You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Post-Polio Syndrome - Management of PCPDocument65 pagesPost-Polio Syndrome - Management of PCPOrion JohnNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- VACEP Sepsis UpdateDocument62 pagesVACEP Sepsis UpdateOrion JohnNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- 2017 ATS 6mwtDocument32 pages2017 ATS 6mwtOrion JohnNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elsevier grants free access to COVID-19 researchDocument12 pagesElsevier grants free access to COVID-19 researchOrion JohnNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Pegasus - Timi 54 PDFDocument21 pagesPegasus - Timi 54 PDFOrion JohnNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- VACEP Sepsis UpdateDocument62 pagesVACEP Sepsis UpdateOrion JohnNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 2016 Guideline For Atrial FibrillationDocument16 pages2016 Guideline For Atrial FibrillationOrion JohnNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Carvedilol in Heart FailureDocument5 pagesCarvedilol in Heart FailureOrion JohnNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Management of CTD in ILDDocument16 pagesManagement of CTD in ILDOrion JohnNo ratings yet
- Pegasus - Timi 54 PDFDocument21 pagesPegasus - Timi 54 PDFOrion JohnNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Wikstrand Et Al-2014-Journal of Internal Medicine PDFDocument10 pagesWikstrand Et Al-2014-Journal of Internal Medicine PDFOrion JohnNo ratings yet
- Pulmonary FibrosisDocument43 pagesPulmonary FibrosisOrion JohnNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Comparable B-Blocker in Heart FailureDocument6 pagesComparable B-Blocker in Heart FailureOrion JohnNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Wikstrand Et Al-2014-Journal of Internal MedicineDocument10 pagesWikstrand Et Al-2014-Journal of Internal MedicineOrion JohnNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- An Introduction To Insulin TherapyDocument23 pagesAn Introduction To Insulin TherapyOrion JohnNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- An Introduction To Insulin TherapyDocument23 pagesAn Introduction To Insulin TherapyOrion JohnNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- 2016 Sepsis Septic ShockDocument39 pages2016 Sepsis Septic ShockOrion JohnNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Fluids in SepsisDocument27 pagesFluids in SepsisOrion JohnNo ratings yet
- 2014 Sepsis & DrugsDocument24 pages2014 Sepsis & DrugsOrion JohnNo ratings yet
- 2015 SepsisDocument41 pages2015 SepsisOrion JohnNo ratings yet
- Noninvasive Ventilation Indications and MonitoringDocument32 pagesNoninvasive Ventilation Indications and MonitoringOrion JohnNo ratings yet
- Pulmonary FibrosisDocument43 pagesPulmonary FibrosisOrion JohnNo ratings yet
- Management of Septic ShockDocument31 pagesManagement of Septic ShockDawn MarcoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Vasopressors in ShockDocument8 pagesVasopressors in ShockOrion JohnNo ratings yet
- Continuous Hemodynamic MonitoringDocument54 pagesContinuous Hemodynamic MonitoringOrion JohnNo ratings yet
- Continuous Hemodynamic MonitoringDocument54 pagesContinuous Hemodynamic MonitoringOrion JohnNo ratings yet
- Pulmonary Function TestsDocument29 pagesPulmonary Function TestsOrion JohnNo ratings yet
- Screening Lung CancerDocument17 pagesScreening Lung CancerOrion JohnNo ratings yet
- Pulmonary Hypertension Drug TherapyDocument337 pagesPulmonary Hypertension Drug TherapyOrion JohnNo ratings yet
- Sickle Cell DiseaseDocument14 pagesSickle Cell DiseaseOrion JohnNo ratings yet
- Surgery For Endocrinological Diseases and Malformations in ChildhoodDocument155 pagesSurgery For Endocrinological Diseases and Malformations in ChildhoodBeng DinNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- IntroductionDocument10 pagesIntroductionFebri WantoNo ratings yet
- Brianna Carden Resume For Portfolio PDFDocument2 pagesBrianna Carden Resume For Portfolio PDFapi-209274086No ratings yet
