You might also like
- Marijuana Policy Progress Report 2019 Legislative UpdateDocument28 pagesMarijuana Policy Progress Report 2019 Legislative UpdateMPP100% (3)
- Medical Marijuana Laws and Anti-Discrimination ProvisionsDocument12 pagesMedical Marijuana Laws and Anti-Discrimination ProvisionsMPPNo ratings yet
- Physician Guide To Cannabis-Assisted Opioid Reduction (Distributed by EB)Document2 pagesPhysician Guide To Cannabis-Assisted Opioid Reduction (Distributed by EB)Lisa Rough100% (6)
- Article Cannabis and CreativityDocument12 pagesArticle Cannabis and CreativityThomas CarswellNo ratings yet
- Robert Connell Clarke - Hashish (1998)Document432 pagesRobert Connell Clarke - Hashish (1998)Lospa Stocazzo100% (3)
- Cannabis Extracts For Beginners and Du - James Brandon PHDDocument39 pagesCannabis Extracts For Beginners and Du - James Brandon PHDColleen Van Schalkwyk100% (1)
- Build Your Own Homemade Smoking DevicesDocument99 pagesBuild Your Own Homemade Smoking DevicesGabriel GabarramNo ratings yet
- Marijuana SlidesDocument61 pagesMarijuana SlidesStephan CarlsonNo ratings yet
- SmartSafeFlorida AdultCannabisMeasureDocument4 pagesSmartSafeFlorida AdultCannabisMeasureTony LangeNo ratings yet
- Juul vs. CounterfeitsDocument20 pagesJuul vs. CounterfeitsJordan Crook100% (2)
- Petition Urging Governors To Protect Medical Cannabis AccessDocument70 pagesPetition Urging Governors To Protect Medical Cannabis AccessMPPNo ratings yet
- Neurological Effects of The THC in Human PresentationDocument9 pagesNeurological Effects of The THC in Human PresentationPalakang PetotNo ratings yet
- Severe Pain and Medical CannabisDocument1 pageSevere Pain and Medical CannabisMPPNo ratings yet
- Severe Pain and Medical CannabisDocument1 pageSevere Pain and Medical CannabisMPPNo ratings yet
- Marijuana and Medicine: Assessing The Science BaseDocument4 pagesMarijuana and Medicine: Assessing The Science BaseMPPNo ratings yet
- Excise Tax GuideDocument26 pagesExcise Tax GuideKaren Cael100% (1)
- Conservative Thinkers and Marijuana Policy ReformDocument2 pagesConservative Thinkers and Marijuana Policy ReformMPP100% (1)
- What Is Rick Simpson OilDocument7 pagesWhat Is Rick Simpson Oilrahinatu mohammedNo ratings yet
- Cannabis Class Action Lawsuit - UHDocument2 pagesCannabis Class Action Lawsuit - UHTony Lange100% (1)
- Statement of PrincipleDocument2 pagesStatement of PrincipleMPP100% (2)
- Marijuana Prohibition FactsDocument5 pagesMarijuana Prohibition FactsMPPNo ratings yet
- Peer-Reviewed Cannabis and Cancer Research ReferencesDocument45 pagesPeer-Reviewed Cannabis and Cancer Research ReferencesCannabinoid AndroidNo ratings yet
- Regulation WorksDocument1 pageRegulation WorksMPPNo ratings yet
- Tax and Regulate BrochureDocument2 pagesTax and Regulate BrochureMPPNo ratings yet
- Model Tax and Regulate Bill SummaryDocument2 pagesModel Tax and Regulate Bill SummaryMPPNo ratings yet
- TenFactsAboutMarijuana PDFDocument10 pagesTenFactsAboutMarijuana PDFwebmaster@drugpolicy.org100% (5)
- Gateway Theory DebunkedDocument2 pagesGateway Theory DebunkedMPPNo ratings yet
- Federal Obstruction of Medical Marijuana ResearchDocument2 pagesFederal Obstruction of Medical Marijuana ResearchMPPNo ratings yet
- CBD Laws OverviewDocument6 pagesCBD Laws OverviewMPPNo ratings yet
- Oklahoma's Low-THC LawDocument1 pageOklahoma's Low-THC LawMPPNo ratings yet
- Cannabis Use and Substantial Reduction in Premature Deaths in The United States.Document53 pagesCannabis Use and Substantial Reduction in Premature Deaths in The United States.Monterey Bud100% (2)
