You might also like
- The Appropriations Law Answer Book: A Q&A Guide to Fiscal LawFrom EverandThe Appropriations Law Answer Book: A Q&A Guide to Fiscal LawNo ratings yet
- Deed of Absolute SaleDocument2 pagesDeed of Absolute SaleRonalyn Bergado LucenaNo ratings yet
- Shriram General Insurance Co. Ltd. claim discharge voucher formatDocument1 pageShriram General Insurance Co. Ltd. claim discharge voucher formatmjanifa67% (6)
- Turtle Mountain Tribal By-Laws For Indian Children Under I.C.W.A. Covering Children Who Do Not Qualify Under Blood Quantum Criteria.Document2 pagesTurtle Mountain Tribal By-Laws For Indian Children Under I.C.W.A. Covering Children Who Do Not Qualify Under Blood Quantum Criteria.ICWATurtleMountainNo ratings yet
- Home Study Course TemplateDocument12 pagesHome Study Course Templategeorge_watts774995No ratings yet
- DRAFT Rosebud Sioux Tribe Hemp Code 7-29-19Document8 pagesDRAFT Rosebud Sioux Tribe Hemp Code 7-29-19Ojinjintka NewsNo ratings yet
- 2020 HCB 6192Document31 pages2020 HCB 6192WXYZ-TV Channel 7 Detroit0% (1)
- Draft Cannabis Ordinance For Unincorporated Riverside CountyDocument58 pagesDraft Cannabis Ordinance For Unincorporated Riverside CountyThe Press-Enterprise / pressenterprise.comNo ratings yet
- Traffic Stop RT 104 (88329)Document2 pagesTraffic Stop RT 104 (88329)News 8 WROCNo ratings yet
- Cannabis Class Action Lawsuit - UHDocument2 pagesCannabis Class Action Lawsuit - UHTony Lange100% (1)
- National Drug Control Strategy 2022Document152 pagesNational Drug Control Strategy 2022Medicinal ColoradoNo ratings yet
- Compassionate Sciences Inc NorthernAPPDocument72 pagesCompassionate Sciences Inc NorthernAPPNew Jersey marijuana documentsNo ratings yet
- CFR 2017 Title42a Vol3Document969 pagesCFR 2017 Title42a Vol3nspanoliosNo ratings yet
- 2021 Petition To Deschedule CannabisDocument5 pages2021 Petition To Deschedule CannabisStephen ZyszkiewiczNo ratings yet
- Vol. 1 Issue 6: Share This Like A Good Joint ..Document16 pagesVol. 1 Issue 6: Share This Like A Good Joint ..Casper LeitchNo ratings yet
- SmartSafeFlorida AdultCannabisMeasureDocument4 pagesSmartSafeFlorida AdultCannabisMeasureTony LangeNo ratings yet
- Property Law TermsDocument6 pagesProperty Law TermsTefo TshukuduNo ratings yet
- 58 Wayne L. Rev. 81 - Much Ado About Nothing Why Rescheduling - Kevin A. SabetDocument21 pages58 Wayne L. Rev. 81 - Much Ado About Nothing Why Rescheduling - Kevin A. SabetWayneLawReviewNo ratings yet
- RST Court AbbreviationsDocument1 pageRST Court AbbreviationsOjinjintka NewsNo ratings yet
- Making Medical Decision For Someone ElseDocument23 pagesMaking Medical Decision For Someone Elseapi-274729393100% (1)
- In Motion: CDTC Executive Director Michael Franchini Announces Retirement!Document6 pagesIn Motion: CDTC Executive Director Michael Franchini Announces Retirement!Jacob BeemanNo ratings yet
- Clark County Clerk Website RESEARCHDocument4 pagesClark County Clerk Website RESEARCHJohnimeNo ratings yet
- Fuel of The Future:: Figure 1 Some Uses of Industrial CannabisDocument8 pagesFuel of The Future:: Figure 1 Some Uses of Industrial CannabishonourebelNo ratings yet
- Bill of Rights WebquestDocument4 pagesBill of Rights Webquestapi-3267961900% (1)
- Hawaii Medical Cannabis Patient and Provider Survey July 2022Document31 pagesHawaii Medical Cannabis Patient and Provider Survey July 2022Baron SekiyaNo ratings yet
- CMMLUO Humboldt Ordinance 2544Document35 pagesCMMLUO Humboldt Ordinance 2544Alex Jennemann-JenkinsNo ratings yet
- Emergency and Disaster Management Act Impacts To The PRRD - CS-COW-002Document5 pagesEmergency and Disaster Management Act Impacts To The PRRD - CS-COW-002Tom SummerNo ratings yet
- New York 501c3 ChecklistDocument6 pagesNew York 501c3 ChecklistFred AbramsonNo ratings yet
