Statement before the United States Senate Committee on Finance
Hearing titled, Social Security: A Fresh Look at Workers Disability Insurance.
SSDI Program Growth Will Continue Unless
Fundamental Reforms Are Implemented
Richard V. Burkhauser
Professor, Cornell University
Visiting Scholar, American Enterprise Institute
July 24, 2014
The views expressed in this testimony are those of the author alone and do not necessarily represent those
of Cornell University or the American Enterprise Institute.
This testimony is primarily based on: Richard V. Burkhauser and Mary C. Daly. 2011. The
Declining Work and Welfare of People with Disabilities: What Went Wrong and a Policy for
Change, AEI Press: Washington DC, and extensions of that work in Burkhauser and Daly
(2012), Daly, Lucking, and Schwabish (2013), Daly (2014) and Burkhauser, Daly, McVicar and
Wilkins (2014).
1
Chairman Wyden, Ranking Member Hatch, and esteemed members of the Committee: Thank
you for the opportunity to testify before the United States Senate Committee on Finance on
workers disability insurance.
The Social Security Disability Insurance (SSDI) program is growing at an unsustainable
pace. Since 1970 the number of disabled worker beneficiaries has increased nearly six-fold,
rising from 1.5 to 8.8 million in 2012. This rapid growth in the rolls has put increasing pressure
on program finances. Inflation-adjusted SSDI expenditures have risen by more than six-fold
from $20 to $137 billion (in 2012 dollars) over this same period. Based on current growth, the
SSDI program is projected to be insolvent by 2016 (Social Security Administration, 2014).
The rapid rise in caseloads and costs are made more worrisome when put in the context of
the broader goals of the SSDI programto protect the economic well-being of people with
disabilities. Since the passage of the Americans with Disabilities Act of 1990 (ADA), the
employment of those with disabilities has declined considerably and their household income has
remained flat. Increasingly, people with disabilities are substituting SSDI benefits for labor
market earnings, making them net withdrawers rather than net contributors to the tax base during
their working age. This outcome challenges the finances of the SSDI program and is at odds with
the view of disability codified in the ADA that people with disabilities are able and willing to
participate in the labor market.
WHY HAVE SSDI CASELOADS RISEN?
Possible explanations for SSDI program growth can be broadly classified into two groups: (1)
those that are focused on one-time events not directly related to the program itselfthe aging of
the population, changes in the underlying severity of disability, the entry of women into the labor
force, or the increase in the normal age of retirement from 65 to 66 in the Social Security Old-
2
Age and Survivor Insurance program (OASI); and (2) those that are focused on changes in
program rules or their applicationthe cyclicality of application rates, the growth in SSDI
benefits relative to wage earnings, and specific changes in rules and their interpretation and
implementation over time.
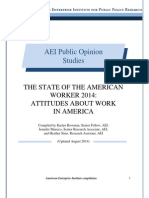
Recent work by Daly, Lucking and Schwabish (2013), updated in Daly (2014), using shift share
analysis argues that once these one-time unrelated factors are accounted for, 43.8 percent of the
growth in SSDI recipiency rates between 1980 and 2012 is program related and will continue to
affect program growth in the future. Research by Duggan and Imberman (2009) and by Autor
and Duggan (2006, 2010) looking at somewhat different periods, find that these program-related
changes affected individual behavior and accounted for an even larger share of program growth.
More importantly all these researchers predict these program-related factors will continue to do
so in the future.
Non-Program-Related Growth Factors
Changes in the age distribution
The most obvious potential driver of SSDI growth is the aging of the population. Since SSDI
benefits are conditioned on having a disability, and disability generally rises with age, the aging
of the baby boom generation will, on net, push up the SSDI rolls. A simple way to gauge the
impact of this change is to fix SSDI recipiency rates by age group in some period and let growth
in the rolls evolve based on changes in the age structure of the population. Autor and Duggan
(2006, 2010) do this and find that between 1984 and 2003, changes in age structure accounted
for about 6 percent of the increase in SSDI receipt among the non-elderly population over the
period. Daly, Lucking and Schwabish (2013), updated in Daly (2014), find that between 1980
3
and 2012 the aging of the population accounted for 17.9 percent of SSDI recipiency growth. (See
Figure 1.)
