You might also like
- 1833 Manuscript 7430 1 10 20180428Document6 pages1833 Manuscript 7430 1 10 20180428sagarNo ratings yet
- 1 Ajaz 2012Document4 pages1 Ajaz 2012Olivia Valentine LekiNo ratings yet
- Hypocalcemia Pada Beta Thalassemia PDFDocument3 pagesHypocalcemia Pada Beta Thalassemia PDFYohana Elisabeth GultomNo ratings yet
- Hipernatremia en UCIDocument7 pagesHipernatremia en UCIcolo_med1077No ratings yet
- Endocrine abnormalities in children with beta thalassemia majorDocument6 pagesEndocrine abnormalities in children with beta thalassemia majorKrisbiyantoroAriesNo ratings yet
- Evaluation of Orofacial Manifestations in 50 Thalassemic Patients: A Clinical StudyDocument0 pagesEvaluation of Orofacial Manifestations in 50 Thalassemic Patients: A Clinical StudyMeilinda AmeiNo ratings yet
- My ThesisDocument10 pagesMy Thesishinduja reddipilliNo ratings yet
- Thalassemia in Iraq Review Article: AbstractDocument4 pagesThalassemia in Iraq Review Article: AbstractRana RaedNo ratings yet
- Thyroid disorders linked to anaemia in Saudi womenDocument15 pagesThyroid disorders linked to anaemia in Saudi womenBassem RefaatNo ratings yet
- Juinjo Abdul MananDocument6 pagesJuinjo Abdul MananMuhammad Hadi ArwaniNo ratings yet
- Chronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsDocument7 pagesChronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsAnonymous FgT04krgymNo ratings yet
- Nej MoDocument9 pagesNej MoNadia Mrz Mattew MuseNo ratings yet
- Diabetes Mellitus in Thalassaemia Major Patients: A Report From The Southeast of IranDocument4 pagesDiabetes Mellitus in Thalassaemia Major Patients: A Report From The Southeast of IrandesilasarybasriNo ratings yet
- Jurnal Thalassemia 4Document10 pagesJurnal Thalassemia 4Lina AnisaNo ratings yet
- Pediatric Transfusion Guidelines ReviewDocument14 pagesPediatric Transfusion Guidelines ReviewAndrea Abigail ChacónNo ratings yet
- Penyakit Ginjal KronikDocument38 pagesPenyakit Ginjal KronikheigymutihaNo ratings yet
- Chen 2013Document6 pagesChen 2013malaNo ratings yet
- Nephrotic Syndrome in Children ProfileDocument8 pagesNephrotic Syndrome in Children ProfilePriyanka BordiyaNo ratings yet
- Causes and Characteristics of Lower GI Bleeding in Iranian ChildrenDocument8 pagesCauses and Characteristics of Lower GI Bleeding in Iranian Childrendr.herusetiawanNo ratings yet
- Clinical Outcome of Donors PDFDocument7 pagesClinical Outcome of Donors PDFEngidaNo ratings yet
- Anemia 1Document8 pagesAnemia 1Patrick ValentinoNo ratings yet
- Research Article: Correlations Between Iron Load and CD4 in Adult Transfusion-Dependent Beta ThalassemiaDocument5 pagesResearch Article: Correlations Between Iron Load and CD4 in Adult Transfusion-Dependent Beta ThalassemiaHyacinth A RotaNo ratings yet
- J Coll Physicians Surg Pak 2018 28 3 206 209Document4 pagesJ Coll Physicians Surg Pak 2018 28 3 206 209Naman KhalidNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 16: HematologyFrom EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyNo ratings yet
- Pattern of Acute Renal Failure at A Referral HospitalDocument7 pagesPattern of Acute Renal Failure at A Referral HospitalminhajulqowimNo ratings yet
- Jurnal 5 - HDFDocument8 pagesJurnal 5 - HDFAndi RiansyahNo ratings yet
- Acute Kidney InjuryDocument50 pagesAcute Kidney InjuryRifhani Atthaya PutriNo ratings yet
- Manuscript 1Document4 pagesManuscript 1maryNo ratings yet
- Molecular, Biochemical and Hematological Investigations of - Thalassemia Children in Bannu KPK PakistanDocument8 pagesMolecular, Biochemical and Hematological Investigations of - Thalassemia Children in Bannu KPK PakistanInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarDocument9 pagesA Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarLianSiahaanNo ratings yet
