You might also like
- 3 Jcs Physician-MedicationauthorizationDocument2 pages3 Jcs Physician-Medicationauthorizationapi-324325031No ratings yet
- A F M /P T B A A S A O - C S S E: Parent/Legal Guardian To CompleteDocument5 pagesA F M /P T B A A S A O - C S S E: Parent/Legal Guardian To CompleteSuresh BayappagariNo ratings yet
- Administration of Medicine Policy 2017 OpeningDocument15 pagesAdministration of Medicine Policy 2017 Openingapi-403062085No ratings yet
- Parental Consent Form For The Self-Administration of Medicines Section 1Document1 pageParental Consent Form For The Self-Administration of Medicines Section 1Darton CollegeNo ratings yet
- Nur 1208 2021 Prep of MedsDocument38 pagesNur 1208 2021 Prep of MedsDannielle EvangelistaNo ratings yet
- Nash Rocky Mount Public Schools Medication Administration Procedure Student Health ServicesDocument10 pagesNash Rocky Mount Public Schools Medication Administration Procedure Student Health ServicesBrayo HeroNo ratings yet
- Module 3 Pharma Safety and Quality of Drug Administration Final PDFDocument10 pagesModule 3 Pharma Safety and Quality of Drug Administration Final PDFMichelle HutamaresNo ratings yet
- MedicationadmformDocument2 pagesMedicationadmformapi-318024104No ratings yet
- 6 1 Administering Medicines August 2016Document4 pages6 1 Administering Medicines August 2016api-253519200No ratings yet
- Medication Policy Dot1Document1 pageMedication Policy Dot1api-254305845No ratings yet
- Rights of Drug AdministrationDocument4 pagesRights of Drug AdministrationAnusha VergheseNo ratings yet
- B.inggis 5 Benar ObatDocument15 pagesB.inggis 5 Benar Obatnita habibaNo ratings yet
- St. Joseph's National School: Administration of Medication Policy - February, 2018Document9 pagesSt. Joseph's National School: Administration of Medication Policy - February, 2018api-284636067No ratings yet
- Medication TeachingDocument3 pagesMedication TeachingRS Sentra Medika CisalakNo ratings yet
- DDSB Medical FormsDocument2 pagesDDSB Medical FormsMarianne RogersNo ratings yet
- Counselor Health Form1Document4 pagesCounselor Health Form1api-245061826No ratings yet
- Health Record Form: Alternative Emergency ContactsDocument1 pageHealth Record Form: Alternative Emergency Contactsemba2015No ratings yet
- Medication Release-Circle TourDocument2 pagesMedication Release-Circle TourksonicoNo ratings yet
- Mayas Med FormDocument3 pagesMayas Med Formapi-289750485No ratings yet
- Clinic FaqDocument3 pagesClinic Faqapi-260540535No ratings yet
- Medication Guidelines-Procedures 7-23-20Document1 pageMedication Guidelines-Procedures 7-23-20api-364654715No ratings yet
- Medication Permit Practioners Written OrdersDocument2 pagesMedication Permit Practioners Written OrdersRoxanne ReyNo ratings yet
- Individual Health Care Plans, EECDocument3 pagesIndividual Health Care Plans, EECBishop SchoolNo ratings yet
- Medication ProcedureDocument6 pagesMedication ProcedureRahmat BudianaNo ratings yet
- Safety and QualityDocument24 pagesSafety and QualityPaula Janine BarrogaNo ratings yet
- Medicine Policy 2011Document10 pagesMedicine Policy 2011centralwebadminNo ratings yet
- MedicationsDocument1 pageMedicationsMary CastilloNo ratings yet
- Oral Medication AdministrationDocument11 pagesOral Medication AdministrationMayank KumarNo ratings yet
- Vaccine Exemption FAQs For TexasDocument3 pagesVaccine Exemption FAQs For TexasscribuoyNo ratings yet
- Test Bank Drug Therapy 4th Edition AschenbrennerDocument8 pagesTest Bank Drug Therapy 4th Edition AschenbrennerShirley Belisle100% (30)
- Parent Medication LetterDocument3 pagesParent Medication Letterapi-449276123No ratings yet
