You might also like
- Antibiotic Treatment Strategies For Community Acquired Pneumonia in AdultsDocument12 pagesAntibiotic Treatment Strategies For Community Acquired Pneumonia in AdultsCumbelia PrimaNo ratings yet
- Jurnal GH TambuntaDocument6 pagesJurnal GH TambuntaIrfan MohammadNo ratings yet
- K 19 20 Metabolism RegulationDocument29 pagesK 19 20 Metabolism RegulationIrfan MohammadNo ratings yet
- Managing Immune Thrombocytopenic Purpura: An UpdateDocument7 pagesManaging Immune Thrombocytopenic Purpura: An UpdateApriliza RalasatiNo ratings yet
- Itp Periop1Document4 pagesItp Periop1Irfan MohammadNo ratings yet
- Dia Care-2015-Siraj-2000-8Document9 pagesDia Care-2015-Siraj-2000-8Irfan MohammadNo ratings yet
- Diagnosis and Management of Clinical ChorioamnionitisDocument18 pagesDiagnosis and Management of Clinical ChorioamnionitisIrfan MohammadNo ratings yet
- Introduction To Metabolism: Departemen Fisiologi Fakultas Kedokteran USUDocument22 pagesIntroduction To Metabolism: Departemen Fisiologi Fakultas Kedokteran USUAnditha Namira RSNo ratings yet
- Itp Periop1Document4 pagesItp Periop1Irfan MohammadNo ratings yet
- Dia Care-2015-Huang-746-51 PDFDocument6 pagesDia Care-2015-Huang-746-51 PDFMohammad IrfanNo ratings yet
- Terapi AntiretroviralDocument13 pagesTerapi AntiretroviralthiamuthiaNo ratings yet
- Maternal Anatomy WilliamsDocument52 pagesMaternal Anatomy WilliamsIrfan MohammadNo ratings yet
- Dia Care 2015 Bellido 2211 6Document6 pagesDia Care 2015 Bellido 2211 6Irfan MohammadNo ratings yet
- CH08 Vaginal Breech DeliveryDocument25 pagesCH08 Vaginal Breech DeliveryShintaPuspitasariNo ratings yet
- Normal Newborn CareDocument49 pagesNormal Newborn CareIrfan MohammadNo ratings yet
- 1989 MollerDocument9 pages1989 MollerIrfan MohammadNo ratings yet
- 2005 HildingssonDocument7 pages2005 HildingssonIrfan MohammadNo ratings yet
- 1987 ReebDocument7 pages1987 ReebIrfan MohammadNo ratings yet
- 1987 ReebDocument7 pages1987 ReebIrfan MohammadNo ratings yet
- Dia Care 2015 Bellido 2211 6Document6 pagesDia Care 2015 Bellido 2211 6Irfan MohammadNo ratings yet
- Dia Care-2015-Zeitler-2285-92Document8 pagesDia Care-2015-Zeitler-2285-92Irfan MohammadNo ratings yet
- 1994 Al NasserDocument9 pages1994 Al NasserIrfan MohammadNo ratings yet
- Guidline EndocarditisDocument54 pagesGuidline EndocarditisIrfan MohammadNo ratings yet
- Antibiotic Treatment Strategies For Community Acquired Pneumonia in AdultsDocument12 pagesAntibiotic Treatment Strategies For Community Acquired Pneumonia in AdultsCumbelia PrimaNo ratings yet
- HipoglikemiaDocument12 pagesHipoglikemiaIrfan MohammadNo ratings yet
- Copd NICE GuidlinesDocument61 pagesCopd NICE GuidlinesIrfan MohammadNo ratings yet
- ITP BJH 2003Document23 pagesITP BJH 2003Mohammad IrfanNo ratings yet
- 2007 NiceDocument249 pages2007 NiceIrfan MohammadNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Assessment of Genetic Diversity in Sesame (Sesamum Indicum L.) Genotypes at Bako and Uke, Western OromiaDocument9 pagesAssessment of Genetic Diversity in Sesame (Sesamum Indicum L.) Genotypes at Bako and Uke, Western OromiaPremier PublishersNo ratings yet
- Correlation and RegressionDocument36 pagesCorrelation and Regressionanindya_kundu100% (3)
- Chapter One:: The Effect of Inflation On Poor People in HargeisaDocument42 pagesChapter One:: The Effect of Inflation On Poor People in Hargeisacankawaab75% (4)
