You might also like
- Politics V Science Understanding Cannabis Therapeutics Before It Gets CensoredDocument3 pagesPolitics V Science Understanding Cannabis Therapeutics Before It Gets Censoredjamie_clark_2No ratings yet
- Tax and Regulate BrochureDocument2 pagesTax and Regulate BrochureMPPNo ratings yet
- Model Tax and Regulate Bill SummaryDocument2 pagesModel Tax and Regulate Bill SummaryMPPNo ratings yet
- Regulation WorksDocument1 pageRegulation WorksMPPNo ratings yet
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDocument1 pageSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNo ratings yet
- Oklahoma's Low-THC LawDocument1 pageOklahoma's Low-THC LawMPPNo ratings yet
- Belize Decriminalizes Marijuana PossessionDocument5 pagesBelize Decriminalizes Marijuana PossessionMichelle WebsterNo ratings yet
- Medical Marijuana Patient CasualtiesDocument2 pagesMedical Marijuana Patient CasualtiesMPP100% (3)
- State Decrim ChartDocument4 pagesState Decrim ChartMPPNo ratings yet
- Federal Enforcement Policy On State Marijuana LawsDocument2 pagesFederal Enforcement Policy On State Marijuana LawsMPP100% (1)
- Marijuana and Medicine: Assessing The Science BaseDocument4 pagesMarijuana and Medicine: Assessing The Science BaseMPPNo ratings yet
- Cannabis Research LetterDocument2 pagesCannabis Research LetterMarijuana MomentNo ratings yet
- Progress Report New York Medical Marijuana ProgramDocument2 pagesProgress Report New York Medical Marijuana ProgramMPPNo ratings yet
- State-by-State Provisions For Adding Qualifying ConditionsDocument5 pagesState-by-State Provisions For Adding Qualifying ConditionsMPPNo ratings yet
- The Economic Implications of Marijuana Legalization in AlaskaDocument46 pagesThe Economic Implications of Marijuana Legalization in AlaskaMPPNo ratings yet
- Overview of Maryland's Medical Marijuana LawDocument3 pagesOverview of Maryland's Medical Marijuana LawMPP100% (1)
- Iowa's Low-THC Law SummaryDocument1 pageIowa's Low-THC Law SummaryMPPNo ratings yet
- Revenue From Adult Use StatesDocument5 pagesRevenue From Adult Use StatesMPPNo ratings yet
- Breakdown of Fees in Adult-Use StatesDocument6 pagesBreakdown of Fees in Adult-Use StatesMPPNo ratings yet
- Marijuana Prohibition FactsDocument5 pagesMarijuana Prohibition FactsMPPNo ratings yet
- Michigan's Medical Marihuana ActDocument27 pagesMichigan's Medical Marihuana Actapi-25946258No ratings yet
- Regulatory Authorities and Medical CannabisDocument3 pagesRegulatory Authorities and Medical CannabisMPPNo ratings yet
- Severe Pain and Medical CannabisDocument1 pageSevere Pain and Medical CannabisMPPNo ratings yet
- SS Usa 04-11Document48 pagesSS Usa 04-11steveurkleNo ratings yet
- Cannabis in The ClinicDocument3 pagesCannabis in The ClinicVianne ArcenioNo ratings yet
- Marijuana - Marijuana As MedicineDocument1 pageMarijuana - Marijuana As MedicinelearnaboutsamNo ratings yet
- Conservative Thinkers and Marijuana Policy ReformDocument2 pagesConservative Thinkers and Marijuana Policy ReformMPP100% (1)
- Cannabis Use and Substantial Reduction in Premature Deaths in The United States.Document53 pagesCannabis Use and Substantial Reduction in Premature Deaths in The United States.Monterey Bud100% (2)
- Model State Adult-Use Legalization and Regulation BillDocument22 pagesModel State Adult-Use Legalization and Regulation BillMPPNo ratings yet
- State Medical Marijuana Program Implementation TimelineDocument1 pageState Medical Marijuana Program Implementation TimelineMPPNo ratings yet
- Statement of PrincipleDocument2 pagesStatement of PrincipleMPP100% (2)
