You might also like
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pathophysiology FinalDocument2 pagesPathophysiology FinallarissedeleonNo ratings yet
- Cholecystitis Litiasis EctomyDocument23 pagesCholecystitis Litiasis EctomyTimothy WilliamsNo ratings yet
- Nursing Care PlansDocument2 pagesNursing Care PlansatchiekNo ratings yet
- LCPDDocument7 pagesLCPDakoismeNo ratings yet
- Meniere's Disease - Case StudyDocument3 pagesMeniere's Disease - Case StudyZORANASNNo ratings yet
- Nursing Interventions CHFDocument3 pagesNursing Interventions CHFbanyenye25100% (1)
- Rle Worksheet Nursing ProcessDocument6 pagesRle Worksheet Nursing ProcessMARVIE JOY BALUMA CABIOCNo ratings yet
- APOLONIO, JC - Natural Theory - Thomas AquinasDocument3 pagesAPOLONIO, JC - Natural Theory - Thomas AquinasJustin ApolonioNo ratings yet
- Brief Description of The Disease/statistical IncidenceDocument2 pagesBrief Description of The Disease/statistical IncidenceLeanne Princess Gamboa100% (1)
- ABDOMINAL ObjectiveDocument9 pagesABDOMINAL ObjectiveXing-Jin RomeroNo ratings yet
- Urinary Incontinence Guide for Care and ManagementDocument5 pagesUrinary Incontinence Guide for Care and ManagementfakrulnersmudaNo ratings yet
- Sheena Khan: Biochemistry Generiic Bs NursingDocument22 pagesSheena Khan: Biochemistry Generiic Bs NursingsharmeenNo ratings yet
- Gordons TypologyDocument3 pagesGordons TypologyMaxinne Allyssa Cancino RoseñoNo ratings yet
- NCPDocument2 pagesNCPMelissa David100% (1)
- Pregnant Aerobics Instructor Case StudyDocument25 pagesPregnant Aerobics Instructor Case StudyGerly LagutingNo ratings yet
- NCP QuizonDocument2 pagesNCP QuizonChe ValenzuelaNo ratings yet
- Introduction To Community Health and Environmental Sanitation PDFDocument44 pagesIntroduction To Community Health and Environmental Sanitation PDFKaty SanchezNo ratings yet
- Cesarean Section PDFDocument9 pagesCesarean Section PDFIeien MuthmainnahNo ratings yet
- Acute Gastroenteritis Case StudyDocument42 pagesAcute Gastroenteritis Case StudyGelah DacanayNo ratings yet
- NCP GeDocument14 pagesNCP GeSuluhTriUtomoNo ratings yet
- NCP NCM 109 Post Partum PeritonitisDocument2 pagesNCP NCM 109 Post Partum PeritonitisHoney MacabuhayNo ratings yet
- NCPDocument10 pagesNCPCristina L. JaysonNo ratings yet
- 11 Digestion and Bowel Elimination 2019 (Nursing) Geriatric NursingDocument44 pages11 Digestion and Bowel Elimination 2019 (Nursing) Geriatric NursingDarla SaulerNo ratings yet
- Nursing Care PlanDocument26 pagesNursing Care PlanDinda MaretaNo ratings yet
- PancreatitisDocument12 pagesPancreatitismardsz100% (5)
- Nursing Diagnosis: Urinary Retention: NOC Outcomes (Nursing Outcomes Classification)Document4 pagesNursing Diagnosis: Urinary Retention: NOC Outcomes (Nursing Outcomes Classification)rem_No ratings yet
- Black & Hawks: Medical-Surgical Nursing Ch 31 Management of Clients with Malnutrition MCQsDocument7 pagesBlack & Hawks: Medical-Surgical Nursing Ch 31 Management of Clients with Malnutrition MCQsNeil Dave SuarezNo ratings yet
- Intussusception: PathophysiologyDocument8 pagesIntussusception: PathophysiologyNaufal AndaluNo ratings yet
- Imbalnce Nutrition Less Than Body RequirementsDocument3 pagesImbalnce Nutrition Less Than Body RequirementselheezaNo ratings yet
- Drug StudyDocument2 pagesDrug StudyNeri ChavezNo ratings yet
