CURRENT OPINION
Text
Pediatr Drugs 2007; 9 (3): 143-148
1174-5878/07/0003-0143/$44.95/0
2007 Adis Data Information BV. All rights reserved.
Delays in Immunization Have Potentially Serious
Health Consequences
Fernando A. Guerra1,2,3
1
2
3
Director of Health, San Antonio Metropolitan Health District, San Antonio, Texas, USA
Department of Pediatrics, University of Texas Health Science Center, San Antonio, Texas, USA
Department of Public Health, Air Force School of Aerospace Medicine, Brooks Air Force Base, San Antonio, Texas, USA
Abstract
When children are not administered vaccinations according to the recommended schedule, they not only fail
to receive timely protection from preventable diseases at a time when they are most vulnerable, but also increase
their risk of never fully completing the vaccination course. Both outcomes compromise a successful childhood
immunization program. Although current data suggest that vaccination rates are near 95% for school-aged
children in the US, the rate of timely vaccination is much lower. A number of large studies have found that the
majority of children are not currently vaccinated on schedule. Moreover, immunization levels for 2- to 3-yearold children have reached a plateau.
It is essential to recognize that low overall rates of the targeted diseases mask the persistent threat they pose if
adherence to vaccination schedules declines. A delay in one vaccine will produce a domino effect if catch-up
adjustments in scheduled visits are not implemented aggressively. Published reports have demonstrated that
failure to adhere to scheduled booster immunizations, not just the initial inoculation, results in resurgence of
disease. Children fall off the vaccination schedule for a variety of reasons. Although many studies suggest that
inadequate availability to healthcare is not a major determinant of delayed immunization, it still factors into
parental decisions. Parents should be reminded of available healthcare options. From the clinicians end,
computerization of healthcare records should allow for the generation of reminders. It is vital for clinicians to be
aware that there are few contraindications to vaccination. They should also be prepared to address parental
concerns regarding the safety of vaccines and should not hesitate to use topical analgesics or distraction
techniques to facilitate inoculation.
With the anticipation of several novel vaccines being added to the childhood and adolescent immunization
schedule in the future, pediatricians face new challenges to not only provide every vaccination, but to do so in a
timely manner. A lack of willingness on the part of the parent, or, occasionally, on the part of the clinician, to
have multiple vaccines administered to the child during a single visit has been shown to be a significant cause of
delayed vaccination. Since combination vaccines reduce the number of shots that need to be administered, the
use of combination vaccines may provide the best opportunity to simplify the immunization schedule, increasing
adherence in the process. Improved adherence to established schedules may present a major opportunity to
further protect children from disease.
According to 20056 aggregate state estimates collected by the
National Immunization Program, more than 95% of children entering kindergarten in the US were vaccinated for polio, measles,
mumps, rubella, diphtheria, tetanus, and pertussis.[1] These rates
demonstrate only an incremental climb over those reported in
20045 and 20034 and are the highest achieved to date for those
series of vaccines.[1,2] As vaccination rates have increased, many
diseases, such as polio and smallpox, have been essentially eliminated from the US.[3] Most recently, the director of the Centers for
Disease Control and Prevention (CDC) declared that rubella, of
144
which only eight US cases were reported in 2006, can no longer be
considered a major health threat in the US.[4,5]
Despite this progress, important challenges remain. In particular, the cumulative rates of vaccination at school admission mask
the frequency with which delivery of one or more doses of the
vaccine is delayed.[6-8] The risks posed by a significant delay,
defined as 6 months, are not just theoretical. Published reports,
most notably those evaluating outbreaks of pertussis, have demonstrated that failure to adhere to scheduled booster immunizations,
not just the initial inoculation, results in resurgence of disease.[9-12]
It is essential to recognize that low overall rates of the targeted
diseases mask the persistent threat they pose if adherence to
vaccination schedules declines. Although the risks posed by specific lengths of delay in vaccination are not well defined and may
differ for different boosters in the series, improved adherence to
established schedules may present a major opportunity to further
protect children from disease.