- Pennsylvania Report On Adult Use Recreational MarijuanaDocument89 pagesPennsylvania Report On Adult Use Recreational MarijuanaMarijuana MomentNo ratings yet
- Targeted Human Development Programs - Investing in The Next GenerationDocument30 pagesTargeted Human Development Programs - Investing in The Next GenerationSara ValentinNo ratings yet
- Progress Report New York Medical Marijuana ProgramDocument2 pagesProgress Report New York Medical Marijuana ProgramMPPNo ratings yet
- Wrongful-Death LawsuitDocument15 pagesWrongful-Death LawsuitTom SteeleNo ratings yet
- Client V Doran Tennessee Auto Accident LawsuitDocument7 pagesClient V Doran Tennessee Auto Accident LawsuitCummings ManookianNo ratings yet
- Oregon Cannabis Jobs ReportDocument15 pagesOregon Cannabis Jobs ReportStatesman Journal100% (1)
- Oklahoma's Low-THC LawDocument1 pageOklahoma's Low-THC LawMPPNo ratings yet
- Georgia GovernmentDocument30 pagesGeorgia GovernmentShawn DaviesNo ratings yet
- Lynn Notice of DeterminationDocument3 pagesLynn Notice of DeterminationSarah LehrNo ratings yet
- Compassion Collective of Camden CountyDocument84 pagesCompassion Collective of Camden CountyNew Jersey marijuana documentsNo ratings yet
- USVI Medical Marijuana BillDocument53 pagesUSVI Medical Marijuana BillMarijuana MomentNo ratings yet
- HHS ResponseDocument11 pagesHHS ResponseSunlight FoundationNo ratings yet
- Developing A Childcare Center Business Plan: 1. Cover Sheet - SummaryDocument3 pagesDeveloping A Childcare Center Business Plan: 1. Cover Sheet - SummaryPrincess Marshalee Foster100% (1)
- State Medical Marijuana Program Implementation TimelineDocument1 pageState Medical Marijuana Program Implementation TimelineMPPNo ratings yet
- Hogan Lovells, The AKA's Law Firm Legal Brief Letter Regarding Kratom Scheduling Docket No. DEA-442Document35 pagesHogan Lovells, The AKA's Law Firm Legal Brief Letter Regarding Kratom Scheduling Docket No. DEA-442pogue972100% (1)
- Leadership Letter 1.21.2022Document11 pagesLeadership Letter 1.21.2022Helen Bennett100% (1)
- US Committee On Financial Services - Financial System Regulatory RestructuringDocument27 pagesUS Committee On Financial Services - Financial System Regulatory RestructuringJH_CarrNo ratings yet
- 37-2013-00078268-Cu-Bt-Ctl Roa-1 12-04-13 Complaint 1386637937306Document118 pages37-2013-00078268-Cu-Bt-Ctl Roa-1 12-04-13 Complaint 1386637937306api-218643948No ratings yet
- Top Ten Reasons To End Marijuana ProhibitionDocument1 pageTop Ten Reasons To End Marijuana ProhibitionMPP100% (1)
- A Generic Nonprofit Articles of Incorporation Tax Exempt LanguageDocument3 pagesA Generic Nonprofit Articles of Incorporation Tax Exempt LanguageDave McGee100% (1)
- Key Aspects of State and D.C. Medical Marijuana LawsDocument16 pagesKey Aspects of State and D.C. Medical Marijuana LawsMPP100% (2)
- Breakdown of Fees in Adult-Use StatesDocument6 pagesBreakdown of Fees in Adult-Use StatesMPPNo ratings yet
- South Dakota Marijuana RulingsDocument16 pagesSouth Dakota Marijuana RulingsMarijuana MomentNo ratings yet
- TenFactsAboutMarijuana PDFDocument10 pagesTenFactsAboutMarijuana PDFwebmaster@drugpolicy.org100% (5)
- Code Enforcement Unit: Annual ReportDocument27 pagesCode Enforcement Unit: Annual ReportRuth SchneiderNo ratings yet
- The History of Cannabis Regulation in Shasta County 10.11.14Document7 pagesThe History of Cannabis Regulation in Shasta County 10.11.14MatthewMeyerNo ratings yet
- Punkin Chunkin LawsuitDocument44 pagesPunkin Chunkin LawsuitDelaware Public MediaNo ratings yet
- Michigan's Medical Marihuana ActDocument27 pagesMichigan's Medical Marihuana Actapi-25946258No ratings yet
- Iowa's Low-THC Law SummaryDocument1 pageIowa's Low-THC Law SummaryMPPNo ratings yet
- Register For Your FEMA SIDDocument3 pagesRegister For Your FEMA SIDpcmundot50% (2)