- NCP PainDocument2 pagesNCP PainApril_Ivy_Raga_3835No ratings yet
- Case Report Chronic OsteomyelitisDocument34 pagesCase Report Chronic OsteomyelitisNardine Roslan100% (1)
- FNCP On Elevated Blood Pressure 2Document4 pagesFNCP On Elevated Blood Pressure 2Aaron EspirituNo ratings yet
- Nursing Care for Fracture PatientDocument2 pagesNursing Care for Fracture Patientbanyenye25No ratings yet
- Diverticular DiseaseDocument8 pagesDiverticular Diseasenurse_enzo100% (1)
- NCP Impaired Physical MobilityDocument2 pagesNCP Impaired Physical MobilityjmaliticNo ratings yet
- Nusing CareplanDocument3 pagesNusing Careplanardec_143No ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Intervention and Rationale EvaluationDocument23 pagesNursing Care Plan Assessment Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Intervention and Rationale EvaluationyusivileidyNo ratings yet
- Urinary EliminationDocument80 pagesUrinary EliminationMentari WardhaniNo ratings yet
- Digestive System 2Document32 pagesDigestive System 2Johnmer AvelinoNo ratings yet
- Nursing Care Plan EportfolioDocument14 pagesNursing Care Plan Eportfolioapi-279212367No ratings yet
- Nursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermDocument4 pagesNursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermErika Danalle ArceoNo ratings yet
- Case 052: Biliary ColicDocument4 pagesCase 052: Biliary ColicZauzaNo ratings yet
- Nursing Care PlansDocument5 pagesNursing Care PlansMargaret SibugNo ratings yet
- PeritonitisDocument6 pagesPeritonitisDiane ArgoteNo ratings yet
- Case No 45: of Intermittent Abdominal Pain Abdominal Bloating and Nausea and Vomiting (NVDocument17 pagesCase No 45: of Intermittent Abdominal Pain Abdominal Bloating and Nausea and Vomiting (NVPremiums of the RoseNo ratings yet
- Nursing Care PlanDocument5 pagesNursing Care PlankingpinNo ratings yet
- Impaired Tissue Integrity - CellulitisDocument3 pagesImpaired Tissue Integrity - CellulitisKelvin Kurt B. AgwilangNo ratings yet
- Videbeck Chapter 8 Assessment - NO NOTESDocument22 pagesVidebeck Chapter 8 Assessment - NO NOTESKatie McFarlandNo ratings yet
- NCM 114 Gerontology - WeeK 1Document38 pagesNCM 114 Gerontology - WeeK 1Jmarie Brillantes Popioco0% (1)
- Case Study Ugib Lower MBDocument65 pagesCase Study Ugib Lower MBQuolette Constante100% (1)
- Signs and Symptoms of Bowel ObstructionDocument6 pagesSigns and Symptoms of Bowel ObstructionKryza Dale Bunado BaticanNo ratings yet
- NCPDocument2 pagesNCPShubhangi SarwanNo ratings yet
- 13 Surgery (Perioperative Client) Nursing Care Plans - NurseslabsDocument31 pages13 Surgery (Perioperative Client) Nursing Care Plans - NurseslabsRena SafitriNo ratings yet
- Nursing Careplan - Rectal CancerDocument5 pagesNursing Careplan - Rectal CancerdrugcardrefNo ratings yet
- Renal Failure NCPDocument3 pagesRenal Failure NCPjsksNo ratings yet
- Assessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Evaluation IndeoendentDocument3 pagesAssessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Evaluation IndeoendentDiane Sarino CabonceNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Addendum For PWBD For Online RegDocument1 pageAddendum For PWBD For Online Regprashanth100% (1)
- Notice Result Extend - NursingOfficer - 2019Document1 pageNotice Result Extend - NursingOfficer - 2019prashanthNo ratings yet
