You might also like
- 2-Emdr Training WorksheetDocument3 pages2-Emdr Training Worksheetapi-273614596100% (12)
- Attacking Anxiety & Depression Workbook (2001) 6.0Document249 pagesAttacking Anxiety & Depression Workbook (2001) 6.0Anjoli Ortowski91% (11)
- RUDAS ScaleDocument2 pagesRUDAS ScaleAnonymous VG1IUtctb100% (1)
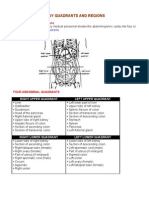
- Organs in The Body Quadrants and RegionsDocument3 pagesOrgans in The Body Quadrants and RegionsDavid HosamNo ratings yet
- CBT Manual for ASDDocument38 pagesCBT Manual for ASDSavu BogdanNo ratings yet
- Advantages Disadvantages: Sedative Premedication Guidelines at RCHDocument3 pagesAdvantages Disadvantages: Sedative Premedication Guidelines at RCHdwNo ratings yet
- Animal Vision EssayDocument6 pagesAnimal Vision EssayFarrah ZainolNo ratings yet
- Zoology Chapter 29Document100 pagesZoology Chapter 29Erika AquinoNo ratings yet
- Epworth Sleep ScaleDocument2 pagesEpworth Sleep ScalefreecouchNo ratings yet
- How Sleepy Are You 2Document1 pageHow Sleepy Are You 2api-321194246No ratings yet
- Epworth Sleepiness ScaleDocument1 pageEpworth Sleepiness ScaleMirza CoricNo ratings yet
- Stanford Sleepiness Scale and Epworth Sleepiness ScaleDocument3 pagesStanford Sleepiness Scale and Epworth Sleepiness ScalePalleti RenukaNo ratings yet
- The Epworth Sleepiness ScaleDocument1 pageThe Epworth Sleepiness ScaleAshok Kumar KrishnamoorthyNo ratings yet
- Patient Fatigue and Sleepiness AssessmentDocument2 pagesPatient Fatigue and Sleepiness Assessmentgitha noviaNo ratings yet
- Pelvic Pain Patient Initial QuestionnaireDocument6 pagesPelvic Pain Patient Initial QuestionnaireVaralakshmi UppuNo ratings yet
- Epworth Sleepiness ScaleDocument1 pageEpworth Sleepiness ScalebutterwalkerNo ratings yet
- Sinha Anxiety Scale in HindiDocument30 pagesSinha Anxiety Scale in HindiAnjali SahayNo ratings yet
- Assessing opioid withdrawalDocument3 pagesAssessing opioid withdrawalSergioMSaraivaNo ratings yet
- Fear QuestionnaireDocument3 pagesFear QuestionnaireTrinidad Cortés LópezNo ratings yet
- Adult NAC RevisedDocument26 pagesAdult NAC RevisedOsan BogdanNo ratings yet
- OET Test 10Document9 pagesOET Test 10shiela8329gmailcomNo ratings yet
- OA treatment goals and risk factorsDocument13 pagesOA treatment goals and risk factorsqartzzNo ratings yet
- OET Test 11Document10 pagesOET Test 11shiela8329gmailcomNo ratings yet
- 1600 12 BookDocument19 pages1600 12 Booktmhprinting1No ratings yet
- SF SleepQualityQuestionnaireDocument1 pageSF SleepQualityQuestionnaireNur DianaNo ratings yet
- HyperventilationDocument8 pagesHyperventilationRatu Pats LaubanNo ratings yet
- Mini-Mental State Examination (MMSE) : Date: OrientationDocument5 pagesMini-Mental State Examination (MMSE) : Date: OrientationCatria BerloiseNo ratings yet
- Epworth Sleepiness ScaleDocument1 pageEpworth Sleepiness ScaleTroy O'BrienNo ratings yet
- Understanding Neurological AssessmentDocument34 pagesUnderstanding Neurological AssessmentTcx YivcNo ratings yet
- Obsessive-Compulsive Disorder SectionDocument19 pagesObsessive-Compulsive Disorder Sectionark1974No ratings yet
- Sleep Plan: Part I: How Sleepy Are You?Document2 pagesSleep Plan: Part I: How Sleepy Are You?shawn1981No ratings yet