1. Timeliness of Vaccination: A Poor Record
Cumulative vaccination rates are a useful measure of the penetration of national immunization programs but they may be misleading for assessing protection from childhood diseases. Whether
rates are evaluated at school entry, when parents must produce an
immunization record as part of the registration process, or at
earlier timepoints, such as at age 2 years, when children are closer
to peak susceptibility for many of the infections vaccines are
designed to prevent, cumulative vaccination data can conceal
significant periods of no or inadequate protection. A number of
large studies have found that the majority of children are not
currently vaccinated on schedule.[13-16]
In 2005, Luman et al.[17] published data from the 2003 National
Immunization Survey (NIS), which collected information on
14 810 children between the ages of 24 and 35 months, and
revealed that only 26% of children were vaccinated in a timely
fashion. While an additional 29% of children received all of their
vaccines <6 months after the schedule, 37% of children had delays
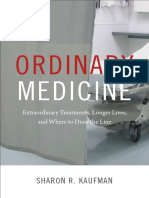
in vaccine delivery of at least 6 months. Serious delays in vaccination, defined as being under-vaccinated for >6 months in at least
four of the six vaccines evaluated (hepatitis B, Haemophilus
influenzae type b, poliovirus, varicella, the combination of diphtheria, tetanus, and acellular pertussis [DTaP], and the combination of measles, mumps, and rubella), were found in 21% of those
surveyed (figure 1). While vaccination rates have been increasing
in school-aged children, immunization levels for 2- to 3-year-old
children have reached a plateau at 7075%.[18]
2007 Adis Data Information BV. All rights reserved.
Number of children under-vaccinated (%)2
Guerra
40
35
Total: 34.2%
Number of vaccines1 delayed
01
23
4
Total: 37.1%
Total: 28.6%
30
25
20
15
10
5
0
<1
16
>6
Under-vaccination period3 (mo)
Fig. 1. Months under-vaccinated during first 24 months of life and number
of vaccines delayed. Delay begins after the end of a recommendation
period and continues until the child is vaccinated or reaches 24 months of
age. Data from Luman et al.[17] 1 One or more doses of six vaccines:
diphtheria, tetanus toxoids, and acellular pertussis; poliovirus; measles,
mumps, and rubella; Haemophilus influenzae type b; hepatitis B; and varicella; 2 Based on weighted data; 3 During the first 24 months of life for one
or more doses of a recommended vaccine.
The overall 2003 NIS results suggest children in the US are
under-vaccinated by a mean of 172 days for all vaccines during the
first 24 months of life.[17] Among children with any delay, 52%
were under-vaccinated for at least 6 months, and 15% of all
children were under-vaccinated for more than 12 of their first 24
months.
2. Delayed Vaccination Poses a Major Threat
There is good evidence that delays in vaccination are associated
with risk. Some simulation models predict up to a 40% increase in
cases of pertussis over 1 year when delays in delivery of the DTaP
combination vaccine exceed 6 months.[19] This prediction has been
supported by several studies of subsequent outbreaks. In one
analysis of a series of pertussis outbreaks in the US in the 1990s,
54% of infants were under-vaccinated for their age.[19] In a significant outbreak that occurred in 19934 in Chicago, 52% of cases
occurred in young infants who had not yet completed the normal
vaccination schedule, but 20% of cases were attributed to failure to
provide vaccination on time.[9] In Auckland, New Zealand, the
odds ratio for developing pertussis in an outbreak during 19957
was increased 4.5-fold by delay in receiving any of the three doses
of DTaP.[20] For a delay in the third dose alone, the odds ratio of
developing pertussis was increased by slightly more than 6-fold.
Moreover, the focus on infection rates in under-vaccinated children does not capture the full impact of missed or delayed immunization. For example, there is evidence that under-vaccinated older
Pediatr Drugs 2007; 9 (3)
Health Consequences of Delays in Immunization
siblings provide an important vector of transmission of pertussis to
infants not yet old enough to receive the vaccine.[21] It is reasonable to predict that other susceptible individuals, such as those who
are immunocompromised, are also at risk when children are undervaccinated.
