You might also like
- AJODO-2013 Claudino 143 6 799Document11 pagesAJODO-2013 Claudino 143 6 799player osamaNo ratings yet
- Articulo 1 AdfDocument5 pagesArticulo 1 AdfANA MARÍA MANCERA CAMACHONo ratings yet
- CVM McnamaraDocument11 pagesCVM McnamaraXnb HajiNo ratings yet
- The Cervical Vertebral MaturationMcNamaraDocument86 pagesThe Cervical Vertebral MaturationMcNamararrnotholtNo ratings yet
- Airway Changes After Cleft Orthognathic Surgery Evaluated by Three-Dimensional Computed Tomography and Overnight Polysomnographic Study (2017)Document7 pagesAirway Changes After Cleft Orthognathic Surgery Evaluated by Three-Dimensional Computed Tomography and Overnight Polysomnographic Study (2017)Jean Carlos Barbosa FerreiraNo ratings yet
- El 2011Document11 pagesEl 2011popsilviaizabellaNo ratings yet
- ARTICULO Cirugia OrtognaticaDocument9 pagesARTICULO Cirugia OrtognaticaDavid DíazNo ratings yet
- A Comparative Analysis of Aerodynamic and Anatomic Characteristics of Upper Airway Before and After Mini-Implant - Assisted Rapid Maxillary ExpansionDocument10 pagesA Comparative Analysis of Aerodynamic and Anatomic Characteristics of Upper Airway Before and After Mini-Implant - Assisted Rapid Maxillary Expansion7vvfm4qqyxNo ratings yet
- A Novel Technique For Short Nose CorrectionDocument74 pagesA Novel Technique For Short Nose CorrectionJWPlasticsurgeryNo ratings yet
- ModelDocument11 pagesModelpopsilviaizabellaNo ratings yet
- Jiang 216Document8 pagesJiang 216Lizbeth K. Espada De la CruzNo ratings yet
- Retrospective Study of Maxillary Sinus Dimensions and Pneumatization in Adult Patients With An Anterior Open BiteDocument6 pagesRetrospective Study of Maxillary Sinus Dimensions and Pneumatization in Adult Patients With An Anterior Open BiteAntonio Pizarroso GonzaloNo ratings yet
- AJODO-2013 Angelieri 144 5 759Document11 pagesAJODO-2013 Angelieri 144 5 759osama-alali100% (1)
- 3-D Airway Analysis Reveals Differences Between Class II and III Skeletal MorphologyDocument4 pages3-D Airway Analysis Reveals Differences Between Class II and III Skeletal MorphologyAndrea BeltránNo ratings yet
- Effects of Rapid Maxillary Expansion On Upper Airway Volume: A Three-Dimensional Cone-Beam Computed Tomography StudyDocument7 pagesEffects of Rapid Maxillary Expansion On Upper Airway Volume: A Three-Dimensional Cone-Beam Computed Tomography StudyVishal SharmaNo ratings yet
- Effect of Class III Bone Anchor Treatment On Airway: Tung Nguyen Hugo de Clerck Michael Wilson Brent GoldenDocument6 pagesEffect of Class III Bone Anchor Treatment On Airway: Tung Nguyen Hugo de Clerck Michael Wilson Brent GoldenQickie AmaliaNo ratings yet
- 020Document13 pages020Lima JúniorNo ratings yet
- 1. 1-s2.0-S0278239119305518-mainDocument15 pages1. 1-s2.0-S0278239119305518-mainALEJANDRA INÉS NIETO ARIASNo ratings yet
- Three-Dimensional Analysis of The Airway With Cone-Beam Computed TomographyDocument9 pagesThree-Dimensional Analysis of The Airway With Cone-Beam Computed TomographySoe San KyawNo ratings yet
- Articulo Cone BeanDocument9 pagesArticulo Cone Beanernesto chavez ruizNo ratings yet