Changes in health and work disability
Another potential driver is health. To qualify for SSDI benefits, individuals must have a
medically determinable ailment expected to last for at least 12 months or result in death. If the
health of the insured population has declined over time this would influence program enrollment
and growth. Surveys asking about activity and work limitations point to a relatively stable
pattern in these measures over the last two decades. Although work and activity limitations rise
with age, there is little evidence that the prevalence within an age-group of such limitations has
increased over time. (For additional discussion see: Burkhauser and Daly 2011)
Entry of women into the workforce.
Changes in the labor force participation of women also have influenced program growth. Since
SSDI is an insurance program, eligibility for benefits requires a fixed number of quarters of
covered employment. The substantial increase in the labor force participation of women has
increased both their SSDI coverage and their receipt of disability benefits. It is straightforward to
compute the magnitude of this change on the total growth in SSDI rolls. Autor and Duggan
(2006, 2010) make these computations as do Daly, Lucking and Schwabish (2013). They both
conclude that the increased number of women in the paid labor force can only explain a fraction
of the total rise in SSDI caseloads since the mid-1980s. For instance, Daly, Lucking and
Schwabish (2013), updated in Daly (2012), find that between 1980 and 2012 the increased
number of women in the paid labor force can explain 16.5 percent of growth.
However they recognize that in 1980, womens SSDI recipiency rate was well below that of
men, even after accounting for the lower eligibility of women. Analysts dont agree on what
4
explains this gap. Some argue it reflects underlying health differences between men and women.
Others maintain that women eligible for SSDI were not representative of the entire population of
women in 1980 and that a more representative sample of women would have had a recipiency
rate similar to mens. They quantify this assumption by setting the recipiency rate for women
equal to that of men in 1980. As Figure 1 shows, this adds another 12.8 percent to their estimates
of how much the greater eligibility of women has contributed to rising recipiency rates.
Daly, Lucking and Schwabish (2013), updated by Daly (2014), then add a final non-program-
related factorthe increase of the normal retirement age to 66 over this period. Doing so
accounts for another 9.1 percent of SSDI growth.
Combining the estimated contributions of population aging, changes in health, the entry of
women into paid work, and the change in the OASI retirement age, Daly, Lucking and
Schwabish (2013), updated in Daly (2014), still find that 43.8 percent of SSDI caseloads over the
last three decades are accounted for by program-related factors. (See Figure 1.) These are factors
whose changes have encouraged workers to increasingly apply for, and Social Security
gatekeepers to increasingly determine them eligible for, SSDI benefits. And, most importantly,
these are factors that will continue to do so and continue to be missed in projections of SSDI
program growth that do not account for them.
Program-Related Growth Factors
Changes in SSDI rules and their implementation.
Caseload fluctuations line up with changes in Social Security Administration (SSA) policies that
make it easier or harder to gain entry to the SSDI rolls. In the late 1970s and early 1980s relative
caseloads fell, first because program gatekeepers were urged to more strictly interpret existing
rules and then because Congress, in 1980, required SSA to reevaluate all current recipients to see
5
if they still met the medical standards. This rule change, which was rigorously enforced by SSA
at the start of the new Reagan administration, resulted in a drop in the SSDI rolls despite a major
recession. By 1983 the widespread reevaluation of those already on SSDI was halted as the
courts and then Congress restricted the SSAs power to reevaluate beneficiaries. Furthermore, in
1984, responding to a backlash against restrictive cuts imposed in the Social Security Disability
Amendments of 1980, policymakers expanded the ways in which a person could medically
qualify for the SSDI program. The 1984 legislation moved away from a strict medical listing
determination of eligibility to one that also considered an applicants overall medical condition
and ability to work. These changes meant that applicants could qualify for SSDI based on having
multiple conditions, even when no single condition would meet the SSDI eligibility threshold. In
addition, the legislation allowed for symptoms of mental illness and pain to be counted when
assessing SSDI eligibility, regardless of whether the person had a verifiable medical diagnosis.
