You might also like
- Mottram escápula1Document6 pagesMottram escápula1Elizabeth VivancoNo ratings yet
- 13 Marchetti 380 384 Pullover Copia 3193891071Document5 pages13 Marchetti 380 384 Pullover Copia 3193891071Angelica GarciaNo ratings yet
- Pullover PDFDocument5 pagesPullover PDFRosaneLacerdaNo ratings yet
- Thoracic MET 2003Document16 pagesThoracic MET 2003sulis tiyowatiNo ratings yet
- 2010 - Manual Therapy PDFDocument5 pages2010 - Manual Therapy PDFYuzo IgarashiNo ratings yet
- Elastico No OmbrosDocument9 pagesElastico No OmbrosallanboxeNo ratings yet
- Acute Effects of Hamstring Stretching On Sagittal Spinal Curvatures and Pelvic TiltDocument10 pagesAcute Effects of Hamstring Stretching On Sagittal Spinal Curvatures and Pelvic TiltOcAn D'scAmpNo ratings yet
- 13 Marchetti 380 384pulloverDocument6 pages13 Marchetti 380 384pullovercderosasNo ratings yet
- The Influence of Initial Posture On The Sit-To-Stand MovementDocument6 pagesThe Influence of Initial Posture On The Sit-To-Stand MovementshodhgangaNo ratings yet
- Manual Therapy: Kuan-Ting Lee, Chiung-Cheng Chuang, Chien-Hung Lai, Jing-Jhao Ye, Chien-Lung WuDocument6 pagesManual Therapy: Kuan-Ting Lee, Chiung-Cheng Chuang, Chien-Hung Lai, Jing-Jhao Ye, Chien-Lung Wuubiktrash1492No ratings yet
- Effect of Task-Oriented Training and Neurodevelopmental Treatment On The Sitting Posture in Children With Cerebral PalsyDocument3 pagesEffect of Task-Oriented Training and Neurodevelopmental Treatment On The Sitting Posture in Children With Cerebral PalsyPhysio SauravNo ratings yet
- Effect of Isometric Horizontal Abduction On Pectoralis Major and Serratus AnteriorDocument7 pagesEffect of Isometric Horizontal Abduction On Pectoralis Major and Serratus AnteriorRudolfGerNo ratings yet
- Pasiv and ActiveDocument4 pagesPasiv and ActiveAna wulandariNo ratings yet
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltDocument3 pagesAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniNo ratings yet
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltDocument3 pagesAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniNo ratings yet
- Manual Therapy: Birgit Castelein, Ann Cools, Thierry Parlevliet, Barbara CagnieDocument6 pagesManual Therapy: Birgit Castelein, Ann Cools, Thierry Parlevliet, Barbara CagnieGuilherme SerpaNo ratings yet
- Influence of GenderDocument10 pagesInfluence of Gendersateesh83No ratings yet
- Balance Perturbation Leads A Stretching Reflexion On Tibialis Anterior MuscleDocument5 pagesBalance Perturbation Leads A Stretching Reflexion On Tibialis Anterior MuscleMatheus AguiarNo ratings yet
- The Effects of Kinesio Taping On Quadriceps Strenth During Isokinetic Exercise in Healthy Non-Athlete WomenDocument6 pagesThe Effects of Kinesio Taping On Quadriceps Strenth During Isokinetic Exercise in Healthy Non-Athlete WomenionNo ratings yet
- Dynamic MRI assessment of diaphragm function during postural activitiesDocument21 pagesDynamic MRI assessment of diaphragm function during postural activitiesMarcus LimaNo ratings yet
- 02 - Biomechanical Analysis of Sit-To-stand Movement in Normal and Obese SubjectsDocument6 pages02 - Biomechanical Analysis of Sit-To-stand Movement in Normal and Obese SubjectsCristian HuequelefNo ratings yet
- Manual Therapy: Original ArticleDocument5 pagesManual Therapy: Original ArticleCleber PimentaNo ratings yet
- 04 - Evaluation of The Stability of Sit-To-standDocument5 pages04 - Evaluation of The Stability of Sit-To-standCristian HuequelefNo ratings yet
- Diederichsen Et Al, 2007Document10 pagesDiederichsen Et Al, 2007Bruno Pascoalini - BiomecânicaNo ratings yet
