You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Petition Urging Governors To Protect Medical Cannabis AccessDocument70 pagesPetition Urging Governors To Protect Medical Cannabis AccessMPPNo ratings yet
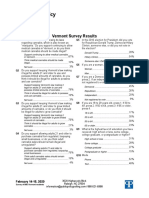
- 2020 Vermont Poll ResultsDocument7 pages2020 Vermont Poll ResultsMPPNo ratings yet
- Simon Poll March 2019Document14 pagesSimon Poll March 2019MPPNo ratings yet
- Marijuana Policy Map May 2020Document1 pageMarijuana Policy Map May 2020MPPNo ratings yet
- Marijuana Policy Progress Report 2019 Legislative UpdateDocument28 pagesMarijuana Policy Progress Report 2019 Legislative UpdateMPP100% (3)
- Prescribing Versus Recommending Medical CannabisDocument2 pagesPrescribing Versus Recommending Medical CannabisMPPNo ratings yet
- Medical Cannabis Provides An Alternative To OpiatesDocument1 pageMedical Cannabis Provides An Alternative To OpiatesMPPNo ratings yet
- GQR Connecticut Poll January 2020Document1 pageGQR Connecticut Poll January 2020MPPNo ratings yet
- MPP Policy Paper - Regulating Cannabis Oil VaporizersDocument7 pagesMPP Policy Paper - Regulating Cannabis Oil VaporizersMPPNo ratings yet
- Decriminalization and Expungement in NY: An Overview of A0840 / S06579Document1 pageDecriminalization and Expungement in NY: An Overview of A0840 / S06579MPPNo ratings yet
- Severe Pain and Medical CannabisDocument1 pageSevere Pain and Medical CannabisMPPNo ratings yet
- Medical Cannabis Implementation TimelinesDocument10 pagesMedical Cannabis Implementation TimelinesMPPNo ratings yet
- 2017 SIU Paul Simon Public Policy Institute Legalization PollDocument7 pages2017 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- Medical Marijuana MapDocument1 pageMedical Marijuana MapMPPNo ratings yet
- U.S. Attorneys' Comments Post Cole Memo RecissionDocument8 pagesU.S. Attorneys' Comments Post Cole Memo RecissionMPPNo ratings yet
- Potential Revenue From Regulating Marijuana in ConnecticutDocument2 pagesPotential Revenue From Regulating Marijuana in ConnecticutMPPNo ratings yet
- What Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?Document2 pagesWhat Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?MPPNo ratings yet
- 2018 SIU Paul Simon Public Policy Institute Legalization PollDocument4 pages2018 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- Progress Report New York Medical Marijuana ProgramDocument2 pagesProgress Report New York Medical Marijuana ProgramMPPNo ratings yet
- New Jersey Progress ReportDocument2 pagesNew Jersey Progress ReportMPPNo ratings yet
- Expungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionDocument1 pageExpungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionMPPNo ratings yet
- Maryland Progress ReportDocument2 pagesMaryland Progress ReportMPPNo ratings yet
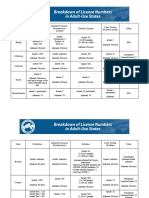
- Breakdown of License Numbers in Adult-Use StatesDocument2 pagesBreakdown of License Numbers in Adult-Use StatesMPPNo ratings yet
- D.C.'s Medical Marijuana ProgramDocument2 pagesD.C.'s Medical Marijuana ProgramMPPNo ratings yet
- Breakdown of Fees in Adult-Use StatesDocument6 pagesBreakdown of Fees in Adult-Use StatesMPPNo ratings yet
- Revenue From Adult Use StatesDocument5 pagesRevenue From Adult Use StatesMPPNo ratings yet
- Medical Marijuana by The NumbersDocument2 pagesMedical Marijuana by The NumbersMPPNo ratings yet
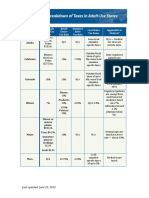
- Breakdown of Taxes in Adult-Use StatesDocument2 pagesBreakdown of Taxes in Adult-Use StatesMPPNo ratings yet
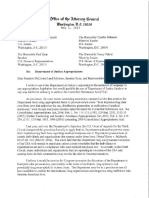
