanoma skin cancer: PUVA FoHow-up Study. 1 Natl Cancer lnst
1998;90: 1278-84.
23. Gange RW, Blackett AD, Matzinger EA, Sutherland BMt Kochevar
!E. Comparative protection efficiency of UVA and UVB-indoced
tans against erythema and formation of endonudease-sensittve
sites in DNA by UVB in human skin. J Invest Dennato11985;85:
3624,
24. Dvgun MS, Johnson BE, Paterson CR. Tanning. protection
against sunburn and vitamin D formation with a W-A .. sun
bed." Br J Dermatol1982;107:275-84.
2 5. Department of Health and Human Services (US), Food and Drug
Administration. Sunlamp products: performance standard; final
rule {21 CFR 1040). Fed Reg 1985;50:36548-52.
26. Department of Health and Human Services (US}, Food and Drug
Administration. Letter from the Director, Office of Compliance,
Center for Devices and Radiological Health, to all manufactur-
ers, importers, and potentia: manufacturers of sunlamp prod-
Homung et al 661
ucts. Subject: poticy on maximum timer interval and exposure
schedule for sunlamp product s, Aug 1986.
27. State of North Carolina: Tanning facilities. Title-151\ NCAC Chap-
tern, Se<.tion 1400. Jan 4, 1990.
28. I< won HT, Mayer JA, Walker KK YuH, Lewis EC. Belch GE. Promo
tion of frequent tanning sessions by indoor tanning facilities:
two studies. J Am Acac! Dermatoi2002;46:70CI-5.
29. Fairdilld AL_ Gemson DH. S.afery information provided to cus-
tomers of New York City suntanning salons. Am J Prev Med
1992;8:381-3.
30. Oliphant JA. Forster JL, McBride CM. The use of commercial tan-
ning fad!ities by suburban Minnesota adolescents. Am J Public
Health 1994;84:476-8.
31. BroyneEI-Rapp F, Dorsey SB, Guin JO. Tne tanning sa!oo: an area
survey of equipment. procedures, and practices. JAm Acad Der-
matol1988;18:i030-8.
32. Beyth R, Hunnicutt M, Alguire PC.
of proprietors' knowledge of risks and precautions. J Am Acad
33. Li!lq uist PP, Baptiste MS, Witzigman MA, Nasca PC. A popula-
tion-based survey of sun lamp and tanning parlor use in New
York State, l990.J Am Acad Dermatol 1994;31:5102.
34. lucd A, Citro HW, Wilson l. Assessment of knowledge of mela-
noma risk factors, prevention, and detection principles in Texas
teenagers. J Surg Res 2001 ;97:179-83.
35. Stem RS, Weinstein MC, Baker SG. Risk reduct!on for nonmela-
noma sltin cancer with childhood >tmscreen use. Arch Dermatol
1986;122:537-45.
36. Diffey BL Use of UV-A sunbeds for cosmetic tanning. Br J Det-
mato[ 1986;115:67-76.
37. Whitmore SE, Morison Wl, Potren CS, Chadwick C. Tanning sa
Jon exposure and mole<ular J Am Acad Dermato!
2001;44:775-80.
38. Fleischer AS Jr, Fleischer 1\B. North Carolina tanning operators:
hazard on the horizon? J Am Acad Defmatol1992;27:199 203.
39. United States Department of Agriculture, UVB Monitodng and
Research Program: 2002. Available from: URL: http://uvb.nrel.
colostate.edo/uvbjnterc.omparison.
40. Lim HW, Cooper K The health impact oho!arradiarion and pre-
veotiOri report of the Environmerlt Council, American
Academy of Dermatology. JAm Acad Dermatol1999;41 :8199.
4 L McGinley J, Martin CJ, MacKie RM. Sunbeds in current U5e in
Scotland: a survey of their output and of ose. Br J Der-
matol1998;139:428-38.
42. The stare of regulations. Tanning Trends Magazine 2001;No-
vember.
43. Fleischer AB Jr, L<:e WJ, Adams DP, ZanoHi MD. Tanning facility
compliance with state and federal regulations in North Carolina:
a poorperformance. J Am Acad Dermatol1993;28:2127.
44. Department of Health and Human Services (US), food and Drug
Administration. Medical devices; >unlamp products perfor-
mance standard; request for comments and information, pro-
posed rule (21 Cffll 020). Fed Reg 1999;64:628890.
it
I
SEP. 25. 201)9 12: 16?M WO MAI N LIBRARY NO. 5421 ?. 2/i
I
Promotion of freqt1ent tanning sessions by
indoot tanning facilities: Two studies
Harry T. Kwon, MPH, GH5," Joni A. PhD,"' Kristlna K. 'W'iillcei:, M.PH,n He.oryl'U,
Lewis, MPI:l,il and C-reorge B. :Belch, PhDb San Diego, california
Backgroun4: 1pdoor mnnl.ng mar incrl!ase the o.Jf melanoma and other health problems. Frequent
users of lndoor tanning fad.lltie.s may b<! nt panlcularbr high dslt
Objecf.ive: In study l Que purpose was to assess the prt':lv-a.lenc:e ;;.nd mttur<! of indoor tanning
advt..rtisemcnta; in study 2 we alrned to assess taru1lng .fuclliry cornp1tance to t'ecommencled exposure
schedules .
.:dlefJJot:!sJ ro study 1, ta.ntlinf!, aclvertiscmcru:, over a 4-mondl period from U San Councy
newspapers were mooftot-ed. Irl study 2, we. assessed com(,)li;mce v.rlr.h t'CCOinmended exporurc l.ichedoles
via a telephone Jnterview of 60 San Diego County tanning facilities.
Results: Approximately 75% of the: indoor "tannins advertlsemenrs promoted unlimited tllnnlng. Only 5%
of facilities were in compllance with recommended tanning achedules, and 10096 offured "unlimired"
tanning pacl.-Rges.
C<mdu.sions. These ilncllngs sug!Je.st that the Indoor raMlng Industry, th.rovgh pticlog incentives that
allow frequent rnay bi! promoting overexposure to UVR. Stronger leglslntion is needed to address
thls l.ssue. 0 A.'TI Acnd Dermatol 2002;46:7005.)
W
ith an expectef.l one million new cases per
year) skin cancet' is the most common of all
cancers and accounts for nearly half of all
cnnce
the 1970s, the incidence 1'2.t:e of
mel.atloma. has Increased siSnlfkantly to about 4%
annually a.t:ld wlll account for more than 9000 deaths
this yenr.l The iJnk berwee.n. e1Cposure to solar
vir.tlet radiation (UVR) Rnd skJ.n cancer Js well accept-
ed by the scientlflc commun1ty,2 Ald1ough the
stttdle..q assessing the relationship between indoot
rannl.ng (le, exposure to artltlclat UVR) and
melanoma have ytelded .mix.ed resultS, t:here now are
nt least 7 srudles that show a sig.alflc.am, elevated
clslc.M Most of 6tudies documented some .fo.rm
o.f a dose-response relationshlp.S Modem ta.nrung
f rom thG Gtnduate .School of Pobllt and me Department of
Mi.lrkctlng,b San Di ego UtlfVtltSity,
Funding; NoM.
Conlll<:t of None.
J\ct:eptl!d May 31,200L
Reprint requezts: Jonl A, Mayer, PhD; Graduate Scl'lool of Public
Health- Hardy Tower 1 19,San Dlago State Diego,
CA 92 i 82-4162.
Copyright 'I> 2002 by tho American AcndciTl)' of Dermawlogy, Inc.
0190962212002/$35.00 + 0 16/T/119560
dol;l0.1067/mjd..200.:2.11!1560'
700
beds use flu.orescem. Ughr: bulbs thai:' emit mostly
WA rays and delivE!r up to 3 tllnes the UVA dose
delfvered by natural sunllshc.5
The demand fo1 rl1tllled !ikln has yielded an expo
nentla.l growth of tannltlg fadlities itt recent years. It
ls estimated that there a4e 28 m.lllion users of mnning
facilities and 50,000 tanning fucillries nadonwJde,
productng a billion dollar !n Sun Dlego
County alone, there more than 100 ranning
irJes.lccated wlthi.n county An estimated 5% oi
the US population are regularuser:!l of mo.nmg
Because of the grO"t\'th of the tannjng fudlicy
industr}r, the 'Food and Drug .A.dmini.stration (FDA)
has esrnblished guideltnes that: lltnit amountS ofUVR
to a person. Currently, the recommended exposure
schedule 1s ''no more than 0.75 mlnin'lal
(MED) 3 times first week," gradually
trlcreasi:og t he thereafter.7 The Federal
'!lade Commission lnrestigatea deceptive and false
01dvertislrlg of tanning devices, indud!l'lg claims that
indoor tan.ning is safc.s Approximate!}' one half of
lhe states ha.ve passed t2lliling fudlity regulati.ons.7
WH. CDRH evh..rarkm 'or sunlamp prnducts.ln:
Proceedings of the Cel'ltets for Disease CoMtrol and
c;onfurence, San Diego, Califr 10. 1999.
J AM N:..:oD 0!:\lM."":!OL
VoLUMt: 46. NUMaEP. S
caUfPrnla's !lila.nte 'Ianning Facility Act of 1968 suu:es
that mntling facilltles must (1) give each customer a
wrlcten statement warning them about specific risks
(eg, not using eye protection may c-ause eye damagl!,
repeated exposure may cause skin cnnce_;:); (2) post
v1arning signs related to U\'R; (3) not da.im t.":lat
using a truming device is safe; (4) have sumdently
trained operators pt:esentl (5) provide each
tamer with sanitized protective eyewenr nnd mn.n
dace use of the eyewear; (6) each customer
how to use the properly; (1) use an accurate
durlng each session; (B) limit each customer ro
the manufacturer's maxinl.Ltm
sure time; (9) obtain signed iillnrmed consem fi:om
each customer acknowledgJ.ng uncler.m.mding of the
warnings; (10) obtnin signed paremal con.sem for
customers aged 14 to 18 years1 atl.d (11) require that
cnsmmern younger tha."l J.4 yeam be accompanied by
a p11rent or legal guar:d.ian)O
In v. previous $tu.dy .recently published in this
Joutnal, our roseru.'Ch gtoup found that 94.4% of 54
indoor taoniflg fudlitles l.n San Diego Councy were
allowfug a sessio.o per 9ay the first week of tannUig.'H
.Dunng that srudYi tlle investlgntors JnfoonuHy encoun
tered promodooal {ocendves that provided ut1nllmit-
ed'1 tanning for a .flat monthly rate. Subsequently, we
conducted the two srudies reported in thl." artlcle
focus spec.lflclilly 0.11 the il.lsue of promoting frequent
truming sassions. ln study l, w (! Sy3temat:lc:;!lly monl
toted newspapers in Sw.1 Diego County, Californ!S., to
nssess the rate of "unlimitect "tann.iog ads. '.lb our
knowledge, this was tl'je first study to evaluate: promo
tio.rutl strategies for soliO.ting indoor QU1nlng &.d.Uty
C:U$t'.Omers. 1'.n srucly2, \Ve conducted a. prutinl
tlon of our fucility compliance study,ll with
emphasiS o%1 d1e numbet ofsessions allowed by oper-
ators during a customer's flrst week and rhe mte of
"uoli . .<nited'
1
tanning fee pl:!ckages .
.METHODS
Stu.dy 1
Study 1 c;on.s!:;u;d of a sy,stematic evalUf.\tion of
promotiooa.I ta.nn.ing advertisements ln local news-
pupe<..,rs. The sample indu.ded 24 newspapers
representing a variety of readerships in San. Diego
Cou:ncy: 'The publlcadons were selected from the vw:-
lous geographic regions of San Diego County and
t:onsisted of daily collegiate
1
comrm.1n:Wfj
and emertainmem newspapers.