The expansion of eligibility to more difficult-to-measure impairments that do not precisely
meet the medical listings means that SSA has increasingly been tasked with making more
subjective decisions about the impact that presenting impairments might have on an applicants
work ability. For applicants who do not meet or exceed the medical listings, program
administrators consider a set of vocational criteria. While these criteria have not changed over
the history of the SSDI program, their use by program gatekeepers to determine benefit
eligibility has risen dramatically since 1991. Currently, they are used to justify the majority of
new awards, especially among those with the more difficult-to-determine conditions of mental
illness and musculoskeletal conditionsthe primary condition of more than 50 percent of all
newly enrolled beneficiaries. (See Burkhauser and Daly, 2011 for fuller discussion.)
Effects on behavior and implications for work capacity
6
The effect of this growing share of marginal applicants is a substantial variation in the flow of
applicants onto the rolls. This variation comes both from fluctuations in applicant inflow and
variations in decision making among SSDI gatekeepers. For example, Maestas, Mullen, and
Strand (2013) using SSA administrative records find that at the initial Disability Determination
Stage (DDS) of decision making, 23 percent of new applicants in 2005 were marginal cases
whose admittance into the program was determined by the luck of drawing an easier rather than a
stricter DDS gatekeeper. Importantly, when they compare the subsequent work histories of those
who entered the program in this way with a matched set of applicants who drew a stricter DDS
gatekeeper, they find the latter groups employment was on average 20 percentage points higher.
This difference is even greater for those with less severe medical conditions. This research
suggests that, increasingly, applicants admitted to the SSDI rolls on these looser criteria have
greater work capacity than assumed for those receiving SSDI benefits.
The differences in allowances are important, especially when one considers how application
rates fluctuate with economic conditions. Plots of the SSDI application rate and the national
unemployment rate show that, with the exception of the double-dip recession in the 1980s,
application rates are highly correlated with the business cycle. They rise during recessions and
fall during periods of economic growth. Disability application rates hit record highs during the
Great Recession and have only modestly declined since then. Most research on the consequence
of business cycles on application rates finds that economic conditions play a substantial role in
SSDI application and award patterns over time. (See Burkhauser and Daly 2012)
In sum, a large share of SSDI growth (43.8 percent based on Daly, Lucking and Schwabish,
2013, updated in Daly, 2014) has been driven by factors other than an aging workforce, health
declines, the increasing SSDI coverage of women, and changes in the OASI normal retirement
7
age. Loosening of program rules in the 1980s has made it more difficult for gatekeepers to judge
eligibility and increased the likelihood that applicants facing rising replacement rates or
declining economic opportunities will apply for SSDI benefits. A growing number of individuals
being allowed onto the rolls could work in some capacity and would do so if they were not
judged eligible for benefits.
One clear indicator these program-related factors have an independent effect on program
growth can be seen in Figure 2. While it is certainly the case that aging baby boomers have
increased program growth as they have become a larger share of the work force, Figure 2 shows
that the growth in the prevalence of SSDI program receipt compared to 1970 has been far higher
at younger than at older ages. The most rapid growth has been among those ages 25 through 39.
Because these recipients are likely to stay on the rolls many more years than those who enter at
older ages, their lifetime impact on program costs will be far higher.
Not factoring in the important role policy changes have had and will continue to have on
program growth can importantly affect SSDI program growth projection. Figure 3 is based on
official Office of the Chief Actuary (OCACT), Social Security Administration, historical and
projected SSDI beneficiary populations (Social Security Administration, 2014). Beneficiary
numbers were obtained from http://www.socialsecurity.gov/OACT/STATS/DIbenies.html and
projections from http://www.socialsecurity.gov/OACT/TR/2013/tr2013.pdf, accessed 7/22/2014.
The data from 1977 to 2013 nicely documents the rapid growth in the SSDI rolls discussed
above. There is no disagreement among scholars with respect to these numbers. The data from
2015 to 2035 are based on OCACT projections of future growth. They are remarkably optimistic
projections that suggest that the one-time events that have propelled SSDI growth since the early
1980s have, for the most part, run their course. There is very modest growth between 2013 and
8
2025 and little or no growth over the following 10 years. Hence, a one-time increase, for
instance, in the SSDI payroll tax will solve both the short- and longer-term SSDI solvency
problem.
