You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Leadership & Management - Assignment/Delegation Scope of PracticeDocument4 pagesLeadership & Management - Assignment/Delegation Scope of PracticeregisterednurseNo ratings yet
- Lecture On Patient SafetyDocument27 pagesLecture On Patient Safetyjvfaderon74No ratings yet
- File Thuyết TrìnhDocument3 pagesFile Thuyết TrìnhBích TuyềnNo ratings yet
- Training Needs AnalysisDocument1 pageTraining Needs AnalysisKayeNo ratings yet
- Concept Map Diagnosis and InterventionsDocument3 pagesConcept Map Diagnosis and Interventionsmenickel3No ratings yet
- Abigail Withers 2020 ResumeDocument1 pageAbigail Withers 2020 Resumeapi-363656404No ratings yet
- Dispenser Agreeement MpyaDocument3 pagesDispenser Agreeement MpyaMussa maguluko100% (3)
- The Role of CBT in Relapse Prevention of SchizophreniaDocument2 pagesThe Role of CBT in Relapse Prevention of SchizophreniaKorn IbraNo ratings yet
- School of Mount St. Mary, Inc.: Learning Module in Health 10Document25 pagesSchool of Mount St. Mary, Inc.: Learning Module in Health 10rom keroNo ratings yet
- Nursing Care For HiV Patients Facilitator Guide PDFDocument314 pagesNursing Care For HiV Patients Facilitator Guide PDFmalathiNo ratings yet
- Essential Falls Management Series: Managing Falls in Assisted Living (Tideiksaar Excerpt)Document11 pagesEssential Falls Management Series: Managing Falls in Assisted Living (Tideiksaar Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.No ratings yet
- Kaplan Cirugia No Cardiaca PDFDocument584 pagesKaplan Cirugia No Cardiaca PDFNalemi JTNo ratings yet
- Medical English - Than Lan Con English CentreDocument84 pagesMedical English - Than Lan Con English CentreTrần Văn TâmNo ratings yet
- Original PDF Mosbys Dental Drug Reference e Book 12th Edition PDFDocument41 pagesOriginal PDF Mosbys Dental Drug Reference e Book 12th Edition PDFarlene.wax700100% (33)
- SCENAR For Pain ReliefDocument6 pagesSCENAR For Pain ReliefDennis LipterNo ratings yet
- Work Setting of CounselorDocument3 pagesWork Setting of CounselorAngel Rose Sierda MedinaNo ratings yet
- Medicine EnglishDocument32 pagesMedicine EnglishSsetarehNo ratings yet
- AI in Healthcare GROUP4Document10 pagesAI in Healthcare GROUP4Sugandha Gajanan GhadiNo ratings yet
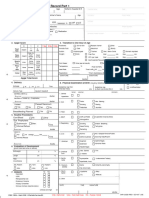
- Form1583A NewbornRecord1and2Document4 pagesForm1583A NewbornRecord1and2miguealliNo ratings yet
- Jadwal September NewDocument20 pagesJadwal September NewWiLly IsmailNo ratings yet
- First Aid Tra Ning: Certificate of Attendance Certificate of AttendanceDocument1 pageFirst Aid Tra Ning: Certificate of Attendance Certificate of AttendanceRichard CortezNo ratings yet
- Permintaan Obat Bulan April 2023Document8 pagesPermintaan Obat Bulan April 2023Putri Nurma SariNo ratings yet
- 2021 The Social Health Determinants of Health and Cancer FinalDocument17 pages2021 The Social Health Determinants of Health and Cancer FinalMilda InayahNo ratings yet
- Autism and Vaccination (Final)Document8 pagesAutism and Vaccination (Final)Rajan JattNo ratings yet
- Target Market Strategies for The Royal PharmacyDocument12 pagesTarget Market Strategies for The Royal PharmacyIsmail MustafaNo ratings yet
- List of 150 Pharmaceutical Companies With Their LocationsDocument9 pagesList of 150 Pharmaceutical Companies With Their LocationsHossain Mohammad Asif100% (1)
- LM Prasad Principles and Practice of Management PDF Free 664l PDFDocument4 pagesLM Prasad Principles and Practice of Management PDF Free 664l PDFBrittany20% (5)
- Clinical ExemplarDocument4 pagesClinical Exemplarapi-272451466No ratings yet
- BC prescription drug regulations summaryDocument2 pagesBC prescription drug regulations summaryRicky TsuiNo ratings yet
- AcronymsDocument153 pagesAcronymsDavid F. Duque G.No ratings yet