You might also like
- Marijuana Legalization (Copypasta Pastiche)Document4 pagesMarijuana Legalization (Copypasta Pastiche)LeEminenceGriseNo ratings yet
- Medical Marijuana PowerpointDocument71 pagesMedical Marijuana PowerpointPagulayan Natividad Aljan100% (1)
- Why Marijuana Should Be LegalDocument62 pagesWhy Marijuana Should Be LegalRenato Ferraz100% (40)
- Position Paper On Marijuana As MedicineDocument4 pagesPosition Paper On Marijuana As Medicinenetmail2307100% (1)
- Final Research Paper - Marijuana LegalizationDocument10 pagesFinal Research Paper - Marijuana LegalizationSaberUmbra92% (13)
- Legalization of Medical Marijuana in The PhilippinesDocument114 pagesLegalization of Medical Marijuana in The PhilippinesJed Daet71% (38)
- Colorado: The Economy After Legalization and RegulationDocument2 pagesColorado: The Economy After Legalization and RegulationMPPNo ratings yet
- Cannabis Legalization EssayDocument3 pagesCannabis Legalization Essayriley1987No ratings yet
- Medical MarijuanaDocument5 pagesMedical Marijuanaapi-322399513No ratings yet
- Marijuana Research PaperDocument11 pagesMarijuana Research PaperJack DohertyNo ratings yet
- Argument Essay FinaleDocument4 pagesArgument Essay Finaleapi-458895222No ratings yet
- Marijuana Research PaperDocument12 pagesMarijuana Research PaperTianna100% (1)
- Why Marijuana Should Not Be LegalizedDocument7 pagesWhy Marijuana Should Not Be LegalizedomondistepNo ratings yet
- Medical Marijuana Protections in The 50 StatesDocument14 pagesMedical Marijuana Protections in The 50 StatesMPPNo ratings yet
- Compilation of Notes If Marijuana Will Be Legalized in The PhilippinesDocument42 pagesCompilation of Notes If Marijuana Will Be Legalized in The PhilippinesLajilaNo ratings yet
- Marijuana LegalizationDocument5 pagesMarijuana LegalizationMatt ImpellusoNo ratings yet
- Argumentative Essay Medical MarijuanaDocument7 pagesArgumentative Essay Medical MarijuanaMaxim Dahan100% (1)
- Medicinal Cannabis BriefingDocument32 pagesMedicinal Cannabis BriefingMiguelSantaellaSerranoNo ratings yet
- Research Methodology: Decriminalizing CannabisDocument6 pagesResearch Methodology: Decriminalizing CannabisShaneil Bryt N Myrie0% (2)
- The Legalization of MarijuanaDocument2 pagesThe Legalization of MarijuanaDanny100% (1)
- MarijuanaDocument8 pagesMarijuanajohnkyleNo ratings yet
- Severe Pain and Medical CannabisDocument1 pageSevere Pain and Medical CannabisMPPNo ratings yet
- Informative Speech Outline - WeedDocument4 pagesInformative Speech Outline - Weedapi-302374942100% (12)
- Medical Marijuana Legalization ImpactDocument55 pagesMedical Marijuana Legalization ImpactSusana G. Bencio100% (2)
- The Impact of Medicinal Recreational Marijuana Legalization On Adolescent Use, Consequences, and Perceived RiskDocument52 pagesThe Impact of Medicinal Recreational Marijuana Legalization On Adolescent Use, Consequences, and Perceived RiskAyena GraceNo ratings yet
- An Argumentative Essay On The Use of Marijuana in MedicineDocument6 pagesAn Argumentative Essay On The Use of Marijuana in MedicineSeth Andrew Salih100% (11)
- Cannabis in The ClinicDocument3 pagesCannabis in The ClinicVianne ArcenioNo ratings yet
- Marijuanaandlaw FinalDocument11 pagesMarijuanaandlaw Finalapi-283892872No ratings yet
- (FINAL) Legalization of Medical Marijuana Affirmative SpeechDocument5 pages(FINAL) Legalization of Medical Marijuana Affirmative SpeechKaye SantosNo ratings yet
- Top 10 Pros and Cons - Medical Marijuana - ProConDocument5 pagesTop 10 Pros and Cons - Medical Marijuana - ProConNews-Press100% (1)