In an analysis of an epidemic in measles in the US that began in
1989, the increase in measles cases was found to be concentrated
in preschool children predominantly from inner city populations
who had not been vaccinated on schedule.[11] Failure to enforce
measles immunization laws for the school-aged children in this
epidemic, which produced 25 000 cases and 60 deaths in 1990
alone, was identified as one of the contributing factors.[22] In
20014, only 177 cases of measles were reported to the CDC, but
100 (56%) were considered preventable because they occurred in
candidates for the vaccine who missed one or more doses.[23] A
study evaluating children who received exemptions from measles
immunizations not only demonstrated a steep increase in measles
cases among those exempted but a substantial increase in cases
among non-exempted individuals.[24]
In a study of H. influenzae type b infections in Canada over a
3-year period (20013), 20 (69%) of the 29 cases occurred in
children without any vaccination or those with incomplete vaccination.[12] While 11 of the cases were in children too young to have
completed the series, nine (i.e. almost half of the cases) occurred in
children with significant delays or whose parents had refused the
initial or subsequent doses.
3. Delayed versus Missed Vaccinations
Vaccination schedules in childhood were developed to provide
protection over peak periods of risk and they serve as one basis for
well child check-ups. Delays in providing vaccine on schedule
pose two major threats. The first is that children will not be
provided immunity when they are most vulnerable. The second is
that a delay in one vaccine will produce a domino effect if catch-up
adjustments in scheduled visits are not implemented aggressively,
extending the period at which children remain at risk for preventable diseases.[25,26]
The first threat is underscored by the fact that the peak incidences of many of the diseases for which vaccines are administered occur early in life. For example, the incidence of H. influenzae infection, although rare before the age of 3 months, rises
steeply over the first year of life, peaking between 6 and 12
months.[27] After 4 years, rates are relatively low. Substantial rates
of pertussis, rubella, and varicella also occur in children under the
age of 3 years. Although the major risk of outbreaks is concen 2007 Adis Data Information BV. All rights reserved.
145
trated in school environments when there is a maximal opportunity
for disease transmission, the risks to preschool children from
serious sequelae of preventable diseases, including those who are
not enrolled in daycare or another setting with close interpersonal
contact, should not be underestimated.
The second threat from delayed immunization is supported by
several studies suggesting that failure to receive vaccinations on
schedule increases the risk of failing to ever achieve full immunization.[25,28] In an evaluation of 4691 children who had missed at
least one immunization between 15 and 24 months of age, 9%
went on to miss the remaining immunizations.[28] This rate of
missed immunization persisted despite subsequent opportunities
to provide immunizations during urgent office visits, which were
made by 53% of under-immunized children during the study
period. In almost 80% of cases, there was no contraindication for
immunization at the time of the urgent visit.
In a study evaluating why children were under-immunized at 3
months of age, defined as failure to receive DTaP, poliovirus,
H. influenzae type b, and hepatitis B vaccines on schedule, the
most significant factor was missed opportunities, such as a decision to forego a scheduled immunization at a time when the child
was ill.[29] Indeed, 85% of children had received at least one dose
of one of the vaccines, suggesting that access to appropriate
healthcare was not a major obstacle. In an analysis of coverage for
the 4 : 3 : 1 : 3 vaccine series (four or more doses of DTaP, three
or more doses of poliovirus vaccine, one or more doses of any
measles-containing vaccine, and three or more doses of H. influenzae type b vaccine) in 1999 NIS data, missed opportunities, not
lack of access to care, was found to be the major factor for undervaccination of non-Hispanic, African American preschoolers.[30]
4. Strict Adherence to Schedules is Critical
All of the currently recommended vaccines have demonstrated
significant protection against the diseases at which they are
targeted, but no protection is absolute. Failure to strive for 100%
participation in recommended vaccination schedules risks exacerbating outbreaks due to both the risks of primary vaccine failure
and diminished herd immunity (the indirect protection received by
the un- or under-immunized segment of a population in which a
large proportion is immunized).[31] Achieving adequate herd immunity is particularly important in a population of young children
who can spread disease quite easily. Both phenomena may explain
disease outbreaks where there have been good but suboptimal
rates of vaccination. A measles outbreak in one school in Texas,
USA, was documented even though only 4.2% were seronegative
Pediatr Drugs 2007; 9 (3)
146
prior to the event.[22] It is possible that cases of disease in unvaccinated children overwhelmed suboptimal immunity to infection
in children who, despite seropositivity, received incomplete vaccination.