- Powered byDocument25 pagesPowered byAditi ParmarNo ratings yet
- Epworth Sleepiness Scale assessmentDocument1 pageEpworth Sleepiness Scale assessmentArik IskandarNo ratings yet
- EMDR WORKSHEET GUIDEDocument3 pagesEMDR WORKSHEET GUIDEKONSELOR SMAGLORIA2No ratings yet
- 4 Symphonies of StressDocument20 pages4 Symphonies of StressGordana KoturNo ratings yet
- PE Protocol With Details PDFDocument7 pagesPE Protocol With Details PDFDominic SloanNo ratings yet
- Zung SelfDocument6 pagesZung SelfRui PereiraNo ratings yet
- Questionnaire 1Document13 pagesQuestionnaire 1Laeeq R MalikNo ratings yet
- Act Epworth ScaleDocument2 pagesAct Epworth ScaleJanie VandeBergNo ratings yet
- TMD Disability IndexDocument2 pagesTMD Disability IndexSamuel Nanda LazuardiNo ratings yet
- Social Anxiety Workbook With PicturesDocument14 pagesSocial Anxiety Workbook With PicturesIulia StoianNo ratings yet
- EMDR Protocolo EstándarDocument11 pagesEMDR Protocolo Estándarrocio villalobosNo ratings yet
- ICBT Patient WorkbookDocument27 pagesICBT Patient WorkbookAnonymous Ax12P2sr100% (1)
- CHAPTER 3 Admission To HospitalDocument13 pagesCHAPTER 3 Admission To HospitalDaria BiancaNo ratings yet
- Trauma Screening Questionnaire (TSQ) : Your Own Reactions Now To The Traumatic EventDocument1 pageTrauma Screening Questionnaire (TSQ) : Your Own Reactions Now To The Traumatic EventJoRed357No ratings yet
- (D Doctor, P Patient) : Chapter 1: Molecular BiologyDocument13 pages(D Doctor, P Patient) : Chapter 1: Molecular BiologyVõ ĐứcNo ratings yet
- Updated Health Assessment Form With Scores 22-1-2023Document9 pagesUpdated Health Assessment Form With Scores 22-1-2023علي الخضيرNo ratings yet
- EMDR Intake PacketDocument6 pagesEMDR Intake PacketLaísNo ratings yet
- APA - DSM5 - Severity of Posttraumatic Stress Symptoms Adult PDFDocument3 pagesAPA - DSM5 - Severity of Posttraumatic Stress Symptoms Adult PDFStephanny Per EspitiaNo ratings yet
- Personal Stress Log: When Did It Situation Take Place? Stress Level ResponseDocument2 pagesPersonal Stress Log: When Did It Situation Take Place? Stress Level ResponseEdgar ManubagNo ratings yet
- Have You Taken Your MedicineDocument15 pagesHave You Taken Your MedicineabrahamisnanNo ratings yet
- Epn 2 Modul 1Document3 pagesEpn 2 Modul 1Ary FahrizanNo ratings yet
- The First 9 ChaptersDocument34 pagesThe First 9 ChaptersSherman KasavalNo ratings yet
- Clear & Simple Medical English in Dialogues: Vocabulary For ESL Health Care ProfessionalsFrom EverandClear & Simple Medical English in Dialogues: Vocabulary For ESL Health Care ProfessionalsNo ratings yet
- Understand Pain Live Well Again: Life Is Now (Tm)From EverandUnderstand Pain Live Well Again: Life Is Now (Tm)Rating: 5 out of 5 stars5/5 (1)
- Better Hearing: How to Improve Hearing without a Hearing Aid and Treat Tinnitus NaturallyFrom EverandBetter Hearing: How to Improve Hearing without a Hearing Aid and Treat Tinnitus NaturallyRating: 1 out of 5 stars1/5 (1)
- How To Release The Genius Within You To Rid Yourself Of Pain, Restore Normal Function, And Live A Life Of Vibrant Health And VitalityFrom EverandHow To Release The Genius Within You To Rid Yourself Of Pain, Restore Normal Function, And Live A Life Of Vibrant Health And VitalityNo ratings yet