- International Journal of Pediatric Otorhinolaryngology: SciencedirectDocument5 pagesInternational Journal of Pediatric Otorhinolaryngology: SciencedirectDiego Andres Hincapie HerreraNo ratings yet
- Pharyngeal Airway Evaluation Following Isolated Surgical Mandibular Advancement: A 1-Year Follow-UpDocument9 pagesPharyngeal Airway Evaluation Following Isolated Surgical Mandibular Advancement: A 1-Year Follow-UpMonojit DuttaNo ratings yet
- Reliability of Habets and Kjellberg TechniquesDocument8 pagesReliability of Habets and Kjellberg TechniquesLuz MendozaNo ratings yet
- Comparison of Airway Dimensions in Skeletal Class I PDFDocument8 pagesComparison of Airway Dimensions in Skeletal Class I PDFSoe San KyawNo ratings yet
- Relationship Between Surface Area and Volume of The Mastoid Air Cell System in Adult HumansDocument8 pagesRelationship Between Surface Area and Volume of The Mastoid Air Cell System in Adult HumansNurul Falah KalokoNo ratings yet
- Chitsazi 2017 AAADocument6 pagesChitsazi 2017 AAAJavi ChavezNo ratings yet
- Jced 5 E231Document8 pagesJced 5 E231ruben dario meza bertelNo ratings yet
- Three-Dimensional Reconstruction of Maxillae Using Spiral Computed Tomography and Its Application in Postoperative Adult Patients With Unilateral Complete Cleft Lip and PalateDocument9 pagesThree-Dimensional Reconstruction of Maxillae Using Spiral Computed Tomography and Its Application in Postoperative Adult Patients With Unilateral Complete Cleft Lip and PalateDiego Andres Hincapie HerreraNo ratings yet
- Effect of Mono and BimaxillaryDocument6 pagesEffect of Mono and BimaxillarytamisatnamNo ratings yet
- BJR 85 897 PDFDocument8 pagesBJR 85 897 PDFRila NurulNo ratings yet
- Effects of Surgically Assisted Rapid Maxillary Expansion On Mandibular Position - A Three - Dimensional StudyDocument7 pagesEffects of Surgically Assisted Rapid Maxillary Expansion On Mandibular Position - A Three - Dimensional StudyDaniel Carvalho de AraújoNo ratings yet
- 2017 AksuDocument7 pages2017 AksuR. Yair Delgado JaimesNo ratings yet
- Cone Beam CT Analysis of Mandibular PositionsDocument8 pagesCone Beam CT Analysis of Mandibular PositionsMilton Francisco Pinto VidalNo ratings yet
- Class II (Comments) PDFDocument102 pagesClass II (Comments) PDFJamal GiriNo ratings yet
- Kim 2010Document11 pagesKim 2010popsilviaizabellaNo ratings yet
- 12 - RyszDocument5 pages12 - RyszElvita Srie WahyuniNo ratings yet
- Comparison of Natural Head Position in Different Anteroposterior MalocclusionsDocument12 pagesComparison of Natural Head Position in Different Anteroposterior MalocclusionsRebin AliNo ratings yet
- Diagnostic Performance of Skeletal Maturity For The Assessment of Midpalatal Suture MaturationDocument7 pagesDiagnostic Performance of Skeletal Maturity For The Assessment of Midpalatal Suture MaturationArthur CésarNo ratings yet
- A Method of Cephalometric Evaluation Mcnamara 1984Document21 pagesA Method of Cephalometric Evaluation Mcnamara 1984Gaurav Pratap SinghNo ratings yet
- 1-s2.0-S0901502721003581-mainDocument7 pages1-s2.0-S0901502721003581-mainCaio GonçalvesNo ratings yet
- J - A Clinico-Radiographic AnalysisDocument34 pagesJ - A Clinico-Radiographic AnalysisSusovan GiriNo ratings yet