The risk of outbreaks from diminishing adherence to vaccination schedules differs by disease. For example, the efficacy of the
vaccine for measles, mumps, and rubella has been estimated to
range from 93% to 98%,[32,33] while the efficacy for the varicella
vaccine ranges from 70% to 90%.[34,35] Similarly, although only
about an 80% immunization rate is required to confer herd immunity to polio, the rate is estimated to be approximately 90% for
measles. Sophisticated mathematical models are not required to
predict that the lowest risk of disease outbreaks is achieved when
the maximum number of children receive full vaccination at the
scheduled doses. However, the number of parents who seek an
exemption from vaccination is increasing across the US.[36] These
children can serve as a reservoir for disease, and may contribute to
community outbreaks by spreading illness to those children who
are under-vaccinated.
One approach to evaluating the risks posed by suboptimal
immunization rates has been the series of studies evaluating disease incidence among children exempted from immunization.[24]
Although all 50 states of the US require proof of immunizations
for school admission, 48 states allow religious exemptions, which
are granted for a variety of criteria.[37] These studies show that the
risk of developing the diseases for which they have not been
vaccinated increases dramatically even when exempted individuals form a small minority of the community in which they live. In
data collected by the CDC from 1985 through 1992, those who
chose to be exempt from vaccination for religious or philosophical
reasons were 35 times more likely to contract measles than vaccinated persons.[24] Outbreaks of pertussis and rubella have also
been recorded in religious communities opposing immunization.[37] Importantly, the risks of non-vaccination are not contained
among children who forego immunization but are passed to vaccinated children, another strong argument for uniform adherence to
recommended vaccination schedules. A study undertaken in Colorado, USA, found exempted children to have a 22.2-fold increased
risk of measles than vaccinated children; rates of disease were also
higher in vaccinated children than expected from national data.[38]
Other studies have also projected an increased risk of preventable
infections in vaccinated children when exposed to unvaccinated
children.[24] The evidence that vaccinated children are put at risk
by inadequately vaccinated children, whether due to missed opportunities, refusal, or delays, is a critical issue for both public health
policy and clinical decisions at the level of the individual patient.
2007 Adis Data Information BV. All rights reserved.
Guerra
In a modeling study based on clinical data, it was calculated that if
the proportion of exemptors doubled, the incidence of measles
infection in non-exempted vaccinated individuals could increase
by as much as 60% depending on intergroup mixing ratios.[24]
The data suggesting that exemptors pose a health risk to children compliant with immunization requirements raises thorny
issues about individual rights. The same issues of responsibility to
the community may also be raised by failure to obtain timely
vaccinations. Children who are not vaccinated on schedule not
only face the risks already enumerated but increase the health risks
of the community at large.
As diseases targeted by vaccines diminish in prevalence due to
successful prevention programs, it is easy to become complacent
about their potential threat. Some diseases, such as poliomyelitis,
have become sufficiently rare that clinicians know of them only
through pictures. However, the pathogens persist in the community, and vaccines are essential to prevent resurgence. In 2006, the
WHO counted 1977 cases of poliomyelitis worldwide.[39] Moreover, not all of the health benefits of vaccines are adequately
captured in statistics. For example, children with respiratory syncytial virus, for which there is not yet a vaccine, are likely to have
a worse outcome if simultaneously infected with another respiratory pathogen, such as H. influenzae.[40]
5. Measures to Increase On-Time Immunization
The program of childhood immunization has already been
adapted to maximize the likelihood of adherence. This includes a
schedule of immunizations that coincides with well child visits
and the effort to use combination vaccines when possible to reduce
the number of inoculations required at each visit.[8,41] There are a
variety of reasons that children fall off the vaccination schedule,
but it is imperative to consider both healthcare- and parent-related
obstacles to full and timely compliance.[42]
On the healthcare side of the equation, good methodology for
ensuring that children registered in a healthcare system, whether
an office practice or managed care organization, are on schedule
for well child visits and scheduled immunizations is an essential
first step.[29,43] Computerization of healthcare records may help
with this task and in generating reminders when appropriate.
