You might also like
- The Pediatric History and Physical Exam PDFDocument18 pagesThe Pediatric History and Physical Exam PDFOxana TurcuNo ratings yet
- (3F) Pediatrics - Pediatric HistoryDocument9 pages(3F) Pediatrics - Pediatric HistoryNomar Nonato100% (2)
- Pediatric History and Physical Exam TemplateDocument4 pagesPediatric History and Physical Exam TemplateJay Pee Tumaliuan Tumanguil0% (2)
- Tickler Final PDFDocument29 pagesTickler Final PDFSerious LeoNo ratings yet
- 01.15.01 Pediatric History Taking and Physical ExamDocument14 pages01.15.01 Pediatric History Taking and Physical ExamMikmik DGNo ratings yet
- Pediatrics H&P TemplateDocument3 pagesPediatrics H&P TemplateMark Ma80% (5)
- OBGYN Revalida Review 2019Document74 pagesOBGYN Revalida Review 2019anonymous100% (1)
- Pedia Revalida ReviewDocument83 pagesPedia Revalida Reviewcbac1990No ratings yet
- Clinical Clerkship Survival GuideDocument100 pagesClinical Clerkship Survival GuideRoendel Bustillo100% (3)
- MCU-FDT Outpatient ENT ServicesDocument2 pagesMCU-FDT Outpatient ENT ServicesvinbNo ratings yet
- Pedia ComputationsDocument5 pagesPedia ComputationsRheenz Fornoles100% (1)
- Philippine Pediatric Society, IncDocument19 pagesPhilippine Pediatric Society, IncAsmphLibrary OrtigasNo ratings yet
- Adolescent health assessmentDocument2 pagesAdolescent health assessmentBobet Reña80% (5)
- History and PEDocument3 pagesHistory and PEBom TnaNo ratings yet
- The Seven Habits of Highly Effective PeopleDocument60 pagesThe Seven Habits of Highly Effective PeopleBBCherriNo ratings yet
- Clinical Practice Guideline on Approach and Treatment of Urinary Tract Infection in ChildrenDocument8 pagesClinical Practice Guideline on Approach and Treatment of Urinary Tract Infection in ChildrenPaula QuiñonesNo ratings yet
- CEA SkillsDocument15 pagesCEA SkillsLloyd Fyl O. Razo75% (4)
- Pediatrics Pediatrics Pediatrics Pediatrics Pediatrics: Pediatrics Pediatrics Pediatrics Pediatrics PediatricsDocument2 pagesPediatrics Pediatrics Pediatrics Pediatrics Pediatrics: Pediatrics Pediatrics Pediatrics Pediatrics PediatricsBobet Reña100% (2)
- Luminare PGI Primer PDFDocument62 pagesLuminare PGI Primer PDFChristine Evan HoNo ratings yet
- FCM - The Impact of Illness To The FamilyDocument4 pagesFCM - The Impact of Illness To The FamilyEzekiel Arteta50% (2)
- Case Report: Pregnant Patient with VomitingDocument8 pagesCase Report: Pregnant Patient with VomitingAbdullah Matar86% (7)
- Derain Carla Elize-Group9 DXRDocument6 pagesDerain Carla Elize-Group9 DXRCarla Elize Derain100% (1)
- History Cs Admitting Notes: + 10 "U" Oxytocin X 8 HDocument7 pagesHistory Cs Admitting Notes: + 10 "U" Oxytocin X 8 HKarl Martin PinedaNo ratings yet
- 02 PEDIA250 (5) Pediatric History Taking PDFDocument11 pages02 PEDIA250 (5) Pediatric History Taking PDFJudith Dianne Ignacio100% (1)
- Febrile SeizuresDocument5 pagesFebrile SeizuresJulmajir Salipmugdar100% (1)
- Pedia HXDocument3 pagesPedia HXeyakoyNo ratings yet
- Med History & PE GuideDocument7 pagesMed History & PE GuideStephanie GaerlanNo ratings yet
- Pediatric Sample Case (Seizure) PDFDocument8 pagesPediatric Sample Case (Seizure) PDFIvan RoiNo ratings yet
- Notes For Pedia HandoutDocument2 pagesNotes For Pedia HandoutAiszel Angeli Pepito Ligo100% (2)
