You might also like
- Reyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MDocument50 pagesReyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MGeraldine Marie Salvo100% (1)
- Steps To Private Placement Programs (PPP) DeskDocument7 pagesSteps To Private Placement Programs (PPP) DeskPattasan U100% (1)
- Embedded CoderDocument8 pagesEmbedded Coderجمال طيبيNo ratings yet
- Safety in Manufacturing: Ergonomics: Awkward PosturesDocument2 pagesSafety in Manufacturing: Ergonomics: Awkward PosturesprashanthNo ratings yet
- Construction of Dormitory & Housing compounds in NorochcholaiDocument33 pagesConstruction of Dormitory & Housing compounds in Norochcholaisaranga100% (1)
- MCQs on Defence Audit Code Chapter 9 and 10Document2 pagesMCQs on Defence Audit Code Chapter 9 and 10Rustam SalamNo ratings yet
- CIS2103-202220-Group Project - FinalDocument13 pagesCIS2103-202220-Group Project - FinalMd. HedaitullahNo ratings yet
- Observational Study DesignDocument45 pagesObservational Study DesignIfanda Ibnu HidayatNo ratings yet
- ICT FX4Model FrameworkDocument20 pagesICT FX4Model FrameworkSnowNo ratings yet
- Binary Data Biostatistics QuizDocument6 pagesBinary Data Biostatistics QuizTilak Venkatesh100% (3)
- Epidemiology ReviewDocument10 pagesEpidemiology ReviewSaurabhNo ratings yet
- Lo Per Amide Therapy For Acute Diarrhea in Children Systematic Review and Meta-AnalysisDocument11 pagesLo Per Amide Therapy For Acute Diarrhea in Children Systematic Review and Meta-AnalysisAprilia R. PermatasariNo ratings yet
- Summ 1619Document8 pagesSumm 1619novialbarNo ratings yet
- Cochrane BVS: Oral Zinc For Treating Diarrhoea in ChildrenDocument25 pagesCochrane BVS: Oral Zinc For Treating Diarrhoea in ChildrenLaura AnguloNo ratings yet
- Mesalamine Dosing Tor Ulcerative Colitis Remission MaintenanceDocument11 pagesMesalamine Dosing Tor Ulcerative Colitis Remission MaintenanceIasa FebrianusNo ratings yet
- Downloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Document28 pagesDownloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Indah Putri permatasariNo ratings yet
- Benefit and Risk of OHA Compared To Insulin in Women With GDMDocument13 pagesBenefit and Risk of OHA Compared To Insulin in Women With GDMNoraNo ratings yet
- HAI Guidelines 2010Document21 pagesHAI Guidelines 2010Mario Suarez MontalvoNo ratings yet
- Jurnal Cbe 1Document21 pagesJurnal Cbe 1Dewi SurayaNo ratings yet
- 673 FullDocument7 pages673 FullAq IfahNo ratings yet
- Chibamebaby@noccd - Edu: Pylorin Is Effective For Patients Afflicted With Dyspepsia. It Is Hypothesized That ThoseDocument8 pagesChibamebaby@noccd - Edu: Pylorin Is Effective For Patients Afflicted With Dyspepsia. It Is Hypothesized That Thoseapi-285705026No ratings yet
- Interventions For Preventing Gestational Diabetes Mellitus: A Systematic Review and Meta-AnalysisDocument15 pagesInterventions For Preventing Gestational Diabetes Mellitus: A Systematic Review and Meta-AnalysisMax PowerNo ratings yet
- Management For Intussusception in Children (Review) : CochraneDocument4 pagesManagement For Intussusception in Children (Review) : CochranefkNo ratings yet
- The Safety of Proton Pump Inhibitors (Ppis) in Pregnancy: A Meta-AnalysisDocument5 pagesThe Safety of Proton Pump Inhibitors (Ppis) in Pregnancy: A Meta-AnalysisSilvia AryaniNo ratings yet
- Skrining GiziDocument7 pagesSkrining GiziifaNo ratings yet
- Eating Disorders Twice as Common in Adolescent Females with DiabetesDocument4 pagesEating Disorders Twice as Common in Adolescent Females with DiabetesWilliam PalandengNo ratings yet
- HamdDocument12 pagesHamdAldiola PerdanaNo ratings yet