Clinicians should also be aware that there are few contraindications to vaccination, most of which can be performed even at a
sick visit. All office visits for children of vaccination age should
be considered opportunities to review immunization records and to
provide vaccines when appropriate. Clinicians should also be
prepared to address parental concerns regarding the safety of
Pediatr Drugs 2007; 9 (3)
Health Consequences of Delays in Immunization
vaccines, which may encompass a broad range of issues. Clinicians should not hesitate to use topical analgesics or distraction
techniques to facilitate inoculation and reduce the potential psychologic burden of needle use for both parent and child. These
techniques have proven to reduce the pain associated with vaccination without affecting protective antibody levels.[44,45] The development of combination vaccines has had an important impact
on reducing the number of injections, a step that both reduces
needle use and facilitates compliance.[46]
On the parental side of the equation, a wide variety of fears
contribute to delays in scheduled vaccinations or induce parents to
forego vaccinations altogether.[47] Some of the most commonly
expressed concerns regard excessive pain produced by multiple
injections at the same visit, the potential for overstimulation of the
immune system, and the potential risks of immunization. A variety
of objective data are available to refute the legitimacy of these
claims in the context of the benefits of immunization.[48,49] However, even far more unreasonable objections cannot be dismissed if
they pose a threat to timely immunization against preventable
diseases. Appropriate education about the risks posed to the child
as well as risks posed to others may prove essential. If injections
are delayed, a catch-up methodology should be in place in order to
bring children up to schedule. As discussed in section 4, one of the
major risks of delaying one immunization is eventual failure to
ever complete the immunization schedule.
It is not enough to recognize that under-vaccination is a problem. Rather, clinicians should embark on specific steps to reduce
the number of children who fail to receive on-time vaccination.
This includes recognizing the sources of missed opportunities,
such as failing to vaccinate a sick child despite the absence of
contraindications, or anticipating potential obstacles for compliance in families, such as limited resources or transportation
problems. Programs are available to provide vaccines even to
children without medical coverage.[50] Clinicians should assume
an active role in caring for children who are at high risk of falling
through the cracks of multiple health programs that impede complete record keeping.
6. Conclusion
The reduction in major diseases of childhood through national
immunization programs has been a story of success, but one that
must be continuously repeated each year with on-time initiation of
the series, boosters, and completion. The threat to building on the
current level of success comes from complacency that prevents
strict adherence to timely administration of vaccines as well as
2007 Adis Data Information BV. All rights reserved.
147
changing perceptions about the urgency of vaccination in a time
when the incidence of many of these diseases is low. While current
US data suggest that vaccination rates are near 95% for schoolaged children, the rate of timely administration of vaccines is
much lower, posing its own threat to the optimal protection against
the morbidity and mortality of serious communicable diseases. It
is appropriate to take satisfaction in the high overall rates of
vaccination, but it is also essential that more be done to improve
timely vaccination.
Acknowledgments
BioCentric, Inc. provided editorial assistance. Funding for these services
was provided to BioCentric, Inc. by GlaxoSmithKline. The author has received no compensation associated with this article.
References
1. CDC. Coverage estimates for school entry vaccinations [online]. Available from
URL: http://www2.cdc.gov/nip/schoolsurv/nationalAvg.asp [Accessed 2007
Feb 16]
2. CDC. Vaccination coverage among children entering 200304 school year in the
United States. MMWR Morb Mortal Wkly Rep 2004; 53: 1041-4
3. CDC. Special report: 50 years of immunization success. CDC annual reports 2005
[online]. Available from URL: http://www.cdc.gov/nip/webutil/about/annualrpts/ar205/special-report-2005.pdf [Accessed 2005 Dec 16]
4. Gerberding J. Rubella no longer a major health threat. National Immunization
Conference; 2005 Mar 21; Washington, DC
5. CDC. Notifiable diseases/deaths in selected cities weekly information. MMWR
Morb Mortal Wkly Rep 2006; 55: 1396
6. Mell LK, Ogren DS, Davis RL, et al. Compliance with national immunization
guidelines for children younger than 2 years, 19961999. Pediatrics 2005; 115:
461-7
7. Barker L, Luman E, Zhao Z, et al. National, state, and urban area vaccination
coverage levels among children aged 1935 months: United States, 2001.