Figure 4 comes from Daly, Lucking and Schwabish (2013), updated in Daly (2014), and
based on Social Security Administration, 2013, OCACT projections. It shows actual SSDI
prevalence rates between 1980 and 2012 and OCACT projections of future prevalence rates at
various times in the past as well as their 2012 projection. In almost all cases, these projections
have substantially underestimated future SSDI program growth. The reason is that OCACT has
not fully taken into consideration the influence of program effects on past behavior that accounts
for the 42.8 percent of program growth discussed above. This is program growth that will
continue into the future unless fundamental changes are made in SSDI policy. My guess is that
absent this policy change, OCACTs current projections will once again underestimate actual
SSDI program growth.
Figure 5 from Daly, Lucking and Schwabish (2013), updated in Daly (2014), provides an
alternative projection of program growth that shows how much more program growth will be if
the 42.8 percent of that growth estimated by Daly, Lucking and Schwabish (2013) and updated
in Daly (2014) continues into the future at the same average rate it has occurred since 1980. To
the degree that this unexplained growth in the OCACT projections once again occurs, any one-
time increase in Social Security taxes to solve the SSDI deficit problem through 2035 will only
be a down payment on future tax increases.
THE CASE FOR FUNDAMENTAL CHANGE
Evidence that growth in U.S. disability rolls has to a large extent been driven by policy and
associated behavioral responses among gatekeepers and workers with disabilities are consistent
9
with those found for the Netherlands during a period when it was known as the sick country of
Europe. (Aarts, Burkhauser and de Jong, 1998). Following many failed attempts to modify the
system from within, in 2001, the Netherlands decided to fundamentally restructure the system.
As can be seen in Figure 6, the results have been notable; the share of the Dutch work force
receiving disability benefits has declined significantly and has done so without raising the rolls in
other transfer programs at the same time that the share of the U.S. work force receiving disability
benefits has grown. (See Figure 6 based on Figure 5.1 in Burkhauser and Daly, 2011).
Burkhauser, Daly, McVicar, and Wilkins (2014) extend this analysis to Great Britain,
Sweden, and Australia and show a similar pattern of disability prevalence rates that are highly
sensitive to disability policy changes. After major increases in their disability prevalence rates,
Sweden and Great Britain also introduced fundamental reforms into their systems that have
reduced their disability prevalence rate over the last decade.
The Dutch reforms focused on reducing inflows onto long-term disability benefits by making
employers more directly bear program costs. The reforms required all Dutch firms to fund the
first two years of disability benefits to their workers and to pay an experience-rated disability tax
based on the number of workers they subsequently moved onto the long-term Dutch disability
insurance program. These reforms provided incentives for employers, who are in the best
position to offer accommodation and rehabilitation, to do so in lieu of moving workers with
disabilities onto cash transfers. Research shows that the reforms led to the development of a
private sector market for disability insurance and the management of impaired workers, which is
credited, in part, with a significant decline in inflows to disability cash benefits. Importantly, the
research shows that the reduction in inflows owes to the fact that workers with disabilities are
more regularly returning to work (de Jong, 2008; van Sonsbeek, 2010).
10
In the spirit of the Dutch reforms, recent proposals by Autor and Duggan (2010) and
Burkhauser and Daly (2011) call for prioritizing supported work over cash benefits for people
with disabilities. Like the Dutch, both proposals focus on slowing the movement of workers with
impairments onto the SSDI rolls, rather than attempting to reduce the current beneficiary
population via the stick of greater enforcement (tried in the 1980s) or the carrot of changing the
incentives for current beneficiaries to return to work (impetus for Ticket to Work). Such
fundamental reforms would end the archaic and counterintuitive policy currently in place that
provides access to work-focused support only after SSDI applicants have gone through an
extended process of demonstrating that they are unable to work.
Autor and Duggan (2010) propose a new mandate on all firms to provide the first two years
of short-term disability insurance. This would increase the willingness of employers to provide
additional accommodation and rehabilitation by more directly linking the cost of disability
payment to firms. It would also create growth in the private insurance market and greater case
management of workers following the onset of a work-limiting impairment and hence greater
return to work. However, it could result in substantial added costs to the system.
