JMM Case Reports (2014)
Case Report
DOI 10.1099/jmmcr.0.000281
Community-acquired Pseudomonas aeruginosa
pneumonia in previously healthy patients
Shingo Tsuji,1 Takeshi Saraya,1 Yasutaka Tanaka,1 Hiroshi Makino,2
Shota Yonetani,2 Koji Araki,2 Daisuke Kurai,1 Haruyuki Ishii,1
Hajime Takizawa1 and Hajime Goto1
Correspondence
Department of Respiratory Medicine, Kyorin University School of Medicine, 6-20-2 Shinkawa,
Mitaka City, Tokyo, Japan
Department of Laboratory Medicine, Kyorin University School of Medicine, 6-20-2 Shinkawa,
Mitaka City, Tokyo, Japan
Takeshi Saraya
saraya@ks.kyorin-u.ac.jp
Introduction: Pseudomonas aeruginosa community-acquired pneumonia is an extremely rare
clinical presentation but has been recognized in anecdotal reports, even in previously healthy
patients.
Case presentation: We describe a previously healthy man who developed P. aeruginosa
community-acquired pneumonia (CAP). He died of septic shock with rapidly progressive
pulmonary consolidation in the right upper lobe (RUL). We reviewed the literature for P.
aeruginosa CAP and identified 19 patients of whom 85 % (n517) had cavitations and/or
consolidations in the RUL. We found that the odds ratio for death of shock at initial presentation
was 8.333 (P50.046, 95 % confidence interval 1.03467.142). We also found that P.
aeruginosa CAP should be considered when individuals present with rapidly expanding cavitary
pneumonia and/or consolidations in the RUL accompanied by septic shock, even if they have no
known severe underlying disease and were previously healthy.
Received 26 October 2013
Accepted 26 March 2014
Conclusion: We showed here that radiological findings of P. aeruginosa CAP, such as cavitary
pneumonia and/or consolidation in the RUL, might be a clinical clue to a diagnosis of CAP as well
as the presence of septic shock.
Keywords: Pseudomonas aeruginosa; cavity; community-acquired pneumonia; septic shock.
Introduction
Published studies have indicated that the incidence of
community-acquired pneumonia (CAP) caused by
Pseudomonas aeruginosa ranges from 0.4 % (Torres and
Menendez, 2010) to 5 % (Leroy et al., 1999) and that the
disease has a 30 % mortality rate (Hatchette et al., 2000).
These infections usually occur in patients with severe
underlying disease, and rarely in healthy individuals. Only
19 patients without any known severe underlying disease
have been reported in the literature since 1968. Here, we
describe a previously healthy man who developed P.
aeruginosa CAP and present a review of the literature.
Case report
A 61-year-old man was referred to our hospital with a
3 day history of productive cough and right chest pain. He
had felt well enough to work full time until the onset of
Abbreviations: CAP, community-acquired pneumonia; RUL, right upper
lobe.
symptoms but appeared ill upon presentation. He had
worked as an office worker for 40 years, and denied any
dust exposure or illicit drug use, or contact with sick
people. He had been administered with oral antihyperglycaemic agents to treat controllable type 2 diabetes
mellitus for over 15 years. His vital signs were as follows:
blood pressure, 104/66 mmHg; heart rate, 128 beats
min21; respiratory rate, 24 min21; body temperature,
38.7 uC; and 98 % oxygen saturation with ambient air,
suggesting systemic inflammatory response syndrome.
Physical findings were normal except for mildly decreased
respiratory sounds over the anterior aspect of the right
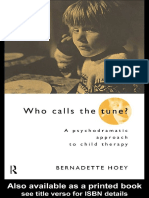
upper lung field. A chest X-ray showed a homogeneous
infiltrate in the right upper lobe (RUL) (Fig. 1a),
indicating CAP. Thoracic CT (Fig. 1b, c) taken on
admission showed consolidation with an air bronchogram
in the RUL together with ground-glass opacities. His
serum laboratory findings were as follows: normal white
blood cell count (8200 ml21) and remarkably elevated Creactive protein at 40.0 mg dl21. There was no detailed
medical history on admission, while haemoglobin A1c
Downloaded from www.microbiologyresearch.org by
G 2014 The Authors. Published by SGM
IP: 114.198.209.88
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0/).