MMWR Morb Mortal Wkly Rep 2002; 51: 664-6
8. Luman ET, Barker LE, McCauley MM, et al. Timeliness of childhood immunizations: a state-specific analysis. Am J Public Health 2005; 95: 1367-74
9. Kenyon TS, Izurieta H, Shulman ST, et al. Large outbreak of pertussis among
young children in Chicago, 1993: investigation of potential contributing factors
and estimation of vaccine effectiveness. Pediatr Infect Dis J 1996; 15: 655-61
10. Farizo KM, Cochi SL, Zell ER, et al. Epidemiological features of pertussis in the
United States, 19801989. Clin Infect Dis 1992; 14: 708-19
11. National Vaccine Advisory Committee. The measles epidemic: the problems,
barriers, and recommendations. JAMA 1991; 266: 1547-52
12. Scheifele D, Halperin S, Law B, et al. Invasive Haemophilus influenzae type b
infections in vaccinated and unvaccinated children in Canada, 20012003.
CMAJ 2005; 172: 53-6
13. Wood D, Halfon N, Pereyra M, et al. Knowledge of the childhood immunization
schedule and of contraindications to vaccinate by private and public providers
in Los Angeles. Pediatr Infect Dis J 1996; 15: 140-5
14. Bolton P, Hussain A, Hadpawat A, et al. Deficiencies in current childhood
immunization indicators. Public Health Reports 1998; 113: 527-32
15. Dominguez SR, Parrott JS, Lauderdale DS, et al. On-time immunization rates
among children who enter Chicago public schools. Pediatrics 2004; 114: 741-7
16. Santoli JM, Huet NJ, Smith PJ, et al. Insurance status and vaccination coverage
among US preschool children. Pediatrics 2004; 113: 1959-64
17. Luman ET, Barker LE, Shaw KM, et al. Timeliness of childhood vaccinations in
the United States. JAMA 2005; 283: 1204-11
Pediatr Drugs 2007; 9 (3)
148
18. CDC. National, state, and urban area vaccination coverage levels among children
aged 1935 months: United States, 2000. MMWR Morb Mortal Wkly Rep
2001; 50: 637-41
19. Dombkowski KJ, Lantz PM, Freed GL. The need for surveillance of delay in ageappropriate immunization. Am J Prev Med 2002; 23: 36-42
Guerra
37. Hinman AR, Orenstein WA, Williamson DE, et al. Childhood immunization: laws
that work. J Law Med Ethics 2002; 30 (3 Suppl.): 122-7
38. Feikin DR, Lezotte DC, Hamman RF, et al. Individual and community risks of
measles and pertussis associated with personal exemptions to immunization.
JAMA 2000; 284: 3145-50
20. Grant CC, Roberts M, Scragg R, et al. Delayed immunisation and risk of pertussis
in infants: unmatched case-control study. BMJ 2003; 326: 852-3
39. Global Polio Eradication Initiative [online]. Available from URL: http://
21. Izurieta HS, Kenyon TA, Strebel PM, et al. Risk factors for pertussis in young
infants during an outbreak in Chicago in 1993. Clin Infect Dis 1996; 22: 503-7
40. Aberle JH, Aberle SW, Pracher E, et al. Single versus dual respiratory virus
22. Wood DL, Brunell PA. Measles control in the United States: problems of the past
and challenges for the future. Clin Microbiol Rev 1995; 8: 260-7
23. CDC. Preventable measles among U.S. residents, 20012004. MMWR 2005; 54:
817-20
24. Salmon DA, Haber M, Gangarosa EJ, et al. Health consequences of religious and
philosophical exemptions from immunization laws. JAMA 1999; 282: 47-53
25. Marshall GS, Happe LE. Impact of first-year DTaP doses on the timeliness of the
fourth dose of DTaP among children in a state Medicaid population [poster no.
269]. 40th National Immunization Conference; 2006 Mar 69; Atlanta (GA)
www.polioeradication.org/casecount.asp [Accessed 2007 Feb 16]
infections in hospitalized infants: impact on clinical course of disease and
interferon-gamma response. Pediatr Infect Dis J 2005; 24: 605-10
41. Meyeroff A, Jacobs RJ, Greenberg DP, et al. Clinician satisfaction with vaccination visits and the role of multiple injections, results from the COVISE study.