Alternatively, Mary Daly and I (Burkhauser and Daly 2011) argue that like the Dutch, the
United States should impose some form of experience rating on firms paying into the SSDI
system. Raising the SSDI payroll tax of firms whose workers enroll in the system at above-
average rates and lowering the SSDI payroll taxes on firms whose workers enroll at below-
average rates via experience rating would more directly link the costs to the firm of one of its
workers moving onto the SSDI program. Employers who bore the costs for both options would
be more incentivized to make the investments in accommodation and rehabilitation that could
prolong the employment tenure of a worker with a disability. This is currently the system used to
11
fund state workers compensation benefits, and the best practices from these state programs
could be considered for SSDI as well. Alternatively, employers who provide short-term private
disability insurance for employees and whose private insurance agents cooperate with SSDI
gatekeepers in managing their cases could be granted a reduction in SSDI tax rates, while firms
that did not offer such private insurance could be charged higher SSDI tax rates. Either of these
reforms would bend the cost curve of projected SSDI program expenditures by reducing
incentives for employers and employees to overuse the system.
Although the details differ, the messages of the Autor and Duggan and Burkhauser and Daly
proposals are the same: The current SSDI program built on the assumption that disability and
employment are mutually exclusive states is both archaic and fiscally unsustainable.
Fundamental reform is needed to restore solvency to the U.S. disability insurance system and to
support continued employment and greater self-sufficiency among workers with disabilities.
12
REFERENCES
Aarts, L. J. M., Burkhauser, R. V. & de Jong, P.R. (1998). Convergence: A Comparison of
European and United States Disability Policy. Terry Thomason, John Burton, and
Douglas Hyatt (eds.), New Approaches to Disability in the Work Place. IRRA Research
Volume, (1998), pp. 299-338.
Autor, D. H., & Duggan, M. G. (2006). The growth in the Social Security disability rolls: A
fiscal crisis unfolding. Journal of Economic Perspectives, 20, 7196.
Autor, D. H., & Duggan, M. G. (2010, December). Supporting work: A proposal for
modernizing the U.S. disability insurance system. Washington, DC: Center for American
Perspective and the Hamilton Project.
Burkhauser, R. V., & Daly, M. (2011). The declining work and welfare of people with
disabilities: What went wrong and a strategy for change. Washington, DC: AEI Press.
Burkhauser, R.V. & Daly, M. (2012). Social Security Disability Insurance: time for fundamental
change. Journal of Policy Analysis and Management, 31 (2): 454-461.
Burkhauser, Richard V., Daly, M., McVicar, D. & Wilkins, R. (2014). Disability Benefit
Growth and Disability Reform in the United States: Lessons from Other OECD Nations.
IZA Journal of Labor Policy 3:4: 1-30.
Daly, M. (2014). Social Security Disability Insurance: Understanding the Past and Preparing for
the Future. Presentation delivered at the National Academy of Social Insurance, 26th
Annual Policy Research Conference, January 29-30.
Daly, M., Lucking B., & Schwabish J. (2013). The Future of Social Security Disability
Insurance. Federal Reserve Board of San Francisco Economic Letter (June 24, 2013).
13
http://www.frbsf.org/economic-research/publications/economic-letter/2013/june/future-
social-security-disability-insurance-ssdi/
de Jong, P. (2008). Recent changes in Dutch disability policy. Working paper, Amsterdam:
University of Amsterdam.
Duggan, M. & Imberman, S.A. (2009) Why Are the Disability Rolls Skyrocketing? The
Contribution of Population Characteristics, Economic Conditions, and Program
Generosity. In Health at Older Ages: The Causes and Consequences of Declining
Disability among the Elderly , Cutler, D.M. and Wise, D.A., editors (p. 337-379),
University of Chicago Press.
Maestas, N., Mullen, K., & Strand, A. (2013). Does Disability Insurance receipt discourage
work? Using examiner assignment to estimate causal effects of SSDI receipt. American
Economic Review 103 (5): 1797-1829.
Social Security Administration. (2013). The 2012 annual report of the board of trustees of the
federal Old Age and Survivors Insurance and federal Disability Insurance Trust Funds.
Washington, DC.
Social Security Administration. (2014). The 2013 annual report of the board of trustees of the
federal Old Age and Survivors Insurance and federal Disability Insurance Trust Funds.
Washington, DC.
van Sonsbeek, J.M. (2010, August). Estimating the effect of recent disability reforms in the
Netherlands. Working paper Amsterdam: University of Amsterdam.
