You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Outdoor Composting Guide 06339 FDocument9 pagesOutdoor Composting Guide 06339 FAdjgnf AANo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Nevada Reply BriefDocument36 pagesNevada Reply BriefBasseemNo ratings yet
- Kopp - Oberst Indictment Press Release (Final)Document2 pagesKopp - Oberst Indictment Press Release (Final)Nia TowneNo ratings yet
- CIS2103-202220-Group Project - FinalDocument13 pagesCIS2103-202220-Group Project - FinalMd. HedaitullahNo ratings yet
- Susan Abbotson - Critical Companion To Arthur Miller - A Literary Reference To His Life and Work-Facts On File (2007) PDFDocument529 pagesSusan Abbotson - Critical Companion To Arthur Miller - A Literary Reference To His Life and Work-Facts On File (2007) PDFTaha Tariq0% (1)
- Variant Configuration Step by Step ConfigDocument18 pagesVariant Configuration Step by Step Configraghava_83100% (1)
- Business Plan - Docx 3-Star Hospitality and Tourism Devt Centre in Mbarara - UgandaDocument49 pagesBusiness Plan - Docx 3-Star Hospitality and Tourism Devt Centre in Mbarara - UgandaInfiniteKnowledge100% (9)
- A Study of Factors Influencing The Consumer Behavior Towards Direct Selling Companies With Special Reference To RCM Products1Document79 pagesA Study of Factors Influencing The Consumer Behavior Towards Direct Selling Companies With Special Reference To RCM Products1Chandan SrivastavaNo ratings yet
- Letter Home Re Threat-Blocked EmailsDocument1 pageLetter Home Re Threat-Blocked EmailsNia TowneNo ratings yet
- City of Syracuse Common CouncilDocument2 pagesCity of Syracuse Common CouncilNia TowneNo ratings yet
- Manufacturing Short Factsheet 3.31.2016Document4 pagesManufacturing Short Factsheet 3.31.2016Nia TowneNo ratings yet
- Family Survivor ChecklistDocument1 pageFamily Survivor ChecklistNia TowneNo ratings yet
- Kopp & Oberst Complaint ArrestDocument1 pageKopp & Oberst Complaint ArrestNia TowneNo ratings yet
- 3-26-16 LTR To Judge Sherwood-Amanda HellmannDocument2 pages3-26-16 LTR To Judge Sherwood-Amanda HellmannNia TowneNo ratings yet
- Barry PetitionDocument94 pagesBarry PetitionNia TowneNo ratings yet
- Kopp & Oberst Complaint ArrestDocument1 pageKopp & Oberst Complaint ArrestNia TowneNo ratings yet
- Kopp Oberst Federal IndictmentDocument7 pagesKopp Oberst Federal IndictmentNia TowneNo ratings yet
- Letter To All Saints ParentsDocument1 pageLetter To All Saints ParentsNia TowneNo ratings yet
- Ryan Lawrence IndictmentDocument2 pagesRyan Lawrence IndictmentNia TowneNo ratings yet
- David SpragueDocument1 pageDavid SpragueNia TowneNo ratings yet
- Jacob Rollins-Young Court Docs (Redacted)Document9 pagesJacob Rollins-Young Court Docs (Redacted)Nia TowneNo ratings yet
- OpioidsDocument4 pagesOpioidsNia TowneNo ratings yet
- Jacob Rollins-Young (Redacted)Document9 pagesJacob Rollins-Young (Redacted)Nia TowneNo ratings yet
- Oswego Co. DA Statement On Thibodeau RulingDocument1 pageOswego Co. DA Statement On Thibodeau RulingNia TowneNo ratings yet
- Anthony Vita Criminal ComplaintDocument7 pagesAnthony Vita Criminal ComplaintNia TowneNo ratings yet
- Paige Sharp Missing Person PosterDocument1 pagePaige Sharp Missing Person PosterNia TowneNo ratings yet
- EasterEggHunt Email MPDocument1 pageEasterEggHunt Email MPNia TowneNo ratings yet
- H 1226971Document1 pageH 1226971Nia TowneNo ratings yet
- Paige Sharp Missing Person PosterDocument1 pagePaige Sharp Missing Person PosterNia TowneNo ratings yet
- Oswego Co. DA Statement On Thibodeau RulingDocument1 pageOswego Co. DA Statement On Thibodeau RulingNia TowneNo ratings yet
- 2016 3 8 Tourism MappingDocument1 page2016 3 8 Tourism MappingNia TowneNo ratings yet
- Community Letter Re-Water, March 3, 2016Document1 pageCommunity Letter Re-Water, March 3, 2016Nia TowneNo ratings yet