- Rehabilitation Exercises To Induce Balanced Scapular Muscle Activity in An Anti-Gravity PostureDocument4 pagesRehabilitation Exercises To Induce Balanced Scapular Muscle Activity in An Anti-Gravity PostureSAMNo ratings yet
- Ji-Hyun Lee - The Effect of Scapular Posterior Tilt ExerciseDocument8 pagesJi-Hyun Lee - The Effect of Scapular Posterior Tilt Exercisesebafigueroa94No ratings yet
- Accepted ManuscriptDocument40 pagesAccepted ManuscriptDaniel CarcamoNo ratings yet
- Paper 1Document9 pagesPaper 1sbarahonacamilaNo ratings yet
- 1 s2.0 S1356689X15002635 MainDocument5 pages1 s2.0 S1356689X15002635 Mainayşe numanoğluNo ratings yet
- Adl Upper LimbDocument8 pagesAdl Upper LimbTirumala RaoNo ratings yet
- Electromyographic Analysis of The Hip Extension Pattern in Visually Impaired AthletesDocument9 pagesElectromyographic Analysis of The Hip Extension Pattern in Visually Impaired AthletesVizaNo ratings yet
- 2016 Influence of Scapular Position On The CORE Musculature Activation in The Prone Plank ExerciseDocument23 pages2016 Influence of Scapular Position On The CORE Musculature Activation in The Prone Plank ExerciseFrancisco Antonó Castro WeithNo ratings yet
- Dickie 2016Document28 pagesDickie 2016FranciscoNo ratings yet
- The Effect of Trunk Strengthening Exercise Using Oscillation On Trunk Muscle Thickness and BalanceDocument11 pagesThe Effect of Trunk Strengthening Exercise Using Oscillation On Trunk Muscle Thickness and Balancekang soon cheolNo ratings yet
- An Exploration of The Function of The Triceps Surae During Normal Gait Using Functional Electrical Stimulation PDFDocument2 pagesAn Exploration of The Function of The Triceps Surae During Normal Gait Using Functional Electrical Stimulation PDFValentinus Adi PamungkasNo ratings yet
- Muscle Function Path Analysis Through Muscle ActivityDocument7 pagesMuscle Function Path Analysis Through Muscle ActivityWebster LimNo ratings yet
- O'Sullivan Posture Muscle Activity 02Document7 pagesO'Sullivan Posture Muscle Activity 02Hugo ArezNo ratings yet
- The Effect of Thoracic Spine MobilizationDocument4 pagesThe Effect of Thoracic Spine MobilizationEric SimasNo ratings yet
- Manual Therapy: Original ArticleDocument6 pagesManual Therapy: Original ArticleRyan SetyantoNo ratings yet
- transverso abdomen2Document4 pagestransverso abdomen2Elizabeth VivancoNo ratings yet
- Salem 201Document6 pagesSalem 201mikelNo ratings yet
- Effectiveness of Schroth and sling exercises for flexibility, balance, spinal angle and chest expansion in scoliosis patientsDocument13 pagesEffectiveness of Schroth and sling exercises for flexibility, balance, spinal angle and chest expansion in scoliosis patientskang soon cheolNo ratings yet
- GaitDocument8 pagesGaitPravin YadavNo ratings yet
- Brazilian Journal of Physical TherapyDocument10 pagesBrazilian Journal of Physical TherapyLuis DavidNo ratings yet
- Cortine, Neck Muscle & GaitDocument4 pagesCortine, Neck Muscle & GaitPhooi Yee LauNo ratings yet
- Biomechanical Analysis of The Standing Long Jump: W - L W, J - H W, H - T L, G - J WDocument4 pagesBiomechanical Analysis of The Standing Long Jump: W - L W, J - H W, H - T L, G - J W陳俞良No ratings yet
- artigolegpress2022Document11 pagesartigolegpress2022Lina M GarciaNo ratings yet
- Gong's mobilization increases shoulder abduction more than glidingDocument3 pagesGong's mobilization increases shoulder abduction more than glidingIVAN VERGARANo ratings yet
- Journal of Bodywork & Movement TherapiesDocument6 pagesJournal of Bodywork & Movement TherapiesLuqmanul HakimNo ratings yet
- Title: Instructions For UseDocument5 pagesTitle: Instructions For UseAnonymous b2k9ABe7eNo ratings yet
