You might also like
- Islamic University of Gaza Faculty of Medicine ROOM Video Conf. Fifth Floor Male and Female Students - 6th Year Week 1Document2 pagesIslamic University of Gaza Faculty of Medicine ROOM Video Conf. Fifth Floor Male and Female Students - 6th Year Week 1salamredNo ratings yet
- Chronic DiarrheaDocument6 pagesChronic DiarrheasalamredNo ratings yet
- MCQ On MenopauseDocument4 pagesMCQ On Menopausesalamred100% (3)
- Pelvis Types and Labor StagesDocument7 pagesPelvis Types and Labor Stagessalamred100% (1)
- RadiologyDocument5 pagesRadiologysalamredNo ratings yet
- MCQs Psy Exam44 First GroupDocument7 pagesMCQs Psy Exam44 First Groupsalamred100% (2)
- Psychiatry Final Exam 2014Document2 pagesPsychiatry Final Exam 2014Ibrahem Y. NajjarNo ratings yet
- HemoptysisDocument3 pagesHemoptysissalamredNo ratings yet
- MCQ Net 3Document5 pagesMCQ Net 3salamredNo ratings yet
- ةعومجم نم لا Reports ةيطغم جهنملا ءاشنا لا مكبجعت: Report of toxicologyDocument14 pagesةعومجم نم لا Reports ةيطغم جهنملا ءاشنا لا مكبجعت: Report of toxicologysalamredNo ratings yet
- Solutions To The Test CasesDocument11 pagesSolutions To The Test CasessalamredNo ratings yet
- امتحان الاشعة العملي النهائيDocument1 pageامتحان الاشعة العملي النهائيsalamredNo ratings yet
- Ortho OSCE 2008Document3 pagesOrtho OSCE 2008salamredNo ratings yet
- MCQs Psy Exam44 First GroupDocument7 pagesMCQs Psy Exam44 First Groupsalamred100% (2)
- MCQs on key psych topicsDocument17 pagesMCQs on key psych topicssalamredNo ratings yet
- اسبيرو طويل مهم جدا الثلاثاءDocument22 pagesاسبيرو طويل مهم جدا الثلاثاءsalamredNo ratings yet
- Choose The Best Appropriate Answerfor Each of The Following QuestionsDocument12 pagesChoose The Best Appropriate Answerfor Each of The Following QuestionssalamredNo ratings yet
- Rectal bleeding causes and treatment optionsDocument21 pagesRectal bleeding causes and treatment optionslinaleen67% (3)
- Longitudinal Esophagotomy (Hellers) 4 Frey"s Syndrome: Sever InfectionDocument4 pagesLongitudinal Esophagotomy (Hellers) 4 Frey"s Syndrome: Sever InfectionsalamredNo ratings yet
- Liver Surgery Procedures & ComplicationsDocument10 pagesLiver Surgery Procedures & ComplicationsIbrahem Y. NajjarNo ratings yet
- The Answer KeyDocument1 pageThe Answer KeysalamredNo ratings yet
- PMC Exam 2006Document27 pagesPMC Exam 2006salamredNo ratings yet
- 333Document13 pages333salamredNo ratings yet
- MSQU Course MontadaDocument39 pagesMSQU Course MontadasalamredNo ratings yet
- A) Basic Surgical SciencesDocument27 pagesA) Basic Surgical SciencessalamredNo ratings yet
- breastطباعةDocument3 pagesbreastطباعةsalamredNo ratings yet
- MCQDocument11 pagesMCQsalamredNo ratings yet
- Choose The Best Appropriate Answerfor Each of The Following QuestionsDocument12 pagesChoose The Best Appropriate Answerfor Each of The Following QuestionssalamredNo ratings yet
- Dr:-Ashraf .I. ObaidDocument22 pagesDr:-Ashraf .I. ObaidsalamredNo ratings yet
- A) Basic Surgical SciencesDocument27 pagesA) Basic Surgical SciencessalamredNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
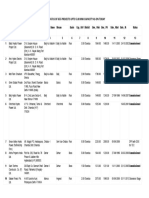
- List/Status of 655 Projects Upto 5.00 MW Capacity As On TodayDocument45 pagesList/Status of 655 Projects Upto 5.00 MW Capacity As On Todayganvaqqqzz21No ratings yet
- A Chat (GPT) About The Future of Scientific PublishingDocument3 pagesA Chat (GPT) About The Future of Scientific Publishingraul kesumaNo ratings yet
- DepEd K to 12 Awards PolicyDocument29 pagesDepEd K to 12 Awards PolicyAstraea Knight100% (1)
- BrianmayDocument4 pagesBrianmayapi-284933758No ratings yet