Clin Pediatr 2004; 43: 87-93
42. Committee on Community Health Services and Committee on Practice and Ambulatory Medicine. Increasing immunization coverage. Pediatrics 2003; 112:
993-6
26. Irigoyen M, Findley SE, Chen S, et al. Early continuity of care and immunization
coverage. Ambul Pediatr 2004; 4: 199-203
43. Randolph GD, Murray M, Swanson JA, et al. Behind schedule: improving access to
27. Heath PT, McVernon J. The UK Hib vaccine experience. Arch Dis Child 2002; 86:
393-9
44. OBrien L, Taddio A, Ipp M, et al. Topical 4% amethocaine gel reduces the pain of
28. Lieu TA, Black SB, Sorel ME, et al. Would better adherence to guidelines improve
childhood immunization rates? Pediatrics 1996; 98: 1062-8
29. Bardenheier BH, Yusuf HR, Rosenthal J, et al. Factors associated with underimmunization at 3 months of age in four medically underserved areas. Public
Health Rep 2004; 119: 479-85
care for children one practice at a time. Pediatrics 2004; 113: 230-7
subcutaneous measles-mumps-rubella vaccination. Pediatrics 2004; 114:
e720-4
45. Cohen LL, Blount RL, Cohen RJ, et al. Comparative study of distraction versus
topical anesthesia for pediatric pain management during immunizations. Health
Psychol 1999; 18: 591-8
30. Daniels D, Jiles RB, Klevens RM, et al. Undervaccinated African-American
preschoolers: a case of missed opportunities. Am J Prev Med 2001; 20 (4
Suppl.): 61-8
46. Koslap-Petraco MB, Parsons T. Communicating the benefits of combination
31. John TJ, Samuel R. Herd immunity and herd effect: new insights and definitions.
Eur J Epidemiol 2000; 16: 601-6
47. Gust DA, Strine TW, Maurice E, et al. Underimmunization among children: effects
32. Davis RM, Whitman EE, Orenstein WA, et al. A persistent outbreak of measles
despite appropriate prevention and control measures. Am J Epidemiol 1987;
126: 438-49
vaccines to parents and health care providers. J Pediatr Health Care 2003; 17:
53-7
of vaccine safety concerns on immunization status. Pediatrics 2004; 114: 16-22
48. Gregson AL, Edelman R. Does antigenic overload exist? The role of multiple
immunizations in infants. Immunol Allergy Clin North Am 2003; 23: 649-64
33. Gustafson TL, Lievens AW, Brunell PA, et al. Measles outbreak in a fully
immunized secondary-school population. N Engl J Med 1987; 316: 771-4
49. Gangarosa EJ, Galazka AM, Wolfe CR, et al. Impact of anti-vaccine movements on
34. Kuter BJ, Weibel RE, Guess HA. Oka/Merck varicella vaccine in healthy children:
final report of a 2-year efficacy study and 7-year follow-up studies. Vaccine
1991; 9: 643-7
50. CDC. ACIP VFC vaccine resolutions [online]. Available from URL: http://
35. Weibel RE, Neff BJ, Kuter BJ. Live attenuated varicella vaccine: efficacy trial in
healthy children. N Engl J Med 1984; 310: 1409-15
36. Omer SB, Pan WK, Halsey NA, et al. Nonmedical exemptions to school immunization requirements: secular trends and association of state policies with pertussis
incidence. JAMA 2006; 296: 1757-63
2007 Adis Data Information BV. All rights reserved.
pertussis control: the untold story. Lancet 1998; 351: 356-61
www.cdc.gov/nip/vfc/acip_vfc_resolutions.htm. [Accessed 2006 Mar 6]
Correspondence: Prof. Fernando A. Guerra, 332 West Commerce, Suite 307,
San Antonio, TX 782052489, USA.