14
9.1
17.9
16.5
12.8
43.8
0
10
20
30
40
50
Increase in
retirement age
Aging of the
population
Women's labor
force
Residual
%
29.2
Recipiency
Catch-Up
SSDI
Eligibility
Sources of SSDI Prevalence Rate Growth, 1980-2012
Source: Social Security Administration, Bureau of Labor Statistics, and FRBSF Staff Calculations. http://www.frbsf.org/economic-
research/publications/economic-letter/2013/june/future-social-security-disability-insurance-ssdi/
Figure 1. (Source: Daly 2014)
15
0
50
100
150
200
250
300
350
400
450
1980 1985 1990 1995 2000 2005 2010
Source: Social Security Administration and FRBSF Staff Calculations. Note:prevalence calculation uses insured population.
1970 = 100
Normalized Growth in SSDI Prevalence by Age
Index
20-29
30-39
40-49
50-59
60-64
Figure 2. (Source: Daly 2014)
Figure 3. (Source: SSA 2014)
16
0
1
2
3
4
5
6
1980 1985 1990 1995 2000 2005 2010 2015 2020
Source: Short and Long range Actuarial Projections of the Old-Age, Survivors, and Disability Insurance Program, (various years),
Bureau of Labor Statistics, Census Bureau, and FRBSF Staff Calculations. http://www.frbsf.org/economic-
research/publications/economic-letter/2013/june/future-social-security-disability-insurance-ssdi/
Beneficiaries per 100 age 20-64 insured population
Past SSA Projections of SSDI Prevalence Rate
%
Actual
2013 Projection
2010 Projection
2005 Projection
2001 Projection
1996 Projection
1991 Projection
1988 Projection
0
1
2
3
4
5
6
1980 1984 1988 1992 1996 2000 2004 2008 2012 2016 2020 2024
Source: Short Range Actuarial Projections of the Old-Age, Survivors, and Disability Insurance Program (2013), Census
Bureau, and FRBSF Staff Calculations. http://www.frbsf.org/economic-research/publications/economic-
letter/2013/june/future-social-security-disability-insurance-ssdi/
Beneficiaries per 100 age 20-64 insured population
Scenarios of Future SSDI Growth
%
2013 Trustees Report
(red dashed line)
Disability Prevalence Rate
Adjusted Disability Prevalence Rate
(net of one-time factors)
Green
bands
denote
range of
possible
future
scenarios
Figure 4. (Source: Daly 2014)
Figure 5. (Source: Daly 2014)
17
Comparison of U.S. and Dutch disability beneficiaries per 1,000 workers
Figure 6. (Source: Burkhauser and Daly 2011)
You might also like
- AEI Special Poll Report: Health Care and The ElectionDocument8 pagesAEI Special Poll Report: Health Care and The ElectionAmerican Enterprise InstituteNo ratings yet
- AEI Special Poll Report: Health Care and The ElectionDocument8 pagesAEI Special Poll Report: Health Care and The ElectionAmerican Enterprise InstituteNo ratings yet
- The International Union For Housing Finance 1914-2014: A 100-Year PerspectiveDocument12 pagesThe International Union For Housing Finance 1914-2014: A 100-Year PerspectiveAmerican Enterprise InstituteNo ratings yet
- The State of The American Worker 2014: Attitudes About Work in AmericaDocument72 pagesThe State of The American Worker 2014: Attitudes About Work in AmericaAmerican Enterprise InstituteNo ratings yet
- Education and OpportunityDocument17 pagesEducation and OpportunityAmerican Enterprise InstituteNo ratings yet
- House Prices and Land Prices Under The Microscope: A Property-Level AnalysisDocument38 pagesHouse Prices and Land Prices Under The Microscope: A Property-Level AnalysisAmerican Enterprise InstituteNo ratings yet
- Retirement Savings 2.0: Updating Savings Policy For The Modern EconomyDocument12 pagesRetirement Savings 2.0: Updating Savings Policy For The Modern EconomyAmerican Enterprise InstituteNo ratings yet
