You might also like
- Lebel Contoh PrintDocument1 pageLebel Contoh PrintnoorgianilestariNo ratings yet
- Kahlil Gibran Part ViiDocument1 pageKahlil Gibran Part ViinoorgianilestariNo ratings yet
- Supraventricular TachycardiaDocument37 pagesSupraventricular TachycardianoorgianilestariNo ratings yet
- Proteomic ReportDocument25 pagesProteomic ReportnoorgianilestariNo ratings yet
- ACHMDocument1 pageACHMnoorgianilestariNo ratings yet
- Body Dysmorphic TraynorDocument12 pagesBody Dysmorphic TraynornoorgianilestariNo ratings yet
- Basic Concepts of Fluid and Electrolyte TherapyDocument136 pagesBasic Concepts of Fluid and Electrolyte Therapynoorgianilestari100% (2)
- Medical Disciplinary-Tugas Prof EkaDocument3 pagesMedical Disciplinary-Tugas Prof EkanoorgianilestariNo ratings yet
- Pa To GenesisDocument1 pagePa To GenesisnoorgianilestariNo ratings yet
- Daftar Pustaka Hipertensi, Diabetes dan AsmaDocument2 pagesDaftar Pustaka Hipertensi, Diabetes dan AsmanoorgianilestariNo ratings yet
- Van Den Berghe G, Wouters P, Weekers F, Et Al. Intensive Insulin Therapy in Critically Ill Patients. N Engl J Med 345: 1359-1367, 2001Document1 pageVan Den Berghe G, Wouters P, Weekers F, Et Al. Intensive Insulin Therapy in Critically Ill Patients. N Engl J Med 345: 1359-1367, 2001noorgianilestariNo ratings yet
- Van Den Berghe G, Wouters P, Weekers F, Et Al. Intensive Insulin Therapy in Critically Ill Patients. N Engl J Med 345: 1359-1367, 2001Document1 pageVan Den Berghe G, Wouters P, Weekers F, Et Al. Intensive Insulin Therapy in Critically Ill Patients. N Engl J Med 345: 1359-1367, 2001noorgianilestariNo ratings yet
- Family Medicine Residents Orthopedic Rotation HandoutDocument18 pagesFamily Medicine Residents Orthopedic Rotation HandoutRuth PoeryNo ratings yet
- Blood TransfusionDocument30 pagesBlood TransfusionnoorgianilestariNo ratings yet
- Jadwal Koas IPDDocument11 pagesJadwal Koas IPDnoorgianilestariNo ratings yet
- Diagnosis MeningitisDocument25 pagesDiagnosis MeningitisnoorgianilestariNo ratings yet
- Hasil UrinalysisDocument1 pageHasil UrinalysisnoorgianilestariNo ratings yet
- Visum et repertum report 1 October 2014Document4 pagesVisum et repertum report 1 October 2014noorgianilestariNo ratings yet
- Otitis Media AkutDocument9 pagesOtitis Media AkutnoorgianilestariNo ratings yet
- Frozen ShoulderDocument14 pagesFrozen ShouldernoorgianilestariNo ratings yet
- WEEK Orthopedics DR JohnDocument16 pagesWEEK Orthopedics DR JohnnoorgianilestariNo ratings yet
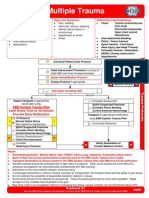
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDocument1 pageMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonNo ratings yet
- CiminoDocument2 pagesCiminonoorgianilestariNo ratings yet
- Diagnosis MeningitisDocument25 pagesDiagnosis MeningitisnoorgianilestariNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Flight Instructor Patter Ex17Document1 pageFlight Instructor Patter Ex17s ramanNo ratings yet
- Pub - Perspectives On Global Cultures Issues in Cultural PDFDocument190 pagesPub - Perspectives On Global Cultures Issues in Cultural PDFCherlyn Jane Ventura TuliaoNo ratings yet
- Agitators: Robert L. Bates, President Chemineer, IncDocument24 pagesAgitators: Robert L. Bates, President Chemineer, InctenshinomiyukiNo ratings yet
- Footprints 080311 For All Basic IcsDocument18 pagesFootprints 080311 For All Basic IcsAmit PujarNo ratings yet
