You might also like
- Cluster Drive Report: Port-Harcourt - ObigboDocument50 pagesCluster Drive Report: Port-Harcourt - ObigboChika AlbertNo ratings yet
- Site Data & Test Report-Node B New SiteDocument47 pagesSite Data & Test Report-Node B New SiteChika AlbertNo ratings yet
- Cluster Drive Report: Port-Harcourt - ObigboDocument50 pagesCluster Drive Report: Port-Harcourt - ObigboChika AlbertNo ratings yet
- Cluster Drive Report: Port-Harcourt - ObigboDocument50 pagesCluster Drive Report: Port-Harcourt - ObigboChika AlbertNo ratings yet
- Final R5 Data Report TemplateDocument43 pagesFinal R5 Data Report TemplateChika AlbertNo ratings yet
- Computer Village Pre-Drive Test Report For AIRTEL Network: Date: 30-08-2018Document39 pagesComputer Village Pre-Drive Test Report For AIRTEL Network: Date: 30-08-2018Chika AlbertNo ratings yet
- 2G C11&C26 - 45 Sites - 2.25Document12 pages2G C11&C26 - 45 Sites - 2.25Chika AlbertNo ratings yet
- The Inexhaustible GodDocument6 pagesThe Inexhaustible GodChika AlbertNo ratings yet
- Mobile Handset Cellular NetworkDocument64 pagesMobile Handset Cellular NetworkSandeep GoyalNo ratings yet
- Case A α AGCH overload at the BTS β: Technology Cases Causes Cause Code Solution CodeDocument8 pagesCase A α AGCH overload at the BTS β: Technology Cases Causes Cause Code Solution CodeChika AlbertNo ratings yet
- Table View DataDocument32 pagesTable View DataChika AlbertNo ratings yet
- Eni Office To Villagio Tss - Los - Summary ReportDocument13 pagesEni Office To Villagio Tss - Los - Summary ReportChika AlbertNo ratings yet
- About ModelingDocument5 pagesAbout ModelingChika AlbertNo ratings yet
- Lg9114 - 2g SSV ReportDocument24 pagesLg9114 - 2g SSV ReportChika AlbertNo ratings yet
- Abuja Physical Optimization Audit ReportDocument32 pagesAbuja Physical Optimization Audit ReportChika AlbertNo ratings yet
- GIM 11 5 Kaufman 200498 SDC1Document11 pagesGIM 11 5 Kaufman 200498 SDC1jawadg123No ratings yet
- 2G C11&C26 - 45 Sites - 2.25Document12 pages2G C11&C26 - 45 Sites - 2.25Chika AlbertNo ratings yet
- Gariki Cluster Pre - Post Report Poor StretchesDocument14 pagesGariki Cluster Pre - Post Report Poor StretchesChika AlbertNo ratings yet
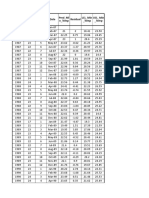
- Months Month Date Residual Min - Te MP Pred - Mi N - Temp LCL - Min - Temp UCL - Min - TempDocument13 pagesMonths Month Date Residual Min - Te MP Pred - Mi N - Temp LCL - Min - Temp UCL - Min - TempChika AlbertNo ratings yet
- Allocated SiteDocument18 pagesAllocated SiteChika AlbertNo ratings yet
- Eni Office To Md's Residence Tss - Los - Summary ReportDocument13 pagesEni Office To Md's Residence Tss - Los - Summary ReportChika AlbertNo ratings yet
- Eni Office To Md's Residence Tss - Los - Summary ReportDocument13 pagesEni Office To Md's Residence Tss - Los - Summary ReportChika AlbertNo ratings yet
- Eni Office To Md's Residence Tss - Los - Summary ReportDocument13 pagesEni Office To Md's Residence Tss - Los - Summary ReportChika AlbertNo ratings yet
- Ss 2 TFDocument10 pagesSs 2 TFChika AlbertNo ratings yet
- Abuja Physical Optimization Audit ReportDocument32 pagesAbuja Physical Optimization Audit ReportChika AlbertNo ratings yet
- S/N Site ID Site Address Site Cordinate: No3, Iweanya Ugbogoh Crecent, Lekki Phase1Document9 pagesS/N Site ID Site Address Site Cordinate: No3, Iweanya Ugbogoh Crecent, Lekki Phase1Chika AlbertNo ratings yet
- All Links TSS - LOS - Summary ReportDocument14 pagesAll Links TSS - LOS - Summary ReportChika AlbertNo ratings yet
- PS PS Attach Detach MS1Document6 pagesPS PS Attach Detach MS1Chika AlbertNo ratings yet
- PS PS Attach Detach MS1Document6 pagesPS PS Attach Detach MS1Chika AlbertNo ratings yet