On: Wed, 10 Feb 2016 22:41:23
S. Tsuji and others
(a)
(Fig. 2). Only five (25 %) of the cultures were positive for
P. aeruginosa in sputum, whereas 15 (75 %) sputum plus
blood cultures were positive, suggesting a high rate of
bacteraemia upon admission. Eight (40 %) of the patients
were in shock at initial presentation and seven of them had
P. aeruginosa bacteraemia. Univariate analysis identified
septic shock at initial presentation (odds ratio, 8.333; 95 %
confidence interval, 1.03467.142; P50.046), but not
inappropriate initial antimicrobial therapy (50 %, n510),
as a significant factor for mortality. Importantly, the RUL
was involved in 17 (85 %) patients with radiological
findings such as cavitations and/or consolidations.
(b)
(c)
Fig. 1. Chest X-ray (a) showing massive infiltration in the right
upper lung field, and thoracic CT taken on admission (b, c)
showing consolidation with an air bronchogram accompanied by
ground-glass opacities in the RUL.
levels showed only a mild elevation (7.2 %). This might
indicate moderately controlled hyperglycaemia (Nathan et
al., 2008). Sputum Gram staining showed a dominant
Gram-negative bacillus with other bacteria, and these
results were scored as Geckler classification 3. Thus, no
apparent pathogens were identified at that time. Based on
the data, we immediately treated him with ampicillin/
sulbactam (9 g day21) upon admission, but he went into
shock 7 h later and required aggressive treatment including
intubation. In addition, increased serum procalcitonin
(71.8 ng ml21) and endotoxin (179.9 pg ml21) were
found, suggesting that he was in septic shock. At that
time, the treatment was immediately changed to doripenem hydrate (0.75 g day21). Thereafter, P. aeruginosa grew
in both sputum and blood cultures on day 2 after hospital
admission (hospital day 2). All isolates of P. aeruginosa
were non-mucoid type and susceptible to commonly used
anti-pseudomonal b-lactam antibiotics. In addition, the
PFGE profiles suggested that these isolates were identical
(see Fig. S1 available in the online Supplementary
Material). On day 3, his general status rapidly deteriorated
and he died of septic shock.
Our review of the literature (Table 1) uncovered descriptions of P. aeruginosa CAP arising in 19 previously healthy
individuals, as well as the present patient. The ratio of
females to males in the total of 20 patients was 7 : 13 [age
(medianSD), 45.913.6 years]. The initial symptoms
were non-specific, but 15 (75 %), 14 (70 %) and 12
(60 %) of these patients presented with cough, pleuritic
pain and pyrexia, respectively. The duration from initial
onset to admission ranged from 1 to 30 days (median,
3 days), that from admission to intubation was within 24 h
and the mortality rate was 35 % (n57) over a range of 9
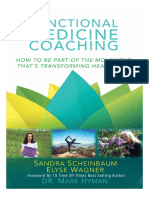
hospital days (median, 1.5 days). KaplanMeier analysis
confirmed a 61.1 % survival probability at hospital day 9
2
Discussion
Approximately 4 % of normal adults can harbour P.
aeruginosa in their pharynx or colon or on the skin (Rose
et al., 1983). Diabetic patients have impaired polymorphonuclear functions including chemotaxis, adherence, phagocytosis and intracellular killing, as well as T-lymphocyte
dysfunction (Gupta et al., 2007). This may induce the
propagation of pathogens including P. aeruginosa.