- Final Result - Nursing Officer Central Hospitals-2019-NETDocument17 pagesFinal Result - Nursing Officer Central Hospitals-2019-NETprashanthNo ratings yet
- Cghs Nabh Application HospitalDocument27 pagesCghs Nabh Application HospitalGaurav SharmaNo ratings yet
- 2TIME TABLE - 2013 Batch Third YearDocument2 pages2TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- Project ReportDocument2 pagesProject ReportprashanthNo ratings yet
- Your Bibliography VancouverDocument1 pageYour Bibliography VancouverprashanthNo ratings yet
- Advt of Nursing Officer For 4 AIIMS - 1Document10 pagesAdvt of Nursing Officer For 4 AIIMS - 1prashanthNo ratings yet
- Medical MalpracticeDocument41 pagesMedical MalpracticeprashanthNo ratings yet
- HMIS Kerala RevisedDocument34 pagesHMIS Kerala RevisedprashanthNo ratings yet
- M.O.S.C.College of Nursing, Kolenchery 3Rd Year B.Sc. Nursing Degree Course (2013-17 Batch) Clinical PlanDocument12 pagesM.O.S.C.College of Nursing, Kolenchery 3Rd Year B.Sc. Nursing Degree Course (2013-17 Batch) Clinical PlanprashanthNo ratings yet
- 8TIME TABLE - 2013 Batch Third YearDocument2 pages8TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
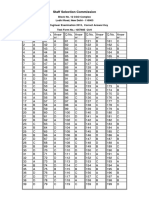
- SSC JE 2015 Exam Correct Answer Key for Test Form 1057685Document2 pagesSSC JE 2015 Exam Correct Answer Key for Test Form 1057685prashanthNo ratings yet
- Post Basic BSC Admn PlanDocument2 pagesPost Basic BSC Admn PlanprashanthNo ratings yet
- United India Insurance Recruitment for 300+ VacanciesDocument29 pagesUnited India Insurance Recruitment for 300+ VacanciesRavi SrivastavaNo ratings yet
- M.O.S.C.College of Nursing 3 Year BSC Nursing Pattern of ExaminationDocument1 pageM.O.S.C.College of Nursing 3 Year BSC Nursing Pattern of ExaminationprashanthNo ratings yet
- OremDocument12 pagesOremprashanthNo ratings yet
- 2TIME TABLE - 2013 Batch Third YearDocument2 pages2TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- Martha RogerDocument10 pagesMartha RogerprashanthNo ratings yet
- Calculation of Clinical HoursDocument1 pageCalculation of Clinical HoursprashanthNo ratings yet
- Diabetic Foot Care OverviewDocument21 pagesDiabetic Foot Care Overviewprashanth100% (4)
- Physical ExaminationDocument39 pagesPhysical ExaminationprashanthNo ratings yet
- Bowel IncontinenceDocument4 pagesBowel IncontinenceprashanthNo ratings yet
- Seminar On BUDGETDocument14 pagesSeminar On BUDGETprashanth60% (5)
- Unit Plan Mental Health NursingDocument2 pagesUnit Plan Mental Health Nursingprashanth100% (1)
- M.O.S.C College Psychiatric Nursing FormsDocument5 pagesM.O.S.C College Psychiatric Nursing FormsprashanthNo ratings yet
- ANP Clinical Rotation 2015 SinuDocument4 pagesANP Clinical Rotation 2015 SinuprashanthNo ratings yet
- M.O.S.C College of Nursing Kolenchery: Anecdotal RecordDocument5 pagesM.O.S.C College of Nursing Kolenchery: Anecdotal RecordprashanthNo ratings yet
- Tuners SndromeDocument9 pagesTuners SndromeprashanthNo ratings yet
- Assessment Format Mental Health NursingDocument11 pagesAssessment Format Mental Health Nursingprashanth100% (1)
- Case Study 4 Liver Disease Introduction To Liver Disease: CausesDocument15 pagesCase Study 4 Liver Disease Introduction To Liver Disease: CausesprabhuNo ratings yet
- 3patient History C.C, Dent HX, Habits 2Document21 pages3patient History C.C, Dent HX, Habits 2ابو العزNo ratings yet