The foJ!orvl.ng operational defmltlons were used
co quantlf}' the races of advertisements. "'nlnning
-adverr;tse{llent" Wa!i defmed or
reference locaced within a nev-:spa.pcr tlmr.
the word "tanning" a!!d referred 1:0 a service provig
ed by the bwilness represented 1n advertise
NO. 54 2 i P. 3/7
Kwost et al 701
s:nem, "Unlimited tanning advenisement" was
dcl:inep any advertisement that .fulfilled the den
nltian above and included (.}]e foUowL11g terms Ol'
offers: unlimited wnning, no limit tanning,
packages ''Vir:houc a specifled period of time en re.n.
der services, with 5 or more se-'Jsloru; with-
in one wr:dt, monthly t!Ulllingpadtages, or if time
period to render tanning services ms not spcdfied
Additional d1a.tactetlstlc.!! recorded for the
n1llg adverdsemenr included dare primed, source of
advertiSement, type of pdnred media, location of
advertisement (sectlon)j classifl.clttiOn of unHmited
c:anntn.g, u.nd cost of service. In add.itloo, each aclver
tlsement was examined to see whetllef ir was in
accorcbnce with Ca.lifomf-a's Fi!tmce Tartnlng FncUlty
Act of 1988, wblch prohibits r:he distribution of pto-
rnotianfll .material claiming t ha( use of a tanlli.ng
device (tanning bed) was safe or free from rJ.sk.lO
Twency-four newspapers were examlnt!:d over a 4-
monrh period rlw.mg rhe wtnter/eady spring season
of 19992000 . .Al:talnment ai newspap<!rs was accom-
plished ln. 3 ways: a.rdllval retrieval at loct:tllibmries;
issue piclced up at drop-o.tfloca.tlonsi and, If app"llca-
blc, visiting publfshers tO (!.:.tilmine When
mnniog advertisements were found, they were pho
tocopled or exdsed, labeled wlrh tt record
tion nt.unbcr, and catalogued OntO a data rccoro U.n.
Data were entered into the Statistical Paclalge fat
the Soclill Sctences (SJ?SS); tht:: is:.;ue of the newspa
per was the ll.O.it of analysts. De.scrlptJve dat:L were
cal.cuhn:ed foL all variables. ASsessments o the prcva
lence of ta.nnlng i\dvertl.semema ln newspapers were
made b}r e:;,:amining the percentage of the .ISsues that
cantaioed. an adventsement, Of these -advertise
mems, the percentage promoting uoJI.lnlted tanning
was computed. A teSt of <l$5ociatJ.on between tanning
a.dverUsemear. and type of newspaper was conduct
ed with a chi-square 1est.
Sll.ldy 2
Study 2 used a crosssectlon:d design consisting of
telephone interviews of ranning facilir<f operai:O!"!$. ill.
Sun PI ego County. The .sample cons!Bted of 60
facilities in San Dtego County. A tanning fadlirt was
defined as any location, place, area., structure, or busi
ness that provided persnn.s access to any tanning
device (Califcro.ia. St1mne of 1988
1
Cl19pcec 23, Se.ction
22702, Pan A) .to A list of tlmfliog fucilicies in San Dtego
Counl'y by means of a document search
tluuugh Paci.fic Ee.U Yellow Page-5 by the lmernet
through d1e St::"...rch engines of 1:he Wide W.c:b.
The search term foe bmb
paper c.Urecwnes WJi5 ''tanning anq
selected w'ere San :Diego, SM
codes of 619,
SEP. 25. 20 09 12: f?PM WO MAI N LIBRARY
702 Kwon et al
I : +. -_-_ __ -__ - I
15 _j(__ --
Q ..
I
105 .- -- -
. _ ., . .... # .. .
_ ......... . .
0 +-. ----,----...,.--.......------!
Month
...,_.._ GGnernl
Tanning
Advertisement
Unlillli!Gd
Ianning
AdVGrt!liSn\0111
:fig' 1. Frequency of UiJJU\l.rlg advertl..semcnl'.!l oveer 1
monihs.
included any fadllcy that was in business and had at
least one ope.mble ta.nn!.ng bed. Random seleccton was
for tanning facllliies d1at were pnrr of a chain (> 1
fadl!o/ with the same business ruuue). One fadlit}' rep-
resentlO!i each chuln vaa selected.
The principal vru:Jables in smdy 2 were
mnnl.ng facUity complla!'1.r.e with recommended
e.'\')?OSI.l!e schedule guiclellne.!l and prevalence of tan-
nlt!g session pacll:uges and pdclng 5crucn1re.'i. Data
were Clillecced in March 2000 by telephone by a 24
year-old male c:onfederace (H. 'f. K) who posed as a
prospecdve customer. coufeder.ate his
1\J:get questions l)y irulicating he had fa.l.c s!cln and
was pJannin..g to vacation in Acapulco in a couple of
weeks .He then asl\ed the opetator about (1) dte
operator's personal re:comme.ndadon for the most
number of times he should tan the .tlm week, (2) the
dlll'1lt1on per sesstou
1
(3) the kinds of packages
offered by the facl.llry, and (4) whed1er rhe .fudllry
offered uunllmlted" truul.lng. Facl.I!Ues were consld-
el.'ed compliant if the opemwr.r; responses wcJ:e
''i\1thln rhe 1-"D.N.s recommended exposure guidelines
on the: frequency of sessl.ons.7 For the duration of
each session, the tecommendatlon is sraced 1.n
terms of .MED racher thrul minutes. Consequendy, ro
conduct the assessment of compliance wil:h dura-
tion, we adopted the lirrUt used ln o. recommeocJa-
tion of the. Council on Scientific American
MediC'al.A.ssociattonZ; we coded ma2cim.um durations
of 30 minutes or Jess as compliant.
'lb assess reliability. all ffl.cillties were interviewed a
S.::!COnd time by a dJferenc lntervie..,re.r. This inter
vi.ewet< was a 25-)'earold male graduate: St'.Jdem. A
modllled script m1d a subser of rhe i!lltial questions
were used. To llS5e'>S further rellabl.li-
ty, the first name of the cannlngfitcllity operaror from
the pntrulry and intervieW Vv'aS
and matched w.hen appllcablc. '8oth. studies were.
NO. 5421 P
U7
t { f
) AM AO.ll OGI\.1\AICt
2002
l'eviewed by and rec.el.ved 11.pprovcl from the
Com;ni.ttee on Protection of Huma..'l Subjects at San
State
I'he SPSS was used for aU statlseical ancly!!es.
Descriptive stati.sdcs wet:e: c:ornputed for all 'Wriables.
}l'requencies were calculated fur categoctcnl varhtblos,
Cl)l-squa.re tests l1Sed to rest the association
bct.\'Veen compliance of tanni ng sessions recommend
eel for !he fu5t week and gender of the. and
the type of fucllity (eg, salon, gym). :Percenc
ment and the 11: statistical te6C were U-'led to assess the
inten'nrer between the two inte.rr!e.;o...-etS.
RESUI:fS
Srudyl
Sam.pln charn.cteri.stlcs nnd of
advertisements. A total of 584 newspaper Issues
out of 606 e!!gible Jsslles was e:mmi.ned over a 4-
month pedod. 1\vemy-rwo issues wore not e..'<alll.ined
elther because the isslle was missing or because 1t
was not recovered. The comprised 14 com-
munity (189 issues, 3:!% of all !Ssues), 4 col
leglate (84 issues, 14%), 4 entertainmen.r;spedal
incerest (68 issues, 12%) , and 2 maJor dally
pets (243 issues, 42%).
Seventy-three tantllng '.ldveltlseftlents were found
and recorded. ll:J.Stlcl on the definition of
an unll.a'ticed tantling adven.lsemenc, 55 tanning
advertisements (75.396) were labeled as offering
unl1mited canning pac:lwges. ltl addition, 7 ran.ntns
adverlise.l"tlentS (9.6%) found to promote saft:
canning whlch a \'iolation of the California
Filante Tan.nis.lg FacLlir:y A.ct of 1988 and l?edcral 'Il'ade
Commission
Pt.icc data. PromotJonal prices locaced in the
fidvcrusement recorc.Jecl if the tanning ;J.dvertfsct-
mem had a momhly-unlimlred package price oc
eco.nOmlc lncentiv-e. For promotional Jn adver-
tisements with mQ.re than 1 month of tanning at n spa..
c:.ific price, a monthlr avera:ge cost was compured. 111e
average cost ofnn unllmlred.rnol\tnly mnning paclc.1gc
was S29.66 (standard de\ll.alion {SDJ, $3.21). FO.!.'tY
one canning advertisements (56.2%) were llnked ( O a
facility chain. Of those cbalrul, 31 advertisements rep-
resented a chrun of 4 facllltles M.d 10 adve.rrlsements
represented a r..hain of 5 or mo1e fadllt1es, all wldtin
the Scm Diego merxopollcan area . .As shown l..rt Plg 1, n
.sea!lOru!l pattern Of a number Of Cli.'i
played was found. More tanning advertisementS
em! and i.mJimjtl.!d) were pre-v-alent toward the end of
the 4-month perJod.
A.ssoctations between newspaJ?e.r type and
advertisement prevaleJ.lc'e. Table I pte:se.ats l.be
proportions of newspapers, by rype, that contained at
least one t;t.nning advenlsem.enc and at least one
J AM ACA.O Dr:r,MA1'0i.
VOWM!i 46, NVI-Ii!El\. 5
WO MAIN LIBRARY NO. 54 21 P. 5/7,
'
J(W01l et al :703 -: '
Table I. Association between tanning advertisements and type of newspaper
Majlll.' Coll.csiatc Coamntnity
Nu. (%) No.(%) No. ('1.1) x'J (t/fJ F
tanntng ad. 0 (-) 1S{26.S%}t 16 {19.0%) 1 (0,5%)il- 101.53 {3) <.001
Had unlimited tanning ad 0 {) 1s 14(16.7%) 1 9826 (3} <.001
----
"Significantly different from other types, but not irom each other.
tStgnificantly d!fferem from collegiate- types.
Table ll. Percelitage agreemGnt between observers and K statistics
Same: (IJllll:li!Ur (:u "" 15) opCJ'ator {n "' 4!i)
ltt'im "Pt:rtl<mtliiJC: It :gl'c=nt 1:
Sax 100.0 77.3 .335
PreqU<!l'lty/week (50,0"" 42..t'
Duration/session 53.4 ..
58.5 .131
unlimited tanning 100.Qf 10o.o+
The -following cut-offs for Interpreting reliability iTom 11\e kappas w&rQ wed: 0 ro 0.4"' marginal, 0.4\:.o 0.1.$ ::: gocr:I
1
0..1sto 1 :::: l!.lCCGihant.
.. ._could nor be con1puted because row values did r1or equal column valuqs- In a tDbla
1
K r;ould not Che number of non emptY row:s and columns equaled 1.
unlimited tanning advc:rtl::;ment, as the
results of the chi-squru:e analyst-s. An noted, of
newspaper \liM slgnlftCJntly Q.'!soctacl!!d wlrh both the
p1:esence of tmy mo.niag -ad a.od the. of un
unU.mitecl ad. Post hoc multiple c:ompariso.os indica!
ed that ronjO(' and community cypes of newspapers
had .stgnific:andy smaller of tann.ing
advertisemeru:.s tha11. l.he other types of :oew11papers
(collegiate artd erucrtnlmnenr), but were not difl'erem
from each other. Emertal.nment newspapers had .sig-
nificantly propon:I.on.s of tanning ad"'errlse-
meur.s than c.ollegiata nc:.-v.rspapers. J'vtultitude r:ompar-
Ls ons furunl.l.mlted tanning yietdecl parcllel.Uncl.ings.
- Study2
Sample A t mal of 60 telephone
was conducted. Prom un initi<"tl sample of
90 ra.nning facil.it!es, 30 factlitics did not the
inclusion cLiteda, including tlO longer hav4B opera-
ble tanning beds o.r be.l.ng am of business. The tan
nfng fll.Cillty saznple consisted of 51 tanning salons
(8S%), 5 centers (8.3%), and 4 hail.'lbeau-
o/ salons (6.7%). Rcspondent5 included 17 .male and
40 female ma.nlil,S :fadlily opeiiltors. The avel'age com-
p1edon time of the primarr intt.'I."ViCW ;va.s 3.2.3 min-
(SD, 0.96i r4nge, 2-6 minmes).