- Animal-Derived Surfactants Versus Past and Current Synthetic Surfactants: Current StatusDocument33 pagesAnimal-Derived Surfactants Versus Past and Current Synthetic Surfactants: Current StatusSiska LesnussaNo ratings yet
- MSTF Guideline Bowel Cleansing Oct 2014Document18 pagesMSTF Guideline Bowel Cleansing Oct 2014CynthiaNo ratings yet
- Gestational Diabetes Literature ReviewDocument12 pagesGestational Diabetes Literature Reviewc5rfkq8n100% (1)
- Eating Disorders - Overview of Epidemiology, Clinical Features, and Diagnosis - UpToDateDocument39 pagesEating Disorders - Overview of Epidemiology, Clinical Features, and Diagnosis - UpToDateDylanNo ratings yet
- Blood Pressure, Serum Total Cholesterol and Contraceptive Pill Use in 17-Year-Old GirlsDocument5 pagesBlood Pressure, Serum Total Cholesterol and Contraceptive Pill Use in 17-Year-Old GirlsLucerito MartinezNo ratings yet
- Dokumen Tanpa JudulDocument10 pagesDokumen Tanpa JudulZakia AmeliaNo ratings yet
- Controlled Trial Lansoprazole For Children With Poorly Controlled Asthma: A RandomizedDocument4 pagesControlled Trial Lansoprazole For Children With Poorly Controlled Asthma: A RandomizedJames HollandNo ratings yet
- Fluid bolus increases mortality in children with severe febrile illness and impaired circulationDocument8 pagesFluid bolus increases mortality in children with severe febrile illness and impaired circulationVladimir BasurtoNo ratings yet
- Systematic Review of Probiotics For The Treatment of Community-Acquired Acute Diarrhea in ChildrenDocument8 pagesSystematic Review of Probiotics For The Treatment of Community-Acquired Acute Diarrhea in ChildrenSandraJSantosNo ratings yet
- 4713-7 8.16 Afzaninawati Suria YusofDocument5 pages4713-7 8.16 Afzaninawati Suria Yusof568563No ratings yet
- Ref 32 Impact Hiperglikemia Pada ALLDocument5 pagesRef 32 Impact Hiperglikemia Pada ALLmuarifNo ratings yet
- Nonpharmacologic Treatments For Childhood Constipation: Systematic ReviewDocument9 pagesNonpharmacologic Treatments For Childhood Constipation: Systematic ReviewSardito PhanNo ratings yet
- Systematic Review: Antacids, H - Receptor Antagonists, Prokinetics, Bismuth and Sucralfate Therapy For Non-Ulcer DyspepsiaDocument13 pagesSystematic Review: Antacids, H - Receptor Antagonists, Prokinetics, Bismuth and Sucralfate Therapy For Non-Ulcer DyspepsiaAaquib AmirNo ratings yet
- Articulo 1Document8 pagesArticulo 1Silvia CastellanosNo ratings yet
- The Effect of Prenatal Antidepressant Exposure On Neonatal Adaptation A Systematic Review and MetanalysisDocument16 pagesThe Effect of Prenatal Antidepressant Exposure On Neonatal Adaptation A Systematic Review and MetanalysisDantrsNo ratings yet
- A Trial of An Anamnesis Based Score Applied As A.95804Document8 pagesA Trial of An Anamnesis Based Score Applied As A.95804ANA BEATRIZ MUNOZ URRIBARRINo ratings yet
- Articulo 2Document4 pagesArticulo 2Jorge012No ratings yet
- (ARTIGO) ARCELUS, Et Al. - Prevalence of Eating Disorders Amongst Dancers. A Systemic Review and Meta-Analysis (2013) - PUBMEDDocument28 pages(ARTIGO) ARCELUS, Et Al. - Prevalence of Eating Disorders Amongst Dancers. A Systemic Review and Meta-Analysis (2013) - PUBMEDGuido BrustNo ratings yet
- 33 Prabu RamDocument5 pages33 Prabu RameditorijmrhsNo ratings yet
- Canan 2017Document9 pagesCanan 2017Ioana CristinaNo ratings yet
- Lichen PlanusDocument7 pagesLichen PlanusHania KhanNo ratings yet
- Fiber and HemmerhoidsDocument8 pagesFiber and HemmerhoidsHendry RamadhanNo ratings yet
- Gestational Diabetes Mellitus Update and Review of LiteratureDocument5 pagesGestational Diabetes Mellitus Update and Review of Literatureauhavmpif100% (1)
- Association Between Cholesterol IntakeDocument6 pagesAssociation Between Cholesterol IntakeMohammed OmarNo ratings yet
