You might also like
- 17oncology1 Growth Disturbances TextsDocument28 pages17oncology1 Growth Disturbances TextsDrDeepak PawarNo ratings yet
- List of FiguresDocument2 pagesList of FiguresDrDeepak PawarNo ratings yet
- Data Collection FormDocument2 pagesData Collection FormDrDeepak PawarNo ratings yet
- Tables and GraphsDocument17 pagesTables and GraphsDrDeepak PawarNo ratings yet
- Methodology DMDocument3 pagesMethodology DMDrDeepak PawarNo ratings yet
- DM Conclusion 222Document2 pagesDM Conclusion 222DrDeepak PawarNo ratings yet
- Results and DiscussionDocument5 pagesResults and DiscussionDrDeepak PawarNo ratings yet
- List of FiguresDocument2 pagesList of FiguresDrDeepak PawarNo ratings yet
- Review LiteratureDocument23 pagesReview LiteratureDrDeepak Pawar50% (4)
- 7-Steps For DI Systematic ApproachDocument8 pages7-Steps For DI Systematic ApproachDrDeepak Pawar71% (7)
- INTRODUCTIONDocument5 pagesINTRODUCTIONDrDeepak PawarNo ratings yet
- Assessing Diabetes AwarenessDocument7 pagesAssessing Diabetes AwarenessDrDeepak PawarNo ratings yet
- 01 M006 36157Document12 pages01 M006 36157DrDeepak PawarNo ratings yet
- ACRONYMSDocument2 pagesACRONYMSDrDeepak PawarNo ratings yet
- Oligo Research Article PDFDocument4 pagesOligo Research Article PDFDrDeepak PawarNo ratings yet
- 01 M039 43754Document16 pages01 M039 43754DrDeepak PawarNo ratings yet
- Chapter 3 Aim and ObjectivesDocument1 pageChapter 3 Aim and ObjectivesDrDeepak PawarNo ratings yet
- Introduction to Toxicology Concepts and UnitsDocument40 pagesIntroduction to Toxicology Concepts and UnitsFauzan FasnidNo ratings yet
- Antibiotics For Upper Respiratory Tract Infections: Follow-Up Utilization and Antibiotic UseDocument5 pagesAntibiotics For Upper Respiratory Tract Infections: Follow-Up Utilization and Antibiotic UseDrDeepak PawarNo ratings yet
- Lower Respiratory Tract Infections SeminarDocument45 pagesLower Respiratory Tract Infections SeminarDrDeepak PawarNo ratings yet
- Barbiturate PoisoningDocument3 pagesBarbiturate PoisoningDrDeepak PawarNo ratings yet
- A Seminar On Lower Respiratory Tract Infections: Click To Edit Master Subtitle StyleDocument44 pagesA Seminar On Lower Respiratory Tract Infections: Click To Edit Master Subtitle StyleDrDeepak PawarNo ratings yet
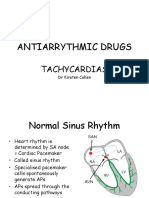
- Antiarrythmic Drugs: TachycardiasDocument36 pagesAntiarrythmic Drugs: TachycardiasDrDeepak PawarNo ratings yet
- Typhoid Fever AND Paratyphoid Fever: Guoli Lin Department of Infectious Diseases The Third Affiliated Hospital of SYSUDocument70 pagesTyphoid Fever AND Paratyphoid Fever: Guoli Lin Department of Infectious Diseases The Third Affiliated Hospital of SYSUDrDeepak PawarNo ratings yet
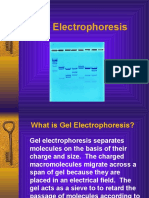
- GelelctroDocument11 pagesGelelctroDrDeepak PawarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Historic Costume: (Early 15 Century) 1400-1500 European FashionDocument33 pagesHistoric Costume: (Early 15 Century) 1400-1500 European FashionRaina varshneyNo ratings yet
- Who Would Think That Love - LyricDocument1 pageWho Would Think That Love - LyricNatália RamosNo ratings yet
- Explosion Proof ClassificationsDocument2 pagesExplosion Proof Classificationsneurolepsia3790No ratings yet
- Jamel P. Mateo, Mos, LPTDocument7 pagesJamel P. Mateo, Mos, LPTmarieieiemNo ratings yet
- Poe. Ligeia PDFDocument12 pagesPoe. Ligeia PDFClaudia Henríquez FaríasNo ratings yet
