You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Toyota HiluxDocument34 pagesToyota HiluxLeo Te100% (6)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Crochet Triple Stitch CardiganDocument4 pagesCrochet Triple Stitch CardiganAnonymous FXsb2M100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 4320 Tractor IntroductionDocument9 pages4320 Tractor Introductionodali batista0% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- US Army Boxing - West Point Trainers Manual 51pDocument51 pagesUS Army Boxing - West Point Trainers Manual 51pLo Shun Fat100% (1)
- Doha Port Redevelopment - Combined Mina District & Seawater Diving Pool Check List For Drilling MachineDocument42 pagesDoha Port Redevelopment - Combined Mina District & Seawater Diving Pool Check List For Drilling MachineGia ArnelleNo ratings yet
- Modern AGE - Companion (GRR6304)Document130 pagesModern AGE - Companion (GRR6304)Kárpáti Géza83% (6)
- The Best Visual Volkswagen Beetle History 59 Pags en InglesDocument59 pagesThe Best Visual Volkswagen Beetle History 59 Pags en IngleskrustigrusNo ratings yet
- LMOP Item CardsDocument8 pagesLMOP Item CardschrisNo ratings yet
- Sacred Oath: Oath of The Vampire LordDocument2 pagesSacred Oath: Oath of The Vampire LordTyler Davis100% (2)
- Macrocycle I 2014-15 PDFDocument18 pagesMacrocycle I 2014-15 PDFРадић СтефанNo ratings yet
- Hoist Drum Assy 4100XPCDocument3 pagesHoist Drum Assy 4100XPCFrancisco GonzalezNo ratings yet
- Measure Lower Extremity Function LEFSDocument2 pagesMeasure Lower Extremity Function LEFSonutza_onaNo ratings yet
- Measure Fall RiskDocument10 pagesMeasure Fall RiskAlvaro FernandoNo ratings yet
- Treinamento Sensório MotorDocument8 pagesTreinamento Sensório MotorDébora SouzaNo ratings yet
- Sympathetic Blockade For Complex Regional Pain SyndromeDocument2 pagesSympathetic Blockade For Complex Regional Pain SyndromeAlvaro FernandoNo ratings yet
- Paper 16Document6 pagesPaper 16Alvaro FernandoNo ratings yet
- Cold Hypersensitivity Increases With Age in Mice With Sickle Cell DiseaseDocument10 pagesCold Hypersensitivity Increases With Age in Mice With Sickle Cell DiseaseAlvaro FernandoNo ratings yet
- Stress Breath Fascia PHDocument7 pagesStress Breath Fascia PHAlvaro FernandoNo ratings yet
- Ot and Driving Assessment AustraliaDocument5 pagesOt and Driving Assessment AustraliaAlvaro FernandoNo ratings yet
- Energy Research & Social Science: Yael Parag, Kathryn B. JandaDocument11 pagesEnergy Research & Social Science: Yael Parag, Kathryn B. JandaAlvaro FernandoNo ratings yet
- 1 s2.0 S0304395914004758 MainDocument8 pages1 s2.0 S0304395914004758 MainAlvaro FernandoNo ratings yet
- Conditioned Pain Modulation and Offset Analgesia: Different Avenues To Inhibit PainDocument2 pagesConditioned Pain Modulation and Offset Analgesia: Different Avenues To Inhibit PainAlvaro FernandoNo ratings yet
- 1 s2.0 S0304395914004485 MainDocument13 pages1 s2.0 S0304395914004485 MainAlvaro FernandoNo ratings yet
- Rehab For CopdDocument12 pagesRehab For CopdAlvaro FernandoNo ratings yet
- A Mechanism-Based Classification of Phantom Limb Pain: Sarah C. Griffin, Jack W. TsaoDocument7 pagesA Mechanism-Based Classification of Phantom Limb Pain: Sarah C. Griffin, Jack W. TsaoAlvaro FernandoNo ratings yet
- 1 s2.0 S0894113006000949 MainDocument10 pages1 s2.0 S0894113006000949 MainAlvaro FernandoNo ratings yet
- CH 01Document5 pagesCH 01Alvaro FernandoNo ratings yet