- Permission To TreatDocument1 pagePermission To TreatMark McCoyNo ratings yet
- Pharamacology Notes 3Document7 pagesPharamacology Notes 3Martinet CalvertNo ratings yet
- Administration of Medicines Policy V2 09.21-35936Document19 pagesAdministration of Medicines Policy V2 09.21-35936Abbie StorerNo ratings yet
- Rights in Drug Administration and Medication ErrorsDocument12 pagesRights in Drug Administration and Medication ErrorsLumina lNo ratings yet
- Chapter 26: Prescribing Medications in Pediatrics Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument3 pagesChapter 26: Prescribing Medications in Pediatrics Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Ethics Uworld NotesDocument3 pagesEthics Uworld NotesActeen MyoseenNo ratings yet
- 12 Rights of Safe Drug AdministrationDocument2 pages12 Rights of Safe Drug Administrationlilcheeza77% (74)
- Administration of MedicinesDocument10 pagesAdministration of Medicinesapi-246052062No ratings yet
- Drug AdministrationDocument30 pagesDrug AdministrationandreabreeNo ratings yet
- Pharma Nursing ProcessDocument6 pagesPharma Nursing ProcessJay Bond QuiapoNo ratings yet
- 504.17 MedicationDocument3 pages504.17 MedicationMinidoka County Joint School DistrictNo ratings yet
- Ten Rights of Medication Administration With NursingimplicationsDocument4 pagesTen Rights of Medication Administration With NursingimplicationsKatrina BuenconsejoNo ratings yet
- Medications OSCE Criteria 2011-12Document3 pagesMedications OSCE Criteria 2011-12Kim GuevarraNo ratings yet
- Oral Medication PharmacologyDocument4 pagesOral Medication PharmacologyElaisa Mae Delos SantosNo ratings yet
- Pharmacy Cbahi Questions 2022Document12 pagesPharmacy Cbahi Questions 2022osama hosni100% (1)
- Leadership & Management Ethical - LegalDocument51 pagesLeadership & Management Ethical - Legalamasoud96 amasoud96No ratings yet
- 10 Rights of Drug Administration With Nursing ImplicationsDocument3 pages10 Rights of Drug Administration With Nursing ImplicationsJet Bautista100% (6)
- Focus On Nursing Pharmacology Karch 5th Edition Test BankDocument17 pagesFocus On Nursing Pharmacology Karch 5th Edition Test Bankhannahhuffmanabjskxqgnm100% (36)
- GUIDE TO SAFE MEDICINE DISPENSINGDocument7 pagesGUIDE TO SAFE MEDICINE DISPENSINGGizelle Mae Pasiol-MacayanNo ratings yet
- Bill Preamble and Section 1 For Gov Formatted Correctly Bill Section 2 Bill Section 3Document3 pagesBill Preamble and Section 1 For Gov Formatted Correctly Bill Section 2 Bill Section 3api-302995574No ratings yet
- Neo Registration Forms ADocument4 pagesNeo Registration Forms Aapi-247079386No ratings yet
- Administer Drugs SafelyDocument5 pagesAdminister Drugs SafelyIsmael JaaniNo ratings yet
- Guidelines For ConsentDocument4 pagesGuidelines For ConsentYwagar YwagarNo ratings yet
- Inform ConsentDocument9 pagesInform ConsentMeta Bachtiar100% (1)
- Principles of Drug Delivery for NursesDocument3 pagesPrinciples of Drug Delivery for NursesAjiNo ratings yet
- Medication Authorization FormDocument1 pageMedication Authorization Formheather579No ratings yet
- Administrating of MedicationDocument3 pagesAdministrating of MedicationS BindhiyaNo ratings yet
- Pharmacology A Patient Centered Nursing Process Approach Kee 8th Edition Test Bank Full DownloadDocument7 pagesPharmacology A Patient Centered Nursing Process Approach Kee 8th Edition Test Bank Full Downloadchristinehallpkadrcnjxs100% (42)
- Edutopia 10tips Classrm Management GuideDocument14 pagesEdutopia 10tips Classrm Management Guideapi-317520334No ratings yet
- Report Card Comments - Deecd - November 2014Document23 pagesReport Card Comments - Deecd - November 2014api-202232251No ratings yet