Xutcrobserver :tcHability. Percent agreement
observers nnd 1<: stiHistlc values for inter-
views wirh !:he same or operator by both
interviewers were Fifteen of the fut;lliLy
operators (15%) were .imeE'viewed by both intc(Vicw
'n.ble :m. Summary oftnnnlng fac:llity respon5e to
Interview questions
NO. o! tlmllht!:l'
Item nnd tesprnsse lllt!flki e:t 'Xo
Frequency du!ing ffm: week
3/ 6JJ
Every atier day 17 28.3
Three or 4 6.7
Unable to detarminew 2 a.3
DUI<.ltlon per session
3-.5 min 1 3.3
6-10 min 44 73..3
1H5 mrn 0 10
Hi-:20 mit) 5 8.3
Unable to determine*
..
.. ...., ,. , 5
Have unlimltu:d tanning
Yes ' 60 100
Come in as much as I want
Yes 43 7!.7
Only once per 17 28.3
.. Respr.mdent5 replied That they nt:eded to sel! rhe customer be-fore
glving an anower,
e.rs. These data are shown in Table II. lCValues for 5 <lf
the 8 could nOt be computed. Wrth the r.1w
perr.encage agreemenr dQ.ta, agteemenc mnged fl:om
42_2% to 100%, wtth higher
found for ol,:lservatlons of same opemmr.
Com.plinnctl: and other outcomes, Table lli
presenr.s the distribucton of responses to the confcd-
'
I
2- 2""9 .? '7
9
M
sr. .. IJU L:! ;,
704 )(won et al
WD MAIN LIBRARY
etme's key''quescions. Only 4 of 58 specific respans
es (6.8%) to the recom-
mendation v.'Cf' class .!fled as com pliant 3 times
per week). In conuwt, of the 57 ope(il.tors who gave
<1 spcdfic number of mtnutes for the duration rec-
ommendation, all responded with a dmat.ion of Jess
than go minutes and were coo5idered compliant
Tests of assoCiation were performed to assess re1a-
tionshlps benva:en cornplJance with recommenda
dons and gender of operowr Md f'llCiHty rype (eg,
salon, gym). No srntistica.lly significant val-
ues were found between any of t.11e complitmcc ourr
COJ;ne$ and either operator gender or hcilicy type.
All60 facilities (100%) reported offering unlimited
raruung facilities released
monthly-unHm.lted tanning package p.dce.'J over tbe
phone. n vrnge cost per m.otnh of <tn unlimited
tanning pru::kage was $38.50 (SD, $8.10). The mnge
of reported prtces was from $15 $55. Duling me
second (J:citli!bllicy) mrerview; 59 of the 60 facilities
releru;ed single ranrung sesslon prices; these were
not -assesst!d during the primacy interview. The aver-
age cost of a aln8le. ta.nnlng -.vas (SD,
$1,16). The price.11 rnnged.frorn $4 ro $10 per session.
DISCUSSION
A lr.ey f:lndl.ng from these two studies
the frequent use by lndoor ra.n.n1ng facilities of
"un.U.mJ.ted" tatllliJlg ns a promotion1ll S!nt
egy. 'fl'l!ee !ourchs of the prlnt ads used this strategy;
md aU of the facUlties in ol..lr sample offered it as a
payment option. Compatible wirh tl'l.k; pL<:actk:e, the
majadq of facUity operto.r:s they would
rlllow a confederate to tan at b..lgh ire-
(that (!.X<:eed the E:DA!s reconunended
guJdellnes). Although our datn on wn.n1.ng duration
were more encou.rag.lng, allowing such frequent ses-
slom .may result L"'l consumer_,, ov-ereii:
posure to tJVR.
Not surpriSingly, this 2000 sample of local
facilities overlapped with t..l1.e sample ln our 1998
study;ll the patterns of compliance were
ble, with low cornpll.:-u1ce wlm the freqllency recom
mendation high compli.ance with the duration
limit. Other studieii also have reponed low compU-
ance with the frequency
'fo our knowledge, ours are the only lltudies ro
elate tha( have exam.lned pridng su-are
gies. 'The aYerage package price quoted ln the ads
(study l) v.'OU) lovver than the average price gh:en by
facility operators .in the srudy 2 lmerviews. TWs may
have been due to a gt'earec tendenqr of lowec priced
fadllrles (relative ro higher priced factlities) ro adver-
tise and/or to the:: ,occurrence of om.H:Jme-only pro
motional prices quoted in the ads. l:Jsing the mean
NO. 5421 F'. 5/7
JAM N:.AD
M;.v 2002
monthly unlimited tancung price based on
our !merview data, we estimate that a consumer ran.
!ling daily over a 50-d.ay pertod would pay approxi
mately $1.28 per session. In coru:rasc! the single scs-
.sion price was $6..48, (The monilily of
strategies are S38.SO and I.'Cspecrlvdy.)
We do not have direct evidence mat the padtage
pricing stro.t.egy p.tomo[es greater session frequency
(and cumulative thm the individual ses-
s.lon strategy. However, it: is likely that t:he former
srntegy attracts a larger number of firsc.-tlme users,
glven tbat it provides an 80% discount. This discounr
m<ty be particuladyattracthe to adolescem.s, who may
have less money, place a high value on being
canned,14 and may be at great;er risk for skin c:a..rttet
chan adults because of cum.u.lativ.e UVR
YoU!lg age (16-24 yearn) predicted sun bed Wle among
New York state residemslll and a survey of adoles-
centS )n St. Paul showe.d h1gh rates of indoor tlli'U11ng,
particularly among gl.d.!i.l9
Borh studies h!td methodologic llmlratlons. Stt1dy
l would. .ru..ve been strengthened by sa.mpll.ns :news-
papers over a l2-month pedod and by obtaining tel:t-
ability estimates. 1o litudy 2, respondents reported
their pi'llCtices for a fun1re Vl.<ilt; these dutn may nm
carcelate with the p.rncdces dt1ring- an actual vJ.sir. In
addition, the aw:eement estimates
were tl!:lfltl.vcly low for some of the va.rla.bles. The
lack of concordaace may be explaioed, in part, by
interviewing different operators a'( most of the f.J.cili
ties. It may nlso refie'.ct a lad; of !:Otl$lstency itl whac
one operatqr sa:ys tO dlfferertt clients. Finally, .all
indoor rannlng .fu.cilities in Diego Councy mey
not have been listed in the Yellow Pages or Internet
dlcectodes. bcaur.y salons and or.her
businesses offering indoor tru111.l.ng ns an ancillary
service mny not htYe had A liSting under "Wlnh'lg
S!tlons." Thus the search Stmlegy m11y have omitted
some tru"..ning bU.'llt"!!Ses. !:n futut'e studies, st1pple-
mental. daraba.ses, such ;,;s .American .Busin<e:-JS Disc
aa.d Dun & Bradstreet Marketing Servke
1
should be
Utled l:O 1dentif{ potential oltes.
As stated in our artlcle,ll ro improve con
sumer safety we .recomn1end mru\dmory openttor
trai.nrng and systematic of e:Osth"'g .t.eg-
ulations. Because r:he frequency criterion is
only a recommendatlo.n, fedem.l, smte, and local pol-
should consider changing it to a regula-
tion. (The FDA f..."Urnntly iS revisions to
sunlamp product perfo1ma.nce st'atld.ws,20) Flnaliy,
additionaL e-w:ploration is warranted of the ''unllrnit-
tanning p.romoctonal strntegtes.
need to ststematically the specific impacts
these strategies have on facilicy use, pa.rtic:ulady
alllong adolescents,. In tne meantime, given the
J .AM Ac;..o Dcl'lMATOL
VOt.VMt: 46. NvMll:.a S
WO MAIN LIBRARY
wiciesprea.C! use of these :mnregies, health advocates
should develop interventions targeted at consumers
(and their parents), informing them about e;,po!lure
guidelines. A.s one lmerventlon component, select.
cornmuniC;ltlons could be: in the same media
that prim indoor raaning adven!semems.
1. Ametb:an Soder:y. Canter facts ond flgure.s, .2000,
Adama: Ametk:iln of Soc:lccy; 2000.
2. Col.intll on Sc:ientiRI: Affairs. Harmful effe:cts or ultraviolet radla-
tkln.JAMA 1939;2.62::380-4_
3. Swerdl ow AJ. Weins-tock MA.. Do t:IMII'\9 inm;u t:ilvae
me.lanoma? An epidemiologic: Msessment. JAm Aod [);:rmatol
1998;38:89-!lS.
/l, WestetdahiJ
1
lng1ar C, A; Jonsson N, Olsson H. of
cutaneous malignant melanoma In rctlatlon to of
furthtH I.'!V!dohctl for UV-A flr J Cil11I:Ot :moo:
82:ts9:M.
s. at.. U!e of W A !iUtlbl!d$ for ( OSOietic: tanning. Dr J
Dsrmrllo1 1986:11 5:6776.
6. Deleo VA.. T11nnlng 511lons. In: American Academy of
Oermatology, edltor.s. Pmceedlng,s ot nnt!onal c.onferanrf! on
en'Jinlnmenrnl ha'l2rds to the skin, Octobt!r 1992. Sch;annburg
lll):Amatien Aclltl!!tr1)1 of D!lfm;jtolagy: Hl91.\, p. 37-4l ,
7. US of Health ;sntl HlJmnn .Servlc:e.s . Quality c:Jntrol
guTde for 'products. Jlodwllie !MD); Public Hoillth
1988. OHHS Publfc;:tr!on No. FDA 88-8:!34.
8. Trade Indoor tanning (!'actsheetl; 1997
(Miinej. Avallabla lib IJAL.:
Atces3oo Janunry 15,2000.
9. Amerlc:an Academy of Oermnology. American Acaderny of
Dermatology JiUmtnary cf tanning pnrlor legl$latfot\f
Schaumbu'l! (ltl:Ammknn Acodarny of Dermatology; 1995.
NO. 5421 P. 7/i
Kwon et al 705
10. Coslifornla Department l)f Health Servlci'i$, Department of
Consumer Affairs. Fllilnte TIIMII1g facUl tY Act af 1 !168. Business
hnd Code: ChaptGr 1998.
11. Culley CA. Mnyer JA, Busic AJ. Etchenfleld t.f. Sabis JF,
et al. Compliance with fGdlllral and stare ll'lgislatlon by todaot
t1lnnlng f!lcllmesll' Sl.\tl OiQgo.J Am Acad Dermatoi20D1;44:53
60.
12.. Bruyneel,Rapp F, SB, GvJn JO.Tha roMing salon: an ;;rea
survey procadures, and practices.) Am Acad
Dlltmawl 19S8;1S:l03o-S.
13. Falrch!id A, Gemson D. Safety infoi'lnatllm pmvid.ed to
mmers of toJew York. dty Am J Prev Ma.c.J
1 !192;8:381-3.
14. Mermelneln !U, Riesenberg LA. Changing ktlawlo:!;lge and ani
tudes about skin cancur risk fltctors lo adolestems. Health
'P.'I}'Chor 1 992i11:371-6.
1.5. Mark; R.An overview of skin lnddar.<:tl and causation.
Cllnc;er S.uppi199S;7S:607-1l
11.1. Marks R. Sltin canclilr- chlldhood prottlttlon
proteaion. Med J Aun 1997;1 117l475-<i.
17. Weinstock MA. Coldln Gl\, Willen WC. Stornpfer MJ, Bronstein
BR. Mlhm MC,et ai.Nonhlm111al C'\ltllneaus melanoma lncldQflCQ
In women with sUn t>l!poaure before 20 years or ago.
Pediatrics 1959;B4:Hig.:204.
lB. LllJQUI.si PP, Baptiste lv\S, Mfi. Nasa FC. A popula-
tlon-bilsed .5\lrvey ot sun lamp and tanning parlor In New
York Slllto, 19!lu,J Am Acnd Dermarol l9!l4;31:5102.