However, whether the presence of diabetes mellitus
influences the infection-related mortality and infection
itself is still under debate (Knapp, 2013). For example, a
multivariate analysis by Torres and Menendez (2010)
showed that independent predictors for CAP due to P.
aeruginosa included chronic respiratory disease and enteral
tube feeding but not diabetes mellitus, which supports the
findings of Pennington et al. (1973). The portal of entry for
P. aeruginosa septicaemia is always pneumonia (Ishihara et
al., 1995), and this is almost universally fatal (Baltch and
Griffin, 1977), as in our patient. Our search identified a
mortality rate of 35 %, which was similar to that of a
previous report (30 %) (Hatchette et al., 2000); we also
found that mortality was significantly associated with
having septic shock at the time of initial presentation (odds
ratio, 8.333). However, empirically appropriate therapy for
P. aeruginosa did not contribute to a favourable prognosis.
Based on these findings, we speculated that P. aeruginosa
CAP occurring in previously healthy persons typically
results in bacteraemia, which is sequentially followed by
septic shock irrespective of the use of appropriate antipseudomonal antibiotics. In accordance with this viewpoint, the increased serum endotoxin level in our patient
supported this hypothesis. Although various bacterial
factors such as surface components, the type III secretion
system, quorum sensing, and scavenging of iron and other
extracellular products has been reported (Sadikot et al.,
2005; Williams et al., 2010), it is possible that the large
amount of endotoxin derived from the pathogen led to
excessive inflammation and resulted in systemic inflammatory response syndrome in the present case.
Okada et al. (2012) recently concluded from thin-section
CT findings of 29 patients with P. aeruginosa pulmonary
infection that ground-glass attenuation or bronchial wall
Downloaded from www.microbiologyresearch.org by
IP: 114.198.209.88
On: Wed, 10 Feb 2016 22:41:23
JMM Case Reports
2011
2011
Shaulov. A
Huhulescu. S
Crnich. C.J
Neth J Med
Infection
ClinInfec Dis
2012
http://jmmcr.sgmjournals.org
1999
Downloaded from www.microbiologyresearch.org by
IP: 114.198.209.88
On: Wed, 10 Feb 2016 22:41:23
Harris. AA
Rose. HD
Fishman. H
Hoogwerf. BJ
West J Med
JAMA
South Med J
Am Rev
Hyslop,. JR
Tex Med
1971
1977
1981
1983
1983
1984
1990
1992
1992
61
49
64
29
47
39
40
27
52
general malaise, fever
cough
Pleuritic pain, fever,
weight loss
fever, chills, cough,
Dyspnea, intermittent
chills, cough, dyspnea
Right pleuritic pain,
sputum
pain, cough, bloody
Fever, malaise, pleuritic
pleuritic pain
drenching sweats, left
Cough, rigors,
left sided pleuritic pain
Fever, mild diarrhea,
pleuritic pain
Dyspnea, cough, right
pleurisy
admission
21
30
14
30
Prognosis
26
35
15
23
53
NA
21
34
13
NA
12
30
28
Elapsed time
discharge
Anti-PAB
onset to
Shock
to death/
Bacteremia
from initial
Duration
RML/RLL
RUL
RUL
RUL
RUL
LLL
LUL
RUL
RUL/LLL
RUL
RUL
RUL
RUL
LLL
RUL/RML,
RUL/RML
Left lobe
RUL/BLL
RUL
RUL
RUL
area
Affected
Con
Con
Cav/Con
Con
Cav/Con
Con
Cav/Con
Con
Con
Con
Con
Cav/Con
Cav/Con
Con
Cav
Con
Cav/Con
Con
Cav/Con
Con
calfindings
Radiologi-
lobe; RML, right middle lobe; RUL, right upper lobe; Y, yes.
A:, alive; Anti-P AB, anti-Pseudomonas antibiotics; BLL, bilateral lower lobe; Cav, cavitation; Con, consolidation; D, dead; ES, endotracheal secretion; LLL, left lower lobe; LUL, left upper lobe; N, no; NA, not available; RLL, right lower
Govan. J
Med J Aust
RespirDis
Quirk. JA
Aust NZ J Med
Henderson, A
Fever, cough, left sided
Med.