- 2018 Model LegislationDocument18 pages2018 Model LegislationPaul MariniNo ratings yet
- Gateway Theory DebunkedDocument2 pagesGateway Theory DebunkedMPPNo ratings yet
- Illinois Pilot Program Act RoadmapDocument19 pagesIllinois Pilot Program Act RoadmapMPPNo ratings yet
- Cannabis Use Disorder Identification TestDocument1 pageCannabis Use Disorder Identification TestMichael_Lee_RobertsNo ratings yet
- Colorado and Washington: Life After Legalization and RegulationDocument2 pagesColorado and Washington: Life After Legalization and RegulationMPP100% (3)
- Rethinking War On DrugsDocument175 pagesRethinking War On DrugsitsanelleNo ratings yet
- Medical Marijuana Laws and Anti-Discrimination ProvisionsDocument12 pagesMedical Marijuana Laws and Anti-Discrimination ProvisionsMPPNo ratings yet
- Legalization of Cannabis Report Analyzes Ethics and ImpactsDocument25 pagesLegalization of Cannabis Report Analyzes Ethics and ImpactsAvital chaerNo ratings yet
- Brett Painter Tech Writing SlideshowDocument17 pagesBrett Painter Tech Writing SlideshowBrett PainterNo ratings yet
- The History of Cannabis Regulation in Shasta County 10.11.14Document7 pagesThe History of Cannabis Regulation in Shasta County 10.11.14MatthewMeyerNo ratings yet
- A Snapshot of Demand For Adult-Use Cannabis in IllinoisDocument27 pagesA Snapshot of Demand For Adult-Use Cannabis in IllinoisTodd FeurerNo ratings yet
- Regulating Cannabis in NunavutDocument10 pagesRegulating Cannabis in NunavutNunatsiaqNewsNo ratings yet
- Top Ten Reasons To End Marijuana ProhibitionDocument1 pageTop Ten Reasons To End Marijuana ProhibitionMPP100% (1)
- Exposing The 'Reefer Madness' of The Parliament of Canada 11of10 ConclusionsDocument14 pagesExposing The 'Reefer Madness' of The Parliament of Canada 11of10 ConclusionsSam VekemansNo ratings yet
- Medical Marijuana OverviewDocument2 pagesMedical Marijuana OverviewMPP0% (1)
- Thesis PresentationDocument17 pagesThesis PresentationBert EnajeNo ratings yet
- 7 31 2014 - CannabisFinalReport PDFDocument23 pages7 31 2014 - CannabisFinalReport PDFlighthouseventureNo ratings yet
- Prescribing Versus Recommending Medical CannabisDocument2 pagesPrescribing Versus Recommending Medical CannabisMPPNo ratings yet
- Argument Essay FinaleDocument4 pagesArgument Essay Finaleapi-458895222No ratings yet
- Economics of Cannabis LegalizationDocument12 pagesEconomics of Cannabis LegalizationMPPNo ratings yet
- Chardan Capital On Cannabis MarketDocument8 pagesChardan Capital On Cannabis MarketotteromNo ratings yet
- PRIMING OF SEEDS WITH DIFFERENT SEAWEED EXTRACTS TO MITIGATE SALINITY STRESS IN PADDY Var. ANNA 4.Document1 pagePRIMING OF SEEDS WITH DIFFERENT SEAWEED EXTRACTS TO MITIGATE SALINITY STRESS IN PADDY Var. ANNA 4.ambikasingaramNo ratings yet
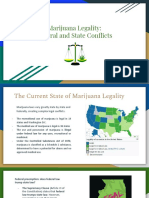
- Marijuana Legality PresentationDocument11 pagesMarijuana Legality PresentationRik E Horoky100% (1)
- Synthetic Cannabinoid Fact Sheet PDFDocument4 pagesSynthetic Cannabinoid Fact Sheet PDFwebmaster@drugpolicy.orgNo ratings yet
- Model State Medical Cannabis BillDocument26 pagesModel State Medical Cannabis BillMPPNo ratings yet
- Med Cannabis Stock SecurityDocument12 pagesMed Cannabis Stock SecurityTrelospapasse BaftisedenyparxeisNo ratings yet
- Texas' Low-THC Medical Cannabis ProgramDocument2 pagesTexas' Low-THC Medical Cannabis ProgramMPPNo ratings yet
- Medical Marijuana Laws and Public SafetyDocument3 pagesMedical Marijuana Laws and Public SafetyMPPNo ratings yet