- A Phase 3 Trial of Luspatercept in Patients with Transfusion-Dependent β-ThalassemiaDocument13 pagesA Phase 3 Trial of Luspatercept in Patients with Transfusion-Dependent β-ThalassemiaSandra SolanoNo ratings yet
- Tilak Gharat Case Report On Acute Renal FailureDocument4 pagesTilak Gharat Case Report On Acute Renal FailureOm PalekarNo ratings yet
- Diabetes Mellitus in Children Suffering From /?-ThalassaemiaDocument6 pagesDiabetes Mellitus in Children Suffering From /?-ThalassaemiadesilasarybasriNo ratings yet
- Anemia After Kidney Transplantation in Adult Recipients Prevalence and Risk Factors (Đã In)Document3 pagesAnemia After Kidney Transplantation in Adult Recipients Prevalence and Risk Factors (Đã In)Mỹ HoàiNo ratings yet
- Renal Calyceal MicrolithiasisDocument3 pagesRenal Calyceal MicrolithiasisVic L. AmecaNo ratings yet
- 469 FullDocument7 pages469 FullCristina Adriana PopaNo ratings yet
- Management of Beta Thalassaemia in Pregnancy: Green-Top Guideline No. 66Document17 pagesManagement of Beta Thalassaemia in Pregnancy: Green-Top Guideline No. 66Ajiss MahriNo ratings yet
- Hyponatremia in The Dialysis PopulationDocument12 pagesHyponatremia in The Dialysis PopulationRESIDENTES MEDICINA INTERNANo ratings yet
- Clinical Profile and Outcome in Children of Dengue Hemorrhagic Fever in North IndiaDocument7 pagesClinical Profile and Outcome in Children of Dengue Hemorrhagic Fever in North IndiaAna Rosida SafwanNo ratings yet
- Prevalence of Hypothyroidism in Beta-Thalassemia PatientsDocument6 pagesPrevalence of Hypothyroidism in Beta-Thalassemia Patientshinduja reddipilliNo ratings yet
- Thyroid Dysfunction and Anaemia in A Large Population-Based StudyDocument5 pagesThyroid Dysfunction and Anaemia in A Large Population-Based StudyRaissa Metasari TantoNo ratings yet
- Hypothyroidism and Serum Ferritin Level in Patients With Major SS ThalassemiaDocument4 pagesHypothyroidism and Serum Ferritin Level in Patients With Major SS ThalassemiaRatu Meutia ArythaNo ratings yet
- Original ArticleDocument4 pagesOriginal ArticleGoto LaluNo ratings yet
- Jurnal MalariaDocument2 pagesJurnal MalariadjebrutNo ratings yet
- CorrelationDocument4 pagesCorrelationrasyidah hasanNo ratings yet
- Iron Deficiency Anemia and Associated Risk Factors Among Teenagers in Najran Saudi ArabiaDocument9 pagesIron Deficiency Anemia and Associated Risk Factors Among Teenagers in Najran Saudi ArabiaZkdlin kaiNo ratings yet
- Risk For Anemia in Pediatric Chronic Kidney Disease Patients: A Report of NAPRTCSDocument8 pagesRisk For Anemia in Pediatric Chronic Kidney Disease Patients: A Report of NAPRTCSchrispeonkNo ratings yet
- Rawalpindi Army Hosp HypothyDocument5 pagesRawalpindi Army Hosp Hypothyhinduja reddipilliNo ratings yet
- Clinical CourseDocument6 pagesClinical CoursePratistha SatyanegaraNo ratings yet
- Ref 14 PDFDocument9 pagesRef 14 PDFFausiah Ulva MNo ratings yet
- Iron Overload in Beta Thalassemia PDFDocument5 pagesIron Overload in Beta Thalassemia PDFyesikaNo ratings yet
- Rhabdomyolysis AbstractDocument1 pageRhabdomyolysis Abstractapi-284057899No ratings yet
- A Premature Neonate LueucicitosisDocument3 pagesA Premature Neonate Lueucicitosisgonococo29No ratings yet
- Beta - Thalassemia Trait - Epidemiological and Clinical Aspects in Children in Constanta CountyDocument9 pagesBeta - Thalassemia Trait - Epidemiological and Clinical Aspects in Children in Constanta CountyAnika Restu PradiniNo ratings yet
- Presymptomatic Hyperuricemia Risks and TreatmentDocument46 pagesPresymptomatic Hyperuricemia Risks and TreatmentDivya Shree100% (1)
- IraqDocument11 pagesIraqKhalifa Al-SulaitiNo ratings yet