- Mandibular Rest Position and ElectricalDocument6 pagesMandibular Rest Position and ElectricalPaula GuerreroNo ratings yet
- Surface Electromyography (Emg) Activity of Abdominal Muscles During Wheelchair's WheelieDocument18 pagesSurface Electromyography (Emg) Activity of Abdominal Muscles During Wheelchair's WheelieMOHD ZAINIZAM ABDULL RASIDNo ratings yet
- Jpts 27 2621Document4 pagesJpts 27 2621vvNo ratings yet
- 1.research PaperDocument18 pages1.research PaperbinNo ratings yet
- Human Movement Science: Brian C. Nairn, Janessa D.M. DrakeDocument11 pagesHuman Movement Science: Brian C. Nairn, Janessa D.M. DrakeQuiroprácticaParaTodosNo ratings yet
- Principles of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodFrom EverandPrinciples of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodShigehiko KatadaNo ratings yet
- Anatomy and Human Movement: Structure and FunctionFrom EverandAnatomy and Human Movement: Structure and FunctionRating: 3.5 out of 5 stars3.5/5 (2)
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- Self-Myofascial Release, Purpose, Methods and TechniquesDocument47 pagesSelf-Myofascial Release, Purpose, Methods and TechniquesJonathan Warncke100% (14)
- Scapular Positioning and Motor Control in Children and Adults A Laboratory StudyDocument6 pagesScapular Positioning and Motor Control in Children and Adults A Laboratory StudyCmmb FisioterapiaNo ratings yet
- Self-Myofascial Release, Purpose, Methods and TechniquesDocument47 pagesSelf-Myofascial Release, Purpose, Methods and TechniquesJonathan Warncke100% (14)
- Motion Analysis Study of A Scapular Orientation ExerciseDocument6 pagesMotion Analysis Study of A Scapular Orientation ExerciseCmmb FisioterapiaNo ratings yet
- Scapular Positioning in Overhead Athletes With and Without Shoulder PDFDocument10 pagesScapular Positioning in Overhead Athletes With and Without Shoulder PDFCmmb FisioterapiaNo ratings yet
- Self-Myofascial Release, Purpose, Methods and TechniquesDocument47 pagesSelf-Myofascial Release, Purpose, Methods and TechniquesJonathan Warncke100% (14)
- Altered Breathing Patterns During Lumbopelvic Motor ControlDocument8 pagesAltered Breathing Patterns During Lumbopelvic Motor Controlubiktrash1492No ratings yet
- Review Scapular Positioning and Movement in Unimpaired ShouldersDocument7 pagesReview Scapular Positioning and Movement in Unimpaired ShouldersCmmb FisioterapiaNo ratings yet
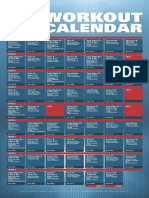
- XT2 Workout Calendar PDFDocument1 pageXT2 Workout Calendar PDFYazmin SotoNo ratings yet
- Motor Control Retraining Exercises For Shoulder Impingement Effects On Function Muscle Activation and Biomechanics in Young AdultsDocument9 pagesMotor Control Retraining Exercises For Shoulder Impingement Effects On Function Muscle Activation and Biomechanics in Young AdultsCmmb FisioterapiaNo ratings yet
- Altered Breathing Patterns During Lumbopelvic Motor ControlDocument8 pagesAltered Breathing Patterns During Lumbopelvic Motor Controlubiktrash1492No ratings yet
- Scapular Positioning in Overhead Athletes With and Without Shoulder PDFDocument10 pagesScapular Positioning in Overhead Athletes With and Without Shoulder PDFCmmb FisioterapiaNo ratings yet
- Hurdles Performance Lead Arm Technique Advancement For Hurdle PerformanceDocument5 pagesHurdles Performance Lead Arm Technique Advancement For Hurdle PerformanceCmmb FisioterapiaNo ratings yet
- Scapular Positioning in Overhead Athletes With and Without Shoulder PDFDocument10 pagesScapular Positioning in Overhead Athletes With and Without Shoulder PDFCmmb FisioterapiaNo ratings yet