- South Colchester Academy Travel Form 2015editableDocument2 pagesSouth Colchester Academy Travel Form 2015editableapi-202232251No ratings yet
- Alignment of Achievement Levels and Reporting Codes - Using BeDocument1 pageAlignment of Achievement Levels and Reporting Codes - Using Beapi-202232251No ratings yet
- Creating An Ipp Report 1Document4 pagesCreating An Ipp Report 1api-202232251No ratings yet
- Key Messages For q1 ReportingDocument2 pagesKey Messages For q1 Reportingapi-202232251No ratings yet
- Secondary Comment Exemplars - Quarter 1Document2 pagesSecondary Comment Exemplars - Quarter 1api-202232251No ratings yet
- Nova Scotia Reporting Codes For Grades 7-12 - November 2014Document1 pageNova Scotia Reporting Codes For Grades 7-12 - November 2014api-202232251No ratings yet
- Educational Leave of 1 Year Application FormDocument2 pagesEducational Leave of 1 Year Application Formapi-202232251No ratings yet
- Teacher Initiated Inservice ApplicationDocument2 pagesTeacher Initiated Inservice Applicationapi-202232251No ratings yet
- Secondary Comment Exemplars - Quarter 1Document2 pagesSecondary Comment Exemplars - Quarter 1api-202232251No ratings yet
- Ed Leaves Less Than 1 Yr Application FormDocument2 pagesEd Leaves Less Than 1 Yr Application Formapi-202232251No ratings yet
- 7-8 Reporting Faq October28 2014Document3 pages7-8 Reporting Faq October28 2014api-202232251No ratings yet
- Nova Scotia Learner Profile For Grades 7-12 - November 2014Document1 pageNova Scotia Learner Profile For Grades 7-12 - November 2014api-202232251No ratings yet
- Short Course Instructions 1Document1 pageShort Course Instructions 1api-202232251No ratings yet
- Short Courses Claim Form BlankDocument2 pagesShort Courses Claim Form Blankapi-202232251No ratings yet
- Alignment of Achievement Levels and Reporting Codes - Using Benchmark Grades in 7-8 - October 20 DoDocument1 pageAlignment of Achievement Levels and Reporting Codes - Using Benchmark Grades in 7-8 - October 20 Doapi-202232251No ratings yet
- Teaching Restorative Practices in The Classroom 7 Lesson CurriculumDocument68 pagesTeaching Restorative Practices in The Classroom 7 Lesson Curriculumapi-202232251No ratings yet
- Conference Application Instructions 1Document1 pageConference Application Instructions 1api-202232251No ratings yet
- Conference Application FormDocument2 pagesConference Application Formapi-202232251No ratings yet
- 5 Weekreportoct 2014Document2 pages5 Weekreportoct 2014api-202232251No ratings yet
- Important Dates To RememberDocument1 pageImportant Dates To Rememberapi-202232251No ratings yet
- October Conference Day FormDocument1 pageOctober Conference Day Formapi-202232251No ratings yet
- Summer PD OpportunitiesDocument1 pageSummer PD Opportunitiesapi-202232251No ratings yet
- PD Committe Meeting Dates 20142015Document1 pagePD Committe Meeting Dates 20142015api-202232251No ratings yet
- Determining A Grade From Outcome Level Scores - October 16 2014Document4 pagesDetermining A Grade From Outcome Level Scores - October 16 2014api-202232251No ratings yet
- SetupvmDocument2 pagesSetupvmapi-202232251No ratings yet
- AccessvmDocument1 pageAccessvmapi-202232251No ratings yet
- Working With Powerteacher GradebookDocument8 pagesWorking With Powerteacher Gradebookapi-202232251No ratings yet
- How To Create An Absence On AesopDocument1 pageHow To Create An Absence On Aesopapi-202232251No ratings yet
- Sensitivity and SpecificityDocument12 pagesSensitivity and Specificitymia farrowNo ratings yet