- Effect of Dual-Task Training (Fixed Priority-Versus-Variable Priority) For Improving Balance in Older AdultsDocument5 pagesEffect of Dual-Task Training (Fixed Priority-Versus-Variable Priority) For Improving Balance in Older AdultsAlvaro FernandoNo ratings yet
- Fall Prevention ProgrammeDocument7 pagesFall Prevention ProgrammeAlvaro FernandoNo ratings yet
- Journal of Science and Medicine in SportDocument6 pagesJournal of Science and Medicine in SportAlvaro FernandoNo ratings yet
- Journal of Science and Medicine in SportDocument6 pagesJournal of Science and Medicine in SportAlvaro FernandoNo ratings yet
- Dual-Task Gait Interference in Early Parkinson's DiseaseDocument12 pagesDual-Task Gait Interference in Early Parkinson's DiseaseAlvaro FernandoNo ratings yet
- Journal of Science and Medicine in SportDocument6 pagesJournal of Science and Medicine in SportAlvaro FernandoNo ratings yet
- A Prototype of An Adjustable Table and An Adjustable Chair For SchoolsDocument15 pagesA Prototype of An Adjustable Table and An Adjustable Chair For SchoolsAlvaro FernandoNo ratings yet
- Dual task constraints influence walking and bimanual coordination in childrenDocument5 pagesDual task constraints influence walking and bimanual coordination in childrenAlvaro FernandoNo ratings yet
- International Journal of Industrial Ergonomics: M.G. Mohamed Thariq, H.P. Munasinghe, J.D. AbeysekaraDocument11 pagesInternational Journal of Industrial Ergonomics: M.G. Mohamed Thariq, H.P. Munasinghe, J.D. AbeysekaraAlvaro FernandoNo ratings yet
- Dual-Task Decrements in Elderly JGMS Dec 2008Document9 pagesDual-Task Decrements in Elderly JGMS Dec 2008Alvaro FernandoNo ratings yet
- Trek Volunteer Info Packet 2015Document6 pagesTrek Volunteer Info Packet 2015api-275865446No ratings yet
- Manual VW Caribe, Rabbit, Golf mk1Document137 pagesManual VW Caribe, Rabbit, Golf mk1Oscar Zendejas82% (11)
- 1988 Autoweek Turin Motor ShowDocument6 pages1988 Autoweek Turin Motor ShowAutoweekUSA100% (1)
- E2876Document3 pagesE2876criveraNo ratings yet
- ParticipantsDocument3 pagesParticipantsLgie LMNo ratings yet
- 2021-22 CIPS Exam Sessions V3.0 FINALDocument1 page2021-22 CIPS Exam Sessions V3.0 FINALTimothy Manyungwa IsraelNo ratings yet
- Instruction Sheet RevisedDocument4 pagesInstruction Sheet RevisedHNo ratings yet
- Nexgen Fabrics Catalogue-2Document62 pagesNexgen Fabrics Catalogue-2Bala VishnuNo ratings yet
- MATERIAL BALANCE TITLEDocument46 pagesMATERIAL BALANCE TITLEG Vamsee KrishnaNo ratings yet
- Physical Education Lesson PlanDocument2 pagesPhysical Education Lesson Plananon_862061355No ratings yet
- Mystery of The Invisible ThiefDocument53 pagesMystery of The Invisible ThiefNikhil Pramod67% (6)
- Rule Book: The Supremacy of Cavalry in The Crusader Era 11th-12th CenturyDocument16 pagesRule Book: The Supremacy of Cavalry in The Crusader Era 11th-12th CenturyDWSNo ratings yet
- Custom Car May 2023Document70 pagesCustom Car May 2023turricanNo ratings yet
- Reviewers For Pe MidtermDocument7 pagesReviewers For Pe MidtermJuzelle BañezNo ratings yet
- Directions Prepositions and Maps Worksheet - 86591Document1 pageDirections Prepositions and Maps Worksheet - 86591Jahayra Céspedes Uceda100% (2)
- Strainer Simple Mod. 72 - 10-18 - 125#Document1 pageStrainer Simple Mod. 72 - 10-18 - 125#Francisco Xavier Geronimo GarciaNo ratings yet
- A10vo28 - 1548Document2 pagesA10vo28 - 1548евгений летецкийNo ratings yet
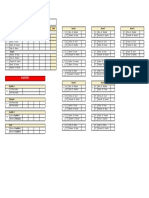
- Badminton FixturesDocument1 pageBadminton FixturesRahulSekharNo ratings yet
- British Expression DictionaryDocument143 pagesBritish Expression DictionarySantoshNo ratings yet