- Petition Urging Governors To Protect Medical Cannabis AccessDocument70 pagesPetition Urging Governors To Protect Medical Cannabis AccessMPPNo ratings yet
- 2020 Vermont Poll ResultsDocument7 pages2020 Vermont Poll ResultsMPPNo ratings yet
- GQR Connecticut Poll January 2020Document1 pageGQR Connecticut Poll January 2020MPPNo ratings yet
- Severe Pain and Medical CannabisDocument1 pageSevere Pain and Medical CannabisMPPNo ratings yet
- Prescribing Versus Recommending Medical CannabisDocument2 pagesPrescribing Versus Recommending Medical CannabisMPPNo ratings yet
- MPP Policy Paper - Regulating Cannabis Oil VaporizersDocument7 pagesMPP Policy Paper - Regulating Cannabis Oil VaporizersMPPNo ratings yet
- Marijuana Policy Progress Report 2019 Legislative UpdateDocument28 pagesMarijuana Policy Progress Report 2019 Legislative UpdateMPP100% (3)
- Medical Cannabis Implementation TimelinesDocument10 pagesMedical Cannabis Implementation TimelinesMPPNo ratings yet
- Medical Cannabis Provides An Alternative To OpiatesDocument1 pageMedical Cannabis Provides An Alternative To OpiatesMPPNo ratings yet
- Decriminalization and Expungement in NY: An Overview of A0840 / S06579Document1 pageDecriminalization and Expungement in NY: An Overview of A0840 / S06579MPPNo ratings yet
- Simon Poll March 2019Document14 pagesSimon Poll March 2019MPPNo ratings yet
- Marijuana Policy Map May 2020Document1 pageMarijuana Policy Map May 2020MPPNo ratings yet
- Progress Report New York Medical Marijuana ProgramDocument2 pagesProgress Report New York Medical Marijuana ProgramMPPNo ratings yet
- 2018 SIU Paul Simon Public Policy Institute Legalization PollDocument4 pages2018 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- Medical Marijuana MapDocument1 pageMedical Marijuana MapMPPNo ratings yet
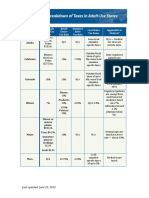
- Breakdown of Taxes in Adult-Use StatesDocument2 pagesBreakdown of Taxes in Adult-Use StatesMPPNo ratings yet
- 2017 SIU Paul Simon Public Policy Institute Legalization PollDocument7 pages2017 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- Potential Revenue From Regulating Marijuana in ConnecticutDocument2 pagesPotential Revenue From Regulating Marijuana in ConnecticutMPPNo ratings yet
- Expungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionDocument1 pageExpungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionMPPNo ratings yet
- What Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?Document2 pagesWhat Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?MPPNo ratings yet
- New Jersey Progress ReportDocument2 pagesNew Jersey Progress ReportMPPNo ratings yet
- U.S. Attorneys' Comments Post Cole Memo RecissionDocument8 pagesU.S. Attorneys' Comments Post Cole Memo RecissionMPPNo ratings yet
- Maryland Progress ReportDocument2 pagesMaryland Progress ReportMPPNo ratings yet
- Breakdown of Fees in Adult-Use StatesDocument6 pagesBreakdown of Fees in Adult-Use StatesMPPNo ratings yet
- D.C.'s Medical Marijuana ProgramDocument2 pagesD.C.'s Medical Marijuana ProgramMPPNo ratings yet
- Sessions Asks Congress To Undo Medical Marijuana ProtectionsDocument3 pagesSessions Asks Congress To Undo Medical Marijuana ProtectionsMPPNo ratings yet
- Medical Marijuana by The NumbersDocument2 pagesMedical Marijuana by The NumbersMPPNo ratings yet
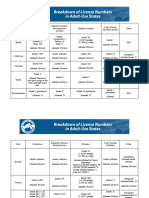
- Breakdown of License Numbers in Adult-Use StatesDocument2 pagesBreakdown of License Numbers in Adult-Use StatesMPPNo ratings yet
- Revenue From Adult Use StatesDocument5 pagesRevenue From Adult Use StatesMPPNo ratings yet