- WP1019 CharterDocument5 pagesWP1019 CharternocnexNo ratings yet
- Soil Testing Lab Results SummaryDocument2 pagesSoil Testing Lab Results SummaryMd SohagNo ratings yet
- 2022 - J - Chir - Nastase Managementul Neoplaziilor Pancreatice PapilareDocument8 pages2022 - J - Chir - Nastase Managementul Neoplaziilor Pancreatice PapilarecorinaNo ratings yet
- Graphs & Charts SummariesDocument20 pagesGraphs & Charts SummariesMaj Ma Salvador-Bandiola100% (1)
- Community Development A Critical Approach PDFDocument2 pagesCommunity Development A Critical Approach PDFNatasha50% (2)
- All Types of Switch CommandsDocument11 pagesAll Types of Switch CommandsKunal SahooNo ratings yet
- Vsip - Info - Ga16de Ecu Pinout PDF FreeDocument4 pagesVsip - Info - Ga16de Ecu Pinout PDF FreeCameron VeldmanNo ratings yet
- RFID Receiver Antenna Project For 13.56 MHZ BandDocument5 pagesRFID Receiver Antenna Project For 13.56 MHZ BandJay KhandharNo ratings yet
- Jiangsu Changjiang Electronics Technology Co., Ltd. SOT-89-3L Transistor SpecificationsDocument2 pagesJiangsu Changjiang Electronics Technology Co., Ltd. SOT-89-3L Transistor SpecificationsIsrael AldabaNo ratings yet
- Monetary System 1Document6 pagesMonetary System 1priyankabgNo ratings yet
- MATH6113 - PPT5 - W5 - R0 - Applications of IntegralsDocument58 pagesMATH6113 - PPT5 - W5 - R0 - Applications of IntegralsYudho KusumoNo ratings yet
- The Power of Networking for Entrepreneurs and Founding TeamsDocument28 pagesThe Power of Networking for Entrepreneurs and Founding TeamsAngela FigueroaNo ratings yet
- Fire Pump System Test ReportDocument12 pagesFire Pump System Test Reportcoolsummer1112143100% (2)
- GEd 105 Midterm ReviewerDocument17 pagesGEd 105 Midterm ReviewerAndryl MedallionNo ratings yet
- Classification of MatterDocument2 pagesClassification of Matterapi-280247238No ratings yet
- English ProjectDocument10 pagesEnglish ProjectHarshman Singh HarshmanNo ratings yet
- Pankaj Screener 10 Oct 2014Document127 pagesPankaj Screener 10 Oct 2014Sadul Singh Naruka100% (1)
- Ethics Book of TAMIL NADU HSC 11th Standard Tamil MediumDocument140 pagesEthics Book of TAMIL NADU HSC 11th Standard Tamil MediumkumardjayaNo ratings yet
- Chapter 1 - The Empirical Beginnings and Basic Contents of Educational PsychologyDocument9 pagesChapter 1 - The Empirical Beginnings and Basic Contents of Educational PsychologyJoshua Almuete71% (7)
- Unit 01 Family Life Lesson 1 Getting Started - 2Document39 pagesUnit 01 Family Life Lesson 1 Getting Started - 2Minh Đức NghiêmNo ratings yet
- Hearing God Through Biblical Meditation - 1 PDFDocument20 pagesHearing God Through Biblical Meditation - 1 PDFAlexander PeñaNo ratings yet
- LAU Paleoart Workbook - 2023Document16 pagesLAU Paleoart Workbook - 2023samuelaguilar990No ratings yet
- Escalado / PLC - 1 (CPU 1214C AC/DC/Rly) / Program BlocksDocument2 pagesEscalado / PLC - 1 (CPU 1214C AC/DC/Rly) / Program BlocksSegundo Angel Vasquez HuamanNo ratings yet
- "The Meeting of Meditative Disciplines and Western Psychology" Roger Walsh Shauna L. ShapiroDocument13 pages"The Meeting of Meditative Disciplines and Western Psychology" Roger Walsh Shauna L. ShapiroSayako87No ratings yet
- Clinnic Panel Penag 2014Document8 pagesClinnic Panel Penag 2014Cikgu Mohd NoorNo ratings yet
- AWS S3 Interview QuestionsDocument4 pagesAWS S3 Interview QuestionsHarsha KasireddyNo ratings yet