You might also like
- Infiltration and Extravasation Update On.10Document9 pagesInfiltration and Extravasation Update On.10Beauty CassieNo ratings yet
- Genetic Journal PDFDocument12 pagesGenetic Journal PDFSasha Hidayat FullNo ratings yet
- Ekstravasasi PDFDocument7 pagesEkstravasasi PDFSasha Hidayat FullNo ratings yet
- Askep Meningitis AnakDocument10 pagesAskep Meningitis AnakSasha Hidayat FullNo ratings yet
- _____ ______ __ _ ____Document6 pages_____ ______ __ _ ____Sasha Hidayat FullNo ratings yet
- Best Evidence-Based Practices To Treat Intravenous InfiltrationDocument1 pageBest Evidence-Based Practices To Treat Intravenous InfiltrationSasha Hidayat FullNo ratings yet
- Revista Paulista DE PediatriaDocument6 pagesRevista Paulista DE PediatriaSasha Hidayat FullNo ratings yet
- MucositisDocument6 pagesMucositisHarry ArdiyantoNo ratings yet
- Harrison Prevention and Management of Pain and Stress in The Neonate 2015Document8 pagesHarrison Prevention and Management of Pain and Stress in The Neonate 2015Sasha Hidayat FullNo ratings yet
- Childhood Trauma Linked to Chronic DiseasesDocument6 pagesChildhood Trauma Linked to Chronic DiseasesSasha Hidayat FullNo ratings yet
- Four perspectives on measuring child care qualityDocument7 pagesFour perspectives on measuring child care qualitySasha Hidayat FullNo ratings yet
- Ok JurnalDocument6 pagesOk JurnalSasha Hidayat FullNo ratings yet
- Genetic Journal PDFDocument12 pagesGenetic Journal PDFSasha Hidayat FullNo ratings yet
- Managing Oral Mucositis Oral Health July 2015Document4 pagesManaging Oral Mucositis Oral Health July 2015fiora.ladesvitaNo ratings yet
- B - PDF PDFDocument11 pagesB - PDF PDFSasha Hidayat FullNo ratings yet
- Position 3Document5 pagesPosition 3Sasha Hidayat FullNo ratings yet
- Evid Based Nurs 2012 Meek 84 5Document3 pagesEvid Based Nurs 2012 Meek 84 5Sasha Hidayat FullNo ratings yet
- 212Document5 pages212Sasha Hidayat FullNo ratings yet
- Ethical SkillDocument8 pagesEthical SkillSasha Hidayat FullNo ratings yet
- Overweight and Obesity Among White, Black, and Mexican American Children: Implications For When To InterveneDocument10 pagesOverweight and Obesity Among White, Black, and Mexican American Children: Implications For When To InterveneSasha Hidayat FullNo ratings yet
- Nejm CER Consent KassDocument3 pagesNejm CER Consent KassSasha Hidayat FullNo ratings yet
- Massase For Cancer 2Document16 pagesMassase For Cancer 2Sasha Hidayat FullNo ratings yet
- Acute Respiratory Distress Syndrome in Pediatric Intensive Care UnitDocument4 pagesAcute Respiratory Distress Syndrome in Pediatric Intensive Care UnitSasha Hidayat FullNo ratings yet
- Position 2Document8 pagesPosition 2Sasha Hidayat FullNo ratings yet
- Hipospadia Ej1083631 OkDocument17 pagesHipospadia Ej1083631 OkSasha Hidayat FullNo ratings yet
- JCCNC v1n4p205 enDocument6 pagesJCCNC v1n4p205 enSasha Hidayat FullNo ratings yet
- Gynecologic Oncology: Nozomi Donoyama, Toyomi Satoh, Tetsutaro Hamano, Norio Ohkoshi, Mamiko OnukiDocument8 pagesGynecologic Oncology: Nozomi Donoyama, Toyomi Satoh, Tetsutaro Hamano, Norio Ohkoshi, Mamiko OnukiSasha Hidayat FullNo ratings yet
- Gynecologic Oncology: Nozomi Donoyama, Toyomi Satoh, Tetsutaro Hamano, Norio Ohkoshi, Mamiko OnukiDocument8 pagesGynecologic Oncology: Nozomi Donoyama, Toyomi Satoh, Tetsutaro Hamano, Norio Ohkoshi, Mamiko OnukiSasha Hidayat FullNo ratings yet
- 4as To Rise Above Moral Distress PDFDocument14 pages4as To Rise Above Moral Distress PDFOscar PerezNo ratings yet
- Oral Care For Cancer PDFDocument10 pagesOral Care For Cancer PDFSasha Hidayat FullNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Effectiveness of structured teaching programme on knowledge regarding effect of junk foodDocument156 pagesEffectiveness of structured teaching programme on knowledge regarding effect of junk foodCynthia Joy Ibhafidon100% (1)
