You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 01 - Newborn Physical ExamDocument2 pages01 - Newborn Physical Examgerald_valeriano0% (1)
- Board Reveiw Electrolyte Acid Base MCQ and AnswerDocument15 pagesBoard Reveiw Electrolyte Acid Base MCQ and AnswerEma100% (8)
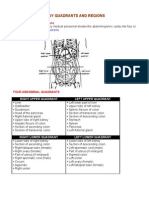
- Organs in The Body Quadrants and RegionsDocument3 pagesOrgans in The Body Quadrants and RegionsDavid HosamNo ratings yet
- Application GuidelinesDocument3 pagesApplication GuidelinesAfricancollegeof HTNo ratings yet
- Year 4 Semester 2 ReportDocument3 pagesYear 4 Semester 2 ReportAfricancollegeof HTNo ratings yet
- About (Founder at African College of Health)Document3 pagesAbout (Founder at African College of Health)Africancollegeof HTNo ratings yet
- Naturopathy YEAR 1 SEMESTER 1 WEEK 2 of 12Document18 pagesNaturopathy YEAR 1 SEMESTER 1 WEEK 2 of 12Africancollegeof HTNo ratings yet
- Year 2 Semester 3 ReportDocument4 pagesYear 2 Semester 3 ReportAfricancollegeof HTNo ratings yet
- Year 5 Semester 2 ReportDocument2 pagesYear 5 Semester 2 ReportAfricancollegeof HTNo ratings yet
- African College of Health: Occupational English Test (OET) NOTESDocument1 pageAfrican College of Health: Occupational English Test (OET) NOTESAfricancollegeof HTNo ratings yet
- ApplyDocument3 pagesApplyAfricancollegeof HTNo ratings yet
- Course Description BHSC (Nat)Document1 pageCourse Description BHSC (Nat)Africancollegeof HTNo ratings yet
- Year 5 Semester 1 ReportDocument2 pagesYear 5 Semester 1 ReportAfricancollegeof HTNo ratings yet
- African College of Health's FormDocument5 pagesAfrican College of Health's FormAfrican College of Health (ACH)No ratings yet
- Year 2 Semester 3 ReportDocument4 pagesYear 2 Semester 3 ReportAfricancollegeof HTNo ratings yet
- ACH's Web PageDocument10 pagesACH's Web PageAfricancollegeof HT100% (1)
- Year 5 Semester 3 ReportDocument2 pagesYear 5 Semester 3 ReportAfricancollegeof HTNo ratings yet
- Year 4 Semester 3 ReportDocument3 pagesYear 4 Semester 3 ReportAfricancollegeof HTNo ratings yet
- ACH's B.PHARM YEAR 4, SEMESTER 3, WEEK 5 NOTESDocument12 pagesACH's B.PHARM YEAR 4, SEMESTER 3, WEEK 5 NOTESAfricancollegeof HTNo ratings yet
- ACH's B.PHARM YEAR 2 SEMESTER 3 WEEK 8 NOTESDocument35 pagesACH's B.PHARM YEAR 2 SEMESTER 3 WEEK 8 NOTESAfricancollegeof HTNo ratings yet
- Year 2 Semester 3 ReportDocument4 pagesYear 2 Semester 3 ReportAfricancollegeof HTNo ratings yet
- ACH's MBBS YEAR 2 SEMESTER 3 WEEK 8 NOTESDocument24 pagesACH's MBBS YEAR 2 SEMESTER 3 WEEK 8 NOTESAfricancollegeof HTNo ratings yet
- ACH's BNS YEAR 2 SEMESTER 3 WEEK 8 NOTESDocument20 pagesACH's BNS YEAR 2 SEMESTER 3 WEEK 8 NOTESAfricancollegeof HTNo ratings yet
- Year 4 Semester 1 ReportDocument3 pagesYear 4 Semester 1 ReportAfricancollegeof HTNo ratings yet
- Year 2 Semester 3 ReportDocument4 pagesYear 2 Semester 3 ReportAfricancollegeof HTNo ratings yet
- ACH's MBBS YEAR 2 SEMESTER 3 WEEK 1 NOTESDocument27 pagesACH's MBBS YEAR 2 SEMESTER 3 WEEK 1 NOTESAfricancollegeof HTNo ratings yet
- ACH's BNS YEAR 2 SEMESTER 3 WEEK 1 NOTESDocument19 pagesACH's BNS YEAR 2 SEMESTER 3 WEEK 1 NOTESAfricancollegeof HTNo ratings yet
- Year 2 Semester 3 ReportDocument4 pagesYear 2 Semester 3 ReportAfricancollegeof HTNo ratings yet
- ACH's BNS YEAR 2 SEMESTER 2 WEEK 5 NOTESDocument37 pagesACH's BNS YEAR 2 SEMESTER 2 WEEK 5 NOTESAfricancollegeof HTNo ratings yet
- Year 2 Semester 3 ReportDocument4 pagesYear 2 Semester 3 ReportAfricancollegeof HTNo ratings yet