- Obstetric and Clinical Medicine - Gynaecological History and ExaminationDocument7 pagesObstetric and Clinical Medicine - Gynaecological History and ExaminationShahin Kazemzadeh100% (1)
- De La Salle Medical department valuesDocument26 pagesDe La Salle Medical department valuesIsabelle SampangNo ratings yet
- PPS Core PediatricsDocument53 pagesPPS Core PediatricsDenise Castro100% (3)
- 10 Warning Signs of ImmunodeficiencyDocument24 pages10 Warning Signs of Immunodeficiencyacque100% (2)
- Pediatric Respiratory Distress: Causes and ManagementDocument323 pagesPediatric Respiratory Distress: Causes and Managementmefav7778520100% (1)
- Leah Paula Briones, MD Marifi Rivera, MD: 2nd Edition 2011Document50 pagesLeah Paula Briones, MD Marifi Rivera, MD: 2nd Edition 2011deniseonscribdNo ratings yet
- Cirrhosis Complications and TreatmentsDocument8 pagesCirrhosis Complications and TreatmentsAlka Sangwan100% (2)
- Pediatrics NotesDocument25 pagesPediatrics Noteskcxie100% (12)
- Pedia Small Notebook EditedDocument17 pagesPedia Small Notebook EditedStarlet Rhonadez Bito-onon Oriel100% (12)
- Intern TicklerDocument10 pagesIntern TicklerRem AlfelorNo ratings yet
- History and Pe ObgynDocument4 pagesHistory and Pe ObgynCara Marrero IguidNo ratings yet
- Quizlet PDFDocument191 pagesQuizlet PDFsr100% (1)
- Pedia Notes: Anthropometric FluidsDocument9 pagesPedia Notes: Anthropometric FluidsIxc Nxc50% (2)
- PEDIATRIC NURSING GROWTH AND DEVELOPMENTDocument55 pagesPEDIATRIC NURSING GROWTH AND DEVELOPMENTJade Q Osit100% (6)
- PPHCH 2012Document41 pagesPPHCH 2012Jill P100% (1)
- Surgery Ple ReviewerDocument5 pagesSurgery Ple ReviewerReinhard Ivan MansibangNo ratings yet
- 1-Review of Neonatal History Taking and Physical ExaminationDocument9 pages1-Review of Neonatal History Taking and Physical ExaminationRogelio Blanco100% (2)
- Gynecology Review: Abigail Elsie Dg. Castro, MD, Maed, Fpogs, Fpsuog August 11, 2017Document198 pagesGynecology Review: Abigail Elsie Dg. Castro, MD, Maed, Fpogs, Fpsuog August 11, 2017Jojo Mendoza100% (1)
- (IM Ward) History Taking Tool PDFDocument15 pages(IM Ward) History Taking Tool PDFleapacis100% (1)
- History Taking in ObgynDocument17 pagesHistory Taking in Obgynselvie87100% (1)
- Formulas and DripsDocument6 pagesFormulas and DripsStarlet Rhonadez Bito-onon Oriel100% (2)
- CPG PCP ListDocument5 pagesCPG PCP ListBryan AtasNo ratings yet
- Pedia Case 1 Dengue 1Document9 pagesPedia Case 1 Dengue 1Rishi Du Agbugay100% (1)
- PM PFC MatrixDocument4 pagesPM PFC MatrixFamed residentsNo ratings yet
- Pharmacology Table - GonzalesDocument14 pagesPharmacology Table - GonzalesMark Angelo PonferradoNo ratings yet
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2No ratings yet
- Pediatric Clinical History Physical Examination TemplateDocument9 pagesPediatric Clinical History Physical Examination TemplateTrisNo ratings yet
- Outline For Pediatric History and Physical Examination History I. Presenting Complaint (Informant/Reliability of Informant)Document4 pagesOutline For Pediatric History and Physical Examination History I. Presenting Complaint (Informant/Reliability of Informant)Hawkar SaeedNo ratings yet
- 7 Pediatric History and Physical ExaminationDocument45 pages7 Pediatric History and Physical ExaminationAmaetenNo ratings yet
- UNDERGRADUATE TEACHING-2 - PagenumberDocument13 pagesUNDERGRADUATE TEACHING-2 - PagenumberZaeem KhalidNo ratings yet
- Guide To The Comprehensive Pediatric H and P Write Up PDFDocument16 pagesGuide To The Comprehensive Pediatric H and P Write Up PDFnanaNo ratings yet
- From Er To Ward 1, 3, Micu: ToopdàDocument2 pagesFrom Er To Ward 1, 3, Micu: ToopdàJay VeeNo ratings yet
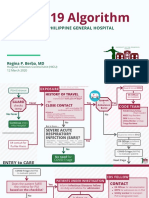
- COVID-19 Algorithm: For The Philippine General HospitalDocument10 pagesCOVID-19 Algorithm: For The Philippine General HospitalJay VeeNo ratings yet
- Emergency DashboardDocument1 pageEmergency DashboardJay VeeNo ratings yet
- RP Manual TemplateDocument9 pagesRP Manual TemplateJay VeeNo ratings yet
- Manual-R B-Medical ClearanceDocument2 pagesManual-R B-Medical ClearanceJay VeeNo ratings yet
- K1MTZDocument1 pageK1MTZJay VeeNo ratings yet
- Gym Work OutDocument19 pagesGym Work OutJay Vee100% (1)
- PPE Selection and Use GuideDocument5 pagesPPE Selection and Use GuideJay Vee100% (1)
- Biological Safety Cabinet Operation and Maintenance ProceduresDocument4 pagesBiological Safety Cabinet Operation and Maintenance ProceduresJay VeeNo ratings yet
- Sample Medical Guidelines: Congestive Heart FailureDocument2 pagesSample Medical Guidelines: Congestive Heart FailureJohanna ShuulukaNo ratings yet
- Department of Emergency Medicine: Philippine General Hospital University of The Philippines Manila Taft Avenue, ManilaDocument1 pageDepartment of Emergency Medicine: Philippine General Hospital University of The Philippines Manila Taft Avenue, ManilaJay VeeNo ratings yet
- Annex 2: Laboratory Assessment Tool / Facility QuestionnaireDocument57 pagesAnnex 2: Laboratory Assessment Tool / Facility QuestionnaireJay VeeNo ratings yet
- Near NCR (National Capital Region) - Quezon CityDocument1 pageNear NCR (National Capital Region) - Quezon CityJay VeeNo ratings yet
- Diseases of The Joint OutlineDocument1 pageDiseases of The Joint OutlineJay VeeNo ratings yet
- Final Covid Guideline PsmidDocument26 pagesFinal Covid Guideline PsmidJay VeeNo ratings yet
- Mental HealthDocument2 pagesMental HealthJay VeeNo ratings yet
- Workout Set A:: Barbell Front Squat (If You Don'T Have Access, Use DBS)Document1 pageWorkout Set A:: Barbell Front Squat (If You Don'T Have Access, Use DBS)Jay VeeNo ratings yet
- ENT-Larynx by Dr. Nixon SeeDocument7 pagesENT-Larynx by Dr. Nixon SeeJay VeeNo ratings yet
- Census MayDocument8 pagesCensus MayJay VeeNo ratings yet
- CK History Final W Pe Sample MentalDocument4 pagesCK History Final W Pe Sample MentalJay VeeNo ratings yet
- CK History Final W Pe Sample MentalDocument4 pagesCK History Final W Pe Sample MentalJay VeeNo ratings yet
- Revised Clinical HX For NewbornDocument3 pagesRevised Clinical HX For NewbornJay VeeNo ratings yet
- Pediatric History and Physical Exam GuideDocument7 pagesPediatric History and Physical Exam GuideIndunil AnuruddhikaNo ratings yet
- Anesthesia Finalsurgical AnestheisaDocument66 pagesAnesthesia Finalsurgical AnestheisaJay VeeNo ratings yet
- The Unhealthy Fast FoodDocument2 pagesThe Unhealthy Fast FoodRikudo AmubaNo ratings yet
- Common Psychosocial Problem in Adolescence: - Substance Abuse - Juvenile Delinquency - Smoking and AlcoholismDocument59 pagesCommon Psychosocial Problem in Adolescence: - Substance Abuse - Juvenile Delinquency - Smoking and AlcoholismSamjhana GautamNo ratings yet