- Economic Insecurity: Americans' Concerns About Their Jobs, Personal Finances, Retirement, Health Costs, Housing, and MoreDocument115 pagesEconomic Insecurity: Americans' Concerns About Their Jobs, Personal Finances, Retirement, Health Costs, Housing, and MoreAmerican Enterprise InstituteNo ratings yet
- Revisiting Equity Market Structure: Principles To Promote Efficiency and FairnessDocument5 pagesRevisiting Equity Market Structure: Principles To Promote Efficiency and FairnessAmerican Enterprise InstituteNo ratings yet
- The Fed: Watchful Waiting This Year, Tough Choices Next YearDocument4 pagesThe Fed: Watchful Waiting This Year, Tough Choices Next YearAmerican Enterprise InstituteNo ratings yet
- How To Improve Economic Opportunity For Women in The USDocument26 pagesHow To Improve Economic Opportunity For Women in The USAmerican Enterprise InstituteNo ratings yet
- Economic Insecurity: Americans' Concerns About Their Jobs, Personal Finances, Retirement, Health Costs, Housing, and MoreDocument114 pagesEconomic Insecurity: Americans' Concerns About Their Jobs, Personal Finances, Retirement, Health Costs, Housing, and MoreAmerican Enterprise InstituteNo ratings yet
- Even If You Like Your Plan, You May Well Lose Your Plan. and Even If You Like Your Doctor, You May Well Lose Your DoctorDocument5 pagesEven If You Like Your Plan, You May Well Lose Your Plan. and Even If You Like Your Doctor, You May Well Lose Your DoctorAmerican Enterprise InstituteNo ratings yet
- AEI Enterprise ReportDocument8 pagesAEI Enterprise ReportAmerican Enterprise InstituteNo ratings yet
- The Ledger 08/15/14Document2 pagesThe Ledger 08/15/14American Enterprise InstituteNo ratings yet
- The Ledger 07/18/14Document2 pagesThe Ledger 07/18/14American Enterprise InstituteNo ratings yet
- The Ledger 08/08/14Document3 pagesThe Ledger 08/08/14American Enterprise InstituteNo ratings yet
- Latin America and Europe Toward A Mutual UnderstandingDocument35 pagesLatin America and Europe Toward A Mutual UnderstandingAmerican Enterprise InstituteNo ratings yet
- Iraq, Iran, Nixon's Resignation and More: A Public Opinion RundownDocument12 pagesIraq, Iran, Nixon's Resignation and More: A Public Opinion RundownAmerican Enterprise InstituteNo ratings yet
- Increasing Economic Opportunity For African Americans: Local Initiatives That Are Making A DifferenceDocument21 pagesIncreasing Economic Opportunity For African Americans: Local Initiatives That Are Making A DifferenceAmerican Enterprise InstituteNo ratings yet
- Culture of How Washington Pays For Medical CareDocument3 pagesCulture of How Washington Pays For Medical CareAmerican Enterprise InstituteNo ratings yet
- The Ledger 08/01/14Document3 pagesThe Ledger 08/01/14American Enterprise InstituteNo ratings yet
- Capital Taxation in The 21st CenturyDocument11 pagesCapital Taxation in The 21st CenturyAmerican Enterprise InstituteNo ratings yet
- AEI Special Poll Report: Health Care and The Affordable Care ActDocument18 pagesAEI Special Poll Report: Health Care and The Affordable Care ActAmerican Enterprise Institute100% (1)
- Does SNAP Support Work? Yes and NoDocument15 pagesDoes SNAP Support Work? Yes and NoAmerican Enterprise InstituteNo ratings yet
- Entrepreneurship For Human FlourishingDocument17 pagesEntrepreneurship For Human FlourishingAmerican Enterprise Institute67% (3)
- Assessing The Impact of The Dodd-Frank Act Four Years LaterDocument36 pagesAssessing The Impact of The Dodd-Frank Act Four Years LaterAmerican Enterprise InstituteNo ratings yet
- What Makes A Bank Systemically Important?Document26 pagesWhat Makes A Bank Systemically Important?American Enterprise InstituteNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Osmeña vs. Pendatun (Digest)Document1 pageOsmeña vs. Pendatun (Digest)Precious100% (2)
