You might also like
- Healthcare InteroperabilityDocument26 pagesHealthcare Interoperabilityarijit00No ratings yet
- Airfix 2011 CatalogueDocument132 pagesAirfix 2011 CatalogueGordon Sorensen0% (1)
- Construction of Dormitory & Housing compounds in NorochcholaiDocument33 pagesConstruction of Dormitory & Housing compounds in Norochcholaisaranga100% (1)
- Healthcare Management SystemDocument66 pagesHealthcare Management Systemmanikmathi100% (1)
- Design and Development of Online Hospital Management Information SystemDocument10 pagesDesign and Development of Online Hospital Management Information SystemRula ShakrahNo ratings yet
- Group Proj III Swot AnalysisDocument9 pagesGroup Proj III Swot Analysisapi-435685106No ratings yet
- The Road To Digital Success in Pharma - McKinsey & CompanyDocument10 pagesThe Road To Digital Success in Pharma - McKinsey & CompanyharshalNo ratings yet
- Healthcare and Hospital Industr1Document46 pagesHealthcare and Hospital Industr1Priya DarshiniNo ratings yet
- Accenture EMR Markets Whitepaper VfinalDocument16 pagesAccenture EMR Markets Whitepaper VfinalcapaxtremeNo ratings yet
- Health Analytics PWCDocument40 pagesHealth Analytics PWCsandeep_prasad17No ratings yet
- Soil Nailing and Rock Anchors ExplainedDocument21 pagesSoil Nailing and Rock Anchors ExplainedMark Anthony Agnes AmoresNo ratings yet
- Electronic Health Record EHR Data Modernizing The Pharmaceutical Research ProcessDocument12 pagesElectronic Health Record EHR Data Modernizing The Pharmaceutical Research ProcessHainah Kariza LeusNo ratings yet
- Big Data Is The Future of Healthcare PDFDocument7 pagesBig Data Is The Future of Healthcare PDFPratap Kumar DheergasiNo ratings yet
- Smart HospitalDocument223 pagesSmart Hospitalevi.setianingsihNo ratings yet
- Group 3 - Healthcare IndustryDocument13 pagesGroup 3 - Healthcare IndustryPeuli DasNo ratings yet
- Big Data in HealthcareDocument15 pagesBig Data in HealthcaresandeeNo ratings yet
- Blockchain Techonology in Healthcare Mangement SystemDocument7 pagesBlockchain Techonology in Healthcare Mangement Systemsmileytej eswarNo ratings yet
- Wearable Health Systems: From Smart Technologies To Real ApplicationsDocument4 pagesWearable Health Systems: From Smart Technologies To Real ApplicationsAbhishek SivaramanNo ratings yet
- Planning Hospitals of The FutureDocument24 pagesPlanning Hospitals of The FutureutkNo ratings yet
- Hype Cycle For Telemedicine and Virtual Care, 2016: Published: 6 July 2016Document52 pagesHype Cycle For Telemedicine and Virtual Care, 2016: Published: 6 July 2016cloudetdelgadoNo ratings yet
- From Big Data To MyhealthDocument46 pagesFrom Big Data To MyhealthHotnCrispy Crispy100% (1)
- M.Sc. DissertationDocument78 pagesM.Sc. DissertationJIMOH ADAMS LUKMANNo ratings yet
- A Review of The Literature On Big Data Analytics in Healthcare PDFDocument20 pagesA Review of The Literature On Big Data Analytics in Healthcare PDFCarlitos PilonietaNo ratings yet
- Data Visualization in Healthcare A Complete Guide - 2019 EditionFrom EverandData Visualization in Healthcare A Complete Guide - 2019 EditionNo ratings yet
- Cloud Computing in HealthcareDocument7 pagesCloud Computing in HealthcareTAN SHEE NEE STUDENTNo ratings yet