- Comparison Between Skeletal, and Facial Measurements of Vertical Dimension in Edentulous PatientsDocument4 pagesComparison Between Skeletal, and Facial Measurements of Vertical Dimension in Edentulous Patientspaula catanaNo ratings yet
- Tepecik 2018Document39 pagesTepecik 2018Lorena PaulaNo ratings yet
- Evaluation of Nose and Paranasal Sinus Disease, Anatomical Variations by Computerized TomographyDocument6 pagesEvaluation of Nose and Paranasal Sinus Disease, Anatomical Variations by Computerized TomographyChika MarzelinaNo ratings yet
- Cephalometric Assessment in OSADocument10 pagesCephalometric Assessment in OSAAkanksha SrivastavaNo ratings yet
- Comparison of The Pharyngeal Airways of PatientsDocument10 pagesComparison of The Pharyngeal Airways of PatientsfriscaNo ratings yet
- Artroscopia de Ombro, Estudo CadavéricoDocument9 pagesArtroscopia de Ombro, Estudo CadavéricoRenato SiqueiraNo ratings yet
- AJODO 2017aksuetalDocument8 pagesAJODO 2017aksuetalALEJANDRA INÉS NIETO ARIASNo ratings yet
- Relation Between Sagittal Position of The Mandible and Pharyngeal Airway Volume in Adults Using Cone Beam Computed TomographyDocument9 pagesRelation Between Sagittal Position of The Mandible and Pharyngeal Airway Volume in Adults Using Cone Beam Computed TomographyIJAR JOURNALNo ratings yet
- Kjod 53 1 35Document10 pagesKjod 53 1 35강북다인치과No ratings yet
- Iwasaki 2009Document9 pagesIwasaki 2009popsilviaizabellaNo ratings yet
- Artikel OccipitomentaDocument12 pagesArtikel OccipitomentaSharon NathaniaNo ratings yet
- Three-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFDocument10 pagesThree-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFSoe San KyawNo ratings yet
- Evaluation of Upper Airways After Bimaxillary OrthognathicDocument8 pagesEvaluation of Upper Airways After Bimaxillary OrthognathicLisbethNo ratings yet
- A Hybrid Method For Airway Segmentation and Automated MeasurementDocument17 pagesA Hybrid Method For Airway Segmentation and Automated Measurementannatje.martens4No ratings yet
- Evaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyDocument10 pagesEvaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyPututu PatataNo ratings yet
- Effects of Case Western Reserve University's Transverse Analysis On The Quality of Orthodontic TreatmentDocument15 pagesEffects of Case Western Reserve University's Transverse Analysis On The Quality of Orthodontic TreatmentIsmaelLouGomezNo ratings yet
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementFrom EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNo ratings yet
- Pulmonary Functional Imaging: Basics and Clinical ApplicationsFrom EverandPulmonary Functional Imaging: Basics and Clinical ApplicationsYoshiharu OhnoNo ratings yet
- Sputnik V en The LancetDocument11 pagesSputnik V en The LancetLARED21No ratings yet
- Validity of Bond Strength TestDocument8 pagesValidity of Bond Strength TestAbad SalcedoNo ratings yet
- 3D Virtual Treatment Planning of Orthognathic Surgery A Step-By-Step Approach For Orthodontists and SurgeonsDocument580 pages3D Virtual Treatment Planning of Orthognathic Surgery A Step-By-Step Approach For Orthodontists and SurgeonsAbad Salcedo100% (4)