- Medical Marijuana Patient CasualtiesDocument2 pagesMedical Marijuana Patient CasualtiesMPP100% (3)
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDocument1 pageSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNo ratings yet
- Regulatory Authorities and Medical CannabisDocument3 pagesRegulatory Authorities and Medical CannabisMPPNo ratings yet
- Delta9 tetrhydrocannabinolTHCDocument22 pagesDelta9 tetrhydrocannabinolTHCMedicalCannabis SpainNo ratings yet
- Thesis PresentationDocument17 pagesThesis PresentationBert EnajeNo ratings yet
- Colorado and Washington: Life After Legalization and RegulationDocument2 pagesColorado and Washington: Life After Legalization and RegulationMPP100% (3)
- Legal Status of Cannabinoids in End-User Products On EU MarketDocument32 pagesLegal Status of Cannabinoids in End-User Products On EU MarketMichal Tőzsér0% (1)
- Progress Report New York Medical Marijuana ProgramDocument2 pagesProgress Report New York Medical Marijuana ProgramMPPNo ratings yet
- Model State Medical Cannabis BillDocument26 pagesModel State Medical Cannabis BillMPPNo ratings yet
- Cannabis Research LetterDocument2 pagesCannabis Research LetterMarijuana MomentNo ratings yet
- Iowa's Low-THC Law SummaryDocument1 pageIowa's Low-THC Law SummaryMPPNo ratings yet
- Michigan's Medical Marihuana ActDocument27 pagesMichigan's Medical Marihuana Actapi-25946258No ratings yet
- Overview of Maryland's Medical Marijuana LawDocument3 pagesOverview of Maryland's Medical Marijuana LawMPP100% (1)
- Cannabis Psychosis Fact Sheet PDFDocument1 pageCannabis Psychosis Fact Sheet PDFricardo_balau8081No ratings yet
- Revenue From Adult Use StatesDocument5 pagesRevenue From Adult Use StatesMPPNo ratings yet
- Synthetic Cannabinoid Fact Sheet PDFDocument4 pagesSynthetic Cannabinoid Fact Sheet PDFwebmaster@drugpolicy.orgNo ratings yet
- State Decrim ChartDocument4 pagesState Decrim ChartMPPNo ratings yet
- State-by-State Provisions For Adding Qualifying ConditionsDocument5 pagesState-by-State Provisions For Adding Qualifying ConditionsMPPNo ratings yet
- Changing Landscape of Cannabis Novel Products Formulations and Methods of Administration PDFDocument5 pagesChanging Landscape of Cannabis Novel Products Formulations and Methods of Administration PDFliaNo ratings yet
- Belize Decriminalizes Marijuana PossessionDocument5 pagesBelize Decriminalizes Marijuana PossessionMichelle WebsterNo ratings yet
- Cannabis For Restless Legs SyndromeDocument1 pageCannabis For Restless Legs SyndromeGi GlerNo ratings yet
- 2018 Model LegislationDocument18 pages2018 Model LegislationPaul MariniNo ratings yet
- Development and Application of A LC-MS/MS Method For The Analysis of Plasma Bioavailabilities of Different Cannabinoids After The Administration of Cannabis Sativa L. Extracts and MarinolTMDocument134 pagesDevelopment and Application of A LC-MS/MS Method For The Analysis of Plasma Bioavailabilities of Different Cannabinoids After The Administration of Cannabis Sativa L. Extracts and MarinolTMamccaw1590No ratings yet
- Marijuana - Marijuana As MedicineDocument1 pageMarijuana - Marijuana As MedicinelearnaboutsamNo ratings yet
- Washington State Board of Pharmacy - Meeting Minutes - 2009-05-07Document11 pagesWashington State Board of Pharmacy - Meeting Minutes - 2009-05-07Cannabis Defense CoalitionNo ratings yet
- FDA CBD ReportDocument18 pagesFDA CBD ReportMarijuana Moment100% (2)
- CBD OIL - A Controversial Way To Get Healthier!Document6 pagesCBD OIL - A Controversial Way To Get Healthier!Ella CincanNo ratings yet