- 11th Grade Persuausive Essay ExampleDocument2 pages11th Grade Persuausive Essay ExampleLindsay LigonesNo ratings yet
- What Is Medical Marijuana?Document11 pagesWhat Is Medical Marijuana?ZAARA ADAMSNo ratings yet
- Medical Marijuana Is Not Regulated As Most Medicines AreDocument3 pagesMedical Marijuana Is Not Regulated As Most Medicines AreElmy GarciaNo ratings yet
- Why Medical Marijuana Should Be LegalizedDocument5 pagesWhy Medical Marijuana Should Be LegalizedMarkNo ratings yet
- Guide To Cannabis For Chronic Pain Patients in EuropeDocument28 pagesGuide To Cannabis For Chronic Pain Patients in EuropeMilosNo ratings yet
- Marijuana and Medicine: Assessing The Science BaseDocument4 pagesMarijuana and Medicine: Assessing The Science BaseMPPNo ratings yet
- Revised Should Marijuana Be Legalized in The USDocument24 pagesRevised Should Marijuana Be Legalized in The USBailey DeitchNo ratings yet
- Final Paper WordDocument8 pagesFinal Paper Wordapi-357159376No ratings yet
- Legalization of Medical Marijuana in the USDocument12 pagesLegalization of Medical Marijuana in the USTeresa SmithNo ratings yet
- Should Marijuana Be Legal For Medicinal PurposesDocument2 pagesShould Marijuana Be Legal For Medicinal PurposesMOHD FITRI SAIMINo ratings yet
- Medical Marijuana: Benefits, Risks & State Laws: Understanding Marijuana: A New Look at The Scientific EvidenceDocument7 pagesMedical Marijuana: Benefits, Risks & State Laws: Understanding Marijuana: A New Look at The Scientific EvidenceLynette CantosNo ratings yet
- House OKs Medical Marijuana BillDocument3 pagesHouse OKs Medical Marijuana BillJennifer Garcia EreseNo ratings yet
- DPA - Fact Sheet - Medical - Marijuana - Jan2015 PDFDocument3 pagesDPA - Fact Sheet - Medical - Marijuana - Jan2015 PDFwebmaster@drugpolicy.orgNo ratings yet
- MMJ-BriefingPaper 0210Document4 pagesMMJ-BriefingPaper 0210toddler1100% (1)
- Is Marijuana Good or BadDocument2 pagesIs Marijuana Good or BadDana MocanuNo ratings yet
- Pain BrochureDocument24 pagesPain Brochurelordhavok33No ratings yet
- Keywords: Ailments, Availability and Legality, Aware, Epilepsy, High, KnowledgeableDocument18 pagesKeywords: Ailments, Availability and Legality, Aware, Epilepsy, High, KnowledgeablePatrick DgNo ratings yet
- Rhetorical Analysis Final DraftDocument5 pagesRhetorical Analysis Final Draftapi-643343018No ratings yet
- NY Physicians For Comp Care - Letter About Smoking - 06 05 2014Document3 pagesNY Physicians For Comp Care - Letter About Smoking - 06 05 2014samueloakford100% (1)
- Medical Marijuana as an Alternative to Prescription MedicationsDocument10 pagesMedical Marijuana as an Alternative to Prescription MedicationsMarcellaNo ratings yet
- The Benefits of Medical Marijuana For Cancer PatientsDocument4 pagesThe Benefits of Medical Marijuana For Cancer PatientsSheryl DiazNo ratings yet
- Cannabis DocumentationDocument20 pagesCannabis DocumentationRicardo CampuzanoNo ratings yet
- 5 Diseases Proven To Respond Better To Cannabis Than Prescription DrugsDocument12 pages5 Diseases Proven To Respond Better To Cannabis Than Prescription DrugsJames BondNo ratings yet
- Medical Marijuana OverviewDocument2 pagesMedical Marijuana OverviewMPP0% (1)
- Complementary Therapies in Medicine: Yuval Zolotov, Lia Eshet, Ofir MoragDocument5 pagesComplementary Therapies in Medicine: Yuval Zolotov, Lia Eshet, Ofir MoragRafael MouraNo ratings yet
- Research Paper 1Document6 pagesResearch Paper 1api-406728189No ratings yet
- Legalization Medical Marijuana Annotated Bibliography FINALDocument9 pagesLegalization Medical Marijuana Annotated Bibliography FINALRyan BloomNo ratings yet