Intensive Care
20
pleuritic pain, chills
Fever, dyspnea, right
1994
Ed)
Cirigliano. MD
Back pain, dyspnea,
Cough, weight loss
fevers, weight loss
Cough, intermittent
pleuritic chest pain
Diarrhea, cough,
colored sputum
blood and rust-
Fever, chills. cough,
Chest pain, cough
hemoptysis
Dyspnea, cough,
cough
Diarrhea, chest pain,
Fever, right back pain
chest pain
Fever, cough, right
Initial symptoms
HospPract (Off
48
54
62
67
40
49
44
39
25
61
Age
fever
Sex
Med.
1995
Vicram . HR
Ishihara. S
Vicram . HR
Conn Med.
Intensive Care
1999
Hatchette. TF
ClinInfec Dis
2000
2003
2012
Kunimasa. K
Okamoto. M
2012
Intern Med
Tsuji. S
Our patient
Year
Intern Med
Author
Journal
Table 1. Clinical and radiological findings of Pseudomonas aeruginosa CAP in healthy individuals.
Fatal CAP with P. aeruginosa in healthy patients
S. Tsuji and others
Harris, A. A. (1984). Community-acquired Pseudomonas aeruginosa
1.0
Survival probability
0.8
0.6
0.4
0.2
0.0
0
10
15
20
25
30
Survival (days)
Fig. 2. KaplanMeier analysis for P. aeruginosa CAP in previously
healthy patients.
thickening were the main findings, but only nine patients
with CAP were included in that study.
The increasing importance of P. aeruginosa as a causal
agent of CAP has recently been recognized, but radiological findings have not yet been defined. Furthermore,
the initial symptoms of P. aeruginosa CAP are not specific
enough for a precise diagnosis. From this perspective, we
showed here that radiological findings of P. aeruginosa
CAP, such as cavitary pneumonia and/or consolidation in
the RUL, might be a clinical clue to a diagnosis of CAP, as
well as the presence of septic shock. Further accumulation
of such cases would be required for a more precise
understanding of the CAP caused by P. aeruginosa.
Acknowledgements
The authors declare no conflicts of interest. This report has no
personally identifiable information, and informed consent was
obtained from the patient.
References
& Griffin, P. E. (1977). Pseudomonas aeruginosa
bacteremia: a clinical study of 75 patients. Am J Med Sci 274,
119129.
Baltch, A. L.
Cirigliano, M. D. & M. A. Grippi (1994). Overwhelming pneumonia in
a healthy young nursing assistant. Hosp Pract (Off Ed) 29(1), 3134.
Crnich, C. J., et al. (2003). Hot tub-associated necrotizing pneumonia
due to Pseudomonas aeruginosa. Clin Infect Dis 36(3), e5557.
Fishman, H. (1983). Primary Pseudomonas pneumonia in a
previously healthy man. South Med J 76(2), 260262.
Govan, J. (1977). Pseudomonas pneumonia with bacteraemia. Med J
pneumonia associated with the use of a home humidifier. West J Med
141(4), 521523.
Hatchette, T. F., et al. (2000). Pseudomonas aeruginosa communityacquired pneumonia in previously healthy adults: case report and
review of the literature. Clin Infect Dis 31(6), 13491356.
Hatchette, T. F., Gupta, R. & Marrie, T. J. (2000). Pseudomonas
aeruginosa community-acquired pneumonia in previously healthy
adults: case report and review of the literature. Clin Infect Dis 31,
13491356.
Henderson, A. (1992). Fulminant primary Pseudomonas aeruginosa
pneumonia and septicaemia in previously well adults. Intensive Care
Med 18(7), 430432.
Hoogwerf, B. J. & M. Y. Khan (1981). Community-acquired
bacteremic Pseudomonas pneumonia in a health adult. Am Rev
Respir Dis 123(1), 132134.