- Balance Scorecard - PPT IIIDocument25 pagesBalance Scorecard - PPT IIINeeraj SharmaNo ratings yet
- Cortana Analytics in Healthcare White PaperDocument16 pagesCortana Analytics in Healthcare White PaperDeyverson Costa100% (1)
- Health 2.0: Health For All, Health by AllDocument4 pagesHealth 2.0: Health For All, Health by AllkatejongbloedNo ratings yet
- The Digital HospitalDocument23 pagesThe Digital HospitalJihad Elias ChahlaNo ratings yet
- The Big Unlock: Harnessing Data and Growing Digital Health Businesses in a Value-Based Care EraFrom EverandThe Big Unlock: Harnessing Data and Growing Digital Health Businesses in a Value-Based Care EraNo ratings yet
- Trends in Telehealth White PaperDocument16 pagesTrends in Telehealth White PaperGalih Permana Qisty100% (1)
- BIM and AM to digitally transform critical water utility assetsDocument20 pagesBIM and AM to digitally transform critical water utility assetsJUAN EYAEL MEDRANO CARRILONo ratings yet
- Pesut Facilitator Using Liberating Structures 1 Slide Per PageDocument35 pagesPesut Facilitator Using Liberating Structures 1 Slide Per PageMohd OtibiNo ratings yet
- Raghupathi-Raghupathi2014 Article BigDataAnalyticsInHealthcarePr PDFDocument10 pagesRaghupathi-Raghupathi2014 Article BigDataAnalyticsInHealthcarePr PDFCristian ZapataNo ratings yet
- Computational Health Informatics in The Big Data Age - A SurveyDocument36 pagesComputational Health Informatics in The Big Data Age - A SurveymuhammadrizNo ratings yet
- Name: Prachi Das Enrolment Number: 20BSP1623 Section: ADocument3 pagesName: Prachi Das Enrolment Number: 20BSP1623 Section: AASHUTOSH KUMAR SINGHNo ratings yet
- Adoption of BI in SMEs PDFDocument22 pagesAdoption of BI in SMEs PDFmaheshNo ratings yet
- Getting Real With Real-World EvidenceDocument19 pagesGetting Real With Real-World EvidencedajcNo ratings yet
- A Study of Advanced Hospital Managaement System: Kumaran S, DR Pusphagaran, Kalai Selvi, Christopher, DeepakDocument8 pagesA Study of Advanced Hospital Managaement System: Kumaran S, DR Pusphagaran, Kalai Selvi, Christopher, Deepakrohising2045No ratings yet
- Real-World Evidence: A Better Life Journey For Pharmas, Payers and PatientsDocument5 pagesReal-World Evidence: A Better Life Journey For Pharmas, Payers and PatientsCognizantNo ratings yet
- Telehealth: Review and Perspectives For SingaporeDocument33 pagesTelehealth: Review and Perspectives For Singaporesuhangmydoc100% (1)
- Utilizing Big DataDocument5 pagesUtilizing Big DataFarheen AhmedNo ratings yet
- Case Study On InnovaccerDocument3 pagesCase Study On InnovaccerAmarnath DixitNo ratings yet
- The Digital Transformation of HealthcareDocument10 pagesThe Digital Transformation of HealthcarewiameNo ratings yet
- Green Hospital Health System SeminarDocument7 pagesGreen Hospital Health System SeminarLaksamana KoetaradjaNo ratings yet
- Healthcare Information System Fortis Hospital Case StudyDocument4 pagesHealthcare Information System Fortis Hospital Case StudySateesh MoreNo ratings yet
- Role of Big Data in Disaster ManagementDocument2 pagesRole of Big Data in Disaster Managementabhinav prakashNo ratings yet
- Bumrungrad's Global Marketing StrategyDocument6 pagesBumrungrad's Global Marketing StrategyMaiAsisNo ratings yet
- Summary Mobile HealthDocument31 pagesSummary Mobile HealthmhemaraNo ratings yet