19. Oliphi!ntJA.Poot.er JL.Mc:Brlde CM.The usn ofc:Jmm,uclal tun
ult'lg rac111rles by &uburban adoi'<SI:f!nts. Am J Public
He11!th T !194;84:476-8.
20, OCJpartment of Health and Human Servlci.!S, Food and Drug
Admlnlmatlo11. M111c!ieal dl'!vrc:6UI; sunlamp products perform
ancs stlmdard; for comments anC/ li'Jformatlon, pto-
posc;;d rtde (21 CFR; 1 0.20). r:rad Reg1999i64:62B6-90.
I'
!.
' :
-----------------------
Compliance with federal and state legislation by
.indoor tanning facilities in San Diego
Carla A. Culky, :.-1PH,
1
Joni /\. Ph[),' burn Edch<orcfl. MPH," April J. Bl>!!'iC,
f. EicheJ'.fietd. Ml'>,h F. $allis, Phi),< f> .L K
Susan L Wooon;f!, rhO" San Dlugo,
&tck,tt;rotn'ld: The ()! ;; 'ld ti1:\ning US <!,.'(';
:lnd !"en .. l..v'v .. hy \ ..
s:ti'e!v reg,;iii;lvi'\S ;lnr . .:: :u o; <;kii1 :ant': ur:u:ar d.;-!mage.
sw\ly {;;:tnli:kd le:c: (.'f !)y ;;u1;;1.<1fi wi<11 ,;;e1e<:kd i,;:deral
r.1:oi:1g ;. )<t:' S;,:r C:J>!r)ty; C.t!iforr:i;;.J, v:s!ted by a ti)d<:(.lerme pnsi'lS
;::m.),spo;;,:Lvt::- Cvnt)Hir;Ce 13 we-re ''Y t!ilb<::
tli(<:<:{ q,,e(y ()( ohS(;f"<>til.lJ of cf ;lfld w.:cn;ing C1;><">ators' :o
ri:>kl-.<S<i:d questtQr:$ aisu were
1(<f.rSU.ft. Nn ft.ciUy l'O:llf.>li><:d with a1! U j p>ott::Uivc
n::;{,tbWm1!: was high ln witt' in.<i.Xlmurn ;aw.l,-,g frequer.cy
<;nd lY;;:n:I'Hil! {:lf>})WXirMHely 'i3%)
Ccnu:luslOh: inve::n;gmof':'> 't{_,:;.)nti'lll::!'id :'t':l;1:i:lt-:)ry,
:t:<; .. (J ..A..m
ue m; :nor ZOC11 , s '>so.)
U
krnvi,lk:t C;1(!i;:.rlon {t;VR) fnY1'\ .-;ufl is a
kr>c"'';\ J'i,;k for ootb
skh1 !\nd i-4 n;t-
b and
fron< !n!JX>f heds r:i.sc has linkt!d ;:.v
./L,h.!i\iuna!l;t, r::ed:c;d
h;h:. :n:1ny i)f s.l.r h; .. ..
dl\':t;-lge tr . .zr ftutn
Jr;dl,)vr t:l(lfihg de;:.;l:::;_:.::. TL<." irdOC' ::f{'.Nc'ig
try, wfHCh ha..> r,:o\..-n SI.>DSI01t')'ialiy
---------------------------------
From 1ne C<<oth.il 1> of ?u biic the :fl.lp<lrt.<l'e"t oi
$&r Dl;lgo Stata a(\d Otvi!or> t.i
H!:<: ty of oan D:<>go .Schoo!
c{ . .:; 3T;O
Oif1>90."
iot jo.;iy 1 :t 2000.
)on1 A. Maya;. P11t.n'
.l \ l 9. 5!1"l S;jf)
c ..
.. by :nt...
C Hl/1/\ 1C63
!lVi: l
r:ing beM:> ptirl'l<trily UVA r..dt;.ti:c.>r
:1nd H' tt)t-!t
prctrecrs f<Hll!'e ,.,,,r.hutn:>.r; ir.
cur1;ra,'i!, ,<;e..-eral health ine!utl:ng tt'.c
uf and ;_l;t:;
/vkdit:al. lobb;;::J [()1 :A
h;u; m Hld<..l(ti' t<\:'tning Tlu.::t.(;
n;que:'".:> wert; 'f'tu:r.;d bv the :i::'1t:l b;.;d;
;l'ldovr :nef;;.r;(trn;.;
11
;,(.:;"((: of ;:.nnn>g :;a AdLlitinn:.>\
d;Jc>. that tb<:! r:::ajo,,ty >"ldo-:;.-
types i a!
<::Ll:;<fk:--.rlon),d h ind:c:.Hmg tt h;gh to
to burn firs\
tn n:idt:l:ly ck.ta
type ;s rf::d for
1-xKn !\Kit. . .i-<t
iy; r.he F{ );)(.]
(_f0;1 ..) .. ;,:rs h,(l,:t(",!
the
(CFFr; .20, ( 'Szi fl htrn i
p hltY: ps. ft_;r t
th(; rOA Lu:;
Material may be protected by copyright law (Title 17, U.S. Code)
l:i r; vf
\\.> -Lin':cfH
ul". vf
r,n:; the ... on
w;::;><ng !ah<::is, ;;s wdL .lS mhcr lp g(::nernL
tht< nper:uk>:\:- of bdJiti(;:; (e?,,
uf are
In :ht:: Fi\l;-;te
An. nl' J 9Bl:t tv<lS cre<><<:d ; p;<..,ten :and pn.l:11o;e
l t
<..:or-np;hHi(';e! ';1y .. ;!) the
hc:1() sVt1"l.e.
safel/ wich inclo0:
In S""'nctn ;ncHvidw.l.!.' hr.vc d1:.:
potert<iat to be expo:.t:.l w hl,gh
.. ' .. ;VR. l9,.!l who f;e,:juem imk<Or f<enr.ing
f.:Kii:h.:s m:;y n;.cLi\';:'!1; high
rh):>cs ;)f CVR .. p:>rth..'>JJ;;riy H IOHI;'<i!'\g are r.n(
rz-; (;{H>opH<erKe w(th ;c:gdations d:ut (:.!tempt w
tf<)i "fhe of thj!-i $t :.;dy
w wi;h ;;dec:
and by San
!!'Wv(,'r
!'\1f:'fH.ODS
of 5<i lllf"lf ;!1);
in San rnr:.tn,:>poiiran an.:<;. A f<Idi!
"J:i...t.; :t:ty
\)f hm;im::>s {h;:u providr.!:> !.>er..;,.,ns :1e.::es:; <my ,l.w
Piql tk..'Vi<:t>. '{; .\ li!'l (If \<H1fd:1g f<tUJirlt..;S Mi$ Ob!:Jin:;J
r.cclm l..lr,,kr tr; :t;<: Sun
Y;;!hl'l a:;d .1 :;e<n>.:h !);':he Blg
:ry ra uf
th<:: S;,q\ i)ie.,f.!0 ;;re:a fn)n1 tht:."e. ll;;h,
wiH . .:: .,,.ere if.n;;;J be out 1X
t1r> r:1fl'ere<f wc::re
'i(r'(,.:;' 'hue more cmm t)lle
h.::d ;: };;.une {fe; :
l.!t for (o:t--
nf ;'ir.d n;.\d
:u1\J IHher ::;t,;pplv
The rr:rn;lr}' clept:!)l .. W<iS r<.Mli!<;il.
ia6hry e:omviian<:e w:tr. -and sra!C rr:g-
.. a:> l<.'i!w..S.'ied by t!iret.."i ui>.scrv;l t icr, of f::u
HH.J Vjrh
t:dleeed lry :; (\'>nkdt:nHe (C r'\, C) w:.o f..>O:'>Cd <J
iun ;lbou! ..
wrl:l(H >0!...}1
;o;;ed t \"1f
ad!;1re:;:;ed by fcdcnll s' .. J:"!br''!i''> Pr(Ektt.::
(Jf o
FH<fnte uf
were ..
1:' nn:: nf !? < .,:, rf .-.:.vi :.d 1 wodd t e ;'' n ;, )fH e ratlla
; fV:."-r': :Jl.":.fy,A'i( ..
:.:uo;
antl .. ..
ger ;,mi other n:; :he
The fecter<i! (<eeo:,n;mem.btit>ns.
d <iu,-::H>un H> r<:C
1s n,; :nc_;:e
0.'<i MEL {rr,;oi:u;,i Jvs<e'; cir;ot:S ;hl" :';r;;:
'Y.tt:t-:<. ir rt: tht.:
<,.J:-'. ti; , . ..
of
.S>)n i H ' of
f)<):;tt!J il'l l:tn;.ing are:.,
;t;1(J r11.q1:(ed for .l'i to :!B
of rhe ..
by bad1 the
hy \he
1 ond
1\(!di\;ofl:dy .. t.ne askt:d the facih:y
5 cpe:)er;cted <eg:m .. ling rhe 1>Hk
tY of iJc!iity u.)<:', ir;citldit'g: ('!)"i\(t:
(2)"Cfl:; { :>w<bl;ffh;"d f!o:n
ni<lg .. {::\)"I;; ir beds :>;oft;T 1..h;lr, <<U!n 'ng
( .. .l r.:ti p,-<.)tt;t,;t nHe !r<..;rr
t CJ'4t;-:er frv:.n
Wt:::rc:
;iun.:; in .rr.:::viO\!$ :;t tl'..lie$. H !()
""'et'e
\;tJtlt:d ftJr ()rher t t vi(!. \r'\CH"\j ..
incl,;ckd ard cy-pes d beds,
(,f H.
rr;a;ic;n abo<1r wr.n:ng m'thi;)e
1 d:t:dng .. ()ne con ..
fedcrde, p:;l'ir.g as '' CUMOtr.er, .,jl
54 f(tc,jhties, :}n..:..i
;.$ nt 2 >V(:'t>kS On<: tn:f ()i <he
r:m<iOi:'l1y to !c <H)
;lzrc:(npr tr..; srjH 0bt.3li'ling
rd1:>.t"-k e1:-t:1r.are.'i of Tw.::,'1;y of 41
(J Gf 1 Wt!r"C
revt'>itt:,1. The .>e(v:d me<<-S\t,cJ <i f.Ltlse! c;f :h<:
v;H;;,bh:s <b :2 t;heck <:;f rest.dts
t\"(Ct';,h.H by Op<::;(
;ito;,;. Ea('h fcrrHile.
t:.nd ;.r: ..
3b';; WIL L1<..h l0 w I 5
mbt;:>..<;. The con ir;\f"O<:Iun:-d f'
sornconc who h"d rcv<..:r \,;Sed l<l!'li\!ng hell:; !:r.=fore.
Shf.;' t() n \an
g,1ng t(l 1-hwail :h<: e'<': m.;)r.ch mi
:>OrH: the ...,,,f;;:;:l Of t:t.;r,':)g bn ..iS: 'H:,
c:ar;; p liti: ;ne ..
.. f,.>r
.:)j)e l nc: fjtt( of
wi! h<!r and
L)C T!te ( .
Matena! may be protected by copyright law (Title 17, U.S. Code}
; i\CAi> Dt U.
!4
or
(n " ];,
Q(Jt".r1t.l()(
:n = Hl
------------
___ K ____ ................
of opt!-l'llf.C(
of
TaMess
ro
llc'.;.,.:ci:r .;rn to (<1\'1
re.;]ui:ed
'N<!>fr><n\j i',gn
Shl..itoff
vf\ bed
t<tr-"lr.g
05: C;m \ 9t 5k! 11 <: <;fi(:N frm Wn<-1i; ;g b;;>ds ?"'
6i.S
2.5.0
lOO.O
1 oc.o
1 (H).O
f.i4.6
10\1;)
84.6
S3.S
7<5.9
76.'1
H>:l.O
Sv.O
l
.4')2
.0;)0
.75S
. .833
.093
.::no
,:16
.000
64.6
':00.0
?69
;QQ.(:.
5.38
769
.,:,, .:)
1(J{>.O
1000
t.$.6
1
7SS
.09:!.