- tmp26DE TMPDocument130 pagestmp26DE TMPFrontiersNo ratings yet
- Chardan Capital On Cannabis MarketDocument8 pagesChardan Capital On Cannabis MarketotteromNo ratings yet
- Brett Painter Tech Writing SlideshowDocument17 pagesBrett Painter Tech Writing SlideshowBrett PainterNo ratings yet
- PTSD and Medical Cannabis ProgramsDocument3 pagesPTSD and Medical Cannabis ProgramsMPP100% (1)
- Breakdown of Fees in Adult-Use StatesDocument6 pagesBreakdown of Fees in Adult-Use StatesMPPNo ratings yet
- SS Usa 04-11Document48 pagesSS Usa 04-11steveurkleNo ratings yet
- 2018 Marijuana and Real Estate A Budding Issue Survey 11-02-2018Document36 pages2018 Marijuana and Real Estate A Budding Issue Survey 11-02-2018Jiell Richardson100% (1)
- Cannabinoids Primer: The Natural Synthesis and Pre-Cursors To CannabinoidsDocument4 pagesCannabinoids Primer: The Natural Synthesis and Pre-Cursors To CannabinoidsBi0hazardxNo ratings yet
- MPP Policy Paper - Regulating Cannabis Oil VaporizersDocument7 pagesMPP Policy Paper - Regulating Cannabis Oil VaporizersMPPNo ratings yet
- 2020 Vermont Poll ResultsDocument7 pages2020 Vermont Poll ResultsMPPNo ratings yet
- Decriminalization and Expungement in NY: An Overview of A0840 / S06579Document1 pageDecriminalization and Expungement in NY: An Overview of A0840 / S06579MPPNo ratings yet
- Medical Cannabis Provides An Alternative To OpiatesDocument1 pageMedical Cannabis Provides An Alternative To OpiatesMPPNo ratings yet
- GQR Connecticut Poll January 2020Document1 pageGQR Connecticut Poll January 2020MPPNo ratings yet
- Medical Cannabis Implementation TimelinesDocument10 pagesMedical Cannabis Implementation TimelinesMPPNo ratings yet
- Potential Revenue From Regulating Marijuana in ConnecticutDocument2 pagesPotential Revenue From Regulating Marijuana in ConnecticutMPPNo ratings yet
- Marijuana Policy Map May 2020Document1 pageMarijuana Policy Map May 2020MPPNo ratings yet
- Simon Poll March 2019Document14 pagesSimon Poll March 2019MPPNo ratings yet
- 2018 SIU Paul Simon Public Policy Institute Legalization PollDocument4 pages2018 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- Medical Marijuana MapDocument1 pageMedical Marijuana MapMPPNo ratings yet
- Prescribing Versus Recommending Medical CannabisDocument2 pagesPrescribing Versus Recommending Medical CannabisMPPNo ratings yet
- Maryland Progress ReportDocument2 pagesMaryland Progress ReportMPPNo ratings yet
- 2017 SIU Paul Simon Public Policy Institute Legalization PollDocument7 pages2017 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- U.S. Attorneys' Comments Post Cole Memo RecissionDocument8 pagesU.S. Attorneys' Comments Post Cole Memo RecissionMPPNo ratings yet
- Breakdown of Taxes in Adult-Use StatesDocument2 pagesBreakdown of Taxes in Adult-Use StatesMPPNo ratings yet
- What Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?Document2 pagesWhat Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?MPPNo ratings yet
- Progress Report New York Medical Marijuana ProgramDocument2 pagesProgress Report New York Medical Marijuana ProgramMPPNo ratings yet
- Sessions Asks Congress To Undo Medical Marijuana ProtectionsDocument3 pagesSessions Asks Congress To Undo Medical Marijuana ProtectionsMPPNo ratings yet
- Expungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionDocument1 pageExpungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionMPPNo ratings yet
- New Jersey Progress ReportDocument2 pagesNew Jersey Progress ReportMPPNo ratings yet
- D.C.'s Medical Marijuana ProgramDocument2 pagesD.C.'s Medical Marijuana ProgramMPPNo ratings yet