- Funcion RenalDocument11 pagesFuncion RenalCarlos AvalosNo ratings yet
- Hyperuricemia Is Associated With Hypertension, Obesity, and Albuminuria in Children With Chronic Kidney DiseaseDocument5 pagesHyperuricemia Is Associated With Hypertension, Obesity, and Albuminuria in Children With Chronic Kidney DiseaseMuh Husni RifaiNo ratings yet
- What Is Thalassemia PDFDocument4 pagesWhat Is Thalassemia PDFexamman123No ratings yet
- 348-Main Article Text (Blinded Article File) - 656-1-10-20171122 PDFDocument4 pages348-Main Article Text (Blinded Article File) - 656-1-10-20171122 PDFEmillya SariNo ratings yet
- Hearing Loss9Document12 pagesHearing Loss9Pratita Jati PermatasariNo ratings yet
- FTT 8Document59 pagesFTT 8Pratita Jati PermatasariNo ratings yet
- Assess Child Growth and Causes of Failure to ThriveDocument49 pagesAssess Child Growth and Causes of Failure to ThrivePratita Jati PermatasariNo ratings yet
- The Cognitive Phenotype in Klinefelter Syndrome: A Review of The Literature Including Genetic and Hormonal FactorsDocument21 pagesThe Cognitive Phenotype in Klinefelter Syndrome: A Review of The Literature Including Genetic and Hormonal FactorsPratita Jati PermatasariNo ratings yet
- Klinefelter 1Document2 pagesKlinefelter 1Pratita Jati PermatasariNo ratings yet
- Failure To Thrive: American Family Physician October 2003Document7 pagesFailure To Thrive: American Family Physician October 2003Pratita Jati PermatasariNo ratings yet
- Klinefelter 29Document4 pagesKlinefelter 29Pratita Jati PermatasariNo ratings yet
- Klinefelter 5Document7 pagesKlinefelter 5Pratita Jati PermatasariNo ratings yet
- Klinefelter 8Document13 pagesKlinefelter 8Pratita Jati PermatasariNo ratings yet
- Klinefelter 7 PDFDocument44 pagesKlinefelter 7 PDFPratita Jati PermatasariNo ratings yet
- Klinefelter 6Document5 pagesKlinefelter 6Pratita Jati PermatasariNo ratings yet
- Klinefelter 3Document12 pagesKlinefelter 3Pratita Jati PermatasariNo ratings yet
- ICU Rounds: Pulmonary Leukostasis as a Complication of LeukemiaDocument6 pagesICU Rounds: Pulmonary Leukostasis as a Complication of LeukemiaPratita Jati PermatasariNo ratings yet
- Chapter 5: Electrolyte and Acid - Base Disorders in MalignancyDocument7 pagesChapter 5: Electrolyte and Acid - Base Disorders in MalignancyPratita Jati PermatasariNo ratings yet
- Klinefelter 2Document18 pagesKlinefelter 2Pratita Jati PermatasariNo ratings yet
- ALL Infiltrasi ParuDocument5 pagesALL Infiltrasi ParuPratita Jati PermatasariNo ratings yet
- Klinefelter ChildhoodDocument9 pagesKlinefelter ChildhoodPratita Jati PermatasariNo ratings yet
- (From J.N. Medical College, Aligarh) : Pulmonary Tuberculosis and LeukemiaDocument3 pages(From J.N. Medical College, Aligarh) : Pulmonary Tuberculosis and LeukemiaPratita Jati PermatasariNo ratings yet
- ALL+gizbur 9Document8 pagesALL+gizbur 9Pratita Jati PermatasariNo ratings yet
- ALL CND p8Document7 pagesALL CND p8Pratita Jati PermatasariNo ratings yet
- ALL Infiltrasi N XIIDocument1 pageALL Infiltrasi N XIIPratita Jati PermatasariNo ratings yet
- Tuberculosis in Acute Leukemia: A Clinico-Hematological ProfileDocument7 pagesTuberculosis in Acute Leukemia: A Clinico-Hematological ProfilePratita Jati PermatasariNo ratings yet
- ALL FeverDocument5 pagesALL FeverPratita Jati PermatasariNo ratings yet
- ALL+gizbur 6Document8 pagesALL+gizbur 6Pratita Jati PermatasariNo ratings yet
- ALL+infiltrasi IntrakranialDocument8 pagesALL+infiltrasi IntrakranialPratita Jati PermatasariNo ratings yet
- ALL Parese Nervus 3Document4 pagesALL Parese Nervus 3Pratita Jati PermatasariNo ratings yet
- ALL GizburDocument3 pagesALL GizburPratita Jati PermatasariNo ratings yet