- A Preliminary Literature Review of Digital Transformation Case StudiesDocument6 pagesA Preliminary Literature Review of Digital Transformation Case StudiesLucija IvancicNo ratings yet
- Healthcare Information SystemDocument9 pagesHealthcare Information SystemcbjdcbsjdNo ratings yet
- Business Intelligence in Health Care IndustryDocument2 pagesBusiness Intelligence in Health Care IndustrysasiarchieNo ratings yet
- Iot in M-Health - FinalDocument27 pagesIot in M-Health - FinalPascal TagneNo ratings yet
- Business Intelligence Tools ComparisonDocument10 pagesBusiness Intelligence Tools ComparisonAbner AugustoNo ratings yet
- FINTECHDocument3 pagesFINTECHNurul AqilahNo ratings yet
- Blockchain For The Cybersecurity of Smart CityDocument66 pagesBlockchain For The Cybersecurity of Smart CityGiovanni PintoNo ratings yet
- An Automated Medical Duties Scheduling System Using Queing Techniques (Chapter 1-5)Document19 pagesAn Automated Medical Duties Scheduling System Using Queing Techniques (Chapter 1-5)ABUBSAKAR SIDIQ AMINUNo ratings yet
- Sustainable Supply Chains A Study of Interaction Among The EnablersDocument23 pagesSustainable Supply Chains A Study of Interaction Among The Enablerswinky5050No ratings yet
- Smart HospitalsDocument57 pagesSmart HospitalsPratik P PatelNo ratings yet
- VodafoneDocument28 pagesVodafoneNavaneet Yadav100% (1)
- Planning An EMR ImplemetationDocument5 pagesPlanning An EMR ImplemetationShruti CholaNo ratings yet
- Big Data in Healthcare Management: A Review of Literature: American Journal of Theoretical and Applied BusinessDocument13 pagesBig Data in Healthcare Management: A Review of Literature: American Journal of Theoretical and Applied BusinessCésar AparicioNo ratings yet
- Big Data Analytics in Cloud Computing For Scientific AnalyticsDocument7 pagesBig Data Analytics in Cloud Computing For Scientific AnalyticsIJRASETPublicationsNo ratings yet
- 1030 Sky-U-Mah Project 3 & 7 Measuring Nursing HandoutDocument9 pages1030 Sky-U-Mah Project 3 & 7 Measuring Nursing HandoutMohd OtibiNo ratings yet
- 930 Sky-U-Mah Project 10 Transform Documentation and Context of Care PosterDocument1 page930 Sky-U-Mah Project 10 Transform Documentation and Context of Care PosterMohd OtibiNo ratings yet
- 930 MN Room Nursing Data Standards HandoutDocument3 pages930 MN Room Nursing Data Standards HandoutMohd OtibiNo ratings yet
- 930 Johnson Project 6 Education PosterDocument1 page930 Johnson Project 6 Education PosterMohd OtibiNo ratings yet
- 930 Johnson Education Certification Accreditation HandoutDocument5 pages930 Johnson Education Certification Accreditation HandoutMohd OtibiNo ratings yet
- 930 Johnson Project 1 Certification PosterDocument1 page930 Johnson Project 1 Certification PosterMohd OtibiNo ratings yet
- PHD Tips 5 Tips For Finding A Dissertation TopicDocument5 pagesPHD Tips 5 Tips For Finding A Dissertation TopicMohd OtibiNo ratings yet
- Effective LeadershipDocument200 pagesEffective LeadershipMohd Otibi100% (1)
- PHD Tips 5 Tips For Finding A Dissertation TopicDocument5 pagesPHD Tips 5 Tips For Finding A Dissertation TopicMohd OtibiNo ratings yet
- Capital Asset Pricing ModelDocument11 pagesCapital Asset Pricing ModelrichaNo ratings yet