- Obesity Metabolic Syndrome and Insulin Dynamics After CranipharyngiomaDocument8 pagesObesity Metabolic Syndrome and Insulin Dynamics After CranipharyngiomaaandakuNo ratings yet
- Racial and Ethnic Disparities in Adherence To Glaucoma Follow-Up Visits in A County Hospital PopulationDocument7 pagesRacial and Ethnic Disparities in Adherence To Glaucoma Follow-Up Visits in A County Hospital PopulationScott MuNo ratings yet
- Gastrico Vs TranspiloricaDocument6 pagesGastrico Vs TranspiloricaMagali FloresNo ratings yet
- Fiber TreatmentDocument8 pagesFiber TreatmentLana AdilaNo ratings yet
- Clinical Medicine Insights: Ear, Nose, ThroatDocument5 pagesClinical Medicine Insights: Ear, Nose, ThroatagustinadianasariaguNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- NIH Public Access: Author ManuscriptDocument7 pagesNIH Public Access: Author ManuscriptAnca RaduNo ratings yet
- Health PhyscologyDocument4 pagesHealth PhyscologySera SazleenNo ratings yet
- Do Spermicides Containing Nonoxynol-9 Prevent Sexually Transmitted Infections: A Meta-AnalysisDocument4 pagesDo Spermicides Containing Nonoxynol-9 Prevent Sexually Transmitted Infections: A Meta-Analysisindah febrianiNo ratings yet
- Chapter 6 - Research MethodDocument15 pagesChapter 6 - Research MethodLalita A/P AnbarasenNo ratings yet
- Homeopathy Reduces Duration of Childhood DiarrheaDocument10 pagesHomeopathy Reduces Duration of Childhood DiarrheaKiran DalabanjanNo ratings yet
- Obat Off-LabelDocument7 pagesObat Off-LabelYulia AfrianiNo ratings yet
- Artigo 2Document8 pagesArtigo 2Willian HolandaNo ratings yet
- Aspirin Preeclampsia Prevention Draft Evidence ReviewDocument153 pagesAspirin Preeclampsia Prevention Draft Evidence ReviewUmair HasanNo ratings yet
- Rumination Syndrome in Children and Adolescents: A School Survey Assessing Prevalence and SymptomatologyDocument6 pagesRumination Syndrome in Children and Adolescents: A School Survey Assessing Prevalence and SymptomatologyryselNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- Post Herpetic NeuralgiaDocument44 pagesPost Herpetic NeuralgiaRia Puji PangestutiNo ratings yet
- Post Herpetic NeuralgiaDocument44 pagesPost Herpetic NeuralgiaRia Puji PangestutiNo ratings yet
- Ep171968 CR PDFDocument9 pagesEp171968 CR PDFaraahNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaaraahNo ratings yet
- Rise of Civilizations Commander Tier ListDocument3 pagesRise of Civilizations Commander Tier ListaraahNo ratings yet
- Acute CholecystitisDocument47 pagesAcute CholecystitisaraahNo ratings yet
- Metabolism of Carbohydrate 2012Document65 pagesMetabolism of Carbohydrate 2012helgaNo ratings yet
- Rise of Civilizations Commander Tier ListDocument3 pagesRise of Civilizations Commander Tier ListaraahNo ratings yet
- Sjrogen's SyndromeDocument2 pagesSjrogen's SyndromearaahNo ratings yet
- Kuliah BSK 2001 (Compatibility Mode)Document5 pagesKuliah BSK 2001 (Compatibility Mode)Immanuel HabeahanNo ratings yet
- Profile Analysis of Urethral Stones at Clinical Pathology LaboratoryDocument4 pagesProfile Analysis of Urethral Stones at Clinical Pathology LaboratoryNovita Anggun Permata SariNo ratings yet
- ReferencesDocument5 pagesReferencesaraahNo ratings yet
- Correlations Baru KDocument2 pagesCorrelations Baru KaraahNo ratings yet
- Occupational Hazards in Home Healthcare: Niosh H RDocument68 pagesOccupational Hazards in Home Healthcare: Niosh H RarintpuspitarestuNo ratings yet
- Occupational Hazards in Home Healthcare: Niosh H RDocument68 pagesOccupational Hazards in Home Healthcare: Niosh H RarintpuspitarestuNo ratings yet
- Poisoning of Promethazine: Dermal AbsorptonDocument2 pagesPoisoning of Promethazine: Dermal AbsorptonaraahNo ratings yet