- List of Philhealth - Car Accredited Professionals As of November 9, 2018Document18 pagesList of Philhealth - Car Accredited Professionals As of November 9, 2018Noble MagallisNo ratings yet
- 9.best Practice in Reporting of ICSRsDocument55 pages9.best Practice in Reporting of ICSRsRaghuram KashyapNo ratings yet
- Overview of Tool and Key Points: Section A: HistoryDocument4 pagesOverview of Tool and Key Points: Section A: HistoryM Naeem ArhamNo ratings yet
- Guidelines for Establishing a PharmacyDocument19 pagesGuidelines for Establishing a PharmacyFranc100% (1)
- Chicken PoxDocument13 pagesChicken PoxNiki AgustinNo ratings yet
- Ncma216: BSN 2Nd Year 1St Semester Prelim 2021: Bachelor of Science in Nursing 2YADocument32 pagesNcma216: BSN 2Nd Year 1St Semester Prelim 2021: Bachelor of Science in Nursing 2YAMARIA STEPHANY DELA CRUZ100% (1)
- SpondylolisthesisDocument121 pagesSpondylolisthesisWilliam Surya HartantoNo ratings yet
- ANTIMICROBIAL DRUGS MECHANISMS AND USESDocument11 pagesANTIMICROBIAL DRUGS MECHANISMS AND USESAudhrey BNo ratings yet
- Check QTC With Eyes - Pharmacy JoeDocument8 pagesCheck QTC With Eyes - Pharmacy JoetrezpozNo ratings yet
- The Lancet VaccinationDocument19 pagesThe Lancet VaccinationyosefNo ratings yet
- Expert Review Report - Clinical Safety of Ivermectin-March 2021Document47 pagesExpert Review Report - Clinical Safety of Ivermectin-March 2021Jim Hoft100% (1)
- Study of Different Treatment Modalities and Outcome in Preterm Babies With Respiratory Distress Syndrome 2017Document4 pagesStudy of Different Treatment Modalities and Outcome in Preterm Babies With Respiratory Distress Syndrome 2017Vita DesriantiNo ratings yet
- Relationship between knowledge, motivation and activeness of cadres in Posyandu of Puskesmas Waturu areaDocument7 pagesRelationship between knowledge, motivation and activeness of cadres in Posyandu of Puskesmas Waturu areaPristika wiyarnaNo ratings yet
- MD NephrologyDocument2,093 pagesMD Nephrologydarwish6m.6elkass100% (2)
- Stool Specimen Collection PDFDocument8 pagesStool Specimen Collection PDFJane CalderonNo ratings yet
- Special Report: Solutions For Joint and Arthritic Pain: by Jon Benson Author, Fit Over 40Document21 pagesSpecial Report: Solutions For Joint and Arthritic Pain: by Jon Benson Author, Fit Over 40tobyNo ratings yet
- Curriculum VitaeDocument2 pagesCurriculum Vitaebriton11No ratings yet
- CLUP 2014 2019 Part 1Document191 pagesCLUP 2014 2019 Part 1Mary Grace RamirezNo ratings yet
- Prenatal Care and Role of Pediatric NurseDocument40 pagesPrenatal Care and Role of Pediatric NurseMANEESH MANI67% (3)
- Paringit vs. Global GatewayDocument2 pagesParingit vs. Global GatewayRobNo ratings yet
- CV N Apply Puri MedikaDocument5 pagesCV N Apply Puri MedikayolandaNo ratings yet
- Ontario Immunization Schedule ENDocument1 pageOntario Immunization Schedule ENMing XieNo ratings yet
- Gestational Diabetes MellitusDocument69 pagesGestational Diabetes MellitusStephen BakingNo ratings yet
- New antibiotics for sepsis managementDocument27 pagesNew antibiotics for sepsis managementOlivia DwimaswastiNo ratings yet
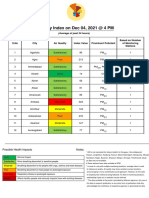
- Air Quality Index On Dec 04, 2021 at 4 PMDocument13 pagesAir Quality Index On Dec 04, 2021 at 4 PMJITANSHUCHAMPNo ratings yet
- Aquatic Animal Health and Immunology Chap-1-IntroductionDocument41 pagesAquatic Animal Health and Immunology Chap-1-IntroductionTaukir AhmedNo ratings yet
- Tuberculosis OrginalDocument11 pagesTuberculosis Orginalthanuja mathew100% (1)
- Medical Auditing Q and ADocument2 pagesMedical Auditing Q and AApril ManjaresNo ratings yet
- COM SAM Corp Pitch ShortDocument15 pagesCOM SAM Corp Pitch ShortSterghios A. MoschosNo ratings yet