- Hydraulic-Fracture Design: Optimization Under Uncertainty: Risk AnalysisDocument4 pagesHydraulic-Fracture Design: Optimization Under Uncertainty: Risk Analysisoppai.gaijinNo ratings yet
- Break-Even Analysis: Margin of SafetyDocument2 pagesBreak-Even Analysis: Margin of SafetyNiño Rey LopezNo ratings yet
- Final Year Project A Report Assessment Form (10%)Document5 pagesFinal Year Project A Report Assessment Form (10%)Chong Ru YinNo ratings yet
- SolidEdge MachineryLibrary V15.00Document139 pagesSolidEdge MachineryLibrary V15.00ttNo ratings yet
- Grand Viva Question For Ece StudentDocument17 pagesGrand Viva Question For Ece Studentapi-35904739086% (7)
- Microprocessor Based Systems: by Nasir Mahmood Nasir - Mahmood@seecs - Edu.pkDocument15 pagesMicroprocessor Based Systems: by Nasir Mahmood Nasir - Mahmood@seecs - Edu.pkMuhammad ZubairNo ratings yet
- Newcomb Theodore MDocument20 pagesNewcomb Theodore MBang Ahmad UstuhriNo ratings yet
- 2014 Chevrolet Cruze maintenance schedule guideDocument2 pages2014 Chevrolet Cruze maintenance schedule guidericardo rodriguezNo ratings yet
- Chapter 6 Performance Review and Appraisal - ReproDocument22 pagesChapter 6 Performance Review and Appraisal - ReproPrecious SanchezNo ratings yet
- Screenshot 2021-10-02 at 12.22.29 PMDocument1 pageScreenshot 2021-10-02 at 12.22.29 PMSimran SainiNo ratings yet
- Cold Fear manual_englishDocument10 pagesCold Fear manual_englishHelmi IsmunandarNo ratings yet
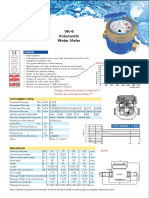
- Baylan: VK-6 Volumetric Water MeterDocument1 pageBaylan: VK-6 Volumetric Water MeterSanjeewa ChathurangaNo ratings yet
- Ibad Rehman CV NewDocument4 pagesIbad Rehman CV NewAnonymous ECcVsLNo ratings yet
- Earth Planet - Google SearchDocument1 pageEarth Planet - Google SearchDaivik Lakkol Eswara PrasadNo ratings yet
- Power Efficiency Diagnostics ReportDocument16 pagesPower Efficiency Diagnostics Reportranscrib300No ratings yet
- CRM Chapter 3 Builds Customer RelationshipsDocument45 pagesCRM Chapter 3 Builds Customer RelationshipsPriya Datta100% (1)
- JAM 2020 Information Brochure: Admission to M.Sc., Joint M.Sc.-Ph.D., M.Sc.-Ph.D. Dual Degree and Integrated Ph.D. ProgrammesDocument51 pagesJAM 2020 Information Brochure: Admission to M.Sc., Joint M.Sc.-Ph.D., M.Sc.-Ph.D. Dual Degree and Integrated Ph.D. ProgrammesVaibhav PachauleeNo ratings yet
- Key Payment For Japan EcomercesDocument9 pagesKey Payment For Japan EcomercesChoo YieNo ratings yet
- FINC 301 MQsDocument40 pagesFINC 301 MQsMichael KutiNo ratings yet
- Unit 4 Probability AssignmentsDocument8 pagesUnit 4 Probability AssignmentsSumycheen BhusalNo ratings yet
- Infineon ICE3BXX65J DS v02 - 09 en PDFDocument28 pagesInfineon ICE3BXX65J DS v02 - 09 en PDFcadizmabNo ratings yet
- GFRDDocument9 pagesGFRDLalit NagarNo ratings yet
- Application For Freshman Admission - PDF UA & PDocument4 pagesApplication For Freshman Admission - PDF UA & PVanezza June DuranNo ratings yet
- Naoh Storage Tank Design Description:: Calculations For Tank VolumeDocument6 pagesNaoh Storage Tank Design Description:: Calculations For Tank VolumeMaria Eloisa Angelie ArellanoNo ratings yet
- Dr Nael Qtati's E-Commerce Business Models Week 1 CourseDocument28 pagesDr Nael Qtati's E-Commerce Business Models Week 1 CourseMohammed LubbadNo ratings yet