- Family Equality ComplaintDocument39 pagesFamily Equality ComplaintHilary LedwellNo ratings yet
- Petition Urging Governors To Protect Medical Cannabis AccessDocument70 pagesPetition Urging Governors To Protect Medical Cannabis AccessMPPNo ratings yet
- 2020 Vermont Poll ResultsDocument7 pages2020 Vermont Poll ResultsMPPNo ratings yet
- Simon Poll March 2019Document14 pagesSimon Poll March 2019MPPNo ratings yet
- Marijuana Policy Map May 2020Document1 pageMarijuana Policy Map May 2020MPPNo ratings yet
- Marijuana Policy Progress Report 2019 Legislative UpdateDocument28 pagesMarijuana Policy Progress Report 2019 Legislative UpdateMPP100% (3)
- Prescribing Versus Recommending Medical CannabisDocument2 pagesPrescribing Versus Recommending Medical CannabisMPPNo ratings yet
- Medical Cannabis Provides An Alternative To OpiatesDocument1 pageMedical Cannabis Provides An Alternative To OpiatesMPPNo ratings yet
- GQR Connecticut Poll January 2020Document1 pageGQR Connecticut Poll January 2020MPPNo ratings yet
- MPP Policy Paper - Regulating Cannabis Oil VaporizersDocument7 pagesMPP Policy Paper - Regulating Cannabis Oil VaporizersMPPNo ratings yet
- Decriminalization and Expungement in NY: An Overview of A0840 / S06579Document1 pageDecriminalization and Expungement in NY: An Overview of A0840 / S06579MPPNo ratings yet
- Severe Pain and Medical CannabisDocument1 pageSevere Pain and Medical CannabisMPPNo ratings yet
- Medical Cannabis Implementation TimelinesDocument10 pagesMedical Cannabis Implementation TimelinesMPPNo ratings yet
- 2017 SIU Paul Simon Public Policy Institute Legalization PollDocument7 pages2017 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- Medical Marijuana MapDocument1 pageMedical Marijuana MapMPPNo ratings yet
- U.S. Attorneys' Comments Post Cole Memo RecissionDocument8 pagesU.S. Attorneys' Comments Post Cole Memo RecissionMPPNo ratings yet
- Potential Revenue From Regulating Marijuana in ConnecticutDocument2 pagesPotential Revenue From Regulating Marijuana in ConnecticutMPPNo ratings yet
- What Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?Document2 pagesWhat Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?MPPNo ratings yet
- 2018 SIU Paul Simon Public Policy Institute Legalization PollDocument4 pages2018 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- Progress Report New York Medical Marijuana ProgramDocument2 pagesProgress Report New York Medical Marijuana ProgramMPPNo ratings yet
- New Jersey Progress ReportDocument2 pagesNew Jersey Progress ReportMPPNo ratings yet
- Expungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionDocument1 pageExpungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionMPPNo ratings yet
- Maryland Progress ReportDocument2 pagesMaryland Progress ReportMPPNo ratings yet
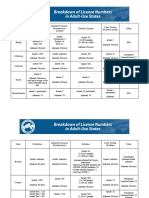
- Breakdown of License Numbers in Adult-Use StatesDocument2 pagesBreakdown of License Numbers in Adult-Use StatesMPPNo ratings yet
- D.C.'s Medical Marijuana ProgramDocument2 pagesD.C.'s Medical Marijuana ProgramMPPNo ratings yet
- Breakdown of Fees in Adult-Use StatesDocument6 pagesBreakdown of Fees in Adult-Use StatesMPPNo ratings yet
- Revenue From Adult Use StatesDocument5 pagesRevenue From Adult Use StatesMPPNo ratings yet
- Medical Marijuana by The NumbersDocument2 pagesMedical Marijuana by The NumbersMPPNo ratings yet
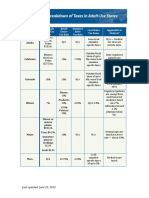
- Breakdown of Taxes in Adult-Use StatesDocument2 pagesBreakdown of Taxes in Adult-Use StatesMPPNo ratings yet
- Sessions Asks Congress To Undo Medical Marijuana ProtectionsDocument3 pagesSessions Asks Congress To Undo Medical Marijuana ProtectionsMPPNo ratings yet
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDocument1 pageSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNo ratings yet
- Block M2 EYE Distribution by MMCDocument3 pagesBlock M2 EYE Distribution by MMCF ParikhNo ratings yet