- Medical Marijuana Research Paper ConclusionDocument6 pagesMedical Marijuana Research Paper Conclusionh02ver8h100% (1)
- Dr. A. Hazekamp Self-Medication With CannabisDocument39 pagesDr. A. Hazekamp Self-Medication With CannabisEl'Nelu Weed100% (2)
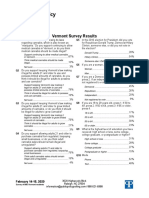
- 2020 Vermont Poll ResultsDocument7 pages2020 Vermont Poll ResultsMPPNo ratings yet
- Simon Poll March 2019Document14 pagesSimon Poll March 2019MPPNo ratings yet
- Petition Urging Governors To Protect Medical Cannabis AccessDocument70 pagesPetition Urging Governors To Protect Medical Cannabis AccessMPPNo ratings yet
- GQR Connecticut Poll January 2020Document1 pageGQR Connecticut Poll January 2020MPPNo ratings yet
- Medical Cannabis Provides An Alternative To OpiatesDocument1 pageMedical Cannabis Provides An Alternative To OpiatesMPPNo ratings yet
- Marijuana Policy Map May 2020Document1 pageMarijuana Policy Map May 2020MPPNo ratings yet
- Decriminalization and Expungement in NY: An Overview of A0840 / S06579Document1 pageDecriminalization and Expungement in NY: An Overview of A0840 / S06579MPPNo ratings yet
- Medical Cannabis Implementation TimelinesDocument10 pagesMedical Cannabis Implementation TimelinesMPPNo ratings yet
- MPP Policy Paper - Regulating Cannabis Oil VaporizersDocument7 pagesMPP Policy Paper - Regulating Cannabis Oil VaporizersMPPNo ratings yet
- Prescribing Versus Recommending Medical CannabisDocument2 pagesPrescribing Versus Recommending Medical CannabisMPPNo ratings yet
- Marijuana Policy Progress Report 2019 Legislative UpdateDocument28 pagesMarijuana Policy Progress Report 2019 Legislative UpdateMPP100% (3)
- Severe Pain and Medical CannabisDocument1 pageSevere Pain and Medical CannabisMPPNo ratings yet
- Maryland Progress ReportDocument2 pagesMaryland Progress ReportMPPNo ratings yet
- 2017 SIU Paul Simon Public Policy Institute Legalization PollDocument7 pages2017 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- 2018 SIU Paul Simon Public Policy Institute Legalization PollDocument4 pages2018 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- Progress Report New York Medical Marijuana ProgramDocument2 pagesProgress Report New York Medical Marijuana ProgramMPPNo ratings yet
- Medical Marijuana MapDocument1 pageMedical Marijuana MapMPPNo ratings yet
- What Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?Document2 pagesWhat Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?MPPNo ratings yet
- Potential Revenue From Regulating Marijuana in ConnecticutDocument2 pagesPotential Revenue From Regulating Marijuana in ConnecticutMPPNo ratings yet
- U.S. Attorneys' Comments Post Cole Memo RecissionDocument8 pagesU.S. Attorneys' Comments Post Cole Memo RecissionMPPNo ratings yet
- New Jersey Progress ReportDocument2 pagesNew Jersey Progress ReportMPPNo ratings yet
- D.C.'s Medical Marijuana ProgramDocument2 pagesD.C.'s Medical Marijuana ProgramMPPNo ratings yet
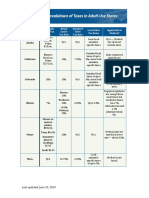
- Breakdown of Taxes in Adult-Use StatesDocument2 pagesBreakdown of Taxes in Adult-Use StatesMPPNo ratings yet
- Expungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionDocument1 pageExpungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionMPPNo ratings yet
- Medical Marijuana by The NumbersDocument2 pagesMedical Marijuana by The NumbersMPPNo ratings yet
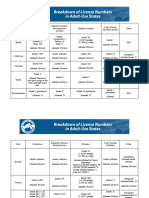
- Breakdown of License Numbers in Adult-Use StatesDocument2 pagesBreakdown of License Numbers in Adult-Use StatesMPPNo ratings yet
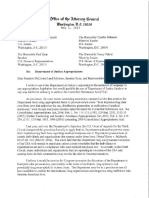