- ACH's MBBS YEAR 2 SEMESTER 1 WEEK 10 NOTESDocument94 pagesACH's MBBS YEAR 2 SEMESTER 1 WEEK 10 NOTESAfricancollegeof HTNo ratings yet
- ACH's MBBS YEAR 2 SEMESTER 1 WEEK 10 NOTESDocument94 pagesACH's MBBS YEAR 2 SEMESTER 1 WEEK 10 NOTESAfricancollegeof HTNo ratings yet
- NO Nama Alat Jumlah Kondisi Baik RusakDocument6 pagesNO Nama Alat Jumlah Kondisi Baik RusakRumah Sakit Umum KartiniNo ratings yet
- DEMO, SXGA, MP90, Initial, D.0x.xx, Rev XXXDocument25 pagesDEMO, SXGA, MP90, Initial, D.0x.xx, Rev XXXahmadba70No ratings yet
- Veta 3 - Datasheet - ENG - 20210315Document2 pagesVeta 3 - Datasheet - ENG - 20210315JuanNo ratings yet
- Trauma y Memoria Procedural 2015 Paper Peter LevineDocument18 pagesTrauma y Memoria Procedural 2015 Paper Peter LevineMaría Regina Castro CataldiNo ratings yet
- Facial Action Coding SystemDocument13 pagesFacial Action Coding SystemBarkha ShahNo ratings yet
- Eng Hamid & Zakaria PDFDocument5 pagesEng Hamid & Zakaria PDFTiga TujuhNo ratings yet
- ACLS JeopardyDocument3 pagesACLS JeopardyLaylee Clare100% (1)
- Blood Supply of BrainDocument49 pagesBlood Supply of BrainDarling Sevenfoldism SynysterNo ratings yet
- Biology: Sexual ReproductionDocument7 pagesBiology: Sexual ReproductionAllan BustamanteNo ratings yet
- Antifungal Task Involving Punicalagin Nystatin Combinations Towards Vaginal Yeast InfectionsqnidvDocument1 pageAntifungal Task Involving Punicalagin Nystatin Combinations Towards Vaginal Yeast Infectionsqnidvhoursail5No ratings yet
- ABO Incompatibility in NewbornsDocument4 pagesABO Incompatibility in NewbornsNollen LaquianNo ratings yet
- Farmakologi Antiagina TTMDocument83 pagesFarmakologi Antiagina TTMEpha Lumban GaolNo ratings yet
- DIPIRO Gagal GinjalDocument19 pagesDIPIRO Gagal Ginjalselfa louhenapessyNo ratings yet
- Pharmacology Toxicology - 4th EdDocument41 pagesPharmacology Toxicology - 4th EdYorlenie Juárez100% (1)
- Sleep Studies: in The Sleep Laboratory and in The Home: Patient EducationDocument2 pagesSleep Studies: in The Sleep Laboratory and in The Home: Patient EducationALINo ratings yet
- Hemodynamic Management Pocket Card PDFDocument8 pagesHemodynamic Management Pocket Card PDFjenn1722No ratings yet
- Cranial NervesDocument118 pagesCranial NervesGan'sNo ratings yet
- Frazeologie EnglezaDocument11 pagesFrazeologie EnglezaMaria MkNo ratings yet
- Artificial OrgansDocument184 pagesArtificial OrganshemavathyrajasekaranNo ratings yet
- Review of Placenta DeliveryDocument3 pagesReview of Placenta DeliverygitapramodhaNo ratings yet
- Myocardial Infarction: Myocardial Infarction (MI) or Acute Myocardial Infarction (AMI), Commonly KnownDocument6 pagesMyocardial Infarction: Myocardial Infarction (MI) or Acute Myocardial Infarction (AMI), Commonly KnownLyka Cuanan CorcueraNo ratings yet
- Frog Dissection (Remote)Document21 pagesFrog Dissection (Remote)Mohammad NiyaifarNo ratings yet
- Understanding CLL: A Guide For Patients Who Want To Take Charge of Chronic Lymphocytic LeukemiaDocument4 pagesUnderstanding CLL: A Guide For Patients Who Want To Take Charge of Chronic Lymphocytic LeukemiaNakul Singh ParkwayIndiaNo ratings yet
- Lab 09 HandoutDocument8 pagesLab 09 HandoutHyenaNo ratings yet
- Uro ChordataDocument4 pagesUro ChordataSana SiddiqueNo ratings yet
- Fantasy/Imagination: Patti M. ValkenburgDocument3 pagesFantasy/Imagination: Patti M. ValkenburgalbertoadalidNo ratings yet
- Proprioceptive Training HandballDocument23 pagesProprioceptive Training HandballRoginicD100% (1)