- Sessions Asks Congress To Undo Medical Marijuana ProtectionsDocument3 pagesSessions Asks Congress To Undo Medical Marijuana ProtectionsMPPNo ratings yet
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDocument1 pageSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Death by Heroin Intoxication in A Body Pusher WithDocument7 pagesDeath by Heroin Intoxication in A Body Pusher WithRuben_Monroy_ClaudioNo ratings yet
- Drug Dosage Calculations Formulas GuideDocument2 pagesDrug Dosage Calculations Formulas Guidems_lezahNo ratings yet
- Erythema MultiformeDocument159 pagesErythema MultiformeWendy EvansNo ratings yet
- 2017 - Stockist ObatDocument6 pages2017 - Stockist ObatUrdona Proteksia NezaraNo ratings yet
- Antiepileptic DrugsDocument39 pagesAntiepileptic Drugsking_goldNo ratings yet
- Drug Study AdenocarcinomaDocument3 pagesDrug Study AdenocarcinomaJoyce AgorNo ratings yet
- Drugs in PregnancyDocument32 pagesDrugs in PregnancyHazar_OtourNo ratings yet
- Gr. 9 - Types of Drugs Slide ShowDocument43 pagesGr. 9 - Types of Drugs Slide ShowdhairyapbNo ratings yet
- Caffeine Piece in WiredDocument4 pagesCaffeine Piece in Wiredthird3planetNo ratings yet
- Management of Infection in Primary Care Adapted For Local UseDocument15 pagesManagement of Infection in Primary Care Adapted For Local UseWizri SuharianiNo ratings yet
- EpinephrineDocument4 pagesEpinephrineHarthwell CapistranoNo ratings yet
- Paws and Claws Pet Care 101Document2 pagesPaws and Claws Pet Care 101pawsandclawspetcareNo ratings yet
- Avoiding CPSEs - Laboratory Medication Vital SignsDocument30 pagesAvoiding CPSEs - Laboratory Medication Vital SignsForNo ratings yet
- Counterfeit DrugsDocument2 pagesCounterfeit DrugsfreeBlidaman0967% (3)
- Classification Revised For Lung Adenocarcinoma: Fighting Tuberculosis in SiberiaDocument24 pagesClassification Revised For Lung Adenocarcinoma: Fighting Tuberculosis in SiberiaYantoNo ratings yet
- Tablas de Dosificacion Kirk 9na EdDocument68 pagesTablas de Dosificacion Kirk 9na EdMarlieth Rosales HernandezNo ratings yet
- BudionoSantoso 2016 BiographyDocument15 pagesBudionoSantoso 2016 Biographyerickn NofrianNo ratings yet
- Travel Information To QatarDocument2 pagesTravel Information To Qatarkaran patelNo ratings yet
- List of Controlled SubstancesDocument2 pagesList of Controlled Substancesspiccolo12100% (1)
- Pembagian Barang BPJS So Des 2019 Kfa MdoDocument56 pagesPembagian Barang BPJS So Des 2019 Kfa Mdokf ttrNo ratings yet
- Acne Vulgaris By: Dr. Majid Suhail Prof DermatologyDocument78 pagesAcne Vulgaris By: Dr. Majid Suhail Prof DermatologyMajid SuhailNo ratings yet
- Irish Pharmacist May 09Document44 pagesIrish Pharmacist May 09John MaguireNo ratings yet
- Daftarstokglobalopname11 05 20 PDFDocument10 pagesDaftarstokglobalopname11 05 20 PDFAlfhie Khafidhatul KhasanahhNo ratings yet
- BCS Classification of 900+ Drugs PDFDocument29 pagesBCS Classification of 900+ Drugs PDFNick DiFranco100% (1)
- Ophthalmic Preparations 1435Document97 pagesOphthalmic Preparations 1435zayedaliNo ratings yet
- Fluoride and Fluoridation: Topical FluoridesDocument3 pagesFluoride and Fluoridation: Topical FluoridesmarkoNo ratings yet
- Beatles - White Album (Score)Document4 pagesBeatles - White Album (Score)LeeEstradaNo ratings yet
- S. No. Division Name Purpose Name Fee Paid As Per GSR 1193Document9 pagesS. No. Division Name Purpose Name Fee Paid As Per GSR 1193VIJAY YADAVNo ratings yet
- Dr. Rajeev - Oral Controlled Release Drug PDFDocument38 pagesDr. Rajeev - Oral Controlled Release Drug PDFParthMairNo ratings yet
- Price List Obat NewDocument19 pagesPrice List Obat NewSri WulandariNo ratings yet