- A Study On Consumers Perception of Millets As A Staple FoodDocument69 pagesA Study On Consumers Perception of Millets As A Staple FoodJerin Geo JosNo ratings yet
- Republika NG PilipinasDocument2 pagesRepublika NG PilipinasAcii monseNo ratings yet
- Cephalexin Med CardDocument2 pagesCephalexin Med CardAnja de VriesNo ratings yet
- PHILIPPINE HEALTH CARE PROVIDERS INC. vs. CIRDocument17 pagesPHILIPPINE HEALTH CARE PROVIDERS INC. vs. CIRDenee Vem MatorresNo ratings yet
- 6610 Assignment 4Document19 pages6610 Assignment 4gyanendraNo ratings yet
- Course Content Related To Chronic Wounds in Nursing Degree Programs in SpainDocument2 pagesCourse Content Related To Chronic Wounds in Nursing Degree Programs in SpainMikey MadRatNo ratings yet
- Physio Assess Form Oct 2022Document5 pagesPhysio Assess Form Oct 2022RishaadNo ratings yet
- Chitoglucan New OverviewDocument6 pagesChitoglucan New OverviewmjmorcelliNo ratings yet
- School Form 8 Sf8 Learner Basic Health and Nutrition Report AutomaticDocument12 pagesSchool Form 8 Sf8 Learner Basic Health and Nutrition Report AutomaticYojmhie Joy Ko100% (2)
- What Is AmpalayaDocument5 pagesWhat Is Ampalayarugu0% (1)
- Assignment 2 HLTH 103 Bhima Devi Poudel Adhikari 220179000Document10 pagesAssignment 2 HLTH 103 Bhima Devi Poudel Adhikari 220179000api-525310113No ratings yet
- Questionnaire BHWDocument2 pagesQuestionnaire BHWRogerQux100% (2)
- Research Themes and Advances in MalariaDocument11 pagesResearch Themes and Advances in Malarialilibeth paola duran plataNo ratings yet
- Proclamation: Special Observances: National Prostate Cancer Awareness Month (Proc. 8045)Document2 pagesProclamation: Special Observances: National Prostate Cancer Awareness Month (Proc. 8045)Justia.comNo ratings yet
- REPORT ON YOGA RESEARCH STUDIES AT ACYTER, JIPMER: 2008 To 2012.Document126 pagesREPORT ON YOGA RESEARCH STUDIES AT ACYTER, JIPMER: 2008 To 2012.Yogacharya Dr Ananda Balayogi BhavananiNo ratings yet
- Types of fitness activities and modifiable risk factorsDocument14 pagesTypes of fitness activities and modifiable risk factorsMaria Cristy CanceranNo ratings yet
- MAPEH 1 (2nd Quarter Complete)Document60 pagesMAPEH 1 (2nd Quarter Complete)Roselyn GutasNo ratings yet
- Betty Neuman's Contributions to Nursing TheoryDocument2 pagesBetty Neuman's Contributions to Nursing TheoryBrecelle DelvoNo ratings yet
- Manual On Minimum Standards of Care in Addiction Treatment CentresDocument61 pagesManual On Minimum Standards of Care in Addiction Treatment CentresGlobal Law FirmNo ratings yet
- Health and Safety Policy Manual Issue 14Document34 pagesHealth and Safety Policy Manual Issue 14caskevNo ratings yet
- Careers in Social Work: Outlook, Pay & MoreDocument9 pagesCareers in Social Work: Outlook, Pay & Morejoel lacayNo ratings yet
- Liver Abscess ThesisDocument7 pagesLiver Abscess Thesisjenniferalexanderfortlauderdale100% (1)
- Nursing Licensure Exam Compilation of TipsDocument3 pagesNursing Licensure Exam Compilation of TipsIkarishinNo ratings yet
- NO Nama Pasien Tanggal Rujukan/Tujuan RsDocument44 pagesNO Nama Pasien Tanggal Rujukan/Tujuan RsfennyNo ratings yet
- Standard No. CEA/Wellness Centre-018Document21 pagesStandard No. CEA/Wellness Centre-018Gladys MatiraNo ratings yet
- Culturally Competent For NursesDocument9 pagesCulturally Competent For Nursesleli khairaniNo ratings yet
- Asthma Management in 40 CharactersDocument10 pagesAsthma Management in 40 CharactersAmalNo ratings yet
- 116 Salalima Vs ECC and SSSDocument4 pages116 Salalima Vs ECC and SSScharmssatellNo ratings yet
- Ethical Issues Faced by Nurses During Nursingpractice in District Layyah PakistanDocument7 pagesEthical Issues Faced by Nurses During Nursingpractice in District Layyah PakistanMawadah Setya RahmawatiNo ratings yet