- Software Customisation Reference ManualDocument269 pagesSoftware Customisation Reference ManualTonthat QuangNo ratings yet
- BMM Cements LTD., Bharat Mines & Minerals, Gudipadu Cement Plant, GudipaduDocument2 pagesBMM Cements LTD., Bharat Mines & Minerals, Gudipadu Cement Plant, GudipaduDeepak Kumar PalNo ratings yet
- ACEE 7: Logic Circuits and Switching Theory: Logic Circuit Design On NI MultisimDocument7 pagesACEE 7: Logic Circuits and Switching Theory: Logic Circuit Design On NI MultisimJaypee100% (1)
- Consultancy Project Assessment SheetDocument1 pageConsultancy Project Assessment SheetSadeeqNo ratings yet
- Neuroplasticity: The Brain's Ability to Change Throughout LifeDocument11 pagesNeuroplasticity: The Brain's Ability to Change Throughout LifeANo ratings yet
- HNI Corporation 2020 Annual Report Highlights Growth StrategyDocument84 pagesHNI Corporation 2020 Annual Report Highlights Growth StrategyRainy DaysNo ratings yet
- Dream Wiebe - ResumeDocument1 pageDream Wiebe - Resumeapi-693810430No ratings yet
- Double Your Income-Hustle & ConquerDocument54 pagesDouble Your Income-Hustle & ConquerHamza ElmoubarikNo ratings yet
- Data Sheets DW Instrumentation 1590398977404Document39 pagesData Sheets DW Instrumentation 1590398977404leonardseniorNo ratings yet
- Project ReportDocument61 pagesProject Reportlove goyal100% (2)
- DCV 03 hk66t102Document15 pagesDCV 03 hk66t102seaqu3stNo ratings yet
- Java Interview Guide - 200+ Interview Questions and Answers (Video)Document5 pagesJava Interview Guide - 200+ Interview Questions and Answers (Video)Anand ReddyNo ratings yet
- African Nations Cup ProjectDocument15 pagesAfrican Nations Cup ProjectAgbor AyukNo ratings yet
- Customer No.: 22855256 IFSC Code: DBSS0IN0811 MICR Code: Branch AddressDocument9 pagesCustomer No.: 22855256 IFSC Code: DBSS0IN0811 MICR Code: Branch AddressBalakrishna SNo ratings yet
- A10 Thunder Series and AX Series: ACOS 2.7.2-P7-SP3 22 December 2015Document360 pagesA10 Thunder Series and AX Series: ACOS 2.7.2-P7-SP3 22 December 2015huonz mrNo ratings yet
- The Impact of Air Cooled Condensers On Plant Design and OperationsDocument12 pagesThe Impact of Air Cooled Condensers On Plant Design and Operationsandi_babyNo ratings yet
- In c1 20 Ex CteDocument7 pagesIn c1 20 Ex CteAlejandro HernándezNo ratings yet
- Philippine Duplicators 13th Month Pay ComputationDocument2 pagesPhilippine Duplicators 13th Month Pay ComputationDennis Jay Dencio ParasNo ratings yet
- Modulen 2 Newtons 2nd Law of Motion Upload 2 v2Document71 pagesModulen 2 Newtons 2nd Law of Motion Upload 2 v2Dyas FerNo ratings yet
- Process Control Lecture 9 (M2)Document53 pagesProcess Control Lecture 9 (M2)lalusebanNo ratings yet
- Strategic Supply Chain Management (Om367, 04835) : Meeting Time & LocationDocument9 pagesStrategic Supply Chain Management (Om367, 04835) : Meeting Time & Locationw;pjo2hNo ratings yet
- Socio-Economic and Government Impact On Business: Lesson 4.4Document18 pagesSocio-Economic and Government Impact On Business: Lesson 4.4racelNo ratings yet
- How to Write Formal IELTS LettersDocument5 pagesHow to Write Formal IELTS Lettersarif salmanNo ratings yet
- Section 9 - ProppantsDocument18 pagesSection 9 - ProppantsIllimination Illuminated MinisatanNo ratings yet
- The Kerdi Shower Book: John P. BridgeDocument7 pagesThe Kerdi Shower Book: John P. BridgeTima ShpilkerNo ratings yet