- 2864Document5 pages2864kemalmiaNo ratings yet
- ALL+gizbur 2Document4 pagesALL+gizbur 2Pratita Jati PermatasariNo ratings yet
- ALL CnsDocument29 pagesALL CnsPratita Jati PermatasariNo ratings yet
- Asanthe Case WorkingsDocument9 pagesAsanthe Case Workingsazhar hussainNo ratings yet
- Preboards 3 Nursing Practice 2 Nov 2021 PDFDocument12 pagesPreboards 3 Nursing Practice 2 Nov 2021 PDFBanana Q0% (1)
- Pediatric Vital Signs Reference Chart PedsCasesDocument1 pagePediatric Vital Signs Reference Chart PedsCasesAghnia NafilaNo ratings yet
- Gray's Anatomy OnlineDocument2 pagesGray's Anatomy OnlineMatthew AxeNo ratings yet
- CORDOCENTESISDocument6 pagesCORDOCENTESISSagar HanamasagarNo ratings yet
- Karl StorzDocument84 pagesKarl StorzWaleed HashimNo ratings yet
- Fast Localised Abdominal Sonography Protocol for Horses with Colic (FLASHDocument6 pagesFast Localised Abdominal Sonography Protocol for Horses with Colic (FLASHludiegues752No ratings yet
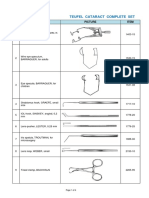
- TEUFEL CATARACT COMPLETE EYE SURGERY SETDocument4 pagesTEUFEL CATARACT COMPLETE EYE SURGERY SETjoe BudiNo ratings yet
- With 650 Bed-Capacity: Staff Nurse Progressive Care Unit-PulmonaryDocument3 pagesWith 650 Bed-Capacity: Staff Nurse Progressive Care Unit-PulmonaryMersalynNo ratings yet
- Medical Tourism HungaryDocument16 pagesMedical Tourism HungaryAnonymous rlXovJGGbNo ratings yet
- Somatom Sessions 16Document42 pagesSomatom Sessions 16Herick SavioneNo ratings yet
- Clinical Abstract (2nd Sem 1st Rotation)Document3 pagesClinical Abstract (2nd Sem 1st Rotation)Michael Gino SarenasNo ratings yet
- PRC Form CasesDocument5 pagesPRC Form CasesAyen Fajardo-HernalNo ratings yet
- General PhysicianDocument3 pagesGeneral PhysicianDiaa MazatyNo ratings yet
- OBGYN Form 4 Take VersionDocument60 pagesOBGYN Form 4 Take VersionValentina BustamanteNo ratings yet
- Transplacental Transmission of The COVID-19 Vaccine MRNA Evidence From Placental, Maternal and Cord Blood Analyses Post-VaccinationDocument13 pagesTransplacental Transmission of The COVID-19 Vaccine MRNA Evidence From Placental, Maternal and Cord Blood Analyses Post-VaccinationP. MihailNo ratings yet
- The Textbook of Clinical Sexual Medicine 2017 PDFDocument634 pagesThe Textbook of Clinical Sexual Medicine 2017 PDFNitika Sinha100% (3)
- Community Outreach ProgramsDocument5 pagesCommunity Outreach ProgramskaranreguNo ratings yet
- Sga 3Document7 pagesSga 3Shane PangilinanNo ratings yet
- 25 Types of Surgical RetractorsDocument5 pages25 Types of Surgical RetractorsJerome Vergel RubianesNo ratings yet
- Manual ObsteDocument1,237 pagesManual ObsterobingpNo ratings yet
- Caesar Surgical Safety ChecklistDocument1 pageCaesar Surgical Safety Checklistdrg. Bobet Evih Hedi I.R., MMRNo ratings yet
- 34CDEFIJKLSTUWYZ001000000000084296Document1 page34CDEFIJKLSTUWYZ001000000000084296Saiq ArshadNo ratings yet
- 10.daftar Pustaka Kti Fauzan Kurniawan 20130310054Document2 pages10.daftar Pustaka Kti Fauzan Kurniawan 20130310054Adeliana SutamiNo ratings yet
- Gynecology and Contraception TopicsDocument24 pagesGynecology and Contraception Topicslizzy596No ratings yet
- 1 Relaxing The Pelvic Floor For Tai Chi and Zhan ZhuangDocument7 pages1 Relaxing The Pelvic Floor For Tai Chi and Zhan ZhuangLiew Yetmeng100% (1)
- Emergent Management of Pleural EffusionsDocument11 pagesEmergent Management of Pleural EffusionsyuliNo ratings yet
- ACOG Practice Bulletin No093 PDFDocument11 pagesACOG Practice Bulletin No093 PDFMarco DiestraNo ratings yet
- Finalprinting-NPM Curriculum03-12-2020Document82 pagesFinalprinting-NPM Curriculum03-12-2020abdullah khalidNo ratings yet
- Emergency SBFR Plan-1Document10 pagesEmergency SBFR Plan-1Miraf MesfinNo ratings yet