- Lab Technician Resume TitleDocument1 pageLab Technician Resume TitleSilvio DTNo ratings yet
- Nutrition in The Critically Ill PatientDocument13 pagesNutrition in The Critically Ill PatientnainazahraNo ratings yet
- Molluscum Contagiosum Andrew N PitzpatrickDocument5 pagesMolluscum Contagiosum Andrew N PitzpatrickHel DaNo ratings yet
- Children's Hospital of Eastern Ontario Pain Scale (CHEOPS)Document3 pagesChildren's Hospital of Eastern Ontario Pain Scale (CHEOPS)Nick O NeillNo ratings yet
- ETHICAL ISSUES IN COUNSELING - SaidaDocument17 pagesETHICAL ISSUES IN COUNSELING - Saidasaidahsalim67% (3)
- T Bar Clasp Retained Removable Partial Denture As An Alternative To Implant Based Prosthetic TreatmentDocument6 pagesT Bar Clasp Retained Removable Partial Denture As An Alternative To Implant Based Prosthetic TreatmentCurcubet OlgaNo ratings yet
- SMLE 2019 CorrectionsDocument112 pagesSMLE 2019 CorrectionsRight VentricleNo ratings yet
- Alzheimer's Research PaperDocument5 pagesAlzheimer's Research PaperJosh BarnutNo ratings yet
- Stroe Be 2017Document27 pagesStroe Be 2017Iris Moreno R100% (1)
- Updates in The Treatment of Eating Disorders in 2022 A Year in Review in Eating Disorders The Journal of Treatment PreventionDocument12 pagesUpdates in The Treatment of Eating Disorders in 2022 A Year in Review in Eating Disorders The Journal of Treatment PreventionMarietta_MonariNo ratings yet
- Letty KuanDocument1 pageLetty KuanchrizthineeNo ratings yet
- What Are Extrapyramidal SymptomsDocument2 pagesWhat Are Extrapyramidal SymptomscristieristiieNo ratings yet
- Child Psychiatric DisordersDocument8 pagesChild Psychiatric DisordersGaurang ShirwadkarNo ratings yet
- Clinical Management in PsychodermatologyDocument294 pagesClinical Management in Psychodermatologymconsultorpsi100% (2)
- GuidlinesDocument10 pagesGuidlinesbubuvulpeaNo ratings yet
- Intricate Internal Anatomy of Teeth and Its Clinical Significance in Endodontics - A ReviewDocument10 pagesIntricate Internal Anatomy of Teeth and Its Clinical Significance in Endodontics - A ReviewManjeevNo ratings yet
- Immunics PDFDocument25 pagesImmunics PDFRedamanNo ratings yet
- Pancreatitis Ishikawa 2016Document19 pagesPancreatitis Ishikawa 2016Limbert RodriguezNo ratings yet
- %quogvkecewrwpevwtgvcmguqpvjgytkpmng: D (#N (Uuc5Ejqvvncpf$Cwocprjqvqitcrj (D (%NKPVQP Wuug (Document1 page%quogvkecewrwpevwtgvcmguqpvjgytkpmng: D (#N (Uuc5Ejqvvncpf$Cwocprjqvqitcrj (D (%NKPVQP Wuug (sonNo ratings yet
- Panic DisorderDocument60 pagesPanic Disordergrinakis100% (1)
- Avoiding Toxic Relationships in RecoveryDocument4 pagesAvoiding Toxic Relationships in RecoverymelodyfathiNo ratings yet
- Dialog EFN2 Sudarmi 30140114040Document2 pagesDialog EFN2 Sudarmi 30140114040sudarmiNo ratings yet
- Itachi's Mysterious Illness Diagnosed as Microscopic PolyangiitisDocument5 pagesItachi's Mysterious Illness Diagnosed as Microscopic PolyangiitisGica AlecuNo ratings yet
- Chart FastingDocument1 pageChart FastingGary S75% (4)
- NeuroblastomaDocument10 pagesNeuroblastomadita100% (1)
- EFT Tapping Points Chart Explains Emotional Links to Each PointDocument9 pagesEFT Tapping Points Chart Explains Emotional Links to Each PointJodi Johnson100% (2)
- Complete Guide To Communication Problems After StrokeDocument22 pagesComplete Guide To Communication Problems After Strokeapi-215453798100% (1)
- Graves DseDocument5 pagesGraves DseHester Marie SimpiaNo ratings yet
- ArthritisDocument15 pagesArthritisPrambudi KusumaNo ratings yet
- Sustained Release Dosage FormsDocument9 pagesSustained Release Dosage FormsJasdeep KaurNo ratings yet