- Sessions Asks Congress To Undo Medical Marijuana ProtectionsDocument3 pagesSessions Asks Congress To Undo Medical Marijuana ProtectionsMPPNo ratings yet
- Breakdown of Fees in Adult-Use StatesDocument6 pagesBreakdown of Fees in Adult-Use StatesMPPNo ratings yet
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDocument1 pageSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNo ratings yet
- Revenue From Adult Use StatesDocument5 pagesRevenue From Adult Use StatesMPPNo ratings yet
- Online shopping behavior studyDocument7 pagesOnline shopping behavior studyNarender SinghNo ratings yet
- Ray Shu vs. Jaime DeeDocument3 pagesRay Shu vs. Jaime DeeHaze Q.100% (1)
- Foreshadowing: What Is It?Document11 pagesForeshadowing: What Is It?David Veach100% (1)
- The Nature Notes of An Edwardian Lady (Holden, Edith) (Z-Library)Document200 pagesThe Nature Notes of An Edwardian Lady (Holden, Edith) (Z-Library)Victoria OyarzunNo ratings yet
- Medical Genetics - I Year, I Semester - List of QuestionsDocument3 pagesMedical Genetics - I Year, I Semester - List of QuestionsGiviko GvinjiliaNo ratings yet
- Drug, Set, and Setting: Norman E. Zinberg M.DDocument176 pagesDrug, Set, and Setting: Norman E. Zinberg M.DItzcoatl Torres AlcantaraNo ratings yet
- TESDA Advanced Housekeeping Course DesignDocument160 pagesTESDA Advanced Housekeeping Course Designjazzy mallariNo ratings yet
- Au Pair ItepDocument3 pagesAu Pair ItepCaio Cezar Augusto100% (1)
- Soal Analytical ExpositionDocument31 pagesSoal Analytical ExpositionRayanggaNo ratings yet
- Judge, Clerk Fined for Illegal MarriagesDocument3 pagesJudge, Clerk Fined for Illegal MarriagesYodh Jamin OngNo ratings yet
- Speech MechanismDocument2 pagesSpeech MechanismangelicaNo ratings yet
- Lab 8Document4 pagesLab 8Thi NguyenNo ratings yet
- Trauma Informed Education 1Document9 pagesTrauma Informed Education 1api-662062431No ratings yet
- Feudalism in Medieval EuropeDocument5 pagesFeudalism in Medieval EuropeDipankar BhattacharjeeNo ratings yet
- Pro Tech 1 CH 2Document29 pagesPro Tech 1 CH 2weldsvNo ratings yet
- EED02 Notes1Document8 pagesEED02 Notes1Lem Merob100% (1)
- Transmission Lines & Wave GuidesDocument8 pagesTransmission Lines & Wave GuidesRajesh ShanNo ratings yet
- Shri Jagannath in Yantra, Tantra and MantraDocument8 pagesShri Jagannath in Yantra, Tantra and Mantraprantik32No ratings yet
- VIBRATION TITLEDocument49 pagesVIBRATION TITLEMark Oliver BernardoNo ratings yet
- UTILITARIANISM: Origin and Nature of The TheoryDocument6 pagesUTILITARIANISM: Origin and Nature of The TheoryCarlisle ParkerNo ratings yet
- High Court and Its JurisdictionDocument7 pagesHigh Court and Its JurisdictionHari GovindNo ratings yet
- Ranor of The North OutlineDocument4 pagesRanor of The North OutlineSean NorthridgeNo ratings yet
- Analysis of The Survey On Mobile PhonesDocument6 pagesAnalysis of The Survey On Mobile PhonesBikesh MaharjanNo ratings yet
- Beklædning MændDocument11 pagesBeklædning MændOrsolya Eszter KiszelyNo ratings yet
- Caregiver Tip SheetDocument3 pagesCaregiver Tip SheetIndiana Family to FamilyNo ratings yet
- Mt103 - Pko Bank Polski Sa (Pko) Formatting Requirements: Status M/O/ C Field Field Name Content CommentsDocument3 pagesMt103 - Pko Bank Polski Sa (Pko) Formatting Requirements: Status M/O/ C Field Field Name Content CommentsSiau HuiNo ratings yet
- Senior Project ProposalDocument8 pagesSenior Project Proposalapi-359781788No ratings yet
- gm07652r PDFDocument21 pagesgm07652r PDFjose luisNo ratings yet
- Zamboanga Phenomenon - 10-Yr-Olds Giving BirthDocument5 pagesZamboanga Phenomenon - 10-Yr-Olds Giving BirthiecscstNo ratings yet