E-mail: fernando.guerra@sanantonio.gov
Pediatr Drugs 2007; 9 (3)
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Strategic Management Questions Chapter 1Document12 pagesStrategic Management Questions Chapter 1Yasmine Abdelbary100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Ordinary Medicine by Sharon R. KaufmanDocument33 pagesOrdinary Medicine by Sharon R. KaufmanDuke University Press100% (1)
- EPI Program Principles Immunization DiseasesDocument4 pagesEPI Program Principles Immunization DiseasesSarahLabadan67% (3)
- Nurses Code of EthicsDocument14 pagesNurses Code of EthicsJhon Mhark GarinNo ratings yet
- Expanded Program On ImmunizationDocument12 pagesExpanded Program On ImmunizationMaria Linda Sibayan-AgusNo ratings yet
- RusDocument42 pagesRusОльга КалмыковаNo ratings yet
- World Health Organization: Cannabis Rescheduling RecommendationsDocument3 pagesWorld Health Organization: Cannabis Rescheduling RecommendationsBen Adlin100% (1)
- History of BFADDocument14 pagesHistory of BFADIsobelNo ratings yet
- Nbns1104 Transculture in NursingDocument8 pagesNbns1104 Transculture in Nursingdicky chongNo ratings yet
- Concepts in Dental Public Health CH 1Document23 pagesConcepts in Dental Public Health CH 1Maria Mercedes LeivaNo ratings yet
- Bu Costy Prosedur Pembersihan Dan Penyimpanan Alat EndosDocument19 pagesBu Costy Prosedur Pembersihan Dan Penyimpanan Alat Endosuling jhonNo ratings yet
- Hsra Monograph No. 9 FinalDocument51 pagesHsra Monograph No. 9 FinalJeffry AcabaNo ratings yet
- Document 5Document25 pagesDocument 5Rhodius NogueraNo ratings yet
- Malaysian health laws and regulations from 1951-2016Document1 pageMalaysian health laws and regulations from 1951-2016keuromokNo ratings yet
- OH InitiativeDocument16 pagesOH InitiativePASCALNo ratings yet
- The Expanded Program On Immunizations of The PhilippinesDocument8 pagesThe Expanded Program On Immunizations of The PhilippinesFritz MirandaNo ratings yet
- Rational Drug Use for Ear, Nose and Throat InfectionDocument18 pagesRational Drug Use for Ear, Nose and Throat InfectionhanumNo ratings yet
- The Role of Research in The Right To Health and The Universal Provision of Health CareDocument5 pagesThe Role of Research in The Right To Health and The Universal Provision of Health CareClaudio Gruber MannNo ratings yet
- Preliminary Requirement For ANDA Filing: International Journal of Drug Regulatory AffairsDocument8 pagesPreliminary Requirement For ANDA Filing: International Journal of Drug Regulatory AffairsEsha JainNo ratings yet
- IMP SREQ RequirementsDocument2 pagesIMP SREQ RequirementsAlexandreau del FierroNo ratings yet
- Dfps Purchased Client Services Contractor InformationDocument6 pagesDfps Purchased Client Services Contractor Informationapi-248787285No ratings yet
- Hubungan Karakteristik Ibu Inpartu Terhadap Kejadian Perdarahan Postpartum Di Rsu Budi Kemuliaan Periode Tahun 2019Document10 pagesHubungan Karakteristik Ibu Inpartu Terhadap Kejadian Perdarahan Postpartum Di Rsu Budi Kemuliaan Periode Tahun 2019MiMa Muach LadyzNo ratings yet
- Emergency Use Authorization: Overview and Considerations For COVID-19 VaccinesDocument17 pagesEmergency Use Authorization: Overview and Considerations For COVID-19 VaccinesKen O'ConnorNo ratings yet
- Understanding Policy, Politics and Decision-MakingDocument48 pagesUnderstanding Policy, Politics and Decision-MakingElemia Lou IsraelNo ratings yet
- Chapter 1 - Orientation To PharmacologyDocument4 pagesChapter 1 - Orientation To Pharmacologydlneisha61No ratings yet
- Unang YakapDocument7 pagesUnang YakapApol AstigNo ratings yet
- Faktor Resiko Penyebab Multidrug Resistant Tuberkulosis: Sistematik ReviewDocument8 pagesFaktor Resiko Penyebab Multidrug Resistant Tuberkulosis: Sistematik ReviewAbduNo ratings yet
- Joint Commission EssayDocument4 pagesJoint Commission Essayapi-340699040100% (1)
- Midwives by The LakeDocument2 pagesMidwives by The LakeMelanie WestonNo ratings yet
- Accountable Care Organizations 3Document80 pagesAccountable Care Organizations 3netgear9No ratings yet