You might also like
- Interact 2Document11 pagesInteract 2Rivan HoNo ratings yet
- Communicating Bad NewsDocument12 pagesCommunicating Bad NewsRudra Pratap SinghNo ratings yet
- 3 Delivering Bad NewsDocument11 pages3 Delivering Bad NewsAry Nahdiyani Amalia100% (1)
- 6 Breaking Bad NewsDocument32 pages6 Breaking Bad NewsAry Nahdiyani AmaliaNo ratings yet
- Pathogenesis Typhoid Fever PDFDocument7 pagesPathogenesis Typhoid Fever PDFAry Nahdiyani Amalia100% (1)
- Hydrocephalus in Adults: Questions I Have: (Hi-dro-SEF-ah-lus) What Is Hydrocephalus?Document8 pagesHydrocephalus in Adults: Questions I Have: (Hi-dro-SEF-ah-lus) What Is Hydrocephalus?anntjitNo ratings yet
- Value of CT in The Diagnosis and Management of Gallstone IleusDocument6 pagesValue of CT in The Diagnosis and Management of Gallstone IleusAry Nahdiyani AmaliaNo ratings yet
- Low Dose CTDocument5 pagesLow Dose CTAry Nahdiyani AmaliaNo ratings yet
- PseudoanaurysmDocument6 pagesPseudoanaurysmAry Nahdiyani AmaliaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 8 Most Common College DiseasesDocument1 page8 Most Common College Diseasesliezl_alvarez_1No ratings yet
- Aminoglycoside PharmacokineticsDocument13 pagesAminoglycoside PharmacokineticsLama SaudNo ratings yet
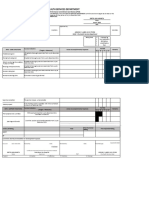
- City Health Services IPCR Performance ReviewDocument8 pagesCity Health Services IPCR Performance ReviewLiecel Valdez100% (2)
- ΕΜΠΥΡΕΤΟ EKPADocument25 pagesΕΜΠΥΡΕΤΟ EKPAElenaNo ratings yet
- Hazardous Materials Management Plan SMDocument26 pagesHazardous Materials Management Plan SMdarmayunitaNo ratings yet
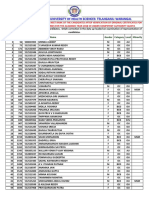
- 1430 Mbbsbdsfinalmeritlist201819 PDFDocument205 pages1430 Mbbsbdsfinalmeritlist201819 PDFVINEETH VinnuNo ratings yet
- Medical Office Management PDFDocument9 pagesMedical Office Management PDFAyessa Joy Tajale100% (1)
- Rheumatoid Arthritis - Lecture SlidesDocument59 pagesRheumatoid Arthritis - Lecture SlidesAndrie GunawanNo ratings yet
- Syndromic Management of Sexually Transmitted InfectionsDocument76 pagesSyndromic Management of Sexually Transmitted Infectionsnamita100% (2)
- Perioperative Nursing Care 1Document17 pagesPerioperative Nursing Care 1Kristian Dave DivaNo ratings yet
- NCM 105 - Infancy NutritionDocument3 pagesNCM 105 - Infancy NutritionCrisheila Sarah PiedadNo ratings yet
- Gradual Dose Reduction Schedule for Psychopharmacological DrugsDocument5 pagesGradual Dose Reduction Schedule for Psychopharmacological DrugsAhmad Mujahid Huzaidi100% (1)
- ACOGAnnualMeeteing Final Program416 1Document218 pagesACOGAnnualMeeteing Final Program416 1BimoNo ratings yet
- Modul 1. Patofisiologi ACSDocument24 pagesModul 1. Patofisiologi ACSFadhilAfifNo ratings yet
- Cardiac Case StudyDocument3 pagesCardiac Case Studydsaitta108No ratings yet
- PEDIATRICS Timetable 5yr, Rot2, Sem1!20!22-NewDocument7 pagesPEDIATRICS Timetable 5yr, Rot2, Sem1!20!22-NewMawanda NasserNo ratings yet
- Questcor ActharDocument6 pagesQuestcor ActharRida el HamdaniNo ratings yet
- Intern Survival Guide Ward 2Document44 pagesIntern Survival Guide Ward 2Keith Swait Zin50% (2)
- Bme ReportDocument15 pagesBme ReportnikitatayaNo ratings yet
- Apert Syndrome - Sultan BaroamaimDocument37 pagesApert Syndrome - Sultan BaroamaimsultanNo ratings yet
- Every Patient Tells A Story by Lisa Sanders, M.D. - ExcerptDocument24 pagesEvery Patient Tells A Story by Lisa Sanders, M.D. - ExcerptCrown Publishing Group76% (17)
- Treatment Outcome and Factors Affecting Time To Recovery in Children With Severe Acute Malnutrition Treated at Outpatient Therapeutic Care ProgramDocument11 pagesTreatment Outcome and Factors Affecting Time To Recovery in Children With Severe Acute Malnutrition Treated at Outpatient Therapeutic Care ProgramMelkamuMeridNo ratings yet
- Education For Parents Regarding Choking Prevention and Handling On Children: A Scoping ReviewDocument8 pagesEducation For Parents Regarding Choking Prevention and Handling On Children: A Scoping ReviewIJPHSNo ratings yet
- September Issue 3 MCJ 36 Pages 2022Document36 pagesSeptember Issue 3 MCJ 36 Pages 2022Sathvika BNo ratings yet
- Infant Feeding Record May 2022Document1 pageInfant Feeding Record May 2022Cyril JaneNo ratings yet
- Crossfit Gym Membership Contract and Receipt TemplateDocument6 pagesCrossfit Gym Membership Contract and Receipt Templatemohit jNo ratings yet
- Low Back Pain Case Study - A Nasty One! But A Good Outcome. - Witty, Pask & BuckinghamDocument4 pagesLow Back Pain Case Study - A Nasty One! But A Good Outcome. - Witty, Pask & BuckinghamermanmahendraNo ratings yet
- AQA Immunity Booklet AnswersDocument6 pagesAQA Immunity Booklet AnswersJames ChongNo ratings yet
- Immunology - Chapter 1 OverviewDocument28 pagesImmunology - Chapter 1 OverviewJJHHJHi100% (1)
- Mei Penyakit UmumDocument1 pageMei Penyakit Umumghaniangga11No ratings yet