- Basic Principle Committee Interim Report 1950Document27 pagesBasic Principle Committee Interim Report 1950Irfan KhanNo ratings yet
- 19TH Century Philippines The World of RizalDocument35 pages19TH Century Philippines The World of RizalKenneth SablayNo ratings yet
- Business Ethics & Social ResponsibilityDocument18 pagesBusiness Ethics & Social ResponsibilitySangeethaNo ratings yet
- The Prison of MediocrityDocument3 pagesThe Prison of MediocrityPenny RonningNo ratings yet
- (Historical Materialism Book Series) Mark E. Blum, William Smaldone (Eds.) - Austro-Marxism - The Ideology of Unity Austro-Marxist Theory and Strategy. 1-Brill (2015)Document563 pages(Historical Materialism Book Series) Mark E. Blum, William Smaldone (Eds.) - Austro-Marxism - The Ideology of Unity Austro-Marxist Theory and Strategy. 1-Brill (2015)Ariel PetruccelliNo ratings yet
- Position Paper Module 11Document18 pagesPosition Paper Module 11ckayNo ratings yet
- Samson v. AguirreDocument2 pagesSamson v. AguirreNoreenesse SantosNo ratings yet
- Class 8th Winter Holiday Homework 2021-22Document5 pagesClass 8th Winter Holiday Homework 2021-22Ishani Ujjwal BhatiaNo ratings yet
- GROUP 2 - The Filipino Is Worth Dying ForDocument2 pagesGROUP 2 - The Filipino Is Worth Dying ForGian DelcanoNo ratings yet
- Animal Testing Speech/EssayDocument3 pagesAnimal Testing Speech/EssayJames1K2No ratings yet
- Kasambahay, or A Domestic Helper. They Basically Serve Our BasicDocument2 pagesKasambahay, or A Domestic Helper. They Basically Serve Our BasicJames HernandezNo ratings yet
- Postal Id Application FormDocument2 pagesPostal Id Application FormDewm Dewm100% (2)
- The Principle of SubsidiarityDocument3 pagesThe Principle of SubsidiarityMark Malaca100% (1)
- Michael Sandel Episode 8Document2 pagesMichael Sandel Episode 8Clara LimNo ratings yet
- Kenneth Plummer Lobbyist ReportsDocument8 pagesKenneth Plummer Lobbyist ReportsSamuel L. RiversNo ratings yet
- Mariategui Aesthetic ThoughtDocument26 pagesMariategui Aesthetic ThoughtSandra ManuelsdóttirNo ratings yet
- Lesson 1Document2 pagesLesson 1Kimberley Sicat BautistaNo ratings yet
- Nseera v. Ashcroft, 10th Cir. (2005)Document9 pagesNseera v. Ashcroft, 10th Cir. (2005)Scribd Government DocsNo ratings yet
- Empowerment, subsistence and a different view of global economyDocument5 pagesEmpowerment, subsistence and a different view of global economyBruna Romero-MelgarNo ratings yet
- 6Document22 pages6Stephanie BarreraNo ratings yet
- Construction of Media MessagesDocument16 pagesConstruction of Media MessagesBakirharunNo ratings yet
- Ninth EditionDocument8 pagesNinth EditionBlackConsciousness100% (1)
- Philhealth Circular 2022 - 0014 - Full Financial Risk Protection For Filipino Health Workers InfectedDocument8 pagesPhilhealth Circular 2022 - 0014 - Full Financial Risk Protection For Filipino Health Workers InfectedNanievanNo ratings yet
- Interpretation of Constitutional Provisions: Case Law Development in IndiaDocument20 pagesInterpretation of Constitutional Provisions: Case Law Development in IndiaRachit MunjalNo ratings yet
- CSA Professional Reading ListDocument18 pagesCSA Professional Reading ListAlexNo ratings yet
- SK Fund GuidelinesDocument10 pagesSK Fund GuidelinesAdry Louise Varon CandariNo ratings yet
- The Disadvantage of Cultural Diversity: 1. Language BarriersDocument2 pagesThe Disadvantage of Cultural Diversity: 1. Language BarriersChris LêNo ratings yet
- US Supreme Court JudgmentDocument2 pagesUS Supreme Court JudgmentPamela FunesNo ratings yet
- Cordora vs. ComelecDocument2 pagesCordora vs. ComelecVanna Vefsie DiscayaNo ratings yet