Huhulescu, S., et al. (2011). Fatal Pseudomonas aeruginosa
pneumonia in a previously healthy woman was most likely associated
with a contaminated hot tub. Infection 39(3), 265269.
Hyslop, J. R. & T. I. Wallace (1971). Primary Pseudomonas
pneumonia. Tex Med 67(11), 112115.
Ishihara, S., et al. (1995). Septic shock due to Pseudomonas
aeruginosa in a previously healthy woman. Intensive Care Med
21(3), 226228.
Ishihara, S., Takino, M., Okada, Y. & Mimura, K. (1995). Septic shock
due to Pseudomonas aeruginosa in a previously healthy woman.
Intensive Care Med 21, 226228.
Knapp, S. ( 2013). Diabetes and infection: is there a link? A minireview. Gerontology 59, 99104.
Kunimasa, K., et al. (2012). Successful treatment of fulminant
community-acquired Pseudomonas aeruginosa necrotizing pneumonia in a previously healthy young man. Intern Med 51(17),
24732478.
Leroy, O., Bosquet, C., Vandenbussche, C., Coffinier, C.,
Georges, H., Guery, B., Alfandari, S., Thevenin, D. & Beaucaire, G.
(1999). Community-acquired pneumonia in the intensive care unit:
epidemiological and prognosis data in older people. J Am Geriatr Soc
47, 539546.
Nathan, D. M., Kuenen, J., Borg, R., Zheng, H., Schoenfeld, D.,
Heine, R. J. & & A1c-Derived Average Glucose Study Group
(2008). Translating the A1C assay into estimated average glucose
values. Diabetes Care 31, 14731478.
Okada, F., Ono, A., Ando, Y., Nakayama, T., Ishii, R., Sato, H., Kira, A.,
Tokimatsu, I., Kadota, J. & Mori, H. (2012). Thin-section CT findings
in Pseudomonas aeruginosa pulmonary infection. Br J Radiol 85,
15331538.
Okamoto, M., et al. (2012). Successful treatment of a previously
healthy woman with Pseudomonas aeruginosa community-acquired
pneumonia with plasmapheresis. Intern Med 51(19), 28092812.
Pennington, J. E., Reynolds, H. Y. & Carbone, P. P. (1973).
Pseudomonas pneumonia. A retrospective study of 36 cases. Am J
Med 55, 155160.
Quirk, J. A. (1990). Community-acquired pseudomonas pneumonia
in a normal host complicated by metastatic panophthalmitis and
cutaneous pustules. Aust N Z J Med 20(3), 254256.
Rose, H. D. (1983). Pseudomonas pneumonia associated with use of a
home whirlpool spa. JAMA 250(15), 20272029.
Rose, H. D., Franson, T. R., Sheth, N. K., Chusid, M. J., Macher, A. M.
& Zeirdt, C. H. (1983). Pseudomonas pneumonia associated with use
Aust 1(17), 627628.
of a home whirlpool spa. JAMA 250, 20272029.
Gupta, S., Koirala, J., Khardori, R. & Khardori, N. (2007). Infections in
Sadikot, R. T., Blackwell, T. S., Christman, J. W. & Prince, A. S.
(2005). Pathogenhost interactions in Pseudomonas aeruginosa
diabetes mellitus and hyperglycemia. Infect Dis Clin North Am 21,
617638, vii.
4
pneumonia. Am J Respir Crit Care Med 171, 12091223.
Downloaded from www.microbiologyresearch.org by
IP: 114.198.209.88
On: Wed, 10 Feb 2016 22:41:23
JMM Case Reports
Fatal CAP with P. aeruginosa in healthy patients
Shaulov, A., et al. (2011). A 44-year-old man with cavitary
Vikram, H. R., et al. (1999). Community acquired Pseudomonas
pneumonia and shock. Neth J Med 69(9), 402, 406.
Torres, A. & Menendez, R. (2010). Enterobacteriaceae and
Pseudomonas aeruginosa in community-acquired pneumonia: the
reality after a decade of uncertainty? Eur Respir J 35, 473 474.