- Minor Ailments During PregnancyDocument47 pagesMinor Ailments During PregnancyDiablo GoliathNo ratings yet
- History Made Easy NotesDocument3 pagesHistory Made Easy NotesTahir AliNo ratings yet
- Management of Globus Hystericusand Role of AntidepressantsDocument5 pagesManagement of Globus Hystericusand Role of AntidepressantsIJAR JOURNALNo ratings yet
- Surgical MCQDocument27 pagesSurgical MCQAhmad Alnemare100% (11)
- Drugs Affecting Gastrointestinal, Endocrine and Renal SystemsDocument35 pagesDrugs Affecting Gastrointestinal, Endocrine and Renal SystemsJewel Ramos GalinatoNo ratings yet
- Hoarseness in AdultsDocument9 pagesHoarseness in AdultsNila Ijma SeptianaNo ratings yet
- Atlas of Gastrointestinal Endoscopy in Dogs and CatsDocument8 pagesAtlas of Gastrointestinal Endoscopy in Dogs and CatsDama Ayu RaniNo ratings yet
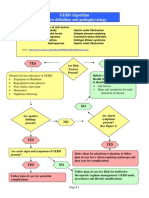
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocument3 pagesGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNo ratings yet
- Gastroesophageal RefluxDocument13 pagesGastroesophageal RefluxHamza AhmedNo ratings yet
- Achalasia EbookDocument48 pagesAchalasia EbookAhmad Farqaleet BhattiNo ratings yet
- The Use of Subcutaneous Omeprazole in The Treatment of Dyspepsia in Palliative Care PatientsDocument3 pagesThe Use of Subcutaneous Omeprazole in The Treatment of Dyspepsia in Palliative Care PatientscarinasheliapNo ratings yet
- GERDDocument32 pagesGERDlumina.sNo ratings yet
- Digestive System NotesDocument72 pagesDigestive System NotesQueen SarrahNo ratings yet
- Esophageal DisorderDocument82 pagesEsophageal DisorderMimo HemadNo ratings yet
- Management of Patients With Oral and Esophageal Disorders PDFDocument85 pagesManagement of Patients With Oral and Esophageal Disorders PDFNixi Mbuthia100% (1)
- Guidelines and Style Guide For Alomedika - Rev 2019Document14 pagesGuidelines and Style Guide For Alomedika - Rev 2019Shandy Suwanto PutraNo ratings yet
- Master Techniques in Surgery Esophageal Surgery 20 PDFDocument598 pagesMaster Techniques in Surgery Esophageal Surgery 20 PDFDima Nestor100% (2)
- Drug StudyDocument5 pagesDrug StudyAika CortesNo ratings yet
- Characteristics of The Novel Potassium-Competitive Acid Blocker Vonoprazan Fumarate (TAK-438)Document18 pagesCharacteristics of The Novel Potassium-Competitive Acid Blocker Vonoprazan Fumarate (TAK-438)mNo ratings yet
- Tegoprazan Vs EsomeprasolDocument9 pagesTegoprazan Vs EsomeprasolAldo Alvarez PinedaNo ratings yet
- Treatment of Sjögren's Syndrome - Constitutional and Non-Sicca Organ-Based Manifestations - UpToDateDocument31 pagesTreatment of Sjögren's Syndrome - Constitutional and Non-Sicca Organ-Based Manifestations - UpToDateGabriel Fernandez FigueroaNo ratings yet
- Demo Cot 2pptDocument22 pagesDemo Cot 2pptDiana NageraNo ratings yet
- Hiatus Hernia - Chinese Herbs, Chinese Medicine, AcupunctureDocument6 pagesHiatus Hernia - Chinese Herbs, Chinese Medicine, AcupunctureCarlCordNo ratings yet
- Drug StudyDocument13 pagesDrug Studyapi-3757116100% (4)
- Written Report GERDDocument11 pagesWritten Report GERDAlthea AlbaniaNo ratings yet
- Easy-to-Swallow, Easy-to-Chew PDFDocument259 pagesEasy-to-Swallow, Easy-to-Chew PDFChatterjee Nikita100% (2)
- Laryngopharyngeal RefluxDocument4 pagesLaryngopharyngeal RefluxrevivalpurposeNo ratings yet
- Alawiya, Jamal Tango P.Document18 pagesAlawiya, Jamal Tango P.Jamal P. AlawiyaNo ratings yet
- Perspectiva Eap PDFDocument11 pagesPerspectiva Eap PDFAndres Felipe Rojas RodriguezNo ratings yet