- Medical Marijuana by The NumbersDocument2 pagesMedical Marijuana by The NumbersMPPNo ratings yet
- Breakdown of Fees in Adult-Use StatesDocument6 pagesBreakdown of Fees in Adult-Use StatesMPPNo ratings yet
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDocument1 pageSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNo ratings yet
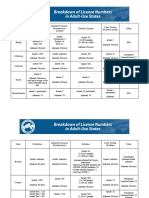
- Breakdown of License Numbers in Adult-Use StatesDocument2 pagesBreakdown of License Numbers in Adult-Use StatesMPPNo ratings yet
- Revenue From Adult Use StatesDocument5 pagesRevenue From Adult Use StatesMPPNo ratings yet
- Reassessment Form (Fillable)Document4 pagesReassessment Form (Fillable)Jason Tutt GinNo ratings yet
- 2019-10-10 Calvert County TimesDocument24 pages2019-10-10 Calvert County TimesSouthern Maryland OnlineNo ratings yet
- Penlon Sigma Delta Vaporizer - User ManualDocument67 pagesPenlon Sigma Delta Vaporizer - User ManualRaza AnwerNo ratings yet
- OHA Response To Governor Vaping 2019Document2 pagesOHA Response To Governor Vaping 2019Mark FurmanNo ratings yet
- David Emmett & Graeme Nice - What You Need To Know About Cannabis - Understanding The FactsDocument120 pagesDavid Emmett & Graeme Nice - What You Need To Know About Cannabis - Understanding The FactsJovana StojkovićNo ratings yet
- About The Company Highland PharmsDocument14 pagesAbout The Company Highland PharmsCannabis WeedNo ratings yet
- Cannabis/Hemp Extract Vaporizers: Standard Classification ForDocument9 pagesCannabis/Hemp Extract Vaporizers: Standard Classification ForSdferwste SrqreNo ratings yet
- Volcano Classic Instructions EN 2020.09Document48 pagesVolcano Classic Instructions EN 2020.09SamNo ratings yet
- ProVari ManualDocument16 pagesProVari ManualPatrickNo ratings yet
- Cannabis Smoke Condensate III: The Cannabinoid Content of VaporisedDocument6 pagesCannabis Smoke Condensate III: The Cannabinoid Content of VaporisedEmanuel PeraltaNo ratings yet
- Cool Fire IV User Manual GuideDocument13 pagesCool Fire IV User Manual GuideNeath MaroonNo ratings yet
- Protective and Risk Factors of CigarettesDocument6 pagesProtective and Risk Factors of Cigarettesfriendell ariasNo ratings yet
- Commercial Dispatch Eedition 10-13-19Document28 pagesCommercial Dispatch Eedition 10-13-19The DispatchNo ratings yet
- Legalization of Marijuana For Medical Purposes in The PhilippinesDocument21 pagesLegalization of Marijuana For Medical Purposes in The PhilippinesChristopher YuNo ratings yet
- Design & Write 2023Document32 pagesDesign & Write 2023Kristin BauerNo ratings yet
- Canna DabsDocument16 pagesCanna DabsVidákZsigmondNo ratings yet
- Vaporizers: II EquipmentDocument2 pagesVaporizers: II EquipmentEugene VovchukNo ratings yet
- MPP Policy Paper - Vaporizers PDFDocument7 pagesMPP Policy Paper - Vaporizers PDFJoseph PreisterNo ratings yet
- Chapter 1 5Document41 pagesChapter 1 5Benjo BataoNo ratings yet
- Electronic Cigarette Fires and Explosions in The United State 09-16Document64 pagesElectronic Cigarette Fires and Explosions in The United State 09-16jafranklin-1No ratings yet
- VaporizerDocument11 pagesVaporizerIhteshamNo ratings yet
- Major Constituents of Cannabis Vape Oil Liquid VapDocument14 pagesMajor Constituents of Cannabis Vape Oil Liquid VapRobby RanidoNo ratings yet
- David Emmett, Graeme Nice - What You Need To Know About Cannabis - Understanding The Facts (2008)Document129 pagesDavid Emmett, Graeme Nice - What You Need To Know About Cannabis - Understanding The Facts (2008)MarcoAntonioNo ratings yet