You might also like
- Adisa. Clinico-Pathological Profile of Head and Neck MalignanciesDocument31 pagesAdisa. Clinico-Pathological Profile of Head and Neck MalignanciesCarlos NaupariNo ratings yet
- Commentary: Provisional Restorations For Anterior ImplantsDocument1 pageCommentary: Provisional Restorations For Anterior ImplantsCarlos NaupariNo ratings yet
- Difficulty IndexDocument7 pagesDifficulty IndexRobins DhakalNo ratings yet
- 2014 Wittneben Rs Cementadas Vs Atornilladas ResaltadoDocument16 pages2014 Wittneben Rs Cementadas Vs Atornilladas ResaltadoCarlos NaupariNo ratings yet
- Dental Wear6Document9 pagesDental Wear6Carlos NaupariNo ratings yet
- 1 s2.0 S0002817714601173 MainDocument4 pages1 s2.0 S0002817714601173 MainCarlos NaupariNo ratings yet
- J 1600-0757 2007 00243 XDocument20 pagesJ 1600-0757 2007 00243 XCarlos NaupariNo ratings yet
- Monolithic CAD CAM Lithium Disilicate Versus VeneeredDocument10 pagesMonolithic CAD CAM Lithium Disilicate Versus VeneeredCarlos NaupariNo ratings yet
- Fisher 10 Años RCT HibridaDocument11 pagesFisher 10 Años RCT HibridaCarlos NaupariNo ratings yet
- The Microflora Adjacent To Ossointegrated Implants Supporting Maxillary Removable ProstheresDocument7 pagesThe Microflora Adjacent To Ossointegrated Implants Supporting Maxillary Removable ProstheresCarlos NaupariNo ratings yet
- Articulo ImplantesDocument9 pagesArticulo ImplantesCarlos NaupariNo ratings yet
- Fractura de Un Pilar PPFDocument3 pagesFractura de Un Pilar PPFCarlos NaupariNo ratings yet
- Protocolo Implantes Carga 3Document15 pagesProtocolo Implantes Carga 3Carlos NaupariNo ratings yet
- List Meta AnalisisDocument22 pagesList Meta AnalisisCarlos NaupariNo ratings yet
- TMD AnxiousDocument9 pagesTMD AnxiousCarlos NaupariNo ratings yet
- 1 s2.0 S0022391313600281 MainDocument8 pages1 s2.0 S0022391313600281 MainKiky COutezNo ratings yet
- 1 s2.0 S002239131360030X MainDocument6 pages1 s2.0 S002239131360030X MainAmar Bhochhibhoya100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Above Knee Amputation Exc PDFDocument5 pagesAbove Knee Amputation Exc PDFSenthilkumar ThiyagarajanNo ratings yet
- Soft Drinks in India: Euromonitor International February 2022Document27 pagesSoft Drinks in India: Euromonitor International February 2022Gayathri22394No ratings yet
- Methods of Investigating Brain and LanguageDocument12 pagesMethods of Investigating Brain and Languagekiranjit_123100% (2)
- Food Production (409) : Sample Question Paper Class X (2018-19) (NSQF)Document2 pagesFood Production (409) : Sample Question Paper Class X (2018-19) (NSQF)Janavi M SNo ratings yet
- Surgery Final NotesDocument81 pagesSurgery Final NotesDETECTIVE CONANNo ratings yet
- Pit VeriscolorDocument5 pagesPit VeriscolorNida Fithria FadhilaNo ratings yet
- Local Conceptual LiteratureDocument3 pagesLocal Conceptual LiteratureNatasha Althea Basada LegaspiNo ratings yet
- Professional Gatekeeping As A Function of Role FidelityDocument2 pagesProfessional Gatekeeping As A Function of Role FidelityNURSETOPNOTCHER100% (3)
- Research Paper For AbortionDocument10 pagesResearch Paper For AbortionMarevisha Vidfather75% (4)
- Proximal Humerus Fractures Epidemiology and TrendsDocument5 pagesProximal Humerus Fractures Epidemiology and TrendsHelena Sofia Fonseca Paiva De Sousa TelesNo ratings yet
- Dat IatDocument4 pagesDat Iatscribd birdNo ratings yet
- Mind Body PDFDocument357 pagesMind Body PDFAzhari RahmatNo ratings yet
- Rosemont Hill Health CenterDocument14 pagesRosemont Hill Health CenterMona SahooNo ratings yet
- A Plant-Growth Promoting RhizobacteriumDocument7 pagesA Plant-Growth Promoting RhizobacteriumdanyjorgeNo ratings yet
- L Sit ProgramDocument23 pagesL Sit Programdebo100% (1)
- Module 4Document107 pagesModule 4roseannurakNo ratings yet
- Environment in Palestine 1Document28 pagesEnvironment in Palestine 1YOSEF DERDESAWENo ratings yet
- Leaving Disasters Behind: A Guide To Disaster Risk Reduction in EthiopiaDocument12 pagesLeaving Disasters Behind: A Guide To Disaster Risk Reduction in EthiopiaOxfamNo ratings yet
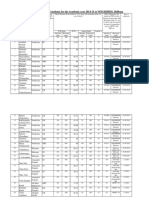
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Document10 pagesAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaNo ratings yet
- Stressors and Coping Mechanisms of Psychologically Distressed MSU-IIT StudentsDocument22 pagesStressors and Coping Mechanisms of Psychologically Distressed MSU-IIT StudentsDarleen Rizel CalumbaNo ratings yet
- Barriers To Bystander CPR in Deprived Communities: Findings From A Qualitative StudyDocument11 pagesBarriers To Bystander CPR in Deprived Communities: Findings From A Qualitative Studygevowo3277No ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.2Document4 pages1 - DS SATK Form - Initial Application of LTO 1.2cheska yahniiNo ratings yet
- Ecological PyramidsDocument19 pagesEcological Pyramidsnandhinidish100% (1)
- Allianz Care Plus Brochure Update 19mar2015 FA R3 5Document11 pagesAllianz Care Plus Brochure Update 19mar2015 FA R3 5Leonard Yang0% (1)
- Radiographic Cardiopulmonary Changes in Dogs With Heartworm DiseaseDocument8 pagesRadiographic Cardiopulmonary Changes in Dogs With Heartworm DiseaseputriwilujengNo ratings yet
- SImOS Nano-Tera 2013Document35 pagesSImOS Nano-Tera 2013nanoteraCHNo ratings yet
- Nursing Interventions for Ineffective Airway ClearanceDocument3 pagesNursing Interventions for Ineffective Airway Clearanceaurezea100% (3)
- Dapagliflozin Uses, Dosage, Side Effects, WarningsDocument8 pagesDapagliflozin Uses, Dosage, Side Effects, WarningspatgarettNo ratings yet
- Occipital LobesDocument46 pagesOccipital LobesLakshya J Basumatary100% (1)
- Speaking Level Placement Test Business English PDFDocument2 pagesSpeaking Level Placement Test Business English PDFLee HarrisonNo ratings yet