- ONCOLOGY Board Exam QuestionDocument11 pagesONCOLOGY Board Exam Questiondimplejane100% (2)
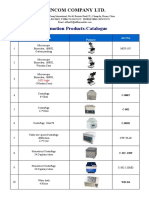
- Wincom Company Catalogue Features Microscopes, Centrifuges and More Medical EquipmentDocument9 pagesWincom Company Catalogue Features Microscopes, Centrifuges and More Medical EquipmentJuan Carlos CrespoNo ratings yet
- Low Intensity Pulsed Ultrasound 2012Document12 pagesLow Intensity Pulsed Ultrasound 2012Joseph SmithNo ratings yet
- Real-Time Tissue Elastography SectionDocument42 pagesReal-Time Tissue Elastography SectionAndrei DumitruNo ratings yet
- Draper & Dash BI Apps For HealthcareDocument22 pagesDraper & Dash BI Apps For HealthcareAnalytics8No ratings yet
- SonoBook 8-9 User Manual V1.0-20170429Document236 pagesSonoBook 8-9 User Manual V1.0-20170429Luis Macías Borges100% (1)
- Ectopic Pregnancy Diagnosis and TreatmentDocument39 pagesEctopic Pregnancy Diagnosis and TreatmentFecky Fihayatul IchsanNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Color Doppler Ultrasound System: Datasheet Release 1.0Document17 pagesColor Doppler Ultrasound System: Datasheet Release 1.0Hea CHNo ratings yet
- Revision History and SpecificationsDocument304 pagesRevision History and SpecificationsSyarif AlfathNo ratings yet
- Ultrasonographic Examination of The Small Intestine, Large IntestineDocument6 pagesUltrasonographic Examination of The Small Intestine, Large IntestineYans PangerunganNo ratings yet
- Submission of RadiologyDocument48 pagesSubmission of RadiologyKartika Singh NarukaNo ratings yet
- Brochure Acuson P500Document12 pagesBrochure Acuson P500Pedro Alexander Romero RodriguezNo ratings yet
- Academy of Life Underwriting - ALU 101 - Basic Life Insurance Underwriting - Textbook For 2022 Exam Cycle (2021)Document359 pagesAcademy of Life Underwriting - ALU 101 - Basic Life Insurance Underwriting - Textbook For 2022 Exam Cycle (2021)KALPESH SHAHNo ratings yet
- Philips Iu22 BrochureDocument16 pagesPhilips Iu22 BrochurecontactoNo ratings yet
- Full Sonography Principles and Instruments 9Th Edition Kremkau Test Bank PDF Docx Full Chapter ChapterDocument33 pagesFull Sonography Principles and Instruments 9Th Edition Kremkau Test Bank PDF Docx Full Chapter Chaptermolecast.bassawkzaa100% (9)
- 5-FUJIFILM-Endoscopy-GuidebookDocument33 pages5-FUJIFILM-Endoscopy-Guidebooklied cnNo ratings yet
- Physics NotesDocument43 pagesPhysics NotesRaj ManovaNo ratings yet
- Operators Manual: E-Z Scan 5500+ SeriesDocument44 pagesOperators Manual: E-Z Scan 5500+ SeriesSadegh ShebaniNo ratings yet
- Instant Download Ebook PDF Essential Ultrasound Anatomy First Edition PDF ScribdDocument47 pagesInstant Download Ebook PDF Essential Ultrasound Anatomy First Edition PDF Scribdandrew.harrell532100% (40)
- CancerDocument228 pagesCancerCrystal Grace100% (1)
- Image Analysis For Biological Sciences - C. A. Glasbey, G. W. HorganDocument211 pagesImage Analysis For Biological Sciences - C. A. Glasbey, G. W. HorganUlises MarmolejoNo ratings yet
- Characterisig Triphasic, Biphasic and MonophasicDocument9 pagesCharacterisig Triphasic, Biphasic and Monophasicraviks34No ratings yet
- Current Concepts in Orthopedic Management of Multiple TraumaDocument8 pagesCurrent Concepts in Orthopedic Management of Multiple TraumanellieauthorNo ratings yet
- Logiq P5: Product DescriptionDocument14 pagesLogiq P5: Product DescriptionrsketchNo ratings yet
- Upper Extremity Venous Doppler Ultrasound PDFDocument12 pagesUpper Extremity Venous Doppler Ultrasound PDFLayla Salomão0% (1)
- AF201 Managerial Accounting Group Assignment Analysis (39Document4 pagesAF201 Managerial Accounting Group Assignment Analysis (39Navinesh Nand100% (1)
- Basic Principles and Safety of Diagnostic Ultrasound in Obstetrics and Gynecology - UpToDateDocument9 pagesBasic Principles and Safety of Diagnostic Ultrasound in Obstetrics and Gynecology - UpToDatemasterchipNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet