You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 3D Virtual Treatment Planning of Orthognathic Surgery A Step-By-Step Approach For Orthodontists and SurgeonsDocument580 pages3D Virtual Treatment Planning of Orthognathic Surgery A Step-By-Step Approach For Orthodontists and SurgeonsAbad Salcedo100% (4)
- Diastema Closure and Long-Term Stability - JCO-OnLINEDocument15 pagesDiastema Closure and Long-Term Stability - JCO-OnLINEAbad SalcedoNo ratings yet
- Diastema Closure and Long-Term Stability - JCO-OnLINEDocument15 pagesDiastema Closure and Long-Term Stability - JCO-OnLINEAbad SalcedoNo ratings yet
- Early Vs Late Orthodontic Treatment of DeepbiteDocument8 pagesEarly Vs Late Orthodontic Treatment of DeepbiteAlvaro Chacón100% (1)
- Sputnik V en The LancetDocument11 pagesSputnik V en The LancetLARED21No ratings yet
- Validity of Bond Strength TestDocument8 pagesValidity of Bond Strength TestAbad SalcedoNo ratings yet
- Zucchelli Et Al-2015-Periodontology 2000Document36 pagesZucchelli Et Al-2015-Periodontology 2000Abad Salcedo100% (1)
- Myths and RealitiesDocument6 pagesMyths and RealitiesAbad SalcedoNo ratings yet
- Phukaoluan2016 PDFDocument16 pagesPhukaoluan2016 PDFAbad SalcedoNo ratings yet
- Myths and RealitiesDocument6 pagesMyths and RealitiesAbad SalcedoNo ratings yet
- Retention in Orthodontics: Verifiable CPD PaperDocument4 pagesRetention in Orthodontics: Verifiable CPD PaperAbad SalcedoNo ratings yet
- Choi 2015Document9 pagesChoi 2015Abad SalcedoNo ratings yet
- Zou Et Al-2015-Clinical Implant Dentistry and Related ResearchDocument11 pagesZou Et Al-2015-Clinical Implant Dentistry and Related ResearchAbad SalcedoNo ratings yet
- 2015-Journal of Clinical PeriodontologyDocument8 pages2015-Journal of Clinical PeriodontologyAbad SalcedoNo ratings yet
- Zuhr Et Al-2014-Journal of Clinical PeriodontologyDocument20 pagesZuhr Et Al-2014-Journal of Clinical PeriodontologyAbad Salcedo100% (1)
- 10 1016@j Ajodo 2009 03 051Document8 pages10 1016@j Ajodo 2009 03 051Abad SalcedoNo ratings yet
- 10 1016@j Ajodo 2009 03 051Document8 pages10 1016@j Ajodo 2009 03 051Abad SalcedoNo ratings yet
- Estetica Dental y EnciaDocument8 pagesEstetica Dental y EnciaAbad SalcedoNo ratings yet
- Analisis de Vomer BasilliDocument14 pagesAnalisis de Vomer BasilliAbad SalcedoNo ratings yet
- The Relationship Between Upper Airways and Craniofacial Morphology Studied in 3D. A CBCTDocument11 pagesThe Relationship Between Upper Airways and Craniofacial Morphology Studied in 3D. A CBCTAbad SalcedoNo ratings yet
- Potential Errors and Misuse of Statistics in StudiesDocument9 pagesPotential Errors and Misuse of Statistics in StudiesAbad SalcedoNo ratings yet
- Jco - 2008 03 157 PDFDocument7 pagesJco - 2008 03 157 PDFAbad SalcedoNo ratings yet
- Diastemas Brasil PDFDocument8 pagesDiastemas Brasil PDFAbad SalcedoNo ratings yet
- Brasil Dias Ten MasDocument7 pagesBrasil Dias Ten MasAbad SalcedoNo ratings yet
- Molar Distalization PDFDocument3 pagesMolar Distalization PDFdruzair00775% (4)
- Roth y DaMONDocument8 pagesRoth y DaMONAbad SalcedoNo ratings yet
- Molar Distalization PDFDocument3 pagesMolar Distalization PDFdruzair00775% (4)
- Stability of Quadhelix Crib Therapy inDocument9 pagesStability of Quadhelix Crib Therapy inAbad SalcedoNo ratings yet
- Epigenetic Influence of KAT6B and HDAC4Document9 pagesEpigenetic Influence of KAT6B and HDAC4Abad SalcedoNo ratings yet
- Pi Is 0889540613006641Document9 pagesPi Is 0889540613006641Abad SalcedoNo ratings yet
- Occlusal Consideration For Mandibular Implant OverdenturesDocument12 pagesOcclusal Consideration For Mandibular Implant OverdenturesFrancisca Dinamarca Lama100% (1)