- Zuhr Et Al-2014-Journal of Clinical PeriodontologyDocument20 pagesZuhr Et Al-2014-Journal of Clinical PeriodontologyAbad Salcedo100% (1)
- Myths and RealitiesDocument6 pagesMyths and RealitiesAbad SalcedoNo ratings yet
- Phukaoluan2016 PDFDocument16 pagesPhukaoluan2016 PDFAbad SalcedoNo ratings yet
- Choi 2015Document9 pagesChoi 2015Abad SalcedoNo ratings yet
- Zucchelli Et Al-2015-Periodontology 2000Document36 pagesZucchelli Et Al-2015-Periodontology 2000Abad Salcedo100% (1)
- Retention in Orthodontics: Verifiable CPD PaperDocument4 pagesRetention in Orthodontics: Verifiable CPD PaperAbad SalcedoNo ratings yet
- Zou Et Al-2015-Clinical Implant Dentistry and Related ResearchDocument11 pagesZou Et Al-2015-Clinical Implant Dentistry and Related ResearchAbad SalcedoNo ratings yet
- Myths and RealitiesDocument6 pagesMyths and RealitiesAbad SalcedoNo ratings yet
- 2015-Journal of Clinical PeriodontologyDocument8 pages2015-Journal of Clinical PeriodontologyAbad SalcedoNo ratings yet
- Diastemas Brasil PDFDocument8 pagesDiastemas Brasil PDFAbad SalcedoNo ratings yet
- Potential Errors and Misuse of Statistics in StudiesDocument9 pagesPotential Errors and Misuse of Statistics in StudiesAbad SalcedoNo ratings yet
- 10 1016@j Ajodo 2009 03 051Document8 pages10 1016@j Ajodo 2009 03 051Abad SalcedoNo ratings yet
- Roth y DaMONDocument8 pagesRoth y DaMONAbad SalcedoNo ratings yet
- 10 1016@j Ajodo 2009 03 051Document8 pages10 1016@j Ajodo 2009 03 051Abad SalcedoNo ratings yet
- Analisis de Vomer BasilliDocument14 pagesAnalisis de Vomer BasilliAbad SalcedoNo ratings yet
- Biomecanica Clase II 2Document8 pagesBiomecanica Clase II 2Abad SalcedoNo ratings yet
- Jco - 2008 03 157 PDFDocument7 pagesJco - 2008 03 157 PDFAbad SalcedoNo ratings yet
- Molar Distalization PDFDocument3 pagesMolar Distalization PDFdruzair00775% (4)
- Estetica Dental y EnciaDocument8 pagesEstetica Dental y EnciaAbad SalcedoNo ratings yet
- Molar Distalization PDFDocument3 pagesMolar Distalization PDFdruzair00775% (4)
- Diastema Closure and Long-Term Stability - JCO-OnLINEDocument15 pagesDiastema Closure and Long-Term Stability - JCO-OnLINEAbad SalcedoNo ratings yet
- Stability of Quadhelix Crib Therapy inDocument9 pagesStability of Quadhelix Crib Therapy inAbad SalcedoNo ratings yet
- Epigenetic Influence of KAT6B and HDAC4Document9 pagesEpigenetic Influence of KAT6B and HDAC4Abad SalcedoNo ratings yet
- Brasil Dias Ten MasDocument7 pagesBrasil Dias Ten MasAbad SalcedoNo ratings yet
- Pi Is 0889540613006641Document9 pagesPi Is 0889540613006641Abad SalcedoNo ratings yet
- Diastema Closure and Long-Term Stability - JCO-OnLINEDocument15 pagesDiastema Closure and Long-Term Stability - JCO-OnLINEAbad SalcedoNo ratings yet
- WP 2012-1 Multiple Risk Factors in Young Children's Development - SABATES, R AND DEX, S PDFDocument32 pagesWP 2012-1 Multiple Risk Factors in Young Children's Development - SABATES, R AND DEX, S PDFAziah ShatarNo ratings yet
- Crim Law CasesDocument33 pagesCrim Law CasesRanrave Marqueda DiangcoNo ratings yet
- Health AssessmentDocument160 pagesHealth AssessmentJerome TingNo ratings yet