Williams, B. J., Dehnbostel, J. & Blackwell, T. S. (2010). Pseudo-
http://jmmcr.sgmjournals.org
aeruginosa pneumonia. Conn Med 63(5), 271273.
monas aeruginosa: host defence in lung diseases. Respirology 15,
10371056.
Downloaded from www.microbiologyresearch.org by
IP: 114.198.209.88
On: Wed, 10 Feb 2016 22:41:23
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- tmpEFCC TMPDocument6 pagestmpEFCC TMPFrontiersNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- tmpCE8C TMPDocument19 pagestmpCE8C TMPFrontiersNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- tmp3CAB TMPDocument16 pagestmp3CAB TMPFrontiersNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- tmp80F6 TMPDocument24 pagestmp80F6 TMPFrontiersNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- tmpF178 TMPDocument15 pagestmpF178 TMPFrontiersNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Tmp1a96 TMPDocument80 pagesTmp1a96 TMPFrontiersNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- tmp6F0E TMPDocument12 pagestmp6F0E TMPFrontiersNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- tmp72FE TMPDocument8 pagestmp72FE TMPFrontiersNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- tmp37B8 TMPDocument9 pagestmp37B8 TMPFrontiersNo ratings yet
- Tmpa077 TMPDocument15 pagesTmpa077 TMPFrontiersNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- tmpE7E9 TMPDocument14 pagestmpE7E9 TMPFrontiersNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- tmpF3B5 TMPDocument15 pagestmpF3B5 TMPFrontiersNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- tmpFFE0 TMPDocument6 pagestmpFFE0 TMPFrontiersNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- tmpE3C0 TMPDocument17 pagestmpE3C0 TMPFrontiersNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- tmpF407 TMPDocument17 pagestmpF407 TMPFrontiersNo ratings yet
- tmp60EF TMPDocument20 pagestmp60EF TMPFrontiersNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- tmp6382 TMPDocument8 pagestmp6382 TMPFrontiersNo ratings yet
- tmp998 TMPDocument9 pagestmp998 TMPFrontiersNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- tmpC0A TMPDocument9 pagestmpC0A TMPFrontiersNo ratings yet
- tmpA0D TMPDocument9 pagestmpA0D TMPFrontiersNo ratings yet
- tmp4B57 TMPDocument9 pagestmp4B57 TMPFrontiersNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- tmp8B94 TMPDocument9 pagestmp8B94 TMPFrontiersNo ratings yet
- tmpD1FE TMPDocument6 pagestmpD1FE TMPFrontiersNo ratings yet
- tmp27C1 TMPDocument5 pagestmp27C1 TMPFrontiersNo ratings yet
- tmp2F3F TMPDocument10 pagestmp2F3F TMPFrontiersNo ratings yet
- tmpB1BE TMPDocument9 pagestmpB1BE TMPFrontiersNo ratings yet
- tmp9D75 TMPDocument9 pagestmp9D75 TMPFrontiersNo ratings yet
- Tmp75a7 TMPDocument8 pagesTmp75a7 TMPFrontiersNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- tmpC30A TMPDocument10 pagestmpC30A TMPFrontiersNo ratings yet
- tmp3656 TMPDocument14 pagestmp3656 TMPFrontiersNo ratings yet
- Peka SainsDocument26 pagesPeka SainsPuvaan RaajNo ratings yet
- Cordis Case Study PDFDocument29 pagesCordis Case Study PDFsingh242No ratings yet
- Final Year Clinical OSCE For Medical UndergraduatesDocument97 pagesFinal Year Clinical OSCE For Medical UndergraduatesSiam Weng LoongNo ratings yet
- 3 DR Hery - Pain Management 2018Document58 pages3 DR Hery - Pain Management 2018Ika IrawatiNo ratings yet
- Is An Ancient Disease That Causes Permanent Physical Disability AmongDocument6 pagesIs An Ancient Disease That Causes Permanent Physical Disability Amongkian5No ratings yet