- Pub - New Directions in Progressive Relaxation TrainingDocument176 pagesPub - New Directions in Progressive Relaxation TrainingRafael Bagus100% (1)
- Star T: Flowchart "Physical Fitness Test"Document1 pageStar T: Flowchart "Physical Fitness Test"Eller-Jed Manalac MendozaNo ratings yet
- Elements (Industrial Plant)Document5 pagesElements (Industrial Plant)Veralyn Mae BondadNo ratings yet
- Blessed Are Those Who MournDocument7 pagesBlessed Are Those Who MournPatrick MabbaguNo ratings yet
- Establishment of Retirement PlanDocument3 pagesEstablishment of Retirement PlanVioleta StancuNo ratings yet
- Reliance Tabletop SonicDocument20 pagesReliance Tabletop SonicbrisaNo ratings yet
- Communicating Across AgesDocument35 pagesCommunicating Across AgesConrad TarihoranNo ratings yet
- EXERCISE 1.1.2: Daub, Elycka Dela Cruz, Jesson Igne, Cyril Joy Labbao, Trinity RZL110 - A56Document7 pagesEXERCISE 1.1.2: Daub, Elycka Dela Cruz, Jesson Igne, Cyril Joy Labbao, Trinity RZL110 - A56-No ratings yet
- 08-05-2021 JR - Super60 ActP (In Coming) Jee-Main WTM-01 Question PaperDocument14 pages08-05-2021 JR - Super60 ActP (In Coming) Jee-Main WTM-01 Question Paperpurandar puneetNo ratings yet
- Cognitive and Psychopathological Aspects of Ehlers DanlosDocument5 pagesCognitive and Psychopathological Aspects of Ehlers DanlosKarel GuevaraNo ratings yet
- RRL CapstoneDocument3 pagesRRL CapstoneMatthew Dane SitoNo ratings yet
- Guidance On The 2010 ADA Standards For Accessible Design Volume 2Document93 pagesGuidance On The 2010 ADA Standards For Accessible Design Volume 2Eproy 3DNo ratings yet
- Exp. 5 Test For Fats and ProteinsDocument6 pagesExp. 5 Test For Fats and ProteinsEMELIE GRACE E CACHERONo ratings yet
- Sara Salon and SpaDocument4 pagesSara Salon and Spasania zehraNo ratings yet
- Typhoid FeverDocument9 pagesTyphoid FeverAli Al.JuffairiNo ratings yet
- A Lesson Design in HELE 6 Chapter 2Document6 pagesA Lesson Design in HELE 6 Chapter 2Jestoni Paragsa100% (5)
- A7V Variable Displacement PumpDocument22 pagesA7V Variable Displacement PumpEduardo CramerNo ratings yet
- Jobaid Investigating Causes PDFDocument16 pagesJobaid Investigating Causes PDFNina MarianaNo ratings yet
- Commercial Inverter AC Service ManualDocument116 pagesCommercial Inverter AC Service ManualEdwin JaramilloNo ratings yet
- EDC MS 6.4 System DescriptionDocument10 pagesEDC MS 6.4 System Descriptionmarsh2002No ratings yet
- Understanding Steam Turbine VibrationDocument30 pagesUnderstanding Steam Turbine VibrationkatibraNo ratings yet
- Norris Claire White Paper Liftware PDFDocument14 pagesNorris Claire White Paper Liftware PDFmeysam NaaNo ratings yet
- The Positive and Negative Syndrome Scale PANSS ForDocument5 pagesThe Positive and Negative Syndrome Scale PANSS ForditeABCNo ratings yet
- Govt Schemes - 1 MWCD MOSJEDocument36 pagesGovt Schemes - 1 MWCD MOSJEshaheen razaNo ratings yet
- Periodic Table of Personality ElementsDocument1 pagePeriodic Table of Personality Elementslilian_vera_1No ratings yet
- HVAC Report FINALDocument65 pagesHVAC Report FINALIanNo ratings yet
- Final Draft - Banana ChipsDocument34 pagesFinal Draft - Banana ChipsAubrey Delgado74% (35)
- 02-Plant Morphology (Exercise)Document5 pages02-Plant Morphology (Exercise)varshavishuNo ratings yet
- (UNISIM (BEHAS) - Introduction To Aerospace) EAS105 - Lab4Document33 pages(UNISIM (BEHAS) - Introduction To Aerospace) EAS105 - Lab4Mohd Ashraf Mohd IsmailNo ratings yet
- DC72D MK2 Genset Controller User Manual V1.5Document61 pagesDC72D MK2 Genset Controller User Manual V1.5Cristobal AvecillaNo ratings yet