14
g;;_;
1QC:t.O
100.0
113.8
1 :)C),(\
.. 3
no
a
57.7
M5
1080
SB.3
--040
-.102
1
.!Yj
44B
.l'.l8
i$3
661
.601
I
.Hi1
............... --.............. -----------
{)fl it'i Of negATN#! i!"fO,
'K Si.1.,SfiC z,1Mll;ll o..- .:)r <:v'umr.s .r. <:cnr!)g<':("Y :obl\,' ;, Or.lC'.
ther ,; .><::'ic:::; o( ;1nd rn:;de
of tbt.: a j':f'O-
;ui.'Oi. Tht> ptot<Ku!
;;p<.:t.:i(k' (c:g, "Dn yo'.J phlviJ..:
;;nd <llt'<:C{if..)r<..:; fl)r (eg, i0.:.>1< fvt danger
W<lrnhiJOI. bed) 1ha: C(l:ouckd diren
iy ,vfi.h the (.>r (..()t,Jes.J().lS Aftt:.r
tit [<Ki1iry, Cn/'lf:!:;;erat<::> ('.'l-,(;lh<:-r Sh!:
$pe<.-:ti( !!> !he fl''-'st:;'\Ce t::Jf
1>1gn:;) recorded v;;:rL1\'11 ;r..
ch(: >( npt;:d {() :en a." p:
bk on the 1is:;essr'l.,e!'1: {i "-l! h.>! A.:l HUdy
on
,,f h un',:!tl ;;: O!l!'go
li i y.
'he $ti! h: the;; Sc;::;,::ll
'Were <;;.dtuht-
ect t(')i' fwr
t!',t: Wt!'rc
r..r cunur,u01J:o; .-<Ji'h:bk:s. 1 \.e..iLS
tvt rc t'O c0 m t nnn g .sd.: o; fa ca ..
t,n r!;:I\Hbility w;;s
e<i by r.-;c<>JI& (;!'the stati;;!i.:.
RES I;1.T,>;
Jflti!-:-r.f).cr-ver r;;:;f<lbility
l
\:,:;iabh::; :;,:,y 20
:ha: were:- vi.Hi-ed \')y A: h;d /
clif
rcren{ the ..
obs,::r,-:!1' y Tr.c:rchrc a;e
hv vers;;s
:ts J(y
z1l f<)<;i't:t<t!S In '";ls
high. v;(!:lbies cturac!er-
f>f the 26 :ha! wen:
;(I ui the 15 v<tr\;lbi-.;:s i!\!er<lh
agr::.-r::ttt>.a: (.)f .R0 or In
WhtC"\ t:')r:c rl>i$ Ci1;.nce vah1e<$ p,rt":;a-:;;:;-
th:i.n .i'
n:hcr
dt:fi;;eli ;AD. 75; maq;;i;1;J.i
n:Jd t:;()f(: cxver. Uy < \J;. Z')
\1.::: J'.11ii I; 1'1 u; n;.. c f,; ( t 1-t e i"'il<: j::)ri t >' uf 111 cs r1!
;;Qn-,p\lf'.)i/<:' ,\i fa.;: ;l;ries wHh (he ;; :1d
\-\'i di .. ;::-t:l {
opcr"'.c.tul:i :Hne)
tr:g
of tao.niog .::md
Th<. ;nnnh_g :;;;rnpk . nf 4.\ !<!f:
.. ;;, beauty ..
to:..:<>re<l In ,t;{: Sun ll!CirordHan T:.;:.
,..,t (;".$ l.on..e.! i fac:!i ty
rrott'l .i ru ! 5, 1;>.,11', ;1;", .. f,.)f 6
}C i .>:.<:1or;;'S had tn ..
i1"": :t.->d !.;\d ;An
of 3 ,., 'ot:!l '1f 325
b: ::l\1 )'< fin:Ji:it.:-..
Materia! may be by copyright law (Title 17. u.s. Code}
. ;\C"t f\; Jl-\-"rot
J .... JAn><
l(l ......... _______ ...... ___ .. _____ _
I
I
i2"
'\
N>Jrni:.tirl V. (:01'1'\!lll..:! wi<.h by
Th.bie H. o( U!r:nil"\9 W'th f-ederal .and tly fadli;y
...............................--..............................-.... ---
-----,------------
.... Jj y,,mtlnjt
(o = $,j) . {c:t., H) _{a ': 1 :IJ ',{' dj P
.............. .... "'---.,.,:;,--
:e9ui.:1J<:n$
Shul-f( >!>N:l COM!)lial'l!
bbeis
.ac.:es:sibie,correcl
01!\et
t:eeloi!ral
tilf'
II)
Ca!ifr<'>ia H<>te
?fl.)ft"(.'.;\1\1 e<;'<I'\'J<ii'4'
s.>..ttiltaec:l
w$C
pcme-d ln
.,...,.,.mlr\'3 s>or. tt9':;1tll<>.
.remalc:C<I'\>;.;?fll fo! l4
S7.4r ..
ss 2'l'fl
l'l 1%
as.lt::t
?4.\%
56%
9l.l%
H}C.OY.i
<!7.8%
75.6%
$/.B<\1.
/S.f}'>:;
7.)%
96.8%
lOOO%
e.s...t%
1<1.6%
6VN>
769'11>
100.0%
\OOOCib
;!6.!1%
.119
.926
.l09
.2(19
.U..t
.077
.004
.143
.lSI
1).47
')
.31l
........ .................. ........ ................... ..... --.. .... __ ..... _ ................. .
nf d""l!ltt!i in COri
variw AH f:Jl' d1e J:.tu!nieJ> !hey
nf.<.;rrcc (<.\ <....r U;;<h Tht:l:>.:
the ''Wt;.Hf O(
Sy;l("f":'l,. t;.nnill_;?, i h;lJ <il (<ffl
nir.3 ... ,f i1H,
:'ir'i{l LN.B r,}Y'\. :n :H.JLJitinn. ;-' hdlttil!.?>
off'Ncd !I-,<:: "Svp<:i'
o"Ortl!! tx.ct: wl'{'h :ls.
t.;'\'A "'' "h;,rn.lu1 l)u,r.ing
The '->r.){:mtor' 35 c_6Si.f
::.od Mak;; T:1::. timr1:lil ion ox
\\'k. Af. l3 (ll.
u{ :5and 2) "l<le$
'n' 26 1") J 4 of
.)6 :.od 4"1 :,r,o 14 (it!e-( ;h.,n t.';)
Compllan.::e with fet'le:r:a\ .:llld
F;!;( l S<'1m<1n7,;:-, c>m9:i<::>(:c: Whh n .. e d
,;, t:ornj)h ..
Tt r:wau .. i
intrc.n.<> w1h {li(<lrrla(d devian1.>i\
lSi:;! 2.0)
Cn:rlpl:<n,e wlll' ii.;(l(.'ml
Hr,r,s. :...-e-all anti by .<ltH'I'\,
!n n1ok il
Ma1ena1 rnay be protected by copyri{;)ht iaw {Titie 17. U.S. Code)
A!V . .
44, "( "M&f !1 1
UJ. to q,..eslions
................... --.. - .... ................... ............................ --.. ............... _
\H ::!t ll)
............ ,,,_ ..._ ............................. .
;. 1;;r,!"\;"'9 sale?
110
01hl?r;
2. Can! from ;..<>lng
Yes
Y>;<s, ; vZJiifi
No
'L Is t.'i>'1nin9ll"l $Mer tr.an Ol.Jtdoor>?
'fes'
ktdir-'!<::: yes
t :>o;
Oth;;:r-t
4. <l t.an prc,lii!t:t me from bttrro
1
'(es.
:r>::Jirect yes
indir<!c r no
S. C,;n I l:iHlC:<:f from f<flning
!r.dlrect yes
Jndirecr nO/ev.:H;Ic;>d
220%
63Jl%
l<1.5%
O.C%
Sr.S%
2.4%
7.3%
53,7%
;1.'1%
.11 .;%
92./%
4.9':9(,
2.4%
0.0%
25.8%
4.9%
4.S>%
---v ------.. ---'----
J8.5's<>
46. ir.j,
7.7%
7.'!%
:3S.5%
61.5%
;:}.0%
33.5%
;)Q%
3a.sr,;,
1."/f.;o
D.O%
0.{)%
'1.7%
,,6.2%
53.8%
0.0%
emu
59J<C.f>
1>.0%
1.9%
815%
!.9%
9.2%
:>O.t%
1.9%
.n.3%
9.1..5%
3.1%
i.9%
31
o;_F.a
3.7'ro
3.7%
10 <.\:'tl'rrDin.tj Eof (aU '"
ln V!,;dy:;.h,
:o f;::,r ..1 wt;,:-:!:
conlbined into lm "<:.>(her" b<:::G<($' ();
sarnrJt: Com:;Ean;;<.:: wi:h odiv.it.1u<;.l f.ed
r::.n;;e<:l fro:n 5.6%
t1> HJO;i;\ As ;;bot-;n. wirh ;,..,(.[ivid\l:d
UIHfr.w'i:-; regLtlaiiGns fmm w 100;'[,,
....-;:,:; :o oc h!gh hr pto
.and nl p1-.::at rn4.'\imun1
Hlluwd r::m; of rhe ::lf
o( la!,.'le;$.
.::1!' U"-JJ< ""':P''s:.,rc L;bel.o;;; ;l:i(J iegibii;!v,
<..ll
for
of w;;rnJng ,,;gr::>. '/.
Rl\)..i o::onecwc:..;:; oF pe:mi.;:;J{)n
lLt::sc betw:ot"' rhe agt<:> ;:J .,<i ;.nd I':\
M:d t'\H t'l0lian.x: 1 ,( ;q'; r;;;,;;,r:a:.c :;hut-off
:>witd .. Ct-,nfe'-kra!es wuc tH'I:-thk-: w : swt""
(..\f
mcn; !ro11; <:ny of 'he ;;j,:;i((.'(l
h<>w
lit: [;:\,} lir7 f
: t(i v;ith ...
Of 10."1 (SC>
Hed ,c; 20 mitWfe!f>, l
ity atov;r:fi {2
20 (lli:HJC The Fv:..:s
for tl.<:ef!> Vjll'iC.S
,,ccord ing t\) skin typ<!, r !! th;cr.:
he HJ 3 a of
jG pt""r l n::;,pun:.e
fvr was r.r:(i
t.;f tLc of J. 0 pe-r
as "'' {CD!.kd <is non-
<.:<.. 'Thu$, .. H
S'):;;e 1
5 per r:,uf
f,-..:
of b-:twcec, t.:(ilf'Y
trpe $:;1.h..1;, t
:.g :ce t:atr,ir;g ..
(i<Al:> (; . wen:
!ound
C':li .. of P
f'oi- !';
p:;r{. ed "' T:<b le U . Nv <:it f!t:>,-e rKl: l)e r< .o;a1 ':l' -, ..
;it:d. (itt'H:t ... f.:)\Hld f{Jc ief1gth uf
Material may be protected by copyright law (Title 17. u.s. Code)
ttl r..:M"l (ic, Glrly i:: th.: t;H\
pr<'X"e: . ') (r. i?ij "" " P ""-' 66tl)
n\' 'fia<HJ
\':Od<.:(J :0 !i
<(:' .. 6 ...fCi:'y' 6 i
whe.r> :iskcd ''Are ,.;;; y
S')'X of '-'P<::!'Z<tor:; cli:ec!y o.- inckt:n:,. if! ih<:r
codc:i :A!i <m
''[unnJng are thl<rt
<W OK if yo;.: ll!i<:: th:cr; in
n:maining opL::>Jtr>rs e:n.swcre<l "no." iodiren n\>,
zlti:er. Th<:' .'Oded :.1:> an n() "I
can't (e!! you : hf.'!v s;ltt, \JJ' f::>.e. from ri:;k. Otl':t:r
'cr :l!! incLded, "i Oui:'( k<H.Iw,"
0r ''I c:m': say"
"C;n; I geE from 'A:>ir;g \an-
:tmg aH o'" orc l>f . .;, ;,"::;;-<,:,;:dy
ur a t.1U<lfifted
:l V<C'S hut
ilk\: ym, out;;;Jc," why
we Ui t1y !et y-o\.: out fur t)f {
a\
Wh-:11 asked ir-, heeL-; than l<.nr:ing
<ltlidO()J$?". r;:plied m g;nt;: <l'' ;ndre-o ;es
res ;ncb.;led. "Tht'n:: .<re
onl) UVA rays y,,v hv-;:: more
C(J n t::..:-< <:ver the ; yp!; :> f r..;y:; : r,(!onrs," <t ct ;)';;)" h;we
o.,er of e:.;.pcS(!