- Skenario 1 Kelompok 8Document16 pagesSkenario 1 Kelompok 8araahNo ratings yet
- WHO classification of soft tissue tumours guideDocument10 pagesWHO classification of soft tissue tumours guidezakibonnie100% (1)
- US LiverDocument42 pagesUS LiveraraahNo ratings yet
- Aggression Self Control Pada Pasien Dengan: Efektifitas Senam Aerobic Low Impact Terhadap Resiko Perilaku KekerasanDocument9 pagesAggression Self Control Pada Pasien Dengan: Efektifitas Senam Aerobic Low Impact Terhadap Resiko Perilaku KekerasanaraahNo ratings yet
- GbmucoDocument4 pagesGbmucoaraahNo ratings yet
- Restore a Disk Image with ClonezillaDocument16 pagesRestore a Disk Image with ClonezillaVictor SantosNo ratings yet
- A Survey of The Advancing Use and Development of Machine Learning in Smart ManufacturingDocument32 pagesA Survey of The Advancing Use and Development of Machine Learning in Smart Manufacturingbeben_19No ratings yet
- Rubrics For Lab Report For PC1 Lab, PC2 Lab, CIC LabDocument4 pagesRubrics For Lab Report For PC1 Lab, PC2 Lab, CIC LabHunie PopNo ratings yet
- Analysis of Financial Ratios of Manufacturing CompaniesDocument61 pagesAnalysis of Financial Ratios of Manufacturing CompaniesNine ZetNo ratings yet
- Dani RodrikDocument12 pagesDani Rodrikprogramas4242No ratings yet
- Examples 5 PDFDocument2 pagesExamples 5 PDFskaderbe1No ratings yet
- Moi University: School of Business and EconomicsDocument5 pagesMoi University: School of Business and EconomicsMARION KERUBONo ratings yet
- G.R. No. 122039 May 31, 2000 VICENTE CALALAS, Petitioner, Court of Appeals, Eliza Jujeurche Sunga and Francisco Salva, RespondentsDocument56 pagesG.R. No. 122039 May 31, 2000 VICENTE CALALAS, Petitioner, Court of Appeals, Eliza Jujeurche Sunga and Francisco Salva, RespondentsJayson AbabaNo ratings yet
- Accor vs Airbnb: Business Models in Digital EconomyDocument4 pagesAccor vs Airbnb: Business Models in Digital EconomyAkash PayunNo ratings yet
- MatrikonOPC Server For Simulation Quick Start Guide PDFDocument2 pagesMatrikonOPC Server For Simulation Quick Start Guide PDFJorge Perez CastañedaNo ratings yet
- Medhat CVDocument2 pagesMedhat CVSemsem MakNo ratings yet
- AXIS Camera Station Installation and Migration Guide: User ManualDocument7 pagesAXIS Camera Station Installation and Migration Guide: User ManualCORAL ALONSONo ratings yet
- Nº SSR-1 NS-R-3 Draf R1 Site Evaluation For Nuclear Installations FRDocument33 pagesNº SSR-1 NS-R-3 Draf R1 Site Evaluation For Nuclear Installations FRdaniel addeNo ratings yet
- WebquestDocument3 pagesWebquestapi-501133650No ratings yet
- Chapter 6 Performance Review and Appraisal - ReproDocument22 pagesChapter 6 Performance Review and Appraisal - ReproPrecious SanchezNo ratings yet
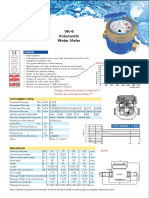
- Baylan: VK-6 Volumetric Water MeterDocument1 pageBaylan: VK-6 Volumetric Water MeterSanjeewa ChathurangaNo ratings yet
- SWOT Analysis of Fruit Juice BusinessDocument16 pagesSWOT Analysis of Fruit Juice BusinessMultiple UzersNo ratings yet
- SISU Datenblatt 7-ZylDocument2 pagesSISU Datenblatt 7-ZylMuhammad rizkiNo ratings yet
- Find The Minimal Sum of Products For The Boolean Expression F Using Quine-Mccluskey MethodDocument15 pagesFind The Minimal Sum of Products For The Boolean Expression F Using Quine-Mccluskey MethodSaira RasulNo ratings yet
- QA InspectionDocument4 pagesQA Inspectionapi-77180770No ratings yet
- The New Breed of Rally BDA: Motor SportDocument8 pagesThe New Breed of Rally BDA: Motor SportHarold MorleyNo ratings yet
- Opening A New Company in Bangladesh (FAQ)Document12 pagesOpening A New Company in Bangladesh (FAQ)nomanpur100% (1)
- Soal Pat Inggris 11Document56 pagesSoal Pat Inggris 11dodol garutNo ratings yet