- Prayers for Freedom over Worry and AnxietyFrom EverandPrayers for Freedom over Worry and AnxietyRating: 5 out of 5 stars5/5 (1)
- Auto Immune Disease and Fibromyalgia: The Traumatic Brain Injury Connection: TRAUMATIC BRAIN INJURY: TBI & POST-CONCUSSION SYNDOME: PCS, #3From EverandAuto Immune Disease and Fibromyalgia: The Traumatic Brain Injury Connection: TRAUMATIC BRAIN INJURY: TBI & POST-CONCUSSION SYNDOME: PCS, #3No ratings yet
- Clinical Lab FeesDocument1 pageClinical Lab FeesdwNo ratings yet
- Hypodontia Review - Good Paper PDFDocument9 pagesHypodontia Review - Good Paper PDFdwNo ratings yet
- Patient Presented With: - Mum (Claudia) Ially Follow-UpDocument1 pagePatient Presented With: - Mum (Claudia) Ially Follow-UpdwNo ratings yet
- Admission To Fellowship/Membership: Royal Australasian College of Dental SurgeonsDocument2 pagesAdmission To Fellowship/Membership: Royal Australasian College of Dental SurgeonsdwNo ratings yet
- AsdfDocument15 pagesAsdfdwNo ratings yet
- Outcomes and Prognostic Factors That Influence The SuccessDocument20 pagesOutcomes and Prognostic Factors That Influence The SuccessdwNo ratings yet
- JDocument2 pagesJdwNo ratings yet
- Clinical Lab FeesDocument1 pageClinical Lab FeesdwNo ratings yet
- Assignment Cover Sheet PDFDocument1 pageAssignment Cover Sheet PDFshuankayNo ratings yet
- Aggregatibacter Actinomycetemcomitans: The JP2 Genotype of and Marginal Periodontitis in The Mixed DentitionDocument7 pagesAggregatibacter Actinomycetemcomitans: The JP2 Genotype of and Marginal Periodontitis in The Mixed DentitiondwNo ratings yet
- Use of CBCT Guidance For Tooth Autotransplantation in ChildrenDocument8 pagesUse of CBCT Guidance For Tooth Autotransplantation in ChildrendwNo ratings yet
- AsdfDocument15 pagesAsdfdwNo ratings yet
- B KDocument2 pagesB KdwNo ratings yet
- Outcomes and Prognostic Factors That Influence The Success PDFDocument20 pagesOutcomes and Prognostic Factors That Influence The Success PDFdwNo ratings yet
- Dental Findings in Patients With Non-Surgical Hypoparathyroidism and Pseudohypoparathyroidism: A Systematic ReviewDocument15 pagesDental Findings in Patients With Non-Surgical Hypoparathyroidism and Pseudohypoparathyroidism: A Systematic ReviewdwNo ratings yet
- KuyfDocument10 pagesKuyfdwNo ratings yet
- FYIDocument1 pageFYIdwNo ratings yet
- Deps Et Al 2015 PDFDocument11 pagesDeps Et Al 2015 PDFdwNo ratings yet
- DCD Thesis Format Guidelines: Melbourne Dental SchoolDocument2 pagesDCD Thesis Format Guidelines: Melbourne Dental SchooldwNo ratings yet
- FYIDocument1 pageFYIdwNo ratings yet
- Bacteria That Cause Cavitation and Severe Early Childhood CariesDocument1 pageBacteria That Cause Cavitation and Severe Early Childhood CariesdwNo ratings yet
- IJPD Submission GuidelinesDocument9 pagesIJPD Submission GuidelinesdwNo ratings yet
- Lancet Kobrynski PDFDocument10 pagesLancet Kobrynski PDFdwNo ratings yet
- Words and Music by Leslie Jordan & David LeonardDocument1 pageWords and Music by Leslie Jordan & David LeonarddwNo ratings yet
- AsdfDocument3 pagesAsdfdwNo ratings yet
- Facial Dysmorphism: Causes and SyndromesDocument1 pageFacial Dysmorphism: Causes and SyndromesdwNo ratings yet
