You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
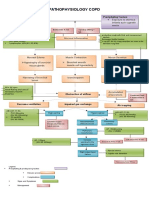
- Copd PathDocument2 pagesCopd Pathnursing concept maps100% (2)
- Ventilator Waveform AnalysisDocument96 pagesVentilator Waveform AnalysisVeerapong Vattanavanit100% (11)
- Basics of Waveform Interpretation: Michael Haines, MPH, RRT-NPS, AE-CDocument76 pagesBasics of Waveform Interpretation: Michael Haines, MPH, RRT-NPS, AE-CMohamed Koriesh100% (1)
- Kaya TimeseriesDocument9 pagesKaya TimeseriesDelvianaNo ratings yet
- Pi Is 0885392404001897Document7 pagesPi Is 0885392404001897DelvianaNo ratings yet
- Acspc 042280 PDFDocument32 pagesAcspc 042280 PDFDelvianaNo ratings yet
- Constriction Band Syndrome WebDocument1 pageConstriction Band Syndrome WebDelvianaNo ratings yet
- Nen006 PDFDocument7 pagesNen006 PDFDelvianaNo ratings yet
- Time Management: Procrastination Tendency in Individual and Collaborative TasksDocument11 pagesTime Management: Procrastination Tendency in Individual and Collaborative TasksDelvianaNo ratings yet
- Cutlerc MucositisasbDocument21 pagesCutlerc MucositisasbDelvianaNo ratings yet
- Kapita SelektaDocument39 pagesKapita SelektaDelvianaNo ratings yet
- Effect of Psycho-Educational Training Program For Parent's Having Child With Leukemia On Their Experience and Psychological WellbeingDocument18 pagesEffect of Psycho-Educational Training Program For Parent's Having Child With Leukemia On Their Experience and Psychological WellbeingDelvianaNo ratings yet
- A Comparison of Vinegar Compresses VsDocument1 pageA Comparison of Vinegar Compresses VsDelvianaNo ratings yet
- Human Becoming TheoryDocument7 pagesHuman Becoming TheoryDelvianaNo ratings yet
- Assessment of Respiratory FunctionDocument4 pagesAssessment of Respiratory FunctionCristine Dominique E. DonaireNo ratings yet
- Albay Hospital Beds and Mechanical Ventilator Capacity (As of May 29, 2021)Document8 pagesAlbay Hospital Beds and Mechanical Ventilator Capacity (As of May 29, 2021)Joco Franz AmanoNo ratings yet
- NCM 112 Lab (Prelims)Document14 pagesNCM 112 Lab (Prelims)Erica Mei CapiliNo ratings yet
- 2019 (Wright Et Al.) - Physical Therapies in Pediatric Respiratory Disease PDFDocument20 pages2019 (Wright Et Al.) - Physical Therapies in Pediatric Respiratory Disease PDFNicolas ParejaNo ratings yet
- General & Multi Speciality Hospitals: Iyyappan K 9844535502Document17 pagesGeneral & Multi Speciality Hospitals: Iyyappan K 9844535502Nandeesh SNo ratings yet
- NIV and HFNCDocument16 pagesNIV and HFNCMarceline GarciaNo ratings yet
- Anesthesia Workstation Ventilation ModesDocument6 pagesAnesthesia Workstation Ventilation Modesmas agung chandraNo ratings yet
- SMS Result and Data 2021Document161 pagesSMS Result and Data 2021ChinaNo ratings yet
- Functional Classification of Ventilator ModesDocument53 pagesFunctional Classification of Ventilator ModesNasrullah KhanNo ratings yet
- Abnormal Lung SoundsDocument6 pagesAbnormal Lung SoundsQuinn Madalang100% (1)
- Client with Difficulty BreathingDocument6 pagesClient with Difficulty BreathingJoji BaitNo ratings yet
- Chapter 53 - Introduction To The Respiratory SystemDocument13 pagesChapter 53 - Introduction To The Respiratory SystemJonathonNo ratings yet
- Protections of the Upper Airway Shield the Lower AirwayDocument3 pagesProtections of the Upper Airway Shield the Lower AirwayPaul JacksonNo ratings yet
- Artificial Respirator - CPR Functioning BY, SANDHYA S.-1703099 SATHVIKA A.-1703104Document15 pagesArtificial Respirator - CPR Functioning BY, SANDHYA S.-1703099 SATHVIKA A.-170310417O3099 Sandhya S.No ratings yet
- RespiraciónDocument7 pagesRespiraciónKarolNo ratings yet
- Mechanical Ventilation in Pediatric PracticeDocument11 pagesMechanical Ventilation in Pediatric PracticeHandris YanitraNo ratings yet
- Diagnosis and Management of Asthma in AdultsDocument12 pagesDiagnosis and Management of Asthma in AdultsRoberto López Mata67% (6)
- Instruction Aerobika 001-Revb InsertOPEPDocument16 pagesInstruction Aerobika 001-Revb InsertOPEPNandhini SivakumarNo ratings yet
- Pediatric Lung Diseases: Empyema and Lung AbscessDocument39 pagesPediatric Lung Diseases: Empyema and Lung AbscessFaisal MoidunnyNo ratings yet
- Approach of TraumaDocument45 pagesApproach of TraumaAqila MumtazNo ratings yet
- COPD Case Studies and AnalysisDocument5 pagesCOPD Case Studies and AnalysisTiara PutriNo ratings yet
- Dr. Sudarto Sppd's FileDocument22 pagesDr. Sudarto Sppd's FileVindy CesarianaNo ratings yet
- Savina 300 BrochureDocument8 pagesSavina 300 BrochureRafa Tejeda100% (1)
- An Approach To Interpreting Spirometry (Finals) PDFDocument25 pagesAn Approach To Interpreting Spirometry (Finals) PDFVanessa CarinoNo ratings yet
- Dyspnea Is An Uncomfortable Abnormal Awareness of Breathing. A Number of DifferentDocument4 pagesDyspnea Is An Uncomfortable Abnormal Awareness of Breathing. A Number of DifferentSita SifanaNo ratings yet
- Edit Dafpus TK 1-1Document3 pagesEdit Dafpus TK 1-1annewidiatmoNo ratings yet
- Assessment Pulmonary ExamDocument3 pagesAssessment Pulmonary Examdd marshallNo ratings yet