'fhe r-<:!m:lir.ing f<::'j)iie;i -wi;h ;1
nv, r)o, <.)r Th.e :ss
jft '"lt ..; Hu
\\'hen fiSK<!d ::l)e,.; I.J:::.1:>e !h'l)tecl from
;;,imT, 96% <:if ,;per;-:t\u;s
:;fflrm<t!l-'dy. The inl:r:::ct ye$
i$ ti''e f<lUW;Ji h.;;n
fr,50;," no ';Y<H-' .-;tiii
1.0 be ::lnd an SPF of l5
Ul,.)l$!de.
"Can I get ,;K.ir; from mnnit:)!,
tn::us:"', >:>f :m:;wcf;-; wer.c
an indirect yc:;. These in.:::<Hicd "':'hert> ;sa
.. ... cr" 'Yun
:;:;tn(<:l- frvrn cvery:l:-ii!"lg" The rY;:Jjorhy ,>t
were ;.1;; :m i:'ldit.ect
of
C<lii::Zf i<; "Burn(Pg ::':1\l:>(.'S :<k\n can-
c.:<.!r: "Tf Th<.: >f
;<) ihe:
,ror.::; a..<d t;>nr;ir:g :ype.
DiSCUSSION
T( c;uf' .S\,:dy .,;f<S the ;o
i'IC tv;;l1
1 A<:" r-. R-'-1r':r;.
i
w-!r.d ro
ctara -:;..ert! t:l>fiecteo
;:.$ ('u${(}rt:ers. [I') V> t;.)m-
p! WH r, fC>'!r'\;;j :1 :';('] !C<.'Ol;;f'J\cm;a.
ai:.t..)
{o \.:Lc-nrs ibo;.H" the ";f
Key nndings below.
wi;h th<.'
fClf .. i!!
C{}r-;1 r!ylng wi; h f<:};Utm tl!r fHI >vidmA
and cvew:;-ar,
the;n f\.>t (:H:;il:ty se. ln ahr;';1ing 'n:nras1.
;,t of
pf .he f:,ci!i{it:'1> were
.. . .:t
Jm c>f :-::-qv:rin,g
.s<.:nt fof 1e the ::he ..
;;boui ri:s.k 1e-r:ded lf.
ron,:ern.s abo" t :he :;;< fety uf i:1dC'>0r t;,rmi(>R t!le
ri$k uf er. tr..t! of
did (G( <.;t !
H!Mig a utnning
f)l'V\\..!\."'{iv;;!
given th: LN h-!1 w;
:he t-y.:
7
: .. 2! !>hGuld
lhcy \)J"l
of t.hey h; f.l
n!r1nlnX .J\'!1 .. tn ..:h
ly
;h:<;: no h.;:H;ty rc<;..,,1r<::d (:H.: of e:/<.:W:.::lr .12
ptaced !:ry lfc ..
of tazt\\il'l6 tihe!y i!:
n >r.:t.ume.;s frotli i.lverexp..,.st;re. h> '.; \"F:
t\1d O\Jt' ..et t):'i
:he on frequt:nqt
po<r :S\'en thot61' ;-he t:onfelk'n=;t: _.,,at-
h;s.ct never v:>ect \<.l!lr:mg be.:J,._, <il<.:
f)f the-y ..
ntng. Ut.he!' i'"p ..
with ttir:n!ng frcq;..!ency
ln,:cni ;,.<:,. rh<lt ,, " "udi m1,ed
r:.uml><?r of 1Cf :t
. d;..1.ring :t
<!.!>:)e.;.;ed. cype.:> \-,f
(.:ouplcd w:t}: 'i t;.x fn . .:quer:cv
c,; the ;,,,,: eveti .,na>lt;.
a,;,:ing beh:wtn:s
zhe n:-tdlog (,(
w(l-; tL:H ;'a'-'d!ut.:s wen: "lOI cnmpiyin,o: wiil!
: p-.>.renc(il fen. ..
(1) k>unr1 w {)!Hn: '1
.... h::-.-ing a (2) l VR
;._;t h ;;; :nHjor tt)O!rH.,u :v:+ ; o 'ht: _, ... t
of .<>!;d (:\j kit::;
t(!ad u> ..
Material may oe protected by copyright law (Title 17, u.s. Code)
l AM ....;l\1!'1
q ....t.
as nt:tt."(l :II :tC:."':e:>l.o:::H5. an.: :a part;;;_..
... ufwrat>l e grnup Ch04t i..<. tnt:.:rn<'i\g w:t!; :; h:gh
e;wi r< ,r,;ut"'L r, 5.Ur.'o::''' of Mint.:(.:.S(;r:,
tnur:ci i ll.a.t rt'.SPl")den!:; use<!
2.1 h!v.L t';lier. i:e
qut.:tEiy fi!'Otect ivt:
:lS repor,..:d ht;.;h k:vels :;ki!t
t' !C l ;ad nui
b; o pt:rmors {.lf> 1h::: ri!\1<.-'i .:;,f wnningY'
!n t'Nl , :)Z i n :--lr.>rth
ir.:;pe<:!t-:d wil h 2.!. .:>t:t<c feuerai
rc,:thc:rrH:>HS. "'' o f C>ttr study w ,'0:",1
('Orn,;::;nl <:( 'CVCI'r.!! ro
<e(';\:;(dy no :) ,,,.r
onl}'! sn '\he f. (\''Jf11"
p: kmce wl t h rcgu i-'oc the 4
in. .;omf;liotnl<:! i() <>ur :>tuct":J W<<:>
n J_g! 1CI'' B5% (v!l 7X'%) f:J r vi::.ib!c
sisns, ; Ol'J';,:; f;;r eye<>.'e<;;
!HY.>j fer a th.i 4:>:.;.; (vs 1 } :'!.> for
nm:.tnc for ml!iOI'S. Hll wever,
t.:,wan.i impr oved c:>mpli
ance. wHh be
\h;Jt l ic u:..cd <:iffere0t
culle C!ion af\(1 in dJ
fNent
Stv.::r:ll cu.;; Sl "tiy
be .-: onsi dered. :"l f'S\ , the
ate w<:.s n-. '>'. aok to V1eo1 every rcorn ni SHt::.
cl.:;.:a or. ::;c:,rne varialJLes (eg, p!:'esencc- t..>f
bb<!b) noc re!lc:.:. r the bst.tlute
Df these r<eg L: l<: tKmS f<x
f11cilic ie:;. Se-.-tn,('l , m1r coafedenHe j::o:;ed ;,:.
cl ien t. i.l.lld ( lf)er<ilv n> rep1>ned '><;%1l
b E: eye g<.::cw) in i!L'nr f,.;t;.1r'-
w..: a,!\5' .. 101;; rl.(',se :nirtiA' 1he
tld i.IIVi ( u wi rh "reaY ac the
tt.m<::. o ! >h<: i r r.he
rwo ootco:ncs no1
tHi i :i<l:npi t: w:.>$ restri (;\etl ro one geo;:;t<l ph
l<: iQt.'iH;on. LvJ'l:;t::qucl1ti y,
"'-'' rn:\y be- li <'fl it ed.
c,f rhc indHdcd (1) '-.:lrg
r:.r of trJ z.nd
vi,.;it>ng ail f;H:ili tics ifl 1he sumc !ll
;,; 1\J.:-f(e <:;ly; ( 2) red1..:c1ng <k:rnand
by r.O( 1!ie t rue p,:rpcs.e of !!<::" ('t'>n-
(3) n ..!; .. ...
tlt!vdnpl r.g, ;')ilu: te::: tirtg, ;lnrl a!:
lil)f'\al and COill11g a,:til ' il;<:.s, of
t!"e tt.s (t ht>s<: procedu!'cs
f<: ii f!bt! tr.}' :A .. im<-il; r.nd ('iJ
flbdt: l,y t>per, .. ;urs -wh.:n ;.x:.;;,:J Sf)!
<.:it'll: q,;(.q!Otl s , l <>dditi('tn ro <:t':Hpii:f'lc-=
wllh ;uud fotlh.:t!d
(1.!lle;y c; l 59
O ur fndi u!, : n con)\t C,et i:-.rl
k l'IV ::f ... ;l fe;y re:giJJl [iOn kuP<! !r:
... ..... ..1rr:1J'\:
'1fH!t'ltt:1r cra\nir'\S
:'1 ! ine o f Ct ...HH3!'r fo r
p.:bii.; id:-. mw;!c, ,, lihUl!l t.:i.nnlr.g
w \c :<>:;.fen. and the;- a:e tb.: "g.a(ektq>er< for
indolH' t.:V;{ l'."<PQ!>l.tr.e.
t :-a\ning of tht-: 111 be Curr;;n(!y,
m:;jcrity of the- ('(('> nvl ;eq.;ln:
.-:md a li i lH:ly repvned !ow
!-laf(;:( y i ss ti!:!:> ?.di
lt_')W i"!at.'\.' ,,r pr<:"viot,.lo\
int:!\i 4;e fen ft::dC:':'d
ant.l r <:t!\. t c;;-<.:;vtOe ;;
..e:) ..H"r ;:;bt.,tJl :l ('hl
be"l'">eti t.$ i,)f ion by
i l", the :::lnd of
<>f.W i'\'l t()(' woul d ;1eJp t'mi; J'f.: ;f:.e
tr iJf ; J;C: Ct)I IH! O( ,
t;; i<ldcH non r o md. r.>pt.:mtor i r<li ning, -:.JC
c o-...mcy or s:;::e h:tu!rh sy::..
v.:rnari-:al:}' monitor fncil;cy compli:u:<:e . lr. C;l.Hfcrnta,
;, -.;;,>!atior. v f :.1ny o! (he st-He p:misli
:,!)!!:'by r, ilf S'l,Q 11.! $l(XI-))l ffm:.rt:"ve,-,
td rha< cou;:ne
C<l Hfc;nil.t (<id m
ate On :he b:J.'>!s ;;f U.Jrre t
sho1k! ?hY
to p:-a<:(in;s r t::l;.o(' d I.>) rhe of ar.;;)
in c.:>:'H:i us:cm, In <:<ll rtrv wi th ot t...!VR;.:;s
:H'Kl h igh tY1d;,;:oma r-.t;c;,_H.ii 1nany lt\d,:::ux -.:.1nning
9-l ere: J'l()l'\t:orr.ptlam v..: : !l and
Our sugl!\oes' rhm upe;;wr:;
lrt fonn\ng abo;;( ;he:
o f use <:'>f [ anni >.g bet.:s .
insr:ec i\ n ur:d enfort:er;-;e;m {)r
:1to;:g vmh high .. , ;_ l<;Ji:!y
<'OL:ld hdn f<:'thxtt 1c. .. n-.:: r:>.
;_ DS.I!.cnon J. c;v.,., .:s nce r:!>r.s,; i (l! !i
;;lld S3:1iC\IJS ce:l Ai, fini< Gi'\
.. Cani;Qr So<:ivl)l of <:!ir.i.:z.l " "<i:YiO<!J't
Alil'l'\IJ: X.,n Ca ! ;..-1. ;::..
2, S111;J:O.t:.r1 SE. !takll (!v . Rok
Oi. t,.,!.urg;,y GP
1
.!diro:.o;. (i;:J(C ! !tt:<tOvil'r c!
on-:ak>yy .. A:;n!:-ri.ct.r. p.
).6)70.
l , /'l ,O. n ov,:rvit;tw of 'kin it>, ideoc\!
c, .... sul).PI
4. ftJ r n e tt:H)Om.Z
) . .J. Oiss.o .. A. l nq vat (. J l.t-'S5::;r.