- Abutment Evaluation&Biomechanics in F.P.D.Document75 pagesAbutment Evaluation&Biomechanics in F.P.D.Himanshu Gupta100% (2)
- Monmeet Instrumentation MMDTDocument18 pagesMonmeet Instrumentation MMDTMonmeet MallickNo ratings yet
- Treatment of Recurrent Depression - John F. GredenDocument208 pagesTreatment of Recurrent Depression - John F. GredenAlexAndraLuciaNo ratings yet
- Psychiatric History and Mental Status ExaminationDocument6 pagesPsychiatric History and Mental Status ExaminationRem AlfelorNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- Normal H&P Write UpDocument4 pagesNormal H&P Write Upsonnynguyen208682No ratings yet
- CBD Dr. SaugiDocument37 pagesCBD Dr. SaugiKikyNo ratings yet
- Miltex General Instruments BrochureDocument5 pagesMiltex General Instruments BrochureMichael Angelo Detalla MacolorNo ratings yet
- Uterine motilityMD20.8.55 Sheet PDFDocument45 pagesUterine motilityMD20.8.55 Sheet PDFNirut SrimakamNo ratings yet
- IMCI Session 2 - An Overview of The IMCIDocument37 pagesIMCI Session 2 - An Overview of The IMCIsarguss14100% (3)
- Scar RemovalDocument3 pagesScar RemovalJacobMsangNo ratings yet
- Amls Als Pretest Version 1.11Document10 pagesAmls Als Pretest Version 1.11ArlanosaurusNo ratings yet
- Nursing Care Plan For AppendectomyDocument5 pagesNursing Care Plan For Appendectomyvanessajane0989% (45)
- Quality Control Lecture 1Document18 pagesQuality Control Lecture 1AhmedEidNo ratings yet
- Psychodrama Children PDFDocument167 pagesPsychodrama Children PDFMonica Monica100% (2)
- Sa-Ahm Five Element AcupunctureDocument12 pagesSa-Ahm Five Element AcupunctureSivaramakrishnan GNo ratings yet
- Stress BustingDocument24 pagesStress BustingMarianne ChristieNo ratings yet
- Antimicrobial Activity Against Celtis AustralisDocument37 pagesAntimicrobial Activity Against Celtis AustralisarunNo ratings yet
- Arixtra Drug StudyDocument2 pagesArixtra Drug StudyEdelweiss Marie Cayetano100% (1)
- Chapter 10 Microbes in Human Welfare Unsolved Important Questions Class 12 PDFDocument6 pagesChapter 10 Microbes in Human Welfare Unsolved Important Questions Class 12 PDFbalaNo ratings yet
- Nitte News Jan-Dec 2010Document88 pagesNitte News Jan-Dec 2010yvj_20006373No ratings yet
- Candida Auris Osteomielitis: Case ReportDocument4 pagesCandida Auris Osteomielitis: Case Reportmarcela fernandezNo ratings yet
- Aromatherapy - Overvew, Safety and Quality IssuesDocument6 pagesAromatherapy - Overvew, Safety and Quality IssuesMBNo ratings yet
- Functional Medicine Coaching PDFDocument142 pagesFunctional Medicine Coaching PDFAnabell Garcia100% (13)
- IDRAC - 359565 - 06-Feb-2023 - Summary of Community Decisions 2023 - C 37 - 01 - On Marketing Authorisations inDocument17 pagesIDRAC - 359565 - 06-Feb-2023 - Summary of Community Decisions 2023 - C 37 - 01 - On Marketing Authorisations inMahadeva BogegowdaNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1459)
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndFrom EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndNo ratings yet
- No Mud, No Lotus: The Art of Transforming SufferingFrom EverandNo Mud, No Lotus: The Art of Transforming SufferingRating: 5 out of 5 stars5/5 (175)
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerFrom EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerRating: 4.5 out of 5 stars4.5/5 (58)