You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Class:-9TH Subject: - Biology Chapter: - 4 (Why Do We Fall ILL)Document26 pagesClass:-9TH Subject: - Biology Chapter: - 4 (Why Do We Fall ILL)DEEPAK KaswanNo ratings yet
- Hepatitis BDocument12 pagesHepatitis BEmicar TecNo ratings yet
- Epidemiology TriangleDocument1 pageEpidemiology TriangleMelDred Cajes BolandoNo ratings yet
- Abo Reverse TypingDocument3 pagesAbo Reverse Typinglindsay becudoNo ratings yet
- PCAP ReportDocument28 pagesPCAP ReportAngeline Zamoras-ToledoNo ratings yet
- CDC Streamlines COVID-19 GuidanceDocument9 pagesCDC Streamlines COVID-19 GuidanceJessica A. BotelhoNo ratings yet
- Surviving COVID-19 PandemicDocument3 pagesSurviving COVID-19 PandemicTrisha Camille OrtegaNo ratings yet
- Japanese EncephalitisDocument35 pagesJapanese EncephalitisMasrizal Dt MangguangNo ratings yet
- Head Lice Infestation GuideDocument17 pagesHead Lice Infestation GuideAstuti Clara Simanjuntak100% (1)
- CONCLUSION-Lab Report MicroDocument2 pagesCONCLUSION-Lab Report Microfdhln sakinahNo ratings yet
- Medication For Staph InfectionDocument7 pagesMedication For Staph InfectiondelmontlabsNo ratings yet
- A. Referencing Using APA Styles: Use The Following Data in Writing References WithDocument3 pagesA. Referencing Using APA Styles: Use The Following Data in Writing References Withangelo barrettoNo ratings yet
- STDs and STIs Chapter 29 Group 4Document53 pagesSTDs and STIs Chapter 29 Group 4Davis Kallan100% (2)
- Topnotch Microbiology Supertable by DR - Cocoy Calderon Jaffar Pineda Troy Soberano UPDATED NOVEMBER 2017Document16 pagesTopnotch Microbiology Supertable by DR - Cocoy Calderon Jaffar Pineda Troy Soberano UPDATED NOVEMBER 2017Jaybee Sarmiento100% (1)
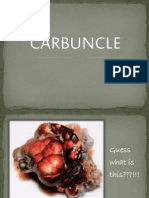
- CarbuncleDocument23 pagesCarbuncleProtantagonistNo ratings yet
- Heron Herbals: Treating Lyme DiseaseDocument3 pagesHeron Herbals: Treating Lyme DiseaseterryvndNo ratings yet
- About Hot Water Seed Treatment: Crop Diseases ControlledDocument3 pagesAbout Hot Water Seed Treatment: Crop Diseases ControlledYusuf UmarNo ratings yet
- Plot No.428, Phase-IV, Udyog Vihar, Gurgaon, Haryana - 122 015Document3 pagesPlot No.428, Phase-IV, Udyog Vihar, Gurgaon, Haryana - 122 015aditya bNo ratings yet
- Could Wearing Masks Long-Term Harm HealthDocument3 pagesCould Wearing Masks Long-Term Harm HealthakbirNo ratings yet
- Brief History of ImmunologyDocument5 pagesBrief History of Immunologyella SyNo ratings yet
- Formulation of Mosquito Repellent Lotion by Using Oregano (, Neem Tree and Lemongrass Extracted OilDocument9 pagesFormulation of Mosquito Repellent Lotion by Using Oregano (, Neem Tree and Lemongrass Extracted OilSimi- Simi0% (1)
- History of ImmunizationDocument37 pagesHistory of Immunizationkaan yükselNo ratings yet
- FHSIS report for Sampaloc BrgyDocument3 pagesFHSIS report for Sampaloc BrgyBe NjNo ratings yet
- pm2 TREMATODESDocument39 pagespm2 TREMATODESshastaNo ratings yet
- AntelmintikDocument17 pagesAntelmintikUlfahl HaerullinaNo ratings yet
- Sariaya Curfew Ordinance Imposes 8pm-5am RestrictionDocument4 pagesSariaya Curfew Ordinance Imposes 8pm-5am RestrictionAlfonseNo ratings yet
- Explanation Text Covid-19Document2 pagesExplanation Text Covid-19Mr ClawNo ratings yet
- Chlamydia InfectionsDocument4 pagesChlamydia InfectionsPearl CalisNo ratings yet
- Knowledge and Practices On Infection Control Among Health Workers in Jinja Regional Referral HospitalDocument8 pagesKnowledge and Practices On Infection Control Among Health Workers in Jinja Regional Referral HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Dengue FeverDocument24 pagesDengue FeverSNN100% (1)