- Municipals March 3Document2 pagesMunicipals March 3Nia TowneNo ratings yet
- Health Depart March 3Document2 pagesHealth Depart March 3Nia TowneNo ratings yet
- Lisa Buske Statement On RulingDocument2 pagesLisa Buske Statement On RulingNia TowneNo ratings yet
- Lawrence, Ryan Felony-ComplaintDocument1 pageLawrence, Ryan Felony-ComplaintSeth PalmerNo ratings yet
- Former Syracuse Officer and Katko Staffer Accused of Stealing From City, StateDocument3 pagesFormer Syracuse Officer and Katko Staffer Accused of Stealing From City, StateNia TowneNo ratings yet
- Restaurant P&L ReportDocument4 pagesRestaurant P&L Reportnqobizitha giyaniNo ratings yet
- 110 TOP Single Phase Induction Motors - Electrical Engineering Multiple Choice Questions and Answers - MCQs Preparation For Engineering Competitive ExamsDocument42 pages110 TOP Single Phase Induction Motors - Electrical Engineering Multiple Choice Questions and Answers - MCQs Preparation For Engineering Competitive Examsvijay_marathe01No ratings yet
- BUS 301 Final AssesmentDocument15 pagesBUS 301 Final AssesmentTanzim ShahriarNo ratings yet
- OrcaSecurity Solution OverviewDocument2 pagesOrcaSecurity Solution Overviewandini eldanantyNo ratings yet
- Recent Advances in Mobile Robotics - TopalovDocument464 pagesRecent Advances in Mobile Robotics - TopalovBruno MacedoNo ratings yet
- Aggregate Demand and Supply: A ReviewDocument36 pagesAggregate Demand and Supply: A ReviewYovan DharmawanNo ratings yet
- Jurisdiction of The Supreme CourtDocument1 pageJurisdiction of The Supreme CourtAnshul Yadav100% (1)
- March 29, 2013 Strathmore TimesDocument31 pagesMarch 29, 2013 Strathmore TimesStrathmore TimesNo ratings yet
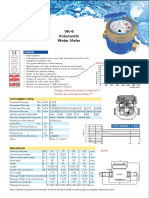
- Baylan: VK-6 Volumetric Water MeterDocument1 pageBaylan: VK-6 Volumetric Water MeterSanjeewa ChathurangaNo ratings yet
- Chapter 6 Performance Review and Appraisal - ReproDocument22 pagesChapter 6 Performance Review and Appraisal - ReproPrecious SanchezNo ratings yet
- HBL Power Systems Rectifier Division DocumentsDocument8 pagesHBL Power Systems Rectifier Division Documentsmukesh_kht1No ratings yet
- Payment Solutions For Travel Platform: SabreDocument2 pagesPayment Solutions For Travel Platform: Sabrehell nahNo ratings yet
- $$TR Sas 114 AllDocument384 pages$$TR Sas 114 Allctudose4282No ratings yet
- University of Cebu-Main Campus Entrepreneurship 100 Chapter 11 QuizDocument3 pagesUniversity of Cebu-Main Campus Entrepreneurship 100 Chapter 11 QuizAnmer Layaog BatiancilaNo ratings yet
- Power Steering Rack Components and Auto Suppliers Reference GuideDocument12 pagesPower Steering Rack Components and Auto Suppliers Reference GuideJonathan JoelNo ratings yet
- QAQC Inspection Services Technical Proposal SummaryDocument69 pagesQAQC Inspection Services Technical Proposal SummaryMathias OnosemuodeNo ratings yet
- Product Datasheet ASSA ABLOY DL6120T enDocument28 pagesProduct Datasheet ASSA ABLOY DL6120T enAbin RajuNo ratings yet
- NSTP 1: Pre-AssessmentDocument3 pagesNSTP 1: Pre-AssessmentMaureen FloresNo ratings yet
- Secure Access Control and Browser Isolation PrinciplesDocument32 pagesSecure Access Control and Browser Isolation PrinciplesSushant Yadav100% (1)
- MTD Microwave Techniques and Devices TEXTDocument551 pagesMTD Microwave Techniques and Devices TEXTARAVINDNo ratings yet
- Day / Month / Year: Certificate of No Criminal Conviction Applicant Data Collection Form (LOCAL)Document4 pagesDay / Month / Year: Certificate of No Criminal Conviction Applicant Data Collection Form (LOCAL)Lhea RecenteNo ratings yet
- Loans and AdvanceDocument8 pagesLoans and AdvanceDjay SlyNo ratings yet
- Torta de Riso Business PlanDocument25 pagesTorta de Riso Business PlanSalty lNo ratings yet