- Principles of Critical Care in Obstetrics-Vol II - 2016Document360 pagesPrinciples of Critical Care in Obstetrics-Vol II - 2016christinejoan100% (1)
- Title: Instructions For UseDocument16 pagesTitle: Instructions For Useestia putriNo ratings yet
- Psychiatric Nursing Practice Test 150 ItemsDocument24 pagesPsychiatric Nursing Practice Test 150 Itemsroseannced100% (1)
- BibliographyDocument34 pagesBibliographyJune Marie Ding100% (1)
- Postnatal Assessment: Name Date: Age: D.O.A: Sex: Hospital: Marital Status: IP .NoDocument11 pagesPostnatal Assessment: Name Date: Age: D.O.A: Sex: Hospital: Marital Status: IP .NoRadha SriNo ratings yet
- Gait and Balance Disorder PDFDocument8 pagesGait and Balance Disorder PDFAlin AmaliyahNo ratings yet
- Dtoxa Cell PDFDocument10 pagesDtoxa Cell PDFRICHIHOTS2100% (1)
- Hyperkalemia & HypokalemiaDocument54 pagesHyperkalemia & Hypokalemiakhangsiean89No ratings yet
- GESTASIONAL DIABETES MELLITUS SimposiumDocument18 pagesGESTASIONAL DIABETES MELLITUS SimposiumHabiby Habibaty QolbiNo ratings yet
- 04.psychiatry SamplesDocument50 pages04.psychiatry SamplesCherinet KibruNo ratings yet
- A Productive and Friendly Epididymitis TreatmentDocument10 pagesA Productive and Friendly Epididymitis TreatmentwozhiainiNo ratings yet
- History Taking in Psychiatry & Mental State Examination PDFDocument30 pagesHistory Taking in Psychiatry & Mental State Examination PDFMersing Haken100% (1)
- Final Report KopinskiDocument11 pagesFinal Report Kopinskiapi-439568635No ratings yet
- Opd NewDocument42 pagesOpd NewNaima YaseenNo ratings yet
- Dubious DiagnosisDocument7 pagesDubious DiagnosisLeonardoNo ratings yet
- Unit Stats: Codex Space Crusade by Usagi3 (Translated From French To English)Document5 pagesUnit Stats: Codex Space Crusade by Usagi3 (Translated From French To English)Luis CuevasNo ratings yet
- Celiac Disease by DR Mohamed EbraheemDocument12 pagesCeliac Disease by DR Mohamed EbraheemFercho MedNo ratings yet
- Peripheral Vascular InterventionsDocument1,225 pagesPeripheral Vascular InterventionsAvinash6614No ratings yet
- Antipsychotic DrugsDocument2 pagesAntipsychotic DrugsDana Mae AfanNo ratings yet
- Unconsciousness: Law and MedicineDocument10 pagesUnconsciousness: Law and MedicineDhivya GaneshNo ratings yet
- Nephrotic Syndrome Definition and CausesDocument23 pagesNephrotic Syndrome Definition and CausesamlymarsNo ratings yet
- Expectorants and Antitussives-Dr - Jibachha Sah, M.V.SC, LecturerDocument26 pagesExpectorants and Antitussives-Dr - Jibachha Sah, M.V.SC, Lecturerjibachha sahNo ratings yet
- Daftar Poster CaseDocument6 pagesDaftar Poster Casebagusputrabali13No ratings yet
- Measles (Case Presentation)Document19 pagesMeasles (Case Presentation)Zam Pamate100% (3)
- UntitledDocument247 pagesUntitledalistair90No ratings yet
- EENT PANCE and PANRE Content Blueprint Patient PresentationsDocument8 pagesEENT PANCE and PANRE Content Blueprint Patient PresentationsThe Physician Assistant LifeNo ratings yet
- PARIET 10mg and 20mg Leaflet - Version Pari/0005/2020Document6 pagesPARIET 10mg and 20mg Leaflet - Version Pari/0005/2020JasonNo ratings yet
- "Ni-Raspa Ako Dahil Nalalag Yung Baby Ko." As Verbalized byDocument1 page"Ni-Raspa Ako Dahil Nalalag Yung Baby Ko." As Verbalized byMary AgorillaNo ratings yet