- Tree CuttingDocument1 pageTree CuttingdwNo ratings yet
- Singapore Zoo, Gardens & Top AttractionsDocument5 pagesSingapore Zoo, Gardens & Top AttractionsdwNo ratings yet
- TableeDocument1 pageTableedwNo ratings yet
- 282-Essentials of Pain Management-Nalini Vadivelu Richard D. Urman Roberta L. Hines-0387875786-Sp PDFDocument859 pages282-Essentials of Pain Management-Nalini Vadivelu Richard D. Urman Roberta L. Hines-0387875786-Sp PDFarief-024100% (2)
- Chapter 43 PosttestDocument6 pagesChapter 43 PosttestGamepage BuckNo ratings yet
- ACLS JeopardyDocument3 pagesACLS JeopardyLaylee Clare100% (1)
- CARDIOVASCULAR - SYSTEM Group No.3 MODULEDocument12 pagesCARDIOVASCULAR - SYSTEM Group No.3 MODULEDavid Paul LanuzaNo ratings yet
- hemiplegia دكتور عزونيDocument4 pageshemiplegia دكتور عزونيRaed AlhnaityNo ratings yet
- Janeways Immunobiology 9Th Edition Murphy Test Bank Full Chapter PDFDocument44 pagesJaneways Immunobiology 9Th Edition Murphy Test Bank Full Chapter PDFJamesWellsoeic100% (9)
- Pelod ScoreDocument7 pagesPelod ScoreAgus SarjonoNo ratings yet
- TonsillectomyDocument27 pagesTonsillectomyRho Vince Caño MalagueñoNo ratings yet
- RTO Z6P5CMB Paket1UASGanjil20182019 PDFDocument20 pagesRTO Z6P5CMB Paket1UASGanjil20182019 PDFGlorya ValensiaNo ratings yet
- How to Dilute Blood and Count White Blood CellsDocument2 pagesHow to Dilute Blood and Count White Blood CellsAlfred ChowNo ratings yet
- The Acute NeurologiDocument343 pagesThe Acute Neurologizee zeeNo ratings yet
- Fungsi Otot-OtotDocument32 pagesFungsi Otot-OtothansenpanjaitanNo ratings yet
- Fantasy/Imagination: Patti M. ValkenburgDocument3 pagesFantasy/Imagination: Patti M. ValkenburgalbertoadalidNo ratings yet
- Endocrine Emergencies CompiledDocument102 pagesEndocrine Emergencies CompiledSubhkanish RavindraNo ratings yet
- PNTD 0005534 s001Document22 pagesPNTD 0005534 s001Paolo VidalNo ratings yet
- Adaptasi Biota LautDocument19 pagesAdaptasi Biota LautBudhi Agung Prasetyo100% (1)
- Yamamoto Acupuncture PDFDocument17 pagesYamamoto Acupuncture PDFcarlos100% (1)
- PrefixDocument6 pagesPrefixbingkydoodle1012No ratings yet
- Hematological and Metabolical Aspects From Laboratory MediDocument109 pagesHematological and Metabolical Aspects From Laboratory MediNadirNo ratings yet
- February Month Brain DiscussionDocument63 pagesFebruary Month Brain DiscussionJulyhathul KuraishiNo ratings yet
- TRACHEA With TransDocument56 pagesTRACHEA With TransLarry YuloNo ratings yet
- Frazeologie EnglezaDocument11 pagesFrazeologie EnglezaMaria MkNo ratings yet
- Biology: Sexual ReproductionDocument7 pagesBiology: Sexual ReproductionAllan BustamanteNo ratings yet
- 18 Tricks To Teach Your BodyDocument4 pages18 Tricks To Teach Your BodyigiNo ratings yet
- Microsyllabus BSC 301Document9 pagesMicrosyllabus BSC 301Anwita JhaNo ratings yet
- Journal Pre-Proof: Journal of Pediatric and Adolescent GynecologyDocument3 pagesJournal Pre-Proof: Journal of Pediatric and Adolescent Gynecologyxavi5_5No ratings yet
- Full Download Holes Human Anatomy and Physiology 15th Edition Shier Solutions ManualDocument35 pagesFull Download Holes Human Anatomy and Physiology 15th Edition Shier Solutions Manualbarovert.o87w100% (29)