\... ot n, ' ui1:o\' rn;l'\ .ln ..:
Sw 11":!ef'l. A' t : EPCI!t>>io! ! \
Mate6al may be protected by copyright i3w (Titl e 17, U.S. Code)
i\, S;;). LO. f'rot.< C. S'hlt>l\01"1 rS. >ley
of 'N>t:)
of Afr. j 1 'Ji :1.32"
43.
7. for ((.}rUJ{)!
:\;lort)
w;...:y
,&:. Ttt., t1e\V
;oclt.:>i <l; lrl.jt.;ry. AI' J l,'l()j !
9. Vi>.. A:ner!O::llf"l ;,;
agr. ct on
:H; sl.tin, O<:wlJer 1 9?}.
g{ I ;::,, 4).
10. l< 1.9vO.OOv.XJ lU ;,.,
F tllr
1
(\'I' W:-1. c;n;,. ev<.l\lil()o'\ of\!'1.:-M;HlO!J !!>:
of tn;,. Na:iac.,;;
M<:h: j/\2): 19')8.
2. jV, KA. tan:-,ins;;: vod
ft.m ACrtG l9'3S;)j:2$398.
;3. o( UVA (o( 3r .}
De 1 1 S:6 7"' 16.
14. Mawn v :1', t. of nnu
rot' !:,i,...j :..iS?.,
) Am (.>;;o.r:..,ato' l
vuHOlty Q(
l ;I'., 2f.>$.$fJ.?
t F<)Q(.i
;i'\fi i)r Xh.;;:. tt !-l(af
::n c,:"' - :J-'0> '"'c
1?. 1 .. ;.r:o S.;!(vkl!s. roo<::
for tt6mrr;etft!) prv-
i2 1 w2c;.
1&. Cdi!fomi ct McalH; of
Att of
/5I C::.d..- f, 23 2':UO'h16
19. :NeA;t:(>< Avai!abie <!.
..
j
L-\"';:.-;s :wen
20. Er,viH>"'"'-'Il.;,! !"',t> !0;\!iMI i>t:
hn p:/ .r,..; yo.JJ'(J t:V ttl;vl'!'\Ccx.
21 . vf t"Ofit:v{
HN<:;.,
l9Sl!>; O;.;HS Nu. ;;CJA) se.a.:B4,
11.. F, :;'5, (,uin JO. Tho! lo<Finp 11!". <!r'l;;
s{..J.rvcy c( A.m
;)"<"'l<>hi.
n. D. ptovict-d <.I.:S
tvmet;; of New City Ar-r. J Med
l.-b/2;.:;,;:m.J.
,tt}. )urv.::.y
vf f ur.-d J ...
1 ffS'1 :24:217
25 S. of 41:--, .. :'d. {C'A}:
199S
;16. (omu:ti or; Afi.:> ;,s, riam' of vlt avicH?t <lti;o.
!ior1. ;
2!, .. Y:J. !).-.d O:ttl
cancer
i=-syc1oi t%12;;::s7i 6.
26, !':. P'oteCtiGi\ a!fo:<l, t:l<:nl'e
. VJ<!C J A.ust 1SS7;14.,,tif5.6.
29. We<tm1od: MA, Coia:t2 GA, WC. .J, Sronsteio
Bf( Pz'Hr-r.l v:. int:)der.t:.e
i1": woln;::O;l .. lO
,98<l;a4: 1<J90:2il4.
){). )Q l; ;;;,.., .,!: ..., ::.1:::' ,:M, <>1 tl.:f1"
by A :"'t J
3' W J. OP. Zl'lvlli M!), Ta(ll''"''-"
w: S.\ate ;r,
Ci'rO!i;><J; il p<:>: J Ac:r 0t-;;r<ll<>o
:.lUi'
3 2. Fit! Jt. ;..B, h.lortn oc tt
-::h.oe J .. 1 "03
33. A.murican :!1\o:i (a!dcr!'\;a.
i.CAi: G.ll'l l9W,.
p,,r;e::c (;<J!"Ki! r y. f .l .);-1-d
........................................... _ ............... _ ....................................................... ]
AVAHABiUTI Of' jOl'RN:\t lSACK 1SSt:ES
/;:;, a fv ;;ub:;,'rih<:r". ;;(\pi<;-::. b;-.k of th-:: ]<:>,rfn:li of ;he 1\l'n.;;<tG;H ,.'\:nde::w <.>f
:or for frorn .. J
is The .. uf r('
\,:-nf;' ofr < ..'ltl :<; . .;e, rift;:.i{ii\ Sc.rvi-:e
1
62!! ti;.irbol [)t, <)rJan:.\(), F.L u;- .. h)t ..
:lt"'iky of p:,nittdar and If fr: :Ju:: ,,(
m;;.y frnw, Bti! & Howeii <t!hi :'\00 I' Z<.:<:i:. Rd, :\.r:r1 Arbor, l\.ii 48 !i)(t,
cs
Matena! may be protected by copyright Jaw (Title 17, u.s. Code)
You might also like
- Relative Importance of Traditional Risk Factors For Malignant Melanoma in The Czech PopulationDocument5 pagesRelative Importance of Traditional Risk Factors For Malignant Melanoma in The Czech PopulationFanialiahsaniNo ratings yet
- Effects On The Skin: SunburnDocument7 pagesEffects On The Skin: SunburnChiragAviyaNo ratings yet
- Skon Cancer Zoe AppalaDocument15 pagesSkon Cancer Zoe AppalabagasNo ratings yet
- Rota Et al-2016-BJOG - An International Journal of Obstetrics & GynaecologyDocument8 pagesRota Et al-2016-BJOG - An International Journal of Obstetrics & GynaecologyMarcel Grignoli da SilvaNo ratings yet
- The Etiology and Epidemiology of Merkel Cell Carcinoma: Curr Probl Cancer 2010 34:14-37. 0147-0272/2010/$34.00 0Document24 pagesThe Etiology and Epidemiology of Merkel Cell Carcinoma: Curr Probl Cancer 2010 34:14-37. 0147-0272/2010/$34.00 0santi lestariNo ratings yet
- International Journal of Engineering Research and DevelopmentDocument8 pagesInternational Journal of Engineering Research and DevelopmentIJERDNo ratings yet
- Holman Et Al. - 1986 - The Causes of Malignant Melanoma Results From TheDocument20 pagesHolman Et Al. - 1986 - The Causes of Malignant Melanoma Results From TheMiguelNo ratings yet
- Journal of Dermatology ResearchDocument17 pagesJournal of Dermatology ResearchAthenaeum Scientific PublishersNo ratings yet
- Antidepressant Medication Use and Breast Cancer RiskDocument6 pagesAntidepressant Medication Use and Breast Cancer RiskinloesNo ratings yet
- Current Cancer Screening IssuesDocument44 pagesCurrent Cancer Screening IssuesNational Press FoundationNo ratings yet
- Sunlight & CancerDocument13 pagesSunlight & CancerMarcoSaliniNo ratings yet
- Insuf Sun ExpoDocument41 pagesInsuf Sun ExpoRafi BouhamoudaNo ratings yet
- Acne and SmokingDocument3 pagesAcne and SmokingHappy FamsNo ratings yet
- Lindqvist Et Al-2014-Journal of Internal Medicine PDFDocument10 pagesLindqvist Et Al-2014-Journal of Internal Medicine PDFAnonymous 2vN7NbQMNo ratings yet
- Articulo 1Document13 pagesArticulo 1Lucero BallesterosNo ratings yet
- Diagnosis and Treatment of Basal Cell and Squamous Cell CarcinomasDocument8 pagesDiagnosis and Treatment of Basal Cell and Squamous Cell CarcinomasAffan AdibNo ratings yet
- Modifiable LifestyleDocument5 pagesModifiable Lifestylemawarni siahaanNo ratings yet
- Digital Dermal Patterns in Carcinoma of BreastDocument4 pagesDigital Dermal Patterns in Carcinoma of BreasteditaNo ratings yet
- Psoriasis treatments and cancer risk updateDocument13 pagesPsoriasis treatments and cancer risk updatemogoscristinaNo ratings yet
- Skin Cancer: Problem: Skin Cancer Is One of The Most Common Types of Cancer in The UK. As ADocument11 pagesSkin Cancer: Problem: Skin Cancer Is One of The Most Common Types of Cancer in The UK. As AlalaNo ratings yet
- Ca CervixDocument17 pagesCa CervixNisa Aprilen GintingNo ratings yet
- A Brief Review: The Epidemiology of Acquired Melanocytic NeviDocument9 pagesA Brief Review: The Epidemiology of Acquired Melanocytic Nevikyle31No ratings yet
- Suggested Answers To Selected Case Studies QuestionsDocument30 pagesSuggested Answers To Selected Case Studies QuestionsSonali NahataNo ratings yet
- Evaluating RisksDocument33 pagesEvaluating RisksDavid TribeNo ratings yet
- Most accurate in-vitro SPF method compared to in-vivo testsDocument4 pagesMost accurate in-vitro SPF method compared to in-vivo testsRosalie BachillerNo ratings yet
- Jid 2009113 ADocument9 pagesJid 2009113 AAMELIA.SYAHUTAMINo ratings yet
- Seminar: Vishal Madan, John T Lear, Rolf-Markus SzeimiesDocument13 pagesSeminar: Vishal Madan, John T Lear, Rolf-Markus SzeimiesAbdul HaseebNo ratings yet
- Basal Cell CDocument7 pagesBasal Cell COjambo FlaviaNo ratings yet
- Routine Dermatologist-Performed Full-Body Skin Examination and Early Melanoma DetectionDocument4 pagesRoutine Dermatologist-Performed Full-Body Skin Examination and Early Melanoma DetectionSeflan Syahir AhliadiNo ratings yet
- Acne Vulgaris 3Document27 pagesAcne Vulgaris 3Ridho ForesNo ratings yet
- Stratification by Unhealthy Weight School Rather Than Age Group Can Easily Discover A Higher Per Cent of Kids at Risk of Nonalcoholic Junk Liver Organ Condition Along With Metabolic Problemscrzqr PDFDocument1 pageStratification by Unhealthy Weight School Rather Than Age Group Can Easily Discover A Higher Per Cent of Kids at Risk of Nonalcoholic Junk Liver Organ Condition Along With Metabolic Problemscrzqr PDFfrancealley77No ratings yet
- HPV testing and colposcopy reduce repeat smears and detect cervical lesionsDocument3 pagesHPV testing and colposcopy reduce repeat smears and detect cervical lesionsAdi PranataNo ratings yet
- Bataille 2004Document7 pagesBataille 2004Bobby JimNo ratings yet
- Tutoriaula 4 ContraseptionDocument15 pagesTutoriaula 4 Contraseptionrsudlubas14% (7)
- Reading 56 PDFDocument25 pagesReading 56 PDFMegha Elizebath PhilipNo ratings yet
- Ductal Carcinoma in SituDocument7 pagesDuctal Carcinoma in SituLittle DevNo ratings yet
- 2016 Matthews Cohort StudiesDocument8 pages2016 Matthews Cohort StudiesLea KallassiNo ratings yet
- Clinicopathological Study of 303 Salivary Gland Tumor PatientsDocument6 pagesClinicopathological Study of 303 Salivary Gland Tumor PatientsreioctabianoNo ratings yet
- Breast Cancer Review ArticleDocument9 pagesBreast Cancer Review ArticleMehtab AhmedNo ratings yet
- Primary Multiple Skin MelanomasDocument8 pagesPrimary Multiple Skin MelanomasCentral Asian StudiesNo ratings yet
- MRI distinguishes serous from non-serous epithelial ovarian cancersDocument12 pagesMRI distinguishes serous from non-serous epithelial ovarian cancersZannuba NoorNo ratings yet
- Scand J Work Environ Health:3-7: Environmental Risk Factors of Breast CancerDocument6 pagesScand J Work Environ Health:3-7: Environmental Risk Factors of Breast CancerKhush BhullarNo ratings yet
- Screening & Diagnostic MammographyDocument53 pagesScreening & Diagnostic Mammographymir-medicinaNo ratings yet
- Brief CommunicationDocument13 pagesBrief CommunicationsantovazNo ratings yet
- Stroke Among Cancer Patients: ArticleDocument8 pagesStroke Among Cancer Patients: Articlevinit sharmaNo ratings yet
- Comparative Study of 5 % Potassium Hydroxide Solution Versus 0.05% Tretinoin Cream For Molluscum Contagiosum in ChildrenDocument4 pagesComparative Study of 5 % Potassium Hydroxide Solution Versus 0.05% Tretinoin Cream For Molluscum Contagiosum in ChildrenMitha Sari IINo ratings yet