- VPA 221 Veterinary Entomology and Acarology: PsoroptidaeDocument7 pagesVPA 221 Veterinary Entomology and Acarology: PsoroptidaeRamesh BeniwalNo ratings yet
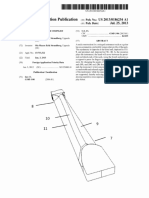
- Trapezoidal Neck Strandberg US20130186254A1Document10 pagesTrapezoidal Neck Strandberg US20130186254A1Percy Stanbury Malaga100% (1)
- Burst FractureDocument5 pagesBurst FractureAzmi FarhadiNo ratings yet
- Splints (Compatibility Mode)Document14 pagesSplints (Compatibility Mode)wese87No ratings yet
- FTU CountDocument1 pageFTU CountOliver QNo ratings yet
- Radiology of Rodents, Rabbits, and Ferrets - An Atlas of Normal Anatomy and PositioningDocument303 pagesRadiology of Rodents, Rabbits, and Ferrets - An Atlas of Normal Anatomy and PositioningCinthia RodriguezNo ratings yet
- Anesthesiology - Pain ManagementDocument284 pagesAnesthesiology - Pain ManagementAngelines Eliche100% (3)
- Frog MusculatureDocument2 pagesFrog MusculaturePatricia SioNo ratings yet
- Biomechanics of Ankle and Foot: Joint Structures and FunctionsDocument38 pagesBiomechanics of Ankle and Foot: Joint Structures and FunctionsAnish BishwakarmaNo ratings yet
- Odynophagia Is Painful SwallowingDocument21 pagesOdynophagia Is Painful SwallowingVien CaagbayNo ratings yet
- GEHealthcare Brochure Discovery MR750w3 0TDocument20 pagesGEHealthcare Brochure Discovery MR750w3 0Tdr9348345000No ratings yet
- Act.07 Toad's External AnatomyDocument7 pagesAct.07 Toad's External AnatomykjfcoierjfoirfNo ratings yet
- Hologic Discovery and Explorer SpecificationsDocument2 pagesHologic Discovery and Explorer SpecificationsQaiserAnwarNo ratings yet
- Medical Terms (Prefixes Suffixes Roots)Document5 pagesMedical Terms (Prefixes Suffixes Roots)David Donovan ManuelNo ratings yet
- ISAK Antrophometric CourseDocument5 pagesISAK Antrophometric Coursekabut81No ratings yet
- Tumor MielumDocument2 pagesTumor MielumFidya Ainun TikhaNo ratings yet
- Introduction To The Body As A Whole 03032022Document28 pagesIntroduction To The Body As A Whole 03032022Aafia sarwarNo ratings yet
- DLab Activity 1 - Understanding Human BodyDocument9 pagesDLab Activity 1 - Understanding Human BodySYDNEY JILL ACHAINo ratings yet
- Basics of Human AnatomyDocument4 pagesBasics of Human AnatomyskidamarinkNo ratings yet
- Physio Anatomy PDFDocument70 pagesPhysio Anatomy PDFevatang100% (1)
- Online Anatomy and Physiology Lab ManualDocument11 pagesOnline Anatomy and Physiology Lab ManualKenken Mijares100% (1)
- A key to seven species of the Neotropical earwig genus IdolopsalisDocument6 pagesA key to seven species of the Neotropical earwig genus Idolopsalisbolosphex1634No ratings yet
- Anatomy of The Peripheral Vascular System-FHHDocument33 pagesAnatomy of The Peripheral Vascular System-FHHOmar Ali AyoubkhanNo ratings yet
- Eizenberg's General AnatomyDocument255 pagesEizenberg's General Anatomymushroom620100% (9)
- filePV 27 05 377Document9 pagesfilePV 27 05 377pifmanNo ratings yet
- The Attachments of The Breast To The Chest Wall: A Dissection StudyDocument12 pagesThe Attachments of The Breast To The Chest Wall: A Dissection StudyjuanrangoneNo ratings yet
- Reflexology For Migraine HeadachesDocument12 pagesReflexology For Migraine Headachescharles100% (1)