- Microalbuminuria Is Associated With Cardiovascular Risk in Prediabetes and PrehypertensionDocument14 pagesMicroalbuminuria Is Associated With Cardiovascular Risk in Prediabetes and Prehypertensionد.عليالنجارالموسويNo ratings yet
- Camacho-Reyes v. ReyesDocument8 pagesCamacho-Reyes v. ReyesStradivariumNo ratings yet
- Prestigi0us BiochemistryDocument30 pagesPrestigi0us Biochemistrybovey69015No ratings yet
- Fatima Memorial Medical & Dental College & AHS, LahoreDocument8 pagesFatima Memorial Medical & Dental College & AHS, LahoreAqsa MohsinNo ratings yet
- The Top 10 Most Common Chronic Diseases For Older AdultsDocument9 pagesThe Top 10 Most Common Chronic Diseases For Older AdultstessahurintNo ratings yet
- Maple Syrup Urine DiseaseDocument14 pagesMaple Syrup Urine DiseasefantasticoolNo ratings yet
- Anesthesia and Myasthenia Gravis2012Document22 pagesAnesthesia and Myasthenia Gravis2012Alisher AgzamovNo ratings yet
- ANTI Ulcer DrugsDocument1 pageANTI Ulcer Drugsapi-3739910100% (1)
- Ca 19 9Document3 pagesCa 19 9डा. सत्यदेव त्यागी आर्यNo ratings yet
- Delusional DisorderDocument4 pagesDelusional DisorderNajm Us Saqib BhatNo ratings yet
- OtitaDocument99 pagesOtitaRoxana SurliuNo ratings yet
- Uswatun Hasanah-195037-2a Rmik (KKPMT)Document4 pagesUswatun Hasanah-195037-2a Rmik (KKPMT)Uswatun HasanahNo ratings yet
- Mon Surgical Infections Boils, Abscess, Ulcer, Cellulitis, Curbuncle, Gangrene, Sinus, Fistula CDocument48 pagesMon Surgical Infections Boils, Abscess, Ulcer, Cellulitis, Curbuncle, Gangrene, Sinus, Fistula CPanna SahaNo ratings yet
- The Weight Loss ManualDocument56 pagesThe Weight Loss ManualSomashekarNo ratings yet
- 2013 BAA - Glossary of Common Medical Prefixes and Suffixes For BAA and BLSDocument5 pages2013 BAA - Glossary of Common Medical Prefixes and Suffixes For BAA and BLSM GavinNo ratings yet
- The Easy Book of Cancer PharmacologyDocument526 pagesThe Easy Book of Cancer Pharmacologybianca100% (3)
- Acute Disease Case Study: Metabolism - HypothermiaDocument8 pagesAcute Disease Case Study: Metabolism - HypothermiaRegina PerkinsNo ratings yet
- Rosenhan - On-Being-Sane-In-Insane-Places PDFDocument10 pagesRosenhan - On-Being-Sane-In-Insane-Places PDFAlexandru Ioan CretuNo ratings yet
- Management of Diabetic Cats With Long Acting InsulinDocument16 pagesManagement of Diabetic Cats With Long Acting Insulindia_dianneNo ratings yet
- Quick Reference DMARDsDocument12 pagesQuick Reference DMARDsEman MohamedNo ratings yet
- PRIMARY HEALTH CARE - IMMUNIZATIONDocument24 pagesPRIMARY HEALTH CARE - IMMUNIZATIONAhmed Azeez100% (1)
- Digestive Health & You - 03062018Document8 pagesDigestive Health & You - 03062018Times MediaNo ratings yet
- Lesson Plan On SchizophreniaDocument22 pagesLesson Plan On SchizophreniaDurga KohaleNo ratings yet
- The Last LeafDocument22 pagesThe Last Leafdunitha dechamma kbNo ratings yet
- Bone Tumor: A. Nithya 1 Year M.SC (Nursing)Document46 pagesBone Tumor: A. Nithya 1 Year M.SC (Nursing)nithya nithyaNo ratings yet
- AP3 Form ApplicationDocument1 pageAP3 Form ApplicationBenjamin AcompaniadoNo ratings yet
- Introduction to Epidemiology and Public HealthDocument22 pagesIntroduction to Epidemiology and Public HealthIbrar Faisal0% (1)
- A Dictionary of Dentistry (Oxford Paperback Reference) by Robert IrelandDocument928 pagesA Dictionary of Dentistry (Oxford Paperback Reference) by Robert IrelandSalam Alyaseen100% (2)