- PS Attach Setup Time (MS)Document2 pagesPS Attach Setup Time (MS)Chika AlbertNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Philippine Saviours: Narratives of Filipino Intensive Care Nurses and Their Ways On Handling Chronically Ill PatientsDocument38 pagesPhilippine Saviours: Narratives of Filipino Intensive Care Nurses and Their Ways On Handling Chronically Ill PatientsHannah SampianoNo ratings yet
- Test AaDocument55 pagesTest AaKaye PatanindagatNo ratings yet
- MDMA-assisted Therapy Significantly Reduces Eating Disorder Symptoms in A Randomized Placebo-Controlled Trial of Adults With Severe PTSDDocument8 pagesMDMA-assisted Therapy Significantly Reduces Eating Disorder Symptoms in A Randomized Placebo-Controlled Trial of Adults With Severe PTSDKayla GreenstienNo ratings yet
- Nurses Progress NotesDocument2 pagesNurses Progress Notesvan100% (1)
- Presentation 1Document16 pagesPresentation 1Azhari AhmadNo ratings yet
- IMCI Chart BookletDocument66 pagesIMCI Chart Bookletnorwin_033875No ratings yet
- Back Pain During PregnancyDocument3 pagesBack Pain During PregnancyDr. Sadhana KalaNo ratings yet
- Blood Testing For DioxinsDocument2 pagesBlood Testing For DioxinstedmozbiNo ratings yet
- Abstrak EnglishDocument1 pageAbstrak EnglishputrapaninjauanNo ratings yet
- Halamang GamotDocument32 pagesHalamang GamotJasmin PastoresNo ratings yet
- Blood and Tissue Flagellates BSCDocument27 pagesBlood and Tissue Flagellates BSCSisay FentaNo ratings yet
- Food Surety - Food Fraud Prevention Checklist (3p)Document3 pagesFood Surety - Food Fraud Prevention Checklist (3p)Mark KwanNo ratings yet
- TheraDocument4 pagesTheramaircusNo ratings yet
- Written Assignment Principles of Applied RehabilitationDocument17 pagesWritten Assignment Principles of Applied RehabilitationRuqaiyah RahmanNo ratings yet
- Nutritional Knowledge Among Malaysian ElderlyDocument12 pagesNutritional Knowledge Among Malaysian ElderlyNoor Khairul AzwanNo ratings yet
- 50 Item Psychiatric Nursing Exam IDocument11 pages50 Item Psychiatric Nursing Exam Iɹǝʍdןnos98% (40)
- Domestic Violence Cycle of Violence Types of Families-2Document22 pagesDomestic Violence Cycle of Violence Types of Families-2api-340420872No ratings yet
- Va Tech ReportDocument260 pagesVa Tech Reportbigcee64No ratings yet
- Asa PSC System PDFDocument2 pagesAsa PSC System PDFKen WonNo ratings yet
- The Real ThesisDocument35 pagesThe Real ThesisDanielle Cezarra FabellaNo ratings yet
- Snake Bite SOPDocument5 pagesSnake Bite SOPRaza Muhammad SoomroNo ratings yet
- SR - Hse Officer (8104)Document5 pagesSR - Hse Officer (8104)Nijo Joseph100% (1)
- The Effectiveness of Information System in Divine Mercy Hospitalsan Pedro LagunaDocument22 pagesThe Effectiveness of Information System in Divine Mercy Hospitalsan Pedro LagunamartNo ratings yet
- Synthesis PaperDocument7 pagesSynthesis Paperapi-379148533No ratings yet
- Types of PovertyDocument6 pagesTypes of PovertyJacobNo ratings yet
- Handbook: Master of Social Work StudiesDocument26 pagesHandbook: Master of Social Work StudiesSukhman ChahalNo ratings yet
- Book - MOSBY'S DENTAL DRUG REFERENCE PDFDocument1,496 pagesBook - MOSBY'S DENTAL DRUG REFERENCE PDFMohamed Faizal78% (9)
- MiraMate Light Pad InstructionsDocument8 pagesMiraMate Light Pad InstructionsLaurentMartinonNo ratings yet
- Personal Safety With Dance: Worksheet in Health Optimizing Physical Education 3 (HOPE3/PEH3)Document9 pagesPersonal Safety With Dance: Worksheet in Health Optimizing Physical Education 3 (HOPE3/PEH3)Cregie Brillantes QuezaNo ratings yet
- PEC in INDIA ExplainationDocument3 pagesPEC in INDIA ExplainationSaumya ChandraNo ratings yet