- CSE602 - Data Warehousing & Data MiningDocument6 pagesCSE602 - Data Warehousing & Data MiningArun MohanNo ratings yet
- Hasil TraceDocument10 pagesHasil TraceHendri SaputraNo ratings yet
- Statistik Deskriptif N: Minimum Maximum Mean Std. DeviationDocument7 pagesStatistik Deskriptif N: Minimum Maximum Mean Std. DeviationLKP KHAFANo ratings yet
- AmphibianDocument13 pagesAmphibiandina AAAAANo ratings yet
- Pramodh TableauDocument3 pagesPramodh TableauAnushyantan NicholasNo ratings yet
- Estimasi Biaya - Kunci JawabanDocument55 pagesEstimasi Biaya - Kunci JawabanGita Akoeb100% (13)
- For Paul FurtonDocument93 pagesFor Paul FurtonaaronkaizenpagaranNo ratings yet
- Aidil - Comparison Trained and Untrained TeachersDocument4 pagesAidil - Comparison Trained and Untrained TeachersSeli adalah Saya50% (2)
- Direct From The Connoisseurs: Articulating Philippine Folk Dance Documentation PracticesDocument6 pagesDirect From The Connoisseurs: Articulating Philippine Folk Dance Documentation PracticesGab Mickaella Arias MatiasNo ratings yet
- R ProgrammingDocument1 pageR ProgrammingwhereareyoudearNo ratings yet
- Evans Analytics2e PPT 08Document73 pagesEvans Analytics2e PPT 08qunNo ratings yet
- Hodgetts The Impact of Autism Services On MothersDocument13 pagesHodgetts The Impact of Autism Services On MothersLisandra EmyNo ratings yet
- REGRESSION ANALYSIS 1 and 2 NotesDocument9 pagesREGRESSION ANALYSIS 1 and 2 NotesjayNo ratings yet
- VIFmodel 3Document2 pagesVIFmodel 3Van Joshua NunezNo ratings yet
- Bsu 305 Business Research Methods NotesDocument116 pagesBsu 305 Business Research Methods NoteskeymarbNo ratings yet
- 경통 기말족보Document4 pages경통 기말족보두씨망No ratings yet
- Sap Central Finance WhitepaperDocument14 pagesSap Central Finance WhitepaperKumar Abhishek100% (1)
- TCS Workforce Planning ForecastDocument109 pagesTCS Workforce Planning ForecastPragya Singh BaghelNo ratings yet
- Ebook PDF Using Multivariate Statistics 7th Edition by Barbara G Tabachnick PDFDocument41 pagesEbook PDF Using Multivariate Statistics 7th Edition by Barbara G Tabachnick PDFmartha.keener953100% (33)
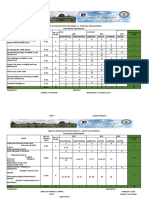
- Table of Specification For Grade 12 - Personal Development First Quarter ExaminationDocument17 pagesTable of Specification For Grade 12 - Personal Development First Quarter ExaminationArgie Joy Marie AmpolNo ratings yet
- Measuring Consumer Preferences for Sales Promotion SchemesDocument13 pagesMeasuring Consumer Preferences for Sales Promotion Schemesthinckollam67% (3)
- ANOVA ProblemsDocument13 pagesANOVA ProblemsAbhijeet Thamake100% (2)
- Barton, BiancaDocument12 pagesBarton, BiancaMARIEL ANTOINETTE DAGANGONNo ratings yet
- Get Annamalai University 1st and 2nd Year Assignment Solution 2020 Call 9025810064Document95 pagesGet Annamalai University 1st and 2nd Year Assignment Solution 2020 Call 9025810064Palaniappan NNo ratings yet
- Instagram Marketing: Driving Sales on Social MediaDocument4 pagesInstagram Marketing: Driving Sales on Social MediamarinaNo ratings yet
- RedSeer - Job Description - Associate ConsultantDocument3 pagesRedSeer - Job Description - Associate ConsultantAnshuman MohantyNo ratings yet
- CHAPTER XVVNNGCNDocument30 pagesCHAPTER XVVNNGCNJomar Peñaflor50% (2)