- Cancer - 2005 - Kirova - Radiation Induced Sarcomas After Radiotherapy For Breast CarcinomaDocument8 pagesCancer - 2005 - Kirova - Radiation Induced Sarcomas After Radiotherapy For Breast CarcinomaRizki Amalia JuwitaNo ratings yet
- Epidemiologyandrisk Factorsofmelanoma: Stephanie Carr,, Christy Smith,, Jessica WernbergDocument12 pagesEpidemiologyandrisk Factorsofmelanoma: Stephanie Carr,, Christy Smith,, Jessica WernbergGabriela AgrigNo ratings yet
- UV CANCER STUDYDocument10 pagesUV CANCER STUDYAlexander HunterNo ratings yet
- Research Paper On Skin CancerDocument7 pagesResearch Paper On Skin Cancernywxluvkg100% (1)
- Gabriel Luciper in DetailsDocument13 pagesGabriel Luciper in DetailsSuresh IndiaNo ratings yet
- Answer of Exercises-Measures of Disease FrequencyDocument7 pagesAnswer of Exercises-Measures of Disease Frequencysanjivdas100% (4)
- Mitochondrial DNA Copy Number and Lung Cancer Risk in A Prospective Cohort StudyDocument3 pagesMitochondrial DNA Copy Number and Lung Cancer Risk in A Prospective Cohort StudyZrt Angie BautizztaNo ratings yet
- Skin CancerDocument3 pagesSkin CancerourskrishNo ratings yet
- B Relative Risk and Odds Ratios ExamplesDocument8 pagesB Relative Risk and Odds Ratios ExamplesJing CruzNo ratings yet
- Jurnal CA TyroidDocument4 pagesJurnal CA TyroidErvina ZelfiNo ratings yet
- PIIS2213398422000902Document7 pagesPIIS2213398422000902Manas BhatiaNo ratings yet
- Acne Scars Journal FinalDocument18 pagesAcne Scars Journal FinalSanti NurfitrianiNo ratings yet
- MelanomaDocument10 pagesMelanomaShalu RjNo ratings yet
- Understand Cancer & Reduce Cancer Risk - Based On The Teachings Of Dr. Andrew Huberman: Empowering You To Safeguard Against ItFrom EverandUnderstand Cancer & Reduce Cancer Risk - Based On The Teachings Of Dr. Andrew Huberman: Empowering You To Safeguard Against ItNo ratings yet
- 2016 12 30 Responsive DocumentsDocument15 pages2016 12 30 Responsive DocumentsCREWNo ratings yet
- Via Electronic Mail OnlyDocument2 pagesVia Electronic Mail OnlyCREWNo ratings yet
- 2016 12 28 Final ResponseDocument2 pages2016 12 28 Final ResponseCREWNo ratings yet
- 2016 12 16 FOIA RequestDocument3 pages2016 12 16 FOIA RequestCREWNo ratings yet
- New York Office of The Attorney General (Trump Foundation Investigation) Request 9-14-16Document2 pagesNew York Office of The Attorney General (Trump Foundation Investigation) Request 9-14-16CREWNo ratings yet
- 2017-01-06 Documents Produced 1Document365 pages2017-01-06 Documents Produced 1CREWNo ratings yet
- 2017-01-06 Documents Produced 2Document36 pages2017-01-06 Documents Produced 2CREWNo ratings yet
- 2016 12 16 FOIA RequestDocument3 pages2016 12 16 FOIA RequestCREWNo ratings yet
- 2017-01-06 Final ResponseDocument2 pages2017-01-06 Final ResponseCREWNo ratings yet
- 2016-12-21 FOIA Request (Documents To Congress)Document3 pages2016-12-21 FOIA Request (Documents To Congress)CREWNo ratings yet
- 2016-12-21 FOIA Request (Communications With Trump and Congress)Document3 pages2016-12-21 FOIA Request (Communications With Trump and Congress)CREWNo ratings yet
- 2016 12 16 FOIA RequestDocument3 pages2016 12 16 FOIA RequestCREWNo ratings yet
- FBI Denial 12-1-2016Document2 pagesFBI Denial 12-1-2016CREWNo ratings yet
- FOIA Request - OGE (Trump Transition) 12-7-16Document3 pagesFOIA Request - OGE (Trump Transition) 12-7-16CREWNo ratings yet
- Florida Office of The Attorney General (Daily Schedules and Travel) Request 9-14-16Document5 pagesFlorida Office of The Attorney General (Daily Schedules and Travel) Request 9-14-16CREWNo ratings yet
- Plaintiffs' Reply in Support of Motion For Preliminary InjunctionDocument2 pagesPlaintiffs' Reply in Support of Motion For Preliminary InjunctionCREWNo ratings yet
- FBN Materials 422.15Document64 pagesFBN Materials 422.15CREWNo ratings yet
- FOIA Request - OGE (Trump Tweets) 12-6-16Document3 pagesFOIA Request - OGE (Trump Tweets) 12-6-16CREWNo ratings yet
- FBI (Giuliani Communications) 11-22-16Document3 pagesFBI (Giuliani Communications) 11-22-16CREWNo ratings yet
- Final Response Letter 10-17-2016Document2 pagesFinal Response Letter 10-17-2016CREWNo ratings yet
- FBI Denial 12-1-2016Document2 pagesFBI Denial 12-1-2016CREWNo ratings yet
- Final Installment 10-17-2016Document47 pagesFinal Installment 10-17-2016CREWNo ratings yet
- FBI Denial 11-29-2016Document1 pageFBI Denial 11-29-2016CREWNo ratings yet
- Plaintiffs' Memorandum in Support of Motion For Temporary InjunctionDocument6 pagesPlaintiffs' Memorandum in Support of Motion For Temporary InjunctionCREWNo ratings yet
- FBI (Congress Communications Re Comey Letter) 11-22-16Document3 pagesFBI (Congress Communications Re Comey Letter) 11-22-16CREWNo ratings yet
- Second Declaration of James L. MartinDocument9 pagesSecond Declaration of James L. MartinCREWNo ratings yet
- FBI (Kallstrom Communications) 11-22-16Document3 pagesFBI (Kallstrom Communications) 11-22-16CREWNo ratings yet
- Complaint For Declaratory Judgment, Temporary and Permanent InjunctionDocument8 pagesComplaint For Declaratory Judgment, Temporary and Permanent InjunctionCREWNo ratings yet
- Memorandum in Opposition To Plaintiffs' Motion For Temporary Injunction and Declaration of Amy Frederick With ExhibitsDocument19 pagesMemorandum in Opposition To Plaintiffs' Motion For Temporary Injunction and Declaration of Amy Frederick With ExhibitsCREWNo ratings yet
- Amended Complaint For Declaratory Judgment, Temporary, and Permanent InjunctionDocument22 pagesAmended Complaint For Declaratory Judgment, Temporary, and Permanent InjunctionCREWNo ratings yet
- CASE PRESENTATION ON CAD-UNSTABLE ANGINA, HYPOKALEMIA, PARONYCHIADocument18 pagesCASE PRESENTATION ON CAD-UNSTABLE ANGINA, HYPOKALEMIA, PARONYCHIASafoora RafeeqNo ratings yet
- Cer 212 Urinary Incontinence Updated 1Document643 pagesCer 212 Urinary Incontinence Updated 1rahmat_husein1No ratings yet
- D20rha25 2013-1Document2 pagesD20rha25 2013-1Icmi KadarsihNo ratings yet
- Periodic Test in MAPEHDocument5 pagesPeriodic Test in MAPEHRudyard MoranteNo ratings yet
- DH 0223Document10 pagesDH 0223The Delphos HeraldNo ratings yet
- Cast, Brace, Traction CompilationDocument13 pagesCast, Brace, Traction CompilationMar Ordanza100% (1)
- Traditional Medicine: Heated Moxibustion and Bloodletting in Tibetan Medical Literature of Dunhuang HeritageDocument3 pagesTraditional Medicine: Heated Moxibustion and Bloodletting in Tibetan Medical Literature of Dunhuang HeritageAigo Seiga CastroNo ratings yet
- Mh-Somatic Symptom Disorders - 2Document9 pagesMh-Somatic Symptom Disorders - 2martinNo ratings yet
- OBESITY Management by NATUROPATHY and YOGADocument80 pagesOBESITY Management by NATUROPATHY and YOGAKanak Soni100% (1)
- OBDocument7 pagesOBWilmaBongotanPadawilNo ratings yet
- EMP Env. Law in NepalDocument43 pagesEMP Env. Law in NepalSeba Videla GNo ratings yet
- 11-Rely Too Much On DoctorsDocument3 pages11-Rely Too Much On DoctorsThu TrangNo ratings yet
- First AidDocument4 pagesFirst Aidrebz100% (1)
- Lipaglyn Product MonographDocument64 pagesLipaglyn Product Monographanurag3069No ratings yet
- Complementary and supplementary feeding essentialsDocument23 pagesComplementary and supplementary feeding essentialsArchana100% (1)
- References: Plant Profile, Phytochemistry and Pharmacology of Argemone Mexicana Linn.A ReviewDocument1 pageReferences: Plant Profile, Phytochemistry and Pharmacology of Argemone Mexicana Linn.A ReviewSachin DatkhileNo ratings yet
- EbolaDocument4 pagesEbolaapi-271224704No ratings yet
- Craniofacial Surgery Dx and Tx TechniquesDocument103 pagesCraniofacial Surgery Dx and Tx TechniquesSiddharth DhanarajNo ratings yet
- MCQ 1Document4 pagesMCQ 1Maxine foyeNo ratings yet
- Universidad de Zamboanga CPT GuideDocument17 pagesUniversidad de Zamboanga CPT GuideShanayra Ismael JayajiNo ratings yet
- Internet Addiction - Prevalenc PDFDocument158 pagesInternet Addiction - Prevalenc PDFDrAvik ChakrabortyNo ratings yet
- Deepbite & Open BiteDocument36 pagesDeepbite & Open BiteNoor Zia100% (1)
- Part 7 Pyeloroplasty: Quick and BloodlessDocument31 pagesPart 7 Pyeloroplasty: Quick and BloodlessAnonymous MmiBnqnDyNo ratings yet
- Acyanotic Congenital Heart Disease With Increased Pulmonary Blood FlowDocument9 pagesAcyanotic Congenital Heart Disease With Increased Pulmonary Blood Flowdrhomiedan100% (1)
- How Do We Take Care of Our Endocrine SystemDocument7 pagesHow Do We Take Care of Our Endocrine SystemAndrei CunananNo ratings yet
- Ineffective Tissue Perfusion NCPDocument5 pagesIneffective Tissue Perfusion NCPJasmin Calata50% (2)
- 9a The Usui Treatment GuideDocument7 pages9a The Usui Treatment Guideapi-26172340100% (1)
- Introduction to Insurance Agents and Customer ServiceDocument46 pagesIntroduction to Insurance Agents and Customer ServicePolireddy Venna100% (2)
- SUBJECT VERB AGREEMENT LET ReviewerDocument2 pagesSUBJECT VERB AGREEMENT LET ReviewerMacky ReyesNo ratings yet
- Porcelain Fused To Metal (PFM) Crowns and Caries in Adjacent TeetDocument5 pagesPorcelain Fused To Metal (PFM) Crowns and Caries in Adjacent Teetbaiq rengganis dewiNo ratings yet