- Adjusted School Reading Program of Buneg EsDocument7 pagesAdjusted School Reading Program of Buneg EsGener Taña AntonioNo ratings yet
- Article Summary Assignment 2021Document2 pagesArticle Summary Assignment 2021Mengyan XiongNo ratings yet
- Global Pre-Qualification - Registration of Vendors For Supply of Various Raw Materials - ProductsDocument2 pagesGlobal Pre-Qualification - Registration of Vendors For Supply of Various Raw Materials - Productsjavaidkhan83No ratings yet
- El Rol Del Fonoaudiólogo Como Agente de Cambio Social (Segundo Borrador)Document11 pagesEl Rol Del Fonoaudiólogo Como Agente de Cambio Social (Segundo Borrador)Jorge Nicolás Silva Flores100% (1)
- The Scavenger's Handbook v1 SmallerDocument33 pagesThe Scavenger's Handbook v1 SmallerBeto TNo ratings yet
- Week 5 WHLP Nov. 2 6 2020 DISSDocument5 pagesWeek 5 WHLP Nov. 2 6 2020 DISSDaniel BandibasNo ratings yet
- English Course SyllabusDocument3 pagesEnglish Course Syllabusalea rainNo ratings yet
- Iso 1964 1987Document11 pagesIso 1964 1987Dina ANDRIAMAHEFAHERYNo ratings yet
- Instant Download Ebook PDF Energy Systems Engineering Evaluation and Implementation Third 3rd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Energy Systems Engineering Evaluation and Implementation Third 3rd Edition PDF Scribdmichael.merchant471100% (43)
- General Physics 1: Activity Title: What Forces You? Activity No.: 1.3 Learning Competency: Draw Free-Body DiagramsDocument5 pagesGeneral Physics 1: Activity Title: What Forces You? Activity No.: 1.3 Learning Competency: Draw Free-Body DiagramsLeonardo PigaNo ratings yet
- A Brief History of The White Nationalist MovementDocument73 pagesA Brief History of The White Nationalist MovementHugenNo ratings yet
- Supplier of PesticidesDocument2 pagesSupplier of PesticidestusharNo ratings yet
- Fatwa Backbiting An Aalim Fatwa Razwiya PDFDocument3 pagesFatwa Backbiting An Aalim Fatwa Razwiya PDFzubairmbbsNo ratings yet
- MT 1 Combined Top 200Document3 pagesMT 1 Combined Top 200ShohanNo ratings yet
- Hbo Chapter 6 Theories of MotivationDocument29 pagesHbo Chapter 6 Theories of MotivationJannelle SalacNo ratings yet
- Genocide/Politicides, 1954-1998 - State Failure Problem SetDocument9 pagesGenocide/Politicides, 1954-1998 - State Failure Problem SetSean KimNo ratings yet
- Christian Mission and Conversion. Glimpses About Conversion, Constitution, Right To ReligionDocument8 pagesChristian Mission and Conversion. Glimpses About Conversion, Constitution, Right To ReligionSudheer Siripurapu100% (1)
- Bajaj Allianz General Insurance Company LimitedDocument9 pagesBajaj Allianz General Insurance Company LimitedNaresh ChanchadNo ratings yet
- Under the Angels Restaurant Transports Guests to Old CracowDocument2 pagesUnder the Angels Restaurant Transports Guests to Old CracowBence KlusóczkiNo ratings yet
- Feminism in Lucia SartoriDocument41 pagesFeminism in Lucia SartoriRaraNo ratings yet
- Bhojpuri PDFDocument15 pagesBhojpuri PDFbestmadeeasy50% (2)
- Research Course Outline For Resarch Methodology Fall 2011 (MBA)Document3 pagesResearch Course Outline For Resarch Methodology Fall 2011 (MBA)mudassarramzanNo ratings yet
- The Greco-Turkish War of 1920-1922: Greece Seeks Territory in Asia MinorDocument14 pagesThe Greco-Turkish War of 1920-1922: Greece Seeks Territory in Asia MinorFauzan Rasip100% (1)
- NAME: - CLASS: - Describing Things Size Shape Colour Taste TextureDocument1 pageNAME: - CLASS: - Describing Things Size Shape Colour Taste TextureAnny GSNo ratings yet
- Voiceless Alveolar Affricate TsDocument78 pagesVoiceless Alveolar Affricate TsZomiLinguisticsNo ratings yet
- Little Match GirlDocument8 pagesLittle Match GirlsubhaseduNo ratings yet