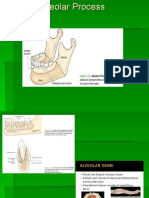
- Alveolar BoneDocument24 pagesAlveolar BoneHanna SouthwellNo ratings yet
- JURNAL - Dental Occlusion and Malocclusion Prevalence, Types and TreatmentDocument8 pagesJURNAL - Dental Occlusion and Malocclusion Prevalence, Types and TreatmentAndrew SipayungNo ratings yet
- Dental Anatomy FactsDocument10 pagesDental Anatomy FactsGhee MoralesNo ratings yet
- Arch Width and Form - A ReviewDocument9 pagesArch Width and Form - A ReviewMafe SalazarNo ratings yet
- Contemporary Oral and Maxillofacial Pathology, 2nd EditionDocument456 pagesContemporary Oral and Maxillofacial Pathology, 2nd Editionaisyarahma zanuaryNo ratings yet
- Session 10. Review of Centric Records RECORDSDocument25 pagesSession 10. Review of Centric Records RECORDSbaraa.abdulrahman.23No ratings yet
- Jurnal Kasus Tambahan 3 - Khairin Yonni (12730)Document6 pagesJurnal Kasus Tambahan 3 - Khairin Yonni (12730)Khairin YonniNo ratings yet
- Asymmetric Maxillary Expansion (AMEX)Document29 pagesAsymmetric Maxillary Expansion (AMEX)Monojit DuttaNo ratings yet
- Pages 9,10Document2 pagesPages 9,10Kifah Nadim AlyassinNo ratings yet
- 001 - 05 - DR Michael Melkers - Occlusion in Everyday PracticeDocument40 pages001 - 05 - DR Michael Melkers - Occlusion in Everyday PracticeMinh ThongNo ratings yet
- A Comparative Evaluation Between Cheiloscopic Patterns and Canine Relationship in Primary DentitionDocument4 pagesA Comparative Evaluation Between Cheiloscopic Patterns and Canine Relationship in Primary DentitionAbiNo ratings yet
- The Clincal Management of Ectopically Erupting First Permanent MolarsDocument6 pagesThe Clincal Management of Ectopically Erupting First Permanent MolarsFourthMolar.comNo ratings yet
- Extract Jakovac ProtocolDocument10 pagesExtract Jakovac ProtocolstercostasNo ratings yet
- Restoring a Fractured Front ToothDocument8 pagesRestoring a Fractured Front ToothIbramanto WarganegaraNo ratings yet
- MCQs in Oral Pathology-31-33Document3 pagesMCQs in Oral Pathology-31-33Ammar YasirNo ratings yet
- PERMANENT DENTITION KEY FACTORSDocument35 pagesPERMANENT DENTITION KEY FACTORSraj raiNo ratings yet
- Dental Diseases and Conditions ListDocument1 pageDental Diseases and Conditions ListPenagihan Rs Tugu IbuNo ratings yet
- Surgical Aids To Orthodontics FinalDocument77 pagesSurgical Aids To Orthodontics Finalbushra100% (2)
- Comparison of Treatment Effects AfterDocument9 pagesComparison of Treatment Effects AfterFernanda PompeoNo ratings yet
- The Eight Components of A Balanced SmileDocument17 pagesThe Eight Components of A Balanced SmileJose AriasNo ratings yet
- 05 Hardy 1951 The Developments in The Occlusal Patterns of Artificial TeethDocument15 pages05 Hardy 1951 The Developments in The Occlusal Patterns of Artificial Teethjorefe12No ratings yet
- Significant of Apical Third: A ReviewDocument5 pagesSignificant of Apical Third: A ReviewJim Christover NiqNo ratings yet
- Dental Caries Classification Guide - Types, Stages & FactorsDocument80 pagesDental Caries Classification Guide - Types, Stages & FactorsAjinkya KadamNo ratings yet
- Nomenclature, Formulae For Mammalian Teeth and Tooth Numbering SystemsDocument22 pagesNomenclature, Formulae For Mammalian Teeth and Tooth Numbering Systemsamanita238No ratings yet
- Dental CingulumDocument2 pagesDental Cingulumakm BasharNo ratings yet
- Teeth and Tongue LessonDocument4 pagesTeeth and Tongue LessonKriti Shah100% (1)
- Chronology & MorphologyDocument30 pagesChronology & MorphologyAhsan Ul Kayum BhuiyanNo ratings yet
- Injection Moulding TechniqueDocument14 pagesInjection Moulding Techniquedrpooja.kaloniyaNo ratings yet